Back to Archived Journals » Chronic Wound Care Management and Research » Volume 6
Optimal Management Of Chronic Wounds In Paediatric Junctional Epidermolysis Bullosa Patients
Authors McDonald CR, Plevey K, Petrof G, Martinez AE
Received 18 April 2019
Accepted for publication 5 September 2019
Published 3 October 2019 Volume 2019:6 Pages 99—107
DOI https://doi.org/10.2147/CWCMR.S172193
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Marco Romanelli
CR McDonald, K Plevey, G Petrof, AE Martinez
Paediatric Dermatology, Great Ormond Street Hospital for Children NHS Foundation Trust, London, UK
Correspondence: AE Martinez
Paediatric Dermatology, Great Ormond Street Hospital for Children NHS Foundation Trust London, WC1N 3JH, UK
Tel +207 829 780
Email [email protected]
Abstract: Epidermolysis bullosa (EB) is a group of rare genetic mucocutaneous fragility disorders. Patients with EB can experience blister formation following minor skin trauma, which can progress to chronic wounds. These wounds can be painful and difficult to manage. There are four major types of EB which are defined by the defective protein and the layer within the skin this protein is located. Junctional epidermolysis bullosa (JEB) is caused by mutations within the lamina lucida proteins which are located at the dermoepidermal junction. The prognosis of JEB varies considerably between the different subtypes of JEB, with JEB generalised severe being the most severe, with high mortality within the first 2 years of life. On the opposite end, patients with JEB localised would be expected to have normal life expectancy. In this review, we discuss the management of chronic wounds in paediatric patients with JEB, including suitable wound cleansing, recommended dressings and topical preparations for chronic wound treatments. We include chronic wounds over specific anatomical sites which are frequent in patients with JEB and their recommended management. Important differences between the subtypes of JEB, and specifics on dressings suitable in the neonatal and infancy period are highlighted. Symptom care of wounds in these children, such as pain, infection, pruritus and overgranulation are also addressed. Finally, we highlight the changes to practice which have occurred in recent years and novel treatments which have been trialled and can be considered.
Keywords: junctional epidermolysis bullosa, paediatric JEB, wound management
Introduction
Epidermolysis bullosa (EB) is a group of inherited skin fragility disorders. The 2014 classification of EB separated the condition into four main groups based on the level of cleavage at the dermal/epidermal junction. These four groups are EB simplex, junctional EB (JEB), dystrophic EB and Kindler syndrome. JEB is caused by mutations within the anchoring proteins between the epidermis and dermis. These are laminin 332, collagen XVII, alpha-3 integrin and alpha-6-beta-4 integrin. The subtypes of JEB are: JEB generalised severe (JEB-GS), JEB generalised intermediate (JEB-GI), JEB with pyloric atresia, JEB late onset, JEB with respiratory and renal involvement, JEB localised, JEB inversa and laryngo-onycho-cutaneous (LOC) syndrome.1 The estimated prevalence of all types of JEB is 0.49 per 1 million population and incidence 2.68 per 1 million births.2 For a patient to have JEB, they need to inherit two mutated copies of the affected gene, one from each parent. The parents of an individual with an autosomal recessive condition each carry one copy of the defective gene.2
Within the JEB subgroups, there is a large clinical variance in presenting features, complications and prognosis. JEB-GS is the most severe subtype of JEB and carries a very poor prognosis with survival rarely beyond the first few years of life. Following the diagnosis of JEB-GS, maintaining patient comfort is at the forefront of patient care.3 Early referral and input with the local palliative care team is recommended.4 Neonates and infants with JEB-GS have some specific problems with regards to chronic wounds, which include thickened, dystrophic nails at birth and breakdown of skin within the nappy area. Issues commonly faced in patients with JEB-GI includes chronic would overgranulation and malodour. Scarring alopecia frequently occurs in children with JEB-GI. LOC syndrome is a rare subtype of JEB characterised by nail dystrophy, skin and mucosal granulation tissue, especially in the conjunctiva and larynx. Laryngeal involvement occurs from early infancy, which may result in needing a tracheostomy.5 JEB with pyloric atresia requires early neonatal surgical intervention to correct the pyloric atresia. Neonates with JEB with pyloric atresia often have prolonged hospital stay with high mortality rates.1
In this review, we will discuss the general aspects of chronic wound healing for patients with JEB and the challenges faced for patients with different subtypes of JEB. The conclusions and recommendations listed in this review are from nursing and medical experience at a tertiary paediatric dermatology centre, and review of the literature.
General Wound Management
Wound Cleaning
Regular cleaning of chronic wounds in patients with JEB is required to reduce infection risk, reduce odour and aim to aid wound healing. This can be difficult in patients due to pain and skin fragility.6 Cleaning of wounds is most commonly done with bathing and/or showering. The frequency of bathing/showering varies from patient to patient, the authors' experience is that bathing or bed baths tends to be the preference. Some families have daily bathing or showering, while other patients find this level of frequency difficult to maintain. This may be due to pain on removal of the dressings, and the time required to undertake this task. Some families may opt to bath, or shower based on need, such as odour control. Other families prefer to take a segmental approach to bathing, ie, upper limbs one day and lower limbs another day.7
Octenisan® (Aspen medical) is our recommended product for patients for an antimicrobial body wash, used as a liquid soap in the shower or bath. Its ability to produce some bubbles in a bath makes it popular with the paediatric population, along with its non-sting characteristic. Octenisan® is also available in mitt formulation, which can be effective in removing slough from skin; however, it is not tolerated by all children.8 Other antimicrobial body washes include Dermol 500 lotion (Dermal Laboratories Limited), and Dermol 200 shower gel (Dermal Laboratories Limited). Approximately, two teaspoons of table salt mixed with 1 L of water (creating a 0.9% solution) could be used for soaking fingernails, toes and hands to keep them soft in neonates and small infants.8
The use of bleach bathing in patients with EB has been documented to reduce rates of bacterial infections in patients with atopic dermatitis.9 However, paediatric patients have reported that this can sting when there are open wounds. There are no specific recommendations for paediatric patients with JEB with regards to showering or bathing and is up to patient choice. As with all subtypes of EB, it is recommended that a neonate with JEB is not to be bathed until birth damage is healed. This is to minimise discomfort in early stages of life. From the authors experience, during this time, Polymem® (Ferris) is used as a dressing, this releases surfactant when wet which helps to clean the open wounds. Once initial wounds are healed, many babies and children with JEB enjoy bathing. Analgesia (paracetamol and morphine) can also be given 20 to 30 mins prior to bathing to minimise pain if required.10
Use Of Topical Therapies In JEB
Neonates with JEB commonly present with wounds in areas which are difficult to apply dressings, ie, under arms, groin and back of the head (Figure 1). Dressings may also cause “dragging” on unaffected skin resulting in skin damage. Babies are also at risk of choking on smaller dressings used on fingers and toes, thus there are not recommended. Topical wound gels are widely used among this patient group. Barrier creams, for example Proshield™ Plus, are applied to these difficult to dress areas. Proshield™ Plus contains the active ingredient Dimethicone 1% (0.01g in 1g), with inactive ingredient polyethylene glycol, binders and co-polymer bioadhesive.11 This gives the product a tacky consistency, which is able to stay in place on both moist and dry skin.12
 |
Figure 1 A chronic head wound with significant exudate in a neonate with JEB-GS. |
Alginate gels such as Flaminal® Forte or Hydro help to reduce excessive protease activity, thus speeding up the healing process. Flaminal® Forte is used for moderately to heavily exuding wounds on the skin, whilst Flaminal® hydro can be used for slightly to moderately exuding wounds on finger and toenails.
There are several formulations of honey-based topical gels available for patient use. Honey-based topical gels are widely used in all types of JEB, however not all patients tolerate it due to reported stinging on broken skin. Honey works by the action of osmosis, therefore patients may feel a “drawing sensation” which some children find painful. As such, it is not recommended for extensive application on a neonate or young child and should be done with guidance. Melloxy® wound gel is a mix of 40% honey with ozonated vegetable olive oil, thus providing less of a sting than pure honey formulas. We advise patch testing before applying to large, chronic wounds. Babies with JEB often present with wounds on bony prominences towards end of life, that are painful to dress and/or patients may no longer tolerate extensive dressing changes. Honey-based gels such as Melloxy can be used in this instance. Honey is also effective in controlling odour which can be a particular issue for JEB children.
Topical wound gels (for example Flaminal® or Melloxy®) can be applied with barrier creams in difficult to dress wounds. Polyhexamethylene biguanide-based gels, such as Octenillin® wound gel can be used to loosen coatings on crusted wounds, such as the ears and thickened nails. This preparation also cleanses the wound, which is ideal for patients that find it too painful to bathe. Other formulations include Prontosan® wound irrigation solution (B Braun), Prontosan® wound Gel (B Braun), Prontosan® Gel X (B Braun) and Octenicare® repair crème (Schulke).
Barrier creams are also effectively used under the arms and in the groin to reduce friction in paediatric patients with JEB. Barrier creams are also effectively used on the back of the head and on the tips of the ears. Proshield™ Plus and Medihoney® barrier cream are both safe to use in the neonatal period, and provide protection from urine, faeces and other bodily fluids.
Appropriate removal of dressings is also key to skin integrity. Wet dressings can stick to chronic wounds and disturb the formation of new healthy cell growth if pulled or tugged. All dressings should be removed with appropriate adhesive removers that do not irritate the skin. Appeel and Niltac sting free adhesive removers (SMARs) are suitable for use on fragile JEB skin. Some families also utilise Emollin® 50/50 emollient spray for dressing removal which can also double us as a nappy cleansing ointment and gentle moisturiser.13
The authors experience is in alignment with current best practice and other available literature, that in paediatric patients with JEB use of topical steroid ointment (such as dermovate, prednicarbate, halometasone/triclosan cream) may reduce the chronic wound overgranulation and may aid wound healing. Topical steroids should be used with caution due to systemic absorption. Side effects are seen with using ultra potent steroids along with the development of resistant to betamethasone (Fucidine®/Fucicort®) and dependence on fusidic acid. We do not recommend the use of topical antibiotics unless clinical or proven infection and base this on swab results.14 The authors have extensive experience of chronic wound improvement with a Dermovate NN (GSK) 3–5 days course, which commonly results in reduction in hypergranulation tissue.8
Chronic Wound Dressing
Managing chronic wounds in paediatric patients with JEB is problematic due to the fragility of the skin and the risk of dressings causing further friction and abrasions if not secured correctly. The areas of the bodies with frequent chronic wounds in JEB include the scalp (sometimes resulting in scarring alopecia) and lower legs. Babies with JEB present with wet and overgranulating wounds. In JEB-GS facial, nail bed chronic wounds are common. Wound management principles are universally applicable across all types of EB. Open wounds should be dressed with non-adherent dressings. The dressings aim is to encourage wound healing and prevent open wounds sticking to cloths causing further skin damage.8
Dressings which have been shown to protect EB skin from damage and encourage wound healing include PolyMem® and Intrasite Conformable (Smith & Nephew). These dressings are applied directly to the skin and secured with a small piece of tubular bandage such as Tubifast. The frequency of dressing change depends on the patients’ need/preference, most patients opt for dressing changes to be between daily and up to every 3 days. It is recommended that PolyMem is changed daily or when staining is seen on the outside of the dressing. Patient with JEB can have very wet chronic wounds and Polymem Max® (Aspen Medical) may be required, which is extra absorbent, however there is a risk of this becoming increasing heavy on the fragile skin resulting in further friction. If the weather is hot, Intrasite Conformable will need to be changed more frequently to prevent it from drying out and adhering to the wound. Other dressings which can be used as a secondary layer dressing include Mepilex Lite®, Mepilex Transfer® and Mepilex border lite® (Mölnlycke Healthcare).15
Allevyn Foam dressings (Smith & Nephew) are also suitable for highly exuding wounds and are ideal to use towards the end of life as they can be kept in place for up to 7 days. This promotes comfort during the palliative stage, by limiting dressing changes and avoiding painful interventions.
Specific Wound Management
Chronic Nail And Hand Wounds
Patients of all subtypes of JEB can experience problems with nail bed inflammation, fragility and chronic nail bed wounds. JEB-GS neonates commonly present with thickened, dystrophic nails with periungual swelling at birth (Figure 2). This is not a pathognomonic sign but can aid clinical suspicion while awaiting formal diagnostic testing results.
 |
Figure 2 Right hand of a neonate with JEB-GS with thickened, dystrophic nails with periungual swelling present since birth. |
Nail bed inflammation and breakdown can be very painful and problematic. Recommended management for nailbed wounds begins with adequate analgesia (morphine) and sedatives (midazolam) for symptom management 20 to 30 mins prior to each dressing. Hands and fingers should then be washed in Octenisan or salt water, to help remove sloughy skin from the nail bed and maintain hygiene. A chitosan haemostat dressing (KytoCel, Aspen Medical) can be used if the nail bed is bleeding, this is applied by wrapping a strip of dressing around each nail and securing with transpire tape. KytoCel should be removed in a hand bath, or with adhesive remover spray. Occasionally, chitosan may stick to the nail bed causing distress on removal. An alternative dressing which uses Hydrofiber® technology is Aquacel® Extra™ (ConvaTec), which forms a gel on contact with wound exudate. These nail wounds may remain chronic with loss of nail. The aim of nursing care in this situation is to keep wounds clean and infection free, reduce the level of inflammation, exudate and pain.16 Other dressings which may be considered include Mepitel® One (Möolnlycke Healthcare) or Cuticell® Contact (BSN Medical) with PolyMem® which a useful secondary dressing if the wound is particularly wet. The skin of patients with JEB-GI can be particularly fragile on their hands with trauma from everyday use resulting in chronic wounds (Figure 3). Chronic nailbed fragility is common in patients with LOC syndrome (Figure 4).
 |
Figure 3 Right hand with new and some healing haemorrhagic blisters in a 6-year-old child with JEB-GI. |
 |
Figure 4 Chronic nail bed inflammation in a 6-year-old child with LOC Syndrome. |
Chronic Inguinal And Pubic Wounds
JEB-GS infants can experience extensive breakdown of skin in the nappy area (Figure 5). Hydrogel impregnated gauze, such as Intrasite Conformable can be used on nappy area wounds, along with a barrier product such as Proshield™ Plus. Nappies are further lined to prevent edges rubbing. These dressings should be changed with every wet nappy.8
 |
Figure 5 Chronic nappy wound on an infant with JEB-GS. |
Chronic Facial Wounds
Chronic facial wounds are frequent particularly in children with LOC, starting in infancy and gradually progressing in size during childhood (Figure 6). By 3 years old, this child presented with worsening of an area of granulation tissue on her left lower cheek which rapidly spread in the infraorbital triangle, extending inferiorly past the nasolabial furrow to the angle of the jaw, medially to the philtrum, and superiorly to the infraorbital furrow. She reported pain on the wound being touched, resulting in difficulty cleaning and topical treatment applications. She experienced mild difficulty eating due to the proximity of the lesion to her left lip lateral commissure. The lesion was unresponsiveness to a range of topical treatments. Granulocyte colony-stimulating factorwas administered intravenously over a 6-day period with minimal change. Gradual improvement to the wound was achieved with a 5-day course of dermovate NN and prontonsan wound gel to help remove crusting, then Keragel T then was applied. The lesion has decreased in size but remains problematic.
As previously mentioned, two paediatric patients with JEB-GI had an improvement in chronic facial wounds with long-term use of Infectocortisept® (prednicarbate, halometasone/triclosan cream).14
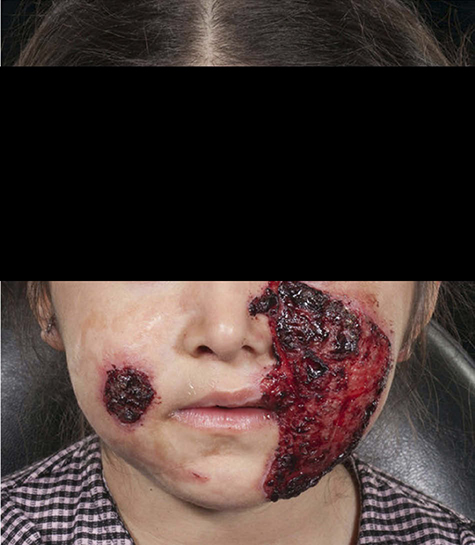 |
Figure 6 Chronic facial wound in a child with LOC syndrome. |
Tracheostomy Management
Management of a tracheostomy requires constant neckties which secure the tracheostomy in place to maintain airway safety. This can result in continued friction and chronic wound formation (Figure 7). The stoma site and the skin below the chin is also at risk of damage from the tracheostomy tube. Once damage and chronic wounds occur at this site, they can be very difficult to manage. Barrier creams and products can help protect this vulnerable area. Dressings commonly used include a lipido-colloid (for example UrgoTul®, UrgoMedical) or a soft silicone mesh (for example Mepitel® or Adaptic Touch™) where wide strips can be used underneath the tracheostomy ties to prevent friction and embedding into the neck of the ties. Allevyn tracheostomy dressing (Smith & Nephew) has non-adherent and absorbent properties work to control excess moisture from secretions. It is important to note that the adherence of these dressings may be too strong for the fragile skin in this area and care to avoid dressing-related damage should be taken. This can be done with the use of adhesive removers during tracheostomy change. As with other subtypes of EB, tracheostomy care in paediatric patients with JEB is recommended under specialist guidance.8
 |
Figure 7 Tracheostomy with a chronic wound around the stoma site in a patient with LOC syndrome. |
Management Of Secondary Chronic Wound Complications
Infection Management And Prevention
As with all subtypes of EB, patients with JEB are managed on a patient by patient basis with regards to infection treatment. Wound cleaning to aid infection prevention is important and can be aided by the use of antiseptics. Parents are encouraged to report any wound changes which may be suggestive of infection. Infection management should be guided by a specialist EB team if infection is suspected. Options include, topical and oral antibiotic treatments. Very rarely if patients are systemically unwell, intravenous antibiotics may be considered after discussion with microbiology. Wound swabs are an important aid to treatment and guide antibiotic use.17 Chronic staphylococcus aureus wound colonisation does not routinely require treatment in patients with JEB.18
Management Of Pruritus In Chronic Wounds
Chronic wound pruritis can be a significant issue for paediatric patients with JEB due to the chronic wounds with excessive granulation tissue.17 This results in a scratch-itch-wound breakdown cycle, difficult for children to break. Antihistamines have limited value in the management of pruritus with all subtypes of EB. However, their sedative value may aid reduction in the urge to scratch, particularly useful at night. If a chronic wound has increased pruritus, exclusion of a wound infection is important.19 Dermacool (Menthol Cream 0.5–1%) or Intrasite Conformable can be used to provide some relief from pruritus. Regular bathing and removal of crusty skin can help manage itch.
Topical polidocanol is a non-ionic surfactant with neuromodulatory anti-pruritic action, local anaesthetic properties and moisturizing effects.20 Topical polidocanol 3% has been found to be safe for paediatric use in drug monitoring survey; however, there are no specific recommendations for its use in paediatric patients with JEB.21 Some subtypes of JEB can have hard, thickened nails, which are particularly abrasive to the skin when the child scratches. Baby mitts can be recommended to help avoid accidental self-inflicted skin trauma by these children secondary to scratching.
Chronic Wound Pain Control
Chronic wound pain control is important in children with JEB. There are no specific measures relating directly to JEB pain management, and each patient is recommended to have a personalised pain management plan. This can often be made in conjunction with the local paediatric symptom care team. Pain assessment in neonates and infants can be challenging and should be frequently reassessed. Pain scores are available but limited in the use of chronic pain.6 Generalised simple steps to minimise wound pain such as ensuring non-adhesive dressings are recommended.22 Pharmacological treatment of wound pain in JEB is non-specific. The NICE guidelines pain ladder is used, paracetamol and NSAIDs are often started early. To optimise pain control, opioids can be carefully introduced to children with JEB. Opioid use can be in both long-acting formulations to provide basal cover and short-acting formulations for use as required for breakthrough pain, commonly prior to dressing changes. It is recommended the use of analgesia 20–30 mins prior to dressing changes to be the most effective.10 Due to the high side effect profile of opioids, which includes potential endocrine changes, constipations, etc., close monitoring of opioid use is required to ensure paediatric patients are on the most appropriate dose.23 Neonatal use of opioids should be introduced under monitoring due to the higher risk of respiratory compromise and reduced clearance.24 The use of oral sucrose in aiding pain control in neonates with JEB for episodes of brief pain should be tried. When patients with JEB become near the end stages of life, oral intake is often very poor. Buccal route for pain medication administration can be more preferable and requires close work with symptom care team.25
Gabapentin has evidence for its use in neuropathic pain. It can be used in children with JEB to provide a basal pain control.26 As with opioids, the dose should be gradually introduced in children. There is some evidence in children that combined therapy of morphine with gabapentin has increased the effectiveness of pain control.27
As with all subtypes of EB, behavioural comfort measures are important factor in managing chronic wound pain in children with JEB. Environmental factors and involving children in their care at a young age can help them to develop a sense of control. Psychological interventions may benefit some children with EB and availability to a paediatric psychologist is recommended.6
Management Of Overgranulation Of Chronic Wounds
Soft silicon mesh dressings have been reported to encourage overgranulation. Topical steroids are helpful for overgranulating wounds as previously discussed, this can be particularly beneficial in the nappy area. Colchicine has been reported to be of benefit in an adult patient with JEB with reduction of granulation tissue and erythema, however it is not widely used in paediatric patients. The mechanism of wound improvement in patients with EB is not fully understood.28
Nasogastric Tube Placement With Chronic Wound Prevention
In all subtypes of JEB, passage of a nasogastric tube (NGT) is discouraged unless absolutely necessary due to the risk of facial skin trauma.8 In JEB with pyloric atresia, an NGT placement for these neonates is an essential part of early life management while they await surgical management.29 Securing the NGT should be done with non-adhesive tape, such as Mepitac® tape (Mölnlycke Healthcare). When required to change the dressing, it is vital to use a silicone medical adhesive remover to reduce the risk of skin damage.30
Blister Prevention And Management Strategies
Protection of the fragile skin of patients with JEB is important with the primary aim to prevent blister formation + thus remove the problem of wound healing. As with all subtypes of EB, blister formation in a child with JEB are not self-limiting and require lancing to prevent enlargement. Procedure of blister care and lancing are as with all subtypes of EB. With clean washed hands, and the patient positioned correctly, a piece of soft gauze should be used to gently compress the blister to increase tension. An orange or blue hypodermic needle should then be slid through the blister at its lowest point to create an entry and exit point. The needle then carefully removed and gauze used to press down on blister. The needle should be disposed in a sharps bin.31
Novel Therapies
A recent study showed that gentamicin could aid the induction of LAMB3 premature termination codons (nonsense mutation) readthrough and produce functional laminin 332 in JEB. This resulted in synthesis and restoration of laminin 332 assembly and secretion. Topical gentamicin has been used as a treatment option for chronic wounds on an infant with JEB-GS with good response (Figure 8), and can be recommended for JEB patients with nonsense mutations in LAMB3.32 Clinical trials are assessing these effects further (https://clinicaltrials.gov/ct2/show/NCT03526159). When considering topical gentamicin in the paediatric population it is important to consider the side effect profile of this medication and application guidance in an out of licence use.33
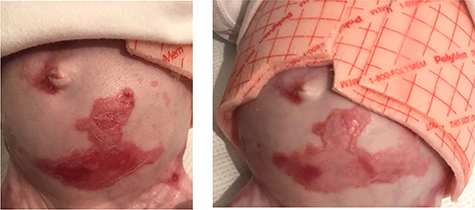 |
Figure 8 Chronic abdominal wound on infant with JEB-GS, demonstrating pre topical gentamicin use (left figure) with improvements after use (right figure). |
The use of cannabinoid (CBD) in paediatric patients with EB is an area of uncertainty. There are no current licenced topical preparations of CBD oils available for use in the UK. A paper indicated that suggested and advertised dermatological use of medical cannabis by dispensaries across USA, Canada and Europe are largely unsubstantiated.34 This may leave parents and patients in difficult with regards to accurate information gathering. Research performed with adults with all subtypes of EB have shown pharmaceutical grade CBD-based medicines can improve pain scores, reduce pruritus and reduce overall analgesic drug intake.35,36 There is no current recommendation for CBD use in paediatric patients with JEB.
Exciting new steps have been made using transgenic stem cells for autologous keratinocyte culture of a functional epidermis which was then transplanted onto a child with JEB.37 This area of research continues to develop providing hope for families bout future applications. There are some reports of the use of allogenic stem cell transplantation (SCT) in paediatric patients with JEB-GS. Patients had a documented initial increase in skin erosions following SCT which then stabilised before deteriorating again. Further research is required to establish safety and efficacy of SCT in this paediatric population.38
Conclusion
Junctional epidermolysis bullosa is one of the most severe subtypes of EB with a wide range in presentation, associated features and severity. Management principles in chronic wounds of paediatric patients with JEB are similar to those in patients with all EB subtypes with some specific features discussed in this article. Wound care recommendations in this article are in line with the 2017 international consensus on best practice guidelines for skin and wound care in epidermolysis bullosa.8 With emerging clinical trials of novel therapies now involving children with JEB advances in wound care are expected but this cannot come soon enough. There is still a desperate need for better ways to manage wounds in junctional and all subtypes of EB.
Acknowledgments
Written email consent for all figures included in this paper has been obtained by the authors.
Disclosure
The authors have no conflict of interest in the writing of this paper.
References
1. Pfendner EG, Lucky AW. Junctional epidermolysis bullosa. In: Adam MP, Ardinger HH, Pagon RA, et al, editors. GeneReviews®. Seattle: University of Washington, Seattle; 1993-2019; 2008 February 22
2. Fine J. Epidemiology of inherited epidermolysis bullosa based on incidence and prevalence estimates from the national epidermolysis bullosa registry. JAMA Dermatol. 2016;152(11):1231–1238. doi:10.1001/jamadermatol.2016.2473
3. Yuen WY, Duipmans JC, Molenbuur B, Herpertz I, Mandema JM, Jonkman MF. Long‐term follow‐up of patients with Herlitz‐type junctional epidermolysis bullosa. Br J Dermatol. 2012;167(2):374–382. doi:10.1111/j.1365-2133.2012.10997.x
4. Laimer M, Lanschuetzer CM, Diem A, Bauer JW. Herlitz junctional epidermolysis bullosa. Dermatol Clin. 2010;28(1):55–60. doi:10.1016/j.det.2009.10.006
5. Cohn HI, Murrell DF. Laryngo-onycho-cutaneous syndrome. Dermatol Clin. 2010;28(1):89–92. doi:10.1016/j.det.2009.10.010
6. Goldschneider KR, Good J, Harrop E, et al. Pain care for patients with epidermolysis bullosa: best care practice guidelines. BMC Med. 2014;12:178. doi:10.1186/s12916-014-00178-2
7. Arbuckle HA. Bathing for individuals with epidermolysis bullosa. Dermatol Clin. 2010;28(2):265–268. doi:10.1016/j.det.2010.01.003
8. Denyer J, Pillay E, Clapham J. Best practice guidelines for skin and wound care in epidermolysis bullosa. An International Consensus. Vienna: Wound International; 2017.
9. Huang T, Abrams M, Tlougan B, Rademaker A, Paller S. Treatment of staphylococcus aureus colonization in atopic dermatitis decreases disease severity. Pediatrics. 2009;123(5):e808–e814. doi:10.1542/peds.2008-2217
10. Junctional epidermolysis bullosa (EB) generalised intermediate type; 2017 February. Available from https://www.gosh.nhs.uk/medical-information/search-medical-conditions/junctional-epidermolysis-bullosa-eb-generalised-intermediate-type. Accessed January 22, 2019.
11. Material safety data sheet proshield Plus; 2014 November 24. Available from: http://www.hrhealthcare.co.uk/product/proshield-plus/. Accessed January 21, 2019.
12. Flynn D, Williams S. Barrier Creams for skin breakdown. Nurs Residential Care. 2011;13:553–558. doi:10.12968/nrec.2011.13.11.553
13. Reimer A, Laszig R, Pfeiffer J, et al. Successful multidisciplinary treatment of chronic facial wounds in junctional epidermolysis bullosa. Acta Derm Venereol. 2018;98(7):711–712. doi:10.2340/00015555-2934
14. King A, Stellar JJ, Blevins A, Shah KN. Dressings and products in pediatric wound care. Adv Wound Care (New Rochelle). 2014;3(4):324–334. doi:10.1089/wound.2013.0477
15. Stevens J. Access to wound dressings for patients living with epidermolysis bullosa — an Australian perspective. Int Wound J. 2014;11(5):505. doi:10.1111/j.1742-481X.2012.01116.x
16. Plevey K. Management of neonates with dystrophic and missing nails in junctional epidermolysis bullosa generalised severe; 2018. Available from: http://program.m-anage.com/ewma2018/en-GB/ProgramSearch/DownloadAbstractOfPresentation/344124. Accessed January 21, 2019.
17. Schober-Flores C. Epidermolysis bullosa: the challenges of a chronic wound. J Dermatol. 2014;6(4):199–205.
18. Van der Kooi-Pol MM, Duipmans JC, Jonkman MF, van Dijl JM. Host-pathogen interactions in epidermolysis bullosa patients colonized with Staphylococcus aureus. Int J Med Microbiol. 2014;304(2):195–203. doi:10.1016/j.ijmm.2013.11.012
19. Danial C, Adeduntan R, Gorell S, et al. Prevalence and characterization of pruritus in epidermolysis bullosa. Pediatr Dermatol. 2015;32(1):53. doi:10.1111/pde.12391
20. Elmariah SB, Lerner EA. Topical therapies for pruritus. Semin Cutan Med Surg. 2011;30(2):118–126. doi:10.1016/j.sder.2011.04.008
21. Freitag G, Höppner T. Results of a postmarketing drug monitoring survey with a polidocanol-urea preparation for dry, itching skin. Curr Med Res Opin. 1997;13(9):529–537. doi:10.1185/03007999709113326
22. Denyer JE. Wound management for children with epidermolysis bullosa. Dermatol Clin. 2010;28:257–264. doi:10.1016/j.det.2010.01.002
23. Katz N, Mazer NA. The impact of opioids on the endocrine system. Clin J Pain. 2009;25(2):170–175. doi:10.1097/AJP.0b013e3181850df6
24. Kart T, Christrup LL, Rasmussen M. Recommended use of morphine in neonates, infants and children based on a literature review: part 1–pharmacokinetics. Paediatr Anaesth. 1997;7(1):5–11.
25. Harrison D, Stevens B, Bueno M, et al. Efficacy of sweet solutions for analgesia in infants between 1 and 12 months of age: a systematic review. Arch Dis Child. 2010;95:406–413. doi:10.1136/adc.2009.174227
26. Chiu YK, Prendiville JS, Bennett SM, Montgomery CJ, Oberlander TF. Pain management of junctional epidermolysis bullosa in an 11-year-old boy. Pediatr Dermatol. 1999;16:465–468. doi:10.1046/j.1525-1470.1999.00120.x
27. De Leeuw TG, Mangiarini L, Lundin R, et al. Gabapentin as add-on to morphine for severe neuropathic or mixed pain in children from age 3 months to 18 years - evaluation of the safety, pharmacokinetics, and efficacy of a new gabapentin liquid formulation: study protocol for a randomized controlled trial. Trials. 2019;20:368.
28. Kim M, Jain S, Harris AG, Murrell DF. Colchicine may assist in reducing granulation tissue in junctional epidermolysis bullosa. Int J Womens Dermatol. 2016;2:56–59. doi:10.1016/j.ijwd.2016.04.001
29. Pfendner EG, Lucky AW. Epidermolysis bullosa with pyloric atresia. In: Pagon RA, Adam MP, Ardinger H, et al, editors. GeneReviews®. University of Washington, Seattle; 1993-2017; 2008 February 22;
30. Denyer J. Reducing pain during the removal of adhesive and adherent products. Br J Nurs. 2011;20(15):S28–S35. doi:10.12968/bjon.2011.20.Sup8.S28
31. Sheehan F. Epidermolysis bullosa (EB): management of the newborn infant with EB; 2017 June. Available from: https://www.gosh.nhs.uk/health-professionals/clinical-guidelines/epidermolysis-bullosa-eb-management-newborn-infant-eb#Blister-care. Accessed January 23, 2019.
32. Lincoln V, Cogan J, Hou Y, et al. Gentamicin induces LAMB3 nonsense mutation readthrough and restores functional laminin 332 in junctional epidermolysis bullosa. Proc Natl Acad Sci. 2018;115(28):E6536–E6545. doi:10.1073/pnas.1803154115
33. Hammersen J, Neuner A, Wild F, Schneider H. Attenuation of severe generalized junctional epidermolysis bullosa by systemic treatment with gentamicin. Dermatology. 2019;235(4):315–322. doi:10.1159/000499906
34. Lim M, Kirchhof MG. Dermatology-related uses of medical cannabis promoted by dispensaries in Canada, Europe, and the United States. J Cutan Med Surg. 2019;23(2):178–184. doi:10.1177/1203475418808761
35. Schräder N, Duipmans J, Molenbuur B, Wolff A, Jonkman M. Combined tetrahydrocannabinol and cannabidiol to treat pain in epidermolysis bullosa: a report of three cases. Br J Dermatol. 2019;180:922–924. doi:10.1111/bjd.17341
36. De Hoop B, Heerdink ER, Hazekamp A. Medicinal cannabis on prescription in the Netherlands: statistics for 2003–2016. Cannabis Cannabinoid Res. 2018;3:54–55. doi:10.1089/can.2017.0059
37. Hirsch T, Rothoeft T, Teig N, et al. Regeneration of the entire human epidermis using transgenic stem cells. Nature. 2017;551(7680):327–332. doi:10.1038/nature24487
38. Hammersen J, Has C, Naumann-Bartsch N, et al. Genotype, clinical course, and therapeutic decision making in 76 infants with severe generalized junctional epidermolysis bullosa. J Invest Dermatol. 2016;136(11):2150–2157. doi:10.1016/j.jid.2016.06.609
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.