Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Optimizing Abrocitinib Use for Atopic Dermatitis in India: Expert Recommendations for Patient Selection, Dosing, and Long‑Term Remission
Authors Kandhari S, De A, Shankar K, G R, Pereira R, Jagadeesan S, Panda M, Singh V, Chakravadhanula U, Banodkar P
Received 21 April 2026
Accepted for publication 13 June 2026
Published 24 June 2026 Volume 2026:19 611587
DOI https://doi.org/10.2147/CCID.S611587
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michela Starace
Sanjiv Kandhari,1 Abhishek De,2 Krupa Shankar,3 Ravichandran G,4 Rickson Pereira,5 Soumya Jagadeesan,6 Maitreyee Panda,7 Vinay Singh,8 Uma Chakravadhanula,9 Pravin Banodkar10
1Department of Dermatology, Dr. Kandhari’s Skin and Dental Clinic, New Delhi, India; 2Department of Dermatology, Calcutta National Medicine College and Hospital, Kolkata, West Bengal, India; 3Department of Dermatology, Mallige Hospital, Bengaluru, Karnataka, India; 4Department of Dermatology, Apollo Gem Hospital, Chennai, Tamil Nadu, India; 5Department of Dermatology, Dr. Rickson’s Dermatherapie Clinic, Mumbai, Maharashtra, India; 6Department of Dermatology, Amrita Hospital, Kochi, Ernakulam, Kerala, India; 7Department of Dermatology, IMS and SUM Hospital, Bhubaneshwar, Odisha, India; 8Department of Dermatology, Vibrance Skin Laser and Cosmetic Clinic, Delhi, India; 9Department of Dermatology, IDEA Skin and Hair Clinic, Hyderabad, Andhra Pradesh, India; 10Department of Dermatology, Skin Crest Clinic, Mumbai, Maharashtra, India
Correspondence: Sanjiv Kandhari, Department of Dermatology, Dr. Kandhari’s Skin and Dental Clinic, New Delhi, 110057, India, Email [email protected]
Abstract: Atopic dermatitis (AD) is a chronic, relapsing inflammatory skin disorder which significantly impairs quality of life due to persistent pruritus, sleep disturbance, and recurrent flares. Conventional systemic therapies, such as cyclosporine and methotrexate, often provide inadequate itch and disease control, with limited safety and poor long-term tolerability. The introduction of targeted small-molecule therapies, particularly Janus kinase (JAK) inhibitors, has substantially transformed AD management by enabling rapid itch relief and sustained clinical improvements. Abrocitinib, an oral selective JAK1 inhibitor, has demonstrated rapid and clinically meaningful reduction in pruritus, improvement in skin lesions, and a favorable benefit–risk profile in pivotal clinical trials. However, guidance regarding its optimal real-world use in Indian patients remains limited. This expert recommendation aims to provide practical, experience-based recommendations for the initiation, dosing, monitoring, and long-term management of abrocitinib in patients with moderate-to-severe AD in India. A multistep approach was employed, including a targeted literature review conducted between September and November 2025, a nationwide survey of 36 experienced dermatologists, and two virtual expert panel meetings involving 10 senior clinicians. Experts have identified abrocitinib as a valuable systemic option, particularly for patients with pruritus‑dominant disease, head and neck involvement, hand eczema, elderly patients with comorbidities, and those inadequately controlled with biologics or other systemic agents. Baseline assessment of hematologic, hepatic, renal, lipid, infectious, cardiovascular, and thrombotic risks was emphasized, with follow-up monitoring recommended at four weeks and following dose modifications. An induction dose of 200 mg once daily was preferred for most patients, with 100 mg reserved for the selected populations. Strategies for maintenance, dose tapering, and treatment transitions were also discussed. Overall, these expert recommendations provide practical real-world guidance supporting the individualized, safe, and effective use of abrocitinib in the Indian clinical setting, while emphasizing the importance of structured monitoring and long-term treatment planning.
Keywords: atopic dermatitis, abrocitinib, Janus kinase inhibitors, itching management, strategy, real-world, India
Introduction
Atopic dermatitis (AD) is a common chronic inflammatory skin disorder that significantly affects patients’ quality of life (QOL) due to frequent flare-ups.1 The clinical presentation of AD is diverse, often marked by recurrent eczema and severe itching, which disrupts daily activities and sleep.2 Currently, topical and systemic treatments (like cyclosporine and methotrexate) are effectively helping many patients with AD, but these mainstay therapies pose limitations for long-term use, quick and effective itch relief in AD patient.3 This led to introduction of newer treatment options like biologics and small molecules for a tailored approach in the management of AD.4 Recent advances in the management of JAK inhibitors have also emphasized the importance of individualized treatment strategies, safety monitoring, and long-term therapeutic optimization in inflammatory skin diseases.5
Dupilumab was the first newer systemic therapy to receive approval for the management of moderate-to-severe AD. However, despite their introduction, unmet needs remain. In Phase 3 trials, more than 60% of patients did not achieve predefined efficacy endpoints, and real-world studies have highlighted that approximately 30% of patients failed to achieve adequate disease control after one year of treatment. These limitations underscore the need to expand the treatment arsenal with effective alternatives.6
To address this gap, Janus kinase (JAK) inhibitors, which target the JAK-signal transducer and activator of the transcription (STAT) pathway, have demonstrated efficacy in treating AD. JAK inhibitors approved by the U.S. Food and Drug Administration (FDA) for AD include oral agents, such as upadacitinib, baricitinib, and abrocitinib, and a topical formulation, such as ruxolitinib. These therapies differ in their JAK-binding site selectivity, as abrocitinib and upadacitinib selectively inhibit JAK1, whereas baricitinib inhibits both JAK1 and JAK2.7 Abrocitinib, the most selective JAK inhibitor for AD, has demonstrated significant efficacy in alleviating pruritus and skin inflammation compared with other therapeutic option.8
However, real-world experience regarding the use of abrocitinib remains limited, especially in terms of practical considerations prior to its initiation and strategies employed during the maintenance phase. Furthermore, the utilization of systemic therapies for atopic dermatitis in India is low, with limited access to JAK inhibitors. This narrative review provides a practical approach to abrocitinib use in Indian patients with AD based on expert opinions on patient selection, optimal dosing patterns, monitoring, and strategies for the maintenance phase.6
To bridge this gap, a panel of 10 dermatologists with more than 15 years of experience in AD management (expert panel) convened to share their practice-driven strategies with abrocitinib. This process consisted of three stages: literature review, a survey conducted among clinical dermatologists, and panel discussion to develop practical treatment strategies for abrocitinib.
Methodology
This manuscript presents expert recommendations derived from a structured literature review, a survey of practicing dermatologists, and expert panel discussions, rather than a formal Delphi-based consensus process.
The goal of the literature search was to review real-world experiences with abrocitinib in moderate-to-severe atopic dermatitis. Relevant studies were identified through databases including PubMed, Scopus, and Google Scholar between September 2025 and November 2025. The literature was reviewed to identify key clinical domains, including ideal patient profiles, dosing preferences, treatment duration, step-down strategies, maintenance of remission, safety considerations, laboratory monitoring, and use in special populations. Based on the literature review, a structured survey questionnaire was developed and validated by the expert panel to capture real-world clinical practices and prescribing patterns. A pan-India survey was subsequently conducted among 36 dermatologists who had ≥12 months of prescribing experience with abrocitinib and over 15 years of clinical and academic experience in managing atopic dermatitis. The survey aimed to gather insights into clinical decision-making, treatment approaches, and practical challenges. The findings from the survey were qualitatively analyzed and used to inform expert recommendations. These insights were further discussed and refined during expert panel meetings, where practical recommendations were formulated and validated based on collective clinical experience. As this was not a formal consensus exercise, predefined agreement thresholds, anonymous voting, or multiple iterative rounds of voting were not employed (Figure 1).
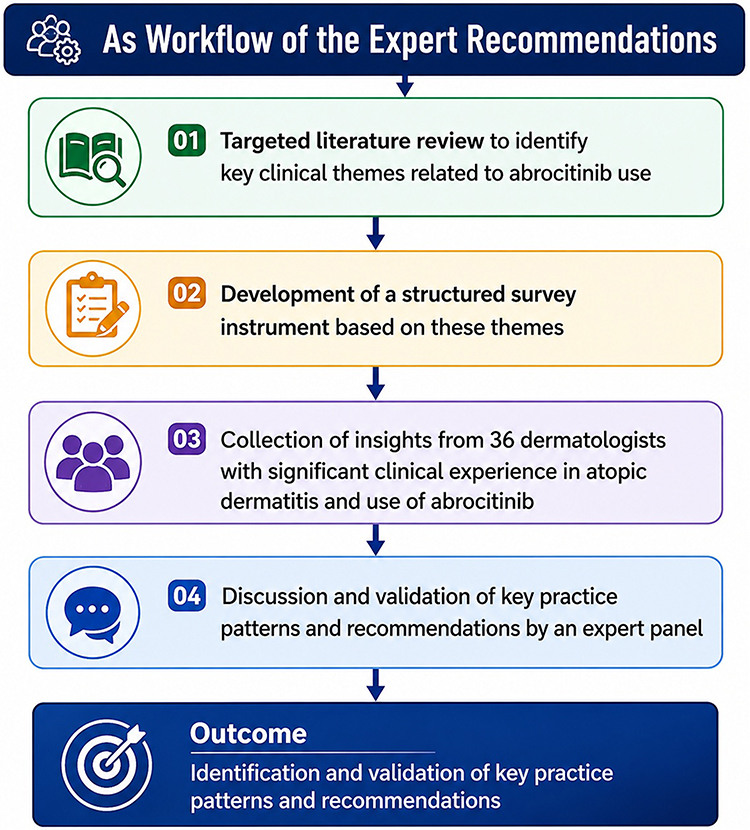 |
Figure 1 Workflow of the expert recommendation. |
Results
This section is based on survey-derived clinical insights and expert panel recommendations, while detailed interpretation and mechanistic discussion are provided in the discussion section. Following the two rounds of virtual meetings, an expert panel of dermatologists reached an agreement regarding the management of atopic dermatitis (AD) and developed a practical treatment strategy for abrocitinib in moderate-to-severe AD. This process culminated in the formation of seven expert recommendation statements organized into five sections: i. optimal positioning of JAK inhibitors, ii. Patient profile of abrocitinib diagnostic evaluation, iv. Preferred Dosing as monotherapy and concomitant medication versus maintenance of remission (Table 1).
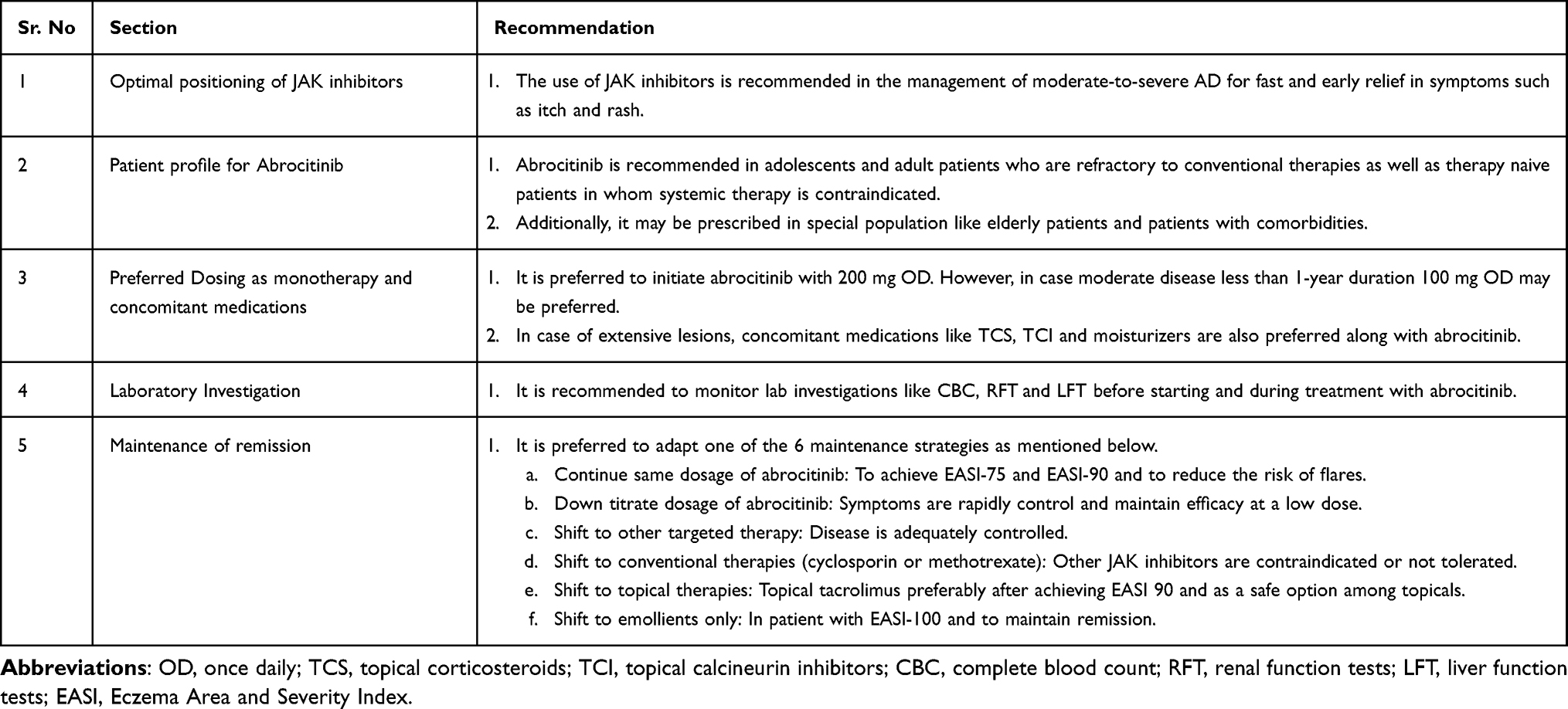 |
Table 1 Expert Recommendations |
Discussion
The dermatology expert panel reached an agreement on seven key statements as follows:
Optimal Positioning of JAK Inhibitors
JAK1 inhibitors play a pivotal role in the management of moderate-to-severe AD, as they offer the advantage of modulating/inhibition of the JAK-STAT Pathway. This inhibition curtails the intracellular signaling of several pro-inflammatory cytokines, particularly: Interleukin-4 (IL-4), Interleukin-13 (IL-13), Interleukin-31 (IL-31), and interferon-γ (IFN-γ) which are responsible for inflammation, pruritus (itching), and skin barrier dysfunction.9 Henceforth, treatment with JAK inhibitors is associated with achieving high-threshold efficacy endpoints such as rapid relief in itch and improvement in disease severity from the start of the treatment. This was further reinforced by findings from the JAK1 Atopic Dermatitis Efficacy and Safety (JADE) clinical trials and a head-to-head comparison with dupilumab, underscoring the advantages of abrocitinib in terms of the speed of onset and depth of response.10
The expert panel broadly concurred that use of JAK inhibitors (JAKi) is recommended as a part of continuum strategy for the management of moderate-to-severe AD for fast and early relief in symptoms such as itch and rash. Moreover, comparing all the available oral JAKi, abrocitinib shows highest selectivity for JAK1 with substantially higher IC50 values for JAK2 and JAK3 compared to upadacitinib, baricitinib, and tofacitinib. Specifically, abrocitinib demonstrated IC50 values of 29 nmol/L for JAK1, 803 nmol/L for JAK2, >10,000 nmol/L for JAK3, and 1250 nmol/L for TYK2, indicating a strong preference for abrocitinib to minimize off-target effects on other JAK isoforms.8 The recently published AD consensus by Sarkar et al also highlights the use of JAK inhibitors in AD management. The article recommended cautious use of tofacitinib owing to the lack of clinical data. However, Sarkar et al recommended the judicious use of abrocitinib in lieu of cost considerations. Hence, experts have recommended the positioning of abrocitinib in the management of AD over other JAK inhibitors such as tofacitinib, especially in India.11
Patient Profile for Abrocitinib
Abrocitinib may be used in most adults and adolescents with moderate-to-severe AD after personalized benefit–risk assessments. Abrocitinib is not indicated for pregnancy or lactating.6 Patients who present with inadequately managed or active infections such as hepatitis B or C and tuberculosis should not take abrocitinib until these conditions are treated appropriately.6 Patients with a previous history of human immunodeficiency virus (HIV) infection, recurrent hepatitis B or C, or those who present with a high risk of undiagnosed disease should be assessed before initiating treatment.6
As there is a potential risk associated with JAK inhibitors, such as MACE, VTE, and malignancies, it is essential to assess baseline risk before abrocitinib initiation. This is also supported by randomized clinical trials and an ongoing long-term JADE extension study, highlighting the importance of evaluating the baseline risk and special considerations for patients aged ≥65 years, in patients with current or past long-term history of smoking, and those at increased risk of MACE (eg. previous history of ASCVD, including myocardial infarction or stroke) or VTE (eg. personal or family history of pulmonary embolism [PE] or deep vein thrombosis [DVT]), or with malignancy risk factors (eg. current malignancy or history of malignancy).6 If a patient presents with clinical comorbidities or other VTE risk factors, such as obesity, prothrombotic disorder, recent trauma or major surgery, or prolonged immobilization, abrocitinib needs to be prescribed with caution. Available clinical data have highlighted that estrogen-containing oral contraceptive pills and hormone replacement therapy also pose a risk of VTE. However, no VTE cases were reported in abrocitinib-treated female patients who received hormonal contraceptives. A single case of VTE (nonfatal bilateral PE) was reported in a patient who received hormone replacement therapy. In cases of past or current history of malignancy, the benefits and risks of JAK inhibitor use in patients should be evaluated according to the severity of the malignancy.6
Abrocitinib in Different Patient Profiles
Emerging real-world evidence, case series, and randomized trials highlight abrocitinib as a safe and efficacious therapy across diverse groups of patients, including pruritus‑dominant AD,12 head‑and‑neck dermatitis (HND),13 hand eczema in patients with atopic dermatitis,14 elderly patients with multiple comorbidities, and patients who do not respond to conventional, selective, or non-selective JAK inhibitors or biologics15(Table 2).
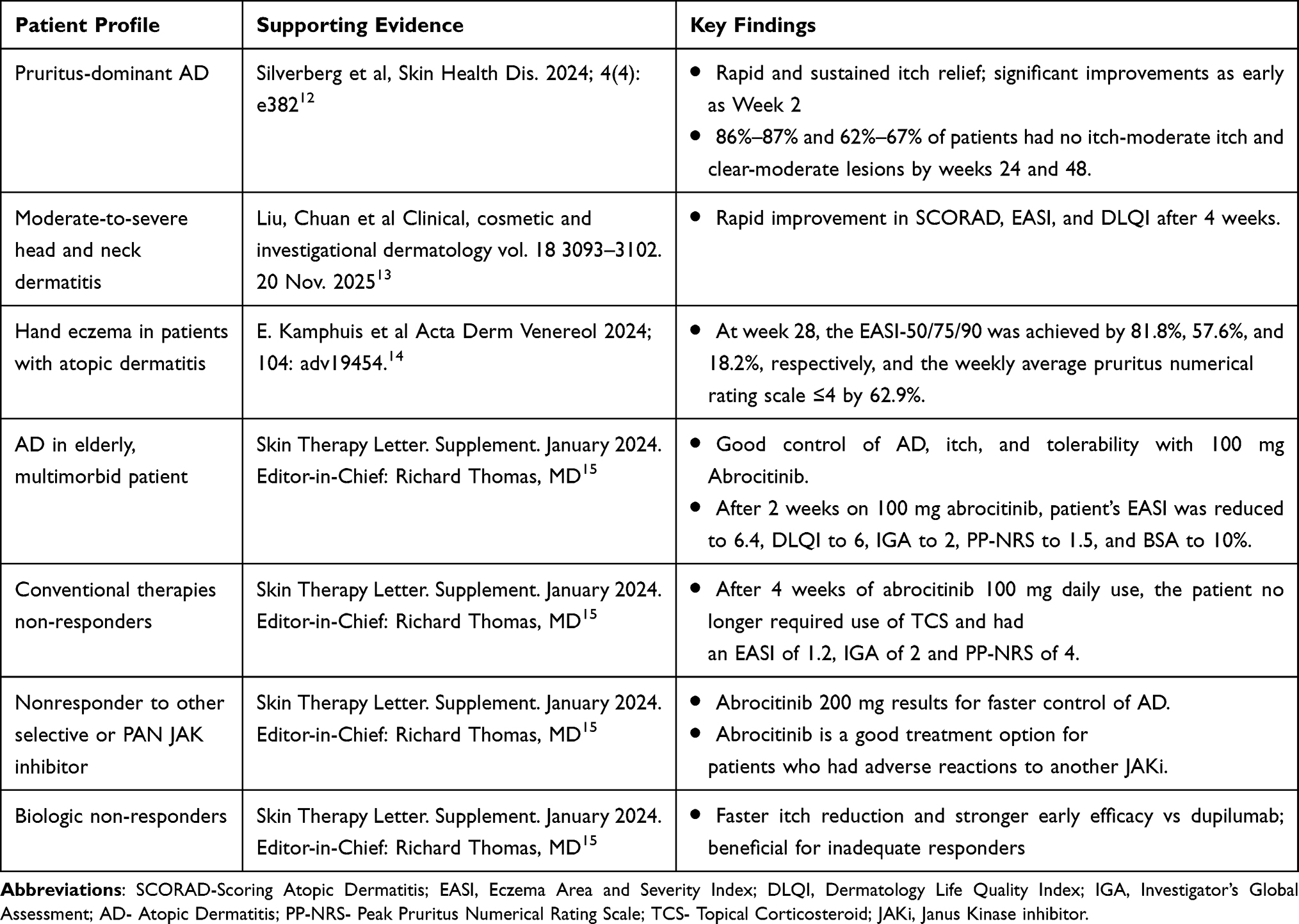 |
Table 2 Summary of the Published Evidence on Abrocitinib in Different Patient Profiles |
The expert panel agreed that abrocitinib is suitable for AD patients who remain uncontrolled on conventional systemic therapies, regardless of disease severity or comorbidities.
Diagnostic Evaluation
If abrocitinib is considered an appropriate treatment, a complete blood count (including platelet count, absolute lymphocyte count [ALC], absolute neutrophil count [ANC], and hemoglobin), lipid parameter measurements, measurements of transaminases, renal function testing, and screening for hepatitis B or C and HIV in accordance with clinical guidelines and local treatment protocols prior to immunosuppressive treatment should be performed.6 Patients should also be evaluated and tested for tuberculosis before initiating abrocitinib; yearly screening should be considered, especially in patients from highly endemic areas. Screening tests, including interferon-γ-release assays (eg. QuantiFERON), tuberculin skin tests, enzyme-linked immunosorbent assay (ELISA) tests, and/or chest X-rays, should be performed before initiating treatment in both adult and adolescent patients.6
Chest radiography may be used along with the QuantiFERON test or only if a patient tests positive using the QuantiFERON test as per the diagnostic criteria. In JADE clinical trials, including adult and adolescent patients, a dose-dependent decrease in platelet count was noted at week 4.6 The median platelet counts subsequently increased and attained a plateau at week 12, and the final 12-week values remained below baseline but were within the normal range. Thrombocytopenia (< 75×103 platelets/mm3) is rare but is more commonly observed in patients aged ≥65 years with an abrocitinib dosage of 200 mg OD. No change over time was observed in ANC, ALC, or hemoglobin; however, in rare cases, lymphopenia has been observed.6
Blood lipid levels should be evaluated before initiating abrocitinib and at week 4 following treatment initiation and managed as needed in consultation with the physician.6 In the JADE clinical trials, abrocitinib was associated with a dose-dependent increase in low-density lipoprotein cholesterol (LDL-C) levels from baseline to week 16, with no notable change in the LDL-C/high-density lipoprotein cholesterol (HDL-C) ratio over 16 weeks.6
It is recommended that patients be evaluated periodically (4 weeks after treatment initiation or 4 weeks after dose increase) during abrocitinib treatment to assess any changes from the baseline, as shown in (Table 3).
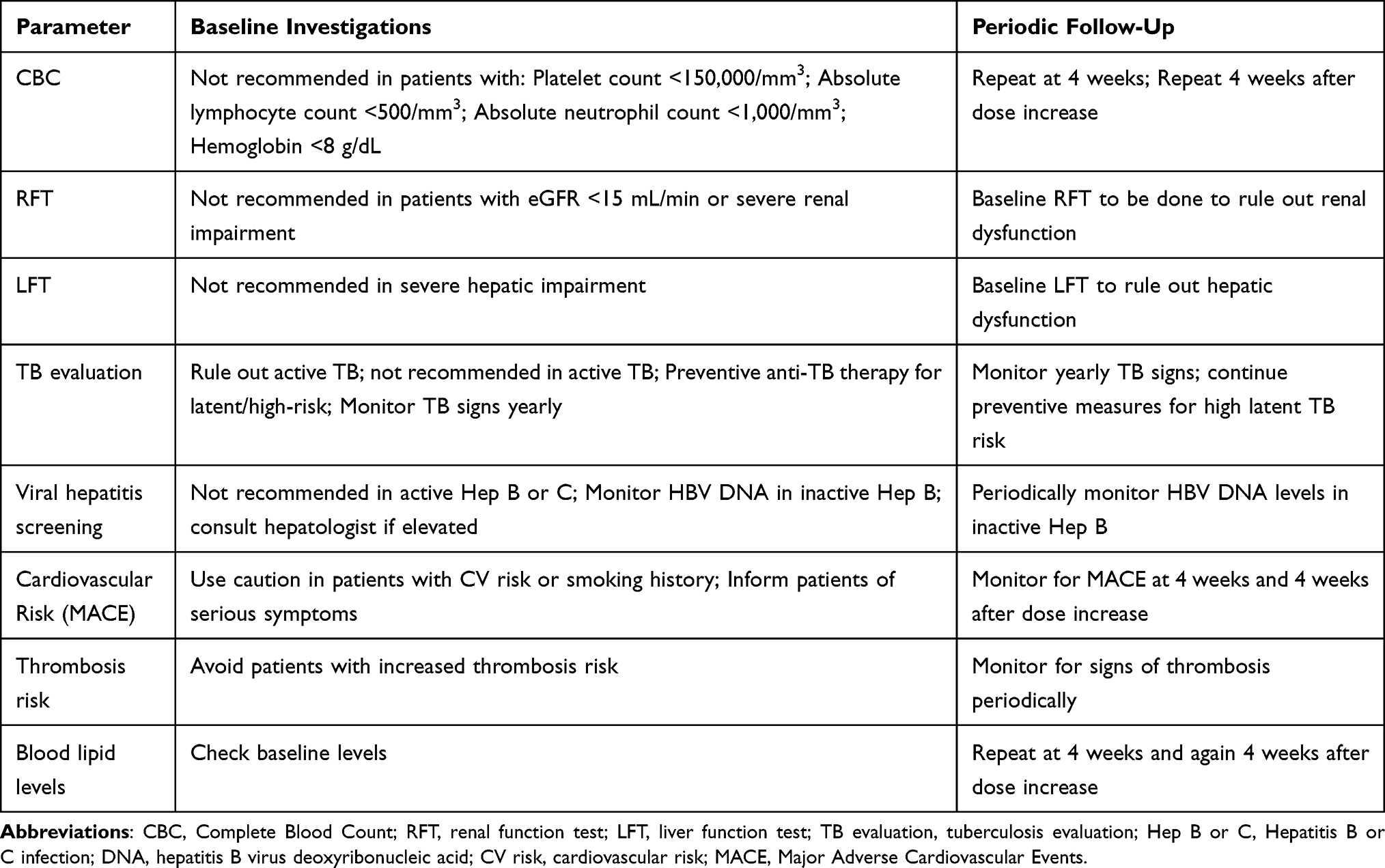 |
Table 3 Baseline Investigations and Monitoring Suggestion for Oral Abrocitinib5,6 |
The expert panel reached a high level of agreement that abrocitinib therapy requires baseline monitoring of lab investigations like hematologic, hepatic, renal, infections, cardiovascular, thrombotic and lipid parameters, followed by focused monitoring at 4 weeks and after dose adjustments. Also, periodically monitor for the sign of cardiovascular events, thrombosis, and lipid changes.
Vaccination
Prior to initiating treatment with abrocitinib, it is recommended that all patients should complete appropriate vaccines including non-live HZ vaccination (eg. Zoster Vaccine Recombinant, Adjuvanted) approximately 2–4 weeks before abrocitinib initiation, especially those who are at a higher risk of HZ (≥50 years old, immunosuppressed, or immunodeficient).6
In patients who already receive abrocitinib, non-live vaccines can be administered at any point during therapy without stopping treatment. Patients should avoid live vaccines immediately starting with, during, and immediately after abrocitinib treatment. It was recommended stopping Live vaccines should be stopped up to at least 1 week before starting abrocitinib and should wait for at least 2–4 weeks after stopping treatment, depending on the vaccine product label.6
Preferred Dosing as Monotherapy and Concomitant Medications
In clinical practice, decisions on appropriate dosing are governed by many clinical factors and patient considerations. However, the overarching goal for both clinicians and patients are to achieve long-term control of AD symptoms, which improves the quality of life with minimal safety concerns.6
Considerations for Abrocitinib as Monotherapy
Patients who present with moderate-to-severe AD for more than 1 year have a recent history of inadequate response to topical medications (topical corticosteroids or topical calcineurin inhibitors administered for ≥4 weeks), history of topical AD treatments being considered medically inadvisable, or requiring systemic therapies to control their disease.15 In these patients, a starting dose of abrocitinib 200-mg once daily should be considered to achieve rapid control. For patients with tolerability concerns or age over 65 years with comorbid conditions such as renal, cardiovascular, and hepatic conditions, a starting dose of 50 or 100 mg of abrocitinib once a day may provide effective disease control while minimizing safety risks.6
This recommendation is consistent with the findings from JADE MONO I and II clinical trials; patients initiated on abrocitinib 200 mg demonstrated higher response rates than those initiated on 100 mg as the starting dose.16,17 By week 12, 61.0%, 44.5%, and 10.4% of patients in the abrocitinib 200 mg, 100 mg OD, and placebo groups achieved ≥75% improvement in the Eczema Area and Severity Index (EASI-75).16,17 Similarly, EASI-90 responses were achieved by 37%, 23.9%,3.9% of patients in the 200 mg, 100 mg OD, and placebo groups, respectively. A comparable trend was observed in pruritus reduction, with 57%, 38%, and 15% of patients in the abrocitinib 200 mg, 100 mg OD, and placebo groups, respectively, achieving a PP-NRS4 score by week 12.16,17
Considerations When Using Abrocitinib in Combination Approaches
In patients with a clinical diagnosis of moderate-to-severe atopic dermatitis for at least 6 months, treatment with systemic therapies for the control of atopic dermatitis within the past year or had an inadequate response to at least 4 consecutive weeks of treatment with medicated topical therapy for atopic dermatitis within the past 6 months.16,18 Patients with moderate-to-severe atopic dermatitis, defined as an affected body surface area of 10% or more, investigator’s Global Assessment of 3 or higher, EASI of 16 or higher, and PP-NRS of 4 or higher at baseline.18 In these patients, topical corticosteroids (TCS), topical calcineurin inhibitors (TCI), and moisturizers may be used in combination with abrocitinib 200 mg to enhance the treatment response and optimal control of the disease.18
As the combination of abrocitinib with other systemic therapies has not been studied, its concomitant use is not recommended in clinical practice because of the potential risk of additive immunosuppression.6 Likewise, no clinical evidence exists for combination phototherapy, and this approach is not recommended because of the potentially increased risk of malignancies such as melanoma or non-melanoma skin cancer.6
The expert panel agreed with above discussion and further emphasized that abrocitinib 200 mg should be considered for moderate to severe with disease duration more than 1 year, while 100 mg for those with moderate disease severity and disease duration under one year.
A structured induction plan for abrocitinib treatment was planned to use personalized dosing and careful baseline and follow-up monitoring (Figure 2).
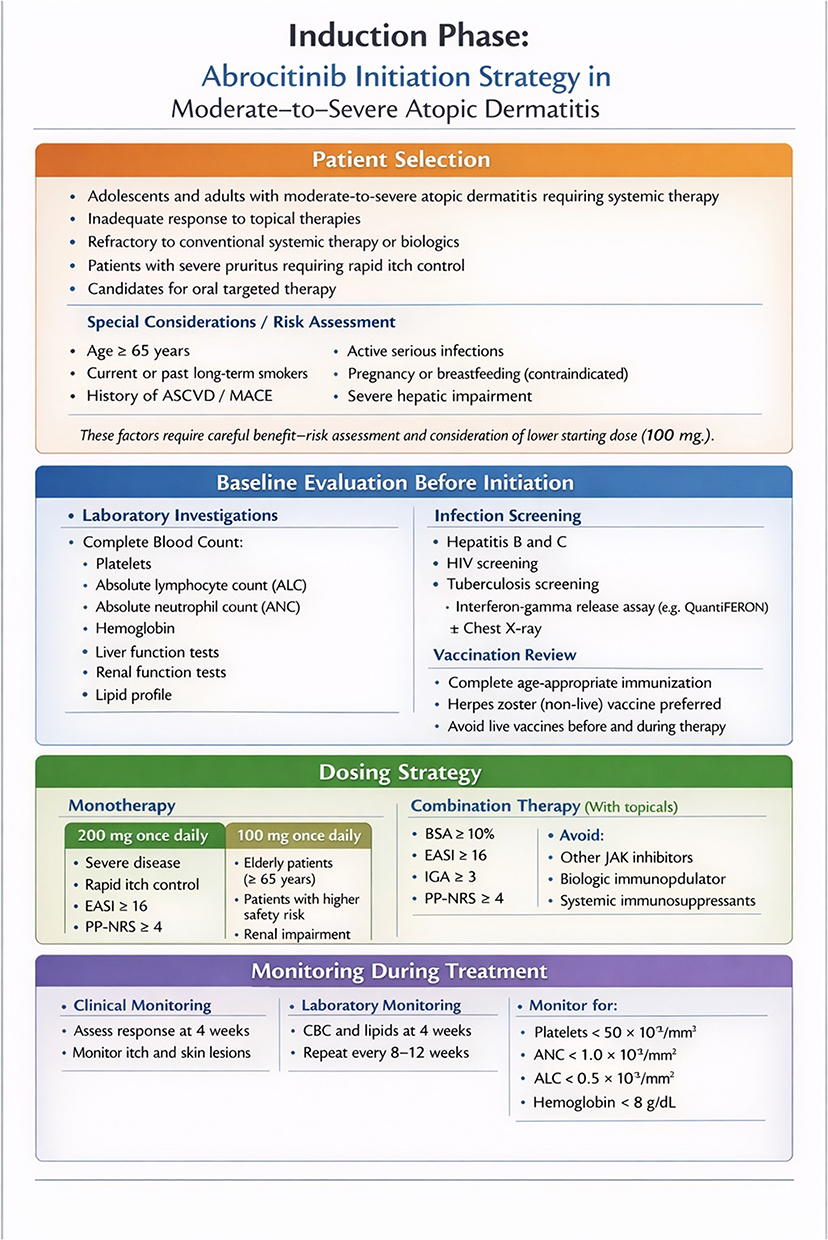 |
Figure 2 Induction phase: Abrocitinib initiation strategy in moderate to severe atopic dermatitis. |
Maintenance of Remission
Published data from the JADE clinical development program supports multiple dosing strategies for both treatment and maintenance phases. Dermatologists can adapt these strategies for long-term disease management to achieve sustained remission (Figure 3).
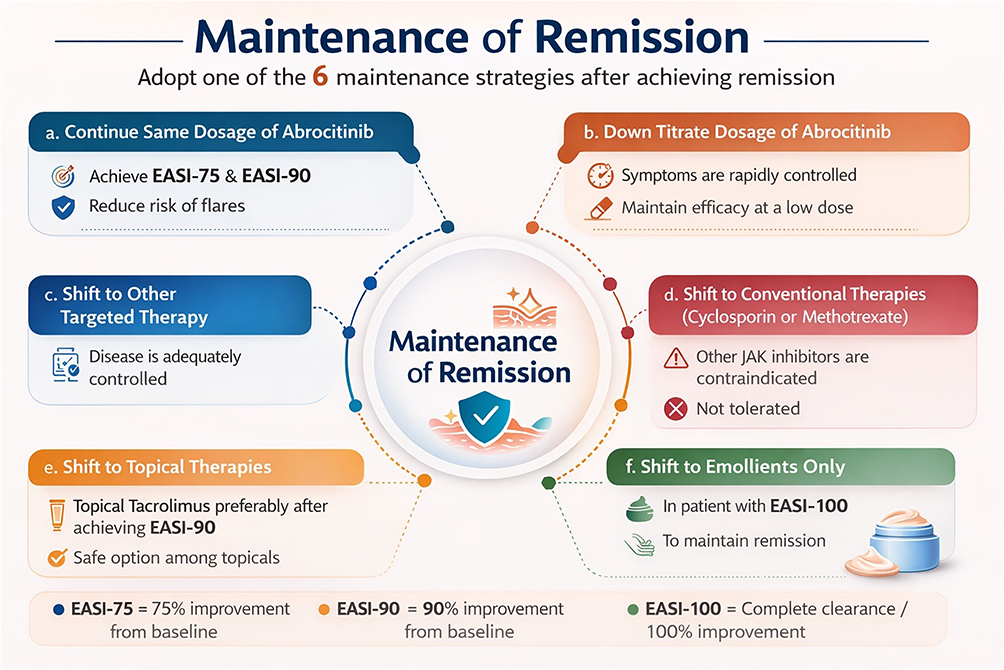 |
Figure 3 Maintenance of remission. |
Maintain the Same Starting Dose of Abrocitinib
In the JADE REGIMEN trial, the maintenance therapy of abrocitinib 200 mg significantly reduced the risk of flares and loss of IGA 0/1 response compared with 100 mg and placebo over 40 weeks, with relative risk reductions of 90% and 78%, respectively.19 Hence, abrocitinib 200 mg is preferred to attain EASI‑75 and EASI‑90 and evidence from clinical trials shows better maintenance of response and lower risk of flare with a higher dose.19
Down Titrate the Starting Dosage of Abrocitinib
In the JADE REGIMEN trial, out of 1233 patients who entered the open-label phase of JADE REGIMEN and received the abrocitinib 200-mg dose, 798 (64.7%) patients achieved response per protocol, of which 265 were randomly allocated (down-titrated) to 100 mg.19 Response rates with abrocitinib 200 mg to 100 mg down-titration were greater compared to treatment withdrawal (placebo) through the maintenance period from week 4 after randomization up to week 40. For example, the EASI-75 response rate at the end of the 40-week maintenance period was 46.5%, which was substantially higher than that of the placebo (14.0%).19 Among patients who were down-titrated from 200-mg dose to 100 mg, 60.8% were also able to maintain a response for the 40-week maintenance period without a flare or need for rescue treatment, compared with 23.6% of patients in the placebo (treatment withdrawal) arm. Henceforth, considering the above evidence, if symptoms are rapidly controlled clinically, stepping down to 100 mg may be a viable option for maintaining efficacy at a low dose.19,20
Shift From Abrocitinib to Other Targeted Therapy
In a 16‑week retrospective study of moderate-to-severe AD comparing abrocitinib, tofacitinib, and cyclosporine, abrocitinib demonstrated greater reductions in mean scores, with EASI improvements of 87% versus 64% and 51%, and NRS improvements of 85% versus 62% and 51%, respectively.21 Hence, in patients with financial constraints or whose disease is adequately controlled, a switch to more affordable targeted therapies such as generic upadacitinib, baricitinib, or tofacitinib should be considered.21
Shift From Abrocitinib to Conventional Therapies
From clinical data and case reports, it has been observed that conventional therapies such as cyclosporine and methotrexate may be used as maintenance therapy at the lowest effective dose to sustain disease control while minimizing risks*.22 Some dermatologists have also shared real-world experiences suggesting that methotrexate can be combined with abrocitinib as an exit strategy for abrocitinib after remission and may be preferable for long-term maintenance. Hence, in patients with financial constraints or in whom other JAK inhibitors are contraindicated or not tolerated, switching to conventional therapies such as cyclosporine or methotrexate may be considered, as these agents have been reported to be relatively safe drugs to maintain the long-term management of moderate-to-severe AD patients.23
* Robust evidence is lacking in adults; further research studies are required to evaluate the safety and tolerability of intermittent or other maintenance cyclosporine strategies in patients with AD.
Shift From Abrocitinib to Topical Therapies
Patients who are in remission phase after abrocitinib monotherapy but experience intermittent flares, and in whom systemic therapies and long-term continuous use of TCS are not recommended. Among them, abrocitinib 200 mg plus medicated topical therapy was an acceptable approach to regain response in patients who experienced a flare, as supported by the JADE REGIME trial during the rescue treatment period. Another way is to adopt sequential therapy with TCS and TCI. This concept is aligned with published systematic reviews and meta-analyses pooling data from two trials and found that sequential therapy with TCS TCI was comparable to monotherapy (TCS or TCI) or emollients. This approach emphasizes not only targeting active lesions but also adopting sequential therapy with an acceptable safety profile.24 A large cohort study by Koo et al and Hanifin et al reported significant findings on tacrolimus ointment for atopic dermatitis, with Koo’s large trial showing effectiveness and good safety over nearly two years in almost 8000 patients, and Hanifin’s study demonstrated benefits for up to four years, highlighting tacrolimus as a valuable long-term option for moderate-to-severe eczema, especially for sensitive areas such as the face. Hence, after attaining EASI, 90 patients can be maintained on other topical therapies, such as tacrolimus, for a longer duration as the safest option in topicals.25
Shift to Emollients Only
According to a recent review article, regular use of emollients prolongs flare-free periods and alleviates symptom intensity during remission in adults. Therefore, once a patient achieves EASI-100, transition to emollient-only therapy is recommended to maintain remission.26 Similar evidence has also been highlighted in the recently published AD consensus by Sarkar et al that moisturizers form the cornerstone of management and offer steroid-sparing benefits in the management of AD.11 The following summarizes the six key strategies for effective maintenance in atopic dermatitis. The findings in these expert recommendations are also aligned with emerging international and European guidelines, which increasingly support the positioning of abrocitinib in patients requiring rapid symptom control or those inadequately managed with other systemic agents. Real-world expert consensus data, including the Italian Delphi consensus (Gargiulo et al, 2024), further reinforce the role of JAK inhibitors in routine clinical practice, particularly emphasizing individualized treatment decisions and safety monitoring.27 Long-term safety considerations remain critical, particularly with respect to cardiovascular events, thromboembolic risks, malignancies, and laboratory abnormalities. Treatment adherence may be positively influenced by the rapid onset of itch relief and the oral route of administration.27 In the Indian context, cost-effectiveness and treatment accessibility are important factors influencing therapeutic decisions. In addition, potential differences in disease phenotype, comorbidities, and environmental exposures between Asian and Western populations highlight the need for region-specific clinical guidance. Finally, the incorporation of treat-to-target strategies in atopic dermatitis management represents an evolving paradigm, emphasizing predefined goals such as itch reduction, improvement in EASI scores, and quality-of-life outcomes, with treatment optimization based on patient response.
Conclusion
Abrocitinib, a highly selective JAK1 inhibitor, offers rapid itch relief, sustained skin clearance, and improved quality of life in patients with moderate-to-severe atopic dermatitis. The expert recommends initiating therapy with 200 mg for severe diseases, followed by titration to the lowest effective dose for maintenance. Regular monitoring of laboratory parameters and individualized risk assessments are essential for safe use. Maintenance strategies include dose adjustment, switching to other targeted or conventional therapies, and transitioning to topical agents or emollients after remission is achieved. These recommendations provide a practical framework for optimizing long-term management of AD in clinical practice.
Ethics Statement
According to the Indian Council for Medical Research (ICMR) guidelines, research involving educational practices such as instructional strategies, evaluation of teaching effectiveness, or comparison of instructional techniques, curricula, or classroom management methods may be exempt from an ethics committee review. Therefore, ethics committee approval was not required for this study.
The ICMR guidelines also state that voluntary informed consent may be waived when the research involves no more than minimal risk, when there is no direct interaction between the researcher and the participants, or when the consent waiver is justified. Based on these provisions, informed consent was not required for this study. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Disclosure
Rickson Pereira reports Honoraria from Received for presentations, outside the submitted work. Soumya Jagadeesan reports Honoraria from Pfizer, Glenmark; Data safety/advisory board participation from Pfizer, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Plant A, Ardern-Jones MR. Advances in atopic dermatitis. Clin Med. 2021;21(3):177–12. doi:10.7861/clinmed.2021-0280
2. Weidinger S, Beck LA, Bieber T, et al. Atopic dermatitis. Nat Rev Dis Primers. 2018;4(1). doi:10.1038/s41572-018-0001-z
3. Grajales DB, Sewdat N, Leo R, Kar S. Unveiling abrocitinib: a thorough examination of the 2022 USFDA-approved treatment for Atopic Dermatitis (AD). Med Drug Discovery. 2023;10:100161. doi:10.1016/j.medidd.2023.100161
4. Shergill M, Bajwa B, Yilmaz O, Tailor K, Bouadi N, Mukovozov I. Biologic and small molecule therapy in atopic dermatitis. Biomedicines. 2024;12(8):1841. doi:10.3390/biomedicines12081841
5. Narcisi A, Di Lernia V, Esposito M, et al. Risk assessment in atopic dermatitis: guidance from a multidisciplinary expert panel. Dermatol Ther (Heidelb). 2025;15(5):1063–1078. PMID: 40164817; PMCID: PMC12033143. doi:10.1007/s13555-025-01391-5
6. Gooderham MJ, de Bruin-Weller M, Weidinger S, et al. Practical management of the JAK1 inhibitor abrocitinib for atopic dermatitis in clinical practice: special safety considerations. Dermatol Ther. 2024;14(8):2285–2296. doi:10.1007/s13555-024-01200-5
7. Schlösser AR, Caron AGM, Den Ouden MS, et al. Successful dose reduction of Janus-kinase Inhibitors in well-controlled atopic dermatitis: a prospective, multicentre, real-world study. Acta dermato-venereologica. 2025;105:adv44165. doi:10.2340/actadv.v105.44165
8. Rosenberg A, Zakria D, DeBusk L, et al. How Janus kinase selectivity impacts efficacy and safety of abrocitinib for atopic dermatitis: an expert consensus panel. Dermatol Online J. 2025;31(4). doi:10.25251/wfz5mg56
9. Ray A, Pandhi D. Abrocitinib: a comprehensive review of its use in dermatology beyond atopic dermatitis. Indian J Skin Allergy. 2025;4:25–42. doi:10.25259/IJSA_54_2024
10. Nogueira M, Torres T. Janus kinase inhibitors for the treatment of atopic dermatitis: focus on abrocitinib, baricitinib, and upadacitinib. Dermatol Pract Concept. 2021;11(4):e2021145. doi:10.5826/dpc.1104a145
11. Sarkar R, Mohapatra L, Gupta D, et al. Standardising the diagnosis and management of atopic dermatitis in India: a consensus statement by the modified Delphi method by IADVL Special Interest Group of Pediatric Dermatology (STAND AD). Indian J Dermatol Venereol Leprol. 2025:1–11. doi:10.25259/IJDVL_1102_2025
12. Silverberg JI, Thyssen JP, Lazariciu I, Myers DE, Güler E, Chovatiya R. Abrocitinib may improve itch and quality of life in patients with itch-dominant atopic dermatitis. Skin Health Dis. 2024;4(4):e382. doi:10.1002/ski2.382
13. Liu C, Pan Y, Xiong J, Saputra AD, Chen S, Cai T. Abrocitinib for head and neck dermatitis: case series and literature review. Clini Cosmet Investig Dermatol. 2025;18: 3093–3102. doi:10.2147/CCID.S549045
14. Kamphuis E, Boesjes CM, Loman L, et al. Real-world experience of abrocitinib treatment in patients with atopic dermatitis and Hand Eczema: up to 28-week results from the BioDay Registry. Acta Derm Venereol. 2024;104:adv19454. doi:10.2340/actadv.v104.19454
15. Lynde CW, Andriessen A, Barankin B, et al. Real world insights from atopic dermatitis patients treated with abrocitinib. Skin Ther Lett. 2024;(Suppl):1–9.
16. Simpson EL, Sinclair R, Forman S, et al. Efficacy and safety of abrocitinib in adults and adolescents with moderate-to-severe atopic dermatitis (JADE MONO-1): a multicentre, double-blind, randomised, placebo-controlled, phase 3 trial. Lancet. 2020;396(10246):255–266. doi:10.1016/S0140-6736(20)30732-7
17. Silverberg JI, Simpson EL, Thyssen JP, et al. Efficacy and safety of abrocitinib in patients with moderate-to-severe atopic dermatitis: a randomized clinical trial. JAMA Dermatol. 2020;156(8):863–873. doi:10.1001/jamadermatol.2020.1406
18. Reich K, Thyssen JP, Blauvelt A, et al. Efficacy and safety of abrocitinib versus dupilumab in adults with moderate-to-severe atopic dermatitis: a randomised, double-blind, multicentre phase 3 trial. Lancet. 2022;400(10348):273–282. doi:10.1016/S0140-6736(22)01199-0
19. Blauvelt A, Silverberg JI, Lynde CW, et al. Abrocitinib induction, randomized withdrawal, and retreatment in patients with moderate-to-severe atopic dermatitis: results from the JAK1 Atopic Dermatitis Efficacy and Safety (JADE) REGIMEN phase 3 trial. J Am Acad Dermatol. 2022;86(1):104–112. doi:10.1016/j.jaad.2021.05.075
20. Silverberg JI, Simpson E, Gooderham M, Weidinger S, Watkins M, Alderfer J. Tailoring abrocitinib treatment for moderate-to-severe atopic dermatitis to patient disease course: a narrative review. Dermatol Ther. 2025. doi:10.1007/s13555-025-01618-5
21. Bashir S. Clinical assessment of abrocitinib, tofacitinib, and cyclosporine in adult patients with moderate to severe atopic dermatitis: a retrospective analysis. Cureus. 2025;17(6):e85448. doi:10.7759/cureus.85448
22. Camp RD, Reitamo S, Friedmann PS, Ho V, Heule F. Cyclosporin A in severe, therapy-resistant atopic dermatitis: report of an international workshop, April 1993. Br J Dermatol. 1993;129(2):217–220. doi:10.1111/j.1365-2133.1993.tb03532.x
23. Lee JH, Yun S-J, Lee J-B, et al. Therapeutic efficacy and safety of methotrexate in moderate-to-severe atopic dermatitis: a retrospective study of Korean patients at tertiary referral hospital. Ann Dermatol. 2020;32(5):402–408. doi:10.5021/ad.2020.32.5.402
24. Dhar S, De A, Saha A, et al. Intermittent or sequential topical Tacrolimus in atopic dermatitis: systematic review and meta-analysis. Cureus. 2023;15(12):e50640. doi:10.7759/cureus.50640
25. Koo JY, Fleischer AB, Abramovits W, et al. Tacrolimus ointment is safe and effective in the treatment of atopic dermatitis: results in 8000 patients. J Am Acad Dermatol. 2005;53(2 Suppl 2):S195–S205. doi:10.1016/j.jaad.2005.04.063
26. Kowalska MK, Orłowska SM, Bednarczyk Ł. Applied research on atopic dermatitis with special emphasis on the role of emollients in this disorder: a review. Appl Sci. 2024;14:8315. doi:10.3390/app14188315
27. Gargiulo L, Ibba L, Malagoli P, et al. Management of patients affected by moderate-to-severe atopic dermatitis with JAK inhibitors in real-world clinical practice: an Italian Delphi Consensus. Dermatol Ther. 2024;14(4):919–932. PMID: 38509380; PMCID: PMC11052938. doi:10.1007/s13555-024-01135-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Successful Treatment of Atopic Dermatitis with a Predominant Nipple Involvement by Abrocitinib During COVID-19 Pandemic: A Case Report
Teng Y, Tang H, Yu Y, Fan Y, Tao X, Xu D
Journal of Asthma and Allergy 2023, 16:789-792
Published Date: 1 August 2023
Abrocitinib Improved Dupilumab-Resistant Severe Atopic Dermatitis with Comorbid Mild Alopecia Areata in a 12-Year-Old Boy: A Case Report with 1-Year Follow-Up
Liu X, Song B, Jin H
Journal of Asthma and Allergy 2024, 17:305-311
Published Date: 2 April 2024
Concurrent Refractory Atopic Dermatitis and Generalized Vitiligo Successfully Treated with Abrocitinib: A Case Report
Shao X, Pan X, Chen Y, Zhu Y, Chen S, Chen J
Journal of Asthma and Allergy 2024, 17:1259-1263
Published Date: 3 December 2024
Abrocitinib for Head and Neck Dermatitis: Case Series and Literature Review
Liu C, Pan Y, Xiong J, Saputra AD, Chen S, Cai T
Clinical, Cosmetic and Investigational Dermatology 2025, 18:3093-3102
Published Date: 20 November 2025
Effectiveness of Abrocitinib in Atopic Dermatitis Presenting with Hand–Foot Eczema and Nail Dystrophy: A Case Report
Ma A, Deng Y
Clinical, Cosmetic and Investigational Dermatology 2026, 19:596189
Published Date: 1 May 2026