Back to Journals » Clinical Ophthalmology » Volume 13
Optimal management of pediatric keratoconus: challenges and solutions
Authors Olivo-Payne A ![]() , Abdala-Figuerola A, Hernandez-Bogantes E, Pedro-Aguilar L, Chan E, Godefrooij D
, Abdala-Figuerola A, Hernandez-Bogantes E, Pedro-Aguilar L, Chan E, Godefrooij D
Received 27 February 2019
Accepted for publication 18 June 2019
Published 10 July 2019 Volume 2019:13 Pages 1183—1191
DOI https://doi.org/10.2147/OPTH.S183347
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Andrew Olivo-Payne,1 Alexandra Abdala-Figuerola,2 Erick Hernandez-Bogantes,3 Lucero Pedro-Aguilar,4 Elsie Chan,5 Daniel Godefrooij6
1Cornea and Refractive Surgery Department, Instituto De Oftalmología Fundación Conde De Valenciana, Mexico City, Mexico; 2Cornea Department, Grupo Oftalmologico Abdala-Figuerola, Barranquilla, Colombia; 3Cornea Department, Centro Ocular, Heredia, Costa Rica; 4Instituto De Oftalmología Fundación Conde De Valenciana, Mexico City, Mexico; 5Cornea Unit, Royal Victorian Eye and Ear Hospital, Centre for Eye Research Australia, University of Melbourne, Melbourne, Australia; 6Utrecht Cornea Research Group, Universitair Medisch Centrum Utrecht, Utrecht, Netherlands
Abstract: Keratoconus (KC) shows several distinctive features in clinical appearance, disease progression, and treatment in children compared with adults. Therefore, diagnostic, clinical care, and therapeutic approaches are different. However, pediatric keratoconus is often undiagnosed and thus untreated in many cases. Once diagnosis has been made, compliance with treatment recommendations is often poor. Pediatric keratoconus also tends to have more rapid progression than in adults; therefore, early detection and treatment are paramount to prevent serious vision impairment, which can affect the child’s development. This review of pediatric keratoconus discusses important issues such as worldwide epidemiology, clinical features in children compared to adults, and challenges in diagnosis and treatment and focuses on the most appropriate management strategies based on the best available current evidence.
Keywords: cornea, pediatric, keratoconus, crosslinking, corneal transplant, ICRS
Introduction
Keratoconus (KC) is a progressive, bilateral, thinning disorder of the cornea in which biomechanical changes in corneal collagen fibers result in progressive increase in corneal curvature and thinning.1,2 Occurring at an estimated (variable) prevalence in the general population of approximately 1:375 to 1:2,000, patients usually present with a deterioration in visual acuity secondary to myopia and irregular astigmatism. Rupture in Descemet’s membrane, acute corneal edema, and subsequent scarring are other causes of vision loss.3,4
Compared to adults, keratoconus in children progresses more rapidly and is usually more severe at the time diagnosis. Hence, prompt management to halt the progression of the disease and enhance visual performance is crucial.
Nonsurgical options such as spectacles and contact lenses (soft, rigid or scleral) in children are not always tolerated and often insufficient to obtain a satisfactory visual acuity. (Table 1)5 Furthermore, none of these conservative options halt progression of the disease. Studies on pediatric keratoconus suggest that at the time of diagnosis, 27.8% are at an advanced stage and 88% progress. Thus, interventions with acceptable safety-efficacy profiles (ie, corneal collagen crosslinking [CXL], and its variations) to increase the biomechanical strength and stability of the cornea have been established. However, in the pediatric population, poor compliance and necessary modifications in treatment modalities create challenges that have yet to be overcome.6–8 This review analyzes the current challenges and solutions in diagnosing and managing pediatric keratoconus.
 |
Table 1 Challenges in pediatric keratoconus |
Epidemiology
There is limited evidence regarding the prevalence of Keratoconus (KC) in children. A study in Lebanon reported a prevalence of 1:200,9 and a more recent one in Saudi Arabia found a prevalence of 1 in 25.10 As mentioned previously, the prevalence in the general population is believed to be between 1:375 and 1:2,000.3 The prevalence of keratoconus varies worldwide: from 0.3 per 100,000 in Russia11 to 2,300 per 100,000 in Central India12 and 54.5 per 100,000 in the United States.13 The variability between the results may be due to environmental factors and genetic influence.
A multifactorial etiology has been proposed, although the exact pathogenesis is unclear. Studies have found a correlation between keratoconus and allergic disorders, especially in pediatric patients (Table 2).14–16 Allergic disorders include vernal keratoconjunctivitis, allergic keratoconjunctivitis, and atopic dermatitis, leading to chronic eye rubbing which appears to play an important role in the pathogenesis of the disease.17 Chronic eye rubbing and atopy was first described as a risk factor for keratoconus by Ridley et al in 1959.18 Contact lens wear (particularly with polymethyl methacrylate) is also considered as a precipitating factor due to microtrauma.17,18,19 Although the lack of inflammation has been questioned and recent studies have shown a role of proteolytic enzymes, cytokines, and free radicals, it does not necessarily meet all the classic criteria for an inflammatory disease.20 An increase in inflammatory mediators has also been found in the tear film of patients with keratoconus, suggesting a possible inflammatory etiology.21
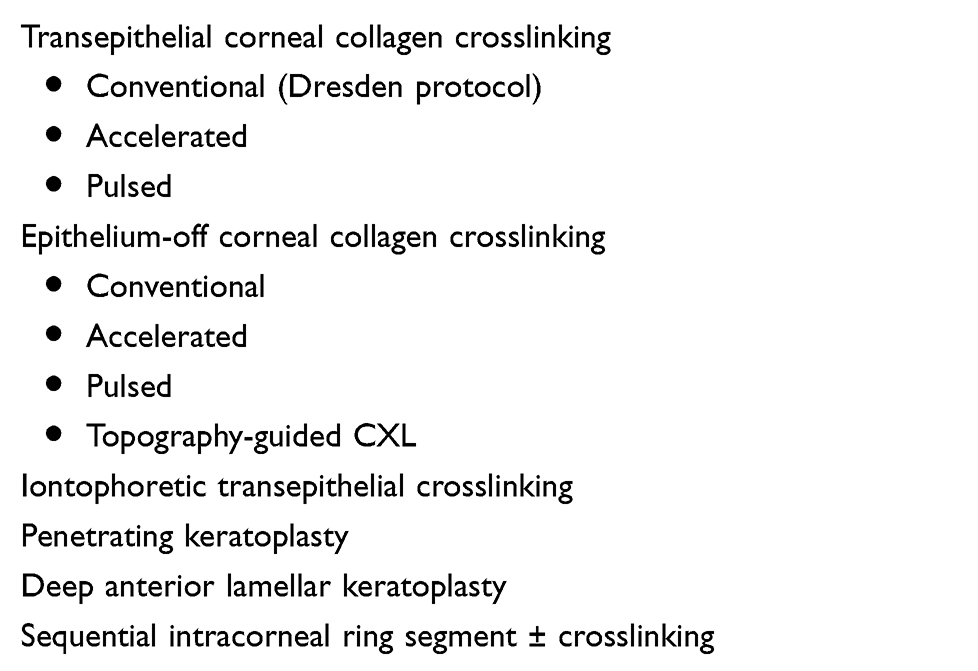 |
Table 2 Surgical options for pediatric keratoconus |
There is also a genetic component to the etiology of keratoconus as it is associated with systemic conditions such as Down´s syndrome, Marfan syndrome, mitral valve prolapse, and collagen tissue diseases. Genetic influence with familiar inheritance is also observed.22,23 Patients with first-degree relatives with keratoconus have 15 to 67 times higher risk in developing corneal ectasia compared to patients with no affected relatives.19,24
Ethnicity has been reported to play a role in keratoconus. Asians have 4.4 times the risk for developing keratoconus than Caucasians, and Indians have steeper corneas than Chinese patients with keratconus.25
Keratoconus is most frequently diagnosed in young adults; it commonly has its onset in puberty and may progress until the third or fourth decade of life. Pediatric keratoconus (onset before 18 years of age) is less common and is more aggressive than adult keratoconus. Few studies about the prevalence and incidence of keratoconus in children have been reported. The youngest case described was a girl with Down syndrome diagnosed at the age of 4 years.26 El-Khoury et al reported 2,972 patients, of which 541 had keratoconus; 16 patients were children 14 years or younger at the time of the diagnosis equating to an incidence of 0.53%, compared to an incidence of 3.78% in adults.9
Clinical features
As previously mentioned, keratoconus is a chronic, progressive bilateral corneal ectasia, most frequently diagnosed in adolescence. In its early stages, the disease can seem unilateral, although posterior corneal elevation is usually detected in both eyes. It is characterized by central or paracentral corneal thinning, irregular corneal astigmatism, and steepening of the cornea, resulting in high myopia and subsequently visual loss. In more advanced cases, rupture in Descemet’s membrane with acute corneal hydrops leads to corneal scarring.19,27
Adult vs pediatric keratoconus
The clinical appearance of keratoconus in children is somewhat different from that seen in adults. Morphologically, the ectatic cornea is more centrally located in pediatric cases; thus, irregular astigmatism is less pronounced.28 However, as keratoconus often progresses asymmetrically, pediatric patients maintain good binocular visual function until both eyes are affected: the “non-dominant” eye can progress without patients noticing a change in their visual acuity; it is only when their “dominant” eye deteriorates that they become more symptomatic and seek help.29 Moreover, ocular aberrations generated by the irregular cornea may be partially compensated by internal ocular structures and the high accommodative power (though not commonly seen in myopic patients) present at a younger age.30 Both of these factors may explain why parents seek ophthalmic care later in the course of the disease, when visual function has deteriorated significantly in their children.23 Al Suhaibani et al reported an inverse correlation between the severity of the disease and the age of onset.31 Hence, keratoconus in the pediatric population is more advanced at the time of diagnosis.
Leoni-Mesplie et al described 216 keratoconic patients, where 49 patients were 15 years or younger and 167 patients were 27 years or older.32 At the time of the diagnosis, 27.8% of the young group had stage IV keratoconus (Amsler-Krumeich classification) versus 7.8% in the adult group. These results were comparable to the study by El-Khoury et al, where 30% of pediatric patients had stage IV keratoconus at the time of the diagnosis.9 Due to the more rapid progression and severity, children have a higher risk of acute corneal hydrops, leading to an increased need for corneal transplantation to improve vision.
Increased corneal curvature has also been reported in pediatric patients compared to adults. Chatzis and Hafezi noted that in 59 keratoconic eyes in patients between the ages of 9 and 19 years, there was an increase in corneal steepening (Kmax) greater than 2 dioptres in 1 year, with a progression rate of 88%.8 Another characteristic observed in children is that central cones are more common, with this group progressing more rapidly than peripheral cones.28
In many cases, these groups of patients require surgical treatment an earlier age: in mild-to-moderate ectasia, corneal crosslinking is recommended to stop progression of the disease whereas in severe cases with corneal scarring, corneal keratoplasty for visual rehabilitation is indicated (Table 3).
 |
Table 3 Risk factors in pediatric keratoconus |
Diagnostic challenges
Keratoconus can be clinically diagnosed on slit-lamp findings (ie, corneal steepening, thinning, Vogt’s striae, and Fleischer ring). However, these changes are seen mainly in moderate-to-severe stages of the disease. Conversely, there may be no obvious changes in the earliest stages of keratoconus, leading the majority of these patients, and importantly, pediatric patients to remain undiagnosed.
Several classification systems for keratoconus exist. One of the earliest is the Amsler–Krumeich classification system, which is divided into 4 stages according to the severity of the disease, incorporating myopia, astigmatism, keratometry readings, central corneal thickness, and the transparency of the cornea. Although this system is widely used among ophthalmologists, it has limitations. It only measures the anterior corneal surface at the center of the cornea. Patients with keratoconus commonly have paracentral corneal thinning; therefore, a full corneal thickness map is more useful for classification purposes.33
Modified Rabinowitz–McDonnel indices are also helpful. It incorporates central keratometric reading (K) and inferior–superior dioptric asymmetry (I/S index). Values higher than K >47.2D and I/S index >1.2 are suggestive of keratoconus.34
Placido disc-based corneal topography had previously been described as the gold standard tool. However, it has the restriction of only measuring the anterior corneal surface. With the advent of newer imaging technologies such as Scheimpflug, optical coherence tomography (OCT), and slit-scan tomography, the anterior and posterior cornea can be measured and are now accepted as the best and widely available tests to diagnose early keratoconus.35
Consequently, developing newer classifications and staging systems is necessary. Using Schiempflug technology (Pentacam, Oculus, Germany), the Belin/Ambrosio Enhanced Ectasia Display (BAD) program assesses the likelihood that a cornea is ectatic. It uses the pachymetry map and anterior and posterior elevation maps and compare it with the standard best-fit-sphere (BFS) from the central 8 mm.36 Additional improvements to this program to enhance the reference surface have subsequently been implemented. This was obtained by eliminating the central 3–4 mm optical zone (cone area) from the standard 8 mm BFS. By doing so, the new reference surface is calculated based on the peripheral normal cornea values; therefore, any abnormal corneal protrusion will be highlighted as pathological.35
Belin et al have also reported the ABCD grading system, a newer tomographic method of staging keratoconus.35 It measures tomographic data and anatomical and functional changes and classifies keratoconus into stages 0–5. The tomographic data are the anterior curvature, posterior curvature, and pachymetry map; the functional changes measure the best-corrected distance visual acuity; the anatomical criteria take into consideration the absence or presence of corneal scarring.
Although corneal tomography is the gold standard for keratoconus screening, in early stages of the disease, it can sometimes be misdiagnosed with topography or tomography alone. High-resolution optical coherence tomography (HR OCT) and high-frequency ultrasound can detect epithelium, stromal, and corneal thickness changes in subclinical keratoconus, which may be more sensitive in diagnosing keratoconus in its earliest stage.37,38
Treatment
Intracorneal ring segment implantation
Only a few retrospective interventional case series have been published regarding intracorneal ring segment (ICRS) implantation for the treatment of pediatric keratoconus, with varying results.39–42 The most recent study combined ICRS and crosslinking and examined visual, refractive, and keratometric outcomes in 12 patients aged 14 years or younger. Corrected distance visual acuity improved 0.18 logMAR (logarithm of the minimum angle of resolution) and unaided visual acuity improved 0.47 logMAR; refraction and keratometry values also improved after 6 months. All parameters stabilized between 6 months and 4 years postoperatively, except for a small but significant improvement in cylinder and uncorrected distance visual acuity after 4 years. The surgery was well tolerated by most patients, and no intraoperative or postoperative complications were reported, except for one ring segment that had to be removed after 2 years due to vascularization and corneal thinning. According to the results of this study, ICRS implantation with cross-linking is a safe and effective procedure for visual rehabilitation in children with keratoconus and poor corrected distance visual acuity. As over 20% of all keratoconus patients demonstrate contact lens intolerance, ICRS implantation could be offered in selected cases, and especially in adolescent patients, assuming a 400-micrometer corneal thickness at the mid-periphery and in the absence of central corneal scarring. As in adults, ICRS results in good visual and topographic results in pediatric patients. However, ICRS alone does not halt the progression of keratoconus.40 Despite promising results, ICRS implantation is not commonly used in the pediatric age group due to the aggressive nature of keratoconus, frequent eye-rubbing, poor patient compliance, unpredictability of results, and the lack of nomograms adapted to pediatric keratoconus.43
Corneal transplant
Diagnosis of keratoconus before adulthood is a poor prognostic factor for disease progression, increasing the probability of the need for a corneal transplant. Corneal transplants for keratoconus in the pediatric population represent 15–20% of all corneal transplants,55 and those with progressive disease have a seven-fold higher risk of requiring a corneal transplant in the future. However, transplantation at a young age is associated with a higher risk of rejection and a poor visual prognosis. It is also a perioperative challenge for the corneal surgeon: preoperative risk factors must be assessed such as age of diagnosis, the existence of any form of allergic disease, the presence of associated genetic or connective tissue disorders, steep keratometric values, patient co-operation, and availability for frequent follow-up visits. Intraoperative challenges such as positive vitreous pressure, low scleral rigidity, and increased fibrin reaction must also be considered. If a transplant is performed at a very young age (although less likely in cases of keratoconus), postoperative care may require multiple examinations under anesthesia which is a risk in itself.27 If patients have a low risk of amblyopia or are beyond the age of amblyopia reversal, then corneal transplantation should be postponed as long as possible.
The interval from the onset of the disease to the development of an advanced stage of keratoconus with visual symptoms is shorter and faster in the pediatric age group. Therefore, every child with a history of atopy, eye rubbing, ocular allergy, or family history should be a suspect for keratoconus and screening is advised from a young age with frequent follow-up visits. An early diagnosis could prevent the progression of the disease and visual loss.
Preventing progression in pediatric keratoconus: solutions
After the diagnosis of keratoconus, it is of paramount importance to prevent progression in order to prevent deterioration of visual acuity and dependency of visual aids. One strategy for halting the progression of keratoconus is to perform corneal CXL.
CXL increases the mechanical strength of the affected cornea using a photosensitizer (riboflavin) and ultraviolet-A irradiation (370-nm wavelength light), which produce ROS, leading to crosslinking of interfibrillar collagen and increasing corneal biomechanical rigidity.44,45 CXL is usually performed for disease progression, although there is no standard definition of progression. It is most commonly defined as an increase in maximum keratometry of at least 1 diopter over 1 year, based on topographic findings. This value of 1 diopter was chosen because of the amount of variability in corneal topography measurements.46 Therefore, “progression” of 0.2 diopters within 1 year might very well be related to measurement error. The measurement error increases with keratoconus severity, leading to substantial amounts of uncertainty in cases with keratometry values above 55 diopters.47
Another important factor to consider when interpreting keratometry values is contact lens wear. Contact lenses alter the shape of the cornea, mostly by remodeling the epithelial surface. The usage of scleral lenses can alter maximum keratometry values by more than a diopter.48 Contact lenses that are placed directly on the cornea, such as rigid gas-permeable contact lenses that are often used in keratoconus, could influence the shape of the cornea even more. Therefore, pediatric contact lens wearers are usually instructed not to wear their contact lenses for one or several weeks before keratometry measurements. The ideal discontinuation time before measurements has not been established partly due to the fact that many keratoconus patients are heavily dependent on contact lenses and are unable to cease lens use for extended periods of time.
Due to the uncertainty of topography measurements alone, other variables are often incorporated to determine whether there is progression of keratoconus. Variables that are often included are corneal thickness, posterior curvature of the cornea, manifest refraction, uncorrected and corrected distance visual acuity, and patient age.35
An inverse relationship has been found between patient age and disease progression; in general, pediatric keratoconus is more likely to progress, and this progression can be very rapid and devastating.31 The Global Consensus on Keratoconus and Ectatic Diseases states that CXL can be beneficial upon diagnosis in young patients with keratoconus.49 However, there is concern about the efficacy and long-lasting effect of CXL in children.8
When counseling pediatric patients and their parents, it is important to understand that the level of evidence for pediatric CXL is inferior to the level of evidence in adults since no randomized controlled trials have been performed in children. Furthermore, the efficacy of pediatric CXL may not be equivalent to the efficacy of CXL in adults; the risk of keratometric progression after pediatric CXL is approximately 22% compared to 2–10% in adults.50 One of the boundaries to performing a randomized, controlled trial in children is that it may be considered unethical to withhold CXL from a child with progressive keratoconus in a control group in order to prove that care without CXL is inferior to care that includes CXL since treatment efficacy has been demonstrated in multiple randomized, controlled trials in adults.51
Conventional vs modified CXL
The original crosslinking protocol included the removal of the central corneal epithelium, application of riboflavin 0.1% as a photosensitizer and an irradiation time of 30 mins using 370 nm ultraviolet-A (UVA) light with an irradiance of 3 mW/cm2.45 This protocol is commonly referred to as the Dresden protocol. Adaptations of this protocol aimed at avoiding the need for epithelium removal (transepithelial CXL) and shortening the treatment time (accelerated CXL). This was attempted in order to prevent postoperative pain and the risk of infection due to epithelium removal and to circumvent the need for the patient to lie still for an extended period of time. This is especially relevant for children because the tolerance of pain and the ability to lie still are usually less at this age. However, the efficacy of transepithelial CXL in halting the progression of keratoconus is inferior to CXL with epithelial removal.52 This is mostly due to the fact that the inability of riboflavin to pass through the intact epithelium. A method that aims to circumvent the removal of the epithelium while enabling the riboflavin to penetrate the cornea stroma is iontophoresis-assisted transepithelial CXL. However, interest in this treatment has diminished since it has been demonstrated to be less effective than standard CXL with epithelium removal in a head-to-head comparison.56
Pulsed CXL
A recent novelty is the introduction of pulsed CXL. During photosensitization, oxygen in the corneal stroma is an important component of the chemical reactions. In accelerated CXL protocols where the irradiation time is markedly reduced, it is thought that there may be insufficient time for replenishment of oxygen levels in the stroma, leading to decreased treatment efficacy. Therefore, by pulsing the UVA irradiation during the exposure time allows oxygen to diffuse deeper into the corneal stroma during pauses in the UVA, which may increase the treatment depth and the resultant corneal stiffening. Literature on pulsed CXL is limited, and although the depth of treatment might be deeper in rabbit corneas the added clinical value of pulsed CXL compared to conventional CXL has not been proven.53
Many studies have been published on the efficacy of accelerated CXL compared to the original Dresden treatment protocol with varying results. However, a head-to-head comparison in randomized, controlled trials with sample sizes large enough to detect small but potentially relevant differences in efficacy is still lacking. Therefore, crosslinking with epithelium removal remains the current gold standard, although alternative photosensitizers are under investigation.
Topography-guided CXL
A treatment protocol that has the potential to replace the standard CXL protocol is topography-guided CXL. The rationale of this treatment is that CXL can be altered based on each individual’s cone shape; the ultraviolet light intensity is augmented based on the corneal topography which can result in more flattening of the ectatic area of the cornea. Topography-guided CXL (photorefractive intrastromal crosslinking, PiXL) has led to superior results in spherical equivalent and visual acuity after 12 months compared to standard CXL in a randomized controlled trial.54
Postoperative management
All patients require antibiotics and topical steroids after CXL. However, some considerations should be taken into account regarding pediatric patients. Children must be under observation for possible intraocular pressure elevation during the topical steroid treatment. Children should not resume the use of contact lenses until complete corneal epithelialization.
Acute pain management is frequently necessary within the first 24–48 hrs after surgery and is particularly important in children where pain tolerance may be lower. Management options include systemic and topical nonsteroidal anti-inflammatory medications, cycloplegic drops, and an eye patch (when only one eye was treated) or a bandage contact lens to improve comfort in these patients.
Challenges after crosslinking
Corneal healing
Complete epithelialization is generally achieved 4 days after the procedure. A mild haze can be observed in a majority of patients on slit-lamp examination, but it does not have any effect on the visual acuity and usually decreases with topical steroid treatment by 2 months after surgery.
Endothelial cell loss
Endothelial cell density (ECD) has not been shown to be affected after CXL in pediatric subjects after 2 years of follow-up.55,57
Failure
In adults, CXL treatment results in a complication rate (loss of 2 or more Snellen lines) of approximately 2.9%.58 Failure of CXL to arrest keratoconus progression may be attributed to different genetic patterns, biomechanical modifications occurring in the corneal stroma, and the negative influence of other conditions such as allergy and atopy. A preoperative maximum keratometry reading of less than 58.0 diopters may reduce the failure rate, and restricting patient age may further reduce the complication rate to 1%.59,60 Other complications include visually significant haze, scarring, and keratitis.
In children, there are limited reports about failure to arrest progression. Shetty et al reported on accelerated CXL outcomes in children younger than 14 years and observed failure in 17.6% of treated cases. Failure was associated with a history of allergic conjunctivitis, where persistent eye rubbing may “nullify” the effect of CXL. Therefore, it is important to actively treat underlying allergic eye disease with topical steroids and topical mast cell stabilizers when it is necessary.57,61
Limbal stem cell damage
There is concern that CXL may potentially damage limbal stem cells. Attention should be paid to the ultraviolet irradiation area at all times, particularly in children, as distraction may lead to inadvertent limbal irradiation. On the other hand, children with concomitant vernal or atopic keratoconjunctivitis may have preexisting subclinical limbal stem cell deficiency; therefore, it is recommended to use a limbal guard to prevent further damage.57
Conclusion
As in adults, several management options are available for the treatment of pediatric keratoconus. The main objectives in children are to halt the progression of the disease, visual loss prevention, and ultimately avoid corneal transplantation.
Currently, the only known treatment that has been proven to prevent progression is crosslinking. CXL performed in children has shown similar initial efficacy as adults in terms of improvement of visual and topographic outcomes; however, long-term outcomes are more variable. CXL can potentially prevent visual loss and prevent the need for corneal transplantation. Allergic eye disease in children with keratoconus should be treated aggressively, especially if they are undergoing CXL. Although there is limited evidence, accelerated CXL appears to show results comparable to those of conventional CXL in arresting the progression of keratoconus in pediatric patients. The optimal CXL protocol for children will depend on the severity of the disease, patient cooperation, and availability of riboflavin and irradiation devices in order to meet the individual patient’s needs.
Due to the scarcity of randomized, controlled trials in pediatric keratoconus, the majority of data are inferred from clinical trials and case series with adult patients. Therefore, currently, authors have been unable to determine a gold standard for the treatment of keratoconus in children.
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Baenninger PB, Bachmann LM, Wienecke L, Thiel MA, Kaufmann C. Pediatric corneal cross-linking: comparison of visual and topographic outcomes between conventional and accelerated treatment. Am J Ophthalmol. 2017;183:11–16. doi:10.1016/j.ajo.2017.08.015
2. McAnena L, O’Keefe M. Corneal collagen crosslinking in children with keratoconus. J Aapos. 2015;19(3):228–232. doi:10.1016/j.jaapos.2015.02.010
3. Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42(4):297–319.
4. Salman AG. Transepithelial corneal collagen crosslinking for progressive keratoconus in a pediatric age group. J Cataract Refract Surg. 2013;39(8):1164–1170. doi:10.1016/j.jcrs.2013.03.017
5. Rathi VM, Mandathara PS, Vaddavalli PK, Srikanth D, Sangwan VS. Fluid filled scleral contact lens in pediatric patients: challenges and outcome. Cont Lens Anterior Eye. 2012;35(4):189–192. doi:10.1016/j.clae.2012.03.001
6. McAnena L, Doyle F, O’Keefe M. Cross-linking in children with keratoconus: a systematic review and meta-analysis. Acta Ophthalmol. 2017;95(3):229–239. doi:10.1111/aos.13224
7. Kankariya VP, Kymionis GD, Diakonis VF, Yoo SH. Management of pediatric keratoconus - evolving role of corneal collagen cross-linking: an update. Indian J Ophthalmol. 2013;61(8):435–440. doi:10.4103/0301-4738.116070
8. Chatzis N, Hafezi F. Progression of keratoconus and efficacy of pediatric [corrected] corneal collagen cross-linking in children and adolescents. J Refract Surg. 2012;28(11):753–758. doi:10.3928/1081597X-20121011-01
9. El-Khoury S, Abdelmassih Y, Hamade A, et al. Pediatric keratoconus in a tertiary referral center: incidence, presentation, risk factors, and treatment. J Refract Surg. 2016;32(8):534–541. doi:10.3928/1081597X-20160513-01
10. Torres Netto EA, Al-Otaibi WM, Hafezi NL, et al. Prevalence of keratoconus in paediatric patients in Riyadh, Saudi Arabia. Br J Ophthalmol. 2018;102(10):1436–1441. doi:10.1136/bjophthalmol-2017-311391
11. Gorskova EN, Sevost’ianov EN. [Epidemiology of keratoconus in the Urals]. Vestn Oftalmol. 1998;114(4):38–40.
12. Jonas JB, Nangia V, Matin A, Kulkarni M, Bhojwani K. Prevalence and associations of keratoconus in rural maharashtra in central India: the central India eye and medical study. Am J Ophthalmol. 2009;148(5):760–765. doi:10.1016/j.ajo.2009.06.024
13. Kennedy RH, Bourne WM, Dyer JA. A 48-year clinical and epidemiologic study of keratoconus. Am J Ophthalmol. 1986;101(3):267–273.
14. Kaya V, Karakaya M, Utine CA, Albayrak S, Oge OF, Yilmaz OF. Evaluation of the corneal topographic characteristics of keratoconus with orbscan II in patients with and without atopy. Cornea. 2007;26(8):945–948. doi:10.1097/ICO.0b013e3180de1e04
15. Cingu AK, Cinar Y, Turkcu FM, et al. Effects of vernal and allergic conjunctivitis on severity of keratoconus. Int J Ophthalmol. 2013;6(3):370–374. doi:10.3980/j.issn.2222-3959.2013.03.21
16. Naderan M, Rajabi MT, Zarrinbakhsh P, Bakhshi A. Effect of allergic diseases on keratoconus severity. Ocul Immunol Inflamm. 2017;25(3):418–423. doi:10.3109/09273948.2016.1145697
17. Jafri B, Lichter H, Stulting RD. Asymmetric keratoconus attributed to eye rubbing. Cornea. 2004;23(6):560–564.
18. Ridley F. Contact lenses in treatment of keratoconus. Br J Ophthalmol. 1956;40(5):295–304. doi:10.1136/bjo.40.5.295
19. Fecarotta CM, Huang WW. Pediatric genetic disease of the cornea. J Pediatr Genet. 2014;3(4):195–207. doi:10.3233/PGE-14102
20. Wisse RP, Kuiper JJ, Gans R, Imhof S, Radstake TR, Van der Lelij A. Cytokine expression in keratoconus and its corneal microenvironment: a systematic review. Ocul Surf. 2015;13(4):272–283. doi:10.1016/j.jtos.2015.04.006
21. Lema I, Duran JA. Inflammatory molecules in the tears of patients with keratoconus. Ophthalmology. 2005;112(4):654–659. doi:10.1016/j.ophtha.2004.11.050
22. Naderan M, Rajabi MT, Zarrinbakhsh P, Farjadnia M. Is keratoconus more severe in pediatric population? Int Ophthalmol. 2017;37(5):1169–1173.
23. Alio JL, Vega-Estrada A, Sanz P, et al. Corneal morphologic characteristics in patients with down syndrome. JAMA Ophthalmol. 2018;136(9):971–978. doi:10.1001/jamaophthalmol.2018.2373
24. Wang Y, Rabinowitz YS, Rotter JI, Yang H. Genetic epidemiological study of keratoconus: evidence for major gene determination. Am J Med Genet. 2000;93(5):403–409.
25. Perez-Straziota C, Gaster RN, Rabinowitz YS. Corneal cross-linking for pediatric keratcoconus review. Cornea. 2018;37(6):802–809. doi:10.1097/ICO.0000000000001579
26. Sabti S, Tappeiner C, Frueh BE. Corneal cross-linking in a 4-year-old child with keratoconus and down syndrome. Cornea. 2015;34(9):1157–1160. doi:10.1097/ICO.0000000000000491
27. Mukhtar S, Ambati BK. Pediatric keratoconus: a review of the literature. Int Ophthalmol. 2018;38(5):2257–2266. doi:10.1007/s10792-017-0699-8
28. Soeters N, van der Valk R, Tahzib NG. Corneal cross-linking for treatment of progressive keratoconus in various age groups. J Refract Surg. 2014;30(7):454–460. doi:10.3928/1081597X-20140527-03
29. Sahebjada S, Fenwick EK, Xie J, Snibson GR, Daniell MD, Baird PN. Impact of keratoconus in the better eye and the worse eye on vision-related quality of life. Invest Ophthalmol Vis Sci. 2014;55(1):412–416. doi:10.1167/iovs.13-12929
30. Schlegel Z, Lteif Y, Bains HS, Gatinel D. Total, corneal, and internal ocular optical aberrations in patients with keratoconus. J Refract Surg. 2009;25(10 Suppl):S951–7. doi:10.3928/1081597X-20090915-10
31. Al Suhaibani AH, Al-Rajhi AA, Al-Motowa S, Wagoner MD. Inverse relationship between age and severity and sequelae of acute corneal hydrops associated with keratoconus. Br J Ophthalmol. 2007;91(7):984–985. doi:10.1136/bjo.2005.085878
32. Leoni-Mesplie S, Mortemousque B, Touboul D, et al. Scalability and severity of keratoconus in children. Am J Ophthalmol. 2012;154(1):56–62 e1. doi:10.1016/j.ajo.2012.01.025
33. Arora R, Gupta D, Goyal JL, Jain P. Results of corneal collagen cross-linking in pediatric patients. J Refract Surg. 2012;28(11):759–762. doi:10.3928/1081597X-20121011-02
34. Rabinowitz YS, Rasheed K. KISA% index: a quantitative videokeratography algorithm embodying minimal topographic criteria for diagnosing keratoconus. J Cataract Refract Surg. 1999;25(10):1327–1335.
35. Belin MW, Duncan JK. Keratoconus: the ABCD grading system. Klin Monbl Augenheilkd. 2016;233(6):701–707. doi:10.1055/s-0042-100626
36. Belin MW, Ambrosio R. Scheimpflug imaging for keratoconus and ectatic disease. Indian J Ophthalmol. 2013;61(8):401–406. doi:10.4103/0301-4738.116059
37. Reinstein DZ, Gobbe M, Archer TJ, Silverman RH, Coleman DJ. Epithelial, stromal, and total corneal thickness in keratoconus: three-dimensional display with artemis very-high frequency digital ultrasound. J Refract Surg. 2010;26(4):259–271. doi:10.3928/1081597X-20100218-01
38. Li Y, Chamberlain W, Tan O, Brass R, Weiss JL, Huang D. Subclinical keratoconus detection by pattern analysis of corneal and epithelial thickness maps with optical coherence tomography. J Cataract Refract Surg. 2016;42(2):284–295. doi:10.1016/j.jcrs.2015.09.021
39. Iqbal M, Elmassry A, Tawfik A, et al. Analysis of the outcomes of combined cross-linking with intracorneal ring segment implantation for the treatment of pediatric keratoconus. Curr Eye Res. 2019;44(2):125–134. doi:10.1080/02713683.2018.1540706
40. Abreu AC, Malheiro L, Coelho J, et al. Implantation of intracorneal ring segments in pediatric patients: long-term follow-up. Int Med Case Rep J. 2018;11:23–27. doi:10.2147/IMCRJ.S151383
41. De Bernardo M, Cornetta P, Rosa N. Safety and efficacy of sequential intracorneal ring segment implantation and cross-linking in pediatric keratoconus. Am J Ophthalmol. 2017;181:182–183. doi:10.1016/j.ajo.2017.06.039
42. Abdelmassih Y, El-Khoury S, Dirani A, et al. Safety and efficacy of sequential intracorneal ring segment implantation and cross-linking in pediatric keratoconus. Am J Ophthalmol. 2017;178:51–57. doi:10.1016/j.ajo.2017.03.016
43. Raiskup F, Theuring A, Pillunat LE, Spoerl E. Corneal collagen crosslinking with riboflavin and ultraviolet-A light in progressive keratoconus: ten-year results. J Cataract Refract Surg. 2015;41(1):41–46. doi:10.1016/j.jcrs.2014.09.033
44. O’Brart DP, Patel P, Lascaratos G, et al. Corneal cross-linking to halt the progression of keratoconus and corneal ectasia: seven-year follow-up. Am J Ophthalmol. 2015;160(6):1154–1163. doi:10.1016/j.ajo.2015.08.023
45. Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003;135(5):620–627.
46. Rozema JJ, Wouters K, Mathysen DG, Tassignon MJ. Overview of the repeatability, reproducibility, and agreement of the biometry values provided by various ophthalmic devices. Am J Ophthalmol. 2014;158(6):1111–20 e1. doi:10.1016/j.ajo.2014.08.014
47. Hashemi H, Yekta A, Khabazkhoob M. Effect of keratoconus grades on repeatability of keratometry readings: comparison of 5 devices. J Cataract Refract Surg. 2015;41(5):1065–1072. doi:10.1016/j.jcrs.2014.08.043
48. Soeters N, Visser ES, Imhof SM, Tahzib NG. Scleral lens influence on corneal curvature and pachymetry in keratoconus patients. Cont Lens Anterior Eye. 2015;38(4):294–297. doi:10.1016/j.clae.2015.03.006
49. Gomes JA, Tan D, Rapuano CJ, et al. Global consensus on keratoconus and ectatic diseases. Cornea. 2015;34(4):359–369. doi:10.1097/ICO.0000000000000408
50. Godefrooij DA, Soeters N, Imhof SM, Wisse RP. Corneal cross-linking for pediatric keratoconus: long-term results. Cornea. 2016;35(7):954–958. doi:10.1097/ICO.0000000000000819
51. Meiri Z, Keren S, Rosenblatt A, Sarig T, Shenhav L, Varssano D. Efficacy of corneal collagen cross-linking for the treatment of keratoconus: a systematic review and meta-analysis. Cornea. 2016;35(3):417–428. doi:10.1097/ICO.0000000000000723
52. Soeters N, Wisse RP, Godefrooij DA, Imhof SM, Tahzib NG. Transepithelial versus epithelium-off corneal cross-linking for the treatment of progressive keratoconus: a randomized controlled trial. Am J Ophthalmol. 2015;159(5):821–8 e3. doi:10.1016/j.ajo.2015.02.005
53. Zhu Y, Reinach PS, Zhu H, et al. Continuous-light versus pulsed-light accelerated corneal crosslinking with ultraviolet-A and riboflavin. J Cataract Refract Surg. 2018;44(3):382–389. doi:10.1016/j.jcrs.2017.12.028
54. Nordstrom M, Schiller M, Fredriksson A, Behndig A. Refractive improvements and safety with topography-guided corneal crosslinking for keratoconus: 1-year results. Br J Ophthalmol. 2017;101(7):920–925. doi:10.1136/bjophthalmol-2016-309210
55. Vinciguerra P, Albe E, Frueh BE, Trazza S, Epstein D. Two-year corneal cross-linking results in patients younger than 18 years with documented progressive keratoconus. Am J Ophthalmol. 2012;154(3):520–526. doi:10.1016/j.ajo.2012.03.020
56. Bikbova G, Bikbov M. Standard corneal collagen crosslinking versus transepithelial iontophoresis-assisted corneal crosslinking, 24 months follow-up: randomized control trial. Acta Ophthalmol. 2016;94(7):e600–e6. doi:10.1111/aos.13032
57. Shetty R, Nagaraja H, Jayadev C, Pahuja NK, Kurian Kummelil M, Nuijts RM. Accelerated corneal collagen cross-linking in pediatric patients: two-year follow-up results. Biomed Res Int. 2014;2014:894095. doi:10.1155/2014/894095
58. Koller T, Mrochen M, Seiler T. Complication and failure rates after corneal crosslinking. J Cataract Refract Surg. 2009;35(8):1358–1362. doi:10.1016/j.jcrs.2009.03.035
59. Touboul D, Efron N, Smadja D, Praud D, Malet F, Colin J. Corneal confocal microscopy following conventional, transepithelial, and accelerated corneal collagen cross-linking procedures for keratoconus. J Refract Surg. 2012;28(11):769–776. doi:10.3928/1081597X-20121016-01
60. Sinha Roy A, Shetty R, Kummelil MK. Keratoconus: a biomechanical perspective on loss of corneal stiffness. Indian J Ophthalmol. 2013;61(8):392–393. doi:10.4103/0301-4738.116057
61. Shetty R, Vunnava KP, Dhamodaran K, et al. Characterization of corneal epithelial cells in keratoconus. Transl Vis Sci Technol. 2019;8(1):2. doi:10.1167/tvst.8.1.2
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.