Back to Journals » International Medical Case Reports Journal » Volume 17
Optic Nerve Hypoplasia – Case Report
Authors Lestak J ![]() , Prazakova L, Fus M
, Prazakova L, Fus M ![]() , Kyncl M
, Kyncl M
Received 21 May 2024
Accepted for publication 12 September 2024
Published 9 October 2024 Volume 2024:17 Pages 835—841
DOI https://doi.org/10.2147/IMCRJ.S479333
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jan Lestak, Lenka Prazakova, Martin Fus, Martin Kyncl
Faculty of Biomedical Engineering, Czech Technical University in Prague, Kladno, 272 01, Czech Republic
Correspondence: Jan Lestak, Faculty of Biomedical Engineering, Czech Technical University in Prague, Kladno, 272 01, Czech Republic, Email [email protected]
Abstract: The case report of a young myope (born in 1997) who was diagnosed with bilateral concentric narrowing of the visual field to 15– 20 degrees in 2021 is presented. On eye fundus, the findings were normal with central excavation c/d=0.5 and 0.4, respectively. OCT showed loss of retinal nerve fiber layer – in both vertical quadrants, including a reduction in the ganglion cell complex. Electrophysiological examination (PERG) showed normal retinal responses. Visual evoked responses (PVEP) after stimulation squared a 1 degree decrease in amplitudes, with no prolongation of P100 latency. When stimulated with 15-minute squares, responses were normal (see Supplementary Figure). Magnetic resonance imaging of the brain showed a narrowing of the chiasm. In conclusion, optic chiasm hypoplasia may not always have distinct morphological and functional manifestations. In addition to imaging methods, electrophysiological examination of the visual analyser was of great help for its verification.
Keywords: optic nerve hypoplasia, visual field, imaging methods, electrophysiological examinations
Introduction
The first report of optic disc appearance in optic nerve hypoplasia (ONH) dates back to 1915.1 The optic nerve head is usually reduced to 1/3 to 1/2 of its normal diameter and is usually lined with a yellowish halo or double ring of atrophic choroid and pigmented leaf, often the size of a normal target. Complete aplasia of the optic nerve is quite uncommon. At the opposite extreme is a not very reduced, pale target with a sectorial visual field and usable visual acuity.2 Histologically, ONH is characterized by a subnormal number of optic nerve axons and is a non-progressive, non-specific manifestation of damage at any site of the optic pathways that occurs before their full development.3–5 In addition to intraocular changes, ONH can also cause intracranial changes. Reeves described agenesis of the septum pellucidum in a four-month-old blind infant.6 These changes were confirmed postmortem by de Morsier, who described the absence of the septum pellucidum. In his report, he stated that one of the specimens was from a woman with a unilaterally vertically rotated optic tract who died of pyelonephritis at the age of 84 with no history of visual problems. This single case gave rise to the term “la dysplasia septo-optique” (septo-optic dysplasia-SOD).7 Brodsky and Glasier described other intracranial abnormalities in SOD. In addition to the absence of the septum pellucidum, these may include thinning of the corpus callosum and dysplasia of the third ventricle, ectopia of the posterior pituitary, and malformations of the cerebral hemispheres.8 Garcia-Filion and Borcher report that currently, children with ONH require monitoring for many systemic, developmental, and even life-threatening problems regardless of the severity of ONH and the presence of brain malformations, including abnormalities of the septum pellucidum. They note that septo-optic dysplasia and de Morsier syndrome are historically inaccurate and clinically misleading terms.9 Histopathological examination showed 90% reduction of optic nerve fibres without finding degenerated axons.10 Visual acuity can range from blindness to normal vision. Associated ophthalmological features include nystagmus (26–86%), strabismus (42–52%), axial myopia and astigmatism.9,11–14
If the finding on the optic nerve papilla is typical and indicative of its hypoplasia and the visual functions correspond to it, then the diagnosis is unproblematic. In case of minimal ophthalmoscopic changes and intact visual acuity, this finding may cause diagnostic difficulties. This led us to present this case report.
Case Report
In 2021, a 24-year-old male presented for ocular exam. Except for the use of spectacles for myopia since age 11, he reported no visual issues. Changes were noted on perimeter exam. On the right eye concentric narrowing to 20 degrees, on the left eye to 15 degrees (see Figure 1).
 |
Figure 1 Visual field report. Bilateral concentric narrowing to 20 (result of right eye on the left) and 15 degrees (result of left eye on the right). Examination was performed with the Octopus 900 (Haag-Streit AG) using the 30–2 program. MD – mean defect and MS – mean sensitivity, dB – decibels. |
Using OCT, we also examined the peripapillary nerve fiber layer (RNFL), using Avanti RTVue XR (Optovue) with a finding of a reduction in its thickness. Right 84.29 µm, left 80.45 µm. Ganglion cells complex (GCC) values were also within pathological values; right 79.22 µm, left 79.01 µm (Figure 2). Because of these changes, the patient was sent to the first author’s workplace for further examination and clarification of the diagnosis.
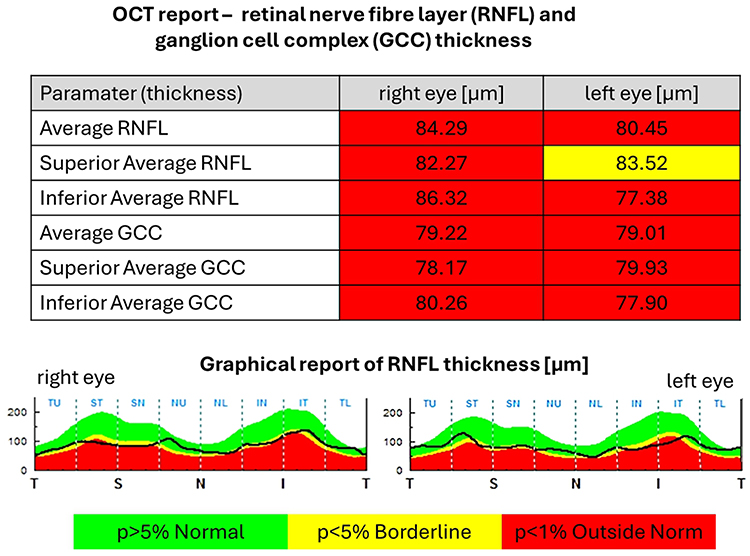 |
Figure 2 OCT report – retinal nerve fibre layer (RNFL) and ganglion cell complex (GCC) thickness. Subfigure A – numerical values, subfigure B – graphic representation of the comparison of values with the normative database. |
During examination, it was found: bulbs were in parallel position, free motility. Diplopia was not reported by the patient. The pupillary reactions were correct. Ocular findings on the anterior segment and optical media were normal. On the fundus papillae with deep central excavation (c/d right=0.5, left=0.4) and no double rim. Otherwise, the findings on the ocular background were normal (Figure 3).
 |
Figure 3 Photographs of the ocular fundus with normal findings. On the right is c/d=0.5, on the left=0.4. according to automatic assessment by OCT 0.84 for right eye and 0.88 for left eye. |
On the right is c/d=0.5, on the left=0.4. The OCT device measured it at 0.84 and left 0.88. Similar to the first workplace, we also demonstrated a decrease in RNFL and vessel density values in both eyes, which was 46% bilaterally. Figure 4.
 |
Figure 4 RNFL and vessel density (VD) values in individual segments of the peripapillary region. Top, right eye findings, bottom, left eye findings. For VD (findings on the right), the values in the nasal segments are significantly lower than in the temporal part of the optic nerve target. The examination was performed with the Optovue OCT device. |
Colour discrimination was correct. Intraocular pressure 14/14 mmHg (Ocular Response Analyser, Reichert Technologies). The pattern electroretinogram (PERG) showed normal retinal responses in both eyes (P50-N95 amplitudes right=19 µV, left=14 µV). Examination of visual evoked potentials (PVEPs) during stimulation with a reversed black-and-white checkerboard of 1-degree field size showed a decrease in N75-P100 amplitudes (right=8.3 µV, left=6.4 µV) without prolonging the latency of the P100 ms peak. Using smaller squares (15 min), normal responses were fitted bilaterally (right=11.6 µV, left=11 µV). Even with this stimulation, the P100 peak latency was not prolonged (6). The examination was performed with the Roland Consult electrophysiological diagnostic system (Germany) according to the ISCEV methodology. The size of the stimulation field was 41×31 angular degrees.15
Based on the above examinations, we concluded the finding as optic nerve hypoplasia with damage mainly to the magnocellular canal. Magnetic resonance imaging (MRI) of the brain revealed no abnormalities. The corpus callosum and hypothalamic–pituitary axis area structures had normal morphology. Frontally, changes consistent with the fenestration of the falx with mesial interdigitations of the frontal lobe cortex were noted. Mild periventricular atrophy of the brain was also observed. There was no evidence of malformations of cortical development, without typical changes indicative of septo-optic pituitary dysplasia. On the second examination, we also focused on the chiasma opticum, whose laterolateral dimension was reduced to 12.4 mm (control group 13.76 ± 0.55 mm).16
Discussion
To understand the abnormalities of the optic nerve target, it is important to know the embryology of the eye. In an embryo about three weeks old, the fetal slit begins to insert ventrolaterally into the eye sac and the peripheral portion of its pedicle. The para-axial mesoderm inserts into it and forms into a primitive papilla at the proximal end of the fetal slit. The embedded mesoderm also forms the hyaloid vascular system, the basis of the retinal vessels. In the seven-week-old embryo, ganglion cells of the retina differentiate in the inner leaflet of the eyecup, whose nerve fibres sprout into the primitive papilla and the peduncle of the cup into the brain.17 As it follows from the above, a prerequisite for proper optic nerve development is the intact development of both the fetal cleft and the mesodermal tissue embedded in it, as well as the retinal ganglion cells. In hypoplasia, it may be conditioned by insufficient formation of the mesodermal base of the papilla or by a gross defect in the differentiation of retinal ganglion cells. Both components may also apply.17
Retinal ganglion cell responses were normal, according to electrophysiological examination. On the left, however, there was a finding compared to the right eye with a lower amplitude of the P50-N95 oscillation (19 µV and 14 µV, respectively). PVEPs showed a decrease in N70-P100 amplitude to 8.3 µV on the right and 6.4 µV on the left after stimulation with large squares. When using small squares, the responses were within the norm (11.6 µV right, 11 µV left). From this, we concluded that it is damage to the magnocellular visual pathway. This is also evidenced by normal visual acuity and intact color perception.
In recent decades, the number of reported cases of ONH has increased. The estimated prevalence is 7.2 per 100,000 population in Sweden and 10.9 per 100,000 population in England.18 More recent work indicates a prevalence of 1.9 and 2.5/100,000 population.19 ONH has become the leading cause of congenital blindness.
The most common intracranial findings during neuroimaging were often the associated features of hypopituitarism and missing septum pellucidum were gated as embryonic linkage “septo-optic dysplasia” or “de Morsier syndrome”. More recent studies suggest that these associations are independent of each other.9 The most prominent and commonly reported prenatal features of ONH are low maternal age and primiparity.20–23 Many reports speculate that the association with young maternal age reflects an increased risk. Evidence for this hypothesis is insufficient due to the lack of findings of risk behaviour in cohort studies using standardised methods. Maternal age and primiparity may be proxies for more underlying health and demographic factors that determine prenatal risk of ONH but have not yet been explored.
ONH has long been associated with recreational drug use (eg LSD) or prescribed use of eg anticonvulsants, quinine, antidepressants,20,21,24–27 viral infection,20,28,29 diabetes of the mother30 and alcohol use during pregnancy.31,32
Almost all of the etiological correlates listed were primarily based on isolated exposures or case reports, which provide the lowest level of evidence. In two small series of case reports of fetal alcohol syndrome, ONH was reported in 25–48%.31,32
Similarly, Otradovec in his monograph indicates exogenous disorders rather than hereditary influences as the cause.2
The patient’s parents were also examined at the second author’s workplace and no ocular abnormalities were detected. We did not receive from the mother any possible connection with the use of the above-mentioned drugs during pregnancy.
The most common neuroimaging findings were absent septum pellucidum (53%), corpus callosum hypoplasia and pituitary abnormalities (13–34%) such as ectopic pituitary, empty sella and infundibular hypoplasia.4,8 Isolated absence of septum pellucidum was associated with normal developmental and endocrinological features.8,13,33
From the ophthalmological point of view, the findings on the optic nerves and chiasm are important in the absence of the above described SOD abnormalities. If there is a congenital loss of retinal ganglion cell axons, then radiological findings on the thinner optic nerves and chiasm should also be a radiological finding. This has been described by Ward et al and Salman et al34,35
Our patient’s findings showed a narrower chiasma on reevaluation. Even after repeated promises, the patient failed to attend for a follow-up MRI and assessment of optic nerve width.
Visual evoked potentials (VEP) and electrophysiological examination may be pathological or normal in patients with SOD.36,37
We found normal electrical functions in the stimulated part of the retina in our patient. In the left eye, where there were greater changes in both the perimeter and the RNFL, the amplitudes from the ganglion cells were lower compared with the right eye. However, I must point out that the examination methodology (ISCEV) recommends only one type of stimulation squares and a stimulation area size of 15 angular degrees (ERG pattern).38
During VEP examinations, 1 and subsequently by 15’ square is used for stimulation. This means that with a sufficiently large stimulation area (in our case 41×31 angular degrees) the status of both parvocellular canal located mainly in the central part and magnocellular ones located in the periphery of the retina can be detected. The ISCEV methodology recommends 15 angular degrees.38
Magnocellular ganglion cells, located mainly in the periphery of the retina, respond to moving objects of low spatial frequency.39
Because the axons of magnocellular RGCs enter from the temporal side of the retina to target the optic nerve at the superior pole (S) and inferior pole (I). Nasal fibers are then all over the nasal side of the target. Therefore, in our patient, the values of vessel density in these places are also the smallest.
If the concentric narrowing of the visual field is caused by an insufficient number of ganglion cells in the retina, then it is by using larger stimulation patterns and sufficient size of the stimulating area that their abnormality can be demonstrated. Our patient had concentric narrowing to 20 and 15 degrees, respectively. We verified this by examining the VEPs using large checkerboard patterns. We did not demonstrate prolongation of P100 latency. There was no morphological correlation to this either.
Conclusion
ONH may not always have distinct morphological and functional manifestations. Our case report is a proof of this. The electrophysiological examination of the visual analyser helped us to verify it. We would like to point out the importance of a sufficient size of the stimulating field.
Data Sharing Statement
The datasets used and/or analysed during the present study are available from the corresponding author on reasonable request.
Ethics Statement
All details, medical records, figures, medical history or test results were used with the written consent for publication from the patient. All data used were anonymized. The presented case report was performed according to the Declaration of Helsinki. No official institutional approval was required by the internal ethics committee of the JL Eye Clinic (Prague, Czech Republic) to publish the details of the case report.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
All authors have nothing to disclose related to this case report. All authors report no conflict of interests.
References
1. Schwarz O. Ein fall von mangelhafter Bildung beider sehnerven [A case of inadequate formation of both optic nerves]. Albrecht von Graefes Arch Klin Ophthalmol. 1915;90:326. German. doi:10.1007/BF01858338
2. Otradovec J. Klinická neurooftalmologie. Praha: Grada Publishing; 2003.
3. Mosier MA, Lieberman MF, Green WR, Knox DL. Hypoplasia of the optic nerve. Arch Ophthalmol. 1978;96:1437–1442. doi:10.1001/archopht.1978.03910060185017
4. Hotchkiss ML, Green WR. Optic nerve aplasia and hypoplasia. J Pediatr Ophthalmol Strabismus. 1979;16(4):225–240. doi:10.3928/0191-3913-19790701-06
5. Novakovic P, Taylor DS, Hoyt WF. Localising patterns of optic nerve hypoplasia-retina to occipital lobe. Br J Ophthalmol. 1988;72:176–182. doi:10.1136/bjo.72.3.176
6. Reeves D. Congenital absence of the septum pellucidum. Bull Johns Hopkins. 1941;69:61–71.
7. De Morsier G. Etudes sur les dysraphies cranioencephaliques: agenesis du septum lucidum acec malformatnio du tractus optique. La Dysplasie Septooptique Schweiz Arch Neurol Psychiatr. 1956;77:267–292.
8. Brodsky MC, Glasier CM. Optic nerve hypoplasia. Clinical significance of associated central nervous system abnormalities on magnetic resonance imaging. Arch Ophthalmol. 1993;111:66–74. doi:10.1001/archopht.1993.01090010070029
9. Garcia-Filion P, Borchert M. Optic nerve hypoplasia syndrome: a review of the epidemiology and clinical associations. Curr Treat Options Neurol. 2013;15:78–89. doi:10.1007/s11940-012-0209-2
10. Saadati HG, Hsu HY, Heller KB, Sadun AA. A histopathologic and morphometric differentiation of nerves in optic nerve hypoplasia and Leber hereditary optic neuropathy. Arch Ophthalmol. 1998;116:911–916. doi:10.1001/archopht.116.7.911
11. Zeki SM. Optic nerve hypoplasia and astigmatism: a new association. Br J Ophthalmol. 1990;74:297–299. doi:10.1136/bjo.74.5.297
12. Weiss AH, Ross EA. Axial myopia in eyes with optic nerve hypoplasia. Graefe’s Arch Clin Exp Ophthalmol. 1992;230:372–377. doi:10.1007/BF00165948
13. Siatkowski RM, Sanchez JC, Andrade R, Alvarez A. The clinical, neuroradio-graphic, and endocrinologic profile of patients with bilateral optic nerve hypoplasia. Ophthalmology. 1997;104:493–496. doi:10.1016/S0161-6420(97)30286-3
14. Mohney BG, Young RC, Diehl N. Incidence and associated endocrine and neurologic abnormalities of optic nerve hypoplasia. JAMA Ophthalmol. 2013;131:898–902. doi:10.1001/jamaophthalmol.2013.65
15. Lešták J, Nutterová E, Pitrová Š, Krejčová H, Bartošová L, Forgáčová V. High tension versus normal tension glaucoma. A comparison of structural and functional examinations. J Clinic Exp Ophthalmol. 2012;5(2). doi:10.4172/2155-9570.S5-006
16. Lešták J, Kynčl M, Fůs M, Marešová K. Optic chiasm width in normal-tension and high tension glaucoma. Cesk Slov Oftalmol. 2020;76:126–128. doi:10.31348/2020/21
17. Karel I, Brachfeld K. Bilateral hypoplasia and aplasia of the optic nerve. Cesk Oftalmol. 1965;21:334–342.
18. Borchert M, Garcia-Filion P. The syndrome of optic nerve hypoplasia. Curr Neurol Rep. 2008;8:395–403. doi:10.1007/s11910-008-0061-7
19. Garne E, Rissmann A, Addor M, et al. Epidemiology of septo-optic dysplasia with focus on prevalence and maternal age – a EUROCAT study. Eur J Med Genet. 2018;61:483–488. doi:10.1016/j.ejmg.2018.05.010
20. Margalith D, Jan JE, McCormick AQ, et al. Clinical spectrum of optic nerve hypoplasia: a review of 51 patients. Dev Med Child Neurol. 1984;26:311–322. doi:10.1111/j.1469-8749.1984.tb04447.x
21. Tornqvist K, Ericsson A, Kallen B. Optic nerve hypoplasia: risk factors and epidemiology. Acta Ophthalmol Scand. 2002;80:300–304. doi:10.1034/j.1600-0420.2002.800313.x
22. Murray PG, Paterson WF, Donaldson MD. Maternal age in patients with septo-optic dysplasia. J Pediatr Endocrinol Metab. 2005;18:471–476. doi:10.1515/JPEM.2005.18.5.471
23. Webb EA, Dattani MT. Septo-optic dysplasia. Eur J Hum Genet. 2010;18:393–397. doi:10.1038/ejhg.2009.125
24. Hoyt C, Billson F. Maternal anticonvulsants and optic nerve hypoplasia. Br J Ophthalmol. 1978;62:3–6. doi:10.1136/bjo.62.1.3
25. West J, Burke J, Strachan I. Carbamazepine, epilepsy, and optic nerve hypoplasia. Br J Ophthalmol. 1990;74:511. doi:10.1136/bjo.74.8.511-a
26. Hellstrom A, Wiklund L, Svensson E. The clinical and morphological spectrum of optic nerve hypoplasia. J Am Assoc Pediatr Ophthalmol Strabismus. 1999;3:212–220. doi:10.1016/S1091-8531(99)70005-4
27. McMahon C, Braddock S. Septo-optic dysplasia as a manifestation of valproic acid embryopathy. Teratology. 2001;64:83–86. doi:10.1002/tera.1049
28. Hittner H, Desmond M, Montgomery J. Optic nerve manifestations of cytomegalovirus infection. Am J Ophthalmol. 1976;81:661–665. doi:10.1016/0002-9394(76)90134-3
29. Burke J, O’Keefe M, Bowell R. Optic nerve hypoplasia, encephalopathy, and neurodevelopmental handicap. Br J Ophthalmol. 1991;75:236–239. doi:10.1136/bjo.75.4.236
30. Kim RY, Hoyt WF, Lessell S, Narahara MH. Superior segmental optic nerve hypoplasia: a sign of maternal diabetes. Arch Ophthalmol. 1989;107:1312–1315. doi:10.1001/archopht.1989.01070020382040
31. Stromland K. Ocular involvement in the fetal alcohol syndrome. Surv Ophthalmol. 1987;31:277–284. doi:10.1016/0039-6257(87)90028-2
32. Ribeiro IM, Vale PJ, Tenedorio PA, Rodrigues PA, Bilhoto MA, Pereira HC. Ocular manifestations in fetal alcohol syndrome. Eur J Ophthalmol. 2007;17:104–109. doi:10.1177/112067210701700114
33. Garcia-Filion P, Epport K, Nelson M, et al. Neuro-radiographic, endocrinologic, and ophthalmic correlates of adverse developmental outcomes in children with optic nerve hypoplasia: a prospective study. Pediatrics. 2008;121:653–659. doi:10.1542/peds.2007-1825
34. Ward DJ, Connolly DJA, Griffiths PD. Review of the MRI brain findings of septo-optic dysplasia. Clin Radiol. 2021;76(2):160.e1–160.e14. doi:10.1016/j.crad.2020.09.007
35. Salman MS, Hossain S, Rozovsky K. Neuroimaging features in children with optic nerve hypoplasia and septo-optic-pituitary dysplasia. Can J Neurol Sci. 2023;26:1–9.
36. Borchert M, Mccullogh D, Rother C, Stout A. Clinical assessment, optic disk measurements, and visual-evoked potential in optic nerve hypoplasia. Am J Ophthalmol. 1995;120:605–612. doi:10.1016/S0002-9394(14)72207-X
37. McCulloch D, Garcia-Filion P, Fink C, Chaplin C, Borchert M. Clinical electrophysiology and visual outcome in optic nerve hypoplasia. Br J Ophthalmol. 2009;94:1017–1023. doi:10.1136/bjo.2009.161117
38. Bach M, Brigell MG, Hawlina M, et al. ISCEV standard for clinical pattern electroretinography (PERG) – 2012 update. Doc Ophthalmol. 2013;126:1–7. doi:10.1007/s10633-012-9353-y
39. Skalicky SE. Ocular and Visual Physiology. Clinical Application. Australia: Springer Science+Business Media Singapore Pte Ltd; 2016:
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.