Back to Journals » OncoTargets and Therapy » Volume 13
Optimal Management of Upper Tract Urothelial Carcinoma: Current Perspectives
Authors Leow JJ, Liu Z, Tan TW ![]() , Lee YM, Yeo EK, Chong YL
, Lee YM, Yeo EK, Chong YL
Received 30 July 2019
Accepted for publication 12 December 2019
Published 6 January 2020 Volume 2020:13 Pages 1—15
DOI https://doi.org/10.2147/OTT.S225301
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Nicola Silvestris
Jeffrey J Leow,1,2,* Zhenbang Liu,1–3,* Teck Wei Tan,1,2 Yee Mun Lee,1,2 Eu Kiang Yeo,1,2 Yew-Lam Chong1,2
1Department of Urology, Tan Tock Seng Hospital, Singapore; 2Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore; 3Department of Surgery, Woodlands Health Campus, Singapore
*These authors contributed equally to this work
Correspondence: Yew-Lam Chong
Department of Urology, Tan Tock Seng Hospital, Singapore
Tel +65 6357 7678/7808
Fax +65 6357 3198
Email [email protected]
Introduction: Upper tract urothelial carcinoma (UTUC) is a relatively uncommon urologic malignancy for which there has not been significant improvement in survival over the past few decades, highlighting the need for optimal multi-modality management.
Methods: A non-systematic review of the latest literature was performed to include relevant articles up to June 2019. It summarizes the epidemiologic risk factors associated with UTUC, including smoking, carcinogenic aromatic amines, arsenic, aristolochic acid, and Lynch syndrome. Molecular pathways underlying UTUC and potential druggable targets are outlined.
Results: Surgical management for UTUC includes kidney-sparing surgery (KSS) for low-risk disease and radical nephroureterectomy (RNU) for high-risk disease. Endoscopic management of UTUC may include ureteroscopic or percutaneous resection. Topical instillation therapy post-KSS aims to reduce recurrence, progression and to treat carcinoma-in-situ; this may be achieved retrogradely (via ureteric catheterization), antegradely (via percutaneous nephrostomy) or via reflux through double-J stent. RNU, which may be performed via open, laparoscopic or robot-assisted approaches, is the gold standard treatment for high-risk UTUC. The distal cuff may be dealt with extravesical, transvesical or endoscopic techniques. Peri-operative chemotherapy and immunotherapy are increasingly utilized; level 1 evidence exists for adjuvant chemotherapy, but neoadjuvant chemotherapy is favored as kidney function is better prior to RNU. Immunotherapy is primarily reserved for metastatic UTUC but is currently being investigated in the perioperative setting.
Conclusion: The optimal management of UTUC includes a firm understanding of the epidemiological factors and molecular pathways. Surgical management includes KSS for low-risk disease and RNU for high-risk disease. Peri-operative immunotherapy and chemotherapy may be considered as evidence mounts.
Keywords: carcinoma, transitional cell, chemotherapy, upper tract urothelial carcinoma, immunotherapy, nephroureterectomy, ureteral neoplasms, ureteral neoplasms
Introduction
Urothelial carcinoma is the fourth most common solid malignancy.1 The majority (90–95%) of cases occur in the lower urinary tract (urinary bladder and urethra) and the rest in the upper urinary tract (renal calyces, renal pelvis, and ureter).2 Upper tract urothelial carcinomas (UTUC) are of the same histological type as lower tract urothelial carcinomas but they have been found to have various phenotypical and genotypical (genetic and epigenetic) differences, which have led clinicians to label them as disparate twins.3 Stage for stage, UTUC follows a different natural history from UCB (urinary carcinoma of the bladder) and often at point of diagnosis, UTUC demonstrates a higher incidence of local invasion at diagnosis.4 However, the management of lower tract urothelial carcinoma remains more extensively studied in the literature by far compared to UTUC, which therefore informs the optimal management strategies for UTUC more by inference than by direct evidence especially for systemic therapies;5 yet we know they should be really be considered “distinct entities in terms of management”.6
A retrospective review of the MD Anderson Cancer Center’s experience in the United States from 1986 to 2004 found that there had been no appreciable improvement in disease-specific survival of UTUC over two decades and called for a change in the treatment paradigm.7 With improving knowledge of the molecular tapestry of UTUC8,9 and with more options in the therapeutic arsenal, the future holds greater promise for the optimal management of UTUC. This review paper aims to focus on the epidemiological factors and molecular pathways for UTUC, optimizing surgical management in both low- and high-risk disease, role of perioperative chemotherapy in UTUC and the recent implementation of immune checkpoint therapy in the management of UTUC.
Methods
We performed a non-systematic review of the latest literature including relevant articles up to June 2019. We included only English articles available in the MEDLINE/Pubmed database. Search terms included “nephroureterectomy”, “upper tract urothelial carcinoma”, “chemotherapy”, “immunotherapy”, and associated search terms. Additionally, references of key articles were reviewed. Finally, abstracts from the past 5 years of the Annual Meeting of American Urological Association (AUA) and American Society of Clinical Oncology (ASCO) were searched online to include any relevant late-breaking abstracts which have not been fully published yet.
Epidemiological Factors
The estimated annual incidence in Western countries is about 2 per 100,000 inhabitants.2 UTUC is three times more common in men than women and has a peak incidence in the age 70–90 yr.1,10 In a Swedish series of 963 patients by Holmang et al, 1.6% of UTUC were bilateral and were associated with bladder cancer diagnosis either before or after UTUC diagnosis in 80% of the cases.11 Renal pelvis UTUCs are twice as common as those found in the ureter.12 In terms of staging, 60% of UTUCs are invasive (≥pT2) at diagnosis in contrast to the 15–25% for bladder cancers.13 About 7% of patients present with metastatic disease.14
Risk factors associated with UTUC are similar to urothelial bladder cancers such as cigarette smoking and various occupational exposures to carcinogenic aromatic amines including benzidine and beta-naphthalene.2,15 However, there are other risk factors specific to UTUC which the clinician should be aware of.
Arsenic
Unusually high incidences of upper urinary tract tumors have been reported in Blackfoot disease-endemic areas in the southwest coastal region of Taiwan, and the arsenic-contaminated water has been postulated to be the cause of this prevalence.16,17 This region has a 1:2 male-to-female ratio for UTUC in contrast to the male predominance found globally. This could be related to the higher exposure of women to arsenic fumes during cooking from the steam generated from boiling water and suggest both inhalation and ingestion risks.18
Balkan Endemic and Chinese Herb Nephropathy
Balkan endemic nephropathy and Chinese herb nephropathy are similar diseases related to UTUC.19 Balkan endemic nephropathy is found in people living in Balkan countries (Bulgaria, Croatia, Greece, Romania, and Serbia) and in this region, urothelial tumors account for almost 50% of all renal tumors.20 It is familial but not obviously inherited suggesting an environmental cause and it is believed to be due to dietary exposure to aristolochic acid (AA). AA is derived from Aristolochic plants (fangchi and clematis) and is a potent carcinogen which causes codon 139 of p53 gene to be mutated leading to UTUC. Aristolactam-DNA adducts are deposited in the renal cortex which may explain why AA-related nephropathy increases the incidence of UTUC and not bladder cancer. AA-related UTUC are more commonly low grade, multiple and bilateral compared to non-AA-related UTUC.21 In Taiwan, the incidence of UTUC is estimated to be 20–25% of all urothelial cancers, the highest worldwide and this has been attributed to the use of aristolochic plants.22 Chinese herb nephropathy causes a progressive renal fibrosis leading to UTUC. UTUC patients with prior AA exposure have been found to have poorer cancer-specific survival.23
Hereditary Nonpolyposis Colorectal Cancer (HNPCC, Lynch Syndrome)
Lynch syndrome or hereditary nonpolyposis colorectal cancer (HNPCC) is an autosomal dominant genetic mutation that impairs DNA mismatch repair that is associated with a high risk of colon cancer as well as other cancers such as endometrial, ovarian, gastric and also urothelial cancers especially that of the upper tract. According to Koornstra et al, patients with this condition have an estimated 22-fold increased relative risk of developing UTUC.24 This has led to experts and guidelines recommending that UTUC patients be screened with a short interview and patients identified as high risk for Lynch/HNPCC syndrome should undergo DNA sequencing for patient and family counseling.2
Molecular Pathways
The understanding of the molecular landscape of UTUC is sparse and often extrapolated from bladder urothelial cancer. However, there are distinct epidemiological and clinicopathological differences between the two suggesting different genetic phenotypes.6 Insight into these molecular pathways is important as it holds the promise for potential targets for therapy.
Recently, Sfakianos et al used a custom next-generation sequencing assay to identify somatic mutations and copy number alterations in 300 cancer-associated genes in tumor and germline DNA from patients with UTUC (n=83) and bladder urothelial cancer (n=102).8 The authors found that although the spectrum of genes mutated was similar, the frequency of alteration in several recurrently mutated genes such as FGFR3, HRAS, TP53, and RB1 was different. In high-grade UTUC, there were more frequent mutations in FGFR3 and HRAS and less TP53 and RB1 as compared to high-grade bladder urothelial cancer.
This molecular tapestry of UTUC was further characterized by Moss et al who carried out whole-exome sequencing on DNA and RNA from UTUC tumor specimens and protein analysis.9 They found 2784 somatic mutations with FGFR3 being the most commonly mutated gene (74%) in both low grade (92%) and high-grade UTUC (60%). High-grade UTUC as compared to low-grade UTUC had higher frequency of mutations in p53 and related interacting pathways with greater genomic instability, copy number alterations, and disruption of cell cycle and apoptotic pathways. The authors were also able to subdivide UTUC into 4 subtypes based on their RNA expression and their unique clinical presentations. Cluster 1 had no PIK3CA mutations, was more common in non-smokers, had higher frequency of high-grade non-muscle invasive tumors and high recurrence rates but favorable survival. Cluster 2 had 100% FGFR3 mutations, had more low-grade non-muscle invasive disease and no bladder recurrences. Cluster 3 also had 100% FGFR3 mutations; 71% PIK3CA and no TP53 mutations; and had high number of smokers and bladder recurrences. All the tumors were non-muscle invasive. Cluster 4 had KMT2D (62.5%), FGFR3 (50%) and TP53 (50%) mutations but no PIK3CA mutations; and had higher numbers of high grade, muscle invasive disease, smokers, carcinoma in situ and shorter survival. Interestingly, CTLA4, CD274 (PDL1) and PDCD1 (PD1) mRNA expression levels were all upregulated in the majority of Cluster 4 cases which represent the most aggressive clinical disease. These three immune checkpoint genes have recently been shown to be effective targets for immunotherapy for various cancers. These data support specific genes as rational therapeutic targets along with immune checkpoint therapies, especially for the most aggressive disease states.
Multiple agents targeting FGFR3 in urothelial cancer are already undergoing studies. Erdafinitib, a pan-FGFR tyrosine kinase inhibitor was shown in a Phase I dose-escalation study to have acceptable toxicity and a substantial signal of activity in patients with advanced urothelial cancer pre-treated with chemotherapy.25 An open-label Phase II trial (BLC2001) recruited 99 patients who had locally advanced and unresectable or metastatic urothelial carcinoma with FGFR alterations and had a history of disease progression during or after at least 1 course of chemotherapy/immunotherapy. This landmark trial, recently published in New England Journal of Medicine, revealed that after receiving a median of 5 cycles of erdafitinib, 40% of patients had an objective tumor response.26
Surgical Management - Kidney-Sparing Surgery for Low-Risk Disease
Traditionally, the gold standard of management of UTUC has been radical nephroureterectomy (RNU) and excision of the bladder cuff.2,27 Although the reported 5-year recurrence-free and cancer-specific survival for 1363 patients at multiple academic centers treated with RNU is reasonable (69% and 73%, respectively),7 RNU reduces the nephron mass by 50% or more depending on split renal function predisposing to chronic kidney disease (CKD) or even end-stage renal failure (ESRF) requiring dialysis. CKD/ESRF is associated with cardiovascular events and increased mortality28,29 and ESRF carries the increased financial burden of lifelong hemodialysis. These problems become more apparent as patients live longer and remaining nephrons shoulder the burden of chronic medical diseases such as hypertension, diabetes, and obesity.
With improvement in current endourological techniques and equipment, kidney-sparing surgery (KSS) allows preservation of the ipsilateral kidney without compromising oncological outcomes2 and survival after KSS has been shown to be similar to RNU in low-risk disease30 hence prompting current guidelines such as EAU2 and NCCN31 to recommend KSS for all low-risk disease and to be considered in select patients with serious CKD or solitary kidney. Low-risk disease is defined as having all of the following features: unifocal disease, tumor size less than 2 cm, low-grade cytology, low-grade URS biopsy and no invasive aspect on CT urogram. An important point to note when offering KSS is that the patient must be willing to undergo repeated and stringent surveillance follow-up including upper tract imaging, flexible cystoscopy, ureteroscopy, and urine cytology.
Endoscopic Management
The retrograde approach with ureteroscopy is more commonly used with new flexible scopes having good distal-tip deflection.32 However, the antegrade approach is still useful for tumors that are in the lower caliceal system that are inaccessible via flexible ureteroscopy. Moreover, antegrade approach allows for lower intrapelvic irrigation pressures due to the large working channel (up to 30Fr diameter) and ability to clear larger tumor volumes. However, this carries the risk of tumor seeding.33,34 With endoscopic management, a risk of understaging and undergrading remains. Novel optical technologies such as confocal laser endomicroscopy are promising adjuncts to provide real-time histologic characterization of UTUC lesions to identify potential candidates for kidney-sparing management.35,36
Segmental Ureteric Resection
Segmental ureteric resection with wide margins allows for ipsilateral kidney preservation and adequate pathological staging and lymphadenectomy can also be performed at the time of surgery.30 Guidelines recommend complete distal ureterectomy with ureteroneocystostomy for low-risk tumors in the distal ureter that cannot be removed completely with endoscopic management and for high-risk tumors when KSS is necessary (e.g., in a solitary kidney).2,31 Segmental resection of the mid and upper ureter is associated with higher failure rates than for the distal ureter.2 Partial pyelectomy or partial nephrectomy is extremely rarely indicated.2
Topical Instillation Therapies for Upper Urinary Tract
The role of topical instillation therapies in UTUC is to reduce risk of recurrence and progression after KSS and to treat carcinoma-in-situ (CIS). Similar to bladder cancer, common agents instilled include bacillus Calmette–Guerin (BCG) and mitomycin C (MMC). However, unlike its bladder counterpart, there is insufficient evidence for current EAU guidelines to make it a recommended treatment.2 The controversial areas are its modality of administration and its clinical effectiveness.
There are currently three methods of instillation of topical therapies into the upper urinary tract described in the literature – antegrade perfusion via a percutaneous nephrostomy tube,37 retrograde perfusion via an open-ended ureteric catheter38 or intravesical administration with vesicoureteral reflux via an indwelling ureteric stent.39 Antegrade perfusion is feasible but carries the potential risks of tumor seeding with the insertion of the nephrostomy tube and the possibility of missing calyxes if the therapy solution flows straight down into the ureter. Retrograde instillation with a ureteric catheter has been described but it has a risk of ureteric obstruction and pyelovenous influx during instillation.2 The main problem with vesicoureteral reflux via indwelling ureteric stent is that reflux is not guaranteed and the therapy solution often does not reach the renal pelvis. Indeed, Yossepowitch et al showed that only 59% of patients had reflux with ureteric stents,40 making this an unreliable method to instill topical agents into the upper urinary tract. There have been an ex-vivo and in-vivo animal comparison study to evaluate the staining intensity of the urinary collecting system at predefined points. In an ex-vivo indigo carmine porcine model study,41 the mean percent of kidney collecting system surface area stained for the nephrostomy tube, double-pigtail stent, and open-ended ureteral catheter groups was 65.2%, 66.2%, and 83.6%, respectively (p=0.002). The authors concluded that retrograde infusion with an open-ended ureteral catheter is the most efficient method. In an attempt to reduce potential confounding factors of a lack of natural ureteral peristalsis and continuous urine production, and the absence of intra-abdominal pressure found in this ex-vivo study,41 Liu et al investigated the staining intensity of the three methods in the collecting system at 6 pre-defined points (upper pole, mid pole, lower pole, renal pelvis, mid ureter, distal ureter) in an in-vivo porcine model.42 Retrograde approach via an open-ended ureteric catheter resulted in the highest mean fluorescence detected at all the 6 pre-defined points compared to the other 2 methods and this was significant on statistical analysis.42 More clinical studies are needed to determine which is the best method among the three.
Instillation of topical therapy to the upper urinary tract has better clinical response for treating CIS than adjuvant therapy for Ta/T1 disease post-KSS. In the large series by Giannarini et al, 42 renal units were treated with antegrade BCG perfusion of the upper urinary tract for curative intent for CIS and 22 renal units for adjuvant intent after ablation of Ta/T1 tumors.43 Recurrence in the CIS group was 40% and progression was 5% while in the Ta/T1 tumors group, recurrence was 59% and progression was 41%. Patients treated with curative intent for CIS significantly better progression-free survival (p<0.01). These results were also similar to a 2009 review by Rastinehad and Smith.44 However, a more recent study showed more promising intermediate-term data.45 Twenty-seven patients and 28 renal units with Ta/T1 UTUC that had complete endoscopic resection underwent induction MMC followed by a maintenance course with median follow-up of 19 months; the 3-year recurrence-free survival, progression-free, and RNU-free survival rates were 60%, 80%, and 76%, respectively. The future of instillation of topical therapy to the upper urinary tract may lie with novel agents to prolong the contact between drug and urothelium such as drug-eluting stents46 and thermosensitive polymers.47
Surgical Management - Surgery for High-Risk Disease
High-risk disease is defined as having any of the following: hydronephrosis, tumor size more than 2 cm, high-grade cytology, high-grade biopsy, multifocal disease, previous radical cystectomy for bladder cancer and variant histology.2 The gold standard for the treatment of high-risk disease is RNU with bladder cuff excision. This may be approached via an open, laparoscopic or robot-assisted laparoscopic approach. A recent review of 42 studies including 7554 patients who underwent open vs laparoscopic nephroureterectomy found no significant differences in oncologic outcomes in most series; however, 3 studies including the only randomized trial reported significantly poorer oncological outcomes among those who underwent laparoscopic RNU particularly in the subgroup of locally advanced (pT3/4) or high-grade UTUC patients.48 Robot-assisted RNU has been described, is increasingly utilized, and reportedly facilitates the bladder cuff excision and reconstruction.49–51
Distal Ureter and Bladder Cuff Excision
In a systemic review and meta-analysis of clinicopathologic factors associated with intravesical recurrence after RNU by Seisen et al,52 it was shown that there is significant risk of tumor recurrence in the distal ureter and its orifice and this area is difficult to survey with imaging or endoscopy. Hence, excision of the bladder cuff/intramural ureter is recommended at the time of RNU.
Three different methods have been used to excise the intramural ureter and a cuff of bladder around the ureteric orifice – extravesical, transvesical and endoscopic techniques.53 The extravesical approach involves dissecting the entire intramural ureter and with gentle traction on the ureter, the distal ureter is resected with its bladder cuff. The transvesical approach involves creating an anterior cystostomy in the bladder, confirming the contralateral ureteral orifice and circumferentially incising the ipsilateral ureteral orifice through the full thickness of the bladder. The anterior cystostomy is then closed in two layers. Endoscopic approach involves placing the patient in the lithotomy position and then using a resectoscope to incise a circumferential 10 mm cuff of bladder mucosa around the ureteral orifice. The incision is then deepened to perivesical fat and the intramural ureter detached. The specimen with the distal ureter cuff is removed en bloc during the RNU.
It has been shown in a large retrospective study of 2681 patients who underwent RNU with various methods for the bladder cuff excision in 24 international institutions to have no differences in cancer-specific or overall survival among the three methods but the endoscopic technique has a higher risk of intravesical recurrence.54 Current EAU guidelines do not recommend a method over the other but ureteral stripping (a dated procedure) is not advised.2
Lymph Node Dissection
The prognostic and potentially curative role of lymph node dissection (LND) at the time of radical cystectomy for bladder cancer has been extensively studied and supported by evidence.55–57 The anatomical templates have also been well established. However, LND at the time of RNU for UTUC has not gained the same oncological role. The lymphatic drainage from UTUC is variable and there is a lack of consensus on anatomical boundaries and selection criteria.58 A detailed description of primary lymph node metastasis sites was first reported by Kondo et al in 2007.59 In a retrospective multi-institutional study from three National Cancer Institute designated comprehensive cancer centers, the authors investigated the patterns of lymph node metastasis in 73 patients undergoing RNU with LND and proposed a dissection template according to the laterality and location of the tumor.60 In a systemic review of anatomical templates of LND for UTUC in 2017,61 the authors found that LND is not routinely performed at the time of RNU and there was a lot of variation in templates among surgeons from different institutions. That said, a LND typically included: the renal hilar, paracaval, precaval, and retrocaval nodes for right-sided tumors of the renal pelvis, upper and middle third of the ureter; while for left-sided tumors, the renal hilar, paraaortic and preaortic nodes. For tumors of the lower ureter, an extended pelvic LND was performed in most cases and the paracaval, paraaortic or presacral nodes in selected series. The therapeutic benefits of LND at the time of RNU still remain controversial but there is a growing body of evidence that shows staging and therapeutic benefits of LND at the time of RNU especially for muscle invasive or locally advanced disease.62,63 Current EAU guidelines recommend LND for invasive disease (pT2 and above).2
Single Post-Operative Bladder Instillation
Intravesical recurrences are common after RNU, with rates up to 22–47%,2 potentially because of implantation from the primary UTUC. In the ODMIT-C trial by O’Brien et al, 144 patients were randomized to receive mitomycin C (MMC) and 140 patients to receive standard care.64 These patients did not have any previous or concurrent history of bladder tumor and all underwent RNU for UTUC. In this trial, a single post-operative dose of MMC given at the time of catheter removal resulted in an absolute reduction in risk of intravesical recurrence in the first year by 11%; the relative reduction in risk was 40% and the number needed to treat to prevent one bladder tumor was 9. Another randomized controlled trial by Ito et al where a single intravesical dose of pirarubicin was given post-RNU within 48 hrs also showed a reduction in the risk for intravesical recurrence.65 A 2019 Cochrane review concluded that single-dose intravesical chemotherapy post-RNU reduces the risk of bladder cancer recurrence over time compared to no instillation (hazard ratio [HR]: 0.51, 95% confidence interval [CI]: 0.32 to 0.82, low-certainty evidence) and that after 12 months follow-up, this would result in 127 fewer bladder cancer recurrences (95% CI: 182 to 44 fewer bladder cancer recurrences) per 1000 participants.66 Current EAU guidelines give it a Grade B recommendation to offer post-operative bladder instillation of chemotherapy to lower the bladder recurrence rate.2
Based on the SWOG S0337 trial by Messing et al for low-grade non-muscle invasive bladder cancer, intravesical instillation of gemcitabine has been shown to significantly reduce recurrence. Given its cheaper price and favorable toxicity profile compared to mitomycin-C, it is also a possible option in the context of UTUC as mentioned in the latest NCCN guidelines.31
Clinical Nomograms and Predictive Tools
There have been numerous pre-operative and post-operative prognostic markers that have been shown to be associated with survival in UTUC. These are mostly based upon retrospective cohort studies. There have been efforts to use these collectively as predictive tools to aid in clinical management.
Preoperatively, there are 2 models that have been developed. The first nomogram is aimed to predict lymph node involvement in locally advanced UTUC, in order to guide clinicians on whether to perform a lymph node dissection or not. Three variables, namely tumor grade, architecture, and location of tumor were found to be independently associated with non-organ-confined disease. Together these 3 variables achieved 76.6% accuracy in prediction of non-organ confined UTUC.67 The second model combines imaging and ureteroscopy variables to help select non-organ-confined UTUC which is likely to benefit from RNU.68 Lastly, a multi-center database was used to develop a preoperative nomogram to help predict disease recurrence to better select patients who can most benefit from RNU.69
There exist 5 different postoperative nomograms. They can help to predict survival rates based on standard pathological features,70–74 which can be helpful for postoperative follow-up and counseling. Another prognostic nomogram based on 2926 patients which are based on 4 variables (namely age, pT stage, pN stage, and architecture) has good prognostic accuracy and risk stratification for patients with high-grade UTUC.75
Medical Management - Peri-Operative Systemic Therapy
Neoadjuvant Chemotherapy
Neoadjuvant chemotherapy for UTUC prior to definitive RNU makes sense because of the availability of 2 renal units during receipt of systemic therapy. Particularly in patients with chronic kidney disease, the surgical-induced loss of 1 kidney (via definitive surgical therapy with RNU) may render a patient ineligible for further systemic therapy. Attaining pathologic down-staging provides important prognostic information as well and has been shown in retrospective studies to accurately predict survival.76 Most studies evaluated platinum-based (cisplatin or carboplatin) regimens,77 although some believe that carboplatin-based regimens are inferior oncologically for UTUC and adds to the delay to surgical therapy. A 2014 meta-analysis revealed 2 trials.78 An update in 2019 revealed 4 retrospective cohort studies76,79–81 found that the pooled odds ratio for the effect of neoadjuvant chemotherapy on downstaging was 0.21 (95% CI, 0.09–0.60; p = 0.004), indicating that those who received neoadjuvant chemotherapy had a 4.76-fold higher probability of having pathologic N stage 0 than the control group which underwent surgery alone.82
Prospective data for neoadjuvant chemotherapy are scarce (Table 1).83 One using neoadjuvant gemcitabine/cisplatin was terminated due to poor accrual (Clinicaltrials.gov identifier: NCT01663285). Another phase 2 trial - the ECOG-ACRIN Research Group 8141 (Clinicaltrials.gov identifier: NCT02412670) - was presented at the Annual Meeting of American Urological Association (AUA) 2018 and showed a pathologic complete response rate of 14% (4/29).84,85 Finally, a phase 2 multi-center prospective single-arm trial (Clinicaltrials.gov identifier: NCT01261728) from Memorial Sloan Kettering Cancer Center was reported at the AUA meeting in May 2019;86 all 53 patients had high-risk UTUC (defined by 1) high-grade histology on biopsy, and/or 2) imaging (cT2-4a) and positive selective cytology) with no metastases, good kidney function (CrCl≥55 mL/min using CKD-EPI), and good performance status (Karnofsky performance status ≥70%). These patients received 12 weeks of neoadjuvant gemcitabine/cisplatin combination chemotherapy administered every 21 days x 4 cycles, prior to definitive surgery (RNU or distal ureterectomy). Notably, all patients underwent ipsilateral RPLND using standardized template as proposed by Matin et al.60 The primary endpoint of pathologic response rate, defined as ≤pT1N0, was 60% (n=32; 95% CI: 47–75%). Of the 21 patients (40%) who did not respond, 5 had pT2 disease, 9 pT3 disease, and 7 had pTany N+ disease. No patients progressed prior to surgery (0%), allaying concerns that “delay” to definitive surgical treatment may predispose to progression. It would not be unreasonable to presume that “progression” was simply determined by the final pathological and nodal staging after RNU; however, this is subject to pre-operative understaging bias known in UTUC.2,32 At a median follow-up for survivors at 2.6 years, the 2-year progression-free survival rate was 76% (95% CI: 64–90%) and 2-year overall survival rate was 89% (95% CI: 80–100%). This is remarkable considering the 2-year survival of high-grade UTUC of ~68% of patients who underwent surgery alone in another series.87
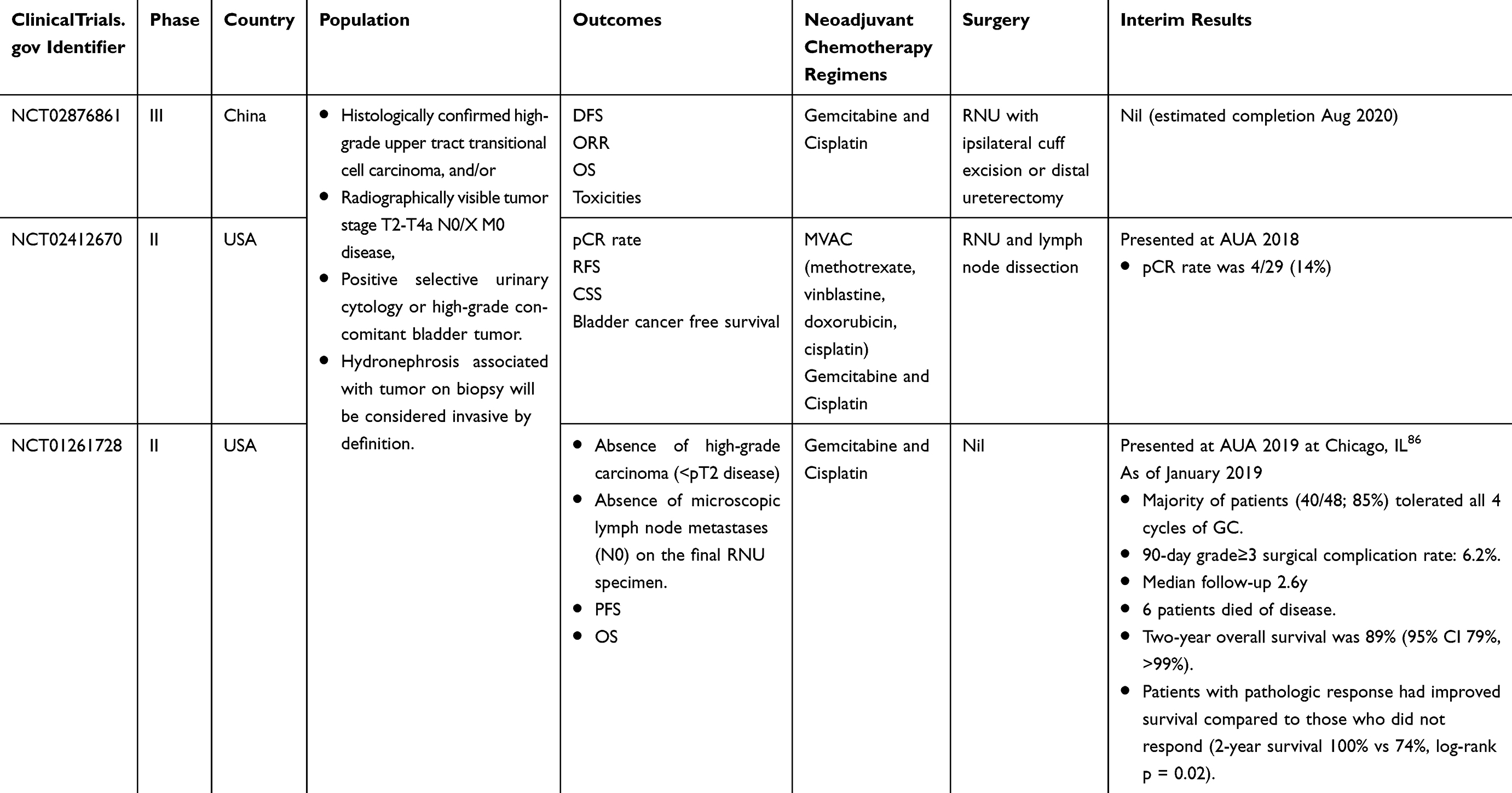 |
Table 1 Ongoing Phase II and III Trials Evaluating the Efficacy of Neoadjuvant Chemotherapy for Upper Tract Urothelial Carcinoma |
Peri-Operative Systemic Therapy – Adjuvant Chemotherapy
Adjuvant chemotherapy has the advantage of accurate pathological staging from the radical nephroureterectomy specimen, and hence preventing over-treatment in non-invasive disease. Leow et al performed meta-analysis of retrospective studies in 2014 which found an overall survival (HR 0.43, 95% CI 0.21–0.89, p=0.023) and disease-free survival benefit (HR 0.49, 95% CI 0.24–0.99, p=0.048) among patients who received adjuvant cisplatin-based chemotherapy compared to those who underwent RNU alone.78 Seisen et al followed on with a large observational study (n=3253) using the National Cancer Data Base in the United States, confirming an overall survival benefit for patients with pT3/T4 and/or pN+ UTUC in the real-world setting,88 with an HR 0.77 (95% CI 0.68–0.88, p<0.001).
Subsequently, results of the POUT trial, a multi-center RCT from the UK found that adjuvant chemotherapy after RNU provided a disease-free survival benefit of 51% (HR 0.49, 95% CI 0.30–0.79, p= 0.003) as compared to surgery alone, with a favorable toxicity profile.89 These results firmly etched and supported the role of adjuvant chemotherapy in the armament of a urologic oncologist in treating patients with high-risk and/or locally advanced UTUC. Publication in a peer-reviewed journal is pending and may be due to immature overall survival data at this time.
Looking to the future, several ongoing trials may shed light on how we can optimize peri-operative therapy for UTUC patients. The European Uro-Oncology Group is currently recruiting patients into their URANUS trial which aims to explore the feasibility of treatment options based on real-world data in various European countries. The URANUS investigators aim to determine the true proportion of patients that fit to receive complete cisplatin-based neoadjuvant or adjuvant chemotherapy, and the proportion and clinical outcome of patients with poor prognostic factors (PS and renal function) who receive only standard treatment of RNU. Secondary outcomes include DFS, OS, and CSS (ClinicalTrials.gov Identifier: NCT02969083).
Peri-Operative Systemic Therapy – Immunotherapy
Checkpoint inhibitors have been extensively investigated in recent years, in part due to favorable objective response rates compared to standard of care chemotherapy.90,91 Approved immunotherapeutic agents for urothelial carcinomas include the following 5 checkpoint inhibitors: pembrolizumab, nivolumab, atezolizumab, durvalumab, and avelumab.92 Table 2 outlines these 5 US FDA-approved PD1/PDL1 drugs for urothelial carcinoma, their mechanisms of actions, dose, and frequency.
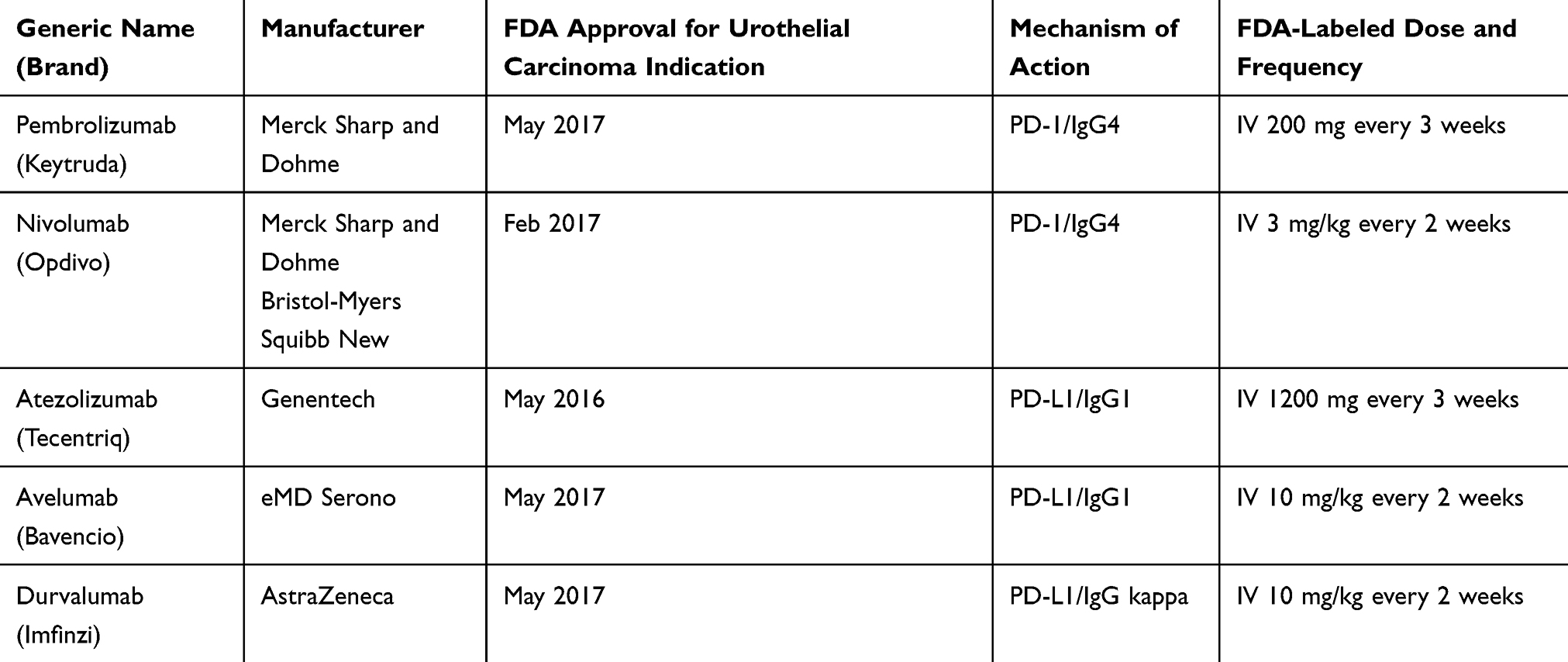 |
Table 2 US FDA Approved PD1/PDL1 Drugs for Urothelial Carcinoma |
Most of the patients included in these trials had urothelial carcinomas of bladder. Only Pembrolizumab93,94 and Atezolizumab95 have Phase III randomized data published (KEYNOTE 045 and IMVigor 211, respectively). Other checkpoint inhibitors have been evaluated with Phase II single-arm trials (Table 3) with favorable objective response rates and toxicities profile.96–99 Within KEYNOTE 045 and IMVigor 211, it is important to note that up to 27% of the included trial population were diagnosed with UTUCs; however, no further published data exist for this sub-group yet.93–95
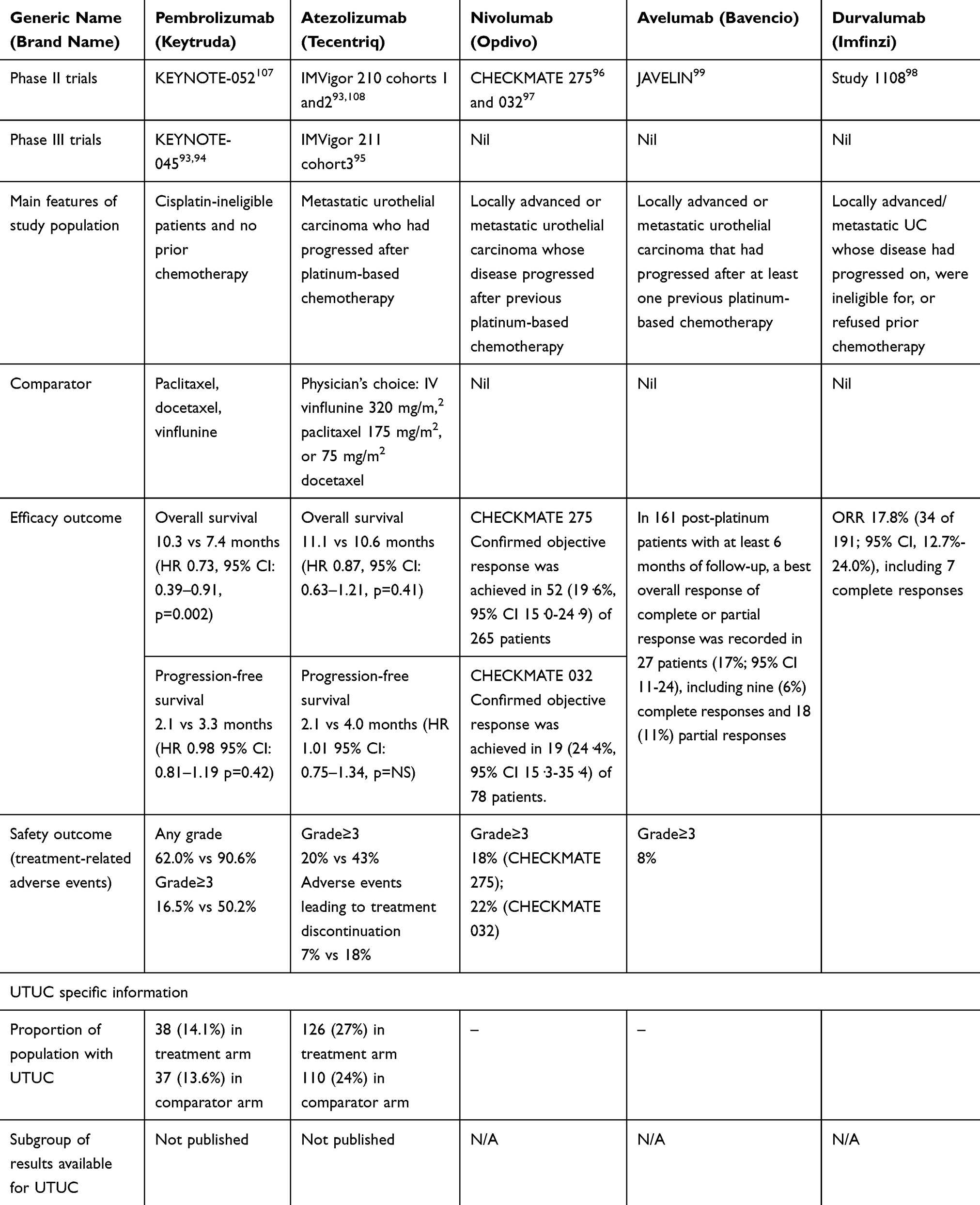 |
Table 3 Landmark Trials for US FDA Approved PD1/PDL1 Drugs for Urothelial Carcinoma |
As these immunotherapeutic agents are increasingly utilized, it is important to be familiar with associated toxicities associated. A systematic review and meta-analysis of treatment-related adverse events of PD-1 and PD-L1 inhibitors used in 125 clinical trials involving 20,128 patients100 found that the most common all-grade adverse events were fatigue (18.26%; 95% CI, 16.49–20.11%), pruritus (10.61%; 95% CI, 9.46–11.83%), and diarrhea (9.47%; 95% CI, 8.43–10.58%), while the most common grade 3 or higher adverse events were fatigue (0.89%; 95% CI, 0.69–1.14%), anemia (0.78%; 95% CI, 0.59–1.02%), and aspartate aminotransferase increase (0.75%; 95% CI, 0.56–0.99%)
Physicians are encouraged to refer to local or international clinical practice guidelines on how best to diagnose, treat and follow-up on toxicities arising from immunotherapy, such as this 2017 guideline from European Society of Medical Oncology.101
Systemic Therapy for Advanced or Metastatic UTUC
In terms of systemic treatments for advanced UTUC, virtually all of what is practiced had been derived from the experience in lower tract urothelial cancers. For metastatic UTUC, extrapolating from metastatic UCB, platinum-based combination chemotherapy, particularly cisplatin-based regimens, forms the mainstay of therapy traditionally. This extrapolation is further backed up by a recent retrospective analysis of prospectively collected data from 3 European Organization for the Research and Treatment of Cancer (EORTC) advanced urothelial carcinoma studies, including 30,924 (methotrexate, vinblastine, doxorubicin and cisplatin vs high dose methotrexate, vinblastine, doxorubicin, and cisplatin), 30,986 (methotrexate, carboplatin, and vinblastine vs gemcitabine and cisplatin in patients who were not candidates for cisplatin) and 30,987 (gemcitabine and cisplatin-paclitaxel vs gemcitabine and cisplatin in candidates for cisplatin). Moschini et al found that the primary tumor location (i.e., bladder vs upper tract) did not significantly affect progress-free or overall survival in patients with locally advanced or metastatic urothelial carcinoma treated with platinum-based combination chemotherapy.102
Ongoing randomized trials in 1st line metastatic urothelial carcinoma include IMvigor 130, DANUBE, KEYNOTE 361, CHECKMATE 901, and JAVELIN.99
Radiotherapy
Adjuvant radiotherapy after RNU had been explored to determine efficacy in improving disease-free survival in pT3 disease; however, 2 retrospective studies have been negative showing no benefit.103,104 A small study (n=31) showed that adding concurrent cisplatin with adjuvant radiotherapy improved overall and disease-free survival compared to adjuvant radiotherapy alone in pT3/4 and/or N+ UTUC; however, this was limited by small numbers and lack of multivariable analysis.105
In the metastatic setting, radiotherapy may be considered for palliative purposes to arrest bleeding that has not responded to conservative measures.
Surgery for Metastatic Disease
Indications for RNU for metastatic UTUC are limited to that of palliative intent, aimed to control symptomatic disease. Moreover, advances in palliative specialist care have diminished the role of RNU, since most pain associated with metastatic disease can be addressed in a multi-disciplinary approach with adequate medical therapy. Possible clinical scenarios necessitating surgical therapy may include (a) very locally advanced disease-causing bowel obstruction that has failed conservative management; (b) refractory bleeding which has failed to respond to conservative measures, super-selective angioembolization and palliative radiotherapy.
Observational studies have found that RNU may be associated with cancer-specific and overall survival in selected patients, particularly in those fit enough to receive cisplatin-based chemotherapy.106 Although the National Cancer Data Base cohort study was well conducted statistically, it is still subject to biases related to observational study design and should be considered hypothesis generating for a future randomized trial addressing this question.
Conclusion
The optimal management of UTUC includes a firm understanding of the epidemiological factors and molecular pathways. Surgical management includes kidney-sparing surgery for low-risk disease and radical nephroureterectomy for high-risk disease. Peri-operative immunotherapy and chemotherapy may be considered as evidence mounts.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69(1):7–34. doi:10.3322/caac.21551
2. Rouprêt M, Babjuk M, Burger M, et al. EAU guidelines on upper urinary tract urothelial carcinoma 2018. Eur Assoc Urol Guidelines. 2018 edition. Vol presented at the EAU Annual Congress Copenhagen 2018. Arnhem, The Netherlands: European Association of Urology Guidelines Office; 2018;73:111–22.
3. Green DA, Rink M, Xylinas E, et al. Urothelial carcinoma of the bladder and the upper tract: disparate twins. J Urol. 2013;189(4):1214–1221. doi:10.1016/j.juro.2012.05.079
4. Raman JD, Messer J, Sielatycki JA, Hollenbeak CS. Incidence and survival of patients with carcinoma of the ureter and renal pelvis in the USA, 1973–2005. BJU Int. 2011;107(7):1059–1064. doi:10.1111/bju.2011.107.issue-7
5. Campbell MT, Shah AY, Matin SF, Siefker-Radtke AO. Optimizing management of upper tract urothelial carcinoma. Urol Oncol. 2017;35(7):492–498. doi:10.1016/j.urolonc.2017.05.009
6. Leow JJ, Chong KT, Chang SL, Bellmunt J. Upper tract urothelial carcinoma: a different disease entity in terms of management. ESMO Open. 2016;1(6):e000126. doi:10.1136/esmoopen-2016-000126
7. Brown GA, Busby JE, Wood CG, et al. Nephroureterectomy for treating upper urinary tract transitional cell carcinoma: time to change the treatment paradigm? BJU Int. 2006;98(6):1176–1180. doi:10.1111/bju.2006.98.issue-6
8. Sfakianos JP, Cha EK, Iyer G, et al. Genomic characterization of upper tract urothelial carcinoma. Eur Urol. 2015;68(6):970–977. doi:10.1016/j.eururo.2015.07.039
9. Moss TJ, Qi Y, Xi L, et al. Comprehensive genomic characterization of upper tract urothelial carcinoma. Eur Urol. 2017;72(4):641–649. doi:10.1016/j.eururo.2017.05.048
10. Shariat SF, Favaretto RL, Gupta A, et al. Gender differences in radical nephroureterectomy for upper tract urothelial carcinoma. World J Urol. 2011;29(4):481–486. doi:10.1007/s00345-010-0594-7
11. Holmang S, Johansson SL. Synchronous bilateral ureteral and renal pelvic carcinomas: incidence, etiology, treatment and outcome. Cancer. 2004;101(4):741–747. doi:10.1002/cncr.v101:4
12. Favaretto RL, Shariat SF, Chade DC, et al. The effect of tumor location on prognosis in patients treated with radical nephroureterectomy at Memorial Sloan-Kettering Cancer Center. Eur Urol. 2010;58(4):574–580. doi:10.1016/j.eururo.2010.07.003
13. Margulis V, Shariat SF, Matin SF, et al. Outcomes of radical nephroureterectomy: a series from the upper tract urothelial carcinoma collaboration. Cancer. 2009;115(6):1224–1233. doi:10.1002/cncr.v115:6
14. Soria F, Shariat SF, Lerner SP, et al. Epidemiology, diagnosis, preoperative evaluation and prognostic assessment of upper-tract urothelial carcinoma (UTUC). World J Urol. 2017;35(3):379–387. doi:10.1007/s00345-016-1928-x
15. Colin P, Koenig P, Ouzzane A, et al. Environmental factors involved in carcinogenesis of urothelial cell carcinomas of the upper urinary tract. BJU Int. 2009;104(10):1436–1440. doi:10.1111/bju.2009.104.issue-10
16. Tan LB, Chen KT, Guo HR. Clinical and epidemiological features of patients with genitourinary tract tumour in a blackfoot disease endemic area of Taiwan. BJU Int. 2008;102(1):48–54. doi:10.1111/j.1464-410X.2008.07565.x
17. Yang MH, Chen KK, Yen CC, et al. Unusually high incidence of upper urinary tract urothelial carcinoma in Taiwan. Urology. 2002;59(5):681–687. doi:10.1016/S0090-4295(02)01529-7
18. Shao IH, Chang YH, Pang ST. Recent advances in upper tract urothelial carcinomas: from bench to clinics. Int j Urol. 2019;26(2):148–159. doi:10.1111/iju.13826
19. Gokmen MR, Cosyns JP, Arlt VM, et al. The epidemiology, diagnosis, and management of aristolochic acid nephropathy: a narrative review. Ann Intern Med. 2013;158(6):469–477. doi:10.7326/0003-4819-158-6-201303190-00006
20. Grollman AP, Shibutani S, Moriya M, et al. Aristolochic acid and the etiology of endemic (Balkan) nephropathy. Proc Natl Acad Sci U S A. 2007;104(29):12129–12134. doi:10.1073/pnas.0701248104
21. Dragicevic D, Djokic M, Pekmezovic T, et al. Survival of patients with transitional cell carcinoma of the ureter and renal pelvis in Balkan endemic nephropathy and non-endemic areas of Serbia. BJU Int. 2007;99(6):1357–1362. doi:10.1111/bju.2007.99.issue-6
22. Chen CH, Dickman KG, Moriya M, et al. Aristolochic acid-associated urothelial cancer in Taiwan. Proc Natl Acad Sci U S A. 2012;109(21):8241–8246. doi:10.1073/pnas.1119920109
23. Zhong W, Zhang L, Ma J, et al. Impact of aristolochic acid exposure on oncologic outcomes of upper tract urothelial carcinoma after radical nephroureterectomy. Onco Targets Ther. 2017;10:5775–5782. doi:10.2147/OTT
24. Koornstra JJ, Mourits MJ, Sijmons RH, Leliveld AM, Hollema H, Kleibeuker JH. Management of extracolonic tumours in patients with Lynch syndrome. Lancet Oncol. 2009;10(4):400–408. doi:10.1016/S1470-2045(09)70041-5
25. Soria J-C, Italiano A, Cervantes A, et al. Safety and activity of the pan–fibroblast growth factor receptor (FGFR) inhibitor erdafitinib in Phase 1 study patients with advanced urothelial carcinoma. Ann Oncol. 2016;27(suppl_6). doi:10.1093/annonc/mdw373.09
26. Loriot Y, Necchi A, Park SH, et al. Erdafitinib in locally advanced or metastatic urothelial carcinoma. N Engl J Med. 2019;381(4):338–348. doi:10.1056/NEJMoa1817323
27. Azemar MD, Comperat E, Richard F, Cussenot O, Roupret M. Bladder recurrence after surgery for upper urinary tract urothelial cell carcinoma: frequency, risk factors, and surveillance. Urol Oncol. 2011;29(2):130–136. doi:10.1016/j.urolonc.2009.06.003
28. Wolf JS
29. Russo P, Huang W. The medical and oncological rationale for partial nephrectomy for the treatment of T1 renal cortical tumors. Urol Clin North Am. 2008;35(4):
30. Seisen T, Peyronnet B, Dominguez-Escrig JL, et al. Oncologic outcomes of kidney-sparing surgery versus radical nephroureterectomy for upper tract urothelial carcinoma: a systematic review by the EAU non-muscle invasive bladder cancer guidelines panel. Eur Urol. 2016;70(6):1052–1068. doi:10.1016/j.eururo.2016.07.014
31. National Comprehensive Cancer Network. Flaig TW, Spiess PE; for the NGP. NCCN Guidelines Version 4.2019 for Bladder Cancer. NCCN Clinical Practice Guidelines in Oncology. 2019.
32. Azizi M, Cheriyan SK, Peyton CC, Foerster B, Shariat SF, Spiess PE. Optimal management of upper tract urothelial carcinoma: an unmet need. Curr Treat Options Oncol. 2019;20(5):40. doi:10.1007/s11864-019-0637-2
33. Palou J, Piovesan LF, Huguet J, Salvador J, Vicente J, Villavicencio H. Percutaneous nephroscopic management of upper urinary tract transitional cell carcinoma: recurrence and long-term followup. J Urol. 2004;172(1):66–69. doi:10.1097/01.ju.0000132128.79974.db
34. Fajkovic H, Klatte T, Nagele U, et al. Results and outcomes after endoscopic treatment of upper urinary tract carcinoma: the Austrian experience. World J Urol. 2013;31(1):37–44. doi:10.1007/s00345-012-0948-4
35. Breda A, Territo A, Guttilla A, et al. Correlation between confocal laser endomicroscopy (Cellvizio((R))) and histological grading of upper tract urothelial carcinoma: a step forward for a better selection of patients suitable for conservative management. Eur Urol Focus. 2018;4(6):954–959. doi:10.1016/j.euf.2017.05.008
36. Liem E, Freund JE, Savci-Heijink CD, et al. Validation of confocal laser endomicroscopy features of bladder cancer: the next step towards real-time histologic grading. Eur Urol Focus. 2018. doi:10.1016/j.euf.2018.07.012
37. Thalmann GN, Markwalder R, Walter B, Studer UE. Long-term experience with bacillus Calmette-Guerin therapy of upper urinary tract transitional cell carcinoma in patients not eligible for surgery. J Urol. 2002;168(4 Pt 1):1381–1385. doi:10.1016/S0022-5347(05)64454-0
38. Katz MH, Lee MW, Gupta M. Setting a new standard for topical therapy of upper-tract transitional-cell carcinoma: BCG and interferon-alpha2B. J Endourol Endourological Soc. 2007;21(4):
39. Irie A, Iwamura M, Kadowaki K, Ohkawa A, Uchida T, Baba S. Intravesical instillation of bacille Calmette-Guerin for carcinoma in situ of the urothelium involving the upper urinary tract using vesicoureteral reflux created by a double-pigtail catheter. Urology. 2002;59(1):53–57. doi:10.1016/S0090-4295(01)01488-1
40. Yossepowitch O, Lifshitz DA, Dekel Y, et al. Assessment of vesicoureteral reflux in patients with self-retaining ureteral stents: implications for upper urinary tract instillation. J Urol. 2005;173(3):890–893. doi:10.1097/01.ju.0000147747.89028.64
41. Pollard ME, Levinson AW, Shapiro EY, et al. Comparison of 3 upper tract anticarcinogenic agent delivery techniques in an ex vivo porcine model. Urology. 2013;82(6):1451e1451–1456. doi:10.1016/j.urology.2013.08.048
42. Liu Z, Ng J, Yuwono A, Lu Y, Tan YK. Which is best method for instillation of topical therapy to the upper urinary tract? An in vivo porcine study to evaluate three delivery methods. Int Braz j. 2017;43(6):1084–1091. doi:10.1590/s1677-5538.ibju.2016.0258
43. Giannarini G, Kessler TM, Birkhauser FD, Thalmann GN, Studer UE. Antegrade perfusion with bacillus Calmette-Guerin in patients with non-muscle-invasive urothelial carcinoma of the upper urinary tract: who may benefit? Eur Urol. 2011;60(5):955–960. doi:10.1016/j.eururo.2011.07.051
44. Rastinehad AR, Smith AD. Bacillus Calmette-Guerin for upper tract urothelial cancer: is there a role? J Endourol Endourological Soc. 2009;23(4):563–568. doi:10.1089/end.2008.0164
45. Metcalfe M, Wagenheim G, Xiao L, et al. Induction and maintenance adjuvant mitomycin C topical therapy for upper tract urothelial carcinoma: tolerability and intermediate term outcomes. J Endourol Endourological Soc. 2017;31(9):946–953. doi:10.1089/end.2016.0871
46. Barros AA, Oliveira C, Reis RL, Lima E, Duarte ARC. In vitro and ex vivo permeability studies of paclitaxel and doxorubicin from drug-eluting biodegradable ureteral stents. J Pharm Sci. 2017;106(6):1466–1474. doi:10.1016/j.xphs.2017.02.023
47. Donin NM, Strauss-Ayali D, Agmon-Gerstein Y, et al. Serial retrograde instillations of sustained release formulation of mitomycin C to the upper urinary tract of the Yorkshire swine using a thermosensitive polymer: safety and feasibility. Urol Oncol. 2017;35(5):272–278. doi:10.1016/j.urolonc.2016.11.019
48. Peyronnet B, Seisen T, Dominguez-Escrig JL, et al. Oncological outcomes of laparoscopic nephroureterectomy versus open radical nephroureterectomy for upper tract urothelial carcinoma: an European Association Of Urology Guidelines systematic review. Eur Urol Focus. 2019;5(2):205–223. doi:10.1016/j.euf.2017.10.003
49. Ribal MJ, Huguet J, Alcaraz A. Oncologic outcomes obtained after laparoscopic, robotic and/or single port nephroureterectomy for upper urinary tract tumours. World J Urol. 2013;31(1):93–107. doi:10.1007/s00345-012-0968-0
50. Marshall S, Stifelman M. Robot-assisted surgery for the treatment of upper urinary tract urothelial carcinoma. Urol Clin North Am. 2014;41(4):521–537. doi:10.1016/j.ucl.2014.07.007
51. Pathak RA, Hemal AK. Techniques and outcomes of robot-assisted nephro-ureterectomy for upper tract urothelial carcinoma. Eur Urol Focus. 2018;4(5):657–661. doi:10.1016/j.euf.2018.08.007
52. Seisen T, Granger B, Colin P, et al. A systematic review and meta-analysis of clinicopathologic factors linked to intravesical recurrence after radical nephroureterectomy to treat upper tract urothelial carcinoma. Eur Urol. 2015;67(6):1122–1133. doi:10.1016/j.eururo.2014.11.035
53. Ark JT, Herrell SD. Chapter 10: Open and laparoscopic nephroureterectomy. In: Smith JA, Howards SS, Preminger GM, Dmochowski RR, editors. Hinman’s Atlas of Urologic Surgery.
54. Xylinas E, Rink M, Cha EK, et al. Impact of distal ureter management on oncologic outcomes following radical nephroureterectomy for upper tract urothelial carcinoma. Eur Urol. 2014;65(1):210–217. doi:10.1016/j.eururo.2012.04.052
55. Gschwend JE, Heck MM, Lehmann J, et al. Extended versus limited lymph node dissection in bladder cancer patients undergoing radical cystectomy: survival results from a prospective, randomized trial. Eur Urol. 2019;75(4):604–611. doi:10.1016/j.eururo.2018.09.047
56. Cole AP, Dalela D, Hanske J, et al. Temporal trends in receipt of adequate lymphadenectomy in bladder cancer 1988 to 2010. Urol Oncol. 2015;33(12):504e509–517. doi:10.1016/j.urolonc.2015.07.015
57. Bruins HM, Veskimae E, Hernandez V, et al. The impact of the extent of lymphadenectomy on oncologic outcomes in patients undergoing radical cystectomy for bladder cancer: a systematic review. Eur Urol. 2014;66(6):1065–1077. doi:10.1016/j.eururo.2014.05.031
58. Roscigno M, Brausi M, Heidenreich A, et al. Lymphadenectomy at the time of nephroureterectomy for upper tract urothelial cancer. Eur Urol. 2011;60(4):776–783. doi:10.1016/j.eururo.2011.07.009
59. Kondo T, Nakazawa H, Ito F, Hashimoto Y, Toma H, Tanabe K. Primary site and incidence of lymph node metastases in urothelial carcinoma of upper urinary tract. Urology. 2007;69(2):265–269. doi:10.1016/j.urology.2006.10.014
60. Matin SF, Sfakianos JP, Espiritu PN, Coleman JA, Spiess PE. Patterns of lymphatic metastases in upper tract urothelial carcinoma and proposed dissection templates. J Urol. 2015;194(6):1567–1574. doi:10.1016/j.juro.2015.06.077
61. Campi R, Minervini A, Mari A, et al. Anatomical templates of lymph node dissection for upper tract urothelial carcinoma: a systematic review of the literature. Expert Rev Anticancer Ther. 2017;17(3):235–246. doi:10.1080/14737140.2017.1285232
62. Seisen T, Shariat SF, Cussenot O, et al. Contemporary role of lymph node dissection at the time of radical nephroureterectomy for upper tract urothelial carcinoma. World J Urol. 2017;35(4):535–548. doi:10.1007/s00345-016-1764-z
63. Kondo T, Tanabe K. The role of lymph node dissection in the management of urothelial carcinoma of the upper urinary tract. Int J Clin Oncol. 2011;16(3):170–178. doi:10.1007/s10147-011-0234-2
64. O’Brien T, Ray E, Singh R, Coker B, Beard R. British Association of Urological Surgeons Section of O. Prevention of bladder tumours after nephroureterectomy for primary upper urinary tract urothelial carcinoma: a prospective, multicentre, randomised clinical trial of a single postoperative intravesical dose of mitomycin C (the ODMIT-C trial). Eur Urol. 2011;60(4):703–710. doi:10.1016/j.eururo.2011.05.064
65. Ito A, Shintaku I, Satoh M, et al. Prospective randomized phase II trial of a single early intravesical instillation of pirarubicin (THP) in the prevention of bladder recurrence after nephroureterectomy for upper urinary tract urothelial carcinoma: the THP Monotherapy Study Group Trial. J Clin Oncol. 2013;31(11):1422–1427. doi:10.1200/JCO.2012.45.2128
66. Hwang EC, Sathianathen NJ, Jung JH, Kim MH, Dahm P, Risk MC. Single-dose intravesical chemotherapy after nephroureterectomy for upper tract urothelial carcinoma. Cochrane Database Syst Rev. 2019;5:CD013160.
67. Margulis V, Youssef RF, Karakiewicz PI, et al. Preoperative multivariable prognostic model for prediction of nonorgan confined urothelial carcinoma of the upper urinary tract. J Urol. 2010;184(2):453–458. doi:10.1016/j.juro.2010.03.142
68. Favaretto RL, Shariat SF, Savage C, et al. Combining imaging and ureteroscopy variables in a preoperative multivariable model for prediction of muscle-invasive and non-organ confined disease in patients with upper tract urothelial carcinoma. BJU Int. 2012;109(1):77–82. doi:10.1111/j.1464-410X.2011.10288.x
69. Freifeld Y, Ghandour R, Singla N, et al. Preoperative predictive model and nomogram for disease recurrence following radical nephroureterectomy for high grade upper tract urothelial carcinoma. Urol Oncol. 2019;37(10):758–764. doi:10.1016/j.urolonc.2019.06.009
70. Cha EK, Shariat SF, Kormaksson M, et al. Predicting clinical outcomes after radical nephroureterectomy for upper tract urothelial carcinoma. Eur Urol. 2012;61(4):818–825. doi:10.1016/j.eururo.2012.01.021
71. Yates DR, Hupertan V, Colin P, et al. Cancer-specific survival after radical nephroureterectomy for upper urinary tract urothelial carcinoma: proposal and multi-institutional validation of a post-operative nomogram. Br J Cancer. 2012;106(6):1083–1088. doi:10.1038/bjc.2012.64
72. Seisen T, Colin P, Hupertan V, et al. Postoperative nomogram to predict cancer-specific survival after radical nephroureterectomy in patients with localised and/or locally advanced upper tract urothelial carcinoma without metastasis. BJU Int. 2014;114(5):733–740. doi:10.1111/bju.2014.114.issue-5
73. Ku JH, Moon KC, Jung JH, Jeong SH, Kwak C, Kim HH. External validation of an online nomogram in patients undergoing radical nephroureterectomy for upper urinary tract urothelial carcinoma. Br J Cancer. 2013;109(5):1130–1136. doi:10.1038/bjc.2013.462
74. Roupret M, Hupertan V, Seisen T, et al. Prediction of cancer specific survival after radical nephroureterectomy for upper tract urothelial carcinoma: development of an optimized postoperative nomogram using decision curve analysis. J Urol. 2013;189(5):1662–1669. doi:10.1016/j.juro.2012.10.057
75. Krabbe LM, Eminaga O, Shariat SF, et al. Postoperative nomogram for relapse-free survival in patients with high grade upper tract urothelial carcinoma. J Urol. 2017;197(3 Pt 1):580–589. doi:10.1016/j.juro.2016.09.078
76. Kubota Y, Hatakeyama S, Tanaka T, et al. Oncological outcomes of neoadjuvant chemotherapy in patients with locally advanced upper tract urothelial carcinoma: a multicenter study. Oncotarget. 2017;8(60):101500–101508. doi:10.18632/oncotarget.v8i60
77. Hosogoe S, Hatakeyama S, Kusaka A, et al. Platinum-based neoadjuvant chemotherapy improves oncological outcomes in patients with locally advanced upper tract urothelial carcinoma. Eur Urol Focus. 2018;4(6):946–953. doi:10.1016/j.euf.2017.03.013
78. Leow JJ, Martin-Doyle W, Fay AP, Choueiri TK, Chang SL, Bellmunt J. A systematic review and meta-analysis of adjuvant and neoadjuvant chemotherapy for upper tract urothelial carcinoma. Eur Urol. 2014;66(3):529–541. doi:10.1016/j.eururo.2014.03.003
79. Matin SF, Margulis V, Kamat A, et al. Incidence of downstaging and complete remission after neoadjuvant chemotherapy for high-risk upper tract transitional cell carcinoma. Cancer. 2010;116(13):3127–3134. doi:10.1002/cncr.v116:13
80. Liao RS, Gupta M, Schwen ZR, et al. Comparison of pathological stage in patients treated with and without neoadjuvant chemotherapy for high risk upper tract urothelial carcinoma. J Urol. 2018;200(1):68–73. doi:10.1016/j.juro.2017.12.054
81. Porten S, Siefker-Radtke AO, Xiao L, et al. Neoadjuvant chemotherapy improves survival of patients with upper tract urothelial carcinoma. Cancer. 2014;120(12):1794–1799. doi:10.1002/cncr.28655
82. Kim DK, Lee JY, Kim JW, Hah YS, Cho KS. Effect of neoadjuvant chemotherapy on locally advanced upper tract urothelial carcinoma: a systematic review and meta-analysis. Crit Rev Oncol Hematol. 2019;135:59–65. doi:10.1016/j.critrevonc.2019.01.019
83. Aziz A, Dobruch J, Hendricksen K, et al. Perioperative chemotherapy in upper tract urothelial carcinoma: a comprehensive review. World J Urol. 2017;35(9):1401–1407. doi:10.1007/s00345-016-1995-z
84. Hoffman-Censits JH, Margulis V, Hahn NM, Trabulsi EJ, Beaver A, Plimack ER. ECOG 8141: a prospective phase II trial of neoadjuvant systemic chemotherapy followed by extirpative surgery for patients with high grade upper tract urothelial carcinoma. J Clin Oncol. 2016;34(15_suppl):TPS4585–TPS4585. doi:10.1200/JCO.2016.34.15_suppl.TPS4585
85. Hoffman-Censits J, Puligandla M, Trabulsi E, et al. LBA26 Phase II trial of neoadjuvant chemotherapy followed by extirpative surgery for patients with high grade upper tract urothelial carcinoma (HG UTUC): results from ecog-acrin 8141. J Urol. 2018;199(4S):. doi:10.1016/j.juro.2018.03.098
86. Coleman JA, Wong NC, Sjoberg DD, et al. LBA-17: Late-Breaking Abstract: Multicenter Prospective Phase II Clinical Trial of Gemcitabine and Cisplatin as Neoadjuvant Chemotherapy in Patients with High-Grade Upper Tract Urothelial Carcinoma. Chicago, IL: Annual Meeting of American Urological Association 2019; 2019.
87. Olgac S, Mazumdar M, Dalbagni G, Reuter VE. Urothelial carcinoma of the renal pelvis: a clinicopathologic study of 130 cases. Am J Surg Pathol. 2004;28(12):1545–1552. doi:10.1097/00000478-200412000-00001
88. Seisen T, Krasnow RE, Bellmunt J, et al. Effectiveness of adjuvant chemotherapy after radical nephroureterectomy for locally advanced and/or positive regional lymph node upper tract urothelial carcinoma. J Clin Oncol. 2017;35(8):852–860. doi:10.1200/JCO.2016.69.4141
89. Birtle AJ, Chester JD, Jones RJ, et al. Results of POUT: a phase III randomised trial of perioperative chemotherapy versus surveillance in upper tract urothelial cancer (UTUC). J Clin Oncol. 2018;36(6_suppl):407. doi:10.1200/JCO.2018.36.6_suppl.407
90. Weng YM, Peng M, Hu MX, Yao Y, Song QB. Clinical and molecular characteristics associated with the efficacy of PD-1/PD-L1 inhibitors for solid tumors: a meta-analysis. Onco Targets Ther. 2018;11:7529–7542. doi:10.2147/OTT
91. Stenehjem DD, Tran D, Nkrumah MA, Gupta S. PD1/PDL1 inhibitors for the treatment of advanced urothelial bladder cancer. Onco Targets Ther. 2018;11:5973–5989. doi:10.2147/OTT
92. Baldini C, Champiat S, Vuagnat P, Massard C. Durvalumab for the management of urothelial carcinoma: a short review on the emerging data and therapeutic potential. Onco Targets Ther. 2019;12:2505–2512. doi:10.2147/OTT.S141040
93. Rosenberg JE, Hoffman-Censits J, Powles T, et al. Atezolizumab in patients with locally advanced and metastatic urothelial carcinoma who have progressed following treatment with platinum-based chemotherapy: a single-arm, multicentre, phase 2 trial. Lancet. 2016;387(10031):1909–1920. doi:10.1016/S0140-6736(16)00561-4
94. Fradet Y, Bellmunt J, Vaughn DJ, et al. Randomized phase III KEYNOTE-045 trial of pembrolizumab versus paclitaxel, docetaxel, or vinflunine in recurrent advanced urothelial cancer: results of >2 years of follow-up. Ann Oncol. 2019;30:970–976. doi:10.1093/annonc/mdz127
95. Powles T, Duran I, van der Heijden MS, et al. Atezolizumab versus chemotherapy in patients with platinum-treated locally advanced or metastatic urothelial carcinoma (IMvigor211): a multicentre, open-label, Phase 3 randomised controlled trial. Lancet. 2012;109(1):748–757. doi:10.1016/S0140-6736(17)33297-X
96. Sharma P, Retz M, Siefker-Radtke A, et al. Nivolumab in metastatic urothelial carcinoma after platinum therapy (CheckMate 275): a multicentre, single-arm, phase 2 trial. Lancet Oncol. 2017;18(3):312–322. doi:10.1016/S1470-2045(17)30065-7
97. Sharma P, Callahan MK, Bono P, et al. Nivolumab monotherapy in recurrent metastatic urothelial carcinoma (CheckMate 032): a multicentre, open-label, two-stage, multi-arm, phase 1/2 trial. Lancet Oncol. 2016;17(11):1590–1598. doi:10.1016/S1470-2045(16)30496-X
98. Powles T, O’Donnell PH, Massard C, et al. Efficacy and safety of durvalumab in locally advanced or metastatic urothelial carcinoma: updated results from a Phase 1/2 open-label study. JAMA Oncol. 2017;3(9):e172411. doi:10.1001/jamaoncol.2017.2411
99. Patel MR, Ellerton J, Infante JR, et al. Avelumab in metastatic urothelial carcinoma after platinum failure (JAVELIN solid tumor): pooled results from two expansion cohorts of an open-label, phase 1 trial. Lancet Oncol. 2018;19(1):51–64. doi:10.1016/S1470-2045(17)30900-2
100. Wang Y, Zhou S, Yang F, et al. Treatment-related adverse events of PD-1 and PD-L1 inhibitors in clinical trials: a systematic review and meta-analysis. JAMA Oncol. 2019.
101. Haanen J, Carbonnel F, Robert C, et al. Management of toxicities from immunotherapy: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29(Supplement_4):iv264–iv266. doi:10.1093/annonc/mdy162
102. Moschini M, Shariat SF, Roupret M, et al. Impact of primary tumor location on survival from the European Organization for the research and treatment of cancer advanced urothelial cancer studies. J Urol. 2018;199(5):1149–1157. doi:10.1016/j.juro.2017.11.068
103. Hahn AW, Giri S, Pathak R, Bhatt VR, Martin MG. Effect of adjuvant radiotherapy on survival in patients with locoregional urothelial malignancies of the upper urinary tract. Anticancer Res. 2016;36(8):4051–4055.
104. Huang YC, Chang YH, Chiu KH, Shindel AW, Lai CH. Adjuvant radiotherapy for locally advanced upper tract urothelial carcinoma. Sci Rep. 2016;6:38175. doi:10.1038/srep38175
105. Czito B, Zietman A, Kaufman D, Skowronski U, Shipley W. Adjuvant radiotherapy with and without concurrent chemotherapy for locally advanced transitional cell carcinoma of the renal pelvis and ureter. J Urol. 2004;172(4 Pt 1):1271–1275. doi:10.1097/01.ju.0000137910.38441.8a
106. Seisen T, Jindal T, Karabon P, et al. Efficacy of systemic chemotherapy plus radical nephroureterectomy for metastatic upper tract urothelial carcinoma. Eur Urol. 2017;71(5):714–718. doi:10.1016/j.eururo.2016.11.012
107. Balar AV, Castellano D, O’Donnell PH, et al. First-line pembrolizumab in cisplatin-ineligible patients with locally advanced and unresectable or metastatic urothelial cancer (KEYNOTE-052): a multicentre, single-arm, phase 2 study. Lancet Oncol. 2017;18(11):1483–1492. doi:10.1016/S1470-2045(17)30616-2
108. Balar AV, Galsky MD, Rosenberg JE, et al. Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: a single-arm, multicentre, phase 2 trial. Lancet. 2017;389(10064):67–76. doi:10.1016/S0140-6736(16)32455-2
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.