Back to Journals » Journal of Pain Research » Volume 13
Opioid-Sparing Anesthetic Technique for Pediatric Patients Undergoing Adenoidectomy: A Pilot Study
Authors Alghamdi F, Roth C ![]() , Jatana KR, Elmaraghy CA, Rice J, Tobias JD
, Jatana KR, Elmaraghy CA, Rice J, Tobias JD ![]() , Thung AK
, Thung AK
Received 9 September 2020
Accepted for publication 11 November 2020
Published 19 November 2020 Volume 2020:13 Pages 2997—3004
DOI https://doi.org/10.2147/JPR.S281275
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Robert B. Raffa
Faris Alghamdi,1 Catherine Roth,1 Kris R Jatana,2 Charles A Elmaraghy,2 Julie Rice,1 Joseph D Tobias,1 Arlyne K Thung1
1Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital and the Ohio State University College of Medicine, Columbus, OH, USA; 2Department of Otolaryngology and Head & Neck Surgery, Nationwide Children’s Hospital and the Ohio State University, Columbus, OH, USA
Correspondence: Arlyne K Thung
Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, 700 Children’s Drive, Columbus, OH 43205, USA
Tel +1 614 722-4200
Fax +1 614 722-4203
Email [email protected]
Introduction: An opioid-sparing anesthetic involves a multi-modal technique with non-opioid medications targeting different analgesic pathways. Such techniques may decrease adverse effects related to opioids. These techniques may be considered in patients at higher risk for opioid-related adverse effects including obstructive sleep apnea or sleep disordered breathing.
Methods: A prospective, pilot study was performed in 10 patients (3– 8 years of age), presenting for adenoidectomy. The perioperative regimen included oral dextromethorphan (1 mg/kg) and acetaminophen (15 mg/kg) plus single boluses of intraoperative dexmedetomidine (0.5 μg/kg) and ketamine (0.5 mg/kg). Pain scores were assessed in the post anesthesia care unit (PACU) using the FLACC (Face, Legs, Activity, Cry, Consolability) scale. Patients with a pain score > 4 received fentanyl as needed. PACU time, pain scores, and parent satisfaction were recorded. Postoperatively, patients were instructed to use oral acetaminophen or ibuprofen every 6 hours as needed for pain.
Results: The study cohort included 10 patients, 3– 8 years of age. All patients had opioid-free anesthetic care. PACU time ranged from 24 to 102 minutes (median: 56 minutes). FLACC pain scores were 0 for all PACU assessments. Nine patients were discharged home and 1 patient had a planned overnight admission. Following hospital discharge, the pain scores were satisfactory during the 72-hour study period and 90% of the patients’ guardians were satisfied or highly satisfied with their child’s pain control.
Conclusion: This opioid-sparing approach provided safe and effective pain control as well as parental satisfaction following adenoidectomy in children. Additional prospective studies are needed to determine whether this regimen is effective in a larger cohort of patients with and for other otolaryngology procedures.
Keywords: opioid, sparing, analgesia, pediatric, adenoidectomy
Introduction
Adenoidectomy is one of the most common surgeries performed in the pediatric population.1,2 Some of the most frequent indications for surgery include chronic or recurrent otitis media, chronic sinusitis, nasal obstruction, and snoring. Many pediatric patients who have snoring symptoms also have associated SDB or OSA. Adenoidectomy is often performed in conjunction with tonsillectomy; however, it may be performed alone with or without tympanostomy tube placement in the ambulatory setting. Although considered less painful than tonsillectomy, adenoidectomies require pharmacological therapy to manage perioperative pain. Opioid medications remain the mainstay of treatment for postoperative pain despite the associated adverse effect profile, which may be exaggerated in patients with SDB or OSA.3–5 For these patients, the decision to undergo these otolaryngologic procedures and the use of perioperative opioids often mandates prolonged periods of observation or overnight hospital admission due to the potential risk of postoperative respiratory depression.6,7
An opioid-sparing anesthetic technique includes adjunctive non-opioid agents using a multi-modal approach employing a combination of non-opioid medications which target various analgesic pathways.8 These techniques are becoming more popular not only to decrease the incidence of adverse effects related to opioids, but in identifying clinical opportunities to minimize opioid use amidst the backdrop of the national opioid crisis which affects both the adult and pediatric population.9,10 To date, these techniques have been successful in managing pain following various surgical procedures in pediatric patients.8,11–13 The current pilot studies outline a non-opioid technique using a combination of adjunctive agents (acetaminophen, dextromethorphan, ketamine and dexmedetomidine) with analgesic effects in a cohort of children undergoing adenoidectomy. We hypothesized that this technique would provide intraoperative analgesia, postoperative pain management, and facilitate performance of this surgical procedure without the need for perioperative opioids. The goal was to standardize this protocol, demonstrate safety and efficacy through the absence of unanticipated adverse events necessitating unplanned prolonged hospitalization and need for breakthrough pain medication, with the future expansion to a larger cohort including other otolaryngologic procedures.
Methods
This was a prospective pilot study approved by the Institutional Review Board of Nationwide Children’s Hospital (IRB 18-00235). It was conducted in accordance with the regulations of the Declaration of Helsinki for research involving human subjects. The study was registered at Clinicaltrials.gov (NCT03714919). A parent or legal guardian of eligible patients was approached after their preoperative visit with their pediatric otolaryngologist who described the study and asked if they would be willing to allow their child to participate in the opioid-sparing technique. Written informed consent was obtained on the day of surgery. Each patient was followed by a research coordinator throughout the perioperative process which began from the time of enrollment in the preoperative area until discharge from the post anesthesia care unit (PACU).
Eligible patients were those ranging in age from 3 to 8 years of age undergoing adenoidectomy with or without tympanostomy tube placement. Subjects were required to have a parent/guardian who was compliant with routine medical care, capable of subjective evaluation of pain, and able to read, understand and sign the informed consent. Exclusion criteria included patients who had an American Society of Anesthesiologists’ Physical Status ≥4, a known hypersensitivity or allergy to any of the study medications (acetaminophen, dextromethorphan, ketamine, dexmedetomidine, fentanyl), patients who were receiving chronic opioid analgesic therapy prior to surgery, renal disease, hepatic disease, and obesity (body mass index greater than 99th % for age).
Study patients received a standardized anesthetic technique consisting of oral dextromethorphan (1 mg/kg), oral acetaminophen (15 mg/kg), and oral premedication with midazolam (0.3 mg/kg) administered in the preoperative holding area prior to surgery. A lower dose of midazolam was selected to minimize potential additive sedation from the multiple study medications while providing preoperative anxiolysis to all subjects. These medications were administered 15–20 minutes prior to the induction of anesthesia by the inhalation of sevoflurane in a combination of nitrous and oxygen. Following the induction of anesthesia, a peripheral intravenous catheter was placed and propofol (1–1.5 mg/kg) administered to facilitate endotracheal intubation. Intravenous dexmedetomidine (0.5 µg/kg) and intravenous ketamine (0.5 mg/kg) were then also administered. Isoflurane was administered for maintenance anesthesia, titrated to maintain the bispectral index at 50–60 in a combination of air and oxygen with an inspired oxygen concentration of less than 30% to limit the risk of airway fire. All patients received prophylaxis for postoperative nausea and vomiting with ondansetron (0.15 mg/kg) and dexamethasone (0.25 mg/kg). Intraoperative fluid therapy included a minimum of 20–40 mL/kg of lactated ringers. The study medications of acetaminophen, dextromethorphan, dexmedetomidine and ketamine were prepared by research pharmacy with dosing for each medication guided by previously published data. All study medications were controlled by Investigational Drug Services following Research Pharmacy SOPs for the Control of Investigational Drugs.
Following completion of the surgical procedure, the patient was transported to the PACU where tracheal extubation occurred according to our usual routine for rapid turnover of the operating room.14 Baseline vital signs were obtained and pain scores assessed using the FLACC scale (Faces, Legs, Activity, Cry, Consolability).15 The presence of emergence delirium was measured using the PAED scale (Pediatric Agitation and Emergence Delirium).16 Those subjects whose pain score was assessed at <4 received standard postoperative care and no analgesic agents, whereas subjects whose assessed pain scores were >4 received fentanyl (0.5 µg/kg) every 10 minutes as needed.
Variables recorded included time to tracheal extubation, time to first analgesic delivery in the PACU; pain scores, heart rate, blood pressure, and oxygen saturation at PACU arrival and post arrival time points at 5 minutes, 15 minutes, 30 minutes, 45 minutes and 60 minute time points, number of doses of fentanyl administered in the PACU, presence of nausea/vomiting; presence of sedation, presence of respiratory complications as defined by oxygen saturation <90% requiring intervention in the form of supplemental oxygen or pharmacological management, and total PACU time.
Subjects were discharged home from the PACU once standard discharge criteria were met with instructions to administer appropriate weight-based doses of oral acetaminophen every 6 hours as needed for pain with additional ibuprofen every 6 hours for break through pain. Families of study subjects were also given a pain diary to record pain scores using the Wong Baker FACES scale17 and analgesic use from hospital discharge to 72 postoperative hours. A member of the study team contacted a parent or guardian by telephone to obtain this information, answer any questions regarding post-anesthetic recovery, and evaluate their satisfaction with the anesthetic and analgesic care (1–5 scale; 5 = highly satisfied).
The primary outcome was the analgesic efficacy of a multi-modal, non-opioid analgesic regimen for providing surgical analgesia in pediatric patients undergoing adenoidectomy ± tympanostomy tube placement and if there was a need for rescue opioid analgesia in the PACU. The secondary objective was to assess recovery characteristics in the PACU and at home following surgery. Categorical variables were reported as counts with percentages and continuous variables were reported as medians with interquartile ranges.
Results
The study cohort included 10 pediatric patients, ranging in age from 3–8 years, with an ASA physical classification, of 1 or 2. The surgical procedure included adenoidectomy (n=4) or adenoidectomy with myringotomy tube placement (n=6). Patient demographics are outlined in Table 1. Surgical, anesthetic, and postoperative outcomes are listed in Table 2. All of the patients had an opioid-free experience for the entirety of their anesthetic care. As per our institutional standard of care, tracheal extubation was performed in PACU. FLACC pain scores were 0 for all PACU assessments for all patients. The median time from end of the surgical procedure to tracheal extubation was 23 minutes. Total PACU length of stay had a median of 56 minutes with an IQR (interquartile range) of 49 to 65 minutes. Emergence delirium was assessed using the Pediatric Agitation and Emergence Delirium Scale (PAED, Table 3). Although PAED scores were uniformly 12 at the first 3 assessment times, this was due to recovery from anesthesia and not agitation as the patients were not responsive to commands. In this time frame, the children were recovering from anesthesia until they were extubated. Assessment points for PAED at 30 minutes and beyond were generally ≤5 with no patient being restless. Similarly, sedation was noted in 7 out of 10 patients during the early PACU course as they were emerging from anesthesia until tracheal extubation which occurred at a median time for 23 minutes after completion of the surgical procedure. One patient had an episode of nausea and vomiting. Vital signs in the first postoperative hour were within normal limits (Table 4). Median time from the end of surgery to hospital discharge was 122 minutes. Nine patients were discharged home while 1 patient had a planned admission who did not receive additional opioids during the post procedure hospitalization. No medication reactions nor any other complications were seen. Following discharge, the pain scores for the initial 72 postoperative hours were within acceptable ranges (Table 4). One patient did not take any supplemental acetaminophen or ibuprofen after hospital discharge while the remaining 9 received acetaminophen or ibuprofen on at least one postoperative day within the 72-hour recording period. Five of 10 patients’ guardians were highly satisfied with their child’s pain control, four were satisfied, and one was dissatisfied due to high pain scores following discharge home on postoperative days 1–3 (Table 5).
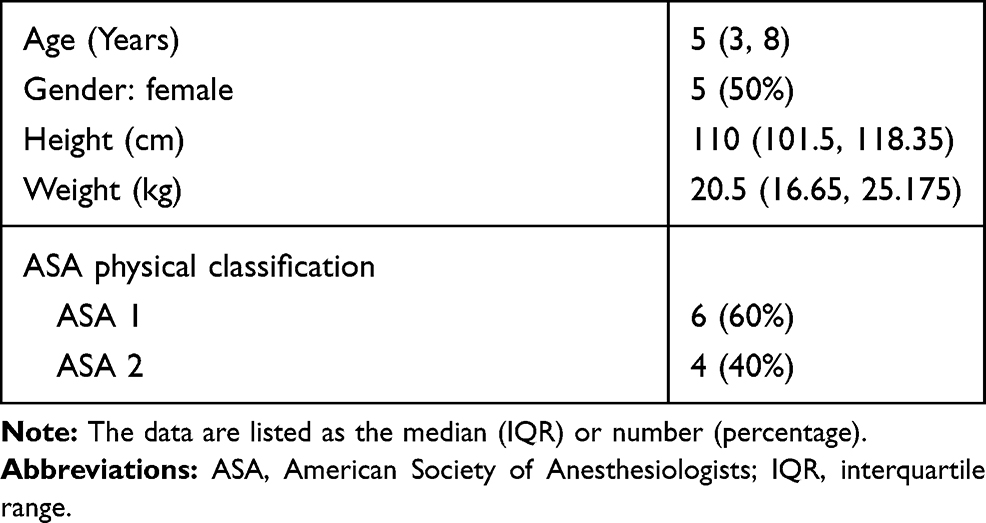 |
Table 1 Demographics of the Study Cohort |
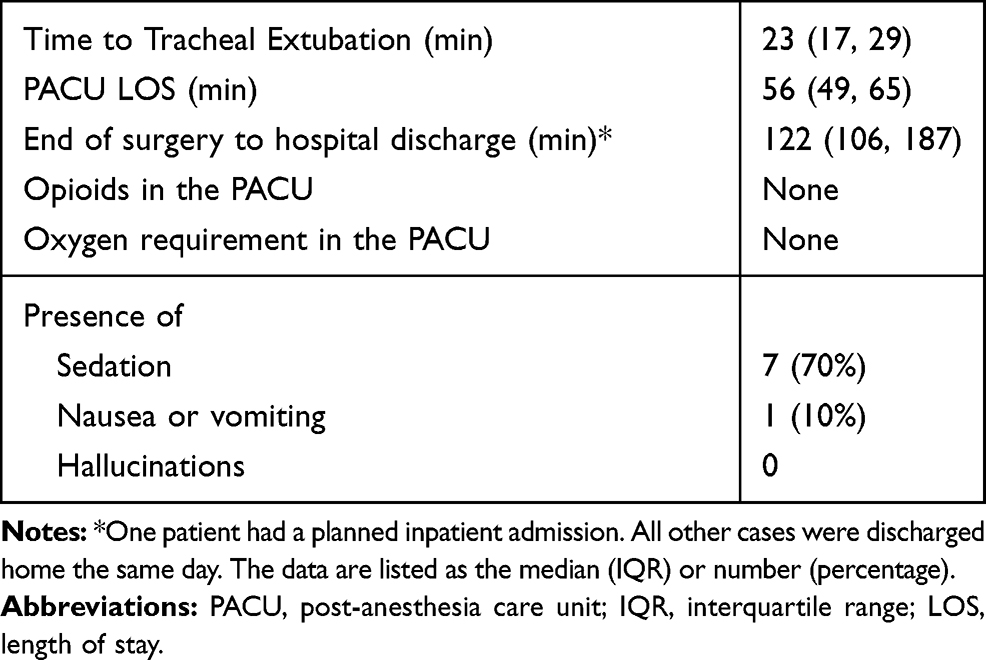 |
Table 2 Postoperative Outcomes |
 |
Table 3 Pediatric Anesthesia Emergence Delirium Scale |
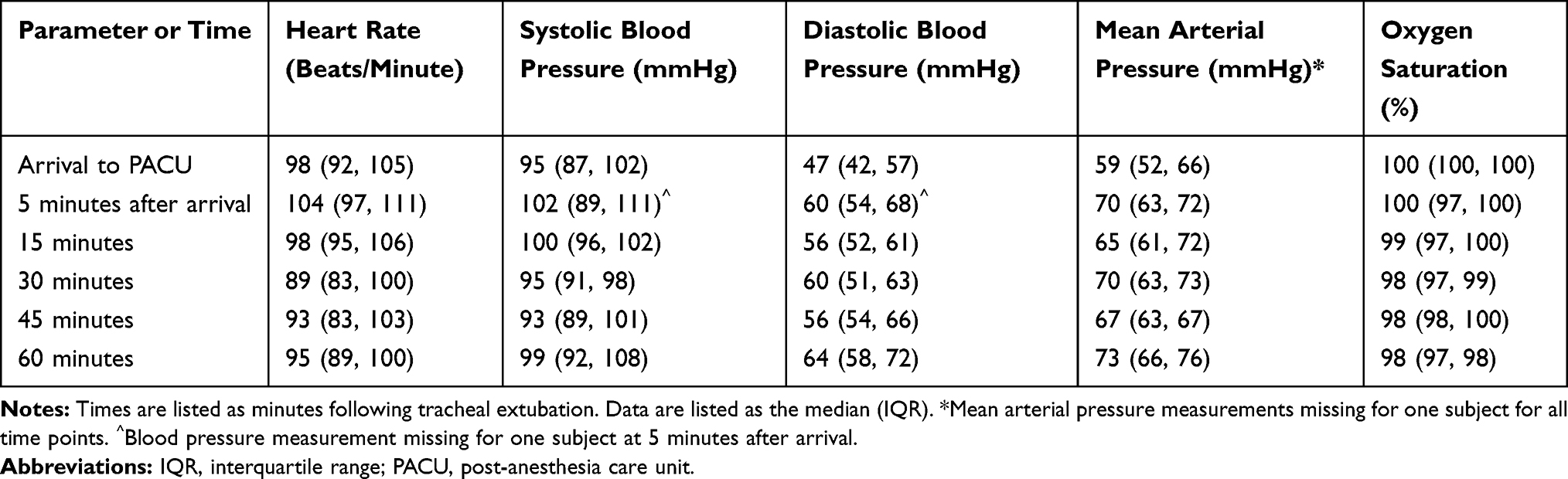 |
Table 4 Postoperative Vital Signs in the Study Cohort |
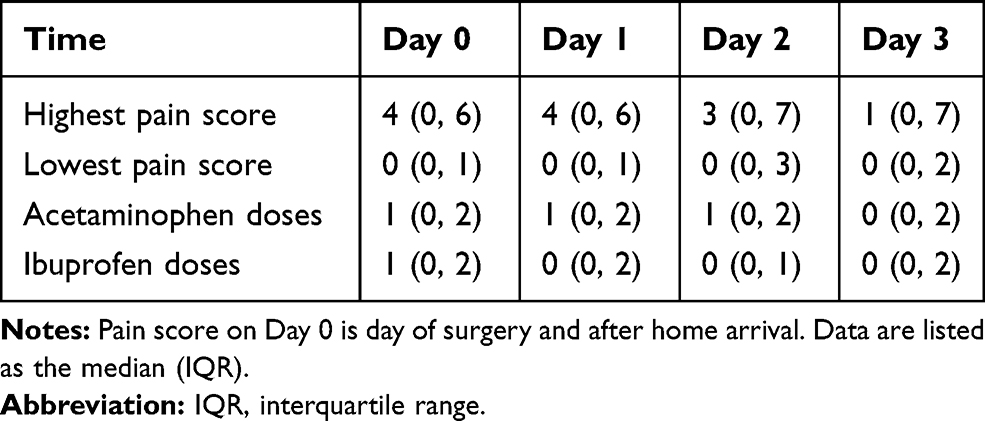 |
Table 5 Clinical Outcomes Following Discharge |
Discussion
In 1853, opioids were introduced into medical practice and have remained the mainstay of pain management for acute postoperative pain. Techniques that provide opioid-sparing analgesia have come into practice to minimize the need for opioids and thus limiting the opioid-related adverse effects to enhance recovery in various perioperative protocols for enhanced recovery after surgery or ERAS, expedite hospital discharge after surgery, and to address the growing concerns regarding opioid diversion, dependency, and addiction. These techniques aimed at enhanced recovery following surgery use adjunctive agents that act through various non-opioid receptors including: acetaminophen, non-steroidal anti-inflammatory agents, α2-adrenergic agonists (clonidine or dexmedetomidine), NMDA receptor antagonists (ketamine or dextromethorphan), and sodium channel blockers (lidocaine).18 To date, the use of an opioid-sparing technique has been previously described in pediatric patients through the use of regional anesthesia and non-opioid medications for various surgical procedures.8,11,12
Our pilot study utilized an opioid-sparing technique for intraoperative and postoperative analgesia that included 4 medications dextromethorphan, acetaminophen, dexmedetomidine, and ketamine. At our institution, preoperative acetaminophen and intraoperative dexmedetomidine are frequently administered, but the use of the other two medications (dextromethorphan and ketamine) was unique additions to the perioperative regimen. Dextromethorphan and acetaminophen were administered preoperatively along with the oral medication (midazolam). Dextromethorphan is a medication commonly used for its antitussive effect in pediatric patients.19,20 In addition to its anti-tussive effects, dextromethorphan acts as an NMDA receptor antagonist thereby providing analgesia.21–23 The preoperative administration of dextromethorphan has been shown to reduce postoperative opioid requirements following adenotonsillectomy in pediatric patients at doses of 1mg/kg.21
Acetaminophen (paracetamol) is a first-line antipyretic and analgesic for mild and moderate pain. Anti-nociceptive effects result from the central inhibition of the cyclo-oxygenase enzyme leading to decreased production of prostaglandins, which in turn diminishes the release of excitatory transmitters involved in nociceptive transmission. It remains a mainstay for the treatment of pain both as a primary agent and as an adjunct in pediatric patient undergoing otolaryngological procedures.24,25 Given cost concerns and lack of proven data to demonstrate a difference in efficacy, we chose to use the oral route for administration.26 Acetaminophen was then administered postoperatively as needed to provide ongoing analgesia with additional ibuprofen available for break-through pain.27
One concern with the preoperative administration of oral medications may be the volume of fluid required in the digestive tract to absorb the medication in a patient who is being kept nil per os (NPO). The 3 medications used in the current study require a small amount of liquid to be administered. In a 10 kg patient, the 3 medications are administered in a total of 7.9 mL including 1.5 mL of the 2 mg/mL midazolam solution (0.3 mg/kg), 1.7 mL of the 30 mg/5 mL dextromethorphan solution (1 mg/kg), and 4.7 mL of the 160 mg/5 mL acetaminophen solution. However, the preoperative administration of oral acetaminophen (the largest volume component of our preoperative regarding) has not been shown to increase gastric volume at the time of anesthetic induction.28 In this study, the authors administered 40 mg/kg of acetaminophen using a solution with a concentration of 50 mg/mL. This would deliver a volume of 8 mL to a 10 kg patient, which is similar to the volume administered to our patients when considering the cumulative volume of the 3 medications. Although all study patients were able to ingest the volume of preoperative medications without difficulty, we concede ingestion of higher volumes may be problematic in other patient populations who are older, have oral aversions or higher dosing weight. However, further studies are needed to determine whether this opioid-sparing technique can be adapted to different patient populations in whom ingestion of larger volumes would be a concern through modifications such as earlier staggered medication administration prior to scheduled surgery.
Intraoperative analgesia was then supplemented with dexmedetomidine and ketamine. Dexmedetomidine is an α2-adrenergic agonist with anxiolytic, nociceptive, and sedative properties that is commonly used for sedation in the intensive care unit setting, procedural sedation, and to decrease the incidence of postoperative emergence delirium. It has been shown to be effective in pediatric patients undergoing ENT procedures due to its desirable effect of providing effective analgesia and reducing emergence agitation and postoperative opioid requirements in dosages ranging from 0.5–1 µg/kg.29–31 In addition, given its limited impact on control of ventilation, dexmedetomidine has been shown to be safe and effective in patients with OSA or SDB.30
Ketamine is a phencyclidine derivative with sedative and analgesic properties modulated through antagonism of the NMDA system. Several studies have demonstrated ketamine’s role as an effective analgesic adjuvant in pediatric patients undergoing various surgical procedures32 and tonsillectomy when combined with opioids, acetaminophen, and dexmedetomidine.33,34 The incidence of potentially concerning adverse effects such as postoperative nausea and vomiting (PONV) as well as emergence delirium are mitigated by the use of a low intraoperative dose (0.5 µg/kg) and coadministration with dexmedetomidine which has been shown to decrease both PONV and emergence delirium after ketamine.34 Although dextromethorphan and ketamine share a similar mechanism of action to provide analgesia with individual studies suggesting efficacy for pain management for each medication, no studies to date have used them in combination. It is possible there is limited synergistic analgesia given similar mechanisms of actions of NMDA blockade although ketamine may have alternative analgesic pathways. Other key intraoperative components of our regimen included the use of isoflurane for maintenance anesthesia to further limit the potential for emergence delirium as well as PONV prophylaxis with the liberal administration of intraoperative fluids, and the prophylactic administration of ondansetron.35,36 In addition to its role in prevention of PONV, dexamethasone has been shown to improve analgesia and limit opioid needs following adenotonsillectomy in children.37
The current pilot study was an exploratory endeavor to determine whether the study medications could provide a feasible analgesic regimen for pediatric patients undergoing adenoidectomy in the absence of ketorolac. To our knowledge, this is the first study describing the combined use of dextromethorphan, acetaminophen, ketamine and dexmedetomidine to manage pain for pediatric patients undergoing otolaryngologic procedures. Although the use of ketorolac has been utilized for pediatric otolaryngological procedures without a reported increase of postoperative bleeding,11,38,39 a lack of consensus remains due to institutionally dependent tonsillar bleeding rates and differing perceptions among otolaryngologists regarding risk factors and causes of post tonsillectomy hemorrhage. Of note, the pediatric otolaryngologists within our institution preferred to exclude ketorolac in the current study due to conflicting evidence regarding the potential risk of bleeding.40,41
Limitations of the pilot study include the lack of a comparator group and absence of a large study cohort to identify adverse events with lower incidences attributed to study medications. In addition, because the postoperative questionnaire did not include specifics regarding recovery beyond the numerical scales of pain management and parental satisfaction, detailed information regarding postoperative recovery was limited to what the parents chose to disclose at the 72 hour follow up phone call.
Although the impact of the results of this pilot study is limited due to its numbers, we found that adenoidectomy could be safely performed without excessive pain with an opioid-sparing technique. None of the patients required intraoperative or postoperative opioids. All were able to be effectively discharged within approximately 2 hours of completion of the procedure. Parents and guardians were highly satisfied or satisfied with the perioperative course in 9 of the 10 patients. Additional analgesia may have been provided by the inclusion of oral or intravenous non-steroidal anti-inflammatory agents into the regime including intravenous ibuprofen or a cyclo-oxygenase type II inhibitor such as Celecoxib. These agents have been shown to be effective in decreasing opioid consumption, lessening pain intensity, and improving the postoperative course following adenotonsillectomy in children without increasing the incidence of bleeding complications.42–44 Based on the findings of this pilot study, future studies should focus on continued adaptations and modifications to various non opioid pain techniques with regard to differing dosing, timing and medication combinations. More importantly, further studies with larger pediatric cohorts are needed to evaluate what types of more painful procedures such as adeno-tonsillectomy and at-risk patients such as those with obesity and obstructive sleep apnea would benefit from an opioid-sparing analgesic approach without compromising pain management while minimizing opioid-related side effects.
Data Sharing Statement
Deidentified data and protocol requests may be made to the corresponding author. Each request will be reviewed to ensure that there is no sharing of identifiable data. If the request is deemed appropriate, data may be provided.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cullen KA, Hall MJ, Golosinskiy A. Ambulatory surgery in the United States, 2006. Natl State Rep. 2009;28:1–25.
2. Bhattacharyya N, Lin HW. Changes and consistencies in the epidemiology of pediatric adenotonsillar surgery, 1996–2006. Otolaryngol Head Neck Surg. 2010;143:680–684. doi:10.1016/j.otohns.2010.06.918
3. Schwengel DA, Sterni LM, Tunkel DE, Heitmiller ES. Perioperative management of children with obstructive sleep apnea. Anesth Analg. 2009;109:60–75. doi:10.1213/ane.0b013e3181a19e21
4. Brown KA, Laferrière A, Moss IR. Recurrent hypoxemia in young children with obstructive sleep apnea is associated with reduced opioid requirement for analgesia. Anesthesiology. 2004;100:806–810. doi:10.1097/00000542-200404000-00009
5. Waters KA, McBrien F, Stewart P, Hinder M, Wharton S. Effects of OSA, inhalational anesthesia, and fentanyl on the airway and ventilation of children. J Appl Physiol. 2002;92:1987–1994. doi:10.1152/japplphysiol.00619.2001
6. Hamilton TB, Thung A, Tobias JD, Jatana KR, Raman VT. Adenotonsillectomy and postoperative respiratory adverse events: a retrospective study. Laryngoscope Investig Otolaryngol. 2020;5:168–174. doi:10.1002/lio2.340
7. Arambula AM, Xie DX, Whigham AS. Respiratory events after adenotonsillectomy requiring escalated admission status in children with obstructive sleep apnea. Int J Pediatr Otorhinol. 2018;107:
8. Zhu A, Benzon HA, Anderson TA. Evidence for the efficacy of systemic opioid-sparing analgesics in the pediatric surgical population: a systematic review. Anesth Analg. 2017;125:1569–1587. doi:10.1213/ANE.0000000000002434
9. Harbaugh CM, Lee JS, Hu HM, et al. Persistent opioid use among pediatric patients after surgery. Pediatrics. 2018;141:e20172439. doi:10.1542/peds.2017-2439
10. Burgart AM, Char D. The opioid crisis should lead pediatric anesthesiologists to a broader vision of opioid stewardship. Paediatr Anesth. 2019;29:1078–1080. doi:10.1111/pan.13730
11. Franz AM, Dahl JP, Huang H, et al. The development of an opioid sparing anesthesia protocol for pediatric ambulatory tonsillectomy and adenotonsillectomy – a quality improvement project. Paediatr Anesth. 2019;29:682–689. doi:10.1111/pan.13662
12. Franz AM, Martin LD, Liston DE, et al. In pursuit of an opioid-free pediatric ambulatory surgery center: a quality improvement initiative. Pediatr Anesth. 2020.
13. Dahl JB, Rosenberg J, Dirkes W, et al. Prevention of postoperative pain by balanced analgesia. Br J Anaesth. 1990;64:518–520. doi:10.1093/bja/64.4.518
14. Kako H, Corridore M, Seo S, Elmaraghy C, Lind M, Tobias JD. Tracheal extubation practices following adenotonsillectomy in children: effects on operating room efficiency between two institutions. Paediatr Anaesth. 2017;27:591–595. doi:10.1111/pan.13100
15. Merkel SI, Voepel-Lewis T, Shayevitz JR, Malviya S. The FLACC: a behavioral scale for scoring postoperative pain in young children. Pediatr Nurs. 1997;23:293–297.
16. Sikich N, Lerman J. Development and psychometric evaluation of the paediatric anesthesia emergence delirium scale. Anesthesiology. 2004;100:1138–1145. doi:10.1097/00000542-200405000-00015
17. Wong D, Baker C. Pain in children: comparison of assessment scales. Pediatr Nurs. 1988;14:9–17.
18. Beverly A, Kaye AD, Ljungqvist O, Urman RD. Essential elements of multimodal analgesia in enhanced recovery after surgery (ERAS) guidelines. Anesthesiol Clin. 2017;35:e115–e143. doi:10.1016/j.anclin.2017.01.018
19. Smith SM, Schroeder K, Fahey T. Over-the counter (OTC) medications of acute cough in children and adults in community settings. Cochrane Database Sys Rev. 2014;11:
20. Green JL, Wang GS, Reynolds KM, et al. Safety profile of cough and cold medications use in pediatrics. Pediatrics. 2017;139:e20163070. doi:10.1542/peds.2016-3070
21. Dawson GS, Seidman P, Ramadan H. Improved postoperative pain control in pediatric adenotonsillectomy with dextramethorphan. Laryngoscope. 2001;111:1223–1226. doi:10.1097/00005537-200107000-00015
22. King MR, Ladha KS, Gelineau AM, Anderson TA. Perioperative dextramethorphan as an adjunct for postoperative pain: a meta-analysis of randomized controlled trials. Anesthesiology. 2016;124:696–705. doi:10.1097/ALN.0000000000000950
23. Martin E, Narjoz C, Decleves X, et al. Dextromethorphan Analgesia in a human experimental model of hyperalgesia. Anesthesiology. 2019;131:356–358. doi:10.1097/ALN.0000000000002736
24. Anderson BJ. Paracetamol (acetaminophen): mechanisms of action. Pediatr Anesth. 2008;18:915–921. doi:10.1111/j.1460-9592.2008.02764.x
25. Anderson BJ, Holford NH, Woollard GA, Kanagasundaram S, Mahadevan M. Perioperative pharmacodynamics of acetaminophen analgesia in children. Anesthesiology. 1999:90411–90421.
26. Mallama M, Valencia A, Rijs K, Rietdijk WJR, Klimek M, Calvache JA. A systematic review and trial sequential analysis of intravenous vs oral peri-operative paracetamol. Anaesthesia. 2020. doi:10.1111/anae.15163
27. Berde CB, Sethna NF. Analgesics for the treatment of pain in children. N Engl J Med. 2002;347:1094–1103. doi:10.1056/NEJMra012626
28. Anderson BJ, Rees SG, Liley A, Stewart AW, Wardill MJ. Effect of preoperative paracetamol on gastric volumes and pH in children. Paediatr Anaesth. 1999;9:203–207.
29. Guler G, Akin A, Tosun Z, Ors S, Esmaolgu A, Boyaci A. Single-dose dexmedetomidine reduces agitation and provides smooth extubation after pediatric adenotonsillectomy. Pediatr Anesth. 2005;15:762–766. doi:10.1111/j.1460-9592.2004.01541.x
30. Patel A, Davidson M, Tran M, et al. Dexmedetomidine infusion for analgesia and prevention of emergence agitation in children with obstructive sleep apnea syndrome undergoing tonsillectomy and adenoidectomy. Anesth Analg. 2010;111:1004–1010.
31. Olutoye O, Glover CD, Diefenderfer BS, et al. The effect of intraoperative dexmedetomidine on postoperative analgesia and sedation in pediatric patients undergoing tonsillectomy and adenoidectomy. Anesth Analg. 2010;111:490–495. doi:10.1213/ANE.0b013e3181e33429
32. Dahmani S, Michelet D, Abback PS, et al. Ketamine for perioperative pain management in children: a meta-analysis of published studies. Paediatr Anesth. 2011;21:636–652. doi:10.1111/j.1460-9592.2011.03566.x
33. Elshammaa N, Chidambaran V, Housny W, Thomas J, Zhang X, Michael R. Ketamine as an adjunct to fentanyl improves postoperative analgesia and hastens discharge in children following tonsillectomy – a prospective, double-blinded randomized study. Pediatr Anesth. 2011;21:1009–1014. doi:10.1111/j.1460-9592.2011.03604.x
34. Hadi SM, Saleh AJ, Tang YZ, Daoud A, Mei X, Ouyang W. The effect of KETODEX on the incidence and severity of emergence agitation in children undergoing adenotonsillectomy using sevoflurane-based anesthesia. Int J Pediatr Otorhinolaryngol. 2015;79:671–676. doi:10.1016/j.ijporl.2015.02.012
35. Mason KP. Paediatric emergence delirium: a comprehensive review and interpretation of the literature. Br J Anaesth. 2017;118:335–343. doi:10.1093/bja/aew477
36. Höhne C. Postoperative nausea and vomiting in pediatric anesthesia. Curr Opin Anaesthesiol. 2014;27:303–308. doi:10.1097/ACO.0000000000000073
37. King A, Elmaraghy C, Lind M, Tobias JD. A review of dexamethasone as an adjunct to adenotonsillectomy in the pediatric population. J Anesth. 2020;34:445–452. doi:10.1007/s00540-020-02758-y
38. Chan DK, Parikh SR. Perioperative ketorolac increased post-tonsillectomy hemorrhage in adults but not children. Laryngoscope. 2014;124:1789–1793. doi:10.1002/lary.24555
39. Rabbani CC, Pflum ZE, Ye MJ, et al. Intraoperative ketorolac for pediatric tonsillectomy: effect on post-tonsillectomy hemorrhage and perioperative analgesia. Int J Pediatr Otorhinolaryngol. 2020;138:110341. doi:10.1016/j.ijporl.2020.110341
40. Judkins JH, Dray TG, Hubbell RN. Intraoperative ketorolac and posttonsillectomy bleeding. Arch Otolaryngol Head Neck Surg. 1996;122:937–940. doi:10.1001/archotol.1996.01890210017004
41. Lewis SR, Nicholson A, Cardwell ME, Siviter G, Smith AF. Nonsteroidal anti-inflammatory drugs and perioperative bleeding in paediatric tonsillectomy. Cochrane Database Sys Rev. 2013;7:CD003591.
42. Moss JR, Watcha MF, Bendel LP, McCarthy DL, Witham SL, Glover CD. A multicenter, randomized, double-blind placebo-controlled, single dose trial of the safety and efficacy of intravenous ibuprofen for treatment of pain in pediatric patients undergoing tonsillectomy. Paediatr Anaesth. 2014;24:483–489. doi:10.1111/pan.12381
43. Murto K, Lamontagne C, McFaul C, et al. Celecoxib pharma-cogenetics and pediatric adenotonsillectomy: a double-blinded randomized controlled study. Can J Anaesth. 2015;62:785–797. doi:10.1007/s12630-015-0376-1
44. Michelet D, Andreu-Gallien J, Bensalah T, et al. A meta-analysis of the use of non-steroidal anti-inflammatory drugs for pediatric postoperative pain. Anesth Analg. 2012;114:393–406. doi:10.1213/ANE.0b013e31823d0b45
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.