Back to Journals » Risk Management and Healthcare Policy » Volume 19
Optimizing Health Insurance Claims Processing: The Role of Clinical Documentation Improvement (CDI)
Authors Alumran A ![]() , Aljurbua LI, Bashmakh N, Alakrawi Z, Alrayes SA
, Aljurbua LI, Bashmakh N, Alakrawi Z, Alrayes SA ![]() , AlQahtani SM
, AlQahtani SM
Received 15 December 2025
Accepted for publication 3 April 2026
Published 11 April 2026 Volume 2026:19 586134
DOI https://doi.org/10.2147/RMHP.S586134
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Mecit Can Emre Simsekler
Arwa Alumran,1 Lamis Ibrahim Aljurbua,1 Nada Bashmakh,1 Zahraa Alakrawi,1 Saja A Alrayes,1 Saad M AlQahtani2
1Department of Health Information Management and Technology, College of Public Health, Imam Abdulrahman bin Faisal University, Dammam, Saudi Arabia; 2Department of Orthopedics Surgery, College of Medicine, Imam Abdulrahman bin Faisal University, Dammam, Saudi Arabia
Correspondence: Arwa Alumran, Department of Health Information Management and Technology, College of Public Health, Imam Abdulrahman bin Faisal University, Dammam, 31952, Saudi Arabia, Email [email protected]
Background and Objectives: Clinical Documentation Improvement (CDI) programs have been identified as a financial risk reduction strategy and are becoming increasingly important in payer-provider alignment. This study aimed to evaluate the effect of CDI on insurance claim denials in the context of the healthcare sector in Saudi Arabia and the Vision 2030 healthcare transformation plan.
Methods: A cross-sectional study of secondary data from two public healthcare facilities in Eastern Saudi Arabia. A total of 203 insurance claim denials (2023– 2024 data) were analyzed. Denial reasons, CDI implementation, and patient characteristics were the study variables.
Results: Among the rejected insurance claims, 52.7% of the denials were due to policy, declaration, and billing issues, and 47.3% were due to documentation issues. Denial reasons were significantly different between the two study hospitals. Documentation-related denials were significantly higher in the absence of CDI implementation (86.2%), whereas policy and billing issues were predominant in the hospital with CDI implementation (92%). The absence of CDI implementation was strongly associated with documentation-related denials (OR=73.07). Female patients had lower odds of insurance claim denials (OR=0.055, p< 0.001). Diagnosis was significantly associated with denial reasons (χ2=119.152, p< 0.001).
Conclusion: CDI implementation is associated with a substantial reduction in documentation-related insurance claim denials and policy and billing issues. This study highlights the role of documentation in financial risk reduction and the importance of CDI implementation in healthcare facilities in the context of the healthcare sector in Saudi Arabia and the Vision 2030 healthcare transformation plan.
Keywords: clinical documentation improvement, CDI, insurance claims denials, medical coding, patient records, healthcare systems, healthcare informatics, healthcare quality, documentation accuracy
Introduction
The Health Sector Transformation Program, under the Saudi Vision 2030 initiative, is designed to fundamentally reform healthcare in the Kingdom of Saudi Arabia by improving quality, expanding accessibility, and ensuring financial sustainability.1 In addition, one of the goals of Saudi Vision 2030 was the health sector transformation program, as it aims to privatize the health system, which will oblige health institutions to deal with insurance companies. In this context, insurance claim denial is not only a management problem but also a substantial financial risk for healthcare organizations, which affects their revenue streams and hence their sustainability.
As insurance companies scrutinize claims more closely to ensure proper diagnoses, hospitals work to minimize claim rejections in order to maximize revenues.2 However, documentation deficiencies are often a key factor contributing to insurance claim denials.3,4 As reported by Glance,5 almost 30% of health insurance claims in Saudi Arabia were rejected, with inadequate or improper documentation being a major contributing factor. Improving documentation practices and streamlining the claims process will be crucial for achieving the goals of the Health Sector Transformation Program and ensuring financial sustainability of the healthcare system.
From a risk management viewpoint, insurance claim denial is a systemic risk in the processes and systems of healthcare organizations that needs to be addressed through targeted interventions. Improving documentation practices and streamlining the claims process will be crucial for achieving the goals of the Health Sector Transformation Program and ensuring financial sustainability of the healthcare system.
Maintaining good standards of clinical documentation remains a problem in the health service.6 The pivotal role of accurate and meticulously maintained medical records cannot be overstated as they are essential for overcoming such challenges.7 This highlights the critical need for programs like Clinical Documentation Improvement (CDI), which aim to enhance the quality and organization of clinical data.8 In response, many hospitals have established Clinical Documentation Improvement (CDI) departments that work to reduce irrelevant information and clarify any missing or ambiguous data in patients’ medical records.9
CDI plays an essential role in healthcare organizations by ensuring comprehensive documentation of patient encounters, equipping care teams with essential information to deliver effective treatment.10 Improving documentation practices and streamlining the claims process will be crucial for achieving the goals of the Health Sector Transformation Program and ensuring financial sustainability of the healthcare system.
CDI programs have been widely implemented across the world, especially in the United States and other high-income healthcare systems, and have been associated with improved coding accuracy, reduced insurance claim denial, and better revenue cycle management. CDI is therefore recognized as a risk management tool for healthcare systems to mitigate losses due to documentation deficiencies.
Despite the changing nature of healthcare delivery and the increasing burden on healthcare professionals, the effect of CDI on insurance claim denials has received little attention in the literature, particularly within the Saudi Arabian context. This study seeks to investigate the relationship between CDI implementation and insurance claim denials within Saudi Arabia’s healthcare system. By identifying common reasons for health insurance claims denials in Saudi hospitals, determine the association between these denials and the implementation of Clinical Documentation Improvement (CDI) programs, and investigate additional variables that may influence these denials. The findings provide valuable insights into healthcare practices and policies in Saudi Arabia, contributing to improved health insurance claim processes.
Methods
Study Design
This study employs a quantitative, cross-sectional research design using secondary data from two different hospitals regarding their insurance claims.
Study Settings
The study is conducted in two public hospitals in Eastern Saudi Arabia. One of the hospitals have a Clinical Documentation Improvement (CDI) unit, while the other does not. The two hospitals are similar in their size and the service provided. Both hospitals are governmental secondary hospitals with business centers where they provide paid services.
Participants
Insurance claims from the two hospitals in the study are studied using stratified sampling approaches to recruit a sample of 203 rejected insurance claims. The claims are evenly distributed between hospitals that have CDI units and those that do not.
Inclusion Criteria
Insurance claims that were submitted within the chosen study period (January 2023 to December 2024) are included in this study. Insurance claims related to inpatient encounters in chosen healthcare facilities and processed through standardized coding systems such as ICD-10-AM and ACHI were included. Insurance claims that completed the entire process (ie, submitted to the insurance and processed to a final decision such as approval or rejection) were included. Insurance claims that were complete, including patient demographics, clinical diagnoses, procedures, and corresponding codes, were considered for this study.
Exclusion Criteria
Insurance claims that were not complete or lacked information on key variables such as patient demographics, clinical diagnoses, and procedures, and/or contained data entry errors that could not be verified or corrected were excluded from this study. Insurance claims that were duplicate or not yet processed to a final decision and were awaiting approval or rejection were also not included. Insurance claims related to outpatient services, not covered services, or administrative claims such as canceled or test claims were not included in this study.
Variables
The study will include the total number of insurance claims in each hospital in the period 2023, the total rejected claims, the total approved claims, and reasons for claims rejection. Other variables might be available upon collection of the data.
Data Sources/Measurement
Secondary data from hospital records will be collected using Excel sheets. Relevant health insurance claim data can be systematically extracted and organized with the help of this tool. Recorded variables include the date of the claim, the status of the approval, the reason for the denial, and the presence of the CDI unit.
Ethical approval for this study was granted by the Institutional Review Board of Imam Abdulrahman bin Faisal University, Dammam (IRB-UGS-2024-03-094), in line with the Declaration of Helsinki. The study used existing hospital records and did not involve any direct contact with patients. Because of this, the Institutional Review Board waived the requirement for individual informed consent, as the study posed minimal risk. Patient privacy was carefully protected by anonymizing all data before analysis. The data were handled confidentially, accessed only by the research team, and stored securely in a password-protected electronic system.
Study Size
If we estimated the annual number of insurance claims in the study hospitals to be 20,000. The minimum estimated sample size would be 203 claims, with a sample proportion of 50%, 95% confidence level, and 7% margin of error using the formula denoted by Daniel.11
Statistical Analysis
The Statistical Package for the Social Sciences (SPSS) software, version 29, will be used to analyses the data that has been gathered. Data will be summarized using frequencies and percentages, while bivariate analyses will be conducted using chi-square test. Further analysis will include binary logistic regression to assess the odds ratio relevant to having a CDI unit. The analysis aims to provide insights into the relationship between CDI implementation and insurance claim outcomes, guiding future healthcare practices and policy decisions.
Results
A total of 203 rejected insurance claims from the year 2023 were analyzed. Table 1 summarizes the distribution and characteristics of these claims. Half of the rejected claims (n= 101) originated from the hospital that implemented Clinical Documentation Improvement (CDI). The reasons for rejection were categorized into Policy and Declaration Issues or Billing and Financial (n= 107, 52.7%), and Documentation and Information Issues (n= 96, 47.3%).
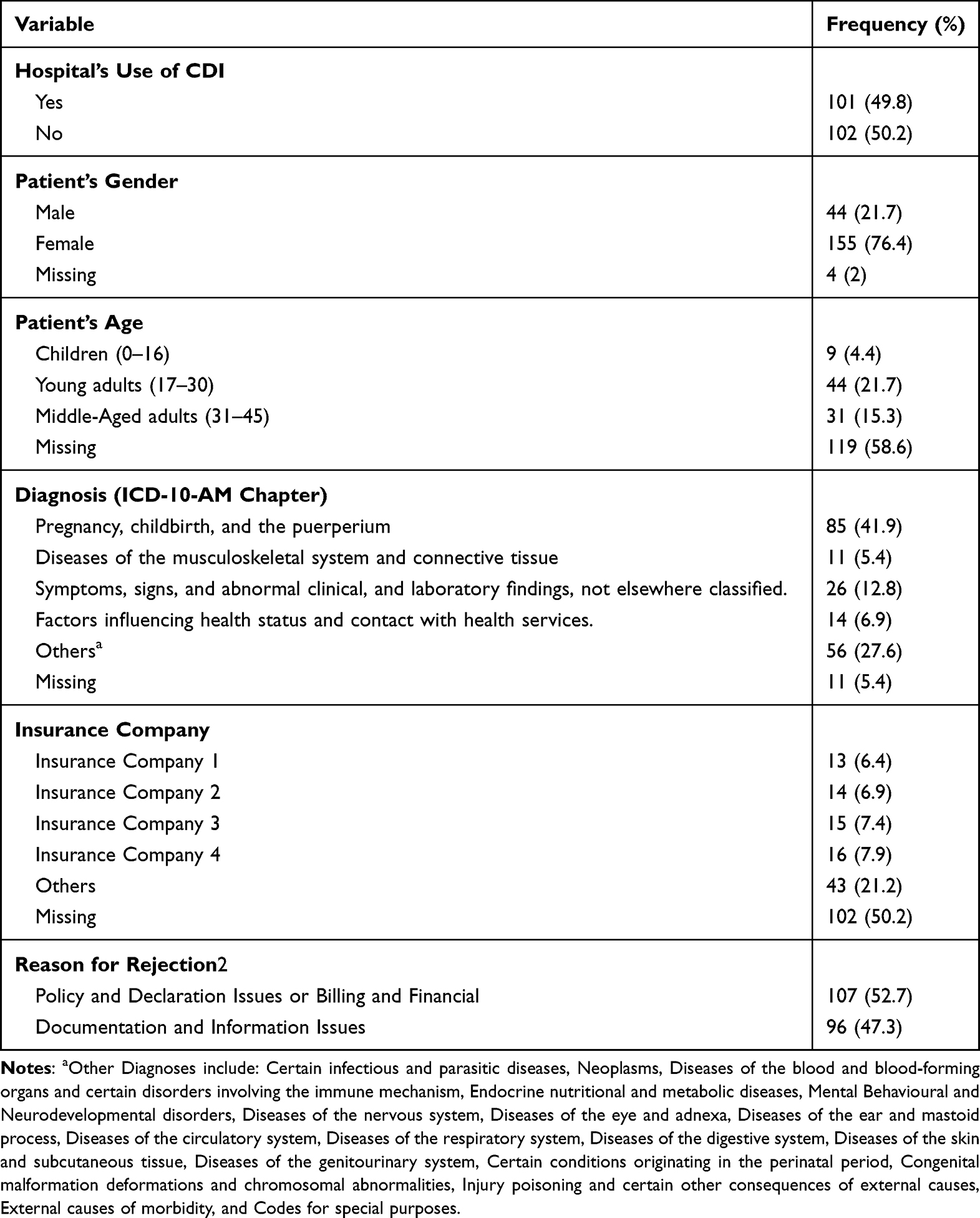 |
Table 1 Univariate Analysis of Factors Associated with Insurance Claim Rejections, Including Hospital CDI Use, Patient Characteristics, and Diagnosis Categories |
Regarding gender, the majority of claimants were female (n= 155, 76%). Age groups were segmented into children (0 to 16 years old, 4%), young adults (17 to 30 years old, 21%), and middle-aged adults (31 to 45 years old, 15%). In addition, among the 203 rejected claims, 28.6% (n= 58) were evenly distributed among four insurance companies.
Claims diagnoses were categorized according to the ICD-10-AM chapters (see Table 1). The highest proportion of diagnoses fell under the chapter for pregnancy, childbirth, and the puerperium (n= 85, 42%), followed by Symptoms, signs, and abnormal clinical, and laboratory findings, not elsewhere classified (n= 26, 13%).
As shown in Table 2, bivariate analysis indicated significant differences in reasons for rejection between hospitals with and without CDI implementation (x2= 124.992, P<0.001, Figure 1). The hospital without CDI primarily faced rejections due to documentation and information issues (n= 88, 86.2%), whereas the hospital with CDI saw more rejections due to policy and declaration issues or billing and financial issues (n= 93, 92%).
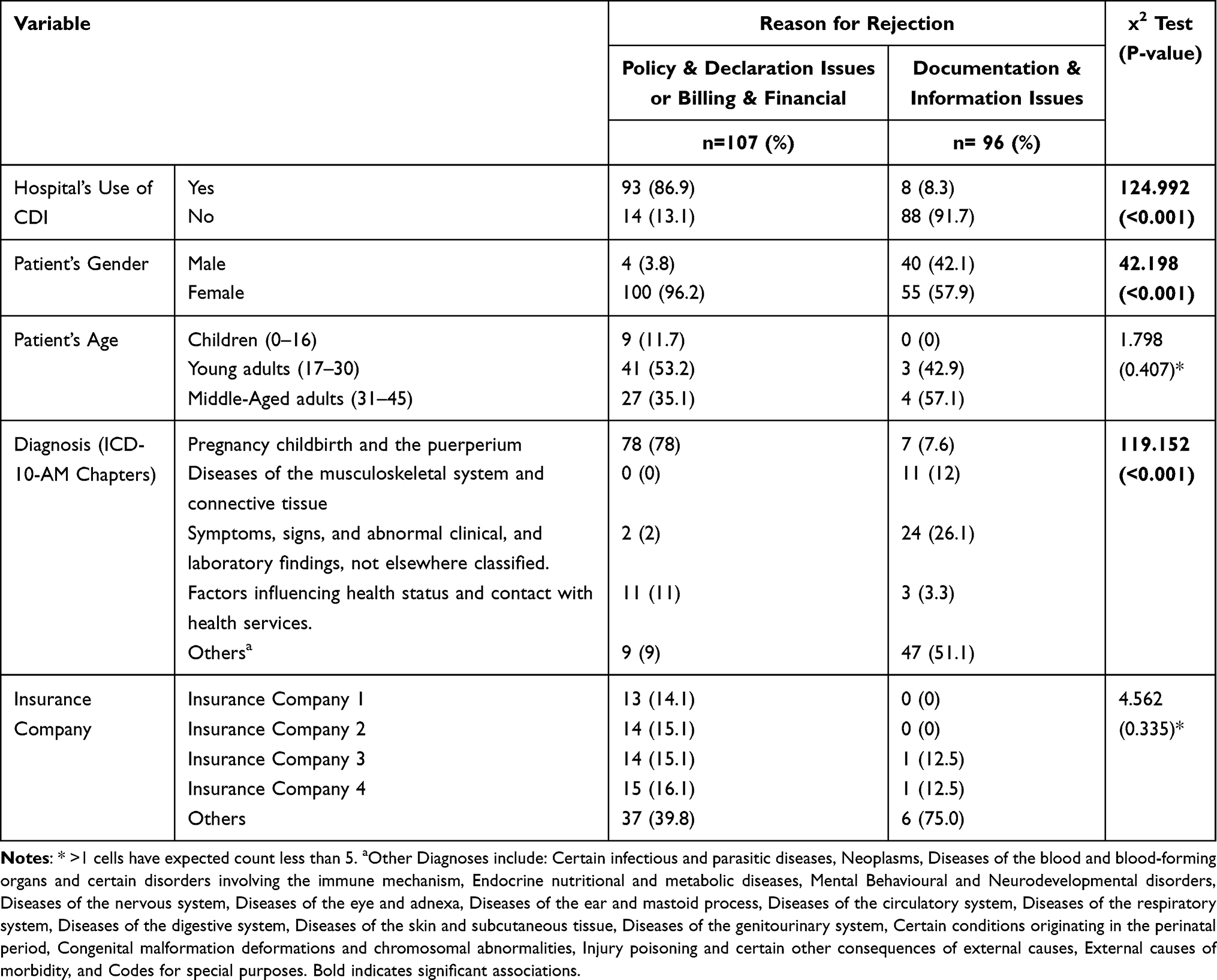 |
Table 2 Bivariate Analysis of Factors Influencing Insurance Claim Rejections Due to Policy, Billing, and Documentation Issues |
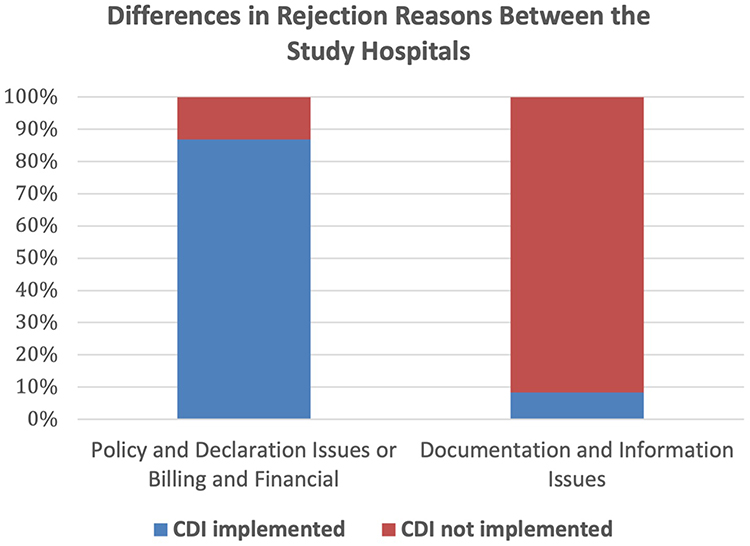 |
Figure 1 Differences in Rejection Reasons Between the Study Hospitals. |
Significant differences in rejection reasons were also observed between genders (x2= 42.198, P<0.001, Table 2). The majority of rejections among females were related to policy and declaration issues or billing and financial issues (n= 100, 64.5%).
Diagnosis significantly influenced claim denials (x2= 119.152, P<0.001). Claims related to pregnancy, childbirth, and the puerperium had the highest denial rate due to policy and declaration issues or billing and financial issues (78%, n= 78). Conversely, claims related to Factors influencing health status and contact with health services had the lowest denial rate (3.3%, n= 3) for documentation and information issues (Table 2).
Logistic regression analysis (shown in Table 3) highlighted the impact of CDI on claim denials, showing significantly higher odds of denial due to documentation issues when CDI was not implemented (OR= 73.07, 95% CI [29.23, 182.67], P<0.001). Females exhibited significantly lower odds of claim denial compared to males (OR=0.055, 95% CI [0.019, 0.162], P<0.001). Patient age, diagnosis, and insurance company did not show significant associations with claim denial.
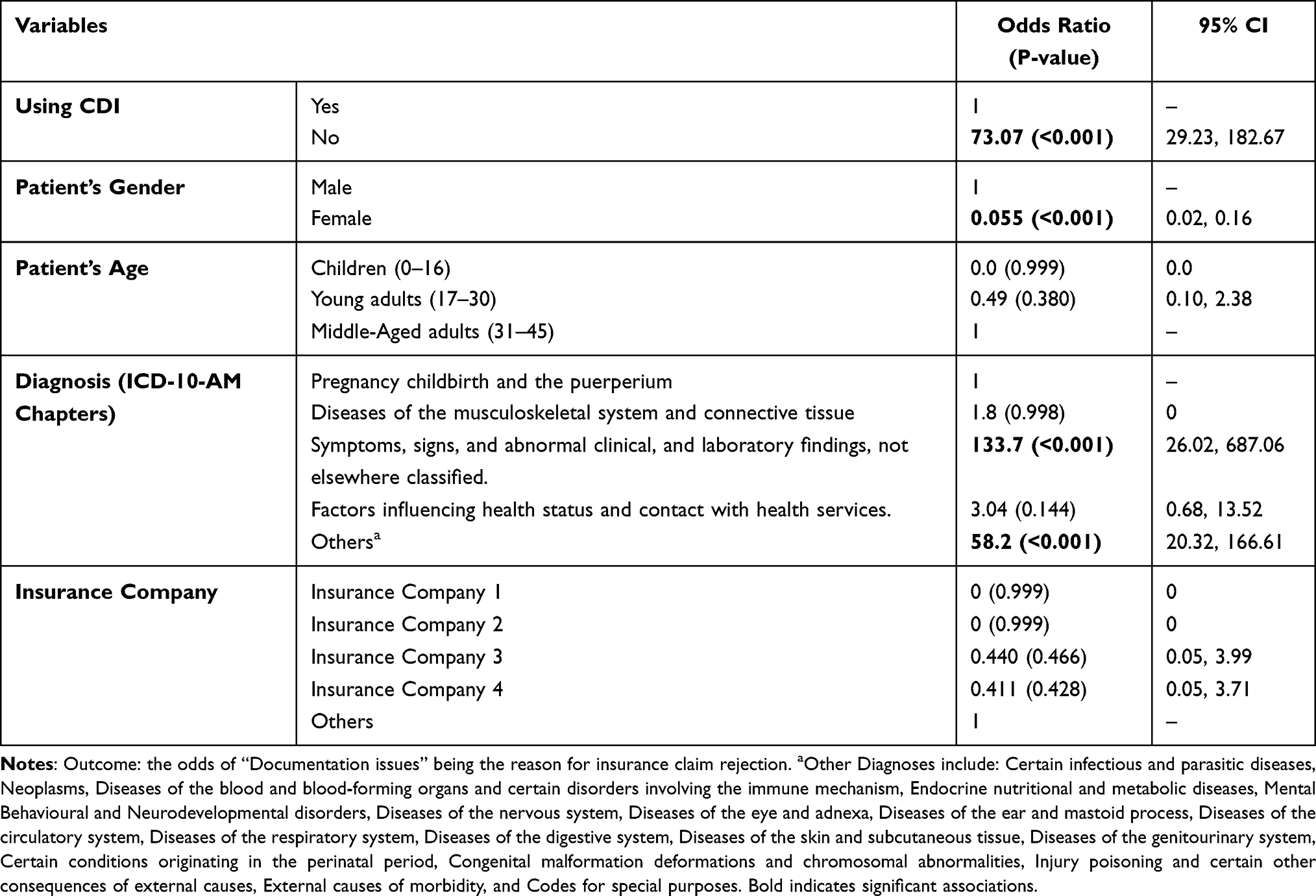 |
Table 3 Binary Logistic Regression to Find the Crude Odds Ratio |
Discussion
The study found that Clinical Documentation Improvement (CDI) programs significantly reduce insurance claim denials due to documentation issues in Saudi hospitals. Hospitals with activated CDI units experienced fewer rejections related to documentation errors compared to those without CDI programs.
The study underscores the importance of CDI in improving documentation accuracy and completeness, leading to fewer claim denials. This aligns with the goals of the Saudi Vision 2030 Health Sector Transformation Program, which aims to enhance healthcare quality and financial sustainability. The implementation of CDI programs emerges as an important factor influencing the probability of claims denial due to documentation issues. This aligns with the research objectives of identifying common reasons for health insurance claims denials and determining the impact of CDI programs.
The result in the study shows that the odds of having a denied claim if the study does not have CDI is 73 more times higher than if the study hospital had a CDI program. This underscores the importance of CDI in reducing documentation deficiencies that lead to claims denials. This finding is consistent with existing literature,9,12 which highlights the role of CDI in improving the accuracy and completeness of clinical documentation. CDI programs serve as a bridge between clinicians and coding staff, ensuring that medical records accurately reflect the care provided, thereby minimizing the likelihood of denials based on insufficient or ambiguous documentation.
The study identifies patient gender as another significant factor influencing claims denial, with females demonstrating lower odds of denial compared to males. While the reason behind this gender disparity in claims denials is that the hospital implementing CDI was a maternity hospital. While patient gender and diagnosis may influence healthcare utilization and coding practices,13 however, the study signifies that their impact on claims denials appears to be mediated by the presence of CDI programs rather than their actual impact. In addition, patient age, diagnosis, and insurance company did not show significant influence on claims denials in both study hospitals.
CDI improves the accuracy and completeness of clinical documentation, thereby reducing the probability of claims denials. However, it is essential to know that CDI represents an approach to addressing documentation issues rather than a strategy to prevent them. Thus, while CDI programs reduce the consequences of poor documentation, they do not address the root causes of documentation deficiencies, such as inadequate training, time constraints, or system inefficiencies.14
The study’s strengths lie in its exploration of Clinical Documentation Improvement (CDI) in the context of Saudi Arabia, an area relatively unexplored in the kingdom. Being among the first to delve into the relationship between CDI and insurance claim denials in Saudi hospitals, this research fills a significant gap in the existing literature. Furthermore, its potential utility to the Ministry of Health in Saudi Arabia cannot be understated, as understanding the impact of CDI on insurance claim denials can inform policy decisions aimed at improving healthcare quality and financial stability.
However, several weaknesses should be acknowledged. Firstly, the nascent stage of CDI implementation in Saudi hospitals poses a challenge, as it may not yet represent best practices. This limitation underscores the need for cautious interpretation of the results, recognizing that CDI practices may still be evolving. Additionally, the sensitivity and confidentiality of information contained in insurance claims presented hurdles in data collection. Difficulty in accessing necessary data from hospitals may have limited the comprehensiveness of the study’s findings. In addition, the analysis is limited to rejected claims only, which may restrict insights into overall claim approval dynamics.
Despite these limitations, the study provides valuable insights into the role of CDI in mitigating insurance claim denials in Saudi healthcare settings. Moving forward, it is crucial for future research to continue monitoring the evolution of CDI practices in Saudi hospitals and to explore additional factors influencing insurance claim outcomes. Moreover, efforts to facilitate data access and enhance collaboration with hospitals can strengthen future research endeavors in this area.
Conclusion
The research aimed to understand the impact of Clinical Documentation Improvement (CDI) programs on insurance claim denials in Saudi Arabia’s healthcare system. Specifically, it focused on identifying common reasons for claim denials, assessing the relationship between CDI implementation and claim denials, and investigating other influencing variables. Data was collected from two hospitals, one with a CDI program and one without, and analyzed using various statistical methods.
The study underscores the critical role of CDI in improving documentation accuracy and completeness, thereby mitigating the risk of insurance claim denials. By identifying common reasons for claim denials and assessing the impact of CDI implementation, the research contributes to enhancing healthcare quality and financial stability of the healthcare facilities. The findings suggest that hospitals with CDI units experience fewer claim denials related to documentation deficiencies compared to those without such programs.
From a policy standpoint, these results lend support to further integrating CDI programs into Saudi Arabia’s ever-evolving healthcare landscape. However, there is also the possibility of challenges arising in scaling up the implementation of CDI programs nationwide. These challenges include differences in resources available in each institution, workforce needs, training needs, as well as differences in health information technology. These issues will need to be tackled by developing national guidelines, workforce development, as well as provider-insurer alignment.
Additionally, it is essential to recognize the practical implications of these reported findings. Recommendations include the continued promotion and implementation of CDI programs in Saudi hospitals to address documentation deficiencies effectively. Moreover, ongoing monitoring and evaluation of CDI practices are crucial to ensure their effectiveness and alignment with evolving healthcare needs. It is recommended that future research studies examine additional factors that impact insurance claim results and also examine ways to address the underlying causes of documentation deficits beyond CDI implementation, especially system wide.
Future research endeavors should explore additional factors influencing insurance claim outcomes and investigate strategies to address root causes of documentation deficiencies beyond CDI implementation.
This study, to the best of researchers’ knowledge, is the first study that has been done in Saudi Arabia to address the impact of the CDI programs on revenue cycle in healthcare in terms of claim denials. In fact, his study contributes to advancing our understanding of the role of CDI in mitigating insurance claim denials in the context of the Saudi healthcare system. By bridging the gap between clinical practice and administrative processes, CDI programs offer promising avenues for improving healthcare quality, financial sustainability, and patient outcomes.
Data Sharing Statement
Data can be available from the corresponding author upon request.
Ethical Approval
Ethical approval for this study was granted by the Institutional Review Board of Imam Abdulrahman bin Faisal University, Dammam (IRB-UGS-2024-03-094), in line with the Declaration of Helsinki. The study used existing hospital records and did not involve any direct contact with patients. Because of this, the Institutional Review Board waived the requirement for individual informed consent, as the study posed minimal risk. Patient privacy was carefully protected by anonymizing all data before analysis. The data were handled confidentially, accessed only by the research team, and stored securely in a password-protected electronic system.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There was no source of funding for this research.
Disclosure
The authors report no conflict of interest relevant to this work.
References
1. Saudi Vision 2030. Vision 2030 Web site. [updated 2018]. Available from: https://vision2030.gov.sa/en.
2. Rahman R. The privatization of health care system in Saudi Arabia. Health Serv Insights. 2020;13(1):1178632920934497. doi:10.1177/1178632920934497
3. Opoku K. A Predictive Model of Finance Claims Rejection Under the National Health Insurance Scheme: A Case Study of Selected Health Service Providers in Ashanti Region. University of Cape Coast; 2017.
4. Veazie JI. Take control of your cash: top payer reasons for claim denials. Health Care Collect. 2018;32(2):5.
5. Glance. 9 Reasons health claims are being rejected or denied by insurance in Saudi Arabia. Available from: https://www.glance.care/industry-updates/9-reasons-health-claims-rejected-saudi-arabia/.
6. Farhan J, Al-Jummaa S, Al-Rajhi A, Al-Rayes H, Al-Nasser A. Documentation and coding of medical records in a tertiary care center: a pilot study. Ann Saudi Med. 2005;25(1):46–9. doi:10.5144/0256-4947.2005.46
7. Binfoh K, Agyeman C, Lakhawat P. Assessing the dimensions of hospital records (Medical Records) in delivering quality of service to patients. PharmaTutor. 2018;6(8):1–8. doi:10.29161/PT.v6.i8.2018.1
8. Danzi J, Masencup B, Brucker M, Dixon-Lee C. Case study: clinical documentation improvement program supports coding accuracy. Top Health Inf Manage. 2000;21(2):24–29.
9. Baksh AS. The importance of clinical documentation improvement. Appl Res Proj. 2018;53(1). doi:10.21007/chp.hiim.0053
10. Hess PC. Clinical Documentation Improvement: Principles and Practice.
11. Daniel W. Biostatistics: A Foundation for Analysis in the Health Sciences.
12. Wilson LN. The impact of a clinical documentation improvement program. Indiana University; 2009. Available from: https://scholarworks.iupui.edu/handle/1805/1986.
13. Redondo-Sendino Á, Guallar-Castillón P, Banegas JR, Rodríguez-Artalejo F. Gender differences in the utilization of health-care services among the older adult population of Spain. BMC Public Health. 2006;6(1):155. doi:10.1186/1471-2458-6-155
14. Rouse M, Jones M, Zogleman B, May R, Ekilah T, Gibson C. Resident integration with inpatient clinical documentation improvement: a quality improvement project. BMJ Open Qual. 2022;11(2):e001300. doi:10.1136/bmjoq-2020-001300
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.