Back to Journals » Drug Design, Development and Therapy » Volume 20
Optimizing Colistin Sulfate Dosing in Severe Infections: A Population Pharmacokinetic Model-Guided Approach
Authors Ma Y, Wang Y, Wu X, Wang J, Pang Y, Jia Y, Yang X, Gu J
Received 3 February 2026
Accepted for publication 6 June 2026
Published 15 June 2026 Volume 2026:20 600942
DOI https://doi.org/10.2147/DDDT.S600942
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Anastasios Lymperopoulos
Yingchao Ma,1 Yongjing Wang,1 Xia Wu,1 Jin Wang,1 Yimeng Pang,2 Yaqiang Jia,3 Xiuling Yang,1 Jianjun Gu4
1Department of Pharmacy, The Second Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050051, People’s Republic of China; 2School of Pharmacy, Hebei Medical University, Shijiazhuang, Hebei, 050017, People’s Republic of China; 3Tianjin L’Hospital Medical Research Co., Ltd, Tianjin, 300450, People’s Republic of China; 4Department of Cardiac Surgery, the second Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050051, People’s Republic of China
Correspondence: Jianjun Gu, Department of Cardiac Surgery, The Second Hospital of Hebei Medical University, 215# Heping West Road, Shijiazhuang, Hebei, 050051, People’s Republic of China, Email [email protected] Xiuling Yang, Department of Pharmacy, The Second Hospital of Hebei Medical University, 215# Heping West Road, Shijiazhuang, Hebei, 050051, People’s Republic of China, Email [email protected]
Abstrcat:
Background: Colistin sulfate is effective against carbapenem-resistant Gram-negative bacilli but has a narrow therapeutic window, large pharmacokinetic variability, and high resistance risk. Clinical data remain limited, and individualized dosing guidance is urgently needed. This study aims to establish a population pharmacokinetic (PPK) model to optimize and guide precise individualized dosing of colistin sulfate in critically ill patients.
Methods: Critically ill patients with confirmed CRO infections receiving intravenous colistin sulfate at the Second Hospital of Hebei Medical University from June 2021 to June 2023 were enrolled. A PPK model was developed using NONMEM. Goodness-of-fit (GOF) diagnostics and visual predictive check (VPC) were used to evaluate the predictive performance of the model, while the bootstrap method (BS) was used to assess its stability. Clinical efficacy, microbiological efficacy, and adverse reactions were assessed. Monte Carlo simulation calculated the probability of target attainment (PTA) across different MICs and renal function strata to optimize the colistin sulfate dosing regimen.
Results: Among 51 patients, clinical efficacy was 60.78% (31/51), bacterial clearance 52.94% (27/51), and nephrotoxicity 3.92% (2/51). The PPK model included 123 concentration points (range: 0.12– 4.40 mg/L).A one-compartment linear elimination model best described the PK profile. Typical values of clearance (CL) and volume of distribution (V) were 1.66 L/h and 10.10 L, respectively. Creatinine clearance (CrCL) was identified as a significant covariate affecting CL. Monte Carlo simulation showed that the recommended regimen achieved PTA ≥ 90% only when MIC ≤ 0.5 μg/mL with normal renal function. When MIC ≥ 1 μg/mL, there was a risk of insufficient exposure in patients with normal renal function. When MIC ≥ 2 μg/mL, no dosing regimen achieved PTA ≥ 90%.
Conclusion: Renal function significantly impacts colistin sulfate clearance. Dose adjustment based on CrCL is necessary. The standard dosing regimen risks underexposure in patients with normal renal function and MIC ≥ 1 mg/L. Off-label high-dose regimens should be considered in such cases to ensure adequate drug exposure.
Keywords: colistin sulfate population pharmacokinetics patients with severe infections, administration protocol, precision medication
Introduction
The widespread use of carbapenem antibiotics has led to the emergence and rapid dissemination of carbapenem-resistant gram-negative organisms (CRO), which now represent a significant public health challenge and complicate infection management.1,2 The economic burden associated with CRO infections, including prolonged hospital stays, increased healthcare costs, and higher mortality rates, further exacerbates this public health crisis. Due to the scarcity of new antibacterial agents, polymyxin drugs, previously abandoned because of their nephrotoxicity and neurotoxicity, have been reintroduced in clinical settings due to their potent antibacterial activity against CRO, positioning them as the last line of defense for treating these infections.
The currently available polymyxin drugs include polymyxin B sulfate, colistin methanesulfonate (CMS), and colistin sulfate. Both colistin sulfate and polymyxin B sulfate exhibit direct antibacterial activity without requiring in vivo transformation. In contrast, CMS is an inactive prodrug that must be converted into colistin within the body to achieve its therapeutic effect, leading to delayed and more variable drug exposure.3,4 The key pharmacokinetic/pharmacodynamic (PK/PD) index associated with polymyxin efficacy is the ratio of the area under the concentration-time curve to the minimum inhibitory concentration (AUC/MIC). Suboptimal exposure may lead to treatment failure, whereas excessive exposure increases the risk of nephrotoxicity, the most common dose-limiting adverse reaction. However, pharmacokinetic data regarding colistin sulfate in humans remain limited. Previous studies have demonstrated considerable variability in blood concentrations of polymyxin among individuals, particularly in critically ill patients in the ICU.5,6 This variability is attributed to factors such as microcirculation disorders, hypoproteinemia, and liver and kidney dysfunction, which can significantly influence drug metabolism in vivo. Consequently, substantial differences in pharmacokinetics may arise both between and within individuals.7 Therefore, it is advisable to guide drug administration based on the PK/PD principles of antibacterial agents, thereby optimizing the dosing regimen of colistin sulfate to enhance therapeutic efficacy while minimizing adverse reactions and the development of drug resistance.
Population pharmacokinetics (PPK), grounded in PK/PD principles, has been widely employed to examine the pharmacokinetic parameters of various drugs, thereby providing a robust framework for individualized treatment.8 To date, several PPK studies have been conducted on colistin sulfate, but most have focused on specific populations such as patients with renal impairment or those receiving renal replacement therapy.9–12 Key pharmacokinetic parameters affecting colistin sulfate metabolism and clearance, particularly in critically ill patients with diverse clinical characteristics, remain inadequately characterized. Clinically, there is an urgent need to determine whether the standard dosing regimen achieves adequate drug exposure across varying MIC levels and renal function, and whether renal function-based dose adjustment can improve treatment outcomes while reducing nephrotoxicity. Thus, a more comprehensive investigation into the pharmacokinetic characteristics of colistin sulfate in critically ill patients is crucial for informing personalized medication strategies and ensuring the efficacy and safety of treatments in the ICU.
Compared with previous studies, this research specifically targets a broader cohort of critically ill ICU patients not receiving CRRT or ECMO. A population pharmacokinetic model was established to explore the relationship between patient characteristics and pharmacokinetic parameters. Monte Carlo simulation was performed to identify covariates affecting drug clearance and to optimize dosing regimens across different MIC levels and renal function strata. This study aims to provide a reference for the rational clinical use of colistin sulfate.
Materials and Methods
Patients and Ethics
This study was conducted in accordance with the Declaration of Helsinki and received approval from the Ethics Committee of the Second Hospital of Hebei Medical University (2020-R551). The research focused on patients diagnosed with severe carbapenem-resistant organism (CRO) infections in the intensive care unit (ICU) of the Second Hospital of Hebei Medical University between June 2021 and June 2023, all of whom received intravenous colistin sulfate treatment. Inclusion criteria were as follows: (1) intravenous administration of colistin sulfate (Shanghai New Asia Pharmaceuticals, Shanghai, China) for a minimum of three days; (2) age of 18 years or older; and (3) at least one monitored blood drug concentration value during the treatment period. Exclusion criteria included: (1) death within 24 hours following the administration of colistin sulfate; (2) non-intravenous administration of colistin sulfate; (3) pregnancy or lactation; (4) incomplete medical records; and (5) undergoing continuous renal replacement therapy (CRRT) or extracorporeal membrane oxygenation (ECMO).
Clinical Data Collection
Demographic information, medication usage, and laboratory test data for patients are obtained through the hospital’s electronic medical record system. This data encompasses gender, age, height, weight, underlying diseases, and the Acute Physiology and Chronic Health Evaluation (APACHE) II score. Additionally, it includes details on the dosage of colistin sulfate, administration time, combination therapy, sampling time for therapeutic drug monitoring, blood drug concentration, types of pathogenic bacteria, and minimum inhibitory concentration (MIC). Liver function indicators such as alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin (TBIL), direct bilirubin (DBIL), indirect bilirubin (IBIL), glutamyl transpeptidase (GGT), alkaline phosphatase (ALP), and total bile acid (TBA) are also recorded. Furthermore, renal function indicators, including uric acid (UA), serum urea (UREA), creatinine (Scr), and creatinine clearance rate (CrCL) calculated using the Cockcroft-Gault formula, are documented. Other laboratory parameters include total protein (TP), albumin (ALB), and blood routine regulations such as white blood cell count (WBC), neutrophil percentage (NEUT), hemoglobin (HGB), and platelet count (PLT). Coagulation indicators, including prothrombin time (PT), thrombin time (TT), activated partial thromboplastin time (APTT), prothrombin activity (PA), and fibrinogen (FIB), as well as inflammatory markers such as C-reactive protein (CRP) and procalcitonin (PCT), are also collected.
Dosage Administration and Blood Sample Collection
The recommended standard dose of colistin sulfate is 1 to 1.5 million IU daily, given intravenously in 2 to 3 doses, with the specific dosing regimen being determined by the attending physician. In this study, blood samples were sparsely collected after patients reached a steady state following five doses of colistin sulfate. Peripheral venous blood samples were obtained at three specific time points for therapeutic drug monitoring: trough, intermediate, and peak concentrations. The peak concentration sample was taken 0.5 hours post intravenous infusion completion, the intermediate concentration sample was collected 6 hours after infusion completion, and the trough concentration sample was obtained within 0.5 hours before the subsequent administration.The author conducted the analysis of colistin sulfate blood concentration following a specified protocol. Upon sample collection, the samples underwent immediate centrifugation at 6000 rpm for 5 minutes. Subsequently, 200 μL of serum samples were extracted and supplemented with 20 μL of internal standard working solution (40 μg/mL). Following vortex mixing, 400 μL of methanol-5% trichloroacetic acid (50:50, V/V) was introduced. The mixture was vortexed for 2 minutes, then centrifuged at 10,900 rpm for 5 minutes, and 200 μL of the resulting supernatant was extracted for injection. The serum mass concentration was analyzed using an LC-20C high-performance liquid chromatograph (Shimadzu, Japan) coupled with an API4000+ triple quadrupole mass spectrometer (Applied Biosystems, USA). The method exhibited a satisfactory linear relationship ranging from 0.1 to 10 μg/mL, with a quantitation limit of 0.1 μg/mL. Method validations, including the standard curve, specificity, accuracy, precision, matrix effect, recovery rate, and stability, all conformed to FDA guidelines.
Clinical Efficacy and Adverse Reaction Determination
The clinical efficacy was assessed following the “Technical Guidelines for Clinical Trials of Antibacterial Drugs”.13 Patients undergoing colistin sulfate anti-infection therapy were evaluated upon treatment completion. Outcomes were categorized as full recovery, marked effect, improvement, or no effect. Full recovery entailed the disappearance of infection symptoms and signs, pathogen negativization, and normalization of inflammatory markers. Marked effect indicated significant improvement, with one indicator not fully normalized. Improvement reflected alleviated infection symptoms but persisting abnormal inflammatory markers and positive etiological findings. Ineffectiveness denoted failure to meet recovery, marked effect, or improvement criteria, or disease exacerbation or mortality. Clinical effectiveness encompassed recovery, marked effect, and improvement.The drug sensitivity data were obtained using the micro-dilution method in meat broth. Polymyxin sensitivity was determined based on the Clinical efficacy of polymyxin and guidelines from the Clinical and Laboratory Standards Institute (CLSI),14 the European Committee on Antimicrobial Susceptibility Testing (EUCAST),15 and the United States Committee on Antimicrobial Susceptibility Testing (USCAST).16 Patients who received empirical dosing without positive culture results did not undergo microbiological efficacy analysis. Bacterial clearance was defined as achieving two consecutive negative culture results from the infected site post-treatment. The efficacy of microbial therapy was defined as either bacterial clearance or reduction in bacterial mass.
Nephrotoxicity represents the primary adverse effect of colistin sulfate, with colistin sulfate-associated acute kidney injury (AKI) being defined as AKI occurring during colistin sulfate treatment or within 72 hours post-treatment. The most recent baseline serum creatinine value (SCr) prior to administration is utilized. Diagnostic criteria for AKI are based on the 2012 Kidney Disease: Improving Global Outcomes (KDIGO) clinical practice guideline,17 which includes SCr elevation of ≥0.3 mg/dL (>26.5 µmoL/L) within 48 hours, SCr increase of ≥1.5 times the baseline value within 7 days, or urine output <0.5 mL/kg/h for 6 hours. Exclusion criteria encompass patients with pre-existing chronic kidney disease (CKD), baseline creatinine clearance (CrCL) <80 mL/min pre-administration, and those who underwent chronic renal replacement therapy (CRRT) before treatment.
Establishment and Validation of Population Pharmacokinetic Models
Utilize the nonlinear mixed effects modeling software NONMEM (Version 7.2, ICON Development Solutions, Ellicott City, MD, USA) along with Pirana software (Version 2.8.0) and Perl Speaks NONMEM (Version 5.16.3) to construct models and perform simulations. The choice of the foundational model relies on visual examination of diagnostic graphs and goodness of fit criteria, encompassing the precision and validity of parameter estimation and enhancement of the objective function value (OFV). Model parameters were computed using the first-order conditional estimation method (FOCEI) incorporating inter-individual and residual variations. Inter-individual variability was assessed employing the exponential model, while intra-individual variability was evaluated using the proportional model. Comparison between one-chamber and two-chamber structural models was based on the concentration-time curve of first-level elimination. Evaluation of summation type residuals versus proportional type residuals led to the selection of the model demonstrating the most significant OFV improvement as the foundational model.
The stepwise covariate modeling (SCM) method was utilized to investigate the impact of potential covariates on pharmacokinetic (PK) parameters, encompassing demographic details, medication data, and biochemical markers. Continuous covariates, like age, were represented by power functions, while categorical covariates, such as gender, were depicted by exponential functions. A comprehensive regression model was constructed employing the forward inclusion technique. A reduction in the objective function value (OFV) exceeding 6.63 upon addition of a specific covariate [P < 0.01, degrees of freedom (df) = 1] signified its statistical significance in the model. Once all statistically significant covariates were incorporated, the full regression model was finalized. Subsequently, reverse elimination was conducted, systematically eliminating covariates from the model to monitor changes in OFV. If the increase in OFV was below 10.83 (P < 0.001, df = 1), indicating no significant impact, the covariate was eliminated from the full regression model. This iterative process continued until an OFV change surpassing 10.83 was observed. Evaluation of the relative standard error (RSE) and Shrinkage values of parameter estimates, fine-tuning of the model, and iterative adjustments led to the derivation of the ultimate model.
R (Version 4.3.3 or higher) was utilized to visually assess the final model. The model’s reliability was assessed through a goodfit graph, encompassing actual observations versus population predictions (DV-PRED), dependent variable versus individual predictions (DV-IPRED), scatter plots of conditional weighted residuals for population predictions (CWRES-PRED), and conditional weighted residuals over time (CWRES-TIME). The alignment between predicted and observed values was evaluated by examining the aggregation trend and dispersion in the scatter plot, thus gauging the fitting performance of the final model.
The Bootstrap (BS) method was employed to assess the stability of the final population pharmacokinetic model. One thousand new datasets were generated by resampling with replacement from the original modeling dataset, using individual subjects as the sampling unit. The NONMEM software was then used to re-estimate model parameters for each bootstrap dataset. The median values and 95% confidence intervals (CI) of the bootstrap-derived parameters were calculated. The parameter estimates from the final model were compared against these 95% CIs, and the bias and coverage of the bootstrap distributions were evaluated.
The Visual Predictive Check (VPC) method was employed by simulating the dataset 1,000 times based on the final model’s parameters. This was done to compute the 95% confidence intervals (CIs) for the 5th, 50th, and 95th percentiles of the final model’s fitted concentrations. Subsequently, a visual comparison was made between the simulated data and the observed values to assess any systematic bias and to evaluate the predictive performance of the final model.
Monte Carlo Simulation
The final model conducted 1000 repeated Monte Carlo simulations for eight clinical administration regimens of colistin sulfate under varying renal function conditions to establish the optimal dose adjustment strategy. The ratio of the area under the free concentration-time curve to MIC (fAUC0-24h/MIC) has been identified as the key pharmacokinetic/pharmacodynamic (PK/PD) index for assessing colistin efficacy.18,19 Cheah et al demonstrated that fAUC/MIC should be ≥15.20 The target achievement probability (PTA) for different regimens with fAUC0-24h/MIC≥15, where f equals 0.5, was calculated to determine the optimal regimen with PTA≥90% for colistin sulfate administration. For each dosing regimen, the steady-state 24-hour AUC was calculated as Daily Dose/CL, where CL represents the clearance value sampled from the parameter distribution during the simulation.
The MIC values are 0.5, 1, and 2 mg/L, while the CrCL values range from 10 to 120 mL/min. Eight administration regimens include 0.50MU q12h, 0.50MU q8h, 0.75MU q12h, 0.75MU q8h, 1.00MU q12h, 1.00MU q8h, a loading dose of 1.50MU, maintenance dose of 1.00MU q12h, and another loading dose of 1.50MU. The maintenance dose lasts for 8 hours. The infusion time for each regimen is standardized at 1 hour.
Result
Basic Information of the Patient
This study comprised 51 adult patients and 123 blood drug concentration monitoring points, with 32 males and 19 females. The patients primarily presented with pulmonary infections, abdominal cavity infections, central nervous system infections, bloodstream infections, and urinary tract infections. The predominant CRO isolated was Acinetobacter baumannii (58.00%), followed by Klebsiella pneumoniae (28.00%), Pseudomonas aeruginosa (6.00%), Escherichia coli (4.00%), and Enterobacter cloacae (4.00%).
The median age of all patients was 65.00 (42.00, 70.00) years, with 32 being male, and a median BMI of 24.05 (21.43, 26.10) kg/m2. Patients received a combination therapy regimen consisting of colistin sulfate with one or two other antibacterial drugs for treating isolated CROs. The primary combination drugs included tigecycline in 30 cases (58.82%), carbapenems in 9 cases (17.65%), and cefoperazone sodium and sulbactam sodium in 7 cases (13.73%). A regimen of three antibacterial drugs was used in five cases (9.80%). Colistin sulfate was administered to all patients for a duration ranging from 3 to 31 days, with a median treatment course of 11.50 (7.00, 14.75) days. The CrCL values for all patients ranged from 12.14 to 246.91 mL/min. Table 1 presents the demographic details, clinical parameters, and medication utilization.
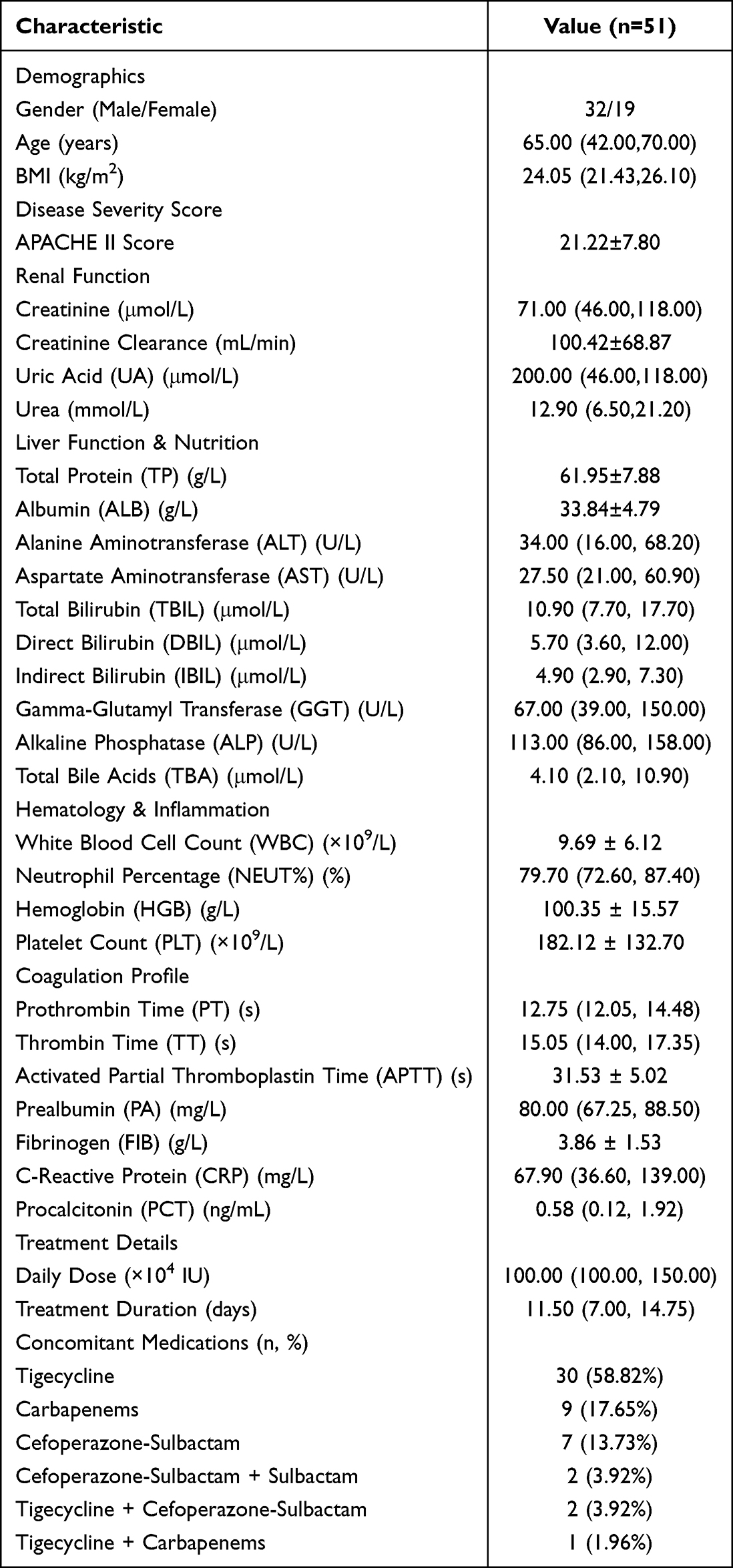 |
Table 1 Includes the Basic Demographic Information of the Patients |
Following the clinical efficacy evaluation criteria, patients underwent assessment post colistin sulfate treatment completion, resulting in 31 patients deemed effectively treated, while 20 patients were considered ineffectively treated, yielding a clinical effectiveness rate of 60.78% (31/51). However, it should be noted that all patients received concomitant antibiotics (eg., tigecycline, carbapenems, or cefoperazone sodium and sulbactam sodium); therefore, the observed clinical response cannot be attributed solely to colistin sulfate. All 51 enrolled patients had confirmed CRO infections with positive baseline cultures. Bacterial clearance was achieved in 27 of these 51 patients (52.94%). Notably, among patients who achieved bacterial clearance, 25 (92.6%) also showed clinical response, suggesting concordance between microbiological and clinical outcomes. The in-hospital mortality rate stood at 21.57%, with eleven patient fatalities.
Regarding adverse reactions, a total of 2 patients (3.92%) experienced acute kidney injury (AKI) during colistin sulfate treatment. One patient developed AKI 4 to 7 days post-administration, while another patient experienced AKI 7 to 14 days after treatment initiation. The creatinine levels of one patient gradually decreased following the discontinuation of colistin sulfate, whereas the other patient ultimately succumbed. In the effective treatment group, one patient (3.23%) developed AKI, and in the ineffective treatment group, one patient (5.00%) also experienced AKI. There was no statistically significant difference in the incidence of colistin-related AKI between the two groups (P > 0.05). Additionally, no other adverse reactions, such as neurotoxicity or skin pigmentation, were observed in any of the patients.
The Population Pharmacokinetic Model of Colistin Sulfate
Fifty-one patients were included in the study, yielding 123 blood samples with colistin sulfate concentrations ranging from 0.12 to 4.40 mg/L for pharmacokinetic (PPK) modeling. The data for modeling primarily consist of sparsely sampled points, with 41.46% (n=51) representing trough concentrations, 34.96% (n=43) peak concentrations, and 23.58% (n=29) concentrations at 6 hours post-administration. Figure 1 illustrates the relationship between colistin sulfate blood concentration and time since the last dose.
 |
Figure 1 Diagnostic goodness-of-fit plots of the base model. (A) Observed concentration (DV) vs. individual predicted concentration (IPRED); (B) DV vs. population predicted concentration (PRED); (C) conditional weighted residuals (CWRES) vs. PRED; and (D) CWRES vs. time. The red lines in the upper panel represent loess smooth lines and linear fit lines, respectively. |
After several iterations, the optimal model was identified as a one-compartment model with linear elimination, which adequately characterized the pharmacokinetic profile of colistin sulfate. Inter-individual variability in clearance was described using an exponential model. Residual unexplained variability was described using a proportional error model: DV = IPRED × (1 + θprop × ε), where ε was assumed to follow a standard normal distribution with a mean of 0 and variance fixed to 1. In this parameterization, the variance of EPS (1) was fixed to define the scale of the random error term, whereas the proportional residual error coefficient θprop was estimated during model development. The estimated parameters of the final model and diagnostic plots are presented in Table 2 and Figure 1.
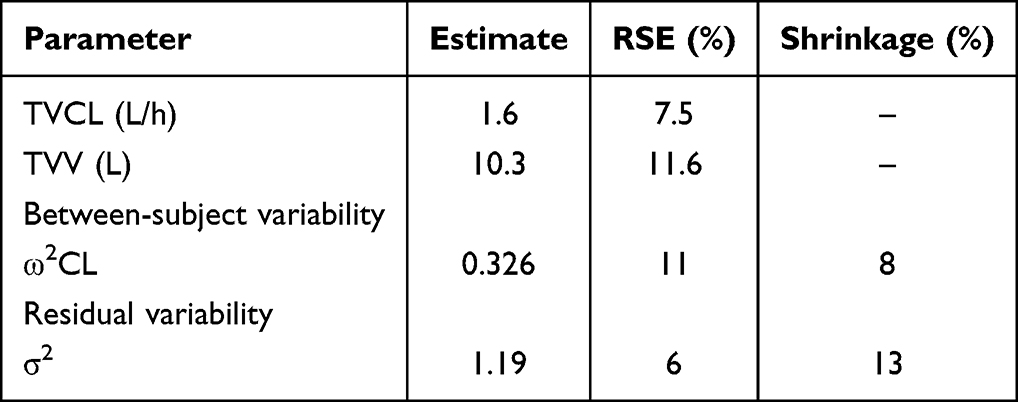 |
Table 2 Population Pharmacokinetic Parameter Estimates from the Base Model |
During the construction of the covariate model, creatinine clearance (CrCL) was established as a valid covariate for the clearance of colistin sulfate. Gender was eliminated during the backward elimination process of the full regression model due to its lack of significant impact. The ultimate population pharmacokinetic (PPK) model is presented below:

V (L) =10.10
Here, CL denotes the individual clearance rate, V denotes the individual distribution volume, and CrCL denotes the creatinine clearance rate. The specific parameters of the ultimate model are detailed in Table 3.
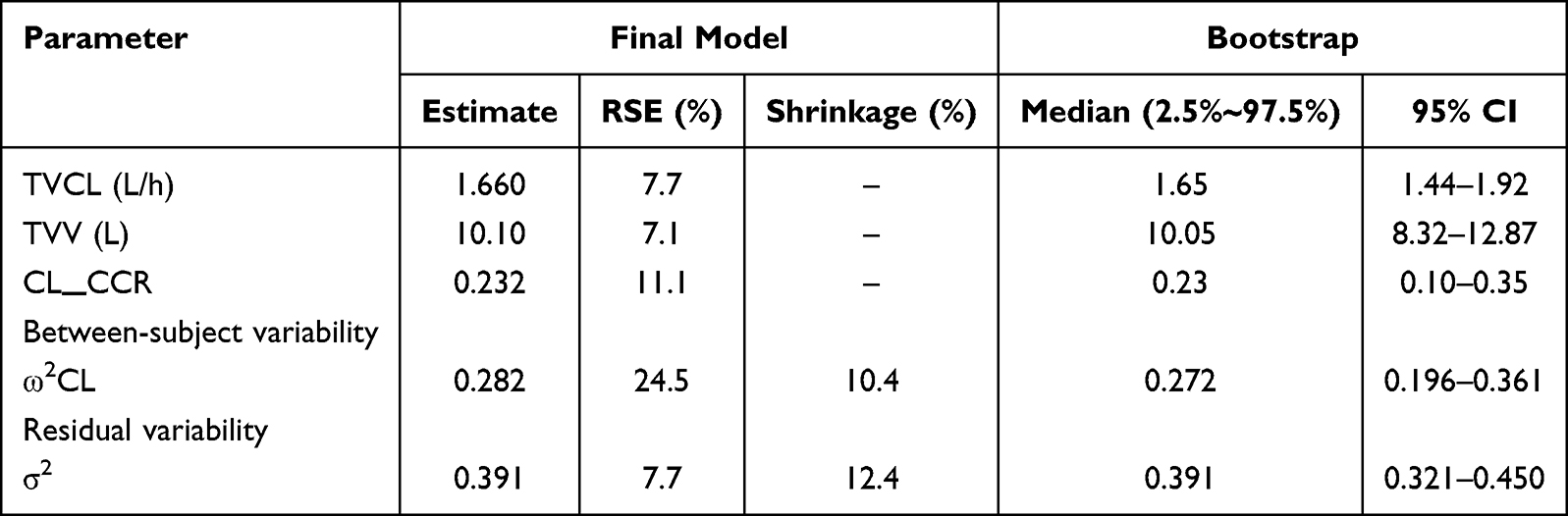 |
Table 3 Population Pharmacokinetic Parameter Estimates from the Final Model |
The bootstrap (BS) method was employed for 1,000 iterations, all resulting in successful fits. The median parameter estimates deviated by less than 10% from the final model estimates, and the 95% confidence intervals (CIs) of the parameter estimates from the final model aligned well with those from the BS method. These results are presented in Table 3. These results indicate that the parameter estimates of the final model were stable and reliable based on the bootstrap analysis.
The goodness-of-fit plot of the final model is presented in Figure 2. Scatter plots of observed concentrations against population predicted (PRED) and individual predicted (IPRED) values showed a reasonable correlation. The conditional weighted residuals (CWRES) of the final model, plotted against PRED and time, demonstrated a predominantly random distribution centered around zero, with the majority of residuals falling within the acceptable range (−2 to 2), indicating an acceptable model fit.
 |
Figure 2 Diagnostic goodness-of-fit plots of the final model. (A) Observed concentration (DV) vs. individual predicted concentration (IPRED); (B) DV vs. population predicted concentration (PRED); (C) conditional weighted residuals (CWRES) vs. PRED; and (D) CWRES vs. time. The red lines in the upper panel represent loess smooth lines and linear fit lines, respectively. |
Visual predictive check (VPC) was performed with 1,000 simulations of the model and dataset, with the results shown in Figure 3. The x-axis represents time (hours) since the last dose, and the y-axis represents the observed concentration. Unfilled circles depict the observed concentration values. The lower, middle, and upper blue lines correspond to the 5th, 50th, and 95th percentiles of the observed concentrations, respectively. The shaded areas represent the 95% confidence intervals of the 5th, 50th, and 95th percentiles of the simulated concentration data. Greater alignment between the percentile lines and shaded areas indicates a better model fit. As shown in Figure 3, most observed concentrations fell within the 90% confidence intervals of the predicted quantiles, with substantial overlap between the lines and shaded areas. This suggests that the simulated and observed data shared similar distribution characteristics.
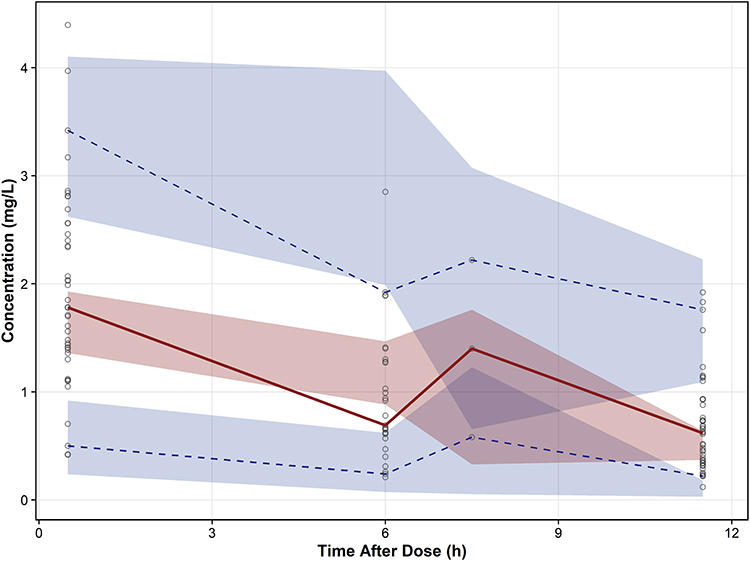 |
Figure 3 Prediction- and variability-corrected visual predictive check (pvcVPC) plot of the final model. The red solid lines represent the median observed concentration, and the semitransparent red fields represent the simulationbased 95% confidence intervals (CIs) for the median. The observed 5th and 95th percentiles are represented by blue dashed lines, and the 90% CIs for the corresponding model predicted percentiles are shown as semitransparent blue fields. The observed concentrations are represented by hollow pdots. |
Collectively, these internal validation results suggest that the final model exhibits reasonable stability and predictive performance. However, external validation in an independent cohort is needed to further confirm its generalizability.
Monte Carlo Simulation
The final model conducted Monte Carlo simulations of eight clinical administration regimens of colistin sulfate under varying renal function conditions. Figure 4 displays the PTA results of these regimens, while Figure 5 and Table 4 present the Css,avg for different dosing regimens across CrCL levels from 10 mL/min to 120 mL/min. Our analysis revealed that at MIC=0.5μg/mL, all eight dosing regimens achieved a PTA exceeding 90% across various CrCL levels. However, at MIC=1.0μg/mL, the 0.50 μg 12h regimen only reached 90% PTA in patients with CrCL≤10mL/min. Moreover, for MIC=1.0μg/mL, the 0.5 μg 8h and 0.75 μg 12h regimens did not attain a PTA of 90% in patients with CrCL≥80mL/min. With MIC=1.0μg/mL, except for the 0.5 μg 12h, 0.5 μg 8h, and 0.75 μg 12h regimens, all other regimens demonstrated a PTA exceeding 90% across different CrCL levels. Lastly, at MIC=2μg/mL, none of the dosing regimens achieved a PTA exceeding 90% in patients with CrCL≥80mL/min. Moreover, we observed that maintaining the daily dose constant for patients (eg., 0.5 MUq at 8-hour intervals and 0.75 MUq at 12-hour intervals) resulted in more uniform PTA performance. When keeping both the maintenance dose and administration frequency constant (eg., 1.50 MUq q12h compared to 1.00 MUq q12h), the loading dose did not significantly impact PTA.
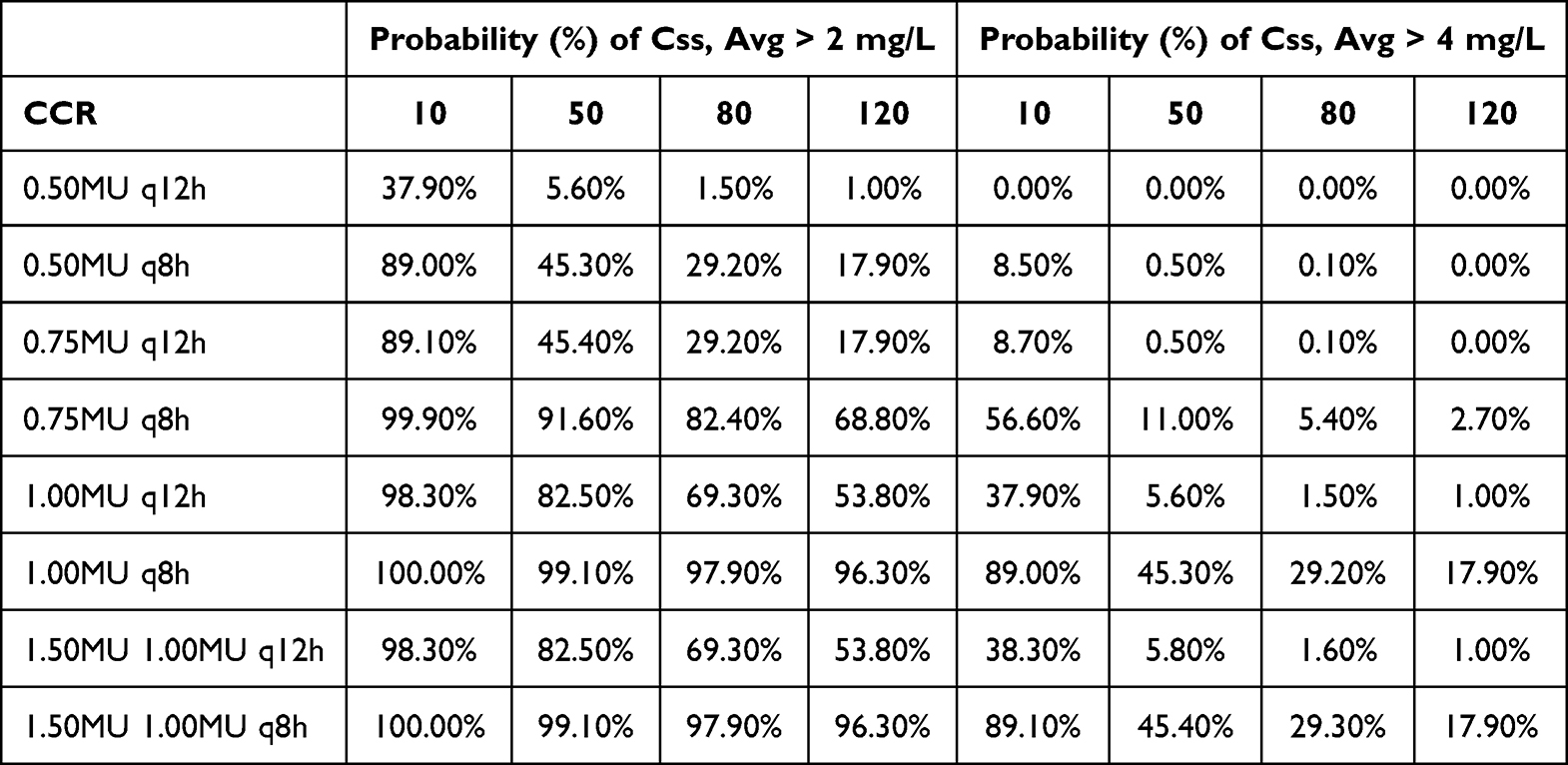 |
Table 4 Probability (%) of Target Css, Avg > 2 mg/L or Css, Avg > 4 mg/L for Different Colistin Sulfate Regimens |
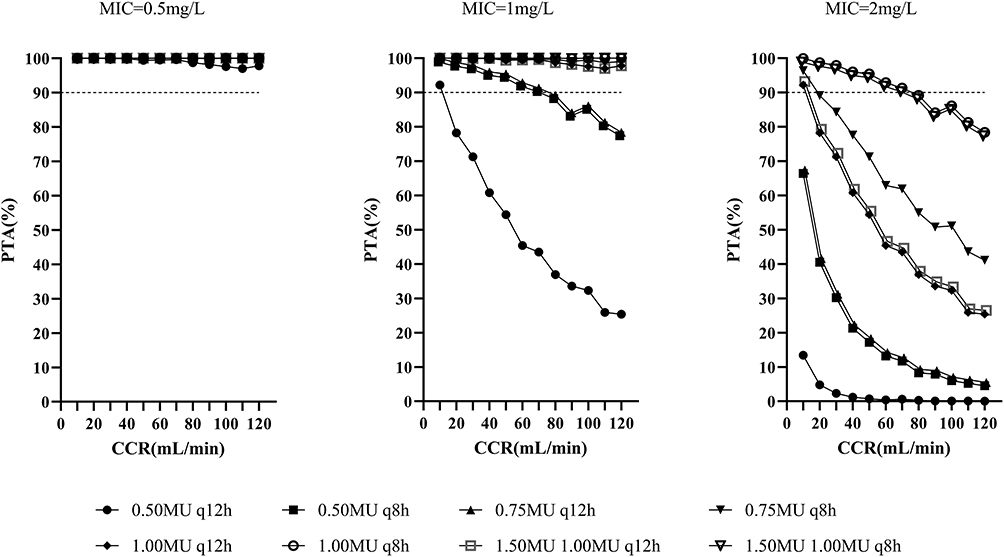 |
Figure 4 Simulated probability of achieving target attainment (fAUC/MIC ≥ 15) of colistin sulfate at each MIC (μg/mL) for different dose regimens in patients with various CCR volumes. |
 |
Figure 5 Violin plots of simulation results of average steady-state plasma colistin concentration (Css, avg) for dosing regimens with various CrCL values. The dotted lines represent the interquartile of simulated exposure; the solid lines represent the median of simulated exposure; the red dashed lines represent potential toxicity concentration (4 mg/L); the blue dashed lines represent the target concentration (2 mg/L). |
Discussion
Polymyxin medications are crucial for treating CRO infections. Despite the importance of colistin sulfate, there is limited research on its pharmacokinetics and clinical data in patients.5,21 This study aimed to optimize the use of colistin sulfate in critically ill patients by developing a population pharmacokinetic model. The model assessed how physiological and pathological factors affect the metabolism of colistin sulfate in infected critically ill patients. Compared to traditional therapeutic drug monitoring, the population pharmacokinetic model offers more precise predictions of drug metabolism. The study involved evaluating pharmacokinetic population parameters, inter-individual variances, and intra-individual variations to identify significant covariates, thus enabling personalized and accurate medication.
Our study suggests that the PK profile of colistin sulfate in critically ill patients is best described by a single-chamber model with nonlinear elimination. The clearance (CL) value for colistin is 1.66 L/h, lower than that of CMS (2.92 L/h),22 but akin to the reported CL range of polymyxin B (1.59–2.86 L/h).23,24 Colistin sulfate and polymyxin B share highly similar molecular structures, differing mainly in a single amino acid on the fatty acid tail chain: phenylalanine for polymyxin B and leucine for colistin sulfate. This similarity suggests comparable pharmacokinetic behaviors between colistin sulfate and polymyxin B. In contrast, CMS is an inactive precursor of polymyxin E, necessitating in-body conversion to an active form for bactericidal activity. Consequently, the intravenous pharmacokinetics of CMS differ significantly from those of colistin sulfate in our investigation.
In this investigation, creatinine clearance (CrCL) was identified as a significant covariate affecting the clearance (CL) of colistin sulfate. The OFV of the base model was −26.121. After inclusion of CrCL on CL, the OFV decreased to −36.826, corresponding to a ΔOFV of −10.705, indicating a significant improvement in model fit. Prior research has indicated that polymyxin B undergoes non-renal metabolism, with its clearance rate unrelated to CrCL.25–28 Nevertheless, recent clinical studies have presented contradictory findings, establishing CrCL as an independent factor impacting polymyxin B clearance.29,30 Yu et al’s pharmacokinetic and pharmacodynamic analysis of colistin sulfate in Chinese patients31 highlighted CrCL as a significant covariate affecting colistin sulfate clearance, consistent with recent findings on polymyxin B pharmacokinetics.32 These results suggest that in patients with renal impairment, the metabolism of colistin sulfate slows down, leading to increased drug concentrations in the body, necessitating dosage adjustments based on creatinine clearance rates.
A total of 51 patients diagnosed with CRO infection were analyzed in this study, with 31 cases (60.78%) showing a positive response to colistin sulfate anti-infection therapy. However, in clinical practice, to prevent the heterogeneity of polymyxin resistance, polymyxins are usually used in combination with one or more other drugs to achieve a synergistic bactericidal effect. In this study, most patients were simultaneously treated with other antibiotics, including tigecycline, carbapenems, and aminoglycosides. Therefore, the observed clinical response is likely to be the result of the combined action of multiple antibiotics rather than the effect of polymyxin sulfate alone. Based on the current data, it is impossible to determine the specific contribution of polymyxin sulfate to these results.The clinical effectiveness of colistin sulfate in this investigation mirrored our prior retrospective analysis33 (54.87%). Similarly, findings from a study on polymyxin B by Lu et al34 demonstrated comparable results. In Lu’s retrospective examination of polymyxin B, 57.6% of CRO-infected patients exhibited an effective response to the treatment. Notably, the daily dosage of colistin sulfate administered in our study was lower than that of polymyxin B in Lu’s research. Lu et al reported a median daily dose of 1.72mg/kg for polymyxin B, while our study utilized a median daily dose of 0.68mg/kg for colistin sulfate. Despite the significant reduction in the daily dosage of colistin sulfate, it achieved a clinical efficacy similar to that of polymyxin B. Additionally, this study involved the estimation of the AUC0-24,ss of colistin sulfate at steady state for each patient.The mean ± standard deviation of AUC0-24,ss was 12.83 ± 7.57 mg/h/L, significantly lower than the pharmacokinetic/pharmacodynamic (PK/PD) target value for polymyxin B, which is recommended in the “International Consensus Guidelines for the Rational Use of Polymyxin”35 to range from 50 to 100 mg/h/L. Consequently, the PK/PD target values for the two drugs may differ, potentially due to their distinct antibacterial activities. Currently, there are no established PK/PD target values for colistin sulfate, and it is not advisable to reference the target value for polymyxin B.
We acknowledge that risk factor analysis for clinical outcomes was not performed in the present study due to the limited sample size focused on PK modeling. Nevertheless, we have previously investigated this topic in a larger cohort of patients receiving colistin sulfate,33 identifying high APACHE II score and vasoactive agent use as independent risk factors for treatment failure, and prolonged treatment duration and higher albumin levels as protective factors. The present PK/PD study complements these findings by providing dose optimization strategies.
The observed microbiological efficacy rate (52.94%) is consistent with previously reported rates for polymyxin antibiotics in CRO infections (range: 45–65%).36–40 The high concordance between bacterial clearance and clinical response (92.6%) reinforces the clinical relevance of achieving microbiological eradication. These findings suggest that colistin sulfate-containing regimens contribute to bacterial clearance in a substantial proportion of patients, although the contribution of concomitant antibiotics cannot be isolated.
The observed 28-day mortality rate in this study (21.57%) is comparable to rates reported in recent literature. For instance, a study of 226 patients receiving colistin sulfate for CRO infections reported a hospital mortality rate of 20.80%.33 A meta-analysis of 695 critically ill patients also demonstrated that mortality was substantially lower in patients who achieved clinical cure (OR 0.05, 95% CI 0.02–0.14).41 Importantly, previous studies have consistently identified higher APACHE II score as an independent risk factor for mortality in patients receiving colistin therapy.42 Our previous retrospective study on the large-scale efficacy and safety assessment of sulfamethoxazole also found this.
Nephrotoxicity represents the primary adverse effect of polymyxin medications. In this study, among 51 patients treated with colistin sulfate, a total of 2 cases (3.92%) developed acute kidney injury (AKI), and the incidence rate was within the lower range reported in previous literature.43–45 Several factors should be considered when interpreting this finding.First, selection bias cannot be excluded, as patients with pre-existing chronic kidney disease were not enrolled, thereby lowering the baseline risk of acute kidney injury (AKI). Second, the limited sample size (n=51) results in wide confidence intervals around this estimate; the true incidence in a larger population may be substantially higher. Third, under-detection is possible given the retrospective design, as mild or subclinical AKI may not have been captured. Fourth, incomplete follow-up may have missed late-onset nephrotoxicity occurring after the observation period. Individualized administration may help optimize drug exposure levels, and the nephrotoxicity risk of polymyxin sulfate may be controlled to a certain extent, but its impact on nephrotoxicity still requires further research. In terms of the occurrence time, the two cases of AKI appeared 4–7 days and 7–14 days after administration, respectively. This time distribution is consistent with the pharmacological characteristics of the time-dependent accumulation of colistin sulfate nephrotoxicity, suggesting that special attention should be paid to changes in renal function one week after treatment. Regarding clinical outcomes, one patient’s creatinine levels gradually normalized following drug cessation, suggesting potential reversibility of renal damage. Another patient ultimately succumbed. While the adverse impact of acute kidney injury (AKI) on prognosis cannot be dismissed, it is more likely attributable to the severity of the patient’s underlying disease and the management of the primary infection. Further analysis indicated that the incidence of AKI in the effective treatment group was 3.23% (1/31), while in the ineffective treatment group it was 5.00% (1/20). However, there was no statistically significant difference between the groups (P > 0.05). This suggests that, within this study cohort, there is no significant association between the occurrence of AKI and treatment outcomes. Considering pharmacological mechanisms, the risk of AKI may be more closely related to individual pharmacokinetic characteristics, baseline renal function, concomitant medications (such as other nephrotoxic agents), and various other factors. Additionally, no other known adverse reactions associated with colistin, such as neurotoxicity and skin pigmentation, were observed in this study.This could be attributed to the limited sample size in this study, the relatively brief treatment duration, or the decrease in peak blood drug levels resulting from personalized dosing. Despite these factors, considering the narrow therapeutic range of colistin sulfate and substantial interindividual pharmacokinetic variability, ongoing monitoring of therapeutic agents and regular assessments of renal function remain imperative.
The ratio of the area under the free concentration-time curve to MIC (fAUC0-24h/MIC) has been confirmed as a PK/PD indicator for evaluating the efficacy of colistin. In the Monte Carlo simulation of this study, we referred to the research of Cheah et al20 on the colistin sulfate PK/PD model, and adopted fAUC0-24h/MIC≥15 as the target value of colistin sulfate PK/PD, with the free drug fraction in plasma being 0.5. The recommended dosage of colistin sulfate as per the instructions is 1 to 1.5MU per day, administered intravenously in 2 to 3 doses. The maximum daily dose should not exceed 1.5MU. Currently, the drug administration regimens used in clinical practice are 0.75MU q8h, 1.00MU q12 h, 1.00MU q8h, 1.5MU 1MU q12 h, and 1.5MU 1MU q8h. Based on the established colistin sulfate PPK model, we conducted Monte Carlo simulations of the above different administration regimens under different MIC and renal function conditions, and determined the optimal administration regimen of colistin sulfate through PTA≥90%. We found that the commonly recommended administration regimen of colistin sulfate in the current instructions can achieve PTA≥90% only when MIC≤0.5μg/mL under normal renal function. When MIC is greater than or equal to 1 μg/mL, a dosage of 0.50 MU every 12 hours may lead to inadequate exposure. At an MIC of 1.0 μg/mL, dosages of 0.50 MU every 8 hours and 0.75 MU every 12 hours can only attain a probability of target attainment (PTA) of at least 90% in patients with renal insufficiency. Patients with a creatinine clearance (CrCL) of 80 mL/min or higher are also at risk of inadequate exposure, necessitating a dosing regimen of 1.00 MU every 12 hours. When MIC is equal to or greater than 2 μg/mL, none of the dosing schedules can achieve a PTA of at least 90% in patients with normal renal function. Therefore, for infected patients with an MIC of 1 mg/L or higher and normal renal function, off-label high-dose regimens should be taken into consideration. It should be noted that the CrCL values in our modeling dataset ranged from 12.14 to 246.91 mL/min. The prediction for CrCL = 10 mL/min (Figure 5) involves a minimal extrapolation of 2.14 mL/min below the lowest observed value. Although this extrapolation is small, caution is warranted when applying the model to patients with CrCL below 12.14 mL/min.
This study has several limitations. Firstly, this is a single-center, small-scale retrospective study, which has a selection bias. The results may be influenced by the unique clinical practices of this center, thereby limiting the generalizability of the research findings. Although the sample size (n=51) is acceptable for a population pharmacokinetic (PPK) analysis, it may limit the detection of certain covariate effects, particularly those with small effect sizes. The limited sample size also precludes external validation of the PPK model, and the broad applicability of the model remains to be confirmed. Further evaluation with larger sample sizes and external cohorts is warranted. The predictive performance of the model was assessed using visual predictive check (VPC). While VPC is a powerful tool for evaluating model performance, its reliability with sparse data is sensitive to sample size and sampling density. In this study, clinical data were collected following routine therapeutic drug monitoring (TDM) practices, and the sparsity of the data may lead to considerable uncertainty in the estimation of extreme percentiles (eg., 5th and 95th). Therefore, VPC was primarily used to detect systematic model bias rather than to provide precise statistical validation. Future prospective studies with more intensive sampling schemes are needed to further validate the predictive performance of the model.Second, patients receiving continuous renal replacement therapy (CRRT) or extracorporeal membrane oxygenation (ECMO) were excluded from this study, which may introduce selection bias. Consequently, our findings may not be generalizable to these critically ill subpopulations.Third, several limitations should be considered when interpreting the clinical outcomes. The extensive use of combination therapy is a major confounder, making it difficult to isolate the specific effect of colistin sulfate on clinical outcomes. Variability in pathogen susceptibility (eg., differences in minimum inhibitory concentration values across patients) and host factors (eg., immune status, APACHE II score, comorbidities, organ dysfunction) may also have influenced clinical outcomes, yet these factors were not adequately accounted for in our analysis. Furthermore, although the study period (June 2021 to June 2023) is adequate for pharmacokinetic assessment, clinical outcomes may be affected by temporal changes in clinical practice, antibiotic resistance patterns, and patient case mix. Given these limitations, the association between colistin sulfate exposure and clinical outcomes should be interpreted with caution. Future studies with control groups or using propensity score matching are warranted to better isolate the specific contribution of colistin sulfate. Fourth, the PK/PD target of colistin sulfate (fAUC/MIC ≥ 15) in this study was derived from a previous study on monotherapy with colistin sulfate. The combination therapy or patient-specific factors may affect the clinical outcomes. Moreover, the Monte Carlo simulation results are based on model assumptions and limited sample data, and the results have limitations. They need to be prospectively validated before being applied in clinical practice. Fifth, this study used calculated free drug concentrations to evaluate efficacy and optimize dosing regimens, rather than measured free drug concentrations. This approach may deviate from actual values, particularly in critically ill patients or those with hypoproteinemia, potentially leading to inaccuracies in the study findings.
In conclusion, further studies with larger sample sizes, multicenter designs, and broader inclusion criteria are needed to validate our findings and to further elucidate the pharmacokinetic and pharmacodynamic characteristics of colistin sulfate, thereby enabling more precise individualized dosing.
Conclusion
This study established a population pharmacokinetic (PPK) model for colistin sulfate in critically ill patients. A one-compartment linear elimination model adequately described the drug’s PK characteristics, and CrCL was identified as a significant covariate affecting clearance. Monte Carlo simulations of eight clinical dosing regimens under varying MIC and renal function conditions revealed that the currently recommended regimens achieved PTA ≥90% only in patients with normal renal function when MIC ≤0.5 μg/mL. For patients with normal renal function and MIC ≥1 mg/L, the standard regimens risk underexposure, and off-label high-dose regimens should be considered.
Ethics Approval and Consent to Participate
The study protocol was approved by the Ethics Committee of the Second Hospital of Hebei Medical University (ID: 2020-R551). Due to the retrospective nature of the study and the use of de-identified patient data, the committee waived the requirement for written informed consent from individual patients. All patient data were anonymized prior to analysis and maintained with strict confidentiality to protect participants’ privacy. The study was conducted in accordance with the Declaration of Helsinki.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Livermore DM, Nicolau DP, Hopkins KL. et al. Carbapenem-resistant enterobacterales, carbapenem resistant organisms, carbapenemase-producing enterobacterales, and carbapenemase-producing organisms: terminology past its “sell-by date” in an era of new antibiotics and regional carbapenemase epidemiology. Clin Infect Dis. 2020;71(7):1776–16. doi:10.1093/cid/ciaa122
2. Jean -S-S, Harnod D, Hsueh P-R. Global threat of carbapenem-resistant gram-negative bacteria. Front Cell Infect Microbiol. 2022;12:823684. doi:10.3389/fcimb.2022.823684
3. Kwa A, Kasiakou SK, Tam VH, et al. Polymyxin B: similarities to and differences from colistin (polymyxin E). Expert Rev Anti Infect Ther. 2007;5(5):811–821. doi:10.1586/14787210.5.5.811
4. Nation RL, Velkov T, Li J. Colistin and polymyxin B: peas in a Pod, or chalk and cheese? Clin Infect Dis. 2014;59(1):88–94. doi:10.1093/cid/ciu213
5. Jin J, Zhu J, Zhu Z, et al. Clinical efficacy and nephrotoxicity of intravenous colistin sulfate in the treatment of carbapenem-resistant gram-negative bacterial infections: a retrospective cohort study. Ann Transl Med. 2022;10(20):1137. doi:10.21037/atm-22-4959
6. Xie Y-L, Jin X, Yan -S-S, et al. Population pharmacokinetics of intravenous colistin sulfate and dosage optimization in critically ill patients. Front Pharmacol. 2022;13:967412. doi:10.3389/fphar.2022.967412
7. Gregoire N, Aranzana-Climent V, Magreault S, et al. Clinical pharmacokinetics and pharmacodynamics of colistin. Clin Pharmacokinet. 2017;56(12):1441–1460. doi:10.1007/s40262-017-0561-1
8. Darwich AS, Polasek TM, Aronson JK, et al. Model-informed precision dosing: background, requirements, validation, implementation, and forward trajectory of individualizing drug therapy. Annu Rev Pharmacol Toxicol. 2021;61(1):225–245. doi:10.1146/annurev-pharmtox-033020-113257
9. Zamri PJ, Lim SMS, Sime FB, et al. A systematic review of pharmacokinetic studies of colistin and polymyxin B in adult populations. Clinical Pharmacokinetics. 2025;64(5):655–689. doi:10.1007/s40262-025-01488-2
10. Sun Q, Li X, Wang G, et al. Population pharmacokinetics of colistin sulfate in critically ill patients based on NONMEM. Scientific Reports. 2025;15(1):18295. doi:10.1038/s41598-025-03503-9
11. Cai X, Chen Y, Fu J, et al. Population pharmacokinetic analysis and dosing optimization of colistin sulphate in lung transplant recipients with pneumonia: a prospective study. Int J Antimicrob Agents. 2024;64(5):107346. doi:10.1016/j.ijantimicag.2024.107346
12. Boonyasiri A, Fuhs DT, Naorungroj T, et al. Disposition of colistin in critically-ill patients on sustained low-efficiency dialysis: a population pharmacokinetic study. Clin Microbiol Infect. 2025;31(9):1526–1531. doi:10.1016/j.cmi.2025.05.021
13. Writing Group of Guidelines for Clinical Trial of Antimicrobial Agents. Guidance for clinical trials of anti-bacterial drugs appendix: antimicrobial reference principle suggestion. Chin J Clin Pharmacol. 2012;30(9):844–856.
14. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing.
15. The european committee on antimicrobial susceptibility testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 10.0,2020[EB/OL]. Available from: http://www.eucast.org.
16. Pogue JM, Jones RN, Bradley JS, et al. Polymyxin susceptibility testing and interpretive breakpoints: recommendations from the United States Committee on Antimicrobial Susceptibility Testing (USCAST). Antimicrob Agents Chemother. 2020;64(2):e01495–19. doi:10.1128/AAC.01495-19
17. Kellum JA, Lameire N; KDIGO AKI Guideline Work Group. Diagnosis, evaluation, and management of acute kidney injury: a KDIGO summary (Part 1). Crit Care. 2013;17(1):204. doi:10.1186/cc11454
18. Dudhani RV, Turnidge JD, Nation RL, et al. fAUC/MIC is the most predictive pharmacokinetic/pharmacodynamic index of colistin against Acinetobacter baumannii in murine thigh and lung infection models. J Antimicrob Chemotherapy. 2010;65(9):1984–1990. doi:10.1093/jac/dkq226
19. Bergen PJ, Bulitta JB, Forrest A, et al. Pharmacokinetic/pharmacodynamic investigation of colistin against Pseudomonas aeruginosa using an in vitro model. Antimicrob Agents Chemother. 2010;54(9):3783–3789. doi:10.1128/AAC.00903-09
20. Cheah S-E, Wang J, Nguyen VTT, et al. New pharmacokinetic/pharmacodynamic studies of systemically administered colistin against Pseudomonas aeruginosa and Acinetobacter baumannii in mouse thigh and lung infection models: smaller response in lung infection. J Antimicrob Chemother. 2015;70(12):3291–3297. doi:10.1093/jac/dkv267
21. Nang SC, Azad MAK, Velkov T, et al. Rescuing the last-line polymyxins: achievements and challenges. Pharmacol Rev. 2021;73(2):679–728. doi:10.1124/pharmrev.120.000020
22. Couet W, Grégoire N, Gobin P, et al. Pharmacokinetics of colistin and colistimethate sodium after a single 80-mg intravenous dose of CMS in young healthy volunteers. Clin Pharmacol Ther. 2011;89(6):875–879. doi:10.1038/clpt.2011.48
23. Wang P, Zhang Q, Feng M, et al. Population pharmacokinetics of polymyxin B in obese patients for resistant gram-negative infections. Front Pharmacol. 2021;12:754844. doi:10.3389/fphar.2021.754844
24. Chen N, Guo J, Xie J, et al. Population pharmacokinetics of polymyxin B: a systematic review. Ann Transl Med. 2022;10(4):231. doi:10.21037/atm-22-236
25. Zavascki AP, Goldani LZ, Cao G, et al. Pharmacokinetics of intravenous polymyxin B in critically ill patients. Clin Infect Dis. 2008;47(10):1298–1304. doi:10.1086/592577
26. Kwa AL, Abdelraouf K, Low JG, et al. Pharmacokinetics of polymyxin B in a patient with renal insufficiency: a case report. Clin Infect Dis. 2011;52(10):1280–1281. doi:10.1093/cid/cir137
27. Sandri AM, Landersdorfer CB, Jacob J, et al. Population pharmacokinetics of intravenous polymyxin B in critically ill patients: implications for selection of dosage regimens. Clin Infect Dis. 2013;57(4):524–531. doi:10.1093/cid/cit334
28. Thamlikitkul V, Dubrovskaya Y, Manchandani P, et al. Dosing and pharmacokinetics of polymyxin B in patients with renal insufficiency antimicrob. Agents Chemother. 2016;61(1):e01337–16.
29. Wang P, Zhang Q, Zhu Z, et al. Population pharmacokinetics and limited sampling strategy for therapeutic drug monitoring of polymyxin B in Chinese patients with multidrug-resistant gram-negative bacterial infections. Front Pharmacol. 2020;11:829. doi:10.3389/fphar.2020.00829
30. Li Y, Deng Y, Zhu Z-Y, et al. Population pharmacokinetics of polymyxin B and dosage optimization in renal transplant patients. Front Pharmacol. 2021;12:727170. doi:10.3389/fphar.2021.727170
31. Yu X-B, Zhang X-S, Wang Y-X, et al. Population pharmacokinetics of colistin sulfate in critically ill patients: exposure and clinical efficacy. Front Pharmacol. 2022;13:915958. doi:10.3389/fphar.2022.915958
32. Yu X-B, Jiao Z, Zhang C-H, et al. Population pharmacokinetic and optimization of polymyxin B dosing in adult patients with various renal functions. Brit J Clin Pharmaco. 2021;87(4):1869–1877. doi:10.1111/bcp.14576
33. Ma Y-C, Sun Y-Q, Wu X, et al. Clinical effectiveness and safety of colistin sulphate in treating infections caused by carbapenem-resistant organisms and analysis of influencing factors. Infect Drug Resist. 2024;17:3793–3804. doi:10.2147/IDR.S473200
34. Lu Q, Li G-H, Qu Q, et al. Clinical efficacy of polymyxin B in patients infected with carbapenem-resistant organisms. Infect Drug Resist. 2021;14:1979–1988. doi:10.2147/IDR.S312708
35. Tsuji BT, Pogue JM, Zavascki AP; International Consensus Guidelines for the Optimal Use of the Polymyxins:Endorsed by the American College of Clinical Pharmacy (ACCP), et al. International consensus guidelines for the optimal use of the polymyxins: endorsed by the American College of Clinical Pharmacy (ACCP), European Society of Clinical Microbiology and Infectious Diseases (ESCMID), Infectious Diseases Society of America (IDSA), International Society for Anti-infective Pharmacology (ISAP), Society of Critical Care Medicine (SCCM), and Society of Infectious Diseases Pharmacists (SIDP). Pharmacotherapy. 2019;39(1):10–39. doi:10.1002/phar.2209
36. Lu X, Zhong C, Liu Y, et al. Efficacy and safety of polymyxin E sulfate in the treatment of critically ill patients with carbapenem-resistant organism infections. Frontiers in Medicine. 2022;9:1067548. doi:10.3389/fmed.2022.1067548
37. Wang J, Shah BK, Zhao J, et al. Comparative study of polymyxin B and colistin sulfate in the treatment of severe comorbid patients infected with CR-GNB. BMC Infect Dis. 2023;23(1):351. doi:10.1186/s12879-023-08339-0
38. Peng D, Zhang F, Chen Y, et al. Multicenter study. Efficacy and safety of colistin sulfate in the treatment of infections caused by carbapenem-resistant organisms: a multicenter retrospective cohort study. J Thoracic Dis. 2023;15(4):1794–1804. doi:10.21037/jtd-23-336
39. Xia GL, Jiang RL. Efficacy and safety of polymyxin B in carbapenem-resistant gram-negative organisms infections. BMC Infect Dis. 2021;21(1):1034. doi:10.1186/s12879-021-06719-y
40. Lu Q, Zhu -H-H, Li G-H, et al. A comparative study of the microbiological efficacy of Polymyxin B on different carbapenem-resistant gram-negative bacteria infections. Front Med. 2021;8:620885. doi:10.3389/fmed.2021.620885
41. Chaiwatanarat T, Srisawat N, Srichana T, et al. Clinical outcomes of colistin methanesulfonate sodium in correlation with pharmacokinetic parameters in critically ill patients with multi-drug resistant bacteria-mediated infection: a systematic review and meta-analysis. J Glob Antimicrob Resist. 2024;38:147–156.
42. Ciftci A, Izdes S, Altintas ND. Factors determining nephrotoxicity and mortality in critical care patients receiving colistin. J Infect Dev Ctries. 2018;11(12):912–918. doi:10.3855/jidc.9443
43. Zhang Y, Dong R, Huang Y, et al. Acute kidney injury associated with colistin sulfate vs. polymyxin B sulfate therapy: a real-world, retrospective cohort study. Int J Antimicrob Agents. 2024;63(1):107031. doi:10.1016/j.ijantimicag.2023.107031
44. Wang G, Bao WY, Qian YF, et al. Efficacy and safety of colistin sulfate combined therapy in the treatment of extensively drug-resistant gram-negative bacilli infections in the ICU. Pharmaceu Clin Res. 2024;32(2):160–164. (in Chinese).
45. Yang P, Shuai W, Ju Y, et al. Acute kidney injury of intravenous colistin sulfate compared with colistimethate sodium: a real-world, retrospective cohort study. BMC Infect Dis. 2025;25(1):1007. doi:10.1186/s12879-025-11401-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.