Back to Journals » Patient Preference and Adherence » Volume 15
Optimal Antihypertensive Medication Adherence Reduces the Effect of Ambient Temperature on Intracerebral Hemorrhage Occurrence: A Case-Crossover Study
Authors Wang P ![]() , Luo S
, Luo S ![]() , Cheng S, Li Y, Song W
, Cheng S, Li Y, Song W ![]()
Received 29 September 2021
Accepted for publication 1 November 2021
Published 10 November 2021 Volume 2021:15 Pages 2489—2496
DOI https://doi.org/10.2147/PPA.S341259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Peng Wang,1,* Shuang Luo,1,* Shuwen Cheng,1 Yaxin Li,2 Weizheng Song1
1Department of Neurosurgery, Chengdu Fifth People’s Hospital/Affiliated Chengdu No.5 People’s Hospital of Chengdu University of TCM, Chengdu, People’s Republic of China; 2West China Fourth Hospital/West China School of Public Health, Sichuan University, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Weizheng Song
Department of Neurosurgery, Chengdu Fifth People’s Hospital/Affiliated Chengdu No.5 People’s Hospital of Chengdu University of TCM, Chengdu, 611130, People’s Republic of China
Tel/Fax +86 28 82726171
Email [email protected]
Background and Purpose: The role of antihypertensive medication adherence in reducing the effect of ambient temperature (TEM) on intracerebral hemorrhage (ICH) pathogenesis is unclear. We aimed to study the influence of ambient TEM on the ICH occurrence in hypertensive patients with different medication adherence.
Methods: We enrolled consecutive ICH patients with a definite history of hypertension in a teaching hospital over a period of six years. Medication adherence was calculated using the proportion of prescription days covered (PDC) to antihypertensive mediation in the last month before the ICH attack. Optimal medication adherence (OMA) was the PDC > 80%, and non-optimal medication adherence (non-OMA) was ≤ 80%. Daily ambient TEM and its variation were collected as the explanatory variables, and dominant air pollutants were gathered as covariates. We adopted a time-stratified case-crossover approach to minimize individual confounders. Conditional logistic regression was conducted to calculate the odds ratio (OR) of daily ambient TEM on ICH occurrence.
Results: We recruited a total of 474 patients in this study. The number of participants with OMA and non-OMA was 249 and 225. Daily mean and max TEM in lag0 to lag2, as well as daily min TEM in lag0 to lag1, were significantly related to ICH onset in all enrolled patients and non-OMA cases. However, only daily TEM in lag0 was meaningfully associated with ICH onset in the OMA cases. The risk of ICH in OMA patients, respectively, changed by 7.9% (OR = 0.921, [0.861, 0.985]) or 6.3% (OR = 0.937, [0.882, 0.995]) when daily mean or max TEM was altered by 1°C in lag0, but the change raised by 10.4% (OR = 0.896, [0.836, 0.960]) or 7.5% (OR = 0.925, [0.868, 0.986]) in non-OMA patients. And the risk varied (OR = 0.933, [0.882, 0.988]) only in non-OMA patients when daily min TEM was altered by 1°C in lag1.
Conclusion: Our results indicate that OMA to antihypertensive drugs reduces the influence of ambient TEM on ICH occurrence in hypertensive patients.
Keywords: intracerebral hemorrhage, risk, ambient temperature, medication adherence
Graphical Abstract:

Introduction
Intracerebral hemorrhage (ICH) is the second common subtype of stroke, with an annual incidence rate of 22 per 100,000 in low- and middle-income countries and 10 per 100,000 in high-income countries.1 The ICH patients, usually with severe intracranial pressure,2 have the worst mortality and disability compared with other stroke types.3 Although several personal risk factors contribute to the pathogenesis, the critical individual factor leading to ICH occurrence is unsatisfactory control of hypertension.3,4 A recent report shows that uncontrolled hypertension three months after ICH is associated with recurrent stroke and mortality.5 In addition, the adverse effect of environmental factors, such as ambient temperature (TEM), on ICH occurrence is also greatly concerned. Researches from regions with different climates worldwide confirm a significant negative correlation between ambient TEM and ICH occurrence.6–10 Elaborate precautions against these risk factors in ICH patients are essential to reduce the incidence of the disease.
Currently, antihypertensive medication adherence has been emphasized in several studies to strengthen primary or secondary prevention.11,12 Optimal medication adherence (OMA) helps control blood pressure in patients with hypertension, especially in the absence of new antihypertensive drugs.4 This good adherence reduces the risk of ICH, either in patients with newly prescribed antihypertensive medications or in those who have suffered from hemorrhagic stroke.13,14 However, it is unclear whether OMA to the antihypertensive drug can reduce the biological effect of the change in ambient TEM. In this study, we supposed that optimal adherence to antihypertensive medication diminishes the influence of ambient TEM on ICH occurrence. We adopted a time stratified case-crossover approach to explore correlation intensity between TEM and ICH occurrence in patients with different antihypertensive medication adherence and discussed the underlying reason for the possible difference in correlation intensity.
Methods
Clinical Data
We retrospectively analyzed the clinical data of ICH patients with a definite history of hypertension in a teaching hospital from January 1, 2014, to December 31, 2019. The hospital (east longitude 103.8° and north latitude 30.7°), located in the west of the city, is the nearest large-scale medical center to the national benchmark climate station in Chengdu (straight-line distance = 6.4km). This city has a subtropical monsoon climate, with characteristics of low wind speed, high humidity, and less sunshine all year round. The inclusion criteria required that the ICH patients had a definite history of hypertension and received chronic disease management in our institution more than one month before onset, with at least one prescription record of antihypertensive drugs. Patients were excluded if they fulfilled one of the following four criteria: (1) patients had large vascular diseases such as aneurysms or vascular malformations, (2) or they were outside the city at the time of ICH onset, (3) or the specific time of symptom occurrence was unknown, (4) or the data was missing. The time of ICH onset was determined based on the occurrence of symptoms.
Medication Adherence
Medication adherence refers to the consistency between the patient’s medication and the prescription. It is a process characterized by three major components: the initiation, the implementation, and the discontinuation.4 On the condition that all the enrolled patients in our study had at least one definite prescription record of antihypertensive drugs, we used the proportion of prescription days covered (PDC) by antihypertensive mediation in the last month before ICH onset to represent the 1-month medication adherence. We collected the prescription records of all participants and calculated the PDC to antihypertensive mediation. OMA was PDC>80%, and non-optimal medication adherence (non-OMA) was PDC ≤ 80%.
Meteorological Data and Air Pollutants
Our study collected data of ambient TEM and their fluctuation as explanatory variables. These parameters included daily mean TEM, maximum (max) TEM, minimum (min) TEM, diurnal and day-to-day variation of TEM. The diurnal variation was the difference value between daily max TEM and min TEM. The day-to-day variation was the absolute value of daily mean TEM in the day minus the one in the previous day. Ambient TEM data were from the National Meteorological Data Center (http://data.cma.cn/).
Three dominant air pollutants in the local city, the PM2.5, NO2, and O3, were entered as covariates, considering their impact on ICH onset.15–17 Pollutant data were from the local Ecological and Environment Bureau (http://sthj.chengdu.gov.cn/).
Statistical Analysis
We adopted a time-stratified case-crossover approach in the present study. This design used patients themselves as a control to minimize individual confounders (Figure 1) The risk factors’ exposure degree of participants at the target event occurrence (case days) was investigated, compared with the exposure degree of the same participants at other times (control days). In other words, the participants were in case and control states in different periods. If exposure was related to the event, the frequency of exposure in case days should be higher than that in control days. In this study, the case days were the days of symptom onset (lag0). The control days were the other corresponding days in the same month with seven days as the interval. Data within two days before onset were included to explore the possible lag effect. Lag1 referred to the previous day before lag0, and lag2 referred to the day before Lag1. The choice of lag1 and lag2 in the control days was consistent with that in the case days.
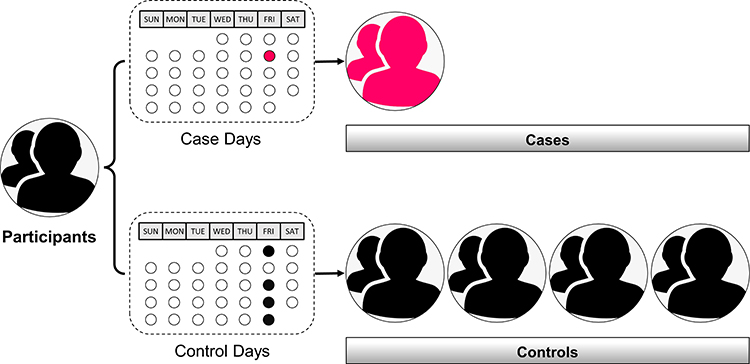 |
Figure 1 A graph illustrates to use of patients as self-control in a time-stratified case-crossover approach. In this study, the case days were the days of symptom onset, and the control days were the other corresponding days in the same month with seven days as the interval. Participants’ exposure to risk factors in case days and control days were compared to judge the correlation between exposure and target event occurrence. |
Numerical variables with normal distributions were expressed as mean (±standard deviation), and numerical variables with non-normal distributions were expressed as median (25–75%). Categorical variables were represented as frequency and percentage. Normal distribution was examined by the Shapiro–Wilk test. The comparison was performed between patients with OMA and non-OMA by the Chi-square test or Mann–Whitney U-test as appropriate. We conducted a conditional logistic regression analysis to explore the effect of daily TEM and their fluctuation on ICH occurrence in all patients and the cases with OMA and non-OMA, respectively. The outcomes were expressed as odds ratio (OR) and 95% confidence interval. A timeline was drawn to illustrate the temporal logic of the included data (Figure 2) R software (4.0.3) and GraphPad (9.0.0) were used for analysis and graphing, and the significance level was 0.05.
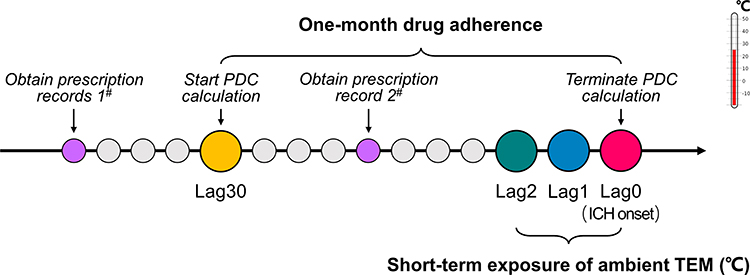 |
Figure 2 A research timeline illustrates the temporal logic of the included data. In this study, lag0 referred to the day when the symptoms of intracerebral hemorrhage (ICH) occurred. Lag1 referred to the previous day before lag0, and lag2 referred to the previous day before Lag1, and so on until lag30. The proportion of prescription days covered (PDC) by antihypertensive mediation in the last month before ICH onset was used to represent the 1-month medication adherence. The ambient temperature (TEM) in lag0 to lag2 were included to study its impact on ICH. |
Results
We enrolled 474 patients who met the research criteria were in this study. There were 299 males and 175 females, with a ratio of 1.7:1.0. The median age was 63.0 years, and about 60% of patients were aged ≥60 years old. More than 70% of the patients had deep ICH, and about 30% had a history of smoking or drinking. The proportion of patients with diabetes or cardiac disease was about 10% and 5%. The main seasons that ICH occurred were winter and spring. According to the 1-month antihypertensive medication adherence, the number of patients with OMA and non-OMA was 249 and 225, respectively. There was no significant difference in age, gender, hemorrhage location, diabetes, smoking, drinking, and onset season between the two groups, except for cardiac disease. Table 1 shows the baseline characteristics of the participants.
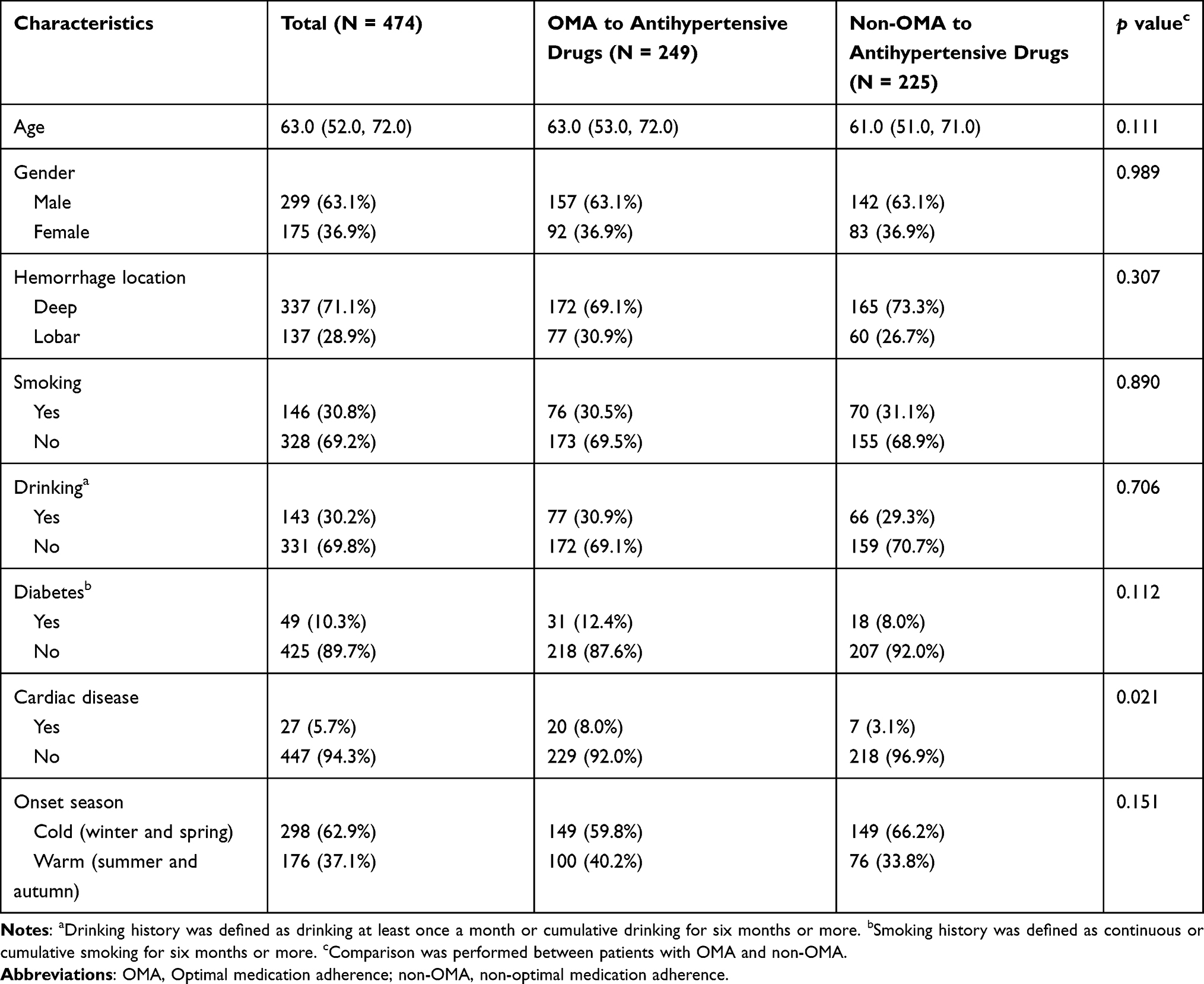 |
Table 1 Baseline Characteristics of Intracerebral Hemorrhage Patients Enrolled in This Study Who Had a History of Hypertension |
In the conditional logistic regression model, daily mean and max TEM in lag0 to 2, and daily min TEM in lag0 to 1, were significantly related to the ICH occurrence in all patients. This pattern persisted in cases with non-OMA. But in cases with OMA, we observed that only daily TEM in lag0 was meaningfully associated with ICH onset. The ORs were also dissimilar in patients with different medication adherence when the daily TEM was altered. For instance, the risk of ICH changed by 7.9% (OR = 0.921, [0.861, 0.985]) or 6.3% (OR = 0.937, [0.882, 0.995]) in OMA patients when daily mean or max TEM was respectively altered by 1°C in lag0, but the change expanded by 10.4% (OR = 0.896, [0.836, 0.960]) or 7.5% (OR = 0.925, [0.868, 0.986]) in non-OMA patients under the same condition. And the occurrence of ICH only changed in non-OMA patients (OR = 0.933, [0.882, 0.988]) when daily min TEM was altered by 1°C in Lag1. We did not observe any correlation of diurnal variation and day-to-day variation of TEM to ICH onset regardless of the medication adherence (Figure 3 and Table 2).
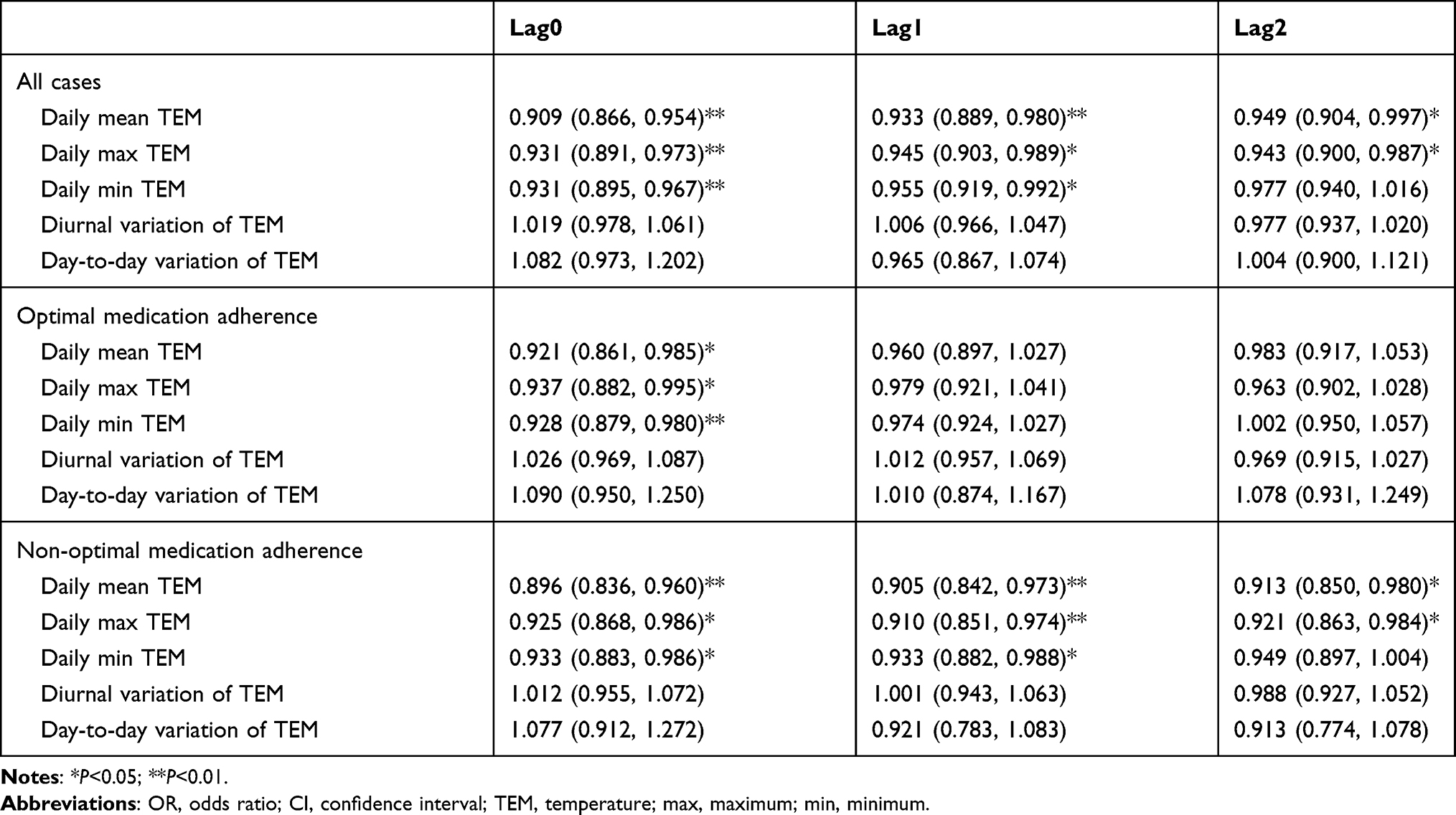 |
Table 2 The Effect of Ambient Temperature on Intracerebral Hemorrhage Occurrence Stratified by Different Antihypertensive Medication Adherence (OR, 95% CI) |
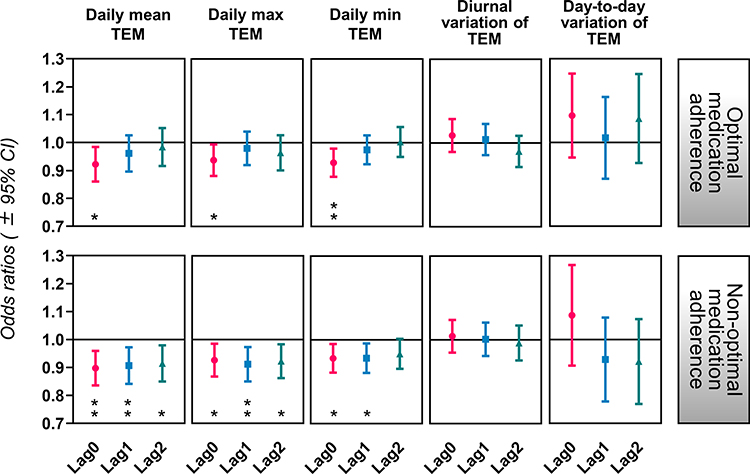 |
Figure 3 The influence of daily ambient temperature (TEM) and their fluctuation on intracerebral hemorrhage onset in patients with different antihypertensive medication adherence. The diurnal variation (the maximum of the day minus the minimum) and the day-to-day variation (the absolute value of the mean in the day minus the one in the previous day) of TEM were calculated to represent fluctuation. Optimal medication adherence was the patient had a proportion of prescription days covered (PDC) > 80%, and non-optimal medication adherence was PDC ≤ 80%. *P < 0.05; **P < 0.01. Abbreviation: CI, confidence interval. |
Discussion
This study is the first to explore the role of antihypertensive medication adherence in reducing the effect of ambient TEM on ICH occurrence. The main findings are: (1) only daily TEM in lag0 was related to ICH onset in OMA patients, (2) and these patients had a lower fluctuation in the risk of ICH when daily TEM altered.
Ambient TEM is a significant factor that affects the risk of ICH. Many studies reveal that short-term exposure to low ambient TEM has a meaningful effect on ICH occurrence.6–10 This meteorological parameter has immediate and delayed influences on the risk of stroke events.9 In the current study, we found that the lag effect of TEM weakened in the patients who had OMA to antihypertensive medications. The fluctuation of ICH risk also diminished when the ambient TEM was altered by 1°C. These results suggest that the benefit of OMA to antihypertensive drugs can reduce the effect of ambient TEM on ICH occurrence. In this study, participants in the OMA group had a higher proportion of cardiac history. This may be because patients who had a history of heart disease were more likely to recognize the harm of irregular administration of antihypertensive drugs. Our study did not observe any correlation of diurnal variation and day-to-day variation of TEM to ICH onset regardless of medication adherence, which is inconsistent with previous research.18–20 This contradiction may be due to different research designs and climatic characteristics.
The possible reason for our findings is that OMA may attenuate the influence of low ambient TEM on blood pressure. Hypertension is a crucial individual factor causing ICH, and the decrease of ambient TEM leads to an increase in blood pressure.21 This low ambient TEM usually causes excitation of the sympathetic nerve, increases the secretion of adrenocortical hormone and thyroid hormone, and activates the renin–angiotensin system. They collectively constrict peripheral blood vessels and enhance blood flow resistance, with the effect of raising blood pressure.21,22 For patients with hypertension, good antihypertensive medication adherence helps maintain the patient’s blood pressure at an optimal level. This may weaken the influence of low ambient TEM on blood pressure and reduce the effect of ambient TEM on ICH occurrence.
In our study, the selection of control was random bidirectional before and after the target event occurrence with seven days as the interval. This way of control selection can simultaneously control the confounding factors such as seasonality and day-of-week effect and eliminate the time trend bias.23 Recently, scholars use an artificial neural network to predict daily stroke occurrences and achieved good prediction performance.24 However, this method lacks interpretability due to the existence of a “black box”. Logistic regression is a handy, fast, and practical modeling method. In particular, the interpretability of the model is simple.25 In our research, a convenient explanation of the model was crucial, and consequently, we adopted classical logistic regression instead of using the neural network technique. Medication adherence is a time-dependent variable.14 Considering that our study observed the effect of short-term TEM exposure (lag0-lag2) on ICH occurrence, we used 1-month PDC before onset to represent patients’ recent medication adherence.
This study also has several potential limitations. Firstly, we used a retrospective method and recruited a small sample size, which may lead to selective bias and decreased credibility of the results. Some factors related to medication adherence, such as socioeconomic status,26 were not included in the study, which may also confound our results. In addition, we used logistic regression to fit the model. Although the model has a satisfactory explanatory ability, the fitting accuracy is not very high. There are problems of overfitting or underfitting, and it is difficult to deal with data imbalance. Secondly, our study proceeded under the condition of subtropical monsoon climate, and the results had regional characteristics. Our conclusions may not be applicable to other climate types. Multi-center researches with a large sample are required. Finally, the present research mainly focused on the role of optimal antihypertensive medication adherence in reducing the effect of ambient TEM on ICH occurrence. Other meteorological factors (such as air pressure, humidity, sunshine) and air pollutants (such as particulate matters, nitrogen oxides, sulfur oxides, ozone) were not included. It is of interest to further explore whether medication adherence can reduce the effect of other environmental factors on ICH occurrence.
Conclusions
In summary, our study indicates that optimal antihypertensive medication adherence helps to reduce the effect of ambient TEM on ICH occurrence in hypertensive patients. The discovery may be an underlying reason to explain the clinical benefit of antihypertensive drugs against environmental hazards, such as a cold wave. Large sample multicenter studies are needed to strengthen our conclusion.
Ethics Approval and Consent to Participate
All procedures performed in this study were following the ethical standards of Ethics Committee of Chengdu Fifth People’s Hospital (ref. no. 2019-085) and the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was not required since data were anonymized. The ethics committee approved the exemption from informed consent.
Acknowledgments
We thank Ms. Qing Qing, who graduated from Massey University in New Zealand, for her English editorial assistance.
Funding
This research was supported by grants from the Foundation of Sichuan Health Commission (19PJ016), and the Youth Innovation Project of Medical Scientific Research in Sichuan Province (Q19016).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. An SJ, Kim TJ, Yoon BW. Epidemiology, risk factors, and clinical features of intracerebral hemorrhage: an update. J Stroke. 2017;19(1):3–10. doi:10.5853/jos.2016.00864
2. Godoy DA, Nunez-Patino RA, Zorrilla-Vaca A, Ziai WC, Hemphill JC
3. Dastur CK, Yu W. Current management of spontaneous intracerebral haemorrhage. Stroke Vasc Neurol. 2017;2(1):21–29. doi:10.1136/svn-2016-000047
4. Burnier M, Egan BM. Adherence in hypertension. Circ Res. 2019;124(7):1124–1140. doi:10.1161/CIRCRESAHA.118.313220
5. Biffi A, Teo KC, Castello JP, et al. Impact of uncontrolled hypertension at 3 months after intracerebral hemorrhage. J Am Heart Assoc. 2021;10(11):e020392. doi:10.1161/JAHA.120.020392
6. Morabito M, Crisci A, Vallorani R, Modesti PA, Gensini GF, Orlandini S. Innovative approaches helpful to enhance knowledge on weather-related stroke events over a wide geographical area and a large population. Stroke. 2011;42(3):593–600. doi:10.1161/STROKEAHA.110.602037
7. Zheng D, Arima H, Sato S, et al. Low ambient temperature and intracerebral hemorrhage: the INTERACT2 Study. PLoS One. 2016;11(2):e0149040. doi:10.1371/journal.pone.0149040
8. Han MH, Yi HJ, Ko Y, Kim YS, Lee YJ. Association between hemorrhagic stroke occurrence and meteorological factors and pollutants. BMC Neurol. 2016;16:59. doi:10.1186/s12883-016-0579-2
9. Mukai T, Hosomi N, Tsunematsu M, et al. Various meteorological conditions exhibit both immediate and delayed influences on the risk of stroke events: the HEWS-stroke study. PLoS One. 2017;12(6):e0178223. doi:10.1371/journal.pone.0178223
10. Ma P, Zhou J, Wang S, et al. Differences of hemorrhagic and ischemic strokes in age spectra and responses to climatic thermal conditions. Sci Total Environ. 2018;644:1573–1579. doi:10.1016/j.scitotenv.2018.07.080
11. Diener HC, Hankey GJ. Primary and secondary prevention of ischemic stroke and cerebral hemorrhage: JACC focus seminar. J Am Coll Cardiol. 2020;75(15):1804–1818. doi:10.1016/j.jacc.2019.12.072
12. Dalli LL, Kim J, Cadilhac DA, et al. Greater adherence to secondary prevention medications improves survival after stroke or transient ischemic attack: a Linked Registry Study. Stroke. 2021;52(11):3569–3577. doi:10.1161/STROKEAHA.120.033133
13. Kim S, Shin DW, Yun JM, et al. Medication adherence and the risk of cardiovascular mortality and hospitalization among patients with newly prescribed antihypertensive medications. Hypertension. 2016;67(3):506–512. doi:10.1161/HYPERTENSIONAHA.115.06731
14. Kim J, Bushnell CD, Lee HS, Han SW. Effect of adherence to antihypertensive medication on the long-term outcome after hemorrhagic stroke in Korea. Hypertension. 2018;72(2):391–398. doi:10.1161/HYPERTENSIONAHA.118.11139
15. Guo Y, Xie X, Lei L, et al. Short-term associations between ambient air pollution and stroke hospitalisations: time-series study in Shenzhen, China. BMJ Open. 2020;10(3):e032974. doi:10.1136/bmjopen-2019-032974
16. Qian Y, Yu H, Cai B, Fang B, Wang C. Association between incidence of fatal intracerebral hemorrhagic stroke and fine particulate air pollution. Environ Health Prev Med. 2019;24(1):38. doi:10.1186/s12199-019-0793-9
17. Wilker EH, Mostofsky E, Fossa A, et al. Ambient pollutants and spontaneous intracerebral hemorrhage in Greater Boston. Stroke. 2018;49:2764–2766. doi:10.1161/STROKEAHA.118.023128
18. Lei L, Bao J, Guo Y, Wang Q, Peng J, Huang C. Effects of diurnal temperature range on first-ever strokes in different seasons: a time-series study in Shenzhen, China. BMJ Open. 2020;10(11):e033571. doi:10.1136/bmjopen-2019-033571
19. Garg RK, Ouyang B, Pandya V, et al. The influence of weather on the incidence of primary spontaneous intracerebral hemorrhage. J Stroke Cerebrovasc Dis. 2019;28(2):405–411. doi:10.1016/j.jstrokecerebrovasdis.2018.10.011
20. Jeong TS, Park CW, Yoo CJ, Kim EY, Kim YB, Kim WK. Association between the daily temperature range and occurrence of spontaneous intracerebral hemorrhage. J Cerebrovasc Endovasc Neurosurg. 2013;15(3):152–157. doi:10.7461/jcen.2013.15.3.152
21. Lavados PM, Olavarria VV, Hoffmeister L. Ambient temperature and stroke risk: evidence supporting a short-term effect at a population level from acute environmental exposures. Stroke. 2018;49(1):255–261. doi:10.1161/STROKEAHA.117.017838
22. Yu B, Jin S, Wang C, et al. The association of outdoor temperature with blood pressure, and its influence on future cardio-cerebrovascular disease risk in cold areas. J Hypertens. 2020;38(6):1080–1089. doi:10.1097/HJH.0000000000002387
23. Janes H, Sheppard L, Lumley T. Case-crossover analyses of air pollution exposure data: referent selection strategies and their implications for bias. Epidemiology. 2005;16(6):717–726. doi:10.1097/01.ede.0000181315.18836.9d
24. Katsuki M, Narita N, Ishida N, et al. Preliminary development of a prediction model for daily stroke occurrences based on meteorological and calendar information using deep learning framework (Prediction One; Sony Network Communications Inc., Japan). Surg Neurol Int. 2021;12:31. doi:10.25259/SNI_774_2020
25. Kang JS, Lee C, Song W, et al. Risk prediction for malignant intraductal papillary mucinous neoplasm of the pancreas: logistic regression versus machine learning. Sci Rep. 2020;10(1):20140. doi:10.1038/s41598-020-76974-7
26. Towfighi A, Cheng EM, Ayala-Rivera M, et al. Randomized controlled trial of a coordinated care intervention to improve risk factor control after stroke or transient ischemic attack in the safety net: Secondary stroke prevention by Uniting Community and Chronic care model teams Early to End Disparities (SUCCEED). BMC Neurol. 2017;17(1):24. doi:10.1186/s12883-017-0792-7
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.