Back to Journals » Drug Design, Development and Therapy » Volume 20
Optimal Interval for Intermittent Epidural Bolus with Ropivacaine-Dexmedetomidine Using the Epidural Dural Puncture Technique for Labour Analgesia: A Coin Bias Up-Down Study
Authors Yin QL, Yu B, Yang ZZ, Li HP, Li X, Kong H ![]()
Received 3 November 2025
Accepted for publication 29 January 2026
Published 2 February 2026 Volume 2026:20 576768
DOI https://doi.org/10.2147/DDDT.S576768
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Anastasios Lymperopoulos
Qiao-Li Yin,1,2,* Bin Yu,1,2,* Zi-Zhong Yang,1,2 Hong-Ping Li,1,2 Xue Li,1 Hao Kong1,2
1Department of Anesthesiology, Peking University First Hospital, Beijing, People’s Republic of China; 2Department of Anesthesiology, Peking University First Hospital Ningxia Women and Children’s Hospital, Yinchuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hao Kong, Department of Anesthesiology, Peking University First Hospital, No. 8 Xishiku Street, Beijing, 100034, People’s Republic of China, Tel +86 10 83575138, Fax +86 10 66551057, Email [email protected]; [email protected]
Purpose: This study aimed to establish the 90% effective interval time for programmed intermittent epidural bolus (PIEB) following dural puncture epidural (DPE) analgesia with a dexmedetomidine ropivacaine combination for primiparas in the first stage of labor.
Patients and Methods: This biased coin up and down sequential allocation trial enrolled 40 nulliparous women requesting labor analgesia. After an initial loading dose, analgesia was maintained with PIEB of a fixed volume of 8 mL of the same solution, starting 1 hour later. The initial PIEB interval was set at 60 minutes for the first patient and subsequently adjusted by ± 5 minutes based on the outcome of the previous patient, following the biased-coin design. A successful interval was defined as no requirement for supplemental analgesia. The primary outcome was the 90% effective PIEB interval (ED90) for the first stage of labor. Secondary outcomes included patient satisfaction, the incidence of motor and sensory block, and adverse events.
Results: Isotonic regression analysis estimated the 90% effective PIEB interval as 34.5 min (95% confidence interval: 31.0– 37.0 min). All patients reported a very high level of satisfaction. The incidence of motor block was 10%, while 37.5% of patients achieved the highest sensory block at the T6 level or above. Notably, no cases of excessive sedation, hypotension, or bradycardia.
Conclusion: For DPE labor analgesia using 8 mL of 0.075% ropivacaine combined with 0.4 μg/mL dexmedetomidine, the optimal PIEB interval is approximately 35 min. This interval can reduce breakthrough pain and the need for rescue analgesia. This finding provides a practical, evidence-based reference for optimizing PIEB regimens in clinical labor analgesia, contributing to improved maternal comfort and labor experience while ensuring safety.
Keywords: labor analgesia, dexmedetomidine, programmed intermittent epidural bolus, dural puncture epidural, time interval
Introduction
Labor analgesia is typically accomplished via epidural administration of local anesthetics. Though effective for pain relief, these agents may cause adverse effects like hypotension and motor block at high doses. Hence, opioids such as fentanyl and sufentanil are often added as adjuvants to reduce the required local anesthetic dose while ensuring adequate analgesia.1 Nevertheless, due to the side effects associated with opioid adjuvants,2 non-opioid alternatives are gaining greater significance. In recent years, there have been an increasing number of reports on the use of dexmedetomidine in neuraxial labor analgesia.3–5 A randomised controlled trial by Zhang et al4 has shown that dexmedetomidine is superior to sufentanil in analgesic effect and duration in first-stage labor during epidural analgesia when combined with ropivacaine without an increase in side effects in both parturients and neonates. A meta analysis included 17 randomised controlled trials that demonstrated, compared with the control group (ropivacaine alone or ropivacaine combined with sufentanil), parturients treated with epidural ropivacaine and dexmedetomidine had better analgesic and sedative effects without a rise in motor block, neonatal asphyxia, or hypoxia.4
The dural puncture epidural (DPE) and programmed intermittent epidural bolus (PIEB) techniques are two novel techniques recently applied in labor analgesia.6,7 The DPE technique involves performing a dural puncture with a spinal needle after successful epidural needle placement, without injecting medication into the subarachnoid space. The spinal needle is then withdrawn, and an epidural catheter is placed in the epidural space for drug administration to achieve labor analgesia. Compared to conventional epidural labor analgesia, the DPE technique provides faster onset of analgesia, reduced incidence of unilateral or patchy sensory blockade, and improved sacral spread;6,8 compared with combined spinal and epidural analgesia, DPE had a significantly lower incidence of pruritus, hypotension, combined uterine tachysystole and hypertonus, and physician top-up intervention and prolonged deceleration.8,9 PIEB refers to the bolus administration of epidural solution at scheduled time intervals. In comparison to continuous epidural infusion with or without patient-controlled epidural analgesia (PCEA), PIEB has been associated with lower pain scores, reduced requirements for rescue analgesia, and higher maternal satisfaction.10 Prior research indicated that combining the DPE technique with the PIEB mode yielded better labor analgesia without increasing adverse maternal or neonatal outcomes.7 PIEB parameter setup involves multiple factors, including the type and concentration of drugs, bolus volume, interval time, and PCEA bolus dose. Among these, interval time is considered a critical parameter in PIEB settings. An appropriate bolus interval can help prevent breakthrough pain, maintain stable analgesia, reduce motor block, and minimize the need for clinician interventions.11,12 Currently, there is significant variability in PIEB settings across different studies, with bolus volumes ranging from 5 to 15 mL, drug concentrations varying widely, and adjuvants including both opioids and non-opioids, leading to PIEB intervals spanning from 30 to 60 minutes.12–15 This lack of standardization highlights the need for targeted dose-finding studies.
Dexmedetomidine, as a highly selective α2-adrenergic agonist, has a longer analgesic duration and fewer respiratory depressive effects compared to traditional opioids.3,4 Its unique pharmacokinetic profile, including slow absorption and sustained action in the epidural space, may influence the optimal PIEB timing by maintaining stable analgesic concentrations for a longer period.16,17 However, the optimal PIEB interval for DPE with dexmedetomidine combined with ropivacaine remains unclear.
In terms of the study population and labor stage, we focused on primiparas in the first stage of labor because this group typically experiences more intense and prolonged labor pain compared to multiparas, and the first stage of labor is a critical period for analgesia management.6,13 Additionally, pain intensity in the second stage of labor is influenced by multiple factors such as fetal descent and maternal pushing efforts, making it difficult to isolate the effect of PIEB interval. Therefore, focusing on the first stage allows for a more accurate evaluation of the efficacy of the PIEB regimen.
Epidemiological data show that the demand for labor analgesia is increasing globally, with over 70% of primiparas requesting neuraxial analgesia to alleviate labor pain.18 In the local population of Ningxia, China, where this study was conducted, the utilization rate of labor analgesia has also risen to 46.59% in 2024,19 highlighting the urgent need for optimizing analgesic regimens to improve the quality of care. Despite the growing use of DPE and PIEB techniques, there remains a critical knowledge gap in the international literature regarding the optimal PIEB interval when combining DPE with the non-opioid adjuvant dexmedetomidine. Most existing studies have focused on opioid-containing regimens, and the few studies involving dexmedetomidine did not adopt the DPE technique. Therefore, we conducted a dose-finding study using a biased coin sequential allocation design to determine the best PIEB interval for first-stage labor analgesia with DPE in 90% of primiparous women. We hypothesized that the optimal PIEB interval for first-stage labor analgesia using DPE with 8 mL of 0.075% ropivacaine combined with 0.4 μg/mL dexmedetomidine falls within the range of 20 to 60 minutes for 90% of parturients.
Materials and Methods
Study Population
This was a prospective, double blind, sequential allocation trial. The study protocol was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee of Peking University First Hospital Ningxia Women and Children’s Hospital in Yinchuan, China (approval number: KJ-LL-2023-61; approval date: September 21, 2023). The trial was registered in the Chinese Clinical Trial Registry at chictr.org.cn (registration identifier: ChiCTR2300078015) on November 27, 2023. Written informed consent was obtained from all participants. The first patient was enrolled on December 21, 2024. This study adheres to the Consolidated Standards of Reporting Trials (CONSORT) statement.
Participants were recruited from patients admitted for childbirth at Peking University First Hospital Ningxia Women and Children’s Hospital. Inclusion criteria were as follows: (i) Age ≥ 18 years; (ii) American Society of Anesthesiologists (ASA) physical status II–III; (iii) Primiparous women with singleton, full-term, cephalic pregnancy planning vaginal delivery; (iv) Cervical dilation < 5 cm; (v) Request for neuraxial labor analgesia. Exclusion criteria included: (i) Contraindications to neuraxial anesthesia (history of central nervous system infection, spinal or intraspinal diseases, systemic infection, localized skin or soft tissue infection at the puncture site, or coagulation disorders); (ii) Hypertensive disorders of pregnancy; (iii) Body mass index (BMI) ≥ 35 kg/m2; (iv) Use of sedatives within 4 hours before epidural analgesia; (v) Allergy to local anesthetics or dexmedetomidine; (vi) Prenatal bradycardia (heart rate [HR] < 60 beats per minute) or hypotension (systolic blood pressure [SBP] < 90 mmHg). Dropout criteria were: (i) Failed neuraxial labor analgesia; (ii) Accidental dural puncture; (iii) Unilateral blockade; (iv) Catheter misplacement into the subarachnoid space or blood vessel; (v) Catheter dislodgement or occlusion during analgesia; (vi) Voluntary withdrawal by the participant (revocation of informed consent); (vii) Investigator-initiated withdrawal (occurrence of serious complications/comorbidities, severe adverse events, etc).
The unknown distribution of data of the BCUD study prevents the development of rigorous rules to calculate the necessary sample size for the estimation of the effective dose for 90% of the population (ED90). Pace et al20 suggested that including at least 20–40 patients will provide stable estimates of the target dose for the most realistic scenarios. We planned to enroll participants who met the inclusion and exclusion criteria and stopped when 40 patients had completed the study.
Initiation and Maintenance of Labor Analgesia
After establishing peripheral intravenous access, maternal vital signs, including non-invasive blood pressure, HR, and oxygen saturation, were monitored, and fetal HR was recorded during uterine relaxation. After obtaining informed consent, neuraxial analgesia was initiated with the parturient in the right lateral position. After standard antiseptic preparation, epidural puncture was performed at the L3-L4 interspace using a 16-gauge Tuohy needle, with the epidural space identified via the loss-of-resistance technique. Dural puncture was then performed using a 25-gauge Whitacre needle; proper placement was confirmed by free cerebrospinal fluid flow before needle withdrawal. An epidural catheter was inserted 5 cm into the epidural space, followed by administration of a 3 mL test dose containing 1.5% lidocaine with 15 μg epinephrine. After 5 minutes of observation to rule out subarachnoid or intravascular injection, 15 mL of the study solution (0.075% ropivacaine combined with 0.4 μg/mL dexmedetomidine) was administered epidurally to initiate labor analgesia. Patients who achieved adequate analgesia (visual analog scale [VAS] score ≤ 30 mm) within 20 minutes post injection were enrolled in the study.
The epidural maintenance solution consisted of 0.075% ropivacaine combined with 0.4 μg/mL dexmedetomidine. With the PIEB bolus volume fixed at 8 mL, the first programmed bolus was administered 1 hour after completion of the epidural loading dose. Based on the biased coin method, the initial PIEB interval was set at 60 minutes, and subsequently adjusted by ± 5 minutes based on the patient’s response (success or failure) to the interval. PCEA settings were as follows: bolus dose 5 mL, lockout interval 10 minutes, and maximum PCEA dose 30 mL. Participants were instructed to use PCEA only for breakthrough pain (VAS > 30 mm) during labor. Following epidural labor analgesia, the parturient is maintained in the left lateral tilt position. If her SBP drops to ≤ 90 mmHg or decreases by more than 20% from baseline, 6 mg of intravenous ephedrine is administered along with appropriate fluid resuscitation. If maternal HR falls to ≤ 50 beats per minute, 0.2 mg of intravenous atropine is given. In cases of fetal bradycardia, the midwife initiates intrauterine resuscitation measures, including maternal repositioning, rapid intravenous fluid administration, and oxygen supplementation, while notifying the obstetrician for further evaluation to determine if emergency cesarean delivery is necessary to ensure fetal safety.
Biased-Coin Design Up-Down Sequential Method
The biased-coin up-and-down (BCUD) sequential allocation methodology was implemented as follows. The first enrolled parturient received an initial interval setting of 60 minutes. For each subsequent participant, the interval was determined based on the preceding subject’s analgesic response. If the previous parturient analgesia failed, the interval for the next participant was decreased by 5 minutes. If the previous parturient analgesia succeeded, the next participant had either a 1/9 probability of receiving a 5 minute longer interval or an 8/9 probability of maintaining the same interval.
A PIEB regimen with its assigned interval was considered successful if the participant required neither PCEA nor anesthesiologist-administered rescue boluses within 6 hours after the initiation of epidural analgesia or until complete cervical dilation, whichever occurred first. Conversely, the regimen was deemed a failed response if either PCEA use or rescue boluses during this period. If a rescue bolus was needed, a vaginal examination was performed to assess cervical dilation and confirm whether the parturient was in the first or second stage of labor.
Predefined stopping rules were applied. No further interval adjustments were made when either inadequate analgesia persisted at the 20 minute minimum interval or satisfactory analgesia was maintained at the 60 minute maximum interval, until formal BCUD algorithm directed modifications were indicated. Interval assignments were exclusively managed through a customized BCUD program developed in Microsoft Excel 2016 by the study statistician. A designated research assistant, who was the sole individual with software access, programmed the infusion pumps to preserve allocation concealment. Rigorous blinding was maintained by concealing pumps in opaque bags, restricting interval knowledge to the research assistant, and keeping all clinical staff (anesthesiologists, nurses) and participants unaware of interval settings. This design ensured authentic double-blind conditions throughout the trial while permitting responsive interval optimization per the BCUD algorithm. The schematic of the BCUD design employed in this study is presented in Supplemental Figure 1.
Primary and Secondary Outcomes
The primary outcome was the 90% effective PIEB interval (EI90) for labor analgesia in the first stage of labor using DPE analgesia with 8 mL of 0.075% ropivacaine combined with 0.4 μg/mL dexmedetomidine.
Secondary outcomes included: (i) pain intensity, measured by the Visual Analog Scale (VAS, 0–100 mm, with 0 mm indicating no pain and 100 mm representing the worst imaginable pain); (ii) sensory blockade level, evaluated by ice chip with the highest dermatomal level at which cold sensation was lost recorded as the sensory blockade plane; (iii) motor block, assessed using the Modified Bromage score (0 = full flexion of knees and ankles; 1 = partial flexion of knees with full flexion of ankles; 2 = inability to flex knees with partial flexion of ankles; and 3 = inability to flex knees and ankles); (iv) maternal adverse events (hypotension defined as SBP≤ 90 mm Hg or a decrease of > 20% from baseline, bradycardia defined as HR≤ 50 beats per minute, sedation degree assessed using the Ramsay Sedation Scale [RSS], with grading criteria as follows: 1 = anxious, agitated, or restless; 2 = cooperative, oriented, and tranquil alert; 3 = responsive to commands; 4 = asleep but with brisk response to light glabellar tap or loud auditory stimulus; 5 = asleep with sluggish response to light glabellar tap or loud auditory stimulus; 6 = asleep with no response; and excessive sedation, defined as an RSS score > 4, and respiratory depression defined as SpO2< 90% while breathing room air); (v) maternal satisfaction, recorded using a VAS (0–100 mm, where 0 mm indicates complete dissatisfaction and 100 mm indicates complete satisfaction); as well as (vi) neonatal outcomes, included Apgar score at 1 min and 5 min after birth, bradycardia (heart rate continuously below 100 beats per minute for ≥ 1 minute), tachypnea (resting respiratory rate continuously exceeding 60 breaths per minute), respiratory depression (meeting any of the following: ① respiratory rate continuously below 30 breaths per minute; ② periodic apnea with a single episode lasting ≥ 20 seconds; ③ irregular respiratory rhythm accompanied by cyanosis and decreased blood oxygen saturation requiring assisted ventilation support), and hypoxemia (transcutaneous oxygen saturation continuously below 90% for ≥ 5 minutes without oxygen inhalation).
Data Collection
Data collection was conducted by trained anaesthesia investigators who were blinded to the study group allocation and research hypotheses, to minimize observer bias. All data were recorded in a standardized case report form (CRF) immediately after collection to ensure accuracy and completeness. For maternal outcomes, assessments were initiated at 20 minutes after the administration of the epidural loading dose, with a second assessment at 60 minutes post-initiation, followed by hourly evaluations thereafter until study completion. Study completion was defined as either 6 hours after the initiation of PIEB or the end of the first stage of labor, whichever occurred first. Maternal vital signs, pain intensity, sensory blockade level, motor block grade, sedation level, and occurrence of adverse events were documented at each time point; maternal satisfaction was recorded after the end of the first stage of labor. For neonatal outcomes, data collection was initiated immediately after delivery. Apgar scores were assessed and recorded at 1 minute and 5 minutes post-birth by a dedicated midwife who was also blinded to the study protocol. Neonatal vital signs were continuously monitored from birth to 4 hours post-delivery, with any adverse reactions documented in detail, including onset time, duration, and intervention measures.
Statistical Analysis
The EI90 was calculated by isotonic regression, and the 95% confidence interval (CI) was obtained with 2000 bootstrapped samples. For continuous variables, the Shapiro–Wilk test was used to assess data normality. Normal distribution data were presented as mean (standard deviation) and were compared using the independent samples t-test. Non-normal distribution data were presented as median (interquartile range) and were compared using the Mann–Whitney U-test. Categorical data were presented as the number of patients (percentage) and were analysed using the χ2 test or Fisher’s test. The statistical software used was R for Windows version 3.4.4 and SPSS for Windows version 24.0 (SPSS Inc., Chicago, Illinois).
Results
A total of 56 patients were assessed between December 2024 and June 2025, with 47 participants recruited. One patient was excluded due to a difficult puncture, and two were excluded for failing to achieve a VAS score of ≤ 30 mm within 20 minutes after completion of the loading dose. One patient was excluded due to a unilateral block, and three patients were excluded as they underwent cesarean delivery before trial completion. Therefore, data from 40 parturients were collected for analysis. The study flow diagram is shown in Figure 1, and demographics and baseline characteristics are presented in Table 1.
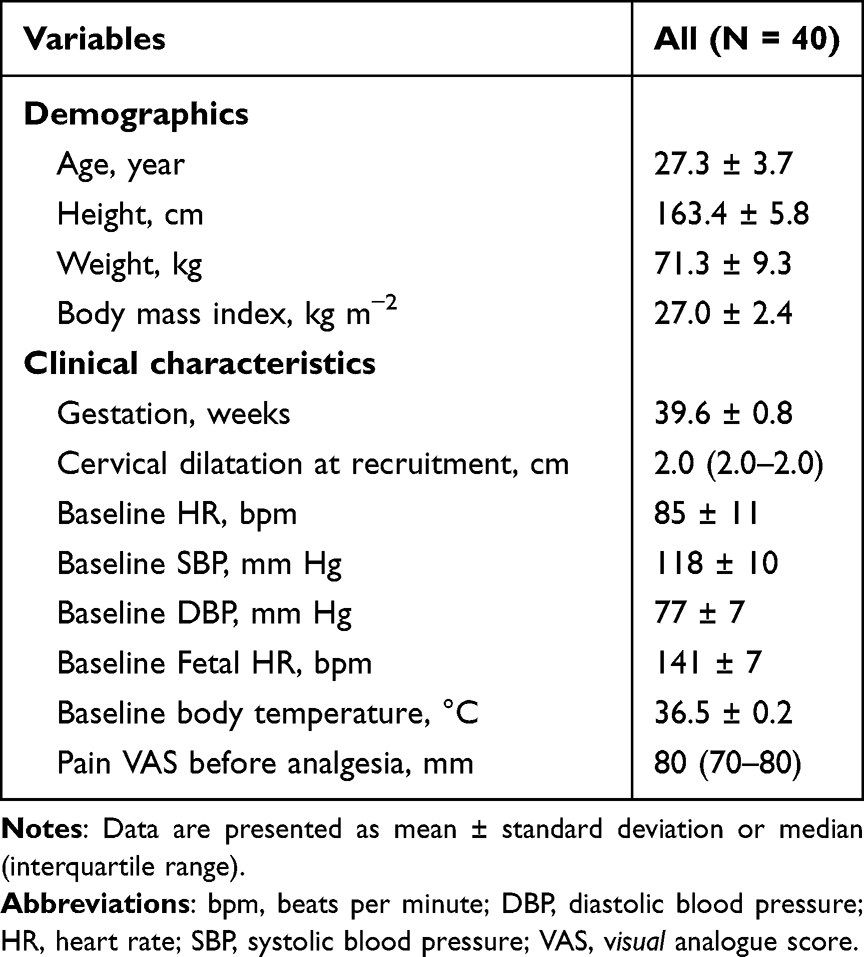 |
Table 1 Demographics and Clinical Characteristics of Maternal Participants |
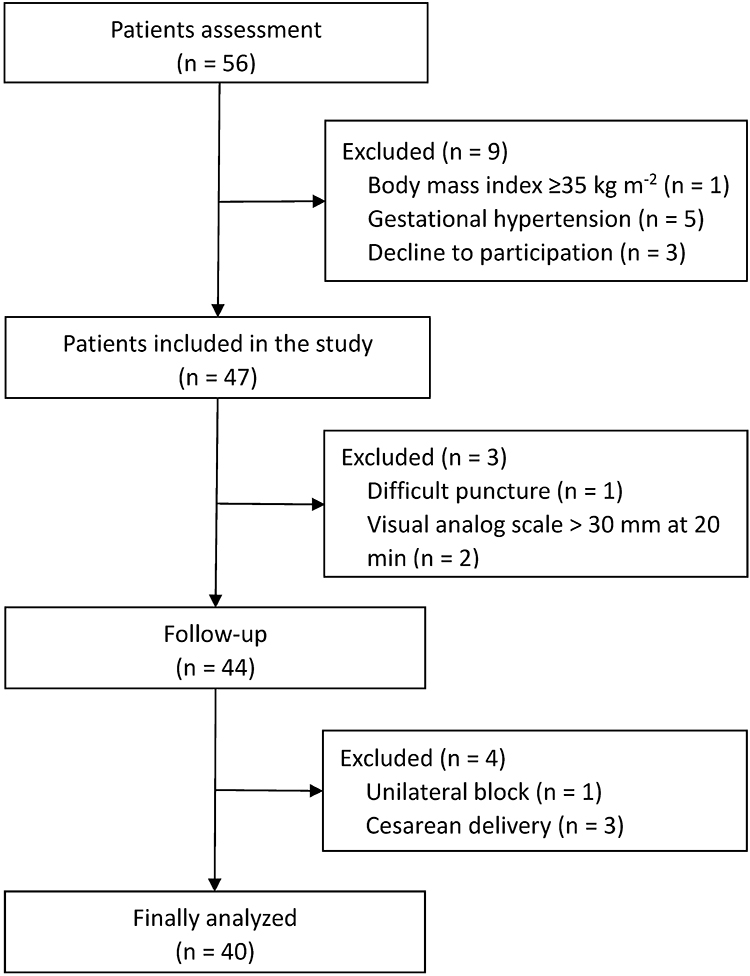 |
Figure 1 Flowchart of the study. |
The allocation sequence of participants and their responses to different PIEB intervals are presented in Figure 2. Isotonic regression analysis estimated the EI90 to be 34.5 minutes (95% CI: 31.0–37.0 minutes).
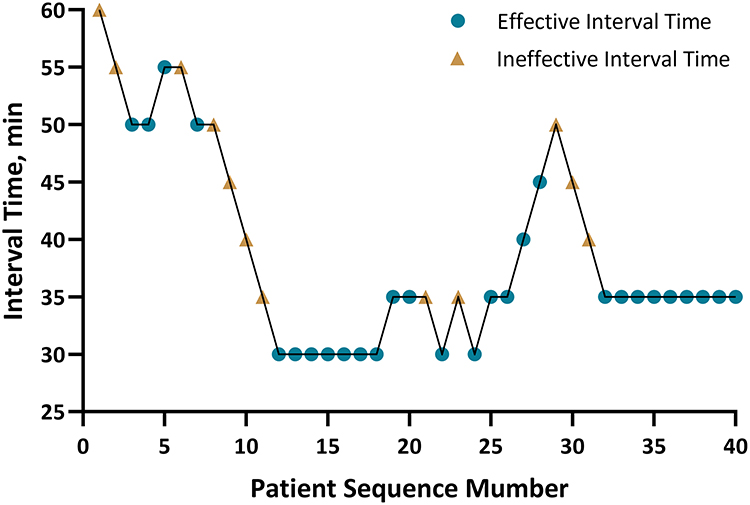 |
Figure 2 Maternal dose-allocation response sequence. |
Figure 3 shows the pain VAS scores and satisfaction VAS scores at baseline before labor analgesia (T0), at 1 hour (T1), 2 hours (T2), 3 hours (T3), 4 hours (T4), 5 hours (T5), and 6 hours (T6) after labor analgesia initiation. Patient satisfaction was uniformly high, with an average score above 92 mm at all time points. The VAS scores for pain of the seven groups are summarized in Table 2.
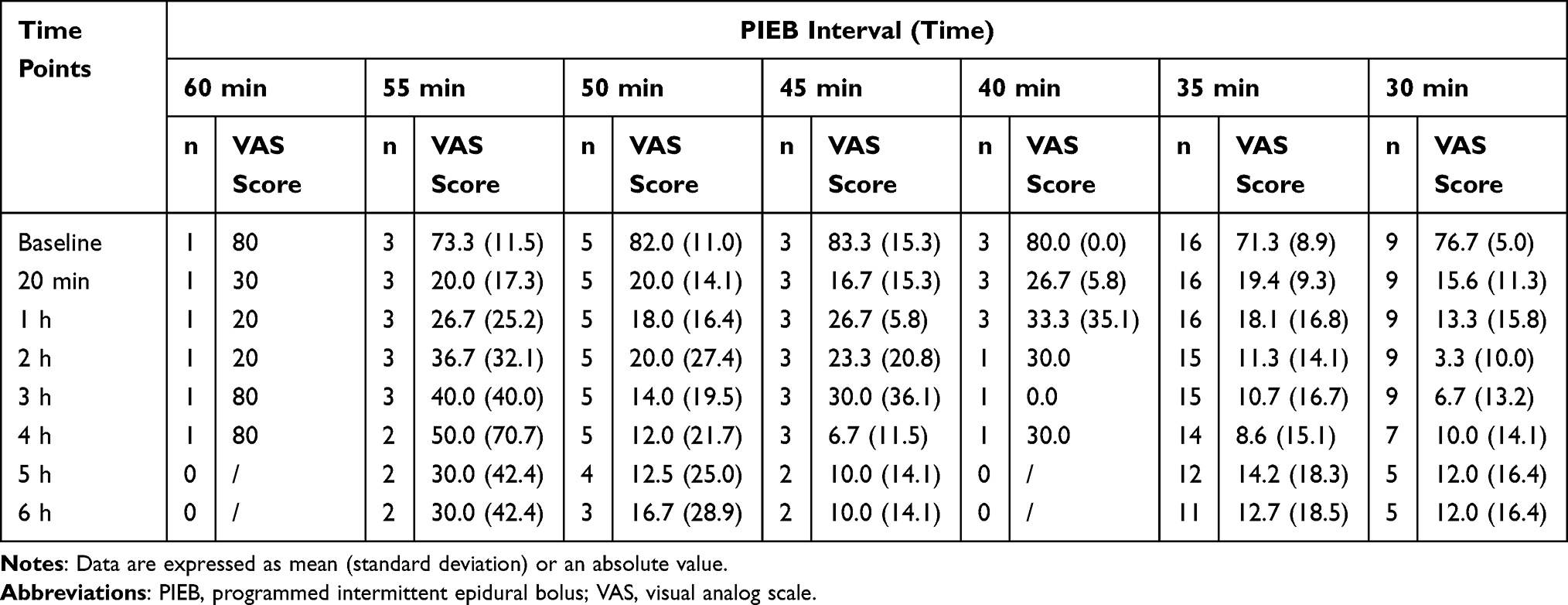 |
Table 2 Pain VAS Score at Various Time Points |
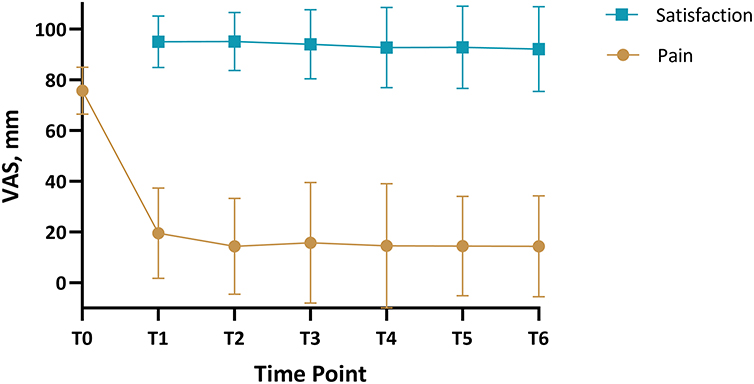 |
Figure 3 Visual analog scale scores for maternal satisfaction and pain. Abbreviations: T0, Before labor analgesia; T1–T6, respectively refer to the 1st to 6th hours after the labor analgesia initiation. |
The response rate for each time interval and the adjusted response rates are presented in Table 3. Patients in the 30 and 35 groups achieved adequate analgesia at rates of 100% and 81.3%, respectively. A total of 12 patients failed to respond to the PIEB regimen: one patient in the 60 group did not achieve adequate analgesia, with the first PCEA request made at 60 minutes; two patients in the 55 group failed to achieve adequate analgesia, with their first PCEA requests at 139 and 30 minutes, respectively; two patients in the 50 group did not achieve adequate analgesia, with first PCEA requests at 50 and 138 minutes, respectively; two patients in the 45 group failed to achieve adequate analgesia, with first PCEA requests at 122 and 120 minutes, respectively; two patients in the 40 group did not achieve adequate analgesia, with first PCEA requests at 30 and 80 minutes, respectively; and three patient in the 35 group failed to achieve adequate analgesia, with the first PCEA request at 58, 60, and 65 minutes. All patients in the 30 group achieved adequate analgesia without requiring a PCEA bolus.
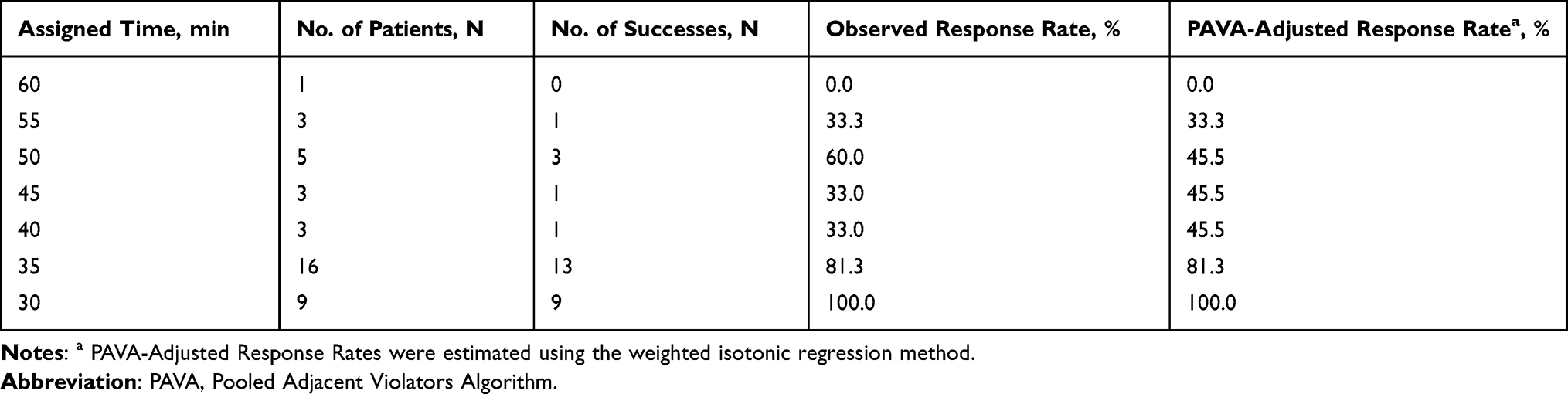 |
Table 3 Observed and Pooled Adjacent Violators Algorithm-Adjusted Response Rates |
Table 4 presents the maternal and neonatal outcomes. For parturients, the outcomes included the motor blockade degree, the highest sensory blockade level, RSS score, incidence of hypotension and bradycardia, and delivery mode for each PIEB interval. In the 35 and 30 groups, one (6.3%) and three (33.3%) patients had a Modified Bromage Score of 1, respectively. The proportions of patients achieving the highest sensory blockade level of T6 were 66.7% (group 30), 37.5% (group 35), 33.3% (group 40), 33.3% (group 45), 20.0% (group 50), and 0.0% (groups 55 and 60). All patients had an RSS score of 2, indicating a calm, cooperative state. No hypotension or bradycardia was observed. Cesarean delivery rates were 11.1% (group 30), 18.7% (group 35), 0% (group 40), 66.7% (group 45), 20% (group 50), 33.3% (group 55), and 0% (group 60). Table 4 also summarizes the 1-min and 5-min Apgar scores of neonates. Specifically, only 1 neonate in group 40 had a 1-min Apgar score of 8, and 1 neonate in the group 35 had a 1-min score of 6; all neonates achieved a 5-min Apgar score of > 8. Although one case of tachypnea and one case of hypoxemia occurred within 4 hours postoperatively, both resolved rapidly without sequelae.
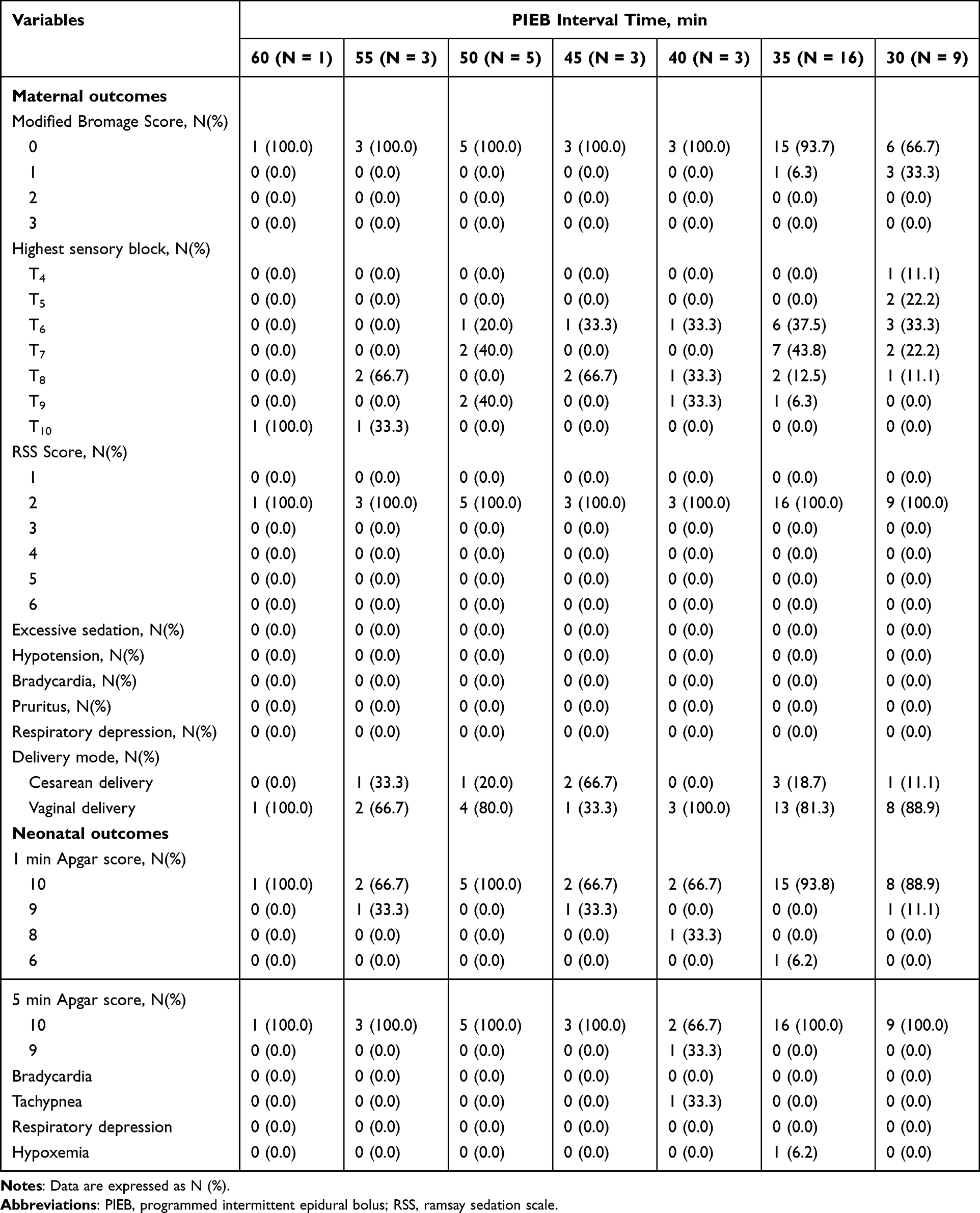 |
Table 4 Maternal and Neonatal Outcomes |
Discussion
In this dose finding study using the biased-coin up-and-down method, we found that when using the DPE technique, the optimum interval time for PIEB between the 8 mL boluses of ropivacaine 0.075% and dexmedetomidine 0.4 μg/mL providing adequate analgesia for 90% nulliparous parturients during the first stage of labor was approximately 35 min. This finding offers a specific, clinically actionable reference for optimizing PIEB parameter setting when combined with the DPE technique, thereby addressing a critical knowledge gap in the use of epidural dexmedetomidine for labor analgesia management.
In recent years, several innovative approaches, such as the DPE and PIEB techniques, along with new non-opioid drugs, have been introduced into clinical practice for labor analgesia. The DPE technique is recognized as a neuraxial analgesia modality with a favorable risk-benefit profile, serving as a viable alternative.6–8 However, the PIEB parameters commonly used in conventional epidural analgesia may not be suitable for the DPE technique. Thus, it is necessary to identify the optimal PIEB interval when combined with the DPE approach. Given the limited data available on PIEB settings specific to the DPE technique, particularly the lack of studies investigating epidural dexmedetomidine administration within this domain, we adopted a fixed 8 mL solution consisting of 0.075% ropivacaine and 0.4 μg/mL dexmedetomidine to investigate the optimal PIEB interval.
Previous studies have explored the optimal concentration of epidural dexmedetomidine for labor analgesia. Ge et al16 found that a low dose of 0.5 μg/mL dexmedetomidine could effectively relieve the labor pain with higher safety and is recommended as the first choice. Liu et al17 demonstrated no additional analgesic benefit of dexmedetomidine greater than 0.4 μg/mL in epidural labor analgesia. Ni et al21 verified the 95% effective dose values for epidural dexmedetomidine combined with 0.075% ropivacaine were 0.357 (0.287 to 0.493) μg/mL. Therefore, a concentration of 0.4 μg/mL dexmedetomidine was used in our study, consistent with the concentration employed in several recent studies.22,23
Previous studies have predominantly focused on identifying optimal PIEB intervals for labor analgesia using opioids combined with ropivacaine. Zhou et al12 determined that the optimal PIEB interval was 39.5 minutes (95% CI 32.5–50.0 minutes) when utilizing 10 mL of 0.08% ropivacaine mixed with 0.3 μg/mL sufentanil for epidural labor analgesia. When using the DEP technique, Song et al13 reported an optimal PIEB interval of approximately 41 minutes with 8 mL of 0.1% ropivacaine combined with 0.3 μg/mL sufentanil, and Yao et al14 found the 95% effective interval of 37.0 (95% CI: 48.4–62.6) minutes with 10 mL of 0.1% ropivacaine and 0.5 μg/mL sufentanil. The hourly ropivacaine consumption in our study was 10.4 mg, which was lower than the 11.7 mg reported by Song et al13 and the 16.2 mg reported by Yao et al.14 Therefore, compared with 0.3 μg/mL sufentanil, 0.4 μg/mL dexmedetomidine can reduce the dosage of ropivacaine. Pang et al24 also demonstrated that epidural dexmedetomidine (0.3 and 0.4 μg/mL) was superior to standard dose epidural fentanyl (2.0 µg/mL) in reducing the mean hourly amount of ropivacaine administered, and minimizing opioid related side effects.
Mei et al15 identified the effective PIEB interval time between boluses of epidural ropivacaine 0.0625% with dexmedetomidine 0.4 μg/mL at a fixed volume of 10 mL in 90% of subjects was 45.4 (95% CI: 35.5–50.5) minutes. The DEP technique was not employed in their study. Compared with our study, their study showed lower hourly consumption of both dexmedetomidine (5.3 μg versus 5.6 μg) and ropivacaine (8.3 mg versus 10.6 mg) than ours. This clearly contradicts the general principle that the epidural drug consumption for parturients using the DPE technique should be lower than that for those not using the DPE technique.7 These contradictory results can be attributed to the following reasons. First, the baseline pain level of parturients before receiving labor analgesia was much lower in Mei et al15 than that in our study and other studies.13,24,25 Second, Mei et al15 calculated the 90% EI using probit regression, whereas ours utilized isotonic regression. Probit regression tends to overestimate EI mainly because its parametric constraints, including the symmetric distribution assumption, cause “over-smoothing” in extreme regions and stray from actual data trends. In contrast, isotonic regression’s nonparametric nature better fits the true dose-effect relationship. Nevertheless, achieving effective analgesia with hourly epidural ropivacaine consumption below 10 mg in PIEB was rarely reported in other labor analgesia research.
In this study, none of the parturients experienced excessive sedation, hypotension, bradycardia, pruritus, or respiratory depression, indicating the safety of the labor analgesia regime. Four parturients had a Modified Bromage Score > 0 in our study. There is currently controversy regarding whether dexmedetomidine may cause lower limb weakness. A study by Jin et al26 found that epidural dexmedetomidine-ropivacaine significantly increased the risk of lower limb weakness compared with sufentanil-ropivacaine (13% vs 1%, P<0.001), whereas Cheng et al,25 Mei et al,15 and Ni et al21 studies reported that epidural dexmedetomidine did not result in a single case of Modified Bromage Score > 0. In our study, 37.5% of patients achieved the highest sensory block at T6 or above, and this incidence fell between the 51.5% reported by Mazda et al27 and the 30.0% reported by Song et al.13 One neonate had a 1-minute Apgar score < 7, while this neonate achieved a 10-point score at 5 minutes. All other neonates had Apgar scores ≥ 8 at both 1 and 5 minutes. Our regimen is safe for neonates.
To translate this finding into hospital protocols, key steps include adopting the 35-minute PIEB interval as the initial setting for eligible nulliparous parturients in the first stage, integrating it with optimized PCEA for individualized rescue dosing, and standardizing pre-PIEB loading doses. Staff education on DPE and dexmedetomidine’s safety will support implementation, reducing workload and improving analgesic stability. Prior research has demonstrated that labor analgesia regimens for multiparas should differ from those for primiparas.28 Future research should validate this interval in multiparas and extend observations to the second and third stages of labor to confirm comprehensive efficacy and safety for broader clinical use.
This study has several limitations to be noted. First, the BCUD method, while optimal for binary outcome-based interval-finding trials, does not support classical statistical power calculations. The stability of the estimated EI90 depended on adequate sequential enrollment (n=40) and minimized outcome variability; however, the lack of power analysis remains an inherent limitation of the BCUD design. Second, the study time frame only allowed assessment of short-term analgesic efficacy (6 hours post-PIEB initiation or end of the first stage of labor), with no long-term follow-up for maternal or neonatal safety outcomes. Short-term neonatal outcomes (eg, Apgar scores) were collected, but long-term neurodevelopmental assessments were not performed. Third, the study population was restricted to nulliparous women with BMI <35 kg/m2, ASA II–III status, and cervical dilation <5 cm at epidural analgesia initiation. This restriction reduced confounding variables but limits the generalisability of findings to multiparous women, obese patients, those with other ASA classifications, or parturients with greater cervical dilation. Fourth, the lack of standardization in labor analgesia drug dosing/volume and variations in anesthetists’ dural puncture practices may have influenced analgesic effects. Although we uniformly used 25-gauge Whitacre needles to mitigate this issue, procedural heterogeneity still introduced potential bias. Fifth, the small sample size (n=40) limited our ability to detect rare adverse events and perform subgroup analyses. While adverse event frequencies were summarized in a dedicated table, larger trials are needed to confirm the safety profile of the dexmedetomidine-ropivacaine combination. Sixth, despite rigorous double-blinding and standardized VAS assessments, participant-reported pain scores may have introduced subjective bias. Finally, it should be noted that epidural dexmedetomidine is considered off-label for labor analgesia in some regions, and clinicians should adhere to local regulatory requirements when using this regimen.
Conclusion
This study demonstrated that the optimal PIEB interval for DPE analgesia with 8 mL of 0.075% ropivacaine plus 0.4 μg/mL dexmedetomidine was approximately 35 min. This interval achieved effective labor analgesia with minimal maternal and neonatal side effects, offering a promising opioid-sparing alternative. Limitations included restricted generalizability to primiparas, negligible motor block favorable for maternal mobility, confirmed short-term dexmedetomidine safety, and a 40-case sample size adequate for EI90 estimation via BCUD design but insufficient for rare adverse event detection, requiring large-sample validation. Globally, this non-opioid regimen addressed opioid-related risks, informed clinical protocols, and provided a precise BCUD design model for similar studies. Future research should verify full-delivery efficacy and optimize PIEB parameters across different drug concentrations,volumes, and combinations.
Abbreviations
ASA, American Society of Anesthesiologists; BCUD, biased-coin up-and-down; BMI, body mass index; CI, confidential interval; DPE, dural puncture epidural; ED90, effective dose for 90% of the population; EI90, effective interval time for 90% of the population; HR, heart rate; PCEA, patient controlled epidural analgesia; PIEB, programmed intermittent epidural bolus; RSS, Ramsay Sedation Scale; SBP, systolic blood pressure; VAS, visual Analog Scale.
Acknowledgments
The authors would like to thank the colleagues from the Department of Anesthesiology and the Department of Obstetrics at Peking University First Hospital Ningxia Women and Children’s Hospital for their assistance in the implementation of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the Natural Science Foundation of Ningxia Hui Autonomous Region (2024AAC03735), the National High-Level Hospital Clinical Research Funding (Interdepartmental Research Project of Peking University First Hospital) (number: 2023IR22), and the Seed funding of Peking University First Hospital Ningxia Women and Children’s Hospital (YJKY-2023-24).
Disclosure
Hao Kong received grants from the Natural Science Foundation of Ningxia Province (2024AAC03735) and the National High-Level Hospital Clinical Research Funding (Interdepartmental Research Project of Peking University First Hospital) (number: 2023IR22). Qiao-Li Yin received grants from the Seed funding of Peking University First Hospital Ningxia Women and Children’s Hospital (YJKY-2023-24). None of the authors has a personal financial interest related to this study.
References
1. Polley LS, Columb MO, Wagner DS, Naughton NN. Dose-dependent reduction of the minimum local analgesic concentration of bupivacaine by sufentanil for epidural analgesia in labor. Anesthesiology. 1998;89(3):626–13. doi:10.1097/00000542-199809000-00011
2. Kuczkowski KM. Respiratory arrest in a parturient following intrathecal administration of fentanyl and bupivacaine as part of a combined spinal-epidural analgesia for labour. Anaesthesia. 2002;57(9):939–940. doi:10.1046/j.1365-2044.2002.279317.x
3. Zhang T, Yu Y, Zhang W, Zhu J. Comparison of dexmedetomidine and sufentanil as adjuvants to local anesthetic for epidural labor analgesia: a randomized controlled trial. Drug Des Devel Ther. 2019;13:1171–1175. doi:10.2147/DDDT.S197431
4. Zhou H, Wen J, Guo G, Zhao Y, Liu W. Evaluation of the effect of dexmedetomidine combined with ropivacaine in epidural labor analgesia: a systematic review and meta-analysis. Minerva Anestesiol. 2022;88(10):842–852. doi:10.23736/S0375-9393.22.16284-X
5. Zhang D, Sun Y, Li J. Application of dexmedetomidine in epidural labor analgesia: a systematic review and meta-analysis on randomized controlled trials. Clin J Pain. 2024;40(1):57–65. doi:10.1097/AJP.0000000000001166
6. Wilson SH, Wolf BJ, Bingham K, et al. Labor analgesia onset with dural puncture epidural versus traditional epidural using a 26-Gauge Whitacre needle and 0.125% bupivacaine bolus: a randomized clinical trial. Anesth Analg. 2018;126(2):545–551. doi:10.1213/ANE.0000000000002129
7. Song Y, Du W, Zhou S, et al. Effect of dural puncture epidural technique combined with programmed intermittent epidural bolus on labor analgesia onset and maintenance: a randomized controlled trial. Anesth Analg. 2021;132(4):971–978. doi:10.1213/ANE.0000000000004768
8. Chau A, Bibbo C, Huang CC, et al. Dural puncture epidural technique improves labor analgesia quality with fewer side effects compared with epidural and combined spinal epidural techniques: a randomized clinical trial. Anesth Analg. 2017;124(2):560–569. doi:10.1213/ANE.0000000000001798
9. Okahara S, Inoue R, Katakura Y, et al. Comparison of the incidence of fetal prolonged deceleration after induction of labor analgesia between dural puncture epidural and combined spinal epidural technique: a pilot study. BMC Pregnancy Childbirth. 2023;23(1):182. doi:10.1186/s12884-023-05473-0
10. George RB, Cobb B, McKenzie C, Riley ET. Implementation of programmed intermittent epidural bolus for the maintenance of labor analgesia. Anesth Analg. 2016;123(4):965–971. doi:10.1213/ANE.0000000000001407
11. Ni F, Wu Z, Zhao P. Programmed intermittent epidural bolus in maintenance of epidural labor analgesia: a literature review. J Anesth. 2023;37(6):945–960. doi:10.1007/s00540-023-03253-w
12. Zhou SQ, Wang J, Du WJ, Song YJ, Xu ZD, Liu ZQ. Optimum interval time of programmed intermittent epidural bolus of ropivacaine 0.08% with sufentanyl 0.3 μg/mL for labor analgesia: a biased-coin up-and-down sequential allocation trial. Chin Med J. 2020;133(5):517–522. doi:10.1097/CM9.0000000000000669
13. Song Y, Du W, Tao Y, et al. Optimum programmed intermittent epidural bolus interval time between 8 mL boluses of Ropivacaine 0.1% with sufentanil 0.3 μg/mL with dural puncture epidural technique for labor analgesia: a biased-coin up-and-down sequential allocation trial. J Clin Anesth. 2022;79:110698. doi:10.1016/j.jclinane.2022.110698
14. Yao HQ, Huang JY, Deng JL, et al. Randomized assessment of the optimal time interval between programmed intermittent epidural boluses when combined with the dural puncture epidural technique for labor analgesia. Anesth Analg. 2023;136(3):532–539. doi:10.1213/ANE.0000000000006201
15. Mei Z, Wang Q, Song S, Lu W, Yu J. Optimum programmed intermittent epidural bolus interval time of ropivacaine 0.0625% with dexmedetomidine 0.4 μg/mL at a fixed volume of 10 mL: a randomized controlled trial. Front Pharmacol. 2024;15:1368222. doi:10.3389/fphar.2024.1368222
16. Ge L, Zhang P, Kong L, et al. Comparison of efficacy and safety of different doses of dexmedetomidine for epidural labor analgesia. Emerg Med Int. 2023;2023:2358888. doi:10.1155/2023/2358888
17. Liu L, Drzymalski D, Xu W, Zhang W, Wang L, Xiao F. Dose dependent reduction in median effective concentration (EC50) of ropivacaine with adjuvant dexmedetomidine in labor epidural analgesia: an up-down sequential allocation study. J Clin Anesth. 2021;68:110115. doi:10.1016/j.jclinane.2020.110115
18. Vaajala M, Kekki M, Mattila VM, Kuitunen I. Fear of childbirth and use of labor analgesia: a nationwide register-based analysis in Finland. Int J Gynaecol Obstet. 2023;162(3):945–949. doi:10.1002/ijgo.14781
19. Wang W, Wang Z, Sun S, Zhang L. Investigation and analysis of the current status of labor analgesia in Medical Institutions in Ningxia. Ningxia Med Univ. 2025:956–961. [In Chinese]. doi:10.16050/j.cnki.issn1674-6309.2025.09.015
20. Pace NL, Stylianou MP. Advances in and limitations of up-and-down methodology: a précis of clinical use, study design, and dose estimation in anesthesia research. Anesthesiology. 2007;107(1):144–152. doi:10.1097/01.anes.0000267514.42592.2a
21. Ni JX, Feng JL, Yao SJ, et al. Determination of the dose-response relationship of epidural dexmedetomidine combined with ropivacaine for labor analgesia. Drug Des Devel Ther. 2022;16:609–618. doi:10.2147/DDDT.S346842
22. Yin J, Cao S, Lei J, et al. Dose-response of epidural ropivacaine with 0.4 μg mL-1 of dexmedetomidine for labor analgesia: a prospective double-blinded study. Medicine. 2024;103(38):e39654. doi:10.1097/MD.0000000000039654
23. Shen YH, Drzymalski DM, Zhu BX, et al. A randomized double-blinded study assessing the dose-response of ropivacaine with dexmedetomidine for maintenance of labor with epidural analgesia in nulliparous parturients. Front Pharmacol. 2023;14:1205301. doi:10.3389/fphar.2023.1205301
24. Pang RY, Shen YH, Jin XQ, et al. Comparison of epidural dexmedetomidine to fentanyl in reducing ropivacaine dose in programmed intermittent epidural bolus plus patient controlled epidural analgesia during labor: a randomized, double-blind, controlled study. Front Med Lausanne. 2022;9:935643. doi:10.3389/fmed.2022.935643
25. Cheng Q, Bi X, Zhang W, Lu Y, Tian H. Dexmedetomidine versus sufentanil with high- or low-concentration ropivacaine for labor epidural analgesia: a randomized trial. J Obstet Gynaecol Res. 2019;45:2193–2201. doi:10.1111/jog.14104
26. Jin KX, Deng CM, Ding T, Qu Y, Wang DX. Impact of dexmedetomidine-ropivacaine versus sufentanil-ropivacaine combination for epidural labour analgesia on neonatal outcomes: a pilot randomised clinical trial. BMJ Open. 2024;14(12):e090208. doi:10.1136/bmjopen-2024-090208
27. Mazda Y, Arzola C, Downey K, Ye XY, Carvalho JCA. Programmed intermittent epidural bolus for labour analgesia: a randomized controlled trial comparing bolus delivery speeds of 125 mL·hr-1 versus 250 mL·hr-1. Can J Anaesth. 2022;69(1):86–96. [English]. doi:10.1007/s12630-021-02132-w
28. Peng Q, Yang Z, Zhang W, Wu X. Comparison of median effective concentration of ropivacaine in multiparas or primiparas during epidural labor analgesia: STROBE compliant. Medicine. 2020;99(1):e18673. doi:10.1097/MD.0000000000018673
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.