Back to Journals » Journal of Pain Research » Volume 10
Optimal control of reaching is disturbed in complex regional pain syndrome: a single-case study
Authors Osumi M, Sumitani M, Kumagaya S, Morioka S ![]()
Received 3 August 2016
Accepted for publication 15 November 2016
Published 12 January 2017 Volume 2017:10 Pages 167—173
DOI https://doi.org/10.2147/JPR.S118846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Micheal Schatman
Michihiro Osumi,1 Masahiko Sumitani,2 Shin-ichiro Kumagaya,3 Shu Morioka1
1Neurorehabilitation Research Center, Kio University, Nara, 2Department of Pain and Palliative Medicine, The University of Tokyo Hospital, 3Research Center for Advanced Science and Technology, The University of Tokyo, Tokyo, Japan
Objective: Disturbance of goal-directed motor control may cause or exacerbate pathological pain in patients with complex regional pain syndrome (CRPS). We conducted a single-case study about motor control involved in reaching with a patient with CRPS in an upper limb.
Methods: Using a three-dimensional measurement system, we recorded reaching movement trajectories of the intact and affected hand before and after pain alleviation by therapeutic nerve blockade. We assessed degrees of tremor in the acceleration phase (from start until maximum peak velocity) and the deceleration phase (from maximum peak velocity until goal). To quantify the smoothness of reaching movements, we analyzed the curves of the trajectories during the initial movement phase (from start and maximum peak acceleration).
Results: The results showed that the tremor of the affected hand was greater than that of the intact hand during the deceleration phase, both before and after pain alleviation. Reaching trajectories of the intact hand smoothly traced curves convexed toward the intact side, while those of the affected hand represented unnaturally rectilinear functions associated with the loss of smooth movements. Further, these unnatural trajectories partially recovered after pain alleviation.
Conclusion: Disturbance of sensorimotor integration and pain-related fear might affect goal-directed motor control in CRPS patients.
Keywords: reaching movement, complex regional pain syndrome, sensorimotor integration, motor control
Introduction
Goal-directed reaching movements involve representative sensorimotor control, planning, and execution, both sequentially and cyclically. Throughout these processes, the trajectory of smooth reaching movement is generally not straight but curved, as observed in previous studies.1,2 A precise curve trajectory is necessary to minimize jerk,3 torque change,4 variance,5 interaction torques,6 and combinations of these.7 Movement disorders such as Parkinson’s disease and cerebellar ataxia disturb goal-directed reaching movement.8,9 Acute experimental pain in healthy subjects has also been found to disturb goal-directed reaching movement.10,11 However, few studies have investigated reaching control in patients with chronic pain in an upper limb. Complex regional pain syndrome (CRPS) type 1 is one of the strongest examples of chronic pain in a limb.12 CRPS is usually preceded by a trauma and is characterized not only by pain but also by sensory dysfunction (i.e., decreased tactile and proprioceptive sensitivity), motor disturbances such as dystonia and decreased maximal force, and mental disorders (e.g., fear of movements, depression, and anxiety).12,13 Although a previous kinematic analysis of CRPS patients revealed signs of tremor,14 the degree of smooth or efficient reaching movement has not been yet analyzed in detail. The lateral curve of trajectories can modulate the execution of smooth and efficient goal-directed movements. Thus, in the present study, we focused on lateral curve trajectories in addition to tremor in a CRPS patient.
Case report
The patient was a 46-year-old female who had undergone a partial mastectomy and a sentinel lymph node biopsy for right breast cancer 1 year prior to the present experiment. After the surgical wound had healed, she continued to experience pain and numbness in the right upper limb. One year after surgery, diffuse muscle weakness and bradykinesia were still observed in the right upper limb, and edema and decreased range of joint motion had emerged in her right hand. Her clinical symptoms met the diagnostic criteria for CRPS15 without neurological deficit, and as she did not exhibit signs of overt nerve injury in the limb, she was diagnosed with CRPS type 1. She developed an extreme fear of contact between the affected hand and any objects owing to hyperalgesia and allodynia. As a result, she always kept the affected hand in a guarded position. Although her anxiety and fear regarding pain aggravation were treated with pregabalin, she clinically maintained her catastrophic thinking in relation to the present pain experience. Throughout the study period, motor controls were assessed under conditions of pregabalin intake. Therefore, any effects of pregabalin should be canceled out when comparing the present kinematic data. The Ethical Review Board of the Faculty of Medicine, the University of Tokyo, approved this study. We explained the protocol of this study to the patient and obtained a written informed consent to publish the case report.
Materials and methods
Apparatus and procedure
We collected kinematic data from both the intact hand (left hand) and the affected hand (right hand). The participant was comfortably seated in front of a table. Two columnar bars (with a diameter of 5 cm and height of 10 cm and 30 cm, respectively) were placed on the table. The tips of the bars represented the start and goal points, respectively. The start bar was placed 20 cm away from the participant and the goal bar was located 30 cm further from the start bar (i.e., 50 cm away from the participant). Both bars were aligned with the sagittal body-midline axis. The participant was required to first pinch the tip of the start bar with her thumb and index finger, which was oriented in an anteroposterior direction (starting position), and then moved her hand from the start position to reach and pinch the tip of the goal bar (goal position). The participant was asked to repeat this sequential-movement process 10 times at a comfortable pace. We first obtained kinematic data for both the intact and affected hands and then repeated the measurement of kinematic data from the affected hand after inducing a regional intravenous nerve blockade (Bier block: 1% lidocaine at 20 mL for the affected forearm) that alleviated pain. Creating an intravenous nerve blockade using lidocaine is known to be an effective treatment for severe pain, allodynia, and edema.16 This treatment had an immediate analgesic effect on the patient. Using the nerve blockade enabled us to compare motor control between pain and painless conditions and thus ascertain whether pain contributed to abnormal motor control in the affected limb. In order to minimalize the effect of hemostasis during intravenous nerve blockade, kinematic data in pain alleviation condition were measured in about half an hour after the release of tourniquet. The kinematic data comprised reaching trajectories that were captured using a magnetic measurement system with six degrees of freedom (3 SPACE FASTRAK; Polhemus Inc.). This system generated a hemispherical electromagnetic field with a radius of 76 cm, which is sufficiently large to measure upper limb movement. The system measured the three-dimensional position and orientation of sensors that were attached to the tips of the index fingers and thumb and to the lateral epicondylus of the wrist. The location of the sensors in the field was collected at a sampling rate of 40 Hz and the data were stored on a personal computer.
Kinematic analysis
The recorded data were visualized and analyzed using Matlab® (MathWorks, Natick, MA, USA). To analyze the tremor of the limb, we divided the reaching trajectory into two phases: the acceleration phase and the deceleration phase. According to a previous report,14 we defined the acceleration phase as the period starting when the forward velocity of the wrist exceeded 5 cm/s and ending when the velocity of the limb reached a maximum value. The acceleration phase is considered to reflect the feedforward (FF) control of goal-directed limb movement.17–19 The deceleration phase was defined as starting immediately after the acceleration phase and lasting until the velocity fell below 5 cm/s. The deceleration phase is considered to reflect the feedback (FB) control of limb movement.18,20,21 To quantify the degree of tremor in each phase, we generated an arbitrary tremor index by calculating the difference between the length of straight lines connecting successive landmarks (i.e., the three-dimensional start and goal positions) and the real movement trajectory of the hand.
To distinguish efficient limb movements from tremor, we set another time frame, termed the initial movement phase, which started at the first motion and ended at the maximum peak acceleration. In this phase, the smooth circular curve of the trajectory was considered to reflect the simple FF control.19 To analyze this, we measured the area under the curve (AUC) of each trajectory by calculating the root mean square value in the initial movement phase. Further, we measured the angle between the sagittal body-midline axis and the initial direction of the trajectory as a reflection of the naturally curved smoothness of each trajectory. These parameters were averaged in the respective conditions (i.e., the intact limb, and the affected limb before and after pain alleviation).
Statistical analysis
We analyzed the maximum velocity of reaching movements among three conditions and analyzed the tremor index during the acceleration and deceleration phases across the three conditions using the Friedman test. We also used the Friedman test to analyze the averaged AUC and trajectory angle during the initial movement phase. Subsequently, we used the Wilcoxon signed-rank test to compare differences in the maximum velocity, the tremor index, and the efficient limb movement analyses among the three conditions. Bonferroni correction was used for the three conditions and the significance level was set at p < 0.0167. We used SPSS version 20.0 (IBM Corporation, Armonk, NY, USA) for all statistical processes.
Results
Visual inspection of the data indicated that two trials with the affected hand under the pain alleviation condition were not recorded correctly. These two trials were removed from the data set.
Maximum velocity of reaching movement
The time series of the reaching velocity in each condition is demonstrated in Figure 1. The Friedman test demonstrated a significant difference in the maximum velocity among the conditions (χ2 = 14.25, p = 0.001) and the Wilcoxon signed-rank test revealed significant differences between the intact limb (mean 51.89±1.91 cm/s standard deviation) and the affected limb before and after pain alleviation (before: 14.58±1.53 cm/s; after: 17.64±3.72 cm/s, p < 0.02). Further, the maximum velocity of the affected limb after pain alleviation tended to improve compared with that before pain alleviation, but this result did not reach significance (p = 0.069).
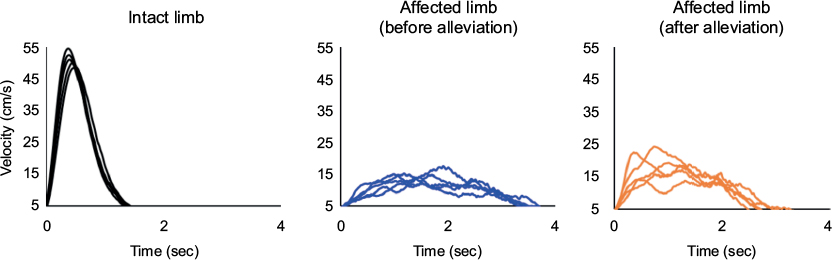 | Figure 1 Time series of goal-directed movement velocity in the intact upper limb (left) and in the affected limb before pain alleviation (middle) and after pain alleviation (right). Bradykinesia was observed in the affected limb (p < 0.017). However, slow reaching movements tended to improve after pain alleviation. |
Tremor index in the acceleration and deceleration phases
During the acceleration phase, the Friedman test demonstrated no significant differences in the tremor indexes among the three conditions (χ2 = 1.00, p = 0.61; Figure 2). However, during the deceleration phase, the Friedman test reached significance (χ2 = 12.25, p = 0.002) and the tremor index of the intact limb was significantly lower than that of the affected hand before and after pain alleviation (Wilcoxon, p < 0.0167; Figure 2).
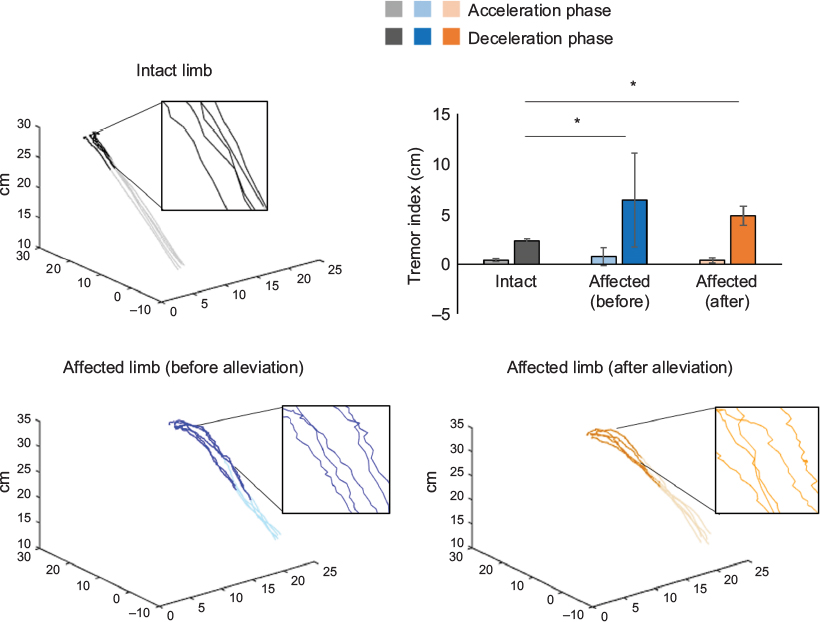 | Figure 2 Examples of goal-directed movement trajectories in the intact upper limb (upper left) and in the affected limb before pain alleviation (lower left) and after pain alleviation (lower right). In the upper right bar graph, light-black, light-blue, and light-orange bars indicate tremor indexes during the acceleration phase in the intact limb and in the affected limb before and after pain alleviation, respectively. Respective dark-colored bars indicate the tremor indexes during the deceleration phase of these three conditions. The tremor indexes during the deceleration phase in the affected limb before and after alleviation were significantly higher than that in the intact limb (*p < 0.017). |
Smoothness of trajectories in the initial movement phase
The Friedman test revealed significant differences in the AUC of trajectories among the conditions (χ2 = 12.25, p = 0.002). Additionally, the AUC of the intact limb was significantly larger than that of the affected limb both before and after pain alleviation (p < 0.016; Figure 3, lower left section). The averaged trajectory direction was significantly different among the conditions (χ2 = 7.75, p = 0.021). The Wilcoxon signed-rank test demonstrated that the trajectory direction of the intact limb was consistently larger than that of the affected limb before pain alleviation (p = 0.0001) but not after pain alleviation (p = 0.119; Figure 3, lower right section).
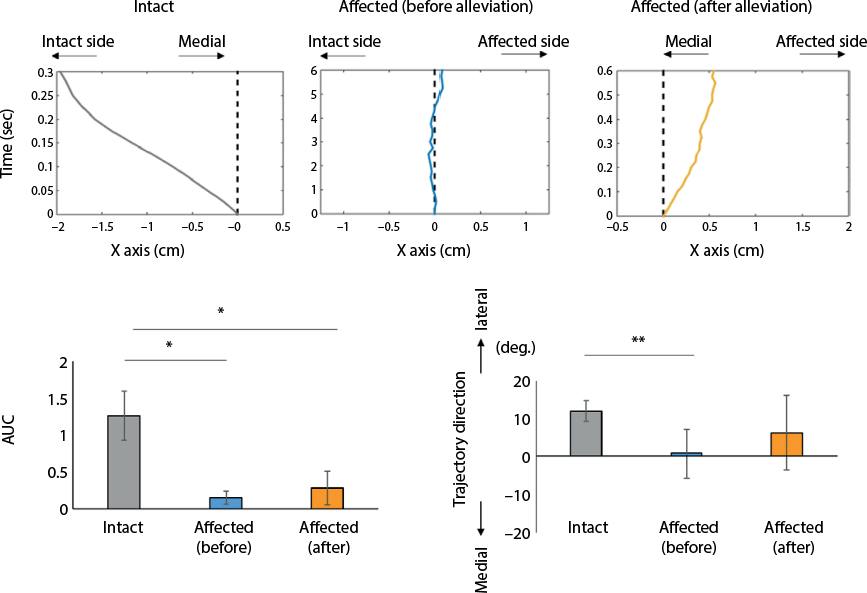 | Figure 3 Examples of goal-directed movement trajectories in the intact upper limb and in the affected limb before and after pain alleviation during the initial movement phase (upper column). The results of area under the curve (AUC) and trajectory direction during the initial movement phase are also shown (lower column). Upper column: The dotted line represents a straight trajectory between the start and goal positions in line with the sagittal body-midline axis. Positive values indicate rightward side (the affected side) and negative values indicate leftward side (the intact side). Lower column: Gray, blue, and orange bars indicate the results for the respective conditions. The AUC of each trajectory was measured by calculating the root mean square value. Trajectory directions in the three conditions are defined as angles between the body-midline axis and the initial movement direction of the intact and affected limbs. *p < 0.017; **p = 0.0001. |
Discussion
In case of our CRPS patient, the velocity of reaching movements performed using the affected limb was slower than that with the intact limb. This reflects bradykinesia in individuals with CRPS, which was reported in a previous study.22 In the present study, we expected that pain or pain-related fear would affect such bradykinesia given the tendency for the velocity to increase after pain alleviation. We mainly used these velocity data to divide reaching movements into those that occurred in the FF versus FB control phases. As a result, visualization of goal-directed movement trajectories of the affected and intact upper limbs revealed that tremor was not prominent in the affected limb during the FF control period compared to the intact limb. However, the trajectory observed during initial movement of the affected limb was rectilinear, unlike the smooth circular-curved trajectory of the intact limb. Immediately after pain alleviation by a neural blockade, the rectilinear initial movement trajectory seemed to partially improve. Further, during FB control of goal-directed movement, tremor of the affected limb was prominent. This did not improve after pain alleviation.
The FF control of goal-directed movement in the affected limb was similar to that in the intact limb. This is compatible with previous reports.14 However, in the more precise initial time frame, the FF control in the affected limb impaired smooth circular-curved trajectories, making them rectilinear instead. Two potential mechanisms may underlie this impairment. First, excessive motor adjustments during FF control would be required to compensate tremor during FB control. Motor control during the FB period might thus be substantially influenced by somatosensory FB context.18,20,21 Capsaicin-induced tonic pain has been found to disrupt proper FB motor controls. Additionally, pain stimulants have been found to interfere with FF control in preparation for movement. This minimizes trajectory corrections in the FB control period.11 Considering that we observed impaired motor control during the FF and FB periods in our participant, pathological pain might first disrupt precise goal-directed movements during the FB control period. The majority of previous reports suggest that CRPS patients have impaired multimodal sensory integration (especially with respect to visual and somatosensory inputs), and movement disorders are also common.23–26 Thus, our participant might have compensated for impaired FB motor control by executing excessive motor adjustments during the FF control period. This notion is supported by a recent pivotal review stated that CRPS patients exhibit a disruption in the sensorimotor loop associated with the affected hand and that visuo-motor rehabilitation strategies can be successful in ameliorating pain and associated movement disorders.27
The other potential mechanism that may explain our results is illustrated by the finding that pain-related fear induces abnormal rectilinear trajectories associated with avoidance of movement-related pain and minimization of the trajectory lengths of goal-directed movements. CRPS patients, like our participant, usually adopt a guarded position with respect to the affected limb and keep it immobilized. When such avoidant behavior is based on fear, a lack of pain increase may reinforce this behavior (classically known as the fear-avoidance model).28 In fact, an anxious personality is considered to be a potential risk factor for developing CRPS.29 Further, operant pain-related fear conditioning can modulate the trajectory pattern of goal-directed movements.30 Therefore, the psychological circumstance of our participant might have contributed to the initial unnatural rectilinear movements. When the neural blockade ameliorated the pain and the related fear, the natural smooth circular-curved movements tended to be restored. This restorative tendency might represent collateral evidence for the effect of pain-related fear on the FF control, but this did not reach statistical significance. We considered not only pain-related fear but also the sensorimotor incongruence of the affected FF control. Our general discussion on this instance of disturbed FF motor control is as follows.
We discussed two explanatory mechanisms for our results: sensorimotor incongruence in the CRPS-affected limb and fear-related abnormal motor control. Following the pain (and fear) alleviation by neural blockade, tremor during the FB control period did not improve. It is possible that deafferentation by local anesthetics disturbs precise FB motor control. An alternative contributing factor might be related to our previous finding that pain alleviation by neural blockade did not normalize but led to over adjustments with respect to visual and somatosensory integration.15 From this view, disturbance of sensorimotor incongruence in the affected limb is still sustained, at least partly, after pain alleviation. Thus, this incomplete sensorimotor integration could subsequently affect FF motor control. Loss of the smooth circular-curved trajectory is a sign of disrupted FF motor control.1,2 This notion could explain why the FF motor control did not recover statistical significance after pain alleviation in our participant. Our present findings indicate that disturbances in both FF and FB motor control in CRPS patients could be explained simply by sensorimotor incongruence. However, the reliability of our conclusion, which was derived from a single patient, should be verified in future studies with larger sample sizes. Overall, taken together with previous studies, our data indicate that visuo-motor rehabilitation strategies should focus on the reestablishment of sensorimotor integration in the affected limb.27,31,32
Limitations and Conclusion
This study has some limitations. First, we sought to clarify the cause of motor abnormality by dividing goal-directed movement into two components (i.e., acceleration and deceleration phase). However, we did clarify the mechanism on the basis of the distorted sensorimotor integration or the pain-related fear. Second, we did not record kinematic data from the intact limb after the nerve block. In the future, we plan to investigate the effect of a nerve block on the intact limb to further clarify the mechanisms of disturbed sensorimotor integration. Despite these limitations, we visualized the distorted sensorimotor integration and pain-related fear in CRPS patients using specific kinematic measures. Thus, our kinematic evaluation strategies might be useful in clarifying these factors in further CRPS patients.
Acknowledgments
This study was supported by a grant from Grants-in-Aid for Scientific Research on Innovative Areas “Constructive Developmental Science”, a Grant-in-Aid for Young Scientists (B), and partially by a Health Labour Science Research Grant from the Japanese Ministry of Health, Labour and Welfare (H24-Ganrinsho-ippan-011 and H26-Kakushintekigan-ippan-060).
Disclosure
The authors report no conflicts of interest in this work.
References
Mistry M, Theodorou E, Schaal S, Kawato M. Optimal control of reaching includes kinematic constraints. J Neurophysiol. 2013;110(1):1–11. | ||
Izawa J, Rane T, Donchin O, Shadmehr R. Motor adaptation as a process of reoptimization. J Neurosci. 2008;28(11):2883–2891. | ||
Flash T, Hogan N. The coordination of arm movements: an experimentally confirmed mathematical model. J Neurosci. 1985;5(7): | ||
Uno Y. Kawato M. Suzuki R. Formation and control of optimal trajectory in human multijoint arm movement. Minimum torque-change model. Biol Cybern. 1989;61(2):89–101. | ||
Harris CM, Wolpert DM. Signal-dependent noise determines motor planning. Nature. 1998;394(6695):780–784. | ||
Goble JA, Zhang Y, Shimansky Y, Sharma S, Dounskaia NV. Directional biases reveal utilization of arm’s biomechanical properties for optimization of motor behavior. J Neurophysiol. 2007;98(3):1240–1252. | ||
Ohta K, Svinin MM, Luo Z, Hosoe S, Laboissière R. Optimal trajectory formation of constrained human arm reaching movements. Biol Cybern. 2004;91(1):23–36. | ||
Alberts JL, Saling M, Adler CH. Stelmach GE. Disruptions in the reach-to-grasp actions of Parkinson’s patients. Exp Brain Res. 2000;134(3):353–362. | ||
Deuschl G, Wenzelburger R, Löffler K, Raethjen J, Stolze H. Essential tremor and cerebellar dysfunction clinical and kinematic analysis of intention tremor. Brain. 2000;123(Pt 8):1568–1580. | ||
Muceli S, Falla D, Farina D. Reorganization of muscle synergies during multidirectional reaching in the horizontal plane with experimental muscle pain. J Neurophysiol. 2014;111(8):1615–1630. | ||
Lamothe M, Roy JS, Bouffard J, Gagné M, Bouyer LJ, Mercier C. Effect of tonic pain on motor acquisition and retention while learning to reach in a force field. PLoS One. 2014;9(6):e99159. | ||
Birklein F, O’Neill D, Schlereth T. Complex regional pain syndrome: an optimistic perspective. Neurology. 2015;84(1):89–96. | ||
Birklein F, Schlereth T. Complex regional pain syndrome-significant progress in understanding. Pain. 2015;156(Suppl 1):S94–S103. | ||
Maihöfner C, Baron R, DeCol R, et al. The motor system shows adaptive changes in complex regional pain syndrome. Brain. 2007;130(Pt 10): | ||
Sumitani M, Shibata M, Sakaue G, Mashimo T; Japanese Complex Regional Pain Syndrome Research Group. Development of comprehensive diagnostic criteria for complex regional pain syndrome in the Japanese population. Pain. 2010;150(2):243–249. | ||
Schwartzman RJ, Patel M, Grothusen JR, Alexander GM. Efficacy of 5-day continuous lidocaine infusion for the treatment of refractory complex regional pain syndrome. Pain Med. 2009;10(2):401–412. | ||
Jeannerod M, editor. Attention and Performance XIII: Motor Representation and Control. Hillsdale, NJ: Laurence Erlbaum Associates; 1990. | ||
Desmurget M, Grafton S. Forward modeling allows feedback control for fast reaching movements. Trends Cogn Sci. 2000;4(11):423–431. | ||
O’Shea J, Gaveau V, Kandel M, et al. Kinematic markers dissociate error correction from sensorimotor realignment during prism adaptation. Neuropsychologia. 2014;55:15–24. | ||
Gentilucci M, Toni I, Chieffi S, Pavesi G. The role of proprioception in the control of prehension movements: a kinematic study in a peripherally deafferented patient and in normal subjects. Exp Brain Res. 1994;99(3):483–500. | ||
Gentilucci M, Toni I, Daprati E, Gangitano M. Tactile input of the hand and the control of reaching to grasp movements. Exp Brain Res. 1997;114(1):130–137. | ||
Schilder JC, Schouten AC, Perez RS, et al. Motor control in complex regional pain syndrome: a kinematic analysis. Pain. 2012;153(4): | ||
Sumitani M, Shibata M, Iwakura T, et al. Pathologic pain distorts visuospatial perception. Neurology. 2007;68(2):152–154. | ||
Sumitani M, Rossetti Y, Shibata M, et al. Prism adaptation to optical deviation alleviates pathologic pain. Neurology. 2007;68(2):128–133. | ||
Bank PJ, Peper CE, Marinus J, Beek PJ, van Hilten JJ. Motor consequences of experimentally induced limb pain: a systematic review. Eur J Pain. 2013;17(2):145–157. | ||
Bank PJ, Peper CL, Marinus J, Beek PJ, van Hilten JJ. Motor dysfunction of complex regional pain syndrome is related to impaired central processing of proprioceptive information. J Pain. 2013;14(11):1460–1474. | ||
Torta DM, Legrain V, Rossetti Y, Mouraux A. Prisms for pain. Can visuo-motor rehabilitation strategies alleviate chronic pain? Eur J Pain. 2016;20(1):64–69. | ||
Leeuw M, Goossens ME, Linton SJ, Crombez G, Boersma K, Vlaeyen JW. The fear-avoidance model of musculoskeletal pain: current state of scientific evidence. J Behav Med. 2007;30(1):77–94. | ||
Dilek B, Yemez B, Kizil R, et al. Anxious personality is a risk factor for developing complex regional pain syndrome type I. Rheumatol Int. 2012;32(4):915–920. | ||
Meulders A, Franssen M, Fonteyne R, Vlaeyen JW. Acquisition and extinction of operant pain-related avoidance behavior using a 3 degrees-of-freedom robotic arm. Pain. 2016;157(5):1094–1104. | ||
Punt TD, Cooper L, Hey M, Johnson MI. Neglect-like symptoms in complex regional pain syndrome: learned nonuse by another name? Pain. 2013;154(2):200–203. | ||
Gierthmühlen J, Binder A, Baron R. Mechanism-based treatment in complex regional pain syndromes. Nat Rev Neurol. 2014;10(9): |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.