Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Operational Standard for Tissue-Extracted Collagen Facial Injection Techniques
Received 15 February 2026
Accepted for publication 12 May 2026
Published 16 June 2026 Volume 2026:19 603794
DOI https://doi.org/10.2147/CCID.S603794
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Yinjie Ao,1 Xiaoyang Wang,2 Bing Shi3
1Department of Plastic Surgery and Medical Cosmetic Center, The Affiliated Eye Hospital, Jiangxi Medical College, Nanchang University, Nanchang, Jiangxi, People’s Republic of China; 2Shanghai Yanfan Medical Cosmetic Clinic, Shanghai, People’s Republic of China; 3Chinese Association of Plastics and Aesthetics, Beijing, People’s Republic of China
Correspondence: Bing Shi, Chinese Association of Plastics and Aesthetics, No. 16, Xisihuan Middle Road, Haidian District, Beijing, 100000, People’s Republic of China, Email [email protected]
Background: Since its first approval in 1981, tissue-extracted collagen injection technology has become an important method for minimally invasive facial rejuvenation, with substantial clinical experience accumulated particularly in the periorbital area. However, due to significant differences in physicochemical properties and metabolic mechanisms compared to hyaluronic acid, its clinical application still faces limitations in understanding and unique complication risks. Furthermore, no unified technical operating standards currently exist internationally.
Methods: This standard is based on a synthesis of multicenter expert clinical experience. It systematically outlines the product characteristics, classification, and specifications of tissue-extracted collagen; defines clinical indications, contraindications, and operational precautions; specifies qualification requirements for medical institutions and operating physicians; establishes protocols for pre-operative assessment, regional injection design, post-operative management, and complication prevention and treatment strategies; and proposes multimodal treatment recommendations combining surgery, thread lifting, energy-based devices, and other fillers.
Clinical Recommendations: Through standardized operating procedures and layered injection techniques, the safety and efficacy of tissue-extracted collagen injection therapy can be effectively improved, reducing the occurrence of complications such as nodules and vascular embolism. Combined treatment strategies further expand the application of collagen in facial rejuvenation, achieving complementary effects and optimizing recovery periods.
Conclusion: This operational standard provides systematic and standardized clinical guidance for tissue-extracted collagen facial injection. It contributes to promoting the appropriate application and healthy development of this technology, enhancing overall treatment quality and patient satisfaction.
Keywords: tissue-extracted collagen, facial rejuvenation, operational standard, complication prevention and management, combination therapy
Introduction
In 1981, the world’s first tissue-extracted collagen injectable filler was approved by the U.S. Food and Drug Administration (FDA) for the improvement of senile wrinkles.1 Between 2009 and 2019, four types of tissue-extracted collagen injectable fillers successively received approval from the National Medical Products Administration (NMPA, formerly the China Food and Drug Administration, CFDA) for marketing in China.2 Over the past 15 years, tissue-extracted collagen injection technology has become one of the important treatment modalities for minimally invasive facial rejuvenation.3 Particularly in the application of minimally invasive periorbital rejuvenation, considerable experience has been accumulated domestically in China. This technique is relatively simple to perform, causes minimal trauma, allows for rapid recovery, and delivers noticeable results post-treatment, making it highly popular among individuals seeking medical aesthetic treatments.4 However, due to significant differences in the physicochemical properties, metabolism, and fate of tissue-extracted collagen compared to hyaluronic acid, numerous misconceptions persist regarding its use in facial treatments, especially in the periorbital region.5 Specific adverse reactions and complications, such as nodules, can occur following injection, and the management strategies for these complications differ markedly from those for hyaluronic acid-related issues.6 Currently, there are no established standards for tissue-extracted collagen injection techniques either domestically or internationally. Strict specifications regarding practitioner qualifications, operational methods, and environmental facilities are lacking. To enhance industry supervision and management, standardize operational procedures, and thereby improve the safety and efficacy of related techniques, the “Operational Standard for Tissue-Extracted Collagen Facial Injection Techniques” has been formulated to promote the healthy and orderly development of the industry.
The operational design outlined in this document is based on a summary of the clinical experience of numerous experts and physicians. It represents a recommended standardized foundational protocol for operators, developed with full consideration of safety and effectiveness. Operators may adopt other diversified and personalized design schemes according to practical circumstances and personal experience, provided they adhere to the general therapeutic principles set forth in this document.
Scope
This document is applicable to medical aesthetic institutions equipped with departments of medical cosmetology or cosmetic dermatology, as well as medical institutions with departments of plastic surgery, cosmetic surgery, and dermatology. It may also serve as a basis for third-party organizations to supervise the medical practices related to tissue-extracted collagen injection techniques and to evaluate medical institutions.
The scope of this operational standard covers the properties, classification, and specifications of tissue-extracted collagen products; clinical application indications, contraindications; requirements for medical institutions; qualifications of operating physicians; pre-treatment preparation; operational design schemes; post-treatment management; prevention and treatment of main complications; recommendations for combined treatment applications; and other content relevant to this therapy.
Based on the methodological process described above — including expert selection, multi-round discussions, in-person consensus meetings, and voting — a final set of recommendations was developed. These recommendations cover 16 facial subunits, including detailed specifications on needle selection (blunt vs. sharp), injection planes (supraperiosteal, subcutaneous, or deep dermis), suggested dose ranges, and complication management strategies. The full recommendations are presented below according to anatomical region.
Product Physicochemical, Biological Characteristics, and Treatment Principles
Types, Composition, and Functions of Collagen
Collagen is a type of fibrous macromolecular protein present in mammals, widely distributed in the extracellular matrix.7 It is the most important, abundant, and prevalent protein within the intercellular spaces of animals, serving functions such as supporting organs and protecting the organism. Currently, 28 types of8 collagens are known from clinical research. Collagen is rich in 18 amino acids including glycine, proline, and alanine, with glycine content being particularly high, constituting about 27% of the amino acids.9–11 It lacks tryptophan and cysteine. Among these, proline and lysine are key components enabling the α-peptide chains to form a triple-helix structure.12 Collagen possesses the function of a signal “relay station”, acting as a ligand in the biological process of cell signal transduction and playing a significant role in cell communication.13 It can trap, store, and transport growth factors and cytokines, thereby serving important roles in processes such as organ development, wound healing, and tissue repair.14 Collagen in the skin is the primary structural protein, accounting for 70% to 80% of its dry weight.15 Skin collagen is synthesized by fibroblasts and consists of 80% to 85% Type I and 10% to 15% Type III collagen.16 Within the dermis, over 80% is predominantly Type I collagen, characterized by thick, densely arranged bundle structures, providing strong support and structural integrity to the skin.8 Loss of Type I collagen will lead to facial wrinkles and depressions. Type III collagen appears as a loose, filamentous network, relatively fine, primarily distributed around Type I collagen at the junction of the epidermis and dermis.17 It is immature, less stable, and has lower tensile strength, providing elasticity and stress resistance to the skin. Type III collagen possesses excellent capabilities in promoting repair and healing, primarily serving nutritive and epidermal management functions.16
Triple-Helix Structure of Collagen
Type I collagen is an important structural protein with biological activity, composed of two identical α1 chains and one α2 chain.18 Each α chain itself adopts a left-handed helical conformation, and the three α chains intertwine to form a right-handed triple-helix structure.19 Type III collagen, on the other hand, is composed of three identical α1 chains.20
Biological Characteristics
As an important protein in organisms, collagen possesses many excellent biological characteristics:
- Low immunogenicity: Collagen, as a natural macromolecule, exhibits low immunogenicity.21
- Strong hydrophilicity: Collagen molecules contain numerous polar hydrophilic groups, and their internal sponge-like, loose, porous structure also has a strong water retention capacity.22
- Biodegradability: Collagenase in the body can hydrolyze collagen into oligopeptides or amino acids, with 80% being utilized by the organism and 20% excreted as urea.23
- Biocompatibility: The natural fibrous structure of collagen provides an excellent growth scaffold and environment for cells.24
- Procoagulant function: Upon contact with blood, platelets in the blood rapidly adhere to collagen fibers, forming fibrin and accelerating clot formation, thereby promoting hemostasis.8
Treatment Principles
Collagen degrades in the body to produce abundant amino acids, such as alanine, arginine, and leucine, which can compete with tyrosine in the skin, thereby inhibiting melanin formation.25 The inherent white color of collagen products provides immediate coverage for dark circle pigmentation.26 Concurrently, injectable collagen can stimulate the formation of new collagen over an extended period in vivo, thus sustainably improving melanin deposition.
During metabolism, collagen decomposes into various amino acids, most of which can be reabsorbed and utilized by human tissues, providing raw materials for the synthesis of new collagen.27
Tissue-extracted collagen possesses high viscoelasticity (no displacement, no deformation), does not absorb water and swell, and results in a more natural facial appearance after injection.27
Tissue-extracted collagen can activate fibroblast activity, improve the extracellular matrix environment, and effectively induce the production of new collagen, thereby densifying the skin tissue.28
Clinical application has found that the probability of vascular embolism caused by collagen injection is very low. When small amounts of vascular embolism occur, they can often be reversed after brief massage or simply waiting, with good prognostic outcomes. In the past three years, domestic expert teams have analyzed this phenomenon in clinical applications and found explanations through animal experiments.29
- Collagen products have very low injection resistance, making it easy to detect deviations in injection depth and partially avoid risks.30
- Collagen particles are very fine and do not exist in a gel state when mixed with water or blood; they can coexist homogeneously. This significantly reduces the likelihood of complete embolization.31
- When a needle enters a blood vessel, blood can be aspirated immediately. After injecting collagen, blood can still be aspirated within a short period during subsequent aspiration, providing ample safety warning. Embolized arteries or veins can recanalize within a relatively short time, and the probability of irreversible embolism is very low.32
Product Classification and Specifications
Product Classification
Currently, the tissue-extracted collagen products marketed in China with corresponding registration certificates can be classified into two categories based on their source: porcine-derived and bovine-derived. Based on the use of glutaraldehyde cross-linking agents, they can be classified as non-crosslinked collagen and crosslinked collagen.33
Product Specifications
Porcine-Derived
- Collagen Implant, Trade Name: Furo Mei (Sunmax Biotechnology Corp., Ltd., Taiwan, China).Composition: Purified Type I collagen derived from porcine skin and phosphate-buffered saline, containing 35 mg of collagen per milliliter.Specification: 0.5 mL/syringe.Porcine-derived:
- Collagen Implant, Trade Name: Fuli Mei (Sunmax Biotechnology Corp., Ltd., Taiwan, China).Composition: Crosslinked Type I collagen purified from porcine skin and phosphate-buffered saline, containing 35 mg of collagen per milliliter.Specification: 1.0 mL/syringe.
- Lidocaine-containing Collagen Implant, Trade Name: Fulai Mei (Sunmax Biotechnology Corp., Ltd., Taiwan, China).Composition: Crosslinked collagen purified from porcine skin and phosphate-buffered solution containing 0.3% lidocaine, with collagen content of 35 mg/mL and lidocaine hydrochloride content of 3 mg/mL.Specification: 1.0 mL/syringe.
Bovine-Derived
Medical Collagen Filler, Trade Name: FILLDERM injectable collagen (Fiman (Changchun) Medical Biotechnology Co., Ltd., Jilin, China).
Composition: A saline suspension containing 3.5% bovine collagen (35 mg/mL) and 0.3% lidocaine hydrochloride.
Specification: 0.5 mL/syringe, 1.0 mL/syringe.
Clinical Application Indications, Contraindications, and Precautions
Clinical Application Indications
Clinical application indications are as follows:
- Correction and improvement of facial wrinkles;
- Correction and improvement of nasolabial folds of varying degrees;
- Improvement of facial depressions and volume deficiencies in various areas;
- Facial contouring and shaping;
- Improvement of dark circles and facial skin texture and tone.
Clinical Application Contraindications and Precautions
Clinical application contraindications and precautions are as follows:
- Contraindicated in individuals allergic to collagen;
- Contraindicated in patients using immunosuppressants;
- Contraindicated in patients with autoimmune diseases and connective tissue disorders;
- Contraindicated in patients with rheumatic diseases;
- Contraindicated in patients with other severe systemic diseases and psychiatric disorders;
- Not recommended for use in pregnant or lactating women and infants;
- Not recommended for use in diabetic patients before effective blood glucose control is achieved;
- Use with caution in individuals on long-term anticoagulant therapy;
- Use with caution in areas previously injected with unknown types of fillers;
- Use with caution in individuals with allergic predisposition.
Requirements for Medical Institutions and Operating Physicians
Requirements for Medical Institutions
Medical institutions shall meet the following requirements:
- They must be legally established medical aesthetic and plastic surgery institutions;
- They must be equipped with a Department of Medical Cosmetology (including but not limited to Cosmetic Surgery, Cosmetic Dermatology, Cosmetic Traditional Chinese Medicine, Cosmetic Dentistry, and Cosmetic Ophthalmology);
- The operating environment must be an operating room or a clean treatment room, equipped with essential emergency equipment and medications.
Qualification Requirements for Operating Physicians
The qualification requirements for operating physicians are as follows:
- The qualifications of the operating physician shall comply with the relevant provisions of Article 11, Chapter 3 of the “Measures for the Administration of Medical Cosmetology Services” (2016 revision) issued by the National Health Commission;
- The operating physician shall have completed the registration as a chief physician in cosmetology;
- The physician shall have received formal training in collagen injection techniques.
Pre-Treatment Preparation and Post-Treatment Management
Preliminary Preparation
Conduct a detailed medical history inquiry and understand the treatment needs of the individual seeking medical aesthetic services, strictly adhering to the indications.
Pre-Treatment Preparation
The following preparations shall be made before treatment:
- Signing of informed consent;
- Facial cleansing;
- Collection of imaging information;
- Disinfection of the treatment area;
- The product must be maintained under cold chain management throughout storage and transportation, and administered immediately upon opening during injection.
Post-Treatment Management
The following management measures shall be taken after treatment:
- Keep the injection sites clean and dry for 12 to 24 hours;
- Cold compress with an ice pack may be applied (ensuring no frostbite occurs);
- Collection of imaging information;
- Management of post-injection complications shall refer to Combination with Surgical Procedures to 10.8.
Operational Design Plan
General Principles
Tissue-extracted collagen (hereinafter referred to as collagen) may be administered for facial injection therapy using either sharp or blunt needles.34 When using sharp needles, a small amount should be injected per point, and effective aspiration must be performed prior to injection. When using blunt needles, fanning, layering, or intermittent retrograde injection techniques are primarily employed. Immediate pressure should be applied after injection to ensure a smooth surface and avoid protrusions.35 Collagen can be injected at various facial layers, ranging from the deep dermis to the supraperiosteal level. When injecting into the deep dermis, non-crosslinked collagen or diluted collagen should be selected whenever possible. Facial injections should follow the sequence from top to bottom, from lateral to medial, and from deep to superficial.36 Depending on specific treatment needs, it may be combined with other injectable fillers. Repeat injections for the same site and layer may be planned within a treatment course ranging from 2 months to 12 months, with adjustments made based on individual circumstances to achieve optimal outcomes.33
Regional Treatment Plan Recommendations
Upper Face Operational Design Plan
Forehead (Figure 1): A blunt needle can be used for supraperiosteal injection. Depending on the degree of volume deficiency, an injection volume of 1 mL to 5 mL may be used.
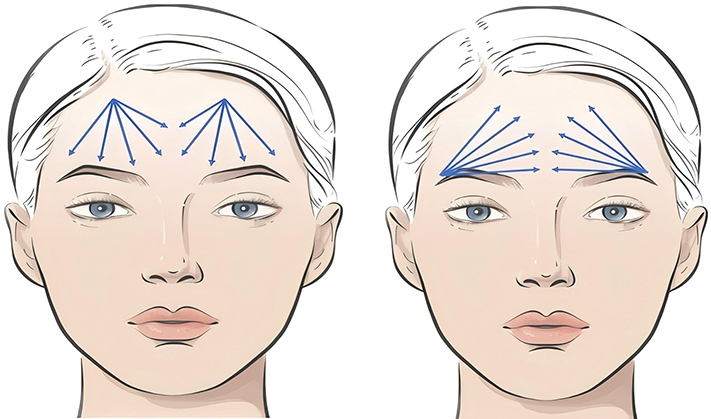 |
Figure 1 Upper Facial Operational Plan Design — Frontal Region. Blue indicates blunt cannula. |
Glabella (Figure 2): A blunt or sharp needle can be used for supraperiosteal injection. The glabellar region can accommodate an injection volume of 0.5 mL to 2 mL.
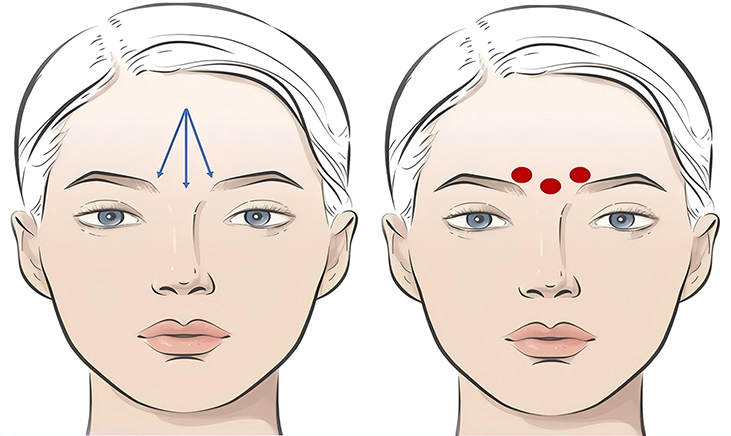 |
Figure 2 Upper Facial Operational Plan Design — Glabellar Region. Blue indicates blunt cannula; red indicates sharp needle. |
Temporal Region (Figure 3): A sharp needle can be used for supraperiosteal injection in the area approximately 1 cm below the temporal crest and 1 cm above the superior orbital rim. Alternatively, a blunt needle can be used for injection into the subcutaneous layer or the superficial aspect of the deep temporal fascia. The recommended volume per side is 0.5 mL to 5 mL.
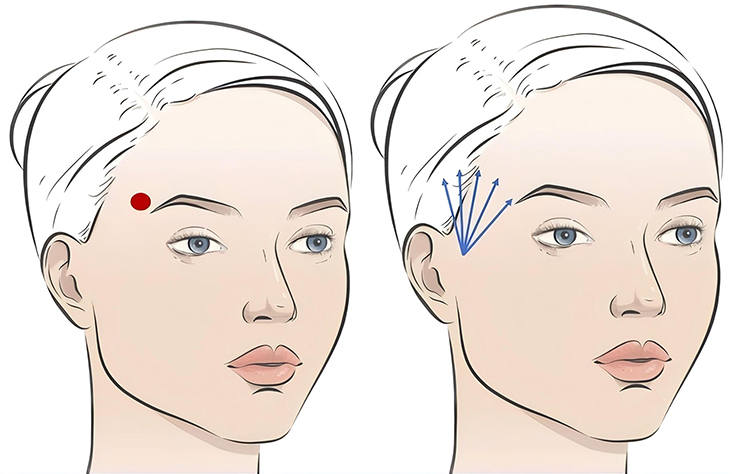 |
Figure 3 Upper Facial Operational Plan Design — Temporal Region. Blue indicates blunt cannula; red indicates sharp needle. |
Eyebrow Ridge (Figure 4): A sharp needle can be used for supraperiosteal injection. Alternatively, a blunt needle can be used for injection into the retro-orbicularis oculi fat (ROOF) layer, subcutaneous fat layer, or the supraperiosteal layer. The recommended volume per side is 0.5 mL to 1 mL.
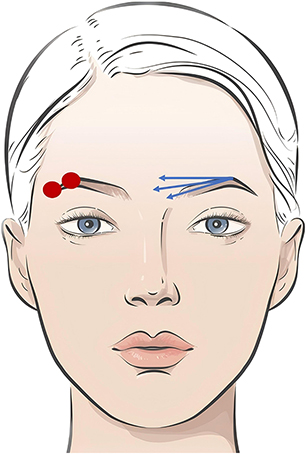 |
Figure 4 Upper Facial Operational Plan Design — Supraorbital Ridge. Blue indicates blunt cannula; red indicates sharp needle. |
Mid-Face Operational Design Plan
Periorbital Area (Figure 5): A sharp needle can be used, contacting the periosteum for injection along the attachment zones of periorbital ligaments, such as the temporal fusion zone, lateral orbital thickening, periorbital retaining ligaments, and the tear trough ligament area, as well as into the suborbicularis oculi fat (SOOF) layer medially and laterally around the orbit. Alternatively, a blunt needle can be chosen for injection onto the periosteum, under the orbicularis oculi muscle, or into the subcutaneous layer. The recommended periorbital injection volume per side is 0.5 mL to 2 mL. For upper eyelid hollowing, a blunt or sharp needle can be used for injection into the ROOF layer or within the orbital septum. The recommended upper eyelid injection volume per side is 0.2 mL to 1 mL.
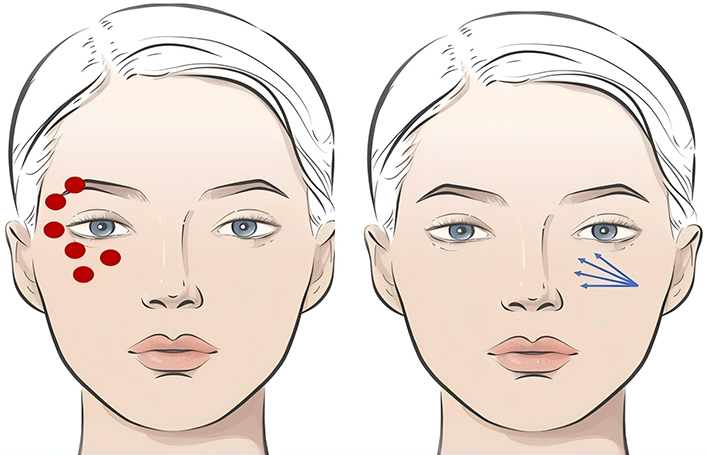 |
Figure 5 Mid-Facial Operational Plan Design — Periorbital Region. Blue indicates blunt cannula; red indicates sharp needle. |
Cheeks (Malar Region) (Figure 6): A blunt needle is typically chosen for injection into the subcutaneous layer. The recommended volume per side is 0.5 mL to 4 mL.
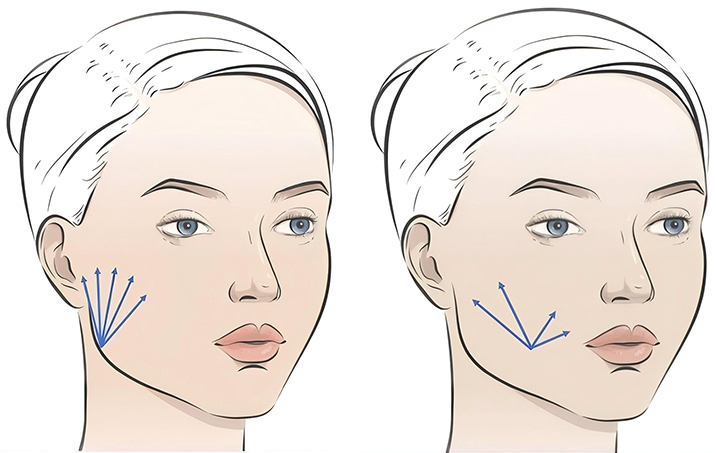 |
Figure 6 Mid-Facial Operational Plan Design — Cheek Region. Blue indicates blunt cannula. |
Nose (Figure 7): A blunt or sharp needle can be used for injection onto the periosteum or into the subcutaneous layer. For defining the double C-curves, a sharp needle contacting the periosteum or a blunt needle for subcutaneous sculpting can be used. The recommended nasal injection volume is 0.5 mL to 2 mL.
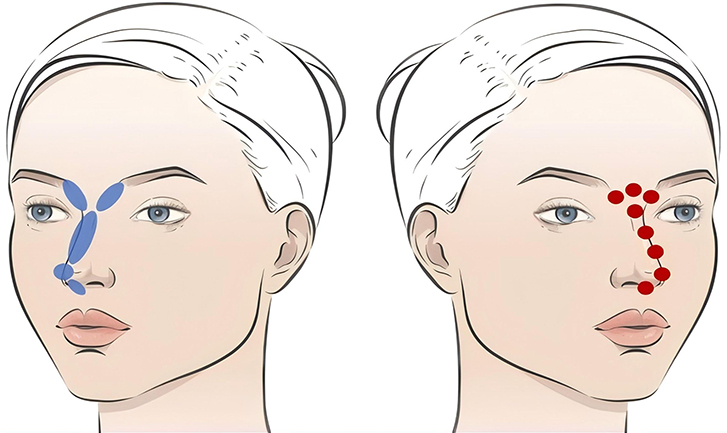 |
Figure 7 Mid-Facial Operational Plan Design — Nasal Region. Blue indicates blunt cannula; red indicates sharp needle. |
Buccal Fat Pad Area (Figure 8): A sharp needle can be used for supraperiosteal injection. When using a blunt needle, injection can be performed into the medial buccal fat compartment. The recommended volume per side is 0.5 mL to 1 mL.
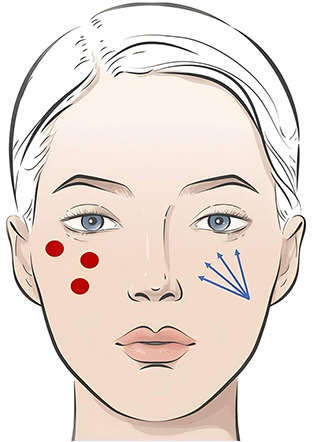 |
Figure 8 Mid-Facial Operational Plan Design — Malar Fat Pad Region. Blue indicates blunt cannula; red indicates sharp needle. |
Nasolabial Folds (Figure 9): A sharp needle can be used for supraperiosteal injection. When using a blunt needle, injection can be performed into the nasolabial fat compartment. The recommended volume per side is 0.5 mL to 2 mL.
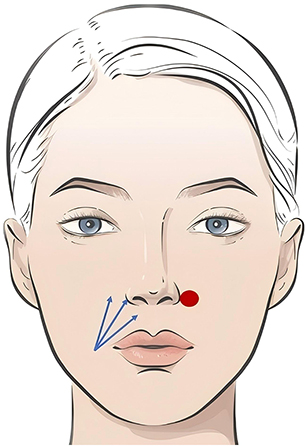 |
Figure 9 Mid-Facial Operational Plan Design — Nasolabial Fold. Blue indicates blunt cannula; red indicates sharp needle. |
Lower Face Operational Design Plan
Pre-jowl Sulcus (Figure 10): A sharp needle can be used, contacting the periosteum in the mandibular ligament area. Alternatively, a blunt needle can be chosen for injection into the deep subcutaneous layer. The recommended volume per side is 0.5 mL to 2 mL.
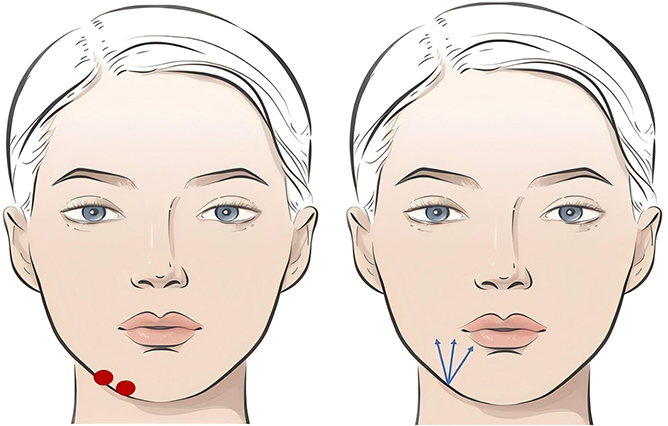 |
Figure 10 Lower Facial Operational Plan Design — Prejowl Sulcus. Blue indicates blunt cannula; red indicates sharp needle. |
Chin (Figure 11): A sharp needle can be used, contacting the periosteum at the pogonion or pre-pogonion point, with blending and transition to areas approximately 1–2 cm on either side. The recommended chin injection volume is 0.5 mL to 4 mL.
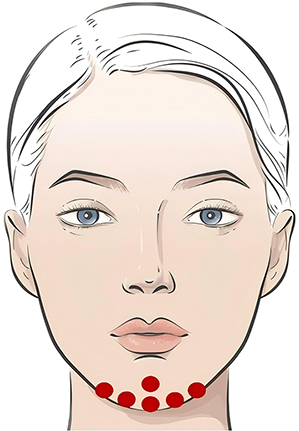 |
Figure 11 Lower Facial Operational Plan Design — Chin Region.red indicates sharp needle. |
Labiomental Fold (Mental Crease) (Figure 12): A blunt needle is typically chosen for injection into the deep subcutaneous layer. The recommended volume per side is 0.5 mL to 1 mL.
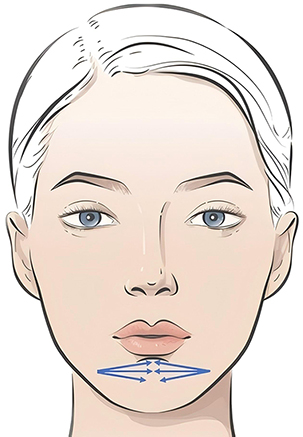 |
Figure 12 Lower Facial Operational Plan Design — Mentolabial Fold. Blue indicates blunt cannula. |
Mandibular Line (Jawline) (Figure 13): At the mandibular angle and mandibular ligament area, a sharp needle can be used for periosteal layer injection. Alternatively, a blunt needle can be chosen for subcutaneous sculpting to enhance the mandibular line contour. The recommended volume per side is 0.5 mL to 1 mL.
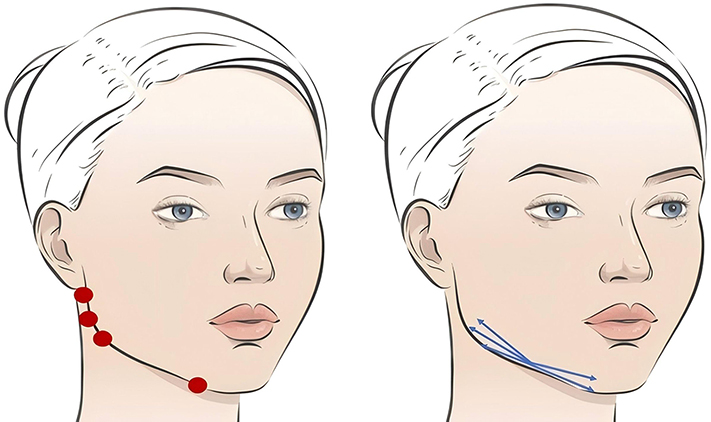 |
Figure 13 Lower Facial Operational Plan Design — Jawline. Blue indicates blunt cannula; red indicates sharp needle. |
Lips (Figure 14): Non-crosslinked collagen can be injected using a sharp needle into the labial mucosa and subdermal layer. The recommended lip injection volume is 0.5 mL to 1 mL.
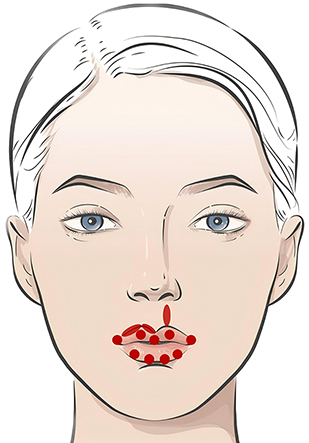 |
Figure 14 Lower Facial Operational Plan Design — Lip Region red indicates sharp needle. |
Operational Design Plan for Other Areas
Neck (Figure 15): A sharp needle may be selected for intradermal or subcutaneous injection. When using a blunt needle, injection is performed into the superficial subcutaneous layer along the neck lines. For the treatment of neck lines alone, the recommended single-session volume is 1 mL to 3 mL.
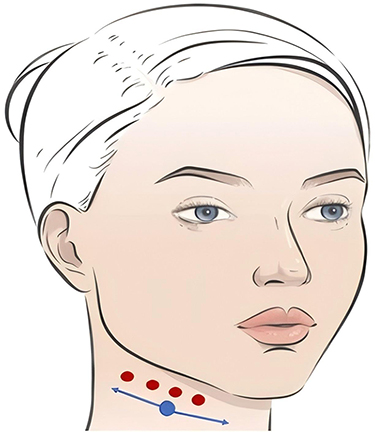 |
Figure 15 Other Regional Operational Plan Design — Neck Region. Blue indicates blunt cannula; red indicates sharp needle. |
Mesotherapy (Figure 16): Collagen is diluted with a diluent (non-crosslinked or minimally crosslinked hyaluronic acid and normal saline) at a ratio of 1:2:2. The mixture is injected into the deep dermal layer, with an injection volume of 0.025 mL per point. The recommended total collagen volume for a full-face treatment is 1 mL to 2 mL per session.
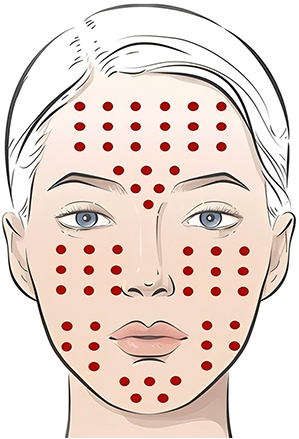 |
Figure 16 Other Regional Operational Plan Design — Mesotherapy. Red indicates sharp needle. |
Major Complications and Their Management
Local Swelling
The common injection techniques involve a combination of blunt and sharp needles. If blunt needles cause mechanical trauma due to aggressive dissection, postoperative swelling is likely.36 To prevent this, practitioners must have a thorough understanding of local anatomy, perform precise injections during the procedure, avoid repeated punctures and blunt dissection with blunt needles, and apply appropriate cold compresses postoperatively. Oral anti-edema medication may also be administered.37
Bruising and Hematoma
Immediate cold compress and pressure can help reduce bruising and hematoma. Topical ointment application 12 hours post-treatment may accelerate the resolution of bruising.38
Pain
Pain is commonly associated with aggressive manipulation, such as nerve irritation or injection into sensitive areas during the procedure. Injectable products containing lidocaine can effectively reduce intraoperative injection pain. If arterial or venous embolism occurs during injection, immediate, intensified pain may be observed.39 Prompt assessment of the injection site for skin mottling or whitening is necessary, and reference should be made to Section 10.8 for further management.
Nodules and Induration
Nodules often result from overly superficial injection, excessive dose per injection point, or failure to massage and shape the area post-injection. Manifestations include abnormal protrusions or white spots at the injection site.40 For nodules detected immediately or shortly after injection, massage may be performed to promote even dispersion. Larger nodules may require aspiration for improvement. Chronic nodules are often associated with induration at the injection site and reduced skin elasticity.41 Management may include intralesional injection of collagenase or corticosteroids, hot compresses, massage, or radiofrequency therapy.
Hyperpigmentation or Hypopigmentation
Hyperpigmentation may be improved with light-based therapy or mesotherapy. Precise control of injection depth and dosage can effectively prevent immediate post-injection skin whitening. If hypopigmentation occurs, management should follow the guidelines in Combination with Other Fillers.
Allergic Reactions
Currently, the telopeptide removal technology in collagen production is highly advanced, making allergic reactions due to product formulation rare. Acute or delayed allergic reactions are more likely associated with individual patient variability or collagen denaturation.42 Strict control of cold chain transportation, pre-procedure verification of product integrity, and thorough inquiry into patient allergy history and immune-related conditions can effectively prevent allergic reactions. If allergic symptoms occur, oral antihistamines may be administered. In severe cases, short-term use of corticosteroids may be added to accelerate collagen degradation and alleviate symptoms.43
Infection
Strict adherence to aseptic technique can effectively prevent infection. If infection is confirmed, local debridement is the primary treatment. Oral or intravenous antibiotics may be administered. If necessary, bacterial culture of drained secretions should guide antibiotic selection.44
Circulatory Impairment
Pre-filling the needle with lidocaine before injection and aspirating before injection can help determine if the needle is within a blood vessel. Injection should be performed slowly. If resistance is encountered or the patient reports pain, injection should be stopped immediately, and the area should be massaged while observing changes in skin color.45 Arterial embolism may present within 10 minutes post-injection with skin whitening or mottling accompanied by severe pain. A capillary refill test may show delayed refill.46 Management may include warm compress massage, topical application of nitroglycerin ointment, vasodilation and microcirculation improvement, along with prophylactic anti-infection treatment. Venous embolism may manifest as a deep blue discoloration near the injection site, possibly occurring within 10 minutes to several hours post-injection. Management may involve local injection of collagenase or corticosteroids, and systemic administration of antibiotics, steroids, aspirin, low-molecular-weight heparin, etc.47 Hyperbaric oxygen therapy may also be considered to provide anticoagulation, reduce inflammation, improve microcirculation, and alleviate tissue hypoxia. Skin necrosis may develop days or weeks later. Management may include wet compresses with nitroglycerin ointment, wound cleansing and dressing changes, and topical application of growth factors to promote tissue regeneration and wound healing. If severe symptoms such as visual field defects, blindness, hearing impairment, limb movement disorders, respiratory distress, or unstable vital signs occur, immediate consultation with a multidisciplinary team including ophthalmology, otorhinolaryngology, respiratory medicine, and interventional radiology is required. Timely symptomatic treatment such as intravascular thrombolysis should be performed.45,48
Recommendations for Combined Therapy Applications
Due to its unique material properties and biological performance, collagen can be widely used in combination with other therapies.
Combination with Surgical Procedures
Collagen can be combined with surgical procedures. Application at the incision site can assist in hemostasis and promote rapid wound healing. In periorbital rejuvenation, collagen filler can be used 3 months postoperatively to improve fine lines, depressions, and hyperpigmentation around the eyes.
Combination with Thread Lifting
Collagen can be combined with thread lifting techniques. Layering collagen along the path of the threads can assist in hemostasis, reduce swelling, aid in thread-tissue adhesion, and minimize displacement of lifted tissues. Additionally, collagen can be injected after thread lifting to improve local depressions, fine lines, enlarged pores, skin sensitivity, and periorbital hyperpigmentation.
Combination with Energy-Based Devices
Energy-based devices employ physical and photobiological principles to create orderly, controlled cutaneous injury, thereby initiating post-traumatic repair mechanisms to achieve regeneration and tissue repair.49 In facial rejuvenation treatments, these devices can improve hyperpigmentation, enlarged pores, and telangiectasia, increase skin hydration, restore barrier function, and reduce fine wrinkles. Post-procedure, combination with collagen mesotherapy can enhance efficacy, shorten recovery time, and reduce adverse reactions. For comprehensive treatment of periorbital aging concerns such as dark circles and tear troughs, intense pulsed light (IPL), Q-switched lasers, picosecond lasers, radiofrequency energy, and focused ultrasound can improve skin tone and texture.50 Following energy-based treatments, provided there is no significant exfoliation or erythema, collagen mesotherapy or filler injections can be immediately combined to yield superior therapeutic outcomes. If open wounds are present (eg., from fractional microneedling radiofrequency), a 1 to 2-week interval is recommended before combination treatment. When performing energy-based therapies after collagen filler injection, an interval of over 2 months is advised.51
Combination with Other Fillers
Collagen presents as an opaque, milky white substance. Subcutaneous injection can optimize skin tone and improve both pigmented and vascular dark circles. In facial soft tissue augmentation, it can be combined with harder, longer-lasting fillers such as hyaluronic acid or biostimulators for supraperiosteal and deep fascial layer injection, leveraging complementary advantages.52 For periorbital filling, collagen offers the distinct benefit of avoiding the Tyndall effect, making its combination particularly advantageous. If the Tyndall effect occurs due to hyaluronic acid filler, hyaluronidase can be used for dissolution followed by collagen injection. When combining collagen with other facial fillers, layered injection is recommended.53 Additionally, as an excellent carrier material, collagen can be directly mixed in specific proportions with injectable materials such as modified hydroxyapatite, polylactic acid, or acellular dermal matrix particles for injection therapy, for which both domestic and international clinical experience has been accumulated.
Combination with Botulinum Toxin
Botulinum toxin type A improves dynamic wrinkles by modulating facial muscle activity. Reduced muscle movement is conducive to the long-term maintenance of facial collagen.54
Combination with Mesotherapy
As a skin nutrient, collagen can be used in mesotherapy. Intradermal injection improves dull complexion, dryness, enlarged pores, and fine wrinkles, and promotes the repair of sensitive skin and melasma. It can be combined with other mesotherapy products, typically administered via intradermal injection following mesotherapy.55
Conclusion
This document establishes a comprehensive technical framework for tissue-extracted collagen facial injection, spanning fundamental principles to clinical practice. It systematically outlines the unique advantages of collagen fillers—such as low immunogenicity, biodegradability, procoagulant function, and non-hydrating properties—differentiating them from hyaluronic acid and other dermal fillers. In conclusion, this operational standard serves as a practical, safety-oriented clinical guide to enhance treatment outcomes and patient satisfaction. It also provides a foundation for professional training, quality assessment, and regulatory oversight, supporting the standardized and sustainable advancement of tissue-extracted collagen injection therapy in clinical practice.
Data Sharing Statement
The datasets used and analysed during the current study available from the corresponding author on reasonable request.
Acknowledgments
The data for this group standard were contributed by the following physicians and companies: Cao Yilin, Beijing BeauCare First Hospital; Shi Bing, The Eighth Medical Center of Chinese PLA General Hospita; Li Qin, Aist Medical Cosmetic Group; Wu Sufan, Zhejiang Provincial People’s Hospital; Long Jianhong, Xiangya Hospital of Central South University; Wu Xiaojun, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine; Chen Guangyu, Plastic Surgery Hospital, Chinese Academy of Medical Sciences; Zhang Ge, Zhengzhou Hanchen Medical Cosmetic Hospital; Wang Yang, Beijing Rende Yimei Medical Cosmetic Clinic; Wang Xiaoyang, Shanghai Yanfan Medical Cosmetic Clinic; Liu Hongmei, Beijing Meiyan Medical Cosmetic Clinic; Xie Hongbin, Peking University Third Hospital; Li Yuanhong, Shenyang Yanyue Medical Cosmetic Clinic; Shao Ying, The First Hospital of Jilin University; Xia Wei, Xi’an Boshi Zhenyan Medical Cosmetic Co., Ltd. Xincheng Medical Cosmetic Clinic; Hong Wei, Jingfu Medical Cosmetic Chain; Pan Baohua, Chongqing Huamei Plastic Surgery Hospital; Han Sheng, Beijing Shouxi BeauCare Medical Cosmetic Clinic; Sun Zhongsheng, Guangdong Second Provincial People’s Hospital; Xia Qiu, Chengdu Gaoxin Xiaqiu Medical Cosmetic Clinic; Wang Zhongjie, Beijing Taimei BeauCare Medical Cosmetic Clinic; Zeng Dong, Guangzhou Zixin Plastic Surgery Hospital; Yu Xiaochun, Tian Hongwei, Beijing Milan Boyu Lidu Medical Cosmetic Hospital; Wang Bo, Beijing Boruina Medical Cosmetic Clinic; Zhao Liang, Suzhou Meibeier Medical Cosmetic Hospital; Li Jialun, Wuhan Pikeli Medical Cosmetic Clinic; Lin Hesheng, Shanghai Fuai Medical Cosmetic Clinic; Liu Zheng, Hangzhou Shuguang Medical Cosmetic Hospital; Su Hong, Urumqi Wancheng Medical Cosmetic Clinic, Xinjiang; Yu Xiang, Guiyang Ruiya Ruimei Medical Cosmetic Clinic; Hao Jingqian, Anshan Shalong Medical Cosmetic Clinic; Zhang Jiajing, Department of Plastic Surgery, Beijing You’anmen Hospital; Ao Yinjie, Plastic Surgery AND Medical Cosmetic Center, The Affliated Eye Hospital, Jiangxi Medical College, Nanchang University. Beijing Xiangzan International Trade Co., Ltd. Fiman (Changchun) Medical Biotechnology Co., Ltd.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no competing interests in this work.
References
1. El Masry MS, Chaffee S, Das Ghatak P, et al. Stabilized collagen matrix dressing improves wound macrophage function and epithelialization. FASEB J. 2019;33(2):2144–18. doi:10.1096/fj.201800352R
2. Fleck CA, Simman R. Modern collagen wound dressings: function and purpose. J Ame College Certified Wound Specialists. 2010;2(3):50–54. doi:10.1016/j.jcws.2010.12.003
3. Bauman L. CosmoDerm/CosmoPlast (human bioengineered collagen) for the aging face. Facial Plastic Surg. 2004;20(2):125–128. doi:10.1055/s-2004-861752
4. Yu W, Han Y, Wu X, et al. A split-face randomized controlled trial of treatment with broadband light for enlarged facial pores. J Dermatolog Treatment. 2021;32(7):766–770. doi:10.1080/09546634.2019.1698701
5. Stochaj AS, Jezierska DH, Kubisz L. Comparing the efficacy of monopolar and bipolar radiofrequency treatment on facial skin in women. J Clin Aesthetic Dermatol. 2022;15(12):22–27.
6. Abe Y, Konno H, Yoshida S, et al. Red light-promoted skin barrier recovery: spatiotemporal evaluation by transepidermal potential. PLoS One. 2019;14(7):e0219198. doi:10.1371/journal.pone.0219198
7. Britt CJ, Marcus B. Energy-based facial rejuvenation: advances in diagnosis and treatment. JAMA Facial Plastic Surg. 2017;19(1):64–71. doi:10.1001/jamafacial.2016.1435
8. Angre T, Kumar A, Singh AK, Thareja S, Kumar P. Role of collagen regulators in cancer treatment: a comprehensive review. Anti Cancer Agents Med Chem. 2022;22(17):2956–2984. doi:10.2174/1871520622666220501162351
9. Kounidas G, Kastora S, Rajpara S. Decoding infraorbital dark circles with lasers and fillers. J Dermatolog Treatment. 2022;33(3):1563–1567. doi:10.1080/09546634.2020.1855297
10. Zhao R, Qiu H, Liu S, Cao L, Yu D, Wang H. Quantifiable clinical efficacy of injectable porcine collagen for the treatment of structural dark circles. J Cosmet Dermatol. 2021;20(5):1520–1528. doi:10.1111/jocd.13982
11. Baumann L. Collagen-containing fillers: alone and in combination. Clin Plast Surg. 2006;33(4):587–596. doi:10.1016/j.cps.2006.08.001
12. Rostan E. Collagen fillers. Facial Plastic Surg Clin North Ame. 2007;15(1):55–61. doi:10.1016/j.fsc.2006.11.001
13. Haneke E. Skin rejuvenation without a scalpel. I. fillers. J Cosmet Dermatol. 2006;5(2):157–167. doi:10.1111/j.1473-2165.2006.00243.x
14. Coleman KR, Carruthers J. Combination therapy with BOTOXtm and fillers: the new rejuvnation paradigm. Dermatologic Therapy. 2006;19(3):177–188. doi:10.1111/j.1529-8019.2006.00072.x
15. Sorushanova A, Delgado LM, Wu Z, et al. The collagen suprafamily: from biosynthesis to advanced biomaterial development. Adv Mater. 2019;31(1):e1801651. doi:10.1002/adma.201801651
16. Selvaraj V, Sekaran S, Dhanasekaran A, Warrier S. Type 1 collagen: synthesis, structure and key functions in bone mineralization. Differ Res Biolog Diver. 2024;136:100757. doi:10.1016/j.diff.2024.100757
17. Momot KI. Hydrated collagen: where physical chemistry, medical imaging, and bioengineering meet. J Phys Chem A. 2022;126(49):10305–10316. doi:10.1021/acs.jpcb.2c06217
18. Martínez-Puig D, Costa-Larrión E, Rubio-Rodríguez N, Gálvez-Martín P. Collagen supplementation for joint health: the link between composition and scientific knowledge. Nutrients. 2023;15(6):23–32. doi:10.3390/nu15061332
19. Su H, Karin M. Collagen architecture and signaling orchestrate cancer development. Trends Cancer. 2023;9(9):764–773. doi:10.1016/j.trecan.2023.06.002
20. Guillard J, Schwörer S. Metabolic control of collagen synthesis. Matrix Biol. 2024;133:43–56. doi:10.1016/j.matbio.2024.07.003
21. Fu R, Fan D, Yang W, et al. Industrial development and biomedical application prospect of recombinant collagen. Sheng wu gong cheng xue bao. 2022;38(9):3228–3242.
22. Gardeazabal L, Izeta A. Elastin and collagen fibres in cutaneous wound healing. Experim Dermatol. 2024;33(3):e15052. doi:10.1111/exd.15052
23. De Gregorio V, Barua M, Lennon R. Collagen formation, function and role in kidney disease. Nat Rev Nephrol. 2025;21(3):200–215. doi:10.1038/s41581-024-00902-5
24. Oosterlaken BM, Vena MP, de With G. In vitro mineralization of collagen. Adv Mater. 2021;33(16):e2004418. doi:10.1002/adma.202004418
25. Szarek P, Ruberti JW. Collagen mechanics. Sub Cellular Biochem. 2026;113:277–342. doi:10.1007/978-3-032-05273-5_10
26. Inacio PAQ, Chaluppe FA, Aguiar GF, Coelho CDF, Vieira RP. Effects of hydrolyzed collagen as a dietary supplement on fibroblast activation: a systematic review. Nutrients. 2024;16(11):56–62. doi:10.3390/nu16111543
27. Tuusa J, Kokkonen N, Tasanen K. BP180/collagen XVII: a molecular view. Int J Mol Sci. 2021;22(22):132–140. doi:10.3390/ijms222212233
28. Bächinger HP, Boudko SP. Mysteries of the collagen triple helix. Matrix Biol. 2025;137:12–18. doi:10.1016/j.matbio.2025.02.003
29. Yu L, Wei M. Biomineralization of collagen-based materials for hard tissue repair. Int J Mol Sci. 2021;22(2):342–351.
30. Tao A, Shu Y, Ding H, Tao G. Injectable fillers for atrophic acne scars: a systematic review of mechanisms, evidence, and clinical algorithms. Clin Cosmet Invest Dermatol. 2026;19:602580. doi:10.2147/CCID.S602580
31. Cong L-Y, Zhang S, Huang J, et al. A study on the aesthetic parameters and proportions of the external contour for minimally invasive facial injection. Aesthetic Plastic Surg. 2024;48(23):4750–4759. doi:10.1007/s00266-024-04232-6
32. Lau E, Ming SY, Yi K. Early clinical experience in the management of nodular complications following cross-linked porcine collagen injection for tear trough augmentation: a two-case report. Cureus. 2026;18(2):e104457.
33. Zhang X, Li B, Gao Y, et al. Localized delivery of mesenchymal stem cell spheroids via an injectable hydrogel for rheumatoid arthritis therapy. ACS Appl Bio Mater. 2026;13(1):e107.
34. Seror J, Stern M, Zarka R, Orr N. The potential use of novel plant-derived recombinant human collagen in aesthetic medicine. Plastic Reconstruct Surg. 2021;148(6s):32s–38s. doi:10.1097/PRS.0000000000008784
35. Jones B, Tonniges JR, Debski A, et al. Collagen fibril abnormalities in human and mice abdominal aortic aneurysm. Acta Biomater. 2020;110:129–140. doi:10.1016/j.actbio.2020.04.022
36. Chu PN, Zhu S, Dai X, Zhu S. A rat model investigation of enhanced facial rejuvenation via PCL microsphere-induced superior collagen neogenesis in the supraperiosteal plane. Aesthetic Plastic Surg. 2026;13(1):342–351.
37. Ding P, Lu E, Li G, Sun Y, Yang W, Zhao Z. Research progress on preparation, mechanism, and clinical application of nanofat. J Burn Care Res. 2022;43(5):1140–1144. doi:10.1093/jbcr/irab250
38. Lee KWA, Chan LKW, Lee CH, et al. Cannula is safer than needle in filler injection? JPRAS Open. 2026;48:415–424. doi:10.1016/j.jpra.2025.12.002
39. Boyd CJ, Nasr HY, Cassidy MF, et al. Experience with injectables performed at a resident department Aesthetic Surgery Clinic. JPRAS Open. 2026;48:735–745. doi:10.1016/j.jpra.2026.01.015
40. Soyal R, Digilli Ayaş B, Çiçekcibaşı AE, Bakdık S. Dangerous anatomical zones in terms of vascular structures for filler injections to the temporal region: a morphometric CT angiography study. Aesthetic Plastic Surg. 2025;42(26):3720–3759.
41. Myers B, Firsowicz M, Kamrani P, Dayan S, Fabi S. Injectables and facelifts: can we coexist? A retrospective chart review assessing injectable treatments preceding and following rhytidectomy. J Cosmet Dermatol. 2026;25(2):e70690. doi:10.1111/jocd.70690
42. Fox A, Guest L, Telfer T. Enhanced patient retention with formal, structured facial assessment and treatment planning: a multi-clinic real-world analysis. J Cosmet Dermatol. 2026;25(2):e70728. doi:10.1111/jocd.70728
43. Rahman E, Michon A, Rao P, et al. Filler-induced lymphatic compromise: in silico modelling of facial safety thresholds and injection techniques. Aesthetic Plastic Surg. 2026;34(21):2723–2759.
44. Borobia Pérez AI, Estévez Espejo JJ, Jiménez-González M, García López RD. Vulvovaginal collagen injection as a regenerative strategy in genitourinary syndrome of menopause: results of a pilot study. J Clin Med. 2026;15(4):399–410. doi:10.3390/jcm15041408
45. Wang T, Khan A, Gong L, Hong K, Qi L, Cui H. Safety and efficacy evaluation of composite collagen in human infraorbital anti-aging and nude mouse skin photoaging. Aesthetic Plastic Surg. 2025;49(9):2399–2410. doi:10.1007/s00266-025-04764-5
46. Baldassarri M, Ricciardello S, Ghinelli D, Perazzo L, Buda R. Porcine collagen injection therapy affects proximal hamstring tendinopathy in athletes by reducing time to return to sport. Sports. 2025;13(10):99–110. doi:10.3390/sports13100359
47. Shah-Desai S, Joganathan V. Novel technique of non-surgical rejuvenation of infraorbital dark circles. J Cosmet Dermatol. 2021;20(4):1214–1220. doi:10.1111/jocd.13705
48. Trinh LN, McGuigan KC, Gupta A. Delayed complications following dermal filler for tear trough augmentation: a systematic review. Facial Plastic Surg. 2022;38(3):250–259. doi:10.1055/s-0041-1736390
49. Goldberg DJ. Correction of tear trough deformity with novel porcine collagen dermal filler (Dermicol-P35). Aesthetic Surg J. 2009;29(3):S9–s11. doi:10.1016/j.asj.2009.02.013
50. Hao Q, Tian W, Chang H, Ai J. Collagen use in periorbital rejuvenation for chinese patients: the restoration injection for optimal rejuvenation technique. Plastic Reconst Surg Global Open. 2025;13(9):e7083. doi:10.1097/GOX.0000000000007083
51. Fink B, Campiche R, Shackelford TK, Voegeli R. Effects of under-eye skin and crow’s feet on perceived facial appearance in women of five ethnic groups. Int J Cosmet Sci. 2025;47(3):510–522. doi:10.1111/ics.13045
52. Cheong S, Yang H, Hao C, Lu F, He Y. Correction of infraorbital dark circles using autologous adipose-derived collagen filler: a novel regenerative option. Aesthetic Plastic Surg. 2024;48(22):4693–4701. doi:10.1007/s00266-024-04417-z
53. D’Arcangelis A, Goswami Chatterjee S, Diaz I, Guehenneux S, Namkoong J, Wu J. In vitro, ex vivo, instrumental and clinical evaluation of a topical cream on the signs of periorbital ageing. Int J Cosmet Sci. 2025;47(1):18–30. doi:10.1111/ics.12987
54. Lee WW, Fagien S, Murdock J, Bell M, Widgerow AD. A multi-center evaluation of restorative eye treatment and inhance with trihex technology to improve aesthetic outcomes when used pre- and post-blepharoplasty. Aesthetic Surg J Open Forum. 2023;5:ojac089. doi:10.1093/asjof/ojac089
55. Bhojani-Lynch T, Shah-Desai S, Bichet J-C, Magalhães B, Poupard K. Real-world evidence on the routine use, efficacy, and safety of a hyaluronic acid-based dermal filler in the periorbital region. Aesthetic Plastic Surg. 2025;49(15):4392–4402. doi:10.1007/s00266-025-04809-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.