Back to Journals » Drug Design, Development and Therapy » Volume 19
Optimal Propofol Dose with Oxycodone for Visceral Pain Relief in Anxious Patients Undergoing Abortion: A Clinical Trial Report
Authors Chen L ![]() , Lu D, Zhang Y, Ji K, Long M, He K
, Lu D, Zhang Y, Ji K, Long M, He K ![]() , Xie K
, Xie K
Received 29 August 2025
Accepted for publication 28 November 2025
Published 18 December 2025 Volume 2025:19 Pages 11307—11316
DOI https://doi.org/10.2147/DDDT.S563921
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Anastasios Lymperopoulos
Lvlv Chen,1,2 Dajiang Lu,3 Yongguo Zhang,1 Kuiquan Ji,1 Mingbo Long,1 Kai He,1 Kangjie Xie4
1Department of Anesthesiology, The People’s Hospital of Qiannan, Duyun, Guizhou, 558000, People’s Republic of China; 2Qiannan Medical College for Nationalities, Duyun, Guizhou, 558000, People’s Republic of China; 3Department of Gynecology, The People’s Hospital of Qiannan, Duyun, Guizhou, 558000, People’s Republic of China; 4Department of Anesthesiology, First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 330300, People’s Republic of China
Correspondence: Kangjie Xie, Department of Anesthesiology, First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 330300, People’s Republic of China, Tel +86-13516721870, Email [email protected]
Introduction/Objective: Patients undergoing induced abortion frequently experience acute visceral pain and preoperative anxiety, the latter of which is known to increase anesthetic requirements. This study aimed to determine the median effective dose (ED50) and the 95% effective dose (ED95) of propofol in combination with oxycodone for alleviating visceral pain, specifically testing the finding that anxiety increases the needed propofol dose.
Methods: Female patients, who were scheduled for elective abortion surgeries, with PAS-7 ≥ 8 were classified as anxious group (Group A), while those with PAS-7 < 8 were classified as non-anxious group (Group N). Both groups received an intravenous dose of 0.10 mg/kg of oxycodone prior to surgery.And 2 to 3 minutes later, the first patient in the sequence received an initial dose of 3.50 mg/kg of propofol, with subsequent doses determined by Dixon’s up-and-down method.
Results: The ED50 (95% CI) for propofol was 1.96 mg/kg (1.87– 2.05) in Group N and 2.42 mg/kg (2.30– 2.53) in Group A; the ED95 (95% CI) was 2.10 mg/kg (2.03– 2.39) and 2.60 mg/kg (2.50– 2.95), respectively. The lack of overlap in the 95% confidence intervals indicates a statistically significant difference between groups.
Conclusion: The combination of 0.10 mg/kg oxycodone and propofol was effective for visceral pain suppression during artificial abortion. Notably, patients with anxiety required higher doses of propofol to achieve satisfactory pain relief during abortion surgeries.
Trial Registration: This human study was approved by the Medical Ethics Committee of the People’s Hospital of Qiannan (QNZY-QNYZKYRC-23-0801) and registered at https://www.chictr.org.cn/ (Date: 09/26/2023, ChiCTR2300076169).
Keywords: oxycodone, propofol, preoperative anxiety, visceral pain, abortion, effective dose
Introduction
Visceral pain is a chronic, non-malignant pain that originates from the organs in the abdomen and pelvis.1–4 During the perioperative period, gynecological abortion procedures often involve varying levels of visceral pain, primarily due to the surgical site.5,6 Severe visceral pain can cause atelectasis and heighten sympathetic nerve activity in patients, which negatively impacts the surgery.7–9 This condition necessitates higher doses of anesthetic drugs like propofol, prolonging both the operation and anesthesia recovery times.10
Patients undergoing abortion surgery often experience varying levels of anxiety, which can stem from multiple sources. Concerns about the surgical procedure and the risks associated with anesthesia are primary factors contributing to this anxiety. Additionally, worries about future fertility and the challenges of childbirth can further heighten these feelings.11,12 Research indicates that anxiety is a complex emotional state characterized by tension, worry, and fear.13 This heightened stress can result in negative physical effects, such as decreased pain tolerance and increased sensitivity to pain, which may complicate the patient’s physiological responses.14,15 This anxiety-induced hyperalgesia likely contributes to the increased demand for anesthetic agents. Propofol, a GABA_A receptor agonist, is the standard sedative-hypnotic used for such procedures. Beyond its sedative effects, propofol also possesses intrinsic anxiolytic properties by enhancing inhibitory neurotransmission in brain regions associated with fear and stress, such as the amygdala. Consequently, preoperative anxiety has been consistently shown to significantly increase the propofol dose required for anesthesia.16–18
The dual μ and κ opioid receptor agonism of oxycodone represents a promising therapeutic avenue for the targeted alleviation of both somatic and visceral pain, particularly in the context of postoperative pain management following abdominal surgeries, as supported by existing literature.19–21 Additionally, oxycodone has demonstrated a pivotal role in the management of cancer pain, neuropathic pain, and inflammatory pain, effectively reducing patients’ pain perception and mitigating concomitant symptoms of anxiety and depression.22,23
Chen et al’s research found that the combined use of propofol and oxycodone during abortion surgery can improve the anesthetic effect, reduce the dosage of propofol, and shorten the recovery time of postoperative orientation.24 Liu et al found through a randomized controlled study that the combined use of propofol and oxycodone in artificial abortion surgery can reduce the dosage of anesthetic drugs.25 However there is a lack of research on the impact of oxycodone on visceral pain in patients who are also dealing with anxiety currently.
In conclusion, we hypothesize that anxious patients require a higher propofol dose for effective visceral pain relief during abortion surgery when combined with oxycodone. The primary objective of this study was to determine the median effective dose (ED50) and the 95% effective dose (ED95) of propofol, administered alongside oxycodone, to alleviate visceral pain in patients experiencing preoperative anxiety during gynecological abortion surgeries. This research aims to clarify the complex relationship between visceral pain and anxiety while optimizing the effectiveness and accuracy of anesthesia. By identifying these dosing parameters, the study seeks to contribute to the development of more personalized anesthesia protocols in clinical settings. Ultimately, this could lead to improved patient care and better outcomes for those undergoing abortion surgery.
Methods
The study was approved by the Medical Ethics Committee of the People’s Hospital of Qiannan (Ethical approval number: QNZY-QNYZKYRC-23-0801) and registered at https://www.chictr.org.cn/ (registration number: ChiCTR2300076169). This work was financially supported by [Scientific Research Fund of Qiannan Medical College for Nantionaities] (Grant number Qnyz2023036). Written informed consent was obtained from all participants prior to the commencement of the study.
Patients who voluntarily consented to undergo painless abortion surgery were included in the study. Eligible participants were aged 18–50 years, had a BMI of 18–30 kg/m2, and were classified as American Society of Anesthesiologists (ASA) Physical Status I or II. Exclusion criteria included known allergies to the treatment drugs, evident difficult airways, mental illness, severe ischemic heart disease, chronic pain, and the use of opioids or nonsteroidal drugs within 48 hours before the abortion. Operation time longer than 5 minutes was also excluded.
All participants underwent an evaluation of preoperative anxiety using the perioperative anxiety scale-7 (PAS-7). Patients with a score of PAS-7 ≥ 8 were categorized into the anxious group (Group A), while those with a score of PAS-7 < 8 were placed in the non-anxious group (Group N). The anesthesiologist administering the drugs and assessing the primary outcome was not blinded to the patient’s group (A or N) due to the nature of the anxiety assessment. However, the researcher performing the statistical analysis was blinded to the group allocations.
All participants received a standardized anesthesia protocol. Prior to undergoing painless induced abortion, patients were instructed to fast for at least 8 hours. Upon arrival in the examination room, each patient was provided with 41% oxygen at a flow rate of 4 L/min via a nasal cannula, while vital signs were continuously monitored. After establishing peripheral intravenous access, patients received a 500 mL infusion of compound sodium chloride at a rate of 250 mL/h. Before the surgery, all patients were administered 0.10 mg/kg of oxycodone intravenously, followed by the administration of propofol 2–3 minutes later. Once the patient exhibited the absence of eyelash reflex, a uterine dilator was placed to proceed with the procedure.
The initial dose was determined to be 3.50 mg/kg for both the anxious group and the non-anxious group. A proportional variation of 0.9 was established between dosages, leading to the following dose increments: 3.50, 3.15, 2.84, 2.55, 2.30, 2.07, 1.86 and 1.67 mg/kg. To tailor the propofol dose for each subsequent patient, Dixon’s up-and-down method was employed. As a dose-finding study using Dixon’s up-and-down method, a formal power analysis is not standard practice. The sample size is determined by the sequential nature of the trial, which typically requires 6–8 crossover points per group to reliably estimate the ED50. The dosage was decreased if the abortion was completed successfully without any significant movements, such as trunk, limb, or head and neck movements, or coughing that could interfere with the procedure. Conversely, if any such movements occurred, the dose was increased. Additionally, a single intravenous dose of 20–50 mg of propofol was administered if the patient exhibited body movements or coughing during the abortion.
After the abortion, the patient was transferred to the Post Anesthesia Care Unit (PACU), where the anesthesiologist was responsible for awakening her. The anesthesiologist documented the patient’s recovery time, heart rate, blood pressure, and oxygen saturation (SpO2). Additionally, any episodes of nausea, vomiting, recovery agitation, or delayed recovery were recorded. Patients remained in the PACU for a minimum of 30 minutes. To assess patient recovery in the PACU, the Steward Score was utilized. Patients were discharged or transferred to the inpatient department once they demonstrated stable vital signs, were able to walk unassisted, achieved a Steward Score of at least 4, and exhibited no significant side effects, such as nausea or vomiting.
Primary Outcome and Assessment
The primary outcome was the effective dose (ED) of propofol that prevented a positive response to visceral pain, defined as significant movements of the trunk, limbs, or head/neck, or coughing that could interfere with the surgical procedure. This assessment was performed by the same senior anesthesiologist for all patients to ensure consistency. While this standardized the evaluation, the subjective nature of this endpoint is acknowledged as a study limitation.
Secondary Outcomes
Various clinical measurements were documented at specific time points: mean arterial pressure (MAP), heart rate (HR), and peripheral capillary oxygen saturation (SpO2) were recorded at 5 minutes after entering the operating room (T1), upon loss of consciousness (T2), during the procedure (T3), at the end of the procedure (T4), and at 5 (T5) and 10 minutes (T6) post-recovery.
Visual analog scale (VAS) scores and ramsay sedation scores were recorded at 5 and 10 minutes after recovery. Other monitored outcomes included postoperative nausea and vomiting (PONV), injection pain, respiratory depression, bradycardia, hypotension, and dizziness. Recovery time was defined as the interval between entering the anesthesia room and when the patient could open their eyes and respond when called. A recovery time exceeding 30 minutes was categorized as delayed recovery. To assess restlessness during the recovery period, the Ramsay sedation score was utilized, where a score of 1 indicated restlessness. Respiratory depression was identified by an SpO2 level below 90%, prompting the administration of jaw support, airway opening, and mask-assisted oxygen. Bradycardia was defined as a heart rate of less than 50 beats per minute, and atropine (0.3–0.5 mg) was given as needed. Hypotension was indicated by two consecutive MAP declines greater than 30% from the baseline, which warranted the administration of 5–10 mg of ephedrine to the patient.
Statistical Analysis
Statistical analysis was conducted using SPSS version 22.0 (SPSS Inc., Chicago, Illinois, USA). Data were presented as means with standard deviations (SD), medians with ranges, or as the number of patients (n), depending on their distribution. The primary outcome, the effective dose (ED50 and ED95) of propofol along with their 95% confidence intervals (95% CI), was calculated using Probit regression analysis. Sequential allocation and dose-effect graphs were created using GraphPad Prism software.
For secondary outcomes, categorical variables were analyzed using the Chi-square test or Fisher’s exact test, as appropriate. Continuous variables were tested for normality; normally distributed data were compared using the independent samples t-test (LSD-t), while non-normally distributed data were assessed using the Mann–Whitney U-test.
A p-value of less than 0.05 was deemed statistically significant.
Results
Between October 2023 and June 2024, a painless abortion was performed on 46 patients in this study, of whom 39 were analyzed using the Probit probability method. The seven excluded patients were due to protocol deviations (eg, surgery duration >5 minutes) or incomplete data. Participants were selected based on their preoperative anxiety assessment using the PAS-7 and were classified two groups, and allocated to intervention within every group (Figure 1).
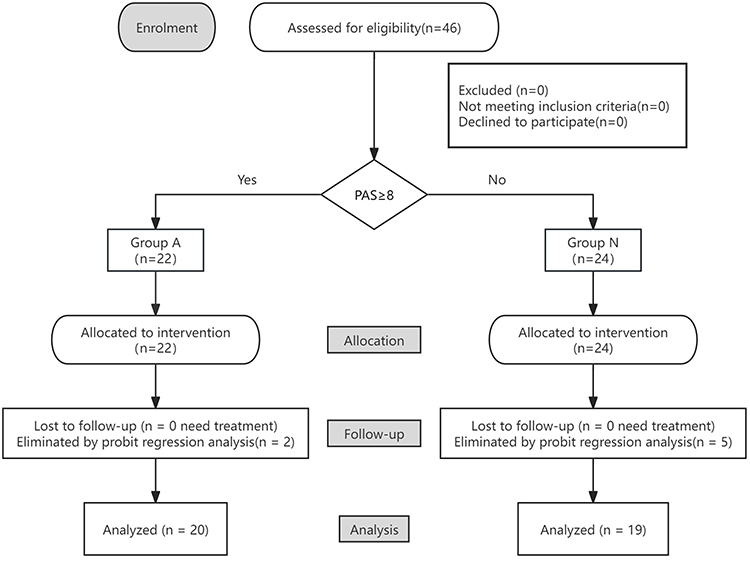 |
Figure 1 Flow diagram showing the inclusion of the participants. |
Analysis of the general characteristics and abortion-related factors revealed no significant differences between the groups (Table 1). However, the PAS-7 scores indicated a statistically significant difference between the two groups.
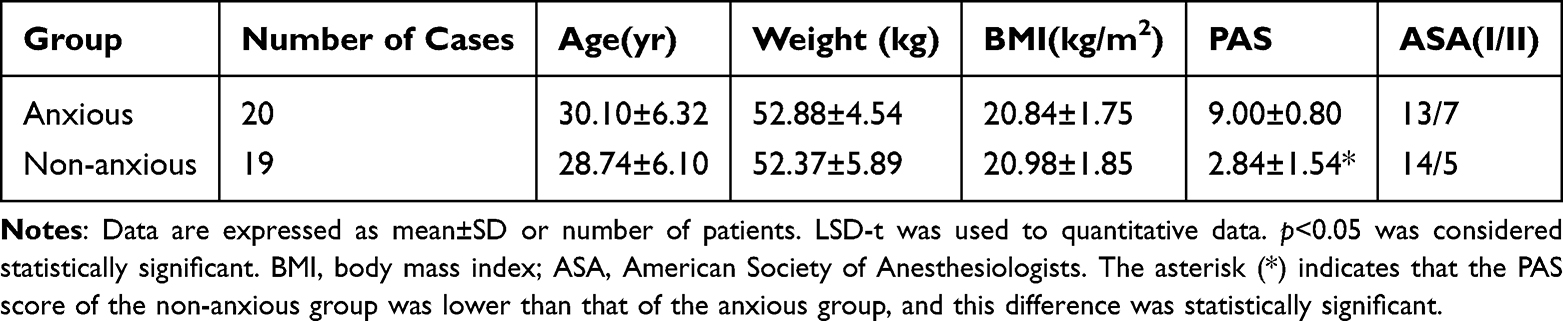 |
Table 1 Overview of the General Characteristics of Patients in the Two Group |
PAS-7<8: The probit model fitted according to probit probability unit regression analysis was as follows: probit (p) = −22.47 + 11.46 × dose, the regression model showed a linear trend, Pearson’s goodness-of-fit test χ2 = 0.001 (p = 1.000), according to the Probit probability and dose confidence limit table: ED50 1.96 mg/kg (95% CI 1.87–2.05 mg/kg), ED95 2.10 mg/kg (95% CI 2.03–2.39 mg/kg).The orders in Dixon’s up-and-down method of the non-anxious group is exhibited in Figure 2. The dose-effect curve of propofol inhibiting visceral pain response of the non-anxious group during abortion when oxycodone is combined is showed in Figure 3.
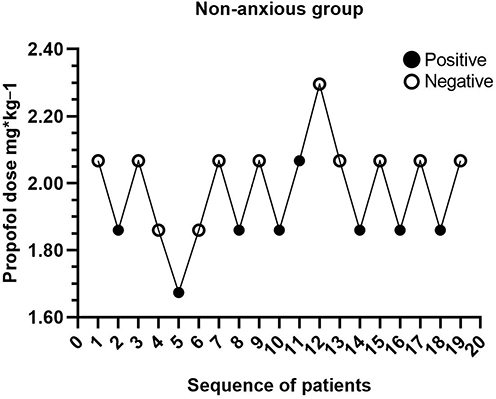 |
Figure 2 Dixon’s up-and-down method plots for the non-anxious group. |
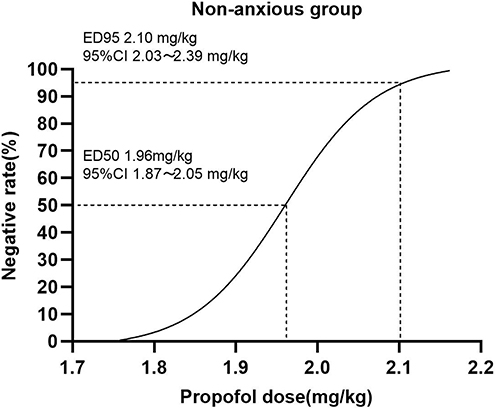 |
Figure 3 The dose-effect curve of propofol inhibiting visceral pain response during abortion in the non-anxious group when oxycodone is combined. |
PAS≥8: The probit model fitted according to probit probability unit regression analysis was as follows: probit (p) = −22.47 + 9.27 × dose, the regression model showed a linear trend, Pearson’s goodness-of-fit test χ2 = 0.001 (p = 1.000), according to the probit probability and dose confidence limit table: ED 50 2.42 mg/kg (95% CI 2.30 ~ 2.53 mg/kg), ED 95 2.60 mg/kg (95% CI 2.50 ~ 2.95 mg/kg). The orders in Dixon’s up-and-down method of the anxiety group is exhibited in Figure 4. The dose-effect curve of propofol inhibiting visceral pain response of the anxious group during abortion when oxycodone is combined is showed in Figure 5.
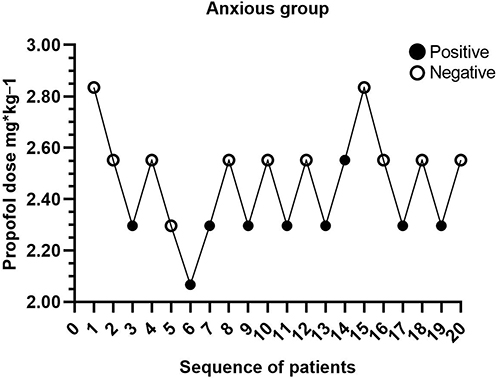 |
Figure 4 Dixon’s up-and-down method plots for the anxious group. |
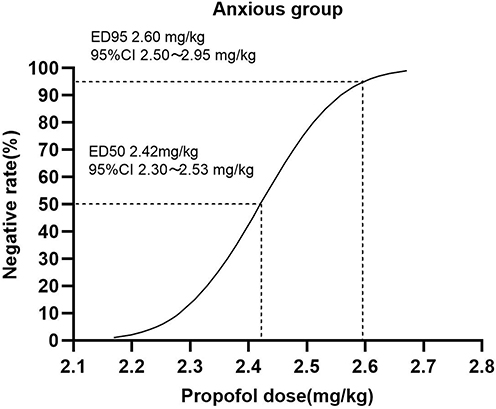 |
Figure 5 The dose-effect curve of propofol inhibiting visceral pain response during abortion in the anxious group when oxycodone is combined. |
Hemodynamic indicators, VAS and Ramsay score of patients are expressed as mean±SD. A significant decline in SBP (mean decline of ~10 mmHg) and DBP (mean decline of ~6 mmHg) was observed at T2. There was no significant difference in postoperative analgesia (VAS) and sedation (Ramsay score) between the two groups (Table 2).
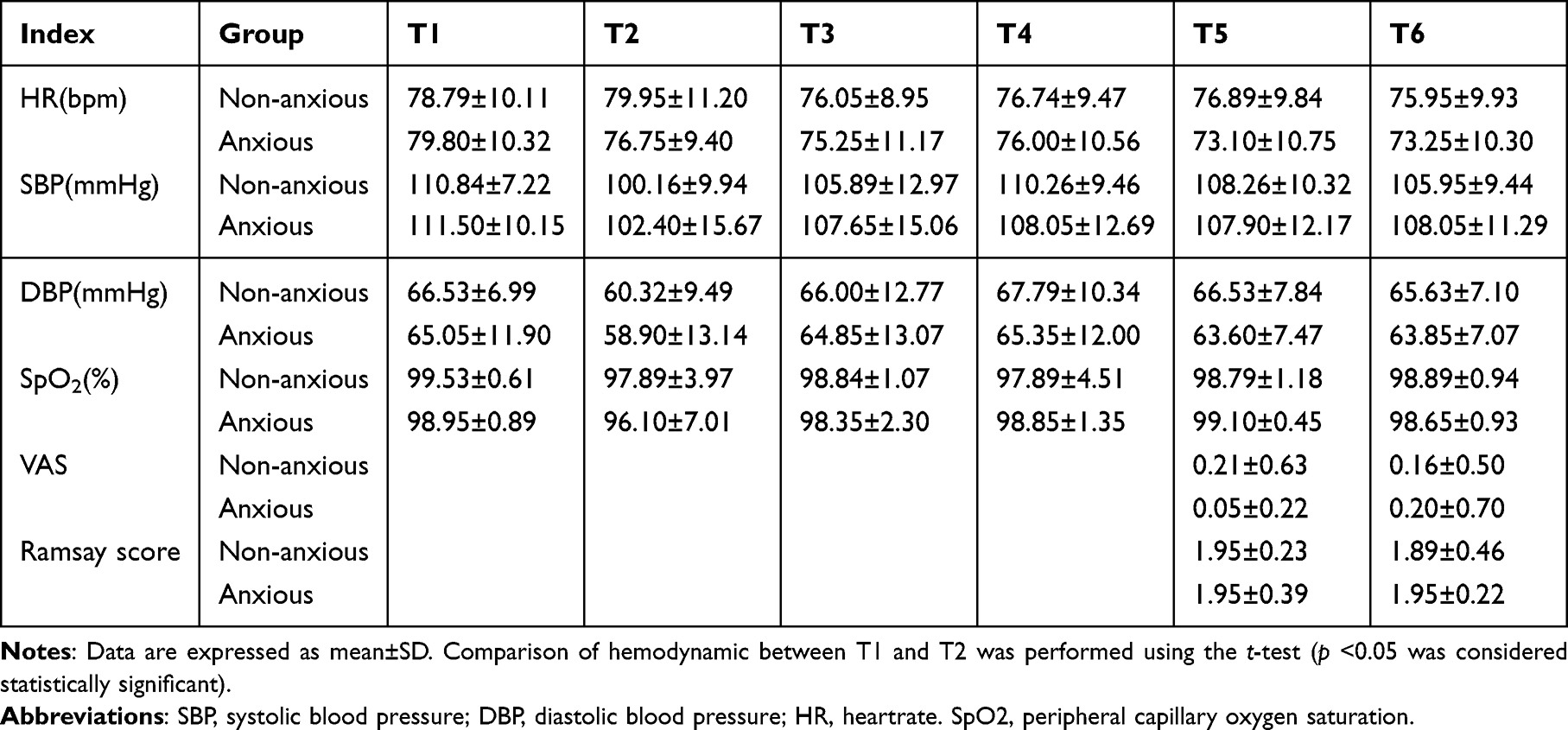 |
Table 2 Hemodynamic Indicators, VAS and Ramsay Score of Patients From Two Groups |
As for adverse events, no significant difference was observed in incidence rate of overall adverse events between the anxiety and non-anxiety groups (Table 3).
 |
Table 3 Comparison of Adverse Events Between the Two Groups[n(%)] |
Discussion
Anxiety is a common mental health issue that greatly affects the quality of life and daily functioning of adults around the world.26,27 A recent cross-sectional, multi-center study revealed substantial variation in the prevalence of preoperative anxiety among Chinese surgical patients across different healthcare institutions. Using the internationally accepted APAIS scale, the prevalence was found to be 7.8%, whereas the newly developed PAS-7 scale, designed specifically for Chinese surgical patients, reported a higher prevalence of 15.8%.28 This discrepancy may be attributed to cultural factors. Chinese patients tend to have reservations about negative psychological feelings and are more likely to express anxiety-related physical discomfort. Therefore, routine preoperative screening for anxiety using tools like the PAS-7 is recommended to guide initial propofol dosing. The PAS-7 scale, which incorporates somatic anxiety into its assessment, was chosen for this experiment to better capture the unique characteristics of anxiety expression in Chinese patients.29 By utilizing this culturally appropriate tool, we aimed to ensure a more accurate assessment of preoperative anxiety in our study population.
Studies have shown that anxiety and interactional relationship between visceral pain, anxiety can lead to the deterioration of the visceral pain, visceral pain itself can also aggravate anxiety.30–34 Previous research on contractions pain suppression of stream of people surgery, propofol is often choose anesthetic sedative drugs. Propofol on GABA receptor, stabilize the neurons, inhibition of emotional stress reaction.35,36 Recently, Le Yu37 et al made a new discovery about the anti-anxiety mechanism of propofol: propofol maintained synaptic E-I balance by acting on GABAAβ3, inhibited the excessive activation of PVNCRH neurons, and thus relieved pain-related anxiety disorders. In this study, patients undergoing abortion surgery were categorized into anxious and non-anxious groups based on their PAS-7 scores. The median effective dose (ED50) and 95% effective dose (ED95) of propofol for alleviating visceral pain were calculated for both groups. The results showed that the required doses of propofol were significantly higher in the anxious group. This increased requirement in anxious patients may be linked to a heightened central nervous system arousal and a reduced pain threshold, necessitating a higher dose to achieve the same level of sedation and analgesia, rather than a difference in drug metabolism. These findings have important implications for clinical anesthesia practice, as they emphasize the need to assess preoperative anxiety and adjust anesthetic doses accordingly to achieve effective pain control and reduce the risk of postoperative complications. By acknowledging the relationship between anxiety and visceral pain, as well as its influence on anesthetic requirements, anesthesiologists can better adapt their management strategies to meet the individual needs of patients.
Oxycodone was utilized as a treatment for visceral pain in both the anxious and non-anxious groups due to its unique mechanism of action. Specifically, oxycodone acts on both μ and κ opioid receptors, providing rapid onset of analgesia with minimal side effects and no ceiling effect on pain relief.38 κ receptors are mainly distributed in the smooth muscle, so the visceral analgesic effect of oxycodone induced by uterine smooth muscle contraction is more significant. Choose oxycodone analgesia, can meet the needs of stream of people surgery anesthesia and quick outcome. In the first stage of Labor, pain is mainly caused by uterine contractions. Zhong H Y39 and others randomized controlled trial showed that epidural oxycodone suitable for labor analgesia. Additionally, oxycodone has been shown to reduce postoperative visceral pain in patients undergoing laparoscopic gastrointestinal surgeries when used as part of a multimodal analgesia regimen,40 further underscoring its efficacy in managing visceral pain.
Previous studies have highlighted the benefits of using oxycodone in combination with propofol for maintaining hemodynamic stability and minimizing adverse reactions during surgical procedures. For instance, one study found that a combination of oxycodone 0.05 mg/kg and propofol effectively maintained hemodynamic stability in patients undergoing painless stomach procedures.41 Similarly, another study demonstrated that a dose of 0.08 mg/kg oxycodone hydrochloride could be safely and effectively used during negative pressure suction, significantly reducing postoperative uterine contraction pain in dysmenorrhea patients.42 In the present study, a combination of oxycodone 0.10 mg/kg and propofol was used, and no significant hemodynamic fluctuations were observed. While a statistically significant drop in blood pressure was observed at induction (T2), a common effect of propofol, these changes were transient and clinically manageable in both groups, with no significant differences in the magnitude of change between them. Additionally, there was no significant difference in the incidence of postoperative visceral pain between anxious and non-anxious patients. While animal studies have suggested that oxycodone may have anxiolytic effects, with stronger effects observed in male rats compared to females,43 the long-term impact of oxycodone on anxiety and other mental health outcomes remains unclear and requires further investigation. Therefore, while oxycodone may provide short-term relief from anxiety, anesthesiologists should be mindful of its potential long-term effects and consider individual patient factors when selecting anesthetic agents.
This study offers important insights into the use of propofol combined with oxycodone for managing anxiety and visceral pain during gynecological abortion surgeries. However, it has several limitations that must be acknowledged. First, the lack of blinding for the anesthesiologist administering the drugs and assessing the primary outcome introduces a potential for observer bias, as their knowledge of the patient’s anxiety group could consciously or unconsciously influence the assessment of “significant movement.” Second, the single-center design and relatively small sample size, while appropriate for an initial dose-finding study using Dixon’s method, limit the generalizability of our findings to broader populations and different clinical settings. Third, and relatedly, the study was not powered to detect differences in rare adverse events; therefore, the conclusion that the safety profile is comparable between groups should be interpreted with caution, as we may have lacked the statistical power to identify true differences. Finally, the primary endpoint, though clinically relevant, was inherently subjective. Despite being assessed by a single experienced anesthesiologist to ensure consistency, the definition of “significant movement” lacks objective quantification and is susceptible to interpretation.
Conclusion
This dose-finding study determined that the combination of 0.10 mg/kg oxycodone and propofol provided effective suppression of visceral pain responses during artificial abortion. Anxious patients required significantly higher propofol doses (ED50 2.42 mg/kg vs 1.96 mg/kg). The similar postoperative pain, sedation scores, and adverse event profiles between groups suggest the regimen’s safety within our cohort. These findings, from a single-center study, underscore the importance of preoperative anxiety assessment for individualized dosing. Future large-scale, multicenter studies are warranted to validate these dosing guidelines.
Abbreviations
Group A, anxious group; Group N, non-anxious group; ED50, the median effective dose; ED95, the 95% effective dose; 95% CI, 95% confidence intervals; ASA, American Society of Anesthesiologists; PAS-7, the perioperative anxiety scale-7; PACU, post anesthesia care unit; SBP, systolic blood pressure; DBP, diastolic blood pressure; MAP, mean arterial pressure; HR, heart rate; SpO2, peripheral capillary oxygen saturation; VAS, visual analog scale; PONV, postoperative nausea and vomiting; SD, standard deviations; LSD-t, the least significant difference t-test; BMI, body mass index; STAI, the state-trait anxiety inventory; VAS, anxiety visual analog scale; SAS, self-rating anxiety scale; SAS, self-rating anxiety scale.
Data Sharing Statement
All data generated in this study are available from the Corresponding author upon reasonable quest.
Ethics Approval and Consent to Participate
The study was approved by the Medical Ethics Committee of the People’s Hospital of Qiannan (Ethical approval number: QNZY-QNYZKYRC-23-0801) and registered at https://www.chictr.org.cn/ (registration number: ChiCTR2300076169). Written informed consent was obtained from all participants prior to the commencement of the study. All clinical investigations should be conducted according to the principles.
Acknowledgments
Thank you to the obstetrics and gynecology doctors of Qiannan People ‘s Hospital for their support and cooperation in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was financially supported by:1. Scientific Research Fund of Qiannan Medical College For Nationalities (Grant number Qnyz2023036); 2. Project supported by the Science and Technology Fund of Guizhou Provincial Health Commission in 2025 (Project No.: gzwkj2025 - 390); 3. Project supported by the Science and Technology Fund of Guizhou Provincial Health Commission in 2025 (Project No.: gzwkj2025 - 081).
Disclosure
The authors declare that there are no conflicts of interest.
References
1. Huang SN, Yang B, Ma L, et al. Bulleyaconitine A Exerts Antianxiety and Antivisceral Hypersensitivity Effects. Front Pharmacol. 2020;11:328. doi:10.3389/fphar.2020.00328
2. Huang SN, Wei J, Huang LT, Ju PJ, Wang YX, Wang Y-X. Bulleyaconitine A Inhibits Visceral Nociception and Spinal Synaptic Plasticity through Stimulation of Microglial Release of Dynorphin A. Neural Plast. 2020;2020:1484087. doi:10.1155/2020/1484087
3. Daes J, Morrell DJ, Hanssen A, et al. Paragastric Autonomic Neural Blockade to Prevent Early Visceral Pain and Associated Symptoms After Laparoscopic Sleeve Gastrectomy: a Randomized Clinical Trial. Obes Surg. 2022;32(11):3551–3560. doi:10.1007/s11695-022-06257-9
4. van Thiel I, Botschuijver S, de Jonge WJ, Seppen J. Painful interactions: microbial compounds and visceral pain. Bba-Mol Basis Dis. 2020;1866(1):165534. doi:10.1016/j.bbadis.2019.165534
5. Qian J, Sun S, Wang M, Yu X. Nonpharmacological pain management interventions in medical and surgical abortion: a scoping review. Int J Nurs Pract. 2023;29(2):e13056. doi:10.1111/ijn.13056
6. Coakley K, Meurice ME, Chang JJ, Lovio M, Harken T. Overnight pain and opioid use after osmotic cervical dilator placement for second trimester dilation and evacuation. Eur J Contracep Repr. 2022;27(2):148–152.
7. Pacheco-Carroza EA. Visceral pain, mechanisms, and implications in musculoskeletal clinical practice. Med Hypotheses. 2021;153:110624. doi:10.1016/j.mehy.2021.110624
8. Li S, Wang Y, Zhang Y, et al. Effect of ultrasound-guided transversus abdominis plane block in reducing atelectasis after laparoscopic surgery in children: a randomized clinical trial. Heliyon. 2024;10(4):e26594. doi:10.1016/j.heliyon.2024.e26594
9. Reynolds CA, Minic Z. Minic Z: chronic Pain-Associated Cardiovascular Disease: the Role of Sympathetic Nerve Activity. Int J Mol Sci. 2023;24(6):5378. doi:10.3390/ijms24065378
10. Liu SM, Shaw KA. Pain management in outpatient surgical abortion. Curr Opin Obstet Gyn. 2021;33(6):440–444. doi:10.1097/GCO.0000000000000754
11. Lamvu G, Carrillo J, Ouyang C, Rapkin A. Chronic Pelvic Pain in Women: a Review. J Am Med Assoc. 2021;325(23):2381–2391. doi:10.1001/jama.2021.2631
12. Yalcin BP, Turan G, Topbas SN, Cakmak K, Kaya C. Comparison of Depression and Anxiety Scores in Multi/Nulliparous Women who have Undergone Dilatation and Curettage. Acta Biomed. 2022;93(2):e2022038. doi:10.23750/abm.v93i2.11089
13. Quenby S, Gallos ID, Dhillon-Smith RK, et al. Miscarriage matters: the epidemiological, physical, psychological, and economic costs of early pregnancy loss. Lancet. 2021;397(10285):1658–1667. doi:10.1016/S0140-6736(21)00682-6
14. Salameh E, Meleine M, Gourcerol G, et al. Chronic colitis-induced visceral pain is associated with increased anxiety during quiescent phase. Am J Physiol Gastr Liver Physiol. 2019;316(6):G692–G700.
15. Clark JR, Yeowell G, Goodwin PC. Trait anxiety and sensory processing profile characteristics in patients with non-specific chronic low back pain and central sensitisation - A pilot observational study. J Bodyw Mov Ther. 2018;22(4):909–916. doi:10.1016/j.jbmt.2017.11.007
16. Li RY, Lin M, Jiang HY, et al. Impact of Anxiety or Depression Symptoms on Propofol Requirements for Sedation in Females: a Prospective Cohort Study. J Clin Pharmacol. 2020;60(10):1376–1384. doi:10.1002/jcph.1631
17. Yilmaz IF, Yilmaz CY, Daskaya H, Kocoglu H. The Effect of Preoperative Anxiety and Pain Sensitivity on Preoperative Hemodynamics, Propofol Consumption, and Postoperative Recovery and Pain in Endoscopic Ultrasonography. Pain Ther. 2021;10(2):1283–1293. doi:10.1007/s40122-021-00292-7
18. Pace L, Howard M, Makar E, Lee J. The association of patient age, race, and demographic features on reported pain and sedation dosing during procedural abortion: a retrospective cohort study. Contraception. 2023;123:110037. doi:10.1016/j.contraception.2023.110037
19. Lao W-L, Song Q-L, Jiang Z-M, Chen W-D, Zheng X-H, Chen Z-H. The Effect of Oxycodone on Post-operative Pain and Inflammatory Cytokine Release in Elderly Patients Undergoing Laparoscopic Gastrectomy. Front Med-Lausanne. 2021;8:700025. doi:10.3389/fmed.2021.700025
20. Li Y, Dou Z, Yang L, Wang Q, Ni J, Ma J. Oxycodone versus other opioid analgesics after laparoscopic surgery: a meta-analysis. Eur J Med Res. 2021;26(1):4. doi:10.1186/s40001-020-00463-w
21. Kong C, Miao F, Wu Y, Wang T. Oxycodone suppresses the apoptosis of hippocampal neurons induced by oxygen-glucose deprivation/recovery through caspase-dependent and caspase-independent pathways via kappa- and delta-opioid receptors in rats. Brain Res. 2019;1721:146319. doi:10.1016/j.brainres.2019.146319
22. Garcia MM, Goicoechea C, Avellanal M, Traseira S, Martin MI, Sanchez-Robles EM. Comparison of the antinociceptive profiles of morphine and oxycodone in two models of inflammatory and osteoarthritic pain in rat. Eur J Pharmacol. 2019;854:109–118. doi:10.1016/j.ejphar.2019.04.011
23. Cajanus K, Neuvonen M, Koskela O, et al. Analgesic Plasma Concentrations of Oxycodone After Surgery for Breast Cancer-Which Factors Matter? Clin Pharmacol Ther. 2018;103(4):653–662. doi:10.1002/cpt.771
24. Zhu X, He X, Fan B, et al. Effect of Propofol Intravenous Anesthesia Combined with Press-Needle Therapy on Analgesic Effect during Painless Abortion. Comput Math Method M. 2022;2022:6543211.
25. Wen J, Liu C, Ding X, et al. Efficacy and safety of ciprofol (HSK3486) for procedural sedation and anesthesia induction in surgical patients: a systematic review and meta-analysis. Heliyon. 2023;9(12):e22634. doi:10.1016/j.heliyon.2023.e22634
26. Friedrich S, Reis S, Meybohm P, Kranke P. Preoperative anxiety. Curr Opin Anesthesio. 2022;35(6):674–678. doi:10.1097/ACO.0000000000001186
27. Juruena MF, Eror F, Cleare AJ, Young AH. The Role of Early Life Stress in HPA Axis and Anxiety. Adv Exp Med Biol. 2020;1191:141–153.
28. Yu J, Zhang Y, Yu T, et al. Preoperative Anxiety in Chinese Adult Patients Undergoing Elective Surgeries: a Multicenter Cross-Sectional Study. World J Surg. 2022;46(12):2927–2938. doi:10.1007/s00268-022-06720-9
29. Zhang C, Liu X, Hu T, et al. Development and psychometric validity of the perioperative anxiety scale-7 (PAS-7). Bmc Psychiatry. 2021;21(1):358. doi:10.1186/s12888-021-03365-1
30. Greenwood-Van MB, Johnson AC. Stress-Induced Chronic Visceral Pain of Gastrointestinal Origin. Front Syst Neurosci. 2017;11:86. doi:10.3389/fnsys.2017.00086
31. Taheri AA, Reisi S, Jafari M, et al. Associations between the perception of dental pain and pain anxiety, mental pain, and dental anxiety in Iranian sample. Int J Psychiat Med. 2024;59(1):34–49. doi:10.1177/00912174231180855
32. Cimpean A, David D. The mechanisms of pain tolerance and pain-related anxiety in acute pain. Health Psychol Open. 2019;6(2):276565175. doi:10.1177/2055102919865161
33. Smit T, Mayorga NA, Rogers AH, et al. Indirect Effects of Negative Mood on Opioid Misuse and Dependence via Anxiety Sensitivity Subfacets: evidence from Adults Reporting Chronic Pain. Subst Use Misuse. 2023;58(4):570–577. doi:10.1080/10826084.2023.2177969
34. Rogers AH, Garey L, Bakhshaie J, Viana AG, Ditre JW, Zvolensky MJ. Anxiety, Depression, and Opioid Misuse Among Adults With Chronic Pain: the Role of Anxiety Sensitivity. Clin J Pain. 2020;36(11):862–867. doi:10.1097/AJP.0000000000000870
35. Parikh A, Krogman W, Walker J. The impact of volatile anesthetics and propofol on phosphatidylinositol 4,5-bisphosphate signaling. Arch Biochem Biophys. 2024;757:110045. doi:10.1016/j.abb.2024.110045
36. Morena M, Berardi A, Valeri D, et al. Effects of ketamine, dexmedetomidine and propofol anesthesia on emotional memory consolidation in rats: consequences for the development of post-traumatic stress disorder. Behav Brain Res. 2017;329:215–220. doi:10.1016/j.bbr.2017.04.048
37. Yu L, Zhu X, Peng K, et al. Propofol Alleviates Anxiety-Like Behaviors Associated with Pain by Inhibiting the Hyperactivity of PVN(CRH) Neurons via GABA(A) Receptor beta3 Subunits. Adv Sci. 2024;11(28):e2309059. doi:10.1002/advs.202309059
38. Umukoro NN, Aruldhas BW, Rossos R, Pawale D, Renschler JS, Sadhasivam S. Pharmacogenomics of oxycodone: a narrative literature review. Pharmacogenomics. 2021;22(5):275–290. doi:10.2217/pgs-2020-0143
39. Zhong HY, Yang ZY, Zhang W, Cai S. Effects of Adding Oxycodone to Ropivacaine on Labor Analgesia: a Randomized Controlled Trial. Clin J Pain. 2020;36(2):96–100. doi:10.1097/AJP.0000000000000777
40. Zhang J, Zhang Y, Yan H, Zhang K. Influence of Preemptive Analgesia with Oxycodone Hydrochloride on Stress Hormone Level of Geriatric Patients undergoing Gastrointestinal Surgery. J Coll Physici. 2020;30(5):476–479.
41. Li YP, Zhou Y. Differential dosing of oxycodone in combination with propofol in diagnostic painless gastroscopy in elderly patients: a prospective randomized controlled trial. Medicine. 2022;101(51):e32427. doi:10.1097/MD.0000000000032427
42. Wang YN, Xu MJ, Feng Y, et al. The efficacy and safety of oxycodone in treating the uterine contraction pain after negative pressure aspiration: a randomized, compared, multicenter clinical study. Medicine. 2022;101(33):e30048. doi:10.1097/MD.0000000000030048
43. Bruijnzeel AW, Behnood-Rod A, Malphurs W, et al. Oxycodone decreases anxiety-like behavior in the elevated plus-maze test in male and female rats. Behav Pharmacol. 2022;33(6):418–426. doi:10.1097/FBP.0000000000000690
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.