Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
OPRM1 A118G Polymorphism and Ondansetron Efficacy for Postoperative Nausea and Vomiting in Laparoscopic Gynaecological Surgery: A Retrospective Cohort Study
Authors Zhao X, Yu Q, Yu G, Liu C, Feng Z, Zhang W
Received 4 July 2025
Accepted for publication 17 November 2025
Published 25 December 2025 Volume 2025:21 Pages 1821—1832
DOI https://doi.org/10.2147/TCRM.S551616
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Xu Zhao,1,* Qingqing Yu,2,* Guanling Yu,2 Chengxiao Liu,1 Zunsai Feng,1 Wenjia Zhang1
1Department of Anesthesiology, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, Shandong, People’s Republic of China; 2State Key Laboratory of Reproductive Medicine and Offspring Health, Center for Reproductive Medicine, Institute of Women, Children and Reproductive Health, Shandong University, Jinan, Shandong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wenjia Zhang, Department of Anesthesiology, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, Shandong, 250021, People’s Republic of China, Tel +86-18615201505, Email [email protected]
Background: The OPRM1 A118G polymorphism has been implicated in modulating susceptibility to postoperative nausea and vomiting (PONV). Ondansetron, a 5-HT3 receptor antagonist, is widely utilized for PONV prophylaxis; however, whether its efficacy is influenced by OPRM1 A118G polymorphism remains unclear.
Methods: We conducted a retrospective cohort study including patients undergoing laparoscopic gynecological surgery between January 2019 and December 2024; propensity score matching was used to adjust for confounders. OPRM1 A118G genotypes (AA, AG, GG) were analyzed through polymerase chain reaction and sequencing. PONV incidence and severity were assessed using the Visual Analog Scale (VAS) at various postoperative time points.
Results: The Ondansetron group had significantly lower PONV incidence within 2 hours (38.82% vs 56.98%, p = 0.0174) and 2 ~ 24 hours (8.24% vs 19.77%, p = 0.0300). The OPRM1 A118G polymorphism was associated with higher PONV risk, particularly in patients with the AG/GG genotypes in the control group. In the Ondansetron group, the association was significant only within 2 hours (p = 0.0460).
Conclusion: The OPRM1 A118G polymorphism is associated with an increased risk of early PONV, particularly in patients with the G allele, which has been related to reduced μ-opioid receptor sensitivity and increased opioid requirements, thereby predisposing patients to a higher PONV risk. Ondansetron significantly reduces PONV incidence and severity, especially in patients with higher genetic susceptibility.
Keywords: postoperative nausea and vomiting, OPRM1, A118G, ondansetron
Introduction
Postoperative nausea and vomiting (PONV) occur within 24 ~ 48 hours after surgery, affecting approximately 30% of patients.1,2 As the most common complication following anesthesia, PONV lead to dehydration, wound dehiscence, prolonged hospital stays, and increased healthcare costs.3,4 It is also a major cause of patient dissatisfaction post-surgery.5
The pathophysiology of PONV is complex, involving interactions between both the peripheral and central nervous systems.6 Peripherally, surgical trauma and anesthetic agents trigger the release of neurotransmitters, including serotonin, in the gastrointestinal tract, which transmits afferent signals to the medullary vomiting center via the vagus nerve.7 Centrally, the vomiting center integrates input from the vestibular system, chemoreceptor trigger zone (CTZ), and cerebral cortex, with the CTZ being particularly responsive to emetogenic substances, such as opioids and metabolites of inhaled anesthetics.8 The emetic reflex is modulated by multiple neurotransmitter systems, including dopamine D2, 5-hydroxytryptamine 3 (5-HT3), histamine H1, muscarinic, and neurokinin-1 (NK1) receptors. In addition, factors such as the type of surgical procedure, intraoperative hypotension leading to cerebral hypoperfusion, interindividual variability, and the administration of postoperative opioids have been identified as contributing to the activation of the emetic pathway.9,10
Recent studies on genetic single-nucleotide polymorphisms (SNPs) have provided significant insights into susceptibility to PONV. While genome-wide association studies have not identified high-impact susceptibility loci for PONV, increasing evidence indicates that genes related to dopamine receptors, particularly DRD2, play a crucial role in modulating dopaminergic neurotransmission within the chemoreceptor trigger zone and vomiting center, which are key components of the emetic reflex pathway.11,12 The DRD2 TaqIA polymorphism (rs1800497) has been reported to alter dopamine receptor density and signaling efficiency, thereby influencing individual susceptibility to PONV and responsiveness to dopamine receptor antagonists. Several studies have confirmed this association, supporting the contribution of dopaminergic pathways to the pathophysiology of PONV.2,12,13 Furthermore, the OPRM1 A118G (rs1799971) polymorphism, a key regulator of pain perception and opioid response, has been shown to indirectly influence PONV susceptibility.14,15 The G allele at this locus results in impaired N-glycosylation of the μ-opioid receptor and reduces its binding affinity for endogenous and exogenous opioids, leading to diminished analgesic effects and a consequent need for higher opioid doses to achieve adequate pain control.15–17 This increased opioid exposure represents an independent risk factor for PONV, linking the OPRM1 genotype to both analgesic efficacy and postoperative emetic risk. Consequently, the OPRM1 A118G polymorphism may serve as a genetic biomarker for predicting PONV risk, facilitating the development of personalized antiemetic strategies.
Ondansetron, a 5-HT3 receptor antagonist, is a critical drug for preventing PONV, especially in laparoscopic gynecological surgeries.18,19 Recent studies have demonstrated that the monotherapy efficacy of ondansetron is approximately 50 ~ 60%, whereas its combination with dexamethasone reduces the incidence of PONV to 12.5%.20 Individual responses to treatment may be influenced by genetic polymorphisms. The OPRM1 A118G polymorphism, which alters μ-opioid receptor function, has been shown to affect opioid sensitivity, a key factor contributing to the development of PONV.15,16 It has been suggested that individuals with the OPRM1 118G allele, particularly women, require higher opioid doses, and the effectiveness of ondansetron in preventing PONV may be limited in this group.5 The aim of the present study is to investigate the differences in the incidence and severity of PONV following ondansetron administration in patients with different OPRM1 A118G genotypes (AA/AG/GG) undergoing laparoscopic gynecological surgery.
Materials and Methods
Participants
This study was a retrospective analysis conducted at March 2025. The patients who underwent laparoscopic gynecological surgery at our institution were included, comprising those who did not receive Ondansetron intervention between January 2019 and December 2021 (Control group) and those who received Ondansetron between January 2022 and December 2024 (Ondansetron group). In our institution, ondansetron was introduced into routine prophylactic use for PONV only after January 2022. Therefore, patients from 2019–2021 naturally formed the control cohort, and those from 2022–2024 constituted the ondansetron cohort. This temporal grouping reflected an institutional practice change rather than a prospective intervention. The patients in the control groups were screened according to propensity score matching using R Studio, with the following covariates: age, BMI, ASA classification, type of underlying disease, anesthesia duration, pneumoperitoneum time, intraoperative blood loss, and total fentanyl dosage. Propensity score matching (PSM) was conducted using a 1:1 nearest-neighbor algorithm with a caliper width of 0.05. The selection of these covariates was based on their potential influence on PONV and anesthetic response. The balance between matched groups was evaluated using standardized mean differences (SMDs), with values <0.1 considered acceptable Average SMD before matching was 0.11; average SMD value after matching was 0.08. The study was approved by Shandong Provincial Hospital Affiliated to Shandong First Medical University (#2025-03-207). Given the retrospective design and use of de-identified data, the requirement for individual informed consent was waived.
The Inclusion Criteria for the Patients Who Underwent Elective Laparoscopic Gynecological Surgery
The patients who met the inclusion criteria were included for analysis: Age ≥ 18 years; American Society of Anesthesiologists (ASA) classification I–II.
The Exclusion Criteria for the Patients Who Underwent Elective Laparoscopic Gynecological Surgery
If the patients met the exclusion criteria, they were exclude from analysis: Inability to understand the Visual Analog Scale (VAS) for pain assessment; Administration of antiemetics or occurrence of nausea and vomiting within 24 hours before surgery; History of allergy to any study-related medications; Use of chemotherapy agents within one week before surgery; Development of severe postoperative complications; History of smoking; History of gastrointestinal ulcers; Use of antitussive drugs or opioids with contraindications to neuroblocking within one week before surgery.
The Assessment of the Incidence and Severity of PONV
In our institution, PONV is routinely assessed and documented by trained anesthesiology nurses and ward physicians as part of standard postoperative care. The assessment is performed at standardized postoperative intervals (0–2 hours and 2–24 hours) according to the institutional monitoring protocol. The incidence and severity of PONV were recorded on postoperative days 1, 2, and 3 in the electronic medical record system. Only patients with complete PONV documentation were included in the analysis. Complete response (CR) was defined as the absence of vomiting without the need for rescue interventions, while complete control (CC) was defined as the absence of both vomiting and nausea. The CR rate (number of CR events/total number of cases) and the CC rate (number of CC events/total number of cases) were calculated. The severity of PONV was evaluated using the VAS,21 with scores ranging from 0 to 10. A score of < 4 was categorized as mild, 4 ~ 7 as moderate, and > 7 as severe. All VAS data used in this study were extracted from routinely recorded postoperative nursing documentation.
The Identification of OPRM1 A118G
Preoperative blood samples routinely collected for standard laboratory testing were retrieved from the institutional biobank for genetic analysis after obtaining ethics committee approval. No additional blood collection was performed for this study. Preoperative blood samples were collected in tubes containing potassium ethylenediaminetetraacetate. Genomic DNA was extracted using the nucleic acid extraction Midi kit (TIANGEN, Beijing, China) according to the manufacturer’s instructions. The extracted genomic DNA was stored at −20°C. Polymerase chain reaction (PCR) amplification was carried out as follows: (1) denaturation at 94°C for 5 minutes; (2) 30 cycles of 94°C for 30 seconds, 56°C for 30 seconds, and 72°C for 30 seconds; (3) final extension at 72°C for 5 minutes; (4) the reaction was held at 4°C. The primers used for PCR amplification were as follows: forward primer, OPRM1-A118G-F, 5’-CACTGATGCCTTGGCGTACTC-3’; reverse primer, OPRM1-A118G-R, 5’-GGAGGGCACAGGCTGTCT-3’. Additionally, a subsequent pyrosequencing analysis employed an extension primer: OPRM1-A118G-S, 5’-GCATGGGTCGGACAGG-3’. The PCR products were purified and sequenced using the ABI3130 sequencer (Applied Biosystems, USA). Sequencing reagents were also provided by Applied Biosystems. The sequencing data were analyzed using Chromas software.
Statistical Analysis
Statistical analysis was performed using SPSS Statistics (version 22.0, IBM Corp., NY, USA). Descriptive data are presented as frequencies, percentages, and means ± standard deviations. Continuous variables were compared using Student’s t-test or Mann–Whitney U-test as appropriate. Categorical variables were compared using Pearson’s chi-square test or Fisher’s exact test. The relationship between gene variants and disease risk was assessed using unconditional logistic regression, with odds ratios (ORs) and 95% confidence intervals (CIs). Hardy-Weinberg equilibrium was used to calculate expected variant frequencies in the control group. Pairwise linkage disequilibrium (LD) (D’ and r2 values) and haplotype frequencies were determined with HAPLOVIEW version 4.2 (Broad Institute, Cambridge, MA), using the CI block definition. To control for type I errors arising from multiple comparisons across genotypes and time points, p-values were adjusted using the Bonferroni correction. The selection of statistical tests was based on data distribution and variable type. A P-value < 0.05 was considered statistically significant.
Results
Inclusion Process of the Recipients
The selection process began with 155 patients in the control group who underwent laparoscopic gynecological surgery between January 2019 and December 2021, and 152 patients in the Ondansetron group who underwent surgery between January 2022 and December 2024, as shown in Figure 1. Following the application of exclusion criteria, including missing data and specific comorbidities, 38 patients from the control group and 37 patients from the Ondansetron group were excluded, resulting in 117 patients in the control group and 115 patients in the Ondansetron group. Propensity score matching was subsequently conducted with a caliper value of 0.05, 86 patients from the control group and 85 from the Ondansetron group were retained for the final analysis. Post-matching standardized mean differences for all covariates were <0.1, confirming adequate group balance.
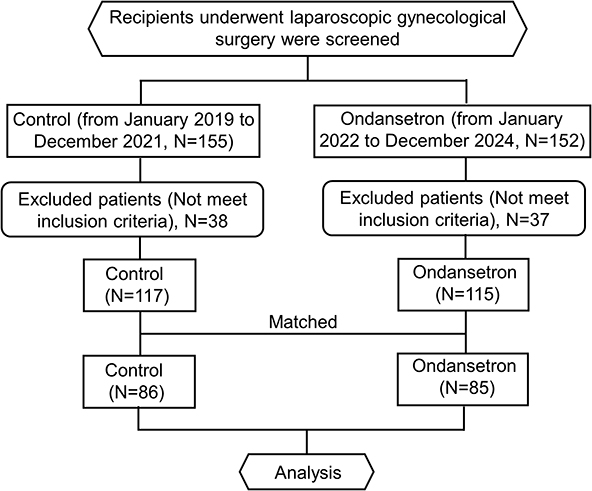 |
Figure 1 The inclusion process of the recipients who underwent laparoscopic gynecological surgery between the control group and the ondansetron group. |
The Comparison of Baseline Clinical Characteristics of the Study Cohort
The baseline clinical characteristics of the study cohort were compared, comprising 86 patients in the control group and 85 patients in the Ondansetron group (Table 1). The mean age of patients in the control group was 32.97 ± 7.24 years, while the Ondansetron group had a mean age of 33.13 ± 8.06 years (p = 0.8886). The mean body mass index (BMI) was 23.76 ± 2.33 kg/m2 in the control group and 24.02 ± 2.51 kg/m2 in the Ondansetron group (p = 0.4838). The distribution of ASA classifications was similar between these two groups, with 56.98% of patients in the control group and 55.29% in the Ondansetron group classified as ASA I (p = 0.8780). In terms of primary diseases, no significant differences were observed between these two groups, with comparable proportions of benign ovarian masses, infertility, and ectopic pregnancy (p = 0.9302). The mean anesthesia duration was 92.82 ± 28.65 minutes for the control group and 95.47 ± 24.86 minutes for the ondansetron group (p = 0.5194), while pneumoperitoneum times were 62.14 ± 17.23 minutes for the control group and 61.32 ± 17.15 minutes for the ondansetron group (p = 0.7559). Intraoperative blood loss was 1026.35 ± 224.09 mL in the control group and 986.72 ± 215.36 mL in the ondansetron group (p = 0.2401). The mean fentanyl dosage administered was 0.27 ± 0.03 mg in the control group and 0.26 ± 0.04 mg in the ondansetron group (p = 0.0986). This confirmed that baseline characteristics were well balanced following PSM.
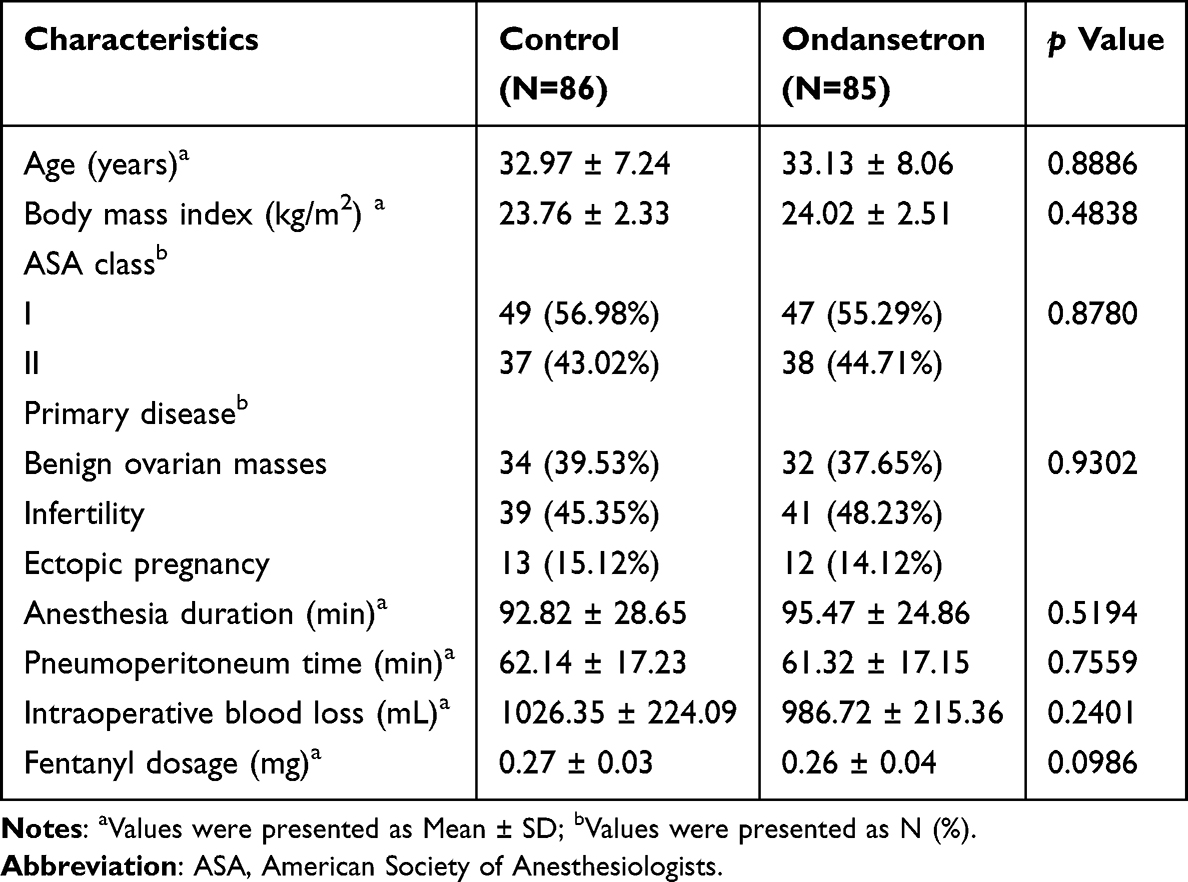 |
Table 1 Baseline Clinical Characteristics of the Study Cohort |
The Incidence and Severity of PONV at Different Times After Surgery
The incidence and severity of PONV at different postoperative intervals (0–2 h and 2–24 h) were compared between the control and Ondansetron groups (Table 2). These time intervals were selected according to the institutional protocol, which distinguishes early and delayed PONV phases. The incidence of PONV within the first 2 hours postoperatively was significantly lower in the ondansetron group (38.82%) compared to the control group (56.98%) (p = 0.0174). A similar trend was observed for the 2 to 24-hour period, with the ondansetron group exhibiting a significantly lower incidence of PONV (8.24%) than the control group (19.77%) (p = 0.0300). The mean VAS scores were also significantly lower in the Ondansetron group at both intervals (all p < 0.0001, Table 2). These findings suggested that ondansetron significantly reduced both the incidence and severity of PONV in patients undergoing laparoscopic gynecological surgery.
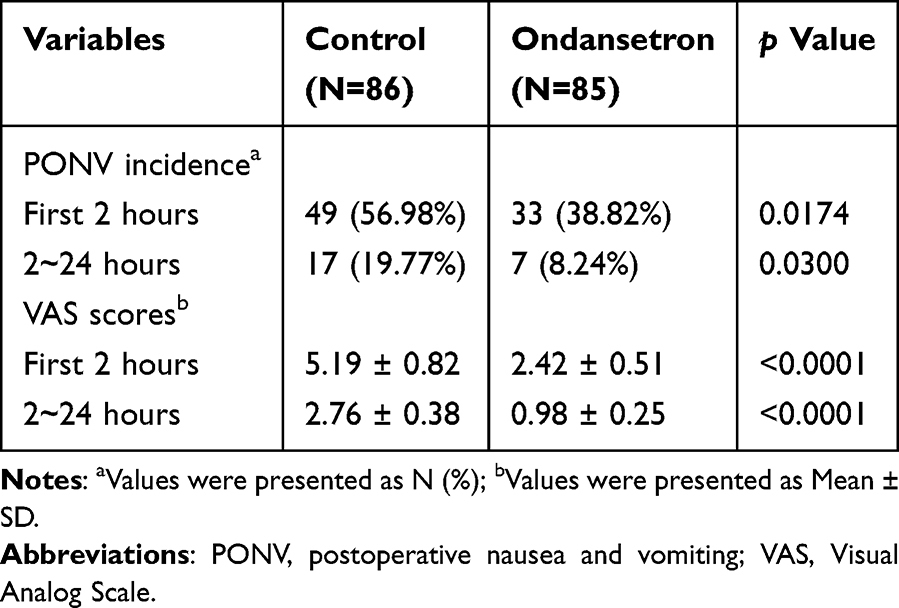 |
Table 2 The Incidence and Severity of PONV at Different Time After Surgery in Control Group and Ondansetron Group |
Frequency of Genotypes of OPRM1 A118G in the Control Group and the Ondansetron Group
To ensure comparability between cohorts, the distribution of OPRM1 A118G genotypes was analyzed in both the control and ondansetron groups (Table 3). In the control group, 43 patients (50.00%) exhibited the AA genotype, 30 patients (34.88%) had the AG genotype, and 13 patients (15.12%) carried the GG genotype. In the ondansetron group, 39 patients (45.88%) were homozygous for the AA genotype, 29 patients (34.12%) were heterozygous (AG), and 17 patients (20.00%) carried the GG genotype. Comparisons of genotype distributions between the two groups were performed using Pearson’s chi-square test, and no significant differences were observed for either the AG (p = 0.866) or GG (p = 0.523) genotypes relative to the AA reference. These results confirm that the OPRM1 A118G genotype frequencies were comparable between the control and ondansetron groups, indicating adequate baseline genetic balance prior to efficacy analyses.
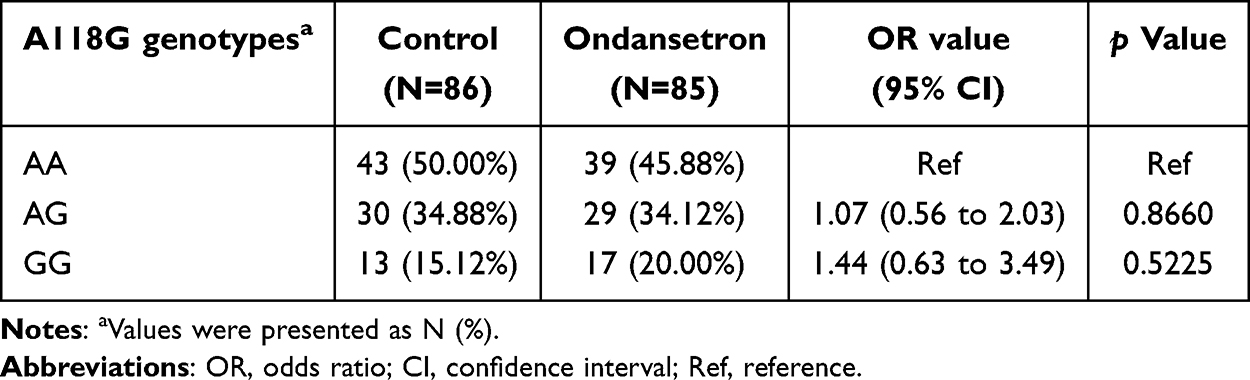 |
Table 3 Frequency of Genotypes of OPRM1 A118G in Control Group and Ondansetron Group |
Presence and the Incidence of PONV at Different Times After Surgery in Various OPRM1 A118G Genotypes in the Control Group
The association between the OPRM1 A118G polymorphism and the incidence of PONV was investigated. The PONV incidence at various time intervals following surgery was shown in Table 4, stratified by OPRM1 A118G genotypes in the control group. The analysis revealed a significant correlation between OPRM1 A118G genotypes and PONV occurrence within the first 2 hours postoperatively (p = 0.0009). Specifically, 37.21% of patients with the AA genotype, 80.00% with the AG genotype, and 69.23% with the GG genotype developed PONV. However, no significant association was observed between 2 and 24 hours (p = 0.2453). In contrast, when the cumulative incidence of PONV over the 0 ~ 24-hour period was assessed, a significant association with the OPRM1 A118G genotype was found (p = 0.0091), with 62.79% of patients with the AA genotype, 90.00% of those with the AG genotype, and 92.31% of those with the GG genotype experiencing PONV. To account for multiple comparisons across time points, raw p-values were adjusted using the Bonferroni method for controlling the false discovery rate, and the corrected analysis results confirmed that our initial main findings were robust. These findings suggested that the OPRM1 A118G polymorphism was significantly associated with the occurrence of PONV, particularly in the early postoperative period.
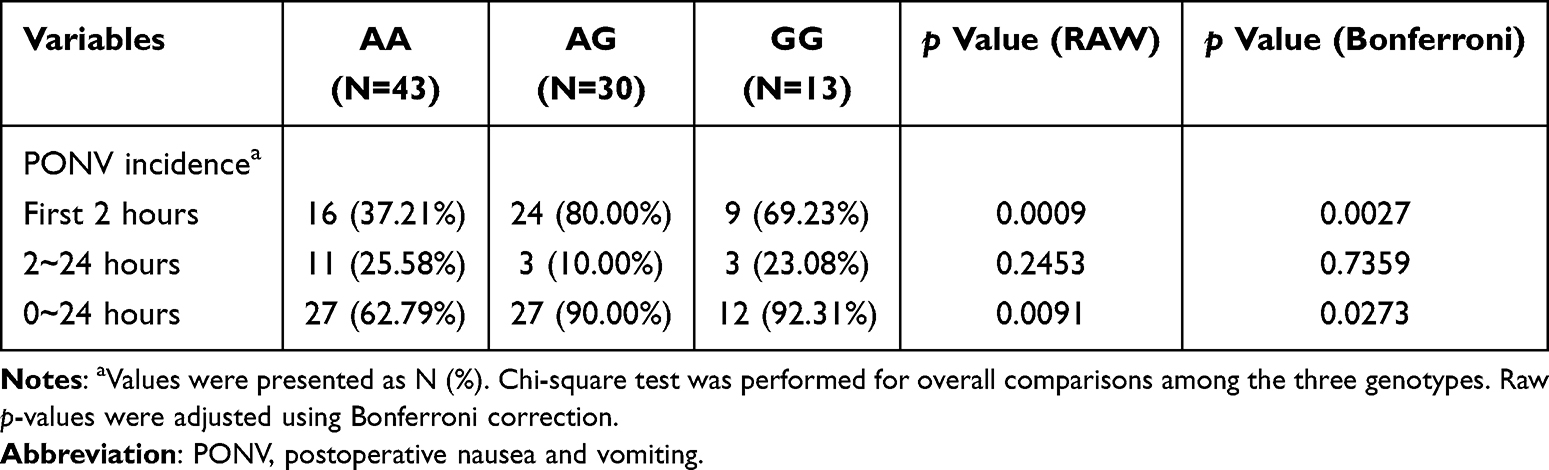 |
Table 4 Presence and the Incidence of PONV at Different Time After Surgery in Various OPRM1 A118G Genotypes in Control Group |
Presence and the Incidence of PONV at Different Times After Surgery in Various OPRM1 A118G Genotypes in the Ondansetron Group
Subsequently, the incidence of PONV at various time intervals following surgery in the ondansetron group was compared in Table 5, stratified by OPRM1 A118G genotypes. A significant association was observed between the OPRM1 A118G genotypes and the occurrence of PONV within the first 2 hours postoperatively (p = 0.0460). Specifically, 25.64% of patients with the AA genotype, 55.17% with the AG genotype, and 41.18% with the GG genotype experienced PONV. However, no significant differences were observed between genotypes regarding the incidence of PONV from 2 to 24 hours post-surgery (p = 0.8170). Additionally, no significant association was found between the OPRM1 A118G genotypes and the cumulative incidence of PONV over the 0 ~ 24 hour period (p = 0.1016), with 35.90% of AA genotype patients, 62.07% of AG genotype patients, and 47.06% of GG genotype patients reporting PONV. To account for multiple comparisons across the three time points, raw p-values were adjusted using the Bonferroni method for false discovery rate control, and the corrected analysis results confirmed that none of the comparisons remained statistically significant after adjustment. These findings suggested that the OPRM1 A118G polymorphism was not associated with the occurrence of PONV in the ondansetron group.
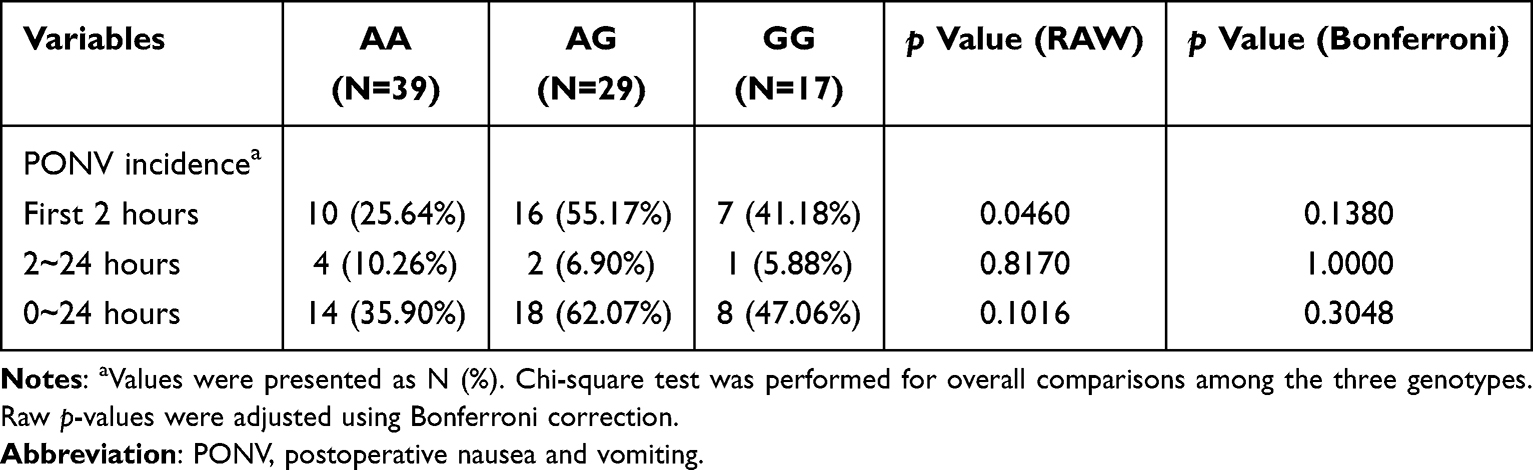 |
Table 5 Presence and the Incidence of PONV at Different Time After Surgery in Various OPRM1 A118G Genotypes in Ondansetron Group |
The Incidence of PONV in the First Two hours After Surgery in Various OPRM1 A118G Genotypes in Two Groups
The incidence of PONV within the first two hours after surgery was compared, stratified by OPRM1 A118G genotypes (AA, AG, and GG) in both the control and Ondansetron groups. In the control group, the incidence of PONV was significantly higher in patients with the AG and GG genotypes compared to those with the AA genotype, with 37.21% of AA, 55.17% of AG, and 59.23% of GG genotype patients experiencing PONV (Figure 2). In contrast, a significant reduction in PONV incidence was observed in the ondansetron group across all genotypes (Figure 2). Specifically, 25.64% of AA, 55.17% of AG, and 41.18% of GG genotype patients in the ondansetron group developed PONV (Figure 2). These findings indicated that the OPRM1 A118G polymorphism, particularly the presence of the G allele, was associated with an increased risk of PONV, and that the ondansetron treatment was effective in mitigating this risk, especially in patients with higher genetic susceptibility.
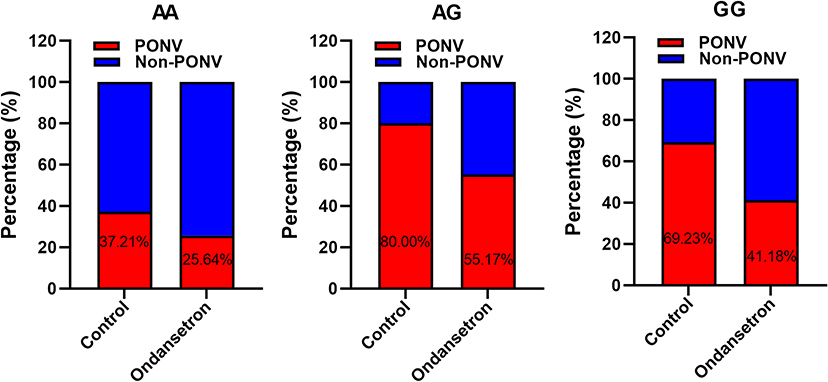 |
Figure 2 The incidence of PONV in the first two hours after surgery in various OPRM1 A118G genotypes in the control group and the ondansetron group. A118G genotypes, including AA, AG, and GG. Abbreviations: PONV, patients with postoperative nausea and vomiting; Non-PONV, patients without postoperative nausea and vomiting. |
Discussion
The application of SNPs for diagnosing PONV offers a significant advantage in identifying genetic susceptibility, facilitating precise risk stratification, and personalized therapeutic interventions. In contrast to traditional clinical risk factors, SNP analysis accounts for genetic variability, thereby elucidating discrepancies in PONV incidence among patients with similar clinical characteristics. Furthermore, SNP profiling can inform the selection of antiemetic therapies, as specific genotypes may modulate drug efficacy, optimizing treatment outcomes. Our findings demonstrated that the OPRM1 A118G polymorphism was significantly associated with the incidence of PONV, particularly in the early postoperative period. Patients carrying the AG and GG genotypes exhibited a higher risk of PONV within the first 2 hours following surgery, suggesting that genetic variability plays a role in PONV susceptibility. Furthermore, ondansetron was effective in reducing the incidence and severity of PONV across all genotypes, particularly in patients with higher genetic susceptibility, such as those with the AG and GG genotypes.
The clinical baseline characteristics of the study cohort showed good comparability between the groups in terms of age, BMI, ASA classification, disease distribution, and surgery-related parameters, consistent with several published studies. Other studies have emphasized the importance of baseline comparability to ensure valid analyses,22,23 which was achieved in this study through stringent inclusion criteria. Notably, some studies reported baseline differences related to race or gender,24,25 which were not addressed in this study’s stratified analyses. Compared to the standardized difference threshold of > 0.1 used in other studies to indicate clinical significance,26 the p-values in this study were well above this threshold, confirming stronger baseline balance.
Several studies have demonstrated that ondansetron significantly reduced the incidence and severity of PONV, which aligned with our findings of a reduction trend in PONV incidence at 0 ~ 2 hours and 2 ~ 24 hours.18,27 It has been reported that a single dose of ondansetron provided comparable efficacy to ramosetron in preventing PONV within 24 hours postoperatively,18 with VAS score improvement consistent with other studies assessing nausea severity.28,29 However, differences in the time window of assessment and duration of effect were noted. Some studies have extended the evaluation period to 48 hours,30 while this study restricted observation to a 24-hour postoperative period. Additionally, it has been reported that the combination of ondansetron and dexamethasone can further reduce the incidence of PONV to 12.5%,20 superior to the single-agent effect observed in our study. Furthermore, some studies suggested that ondansetron’s effect may diminish during the 2 ~ 6-hour postoperative period,31 whereas our study demonstrated sustained efficacy from 2 to 24 hours.
The genotype frequencies of OPRM1 A118G in the control and ondansetron groups were different from those reported in other studies. For instance, in the Saudi population, the A118G polymorphism showed 79.03% for AA, 16.13% for AG, and 4.84% for GG,14 whereas in the control group of this study, the frequencies were 50%, 34.88%, and 15.12%, respectively. This difference may be attributed to population heterogeneity. Additionally, the incidence of PONV within 2 hours postoperatively was significantly higher in patients with AG/GG genotypes compared to AA genotypes, consistent with findings15 that the G allele may impair μ-opioid receptor glycosylation, reducing opioid analgesic effects and increasing PONV risk.16 Furthermore, other research indicated that patients with both the OPRM1 A118G and BDNF G196A polymorphisms showed poorer pain relief,32 further supporting the role of the G allele in promoting postoperative adverse reactions.
Ondansetron significantly reduced the early incidence of PONV in patients with all genotypes, consistent with previous findings,19 suggesting that combining ondansetron with dexamethasone could further reduce the risk of PONV. Other studies have also confirmed that preoperative administration of ondansetron effectively prevents PONV within 24 hours postoperatively in breast cancer patients.33 These results collectively indicate that ondansetron had a consistent effect across patients with different genetic backgrounds. However, another study emphasized that the CYP2D6 metabolic phenotype, rather than the OPRM1 genotype, is a key factor influencing the efficacy of ondansetron.34
CYP2D6 polymorphisms influence the metabolism of opioids, such as codeine, morphine, and fentanyl, which are commonly used for postoperative pain management. Ultra-rapid metabolizers (UMs) metabolize opioids more quickly, leading to higher concentrations of active metabolites and an increased risk of opioid-induced side effects, including PONV. Conversely, poor metabolizers (PMs) may have reduced opioid efficacy, requiring higher doses for adequate pain relief, which could also increase the likelihood of PONV.35,36 Additionally, the interaction between opioids and ondansetron, a 5-HT3 receptor antagonist, may be affected by CYP2D6 polymorphisms. In ultra-rapid metabolizers, higher opioid doses may reduce ondansetron’s effectiveness due to overlapping effects on the vomiting center. Conversely, poor metabolizers might not achieve adequate pain control, complicating the clinical scenario.2,37 These genetic interactions suggest that CYP2D6 polymorphisms could be an important factor influencing PONV risk and antiemetic efficacy. Future studies combining OPRM1 and CYP2D6 polymorphism analyses could optimize PONV prevention strategies, particularly in genetically susceptible individuals.38 Pharmacogenetic testing for both OPRM1 and CYP2D6 could help personalize PONV treatment, improving efficacy and safety while reducing unnecessary opioid use.
Additionally, it was reported that no significant association was found between the OPRM1 A118G polymorphism and opioid-related adverse reactions.39,40 These discrepancies may arise from differences in study design, as this study focused on early PONV within 2 hours postoperatively, whereas other studies assessed long-term adverse reactions. This study found that the OPRM1 A118G polymorphism was significantly associated with PONV only within 2 hours postoperatively, while the cumulative incidence within 24 hours did not show a statistically significant difference in the ondansetron group. In contrast, the combination of Aprepitant and ondansetron has been shown to continuously reduce the risk of PONV over 24 hours, suggesting that genetic sensitivity to different antiemetic drugs may vary depending on the time window.20 Furthermore, the PONV risk in patients with preoperative anxiety was found to be unrelated to the efficacy of ondansetron, further indicating that non-genetic factors may obscure the gene-drug association in PONV.41
This study highlights the clinical implications of the OPRM1 A118G polymorphism in managing PONV in laparoscopic gynecological surgery. It revealed that patients with AG and GG genotypes had a higher risk of PONV, particularly in the first two hours after surgery. Genetic screening for OPRM1 A118G could help identify high-risk patients, enabling more personalized treatment. Ondansetron was effective in reducing PONV across all genotypes, with a greater impact on those with higher genetic susceptibility (AG and GG). These findings suggested that combining ondansetron with other agents like dexamethasone may further benefit high-risk patients. Ultimately, incorporating genetic testing into PONV management could enhance treatment strategies, improving patient outcomes and reducing complications.
Although OPRM1 A118G genotyping provides valuable predictive information for personalized PONV management, its clinical implementation should consider cost and feasibility. The cost of genotyping using PCR and sequencing methods typically ranges between USD 20–50 per sample, depending on the laboratory platform and throughput. This cost is relatively low compared with the overall perioperative care expenses and could be justified for patients at high risk of PONV or those with repeated postoperative emetic episodes. However, large-scale cost–benefit analyses are needed to determine whether routine OPRM1 genetic screening is economically viable in clinical anesthetic practice.
This study still has several limitations. First, the retrospective design limits the ability to establish causal relationships between the OPRM1 A118G polymorphism and PONV, as it relies on pre-existing data and may be subject to biases, such as selection bias and incomplete data. Additionally, the inclusion of cohorts from different time periods may introduce temporal bias, which could affect the consistency of the findings over time. Furthermore, although the sample size is adequate for statistical analysis, it may not fully represent genetic variability across different populations, limiting the generalizability of the findings. For example, the small sample size in the subgroup sizes for GG genotype limits the statistical power to detect moderate effects. These results should be interpreted as preliminary, and further studies with larger cohorts and more diverse populations are needed to confirm these findings. Additionally, the study focused on a 24-hour postoperative period, which does not account for the long-term effects of ondansetron. Lastly, the study did not account for other potentially relevant polymorphisms (eg, CYP2D6) or perioperative interventions (eg, non-antiemetic medications), which may influence PONV outcomes. These factors should be considered in future research to minimize confounding. Future prospective studies involving larger, more heterogeneous cohorts and extended follow-up periods are required to validate and further investigate these findings.
Conclusion
In conclusion, OPRM1 A118G polymorphism is significantly associated with an increased risk of PONV, particularly within the first 2 hours following surgery. However, it is important to note that the findings are based on a 24-hour observation period, and the long-term effects of ondansetron were not assessed in this study. Ondansetron effectively mitigated PONV across all genotypes, with enhanced efficacy observed in patients with higher genetic susceptibility. Future studies incorporating pharmacogenetic testing, particularly OPRM1 and CYP2D6 polymorphisms, may help optimize PONV prevention strategies.
Data Sharing Statement
Data are available on reasonable request.
Ethical Approval
The study was approved by Shandong Provincial Hospital Affiliated to Shandong First Medical University (#2025-03-207). Given the retrospective design and use of de-identified data, the requirement for individual informed consent was waived. The study was performed in strict accordance with the Declaration of Helsinki, Ethical Principles for Medical Research Involving Human Subjects.
Informed Consent
All patients signed the informed consent.
Funding
This study was funded by Horizontal project of the Medical Association (YXH2022ZX02080), and Youth Project of Shandong Provincial Natural Science Foundation (ZR2020QH078).
Disclosure
The authors report no conflicts of interest int his work.
References
1. Timerga S, Befkadu A. Prevalence and associated factors of postoperative nausea and vomiting among adult patients undergoing elective surgery. Ann Med Surg Lond. 2024;86(3):1304–1308. doi:10.1097/MS9.0000000000001678
2. Ahlstrom SE, Bergman PH, Jokela RM, Olkkola KT, Kaunisto MA, Kalso EA. Clinical and genetic factors associated with post-operative nausea and vomiting after propofol anaesthesia. Acta Anaesthesiol Scand. 2023;67(8):1018–1027. doi:10.1111/aas.14261
3. Pratt S, Howard-Ruben J. Implementation of electronic postoperative nausea and vomiting assessment and best practice advisory tools to improve patient care. J Nurs Care Qual. 2024;39(2):136–143. doi:10.1097/NCQ.0000000000000735
4. Nagase S, Imaura M, Nishimura M, et al. Usefulness of criteria for intraoperative management of postoperative nausea and vomiting. J Pharm Health Care Sci. 2022;8(1):11. doi:10.1186/s40780-022-00242-1
5. Ma W, Qi Y, Liu C, Wang M, Zhang Y, Yao W. Effect of individualized treatment strategy on postoperative nausea and vomiting in gynaecological laparoscopic surgery: a double-blind, randomized, controlled trial. BMC Anesthesiol. 2022;22(1):266. doi:10.1186/s12871-022-01809-z
6. Knoth S, Weber B, Lotz H, Vojnar B, Eberhart LHJ. Update PO(N)V - Was gibt es Neues zu Prophylaxe und Therapie von Ubelkeit und Erbrechen nach Operationen? [Update PO(N)V-what is new in the prophylaxis and treatment of postoperative nausea and vomiting?]. Anaesthesiologie. 2025;74(3):171–186. doi:10.1007/s00101-025-01510-z
7. Goss S, Jedlicka J, Strinitz E, et al. Association between intraoperative hypotension and postoperative nausea and vomiting: a retrospective cohort study. Curr Med Res Opin. 2024;40(8):1439–1448. doi:10.1080/03007995.2024.2373885
8. Hussein AM, Yasin JA, Aldalati AY, et al. Olanzapine for the prevention of postoperative nausea and vomiting: an updated meta-analysis with trial sequential analysis. J Pain Symptom Manage. 2025;69(5):e359–e373. doi:10.1016/j.jpainsymman.2025.02.003
9. Aghazarian GS, Lind R, Motola D, et al. Impact of emend on perioperative bariatric surgery antiemetic utilization, patient satisfaction, and costs. Surg Laparosc Endosc Percutan Tech. 2023;33(3):265–269. doi:10.1097/SLE.0000000000001101
10. Zhang R, Zhang WX, Ma XR, Feng Y. Intraoperative sufentanil consumption and the risk of postoperative nausea and/or vomiting: a retrospective observational study. Pain Ther. 2023;12(5):1271–1281. doi:10.1007/s40122-023-00546-6
11. Belkacemi L, Darmani NA. Dopamine receptors in emesis: molecular mechanisms and potential therapeutic function. Pharmacol Res. 2020;161:105124. doi:10.1016/j.phrs.2020.105124
12. Nakagawa M, Kuri M, Kambara N, et al. Dopamine D2 receptor Taq IA polymorphism is associated with postoperative nausea and vomiting. J Anesth. 2008;22(4):397–403. doi:10.1007/s00540-008-0661-z
13. Kirsch P, Reuter M, Mier D, et al. Imaging gene-substance interactions: the effect of the DRD2 TaqIA polymorphism and the dopamine agonist bromocriptine on the brain activation during the anticipation of reward. Neurosci Lett. 2006;405(3):196–201. doi:10.1016/j.neulet.2006.07.030
14. Bagher AM, Hareeri RH. Allele frequency and genotype distribution of the opioid receptor mu-1 (OPRM1) A118G polymorphism in the Western Saudi population. J Appl Biomed. 2023;21(3):160–165. doi:10.32725/jab.2023.012
15. Takemura M, Niki K, Okamoto Y, et al. Comparison of the effects of OPRM1 A118G polymorphism using different opioids: a prospective study. J Pain Symptom Manage. 2024;67(1):39–49e35. doi:10.1016/j.jpainsymman.2023.09.017
16. Zhou Y, Cao L, Yang Y, et al. Is OPRM1 genotype a valuable predictor of VAS in patients undergoing laparoscopic radical resection of colorectal cancer with fentanyl? BMC Anesthesiol. 2023;23(1):173. doi:10.1186/s12871-023-02120-1
17. Nishizawa D, Morino R, Inoue R, et al. Genome-wide association study identifies novel candidate variants associated with postoperative nausea and vomiting. Cancers. 2023;15(19):4729. doi:10.3390/cancers15194729
18. Das S, Kumar A, Gupta A, Kumar A. A randomised controlled trial to compare the effect of ramosetron and ondansetron in prevention of postoperative nausea and vomiting in patients undergoing laparoscopic gynaecological procedures. Cureus. 2022;14(9):e29200. doi:10.7759/cureus.29200
19. Shirozu K, Umehara K, Takamori S, Takase S, Yamaura K. Associations between ondansetron and the incidence of postoperative nausea and vomiting and food intake in Japanese female undergoing laparoscopic gynecological surgery: a retrospective study. J Anesth. 2024;38(2):185–190. doi:10.1007/s00540-023-03295-0
20. Singh MP, Gurunthalingam MP, Gupta A, Singh J. Comparison of aprepitant versus ondansetron for prevention of postoperative nausea and vomiting: a systematic review and meta-analysis with trial sequential analysis. Indian J Anaesth. 2024;68(9):762–775. doi:10.4103/ija.ija_106_24
21. Faiz KW. VAS--visual analog scale. Tidsskr nor Laegeforen. 2014;134(3):323. doi:10.4045/tidsskr.13.1145
22. Lho Y, Kim GO, Kim BY, Son EJ, Kang SH. Effects of administration and intensity of statins on mortality in patients undergoing hemodialysis. Pharmaceuticals. 2024;17(4):498. doi:10.3390/ph17040498
23. Morsi S, Ghozy S, Elfil M, et al. Endovascular thrombectomy for dawn- and DEFUSE-3 ineligible acute ischemic stroke patients: a systematic review and meta-analysis. J Neurol. 2024;271(5):2230–2237. doi:10.1007/s00415-024-12198-3
24. Forcadell-Peris MJ, Vila-Corcoles A, de Diego-Cabanes C, Torras Vives V, Ochoa-Gondar O, Satue-Gracia EM. Evaluating sex differences in pneumococcal disease burden and vaccination effectiveness in adults: a population-based study. J Infect Dis. 2025;231(6):1455–1464. doi:10.1093/infdis/jiae624
25. Kang DY, Ahn JM, Kim JB, et al. Inter-racial differences in patients undergoing transcatheter aortic valve implantation. Heart. 2022;108(19):1562–1570. doi:10.1136/heartjnl-2021-320364
26. Dugard A, Giraudeau B, Dibao-Dina C. Do patients with type 2 diabetes mellitus included in randomised clinical trials differ from general-practice patients? A cross-sectional comparative study. BMJ Open. 2024;14(4):e077582. doi:10.1136/bmjopen-2023-077582
27. Krishnan D, Asokan A, Muthalu A, Suganya S, Sujatha C. A Comparative Study on the Efficacy of Intravenous Palonosetron Versus a Combination of Ondansetron and Dexamethasone as Prophylaxis for Prevention of Postoperative Nausea and Vomiting After Laparoscopic Surgeries. Cureus. 2024;16(10):e72214. doi:10.7759/cureus.72214
28. Wang M, Tong H, Liu Q, et al. Effect of magnetic ball pressing combined with TEAS on postoperative nausea, pain, comfort, and satisfaction in patients undergoing gynecological laparoscopic surgery: a randomized controlled trial. J Perianesth Nurs. 2025;40(4):979–985. doi:10.1016/j.jopan.2024.11.001
29. Zeng M, Li J, Zheng T, Yan X, Yuan F, Xiang B. Electropress needle stimulation for the prevention of postoperative nausea and vomiting in patients undergoing laparoscopic sleeve gastrectomy: a prospective, randomized controlled trial. Obes Surg. 2023;33(9):2831–2840. doi:10.1007/s11695-023-06752-7
30. Long YQ, Wang D, Chen S, et al. Effect of balanced opioid-free anaesthesia on postoperative nausea and vomiting after video-assisted thoracoscopic lung resection: protocol for a randomised controlled trial. BMJ Open. 2022;12(11):e066202. doi:10.1136/bmjopen-2022-066202
31. Yan S, Xu M, Zou X, et al. Acupuncture combined with ondansetron for prevention of postoperative nausea and vomiting in high-risk patients undergoing laparoscopic gynaecological surgery: a randomised controlled trial. United Eur Gastroenterol J. 2023;11(6):564–575. doi:10.1002/ueg2.12421
32. Goncalves FT, Pacheco-Barrios K, Rebello-Sanchez I, et al. Association of Mu opioid receptor (A118G) and BDNF (G196A) polymorphisms with rehabilitation-induced cortical inhibition and analgesic response in chronic osteoarthritis pain. Int J Clin Health Psychol. 2023;23(1):100330. doi:10.1016/j.ijchp.2022.100330
33. Li C, Cui W, Song P, Liu W, Wang X, Yang Q. Effect of ondansetron for preventing postoperative nausea and vomiting after breast cancer surgery. Am J Transl Res. 2022;14(9):6689–6695.
34. Moore C, Williams E, Dyas R, et al. CYP2D6 genotype and associated 5-HT(3) receptor antagonist outcomes: a systematic review and meta-analysis. Clin Transl Sci. 2025;18(2):e70108. doi:10.1111/cts.70108
35. Aroke EN, Hicks TL. Pharmacogenetics of postoperative nausea and vomiting. J Perianesth Nurs. 2019;34(6):1088–1105. doi:10.1016/j.jopan.2019.03.007
36. Niewinski PA, Wojciechowski R, Sliwinski M, et al. CYP2D6 basic genotyping as a potential tool to improve the antiemetic efficacy of ondansetron in prophylaxis of postoperative nausea and vomiting. Adv Clin Exp Med. 2018;27(11):1499–1503. doi:10.17219/acem/69451
37. Janicki PK. Cytochrome P450 2D6 metabolism and 5-hydroxytryptamine type 3 receptor antagonists for postoperative nausea and vomiting. Med Sci Monit. 2005;11(10):RA322–328.
38. Theodosopoulou P, Rekatsina M, Staikou C. The efficacy of 5HT3-receptor antagonists in postoperative nausea and vomiting: the role of pharmacogenetics. Minerva Anestesiol. 2023;89(6):565–576. doi:10.23736/S0375-9393.22.16983-X
39. Xie X, Gu J, Zhuang D, et al. Association between rs1799971 in the mu opioid receptor gene and methadone maintenance treatment response. J Clin Lab Anal. 2022;36(11):e24750. doi:10.1002/jcla.24750
40. Ershad A, Shafiee Dolat Abadi S, Ebrahimian M, et al. Association of the OPRM1 variant rs1799971 (A118G) and clinical manifestations in tramadol poisoned patients: a cross-sectional study. Clin Toxicol. 2024;62(6):357–363. doi:10.1080/15563650.2024.2366921
41. Mou Y, Zhao W, Pan W, et al. A comparison of ondansetron in preventing postoperative nausea and vomiting for patients with or without preoperative anxiety with painless egg retrieval: a prospective, randomized, controlled trial. Gland Surg. 2024;13(8):1522–1534. doi:10.21037/gs-24-175
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.