Back to Journals » Clinical Ophthalmology » Volume 15
One-Year Outcomes of Intracorneal Ring–Segment Insertion Assisted by Femtosecond Laser Simultaneously Performed with Corneal Collagen Cross-Linking for Treatment of Keratoconus
Authors El-Massry A ![]() , Rashid K, Saad S, Osman I
, Rashid K, Saad S, Osman I
Received 11 August 2021
Accepted for publication 29 October 2021
Published 15 November 2021 Volume 2021:15 Pages 4447—4453
DOI https://doi.org/10.2147/OPTH.S333832
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Dr Scott Fraser
Ahmed El-Massry, Khalid Rashid ,† Seham Saad, Ihab Osman
Department of Ophthalmology, Alexandria Faculty of Medicine, Alexandria, Egypt
†Professor Khalid Rashid passed away on January 9, 2021.
Correspondence: Ahmed El-Massry
Department of Ophthalmology, Alexandria Faculty of Medicine, Champollion Street, El-Khartoum Square, El Azareeta Medical Campus, Alexandria, 21131, Egypt
Tel +20 122 215 2435
Email [email protected]
Purpose: To assess the results of simultaneously performed femtosecond laser–assisted Keraring intrastromal corneal ring–segment insertion and corneal collagen cross-linking for the treatment of keratoconus.
Patients and Methods: In this retrospective, noncomparative, interventional study, 30 eyes of 24 progressive-keratoconus patients of both sexes aged 18– 36 years old with poor best-corrected visual acuity (BCVA) and intolerance to contact lenses were included. All patients had been subjected to complete preoperative and postoperative ophthalmological examinations — unaided VA, BCVA, refraction, Pentacam, and contrast sensitivity examinations at 3-month, 6-month, and 1-year follow-ups.
Results: Mean unaided VA had changed significantly from 0.649± 0.239 logMAR preoperatively to 0.514± 0.222 (P=0.014), 0.419± 0.162 (P< 0.001), and 0.379± 0.142 (P< 0.001) logMAR at the three follow-up visits, respectively. Mean BCVA had changed significantly from 0.326± 0.144 logMAR preoperatively to 0.231± 0.140 (P=0.006) at 1-year follow-up. Mean spherical equivalent refraction had decreased significantly at 6-month (P=0.0298) and 1-year follow-up (P=0.0081). Mean steep keratometry (K2) had also significantly reduced from 51.89± 3.81 D to 49.87± 4.57 D (P=0.034) at 6 months and 49.40± 4.39 D (P=0.011) at 1 year. Mean refractive and keratometric astigmatism had significantly decreased at all follow-up visits.
Conclusion: At 1-year follow-up, keraring intrastromal corneal ring–segment insertion assisted by femtosecond laser performed simultaneously with corneal collagen cross-linking resulted in an improvement in visual, refractive, and topographic outcomes, which may suggest it is an effective treatment of keratoconus.
Keywords: keratoconus, corneal collagen cross-linking, Pentacam, ICRS
Introduction
Keratoconus is a progressive, noninflammatory, and bilateral (though asymmetrical) corneal ectatic disease where the cornea assumes a conical shape and thinning. It induces irregular astigmatism, and signs range from mild irregular astigmatism to severe thinning, scarring, and protrusion, leading to marked impairment of vision.1
The incidence and prevalence of keratoconus varies depending on many factors, such as the selected cohort of patients, geographic location, and criteria used for diagnosis. Keratoconus is diagnosed most frequently in young adults without significant sex differences, its onset commonly in puberty, and tends to progress until about the third or fourth decade of life.2
Intrastromal corneal ring segment (ICRS) implantation is an important treatment modality for keratoconus. ICRS was first proposed for the correction of low degrees of myopia, then used to correct ectatic corneal diseases. By shortening the central corneal arc length and redistributing the corneal biomechanical stress, ICRSs induce cornea flattening. Although ICRSs decrease astigmatism and corneal abnormalities, they actually do not eliminate or halt disease progression.3
The use of femtosecond-laser devices allows for simple and safe ICRS implantation with faster tunnel creation and precise control of depth, width, and centration, in addition to better customization of the tunnel and fast postoperative recovery. As such, it has a good impact on the patient satisfaction after surgery.4
Corneal collagen cross-linking (CXL) is the main treatment for keratoconus. It tends to stabilize the cornea and halt progression of the disease. As riboflavin (vitamin B2) is combined with UVA irradiation, it is excited to a triplet state and releases free radicals or reactive oxygen species into the surrounding stroma, resulting in cross-linking by increasing collagen-fiber diameter and the space between collagen fibrils.5
CXL can be combined with an additional refractive treatment, such as ICRS, PRK, PTK, or PIOLs, called “CXL plus.”6 Combining ICRS and CXL performed simultaneously or sequentially has a synergistic action on spherical equivalent refractions and keratometric values.7 However, if CXL is performed before ICRS, the flattening effect of the segments may be limited, due to the already fixed cornea by the effect of CXL into a suboptimal configuration.8 Research has shown no difference when comparing CXL alone with combined ICRS–CXL, and the CXL effect on collagen and corneal biomechanics actually reduced the effect of ICRS.9 To achieve the maximum overall effect, ICRS implantation should be performed first to reshape the cornea, and CXL can then be applied to stabilize the reshaped cornea.10
Patients and Methods
This was a retrospective noncomparative clinical study of 30 eyes of 24 progressive keratoconus patients of both sexes aged 18–36 years who had undergone combined femtosecond laser–assisted ICRS and CXL simultaneously at Roayah Vision Correction Center, Alexandria, Egypt. Institutional review board (ethics committee of Alexandria University Faculty of Medicine) approval was obtained (020940). All cases were operated on by the same surgeon (AEM).
Included were patients with intolerance to rigid gas-permeable contact lenses who had K values 48–<65 D documented with the Pentacam (Allegro Oculyzer, WaveLight, Erlangen, Germany). Excluded were those with K values ≥65 D, presence of active or recent ocular infections or inflammations, acute hydrops, corneal haze or opacities, or who were pregnant or breastfeeding during the study.
Informed consent was given by each patient after receiving a detailed description of the nature of the procedures. The study was conducted in accordance with Declaration of Helsinki tenets. All patients were subjected to complete preoperative and postoperative ophthalmological examinations — uncorrected visual acuity (VA), best-corrected VA (BCVA), refraction, Pentacam, and contrast sensitivity (CS; CSV-1000E, VectorVision, Dayton, OH, USA) — at 3-month, 6-month, and 1-year follow-up.
Patients underwent contrast-sensitivity monocular tests using BCVA and were graded using a ten-point scale for the four spatial frequencies tested: 3 cpd (row A), 6 cpd (row B), 12 cpd (row C), and 18 cpd (row D).
Patients unable to see any of the test strip scored 1 and those unable to see the highest-contrast bar scored 0 then these raw grades were converted into their corresponding log CS scores using definitions provided by VectorVision.11
Surgical Technique
The procedure comprised two steps: femtosecond-laser Keraring (Mediphacos, Belo Horizonte, Brazil) implantation followed by accelerated epithelium-off CXL in the same session. The proper ring segments were selected according to the nomogram provided by the manufacturer (Keraring calculation guidelines).
One of the three types of nomogram (A, B, and C) was used for each case based on corneal asymmetry type, keratometric values, and BCVA. The number of ring segments used was selected depending on many parameters: mainly the type and site of the keratoconus cone, keratometric readings, refraction, and corneal thickness. Topical anesthesia was given (benoxinate eyedrops [Benox, Epico, Cairo, Egypt]). Disinfection (povidone–iodine) of both eyes was performed, followed by draping and speculum application to the eye to be treated.
The first step (ICRS implantation) started with central corneal marking, followed by docking of the contact glass at its curved interface to the cornea by suction pressure. Femtosecond laser (VisuMax, Carl Zeiss Meditec), used for tunnel creation, was applied on the steepest corneal topographic axis at a depth of 80% of corneal thickness. Parameters used were 500 kHz frequency of approximately 1,040 nm wavelength laser, with spot size 1 μm and power of 5 mJ. The patient was released automatically from the laser system, incisions checked to ensure patency and segments implanted using forceps and a Sinskey hook. ICRSs were centered in the middle of the tunnel and equidistant from both incisions.
The second step was to perform CXL. The central 8 mm of the corneal epithelium was removed mechanically within the internal diameter of the rings, then riboflavin solution (0.1% riboflavin 5-phosphate and 20% dextran) was applied every 5 minutes for 30 minutes and continued every 5 minutes during irradiation. During irradiation, an accelerated CXL device (CCL Vario cross-linking system; Peschke Trade, Gdańsk, Poland) was used to emit UVA with wavelength of 370 nm and 18 mW/cm2 irradiance for 5 minutes equivalent to 5,400 mJ of the total energy dosage. At the end of the procedure, a contact lens was placed on each eye treated.
Postoperative Treatment
Postoperative treatment for all patients included topical therapy in the form of antibiotic eyedrops (moxifloxacin 0.5% [Vigamox, Alcon Laboratories, Fort Worth, TX, USA), corticosteroid eyedrops (prednisolone acetate 1% [PredForte, Allergan, Westport, Ireland]), and artificial tears (hypotonic sodium hyaluronate 0.15%). All eyedrop solutions were prescribed for all patients on 2-hourly bases on the first postoperative day, then four times daily in the first week. The frequency of medication was tapered to three times daily in the second week and twice daily in the third week. A systemic analgesic to manage pain due to CXL (diclofenac [Cataflam, Novartis, Switzerland]) was prescribed. Bandage contact lenses were removed on days 3–5.
Statistical Analysis
Data analysis was performed using SPSS 20.0. Quantitative data are described using medians and means ± SD. Qualitative data are presented as numbers and percentages. ANOVA was used for normally distributed data, with post hoc multiple comparisons when ANOVA results were significant. The significance of the postoperative results was determined at the 5% level.
Results
This study included 30 eyes of 24 progressive keratoconus patients who had completed 1-year minimum follow-up. Six patients had bilateral ICRS implantation. There were 13 men (54.17%) and eleven women (45.83%). All patients wereaged 18–36 (26.93±5.85) years.
There was continuous improvement in the UAVA throughout the study. Mean preoperative UAVA was 0.649±0.239 logMAR, and at 3 months, 6 months, and and year had significantly changed to 0.514±0.222 (P=0.014), 0.419±0.162 (P<0.001), and 0.379±0.142 (P<0.001) logMAR, respectively. Mean logMAR- BCVA had significantly improved from 0.326±0.144 logMAR preoperatively to 0.231±0.140 (P=0.006) at 1-year follow-up.
Mean spherical equivalent refraction had significantly decreased by 1.03 D at 6 months (P=0.0298) and 1.34D at 1 year (P=0.0081) from preoperative refraction, while the decrease in mean refractive astigmatism was significant at all follow-up times: at 1 year, there had been about a 2 D decrease from the preoperative value (P<0.001).
There were continuous decreases in all keratometric values, but the steepest K had significantly changed from 51.89±3.81 D preoperatively to 49.87±4.57 D (P=0.034) at 6 months and 49.40±4.39 D (P=0.011) at 1 year postoperatively. The decrease in keratometric astigmatism was significant at 3 months (P=0.041) and at 1 year (P=0.010) postoperatively.
Mean preoperative corneal thickness (at the thinnest location) was 434.90±40.50 µm, and had decreased significantly at 3 months postoperatively to 411.77±43.26 µm (P=0.018), then insignificant decreases thereafter. All these values ware shown in Table 1.
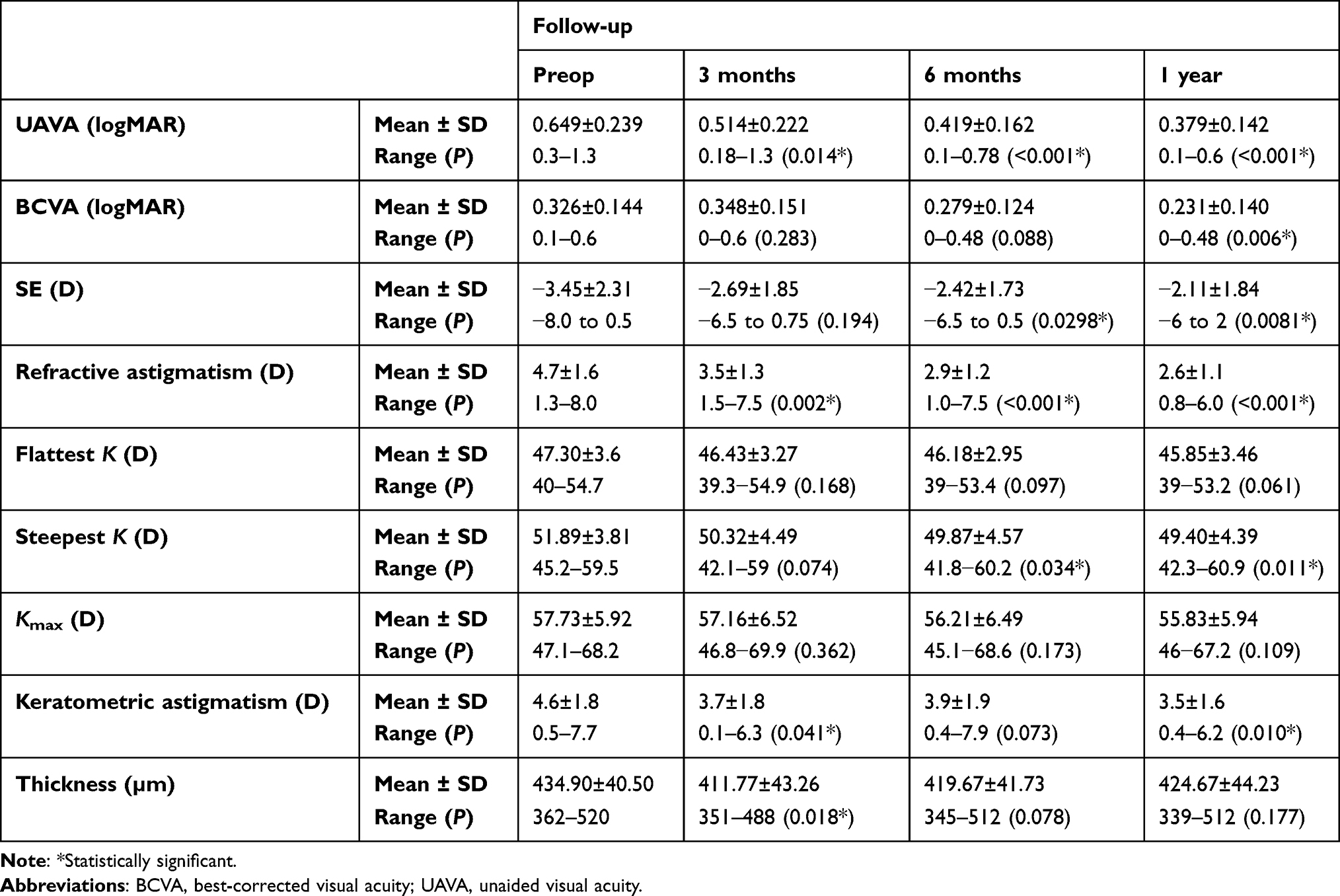 |
Table 1 Pre- and postoperative outcomes |
There was an improvement in mean log CS of low and high frequencies at 1 year from preoperative values, as shown in Table 2. For the 6 cpd frequency, the changes were statistically significant at 3 months (P=0.035), 6 months (P=0.009), and 1 year (P=0.032). Changes in high frequencies were statistically significant at 6 months and 1 year (P=0.036 and P=0.032) and for 18 cpd frequency at 6 months and 1 year (P=0.046 and P=0.018), respectively.
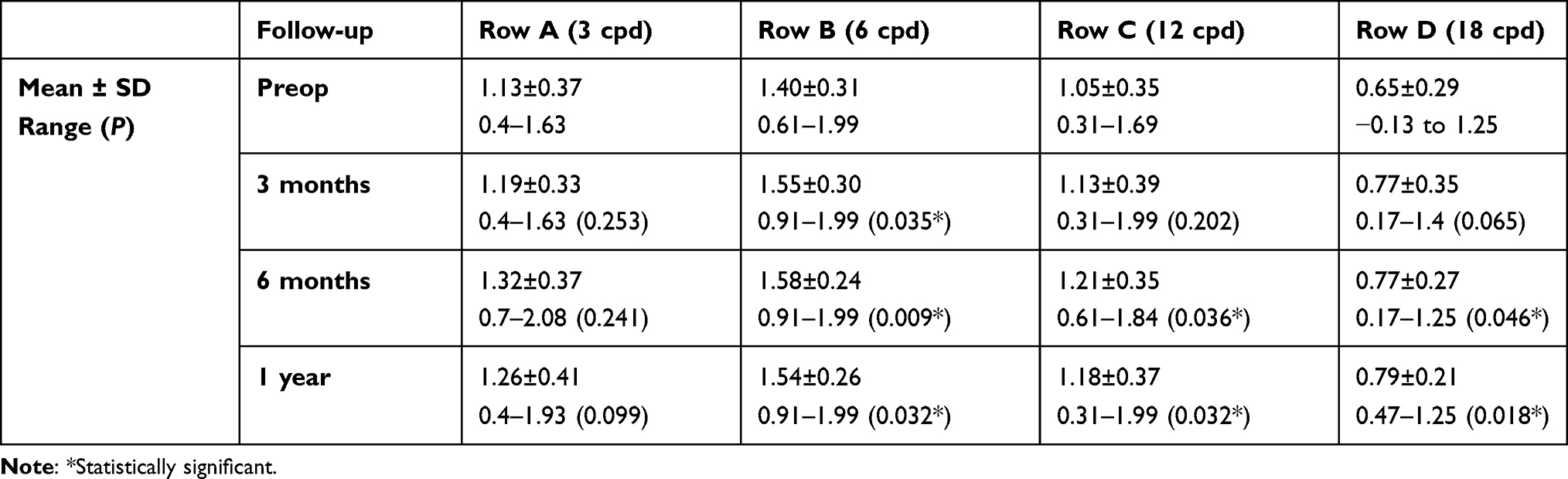 |
Table 2 Pre- and postoperative log contrast sensitivity |
Discussion
CXL with riboflavin (vitamin B2) and UVA has been considered the only true treatment for corneal ectasia that directly addresses the disease pathology, improves corneal biomechanical power, and stabilizes corneal biomechanical indices.12 On a molecular basis, ICRSs do not affect corneal biomechanical properties, but significantly flatten and regularize the central cornea.13 By combining these two methods, a synergism should arise to achieve better treatment results.14 There have been several reports of promising results with the combined treatment of CXL and ICRSs in offering not only stabilization of keratoconus but also improvement in visual and topographic outcomes.7,15
Questions arose about the correct sequence of treatment. CXL can be performed simultaneously with ICRSs before or after their implantation, but there is uncertainty about the ideal sequence of this combination. Liu et al reported no significant differences among three groups of eyes: sole ICRS implantation, ICRS implantation followed immediately by CXL, and CXL followed by ICRS implantation long after.10 On the other hand, Coskunseven et al showed that refractive, keratometric, and visual outcomes were statistically superior when ICRS placement is performed before rather than after CXL, and hypothesized that if performed first, CXL results in corneal stiffening and prevents full effectiveness of ICRSs.14
In our study, femtosecond laser–assisted ICRS implantation was performed with (at the same session) accelerated cross-linking. Analysis of preoperative and postoperative data during the first year’s follow-up proved that the procedure is safe and effective in preventing keratoconus progression, and its effect on visual, refractive, and corneal topography was addressed.
The combined procedure resulted in significant improvement in mean preoperative UAVA from 0.649±0.239 logMAR to 0.379±0.142 logMAR (P<0.001) at 1 year and mean BCVA from 0.326±0.144 logMAR preoperatively to 0.231±0.140 logMAR (P=0.006) at 1 year postoperatively. This improvement in UAVA could be attributed to a decrease in astigmatism, and indicates that the patient may have become more satisfied and less dependent on optical correction. The effectiveness of combined CXL and Keraring implantation using a femtosecond laser in improving vision and decreasing anterior corneal surface irregularities, reported also in Ibrahim et al7 and Coskunseven et al,16 also resulted an improvement in 78% of eyes for uncorrected CVA compared to preoperative levels and a gain of one to three lines of BCVA experienced in 68% of the studied eyes at 1-year follow-up.
Mean spherical equivalent refraction demonstrated a significant reduction of 1.03 D at 6 months (P=0.0298) and 1.34 D at 1 year (P=0.0081) postoperatively from preoperative refraction. We also observed a significant decrease in refractive astigmatism from the preoperative values of 2.03 D (P<0.001) at 1-year follow-up.
Our results correlate well with the studies of Kubaloglu et al17 and Ibrahim et al,7 which proved the success of Keraring implantation in reducing mean spherical equivalent refraction, and also with Coskunseven et al,14 who found astigmatic reduction at 13 months had reduced from −4.68±2.60 D preoperatively to −2.20±1.67 D when CXL was performed after ICRS (Keraring) implantation. This improvement in refraction may be explained by corneal flattening and regularization resulting from ICRS implantation being stabilized by the subsequent CXL application, causing additional stiffening and decreasing cylindrical power.
Regarding keratometry, there was a continuous decrease in all values. Although the changes in flattest K (K1) and maximum K (Kmax) were not significant, the steepest (K2) had significantly decreased by 2.02 D at 6 months (P=0.034) and 2.49 D at 1 year (P=0.011) from preoperative values. Keratometric astigmatism had significantly decreased at all follow-up points, and at 1 year had decreased by about 1 D (P=0.010). Other studies have shown similar findings, such as Henriquez et al,18 who reported significant reduction in mean maximum keratometry of 2.66 D and mean minimum keratometry of 1.61 D at 1 year postoperatively, and observed that the flattening process may continue for years. Kubaloglu et al17 proved a successful decrease in Kmax to 4 D with Keraring implantation after 6 months.
In our study, mean preoperative corneal thickness (at the thinnest location) was 434.90±40.50 µm, and had decreased significantly at 3 months to 411.77±43.26 µm (P=0.018). Although insignificant and not reach preoperative levels, there had been decreases in corneal thinning at other follow-ups. There is some disagreement on the effects of cross linking on corneal thickness, as some authors have reported decreased central corneal thickness from mean baseline readings (P<0.003),19 and others, such as Derakhshan et al20 reported a relatively small (9.1 µm) but significant increase in thickness after CXL. The effect of ICRS was addressed by Brendan et al,21 who reported a significant increase in corneal thickness. His results may be explained by ICRS implantation theoretically inducing corneal collagen remodeling. Acting as “spacers,” the ring segments might have increased corneal pachymetry through interfering in corneal collagen turnover.
There was an improvement in the mean log CS of low and high frequencies over 1 year of follow-up from preoperative values. For the 6 cpd frequency, it was statistically significant at 3 months (P=0.035), 6 months (P=0.009), and 1 year (P=0.032). Changes in high frequencies were statistically significant at 6 months and 1 year: 12 cpd (P=0.036, P=0.032), and 18 cpd (P=0.046, P=0.018) at 6 months and 1 year, respectively. The improvement in CS after CXL is the result of decreasing corneal curvature, astigmatism, and biomechanical stability.22
Mirzaei et al23 reported an improvement in mean CS in eyes undergoing CXL. CS had improved from a mean 1.52±0.16 log CS to 1.68±0.8 log CS (P=0.001) at 1-year follow-up. In other research there was an improvement in CS function after keraring implantation24 especially lower frequencies (3 cpd and 6 cpd), and reduction in the cylindrical component of the refraction.
Our study measured CS for 1 postoperatively, and there was improvement. The current study had no control group, a small sample, and retrospective design, but our results are discussed in relative to previous studies.
Conclusion
Over 1 year of follow-up, ICRS insertion assisted by femtosecond laser performed simultaneously with CXL resulted in improvements in visual, refractive, and topographic outcomes, which may suggest it is an effective treatment of keratoconus.
Acknowledgment
We dedicate this work to the soul of our colleague and professor Dr Khalid Rashid, who shared significantly in the development and implantation of all aspects of this work before leaving our world on January 9, 2021.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Romero JM, Santodomingo RJ, Wolffsohn JS. Keratoconus: a review. Cont Lens Anterior Eye. 2010;33(4):15766.
2. Godefrooij DA, de Wit GA, Uiterwaal CS, Imhof SM, Wisse RP. Age-specific incidence and prevalence of keratoconus: a nationwide registration study. Am J Ophthalmol. 2017;175:169–172. doi:10.1016/j.ajo.2016.12.015
3. Alio JL, Shabayek MH. Intracorneal ring segments (INTACS) for keratoconus correction: long term follow-up. J Cataract Refract Surg. 2006;32:978–985. doi:10.1016/j.jcrs.2006.02.044
4. Sansanayudh W, Bahar I, Kumar NL, et al. Intrastromal corneal ringsegment SK implantation for moderate to severe keratoconus. J Cataract Refract Surg. 2010;36:110–113. doi:10.1016/j.jcrs.2009.07.040
5. McCall AS, Kraft S, Edelhauser HF, et al. Mechanisms of corneal tissue cross-linking in response to treatment with topical riboflavin and long-wavelength ultraviolet radiation (UVA). Invest Ophthalmol Vis Sci. 2010;51:129–138. doi:10.1167/iovs.09-3738
6. Iqbal M, El Massry A, Tawfik A, et al. Evaluation of the effectiveness of cross-linking combined with photorefractive keratectomy for treatment of keratoconus. Cornea. 2018;37(9):1143–1150. doi:10.1097/ICO.0000000000001663
7. Ibrahim O, Elmassry A, Said A, Abdalla M, El Hennawi H, Osman I. Combined femtosecond laser-assisted intracornealring segment implantation and corneal collagen cross-linking for correction of keratoconus. Clin Ophthalmol. 2016;10:521–526.
8. Yeung SN, Ku JY, Lichtinger A, Low SA, Kim P, Rootman DS. Efficacy of single or paired intrastromal corneal ring segment implantation combined with collagen crosslinking in keratoconus. J Cataract Refract Surg. 2013;39:1146–1151. doi:10.1016/j.jcrs.2013.03.022
9. Henriquez MA, Izquierdo L, Bernilla C, McCarthy M. Corneal collagen cross-linking before ferrara intrastromal corneal ring implantation for the treatment of progressive keratoconus. Cornea. 2012;31(7):740–745. doi:10.1097/ICO.0b013e318219aa7a
10. Liu XL, Li PH, Fournie P, Malecaze F. Investigation of the efficiency of intrastromal ring segments with cross-linking using different sequence and timing for keratoconus. Int J Ophthalmol. 2015;8(4):703–708.
11. Mirzaie M, Sadigh AL, Mirzaie A. Contrast sensitivity comparison between two thin lenses, Thinoptx® versus Acrismart®, after micro incision cataract surgery. Iran J Ophthalmol. 2009;21(4):72–75.
12. Ivarsen A, Hjortdal J. Collagen cross-linking for advanced progressive keratoconus. Cornea. 2013;32(7):903–906. doi:10.1097/ICO.0b013e31828321dd
13. Giacomin NT, Mello RG, Medeiros CS, et al. Intracorneal ring segments implantation for corneal ectasia. J Refract Surg. 2016;32(12):829–839. doi:10.3928/1081597X-20160822-01
14. Coskunseven E, Jankov M
15. Alio´ JL, Toffaha BT, Pin˜ero DP, Klonowski P, Javaloy J. Crosslinking in progressive keratoconus using an epithelial debridement or intrastromal pocket technique after previous corneal ring segment implantation. J Refract Surg. 2011;27:737–743. doi:10.3928/1081597X-20110705-01
16. Coskunseven E, Kymionis G, Tsiklis N, et al. One-year results of intrastromal corneal ring segment implantation(KeraRing) using femtosecond laser in patients with keratoconus. Am J Ophthalmol. 2008;145(5):775–779. doi:10.1016/j.ajo.2007.12.022
17. Kubaloglu A, Sari E, Cinar Y, Koytak A, Kurnaz E, Ozerturk Y. Intrastromal corneal ring segment implantation for the treatment of keratoconus. Cornea. 2011;30(1):11–17. doi:10.1097/ICO.0b013e3181e2cf57
18. Henriquez MA, Izquierdo L, Bernilla C, Zakrzewski PA, Mannis M. Riboflavin/ultraviolet A corneal collagen cross-linking for the treatment of keratoconus: visual outcomes and scheimpflug analysis. Cornea. 2011;30(3):281–286. doi:10.1097/ICO.0b013e3181eeaea1
19. Antonios R, Abdul Fattah M, Maalouf F, Abiad B, Awwad S. Central corneal thickness after cross-linking using high-definition optical coherence tomography, ultrasound, and dual scheimpflug tomography: a comparative study over one year. Am J Ophthalmol. 2016;167:38–47. doi:10.1016/j.ajo.2016.04.004
20. Derakhshan A, Shandiz JH, Ahadi M, Daneshvar R, Esmaily H. Short-term outcomes of collagen crosslinking for early keratoconus. J Ophthalmic Vis Res. 2011;6(3):155–159.
21. Brendan P, Flynn B, Bhole A, et al. Mechanical strain stabilizes reconstituted collagen fibrils against enzymatic degradation by mammalian collagenase matrix metalloproteinase 8 (MMP-8). Cornea. 2010;5(8):123–137.
22. Wollensak G, Spoerl E, Seiler T. Stress-strain measurements of human and porcine corneas after riboflavin-ultraviolet-A-induced cross-linking. J Cataract Refract Surg. 2003;29:1780–1785. doi:10.1016/S0886-3350(03)00407-3
23. Mirzaei M, Mortazavi SZ, Taheri N, Sadigh A, Najafi A. Effects of collagen cross-linking on the corneal optical and topographic characteristics in progressive keratoconus. Adv Ophthalmol Vis Syst. 2015;2(3):43.
24. Paranhos J, Paranhos JR, Avila MP, Schor P. Analysis of the correlation between ophthalmic examination and quality of life outcomes following intracorneal ring segment implantation for keratoconus. Arq Bras Oftalmol. 2011;74(6):410–413. doi:10.1590/S0004-27492011000600005
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.