Back to Journals » Clinical Ophthalmology » Volume 10
One-stage bone strip reconstruction technique with balloon sinus dilatation surgery for chronic maxillary atelectasis
Authors Kashima T, Goldberg RA, Kohn JC, Rootman DB
Received 7 January 2016
Accepted for publication 10 March 2016
Published 25 November 2016 Volume 2016:10 Pages 2363—2368
DOI https://doi.org/10.2147/OPTH.S103809
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Tomoyuki Kashima,1 Robert A Goldberg,1 Jocelyne C Kohn,2 Daniel B Rootman1
1Division of Orbital and Oculoplastic Surgery, Stein Eye Institute, University of California, Los Angeles, CA, USA; 2Pasteur Ophthalmology Clinic, Oculoplastic, Orbit and Lacrimal Service, Santiago, Vitacura, Santiago Metropolitan Region, Chile
Purpose: Chronic maxillary atelectasis is characterized by unilateral spontaneous enophthalmos and hypoglobus due to increased orbital volume secondary to maxillary sinus inward deformation. Reformation of the sinus architecture and reconstruction of the orbit are key to a successful outcome. Here, we introduce a one-staged surgery that addresses both these goals.
Patients and methods: We retrospectively reviewed 11 patients treated with one-stage orbital and sinus surgery. A transconjunctival subperiosteal approach was used to create slats in the thinned orbital floor. A nasal endoscopic approach was utilized to access the maxillary sinus and place a modified Foley catheter balloon through the enlarged maxillary ostium. A bridge graft of nasal septal, ear cartilage, or LactSorb was placed on the reconstructed and balloon-supported orbital floor. The balloon was deflated and removed at 10–14 days. All patients underwent complete ophthalmic and orbital evaluation, including standardized photography and radiologic imaging.
Results: Eleven patients, mean age 39.5 years, presented with diplopia in upgaze, superior sulcus deformity, and at least 2 mm of relative enophthalmos. After initial overcorrection, enophthalmos improved in all cases. Symmetry within 1 mm was accomplished in 10 of 11 cases. Follow-up time was 259±320 days. Full motility was recovered in all patients.
Conclusion: We describe a one-staged surgery consisting of cutting slats in the orbital floor, dilating the maxillary sinus with a balloon, and stabilizing the orbital floor with a cartilage graft placement. Our anecdotal experience suggests that this surgical approach can safely achieve normalization of the pathologic sinus outflow and restoration of the orbit anatomy. The balloon ensures orbital floor stability during the healing process, and it may act to stent open the sinus ostium during early mucosal healing.
Keywords: silent sinus syndrome cartilage graft, orbital floor, remodeling
Introduction
Chronic maxillary atelectasis (CMA) or silent sinus syndrome is a rare disorder characterized by inward deformation of the maxillary sinus walls producing spontaneous enophthalmos and hypoglobus.1,2 Various hypotheses of the underlying mechanisms have been proposed, the most commonly accepted being that the occlusion of the maxillary sinus generates negative pressure and that this triggers the thinning and deformation of the bony walls.3 Endoscopic antrostomy is commonly used to reaerate the sinus.4–8 There is no consensus regarding the need for orbital reconstruction, the timing, and the ideal technique.9 In CMA, the radiographic appearance of the orbital floor is reported to present patchy demineralization, decreased bone density, and dramatic thinning.1,9,10 Here, we introduce a one-staged surgery that addresses remodeling orbital floor using bone strip technique with maxillary reconstruction.
Patients and methods
Patients
The charts of all patients undergoing surgery for CMA with orbital cartilage graft and balloon sinus dilatation at the Division of Orbital & Ophthalmic Plastic Surgery at the Jules Stein Eye Institute between July 2009 and July 2015 were reviewed. All patients underwent complete ophthalmic and orbital evaluation, including visual acuity, assessment of extraocular motility, Hertel ophthalmometry, photography, and radiologic imaging.
Surgical technique
All operations were performed under general anesthesia along with local injection of lidocaine 1% with epinephrine and nasal packing soaked in oxymetazoline 0.05%. A transconjunctival approach was used to access the orbital floor in the subperiosteal plane. Using a #15 Bard Parker blade, 4–5 anterior-to-posterior slats, ~4 mm wide, were created in the thinned orbital floor bone (Figure 1A). The slats were parallel to the infraorbital canal, sparing the infraorbital nerve (which was easily visualized in the thinned bone) and sparing the sinus mucus membrane. A graft was harvested from the ear cartilage from the scaphoid fossa and antihelix (n=3) as wide as ~7×35 mm2 or quadrangular cartilage from the septum (n=7) in the septoplasty manner as wide as 20×40 mm2 plane, trimmed, and placed as a bridge over the orbital floor to attach all bone strips as a beam (Figure 1B). In one patient, a resorbable poly-L-lactic acid/polyglycolic acid (PLLA-PGA) copolymer (LactoSorb) was used instead of a cartilage graft. An endoscope was then utilized to access the middle meatus. A right-angled hemostat was placed into the meatus, and the ostium was enlarged as required using a rongeur. The bone strips of the orbital floor were positioned to override each other in the manner of a Chinese fan. A Foley balloon catheter, modified by cutting the tip beyond the balloon, was inserted into the maxillary sinus (Figure 1C) and filled with 5–7 cm3 of saline. The globe position at the end of the procedure was titrated to overcorrect the enophthalmos by 1 mm, anticipating shrinkage during remodeling of orbital bones. After placement of graft or implant, the periosteum and palpebral conjunctiva were left without suturing. The distal end of the Foley was then tied firmly with a 2-0 silk tie, to maintain fluid in the balloon, and cut at the nostril. The balloon was removed in 10–14 days, by cutting above the silk suture to allow the water to drain out of the balloon (Figure 2A–C). Statistical significance was calculated using a Student’s t-test (Excel 2013; Microsoft, Redmond, WA, USA). Written informed consent was obtained from all patients. Ethics approval was obtained from UCLA (University of California, Los Angeles) Institutional Review Board for the study. The research was conducted in adherence to the tenets of the Declaration of Helsinki, and all patients gave informed consent to have their photographs published.
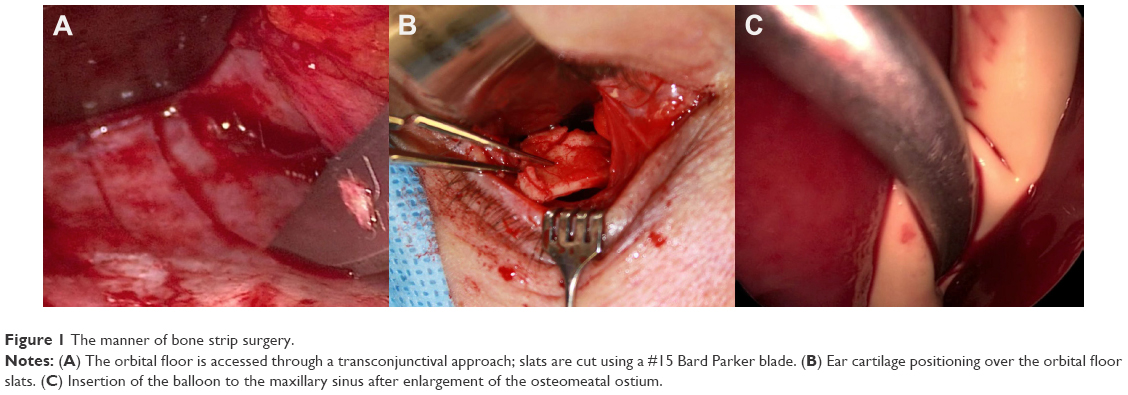 | Figure 1 The manner of bone strip surgery. |
 | Figure 2 Balloon insertion and extraction. |
Results
Eleven patients (10 male), mean age 39.5 years (range 23–62 years), had a diagnosis of maxillary atelectasis and underwent the described surgery. It affected the right eye in 6 cases and the left eye in 5 cases. All 11 patients noticed periorbital asymmetry (100%). Eight of 11 patients presented <1 year after the beginning of the symptoms, and 4 recalled past history of minor orbital trauma (>1 year prior with no history of orbital fracture) and 4 of chronic sinusitis. Two patients had undergone prior sinus surgery for recurrent sinusitis. Five presented with diplopia in upgaze and 2 with orbital pressure and pain. Preoperative examination revealed superior sulcus deformity and at least 2 mm of relative enophthalmos (average: 2.5 mm and range: 2–3 mm) in all patients.
Median and average follow-up periods following surgery were 15.4 weeks and 37±45.7 weeks, respectively (range 2–155 weeks). Postoperative relative enophthalmos was significantly improved in all cases (mean 2.0 mm and range: 1.0–4.0 mm; P<0.0001; Figures 3 and 4). Ten patients (91%) achieved symmetry within 1 mm, except for 1 patient who was settled as −2 mm. All five cases with diplopia improved after surgery. The postoperative self-limited complications observed immediately after surgery were chemosis (n=1; 9%), tooth pain (n=1; 9%), and infraorbital hypoesthesia (n=3; 27%). Complications that required surgical management were infectious sinusitis (n=1; 9%), 1 mm over correction (n=1; 9%), lower eyelid retraction (n=1; 9%), and nasolacrimal duct obstruction (n=1; 9%). There was no relationship between the surgical result and the materials used in orbital floor reconstruction.
 | Figure 3 Data of relative enophthalmos pre- and postsurgery. |
 | Figure 4 Pre- and postoperative photographs and scans. |
Discussion
We propose a one-staged surgery based on unpredictable improvement reported with sinus reaeration surgery alone. Sivasubramaniam et al11 reported complete resolution of enophthalmos in 78% of their patients following endoscopic uncinectomy and maxillary antrostomy. However, the results of this study are difficult to interpret because only 7 patients presented with facial asymmetry and clinical enophthalmos, and there was no objective measurement of exophthalmometry. Two of our cases had successful sinus surgery before presentation but still had residual enophthalmos. Thomas et al12 presented a series of 4 cases of isolated sinus aeration and observed a 16% increase in the sinus volume at postoperative month 9, but half of the patients required orbital surgery as a second stage. The combined approach is generally preferred at this time, as suggested by Brandt and Wright9 when reviewing 31/47 cases treated surgically and Soparkar et al13 who recommended a combined approach after treating 68 cases over the previous 7 years.
The use of a balloon provides early support as a buttress to the reconstituted orbital floor, which may be important during the healing phase. It also allows for intraoperative titration, filling the balloon as required in order to correct the enophthalmos. The balloon can also be used as a tool in procedures where the stability of the strut is compromised, for example, in floor and medial wall orbital fracture.
Postoperative relative enophthalmos significantly improved in all cases, although there were some undercorrections. Undercorrection may relate to incomplete orbital reconstruction or to late remodeling of the orbital floor; certainly, the goal at the time of surgery should be to accurately recreate the internal orbital architecture to a normal, or perhaps slightly overcorrected, configuration.
Various implants have been used in CMA to reconstruct the orbit including porous polyethylene,5,14,15 silicone block,10 Teflon,16 bone graft,6,8 and even hyaluronic acid gel fillers.17 We choose to use cartilage graft because it is an autologous implant and it is easily accessible for surgeons (especially if a septoplasty is also indicated). The graft adds volume, structural support, and forms a scaffold that heals by fibrosis, holding the bony slats in position to reform the orbital floor after the balloon is removed (Figure 5). The graft and implants work as a beam of orbital floor, which means that the graft does not need full width to cover the entire orbital floor. Although it is possible that the periosteum alone would allow the collapsed bone fragments to heal, in our early anecdotal experience before using the additional “beam” graft, undercorrections were more frequent. Absorbable alloplastic implants are another appropriate choice, and we used polydioxanone plate in one case. However, the cartilage graft seems to encourage formation of a stable orbital floor in our anecdotal experience and has the advantage of autogenous material. Thin bone grafts, including perpendicular plate bone, are another choice of material for the beam graft.
 | Figure 5 Scheme of bone strip floor reconstruction. |
Three patients noted pain and numbness in the infraorbital nerve distribution immediately after surgery, presumably related to balloon-induced pressure on the infraorbital nerve, and resolved after the balloon was removed, leaving no permanent damage.
We noted one case of postoperative nasolacrimal duct obstruction, which was successfully treated with endoscopic dacryocystorhinostomy. Chronic atelectasis can distort the sinus anatomy, making it difficult to identify the nasolacrimal duct running on the lateral nasal wall. The anatomy of the nasolacrimal duct should be considered in performing the antrostomy, and in difficult cases, intraoperative nasolacrimal intubation might be appropriately considered.
Postoperative sinusitis was noted only in one patient. Postoperative swelling can obstruct the newly created ostium, and the balloon may serve as a foreign body, exacerbating a postoperative infectious sinusitis. If infection develops, then endoscopic evaluation and mechanical rinsing of the sinus may be indicated, along with antibiotics. However, in our patients, no postoperative antibiotics were prescribed routinely.
Finally, a one-stage “Chinese fan” orbital slat bony floor reduction, orbital beam cartilage graft placement, and balloon sinus dilatation surgery may efficiently achieve reconstitution of the maxillary sinus architecture and outflow, as well as simultaneously achieving restoration of orbital anatomy. The balloon ensures both orbital floor stability and osteum patency by acting as a buttress and stent, respectively, during the healing process. The cartilage beam graft may serve as a scaffold to promote healing of the orbital floor in a normalized position and may provide some orbital volume. Based on our anecdotal experience, we believe that one-stage orbitosinus reconstruction using a maxillary balloon to support a cartilage graft over bony slats may represent a safe and effective treatment for CMA.
Acknowledgments
This study had no financial support. This article contains discussion of off-label use of Foley catheter.
Disclosure
The authors alone are responsible for the content and writing of the article. The authors report no conflicts of interest in this work.
References
Soparkar CN, Patrinely JR, Cuaycong MJ, et al. The silent sinus syndrome. A cause of spontaneous enophthalmos. Ophthalmology. 1994;101:772–778. | ||
Bahgat M, Bahgat Y, Bahgat A. Silent sinus syndrome. BMJ Case Rep. 2012. Available from: http://casereports.bmj.com/content/2012/bcr-2012-007198.full.pdf. | ||
Davidson JK, Soparkar CN, Williams JB, Patrinely JR. Negative sinus pressure and normal predisease imaging in silent sinus syndrome. Arch Ophthalmol. 1999;117:1653–1654. | ||
Blackwell KE, Goldberg RA, Calcaterra TC. Atelectasis of the maxillary sinus with enophthalmos and midface depression. Ann Otol Rhinol Laryngol. 1993;102(6):429–432. | ||
Behbehani R, Vacareza N, Bilyk JR, Rubin PA, Pribitkin EA. Simultaneous endoscopic antrostomy and orbital reconstruction in silent sinus syndrome. Orbit. 2006;25(2):97–101. | ||
Dinis PB, Branco C, Subtil J. Endonasal endoscopic repair of the orbital floor defect in the silent sinus syndrome. Otolaryngol Head Neck Surg. 2006;135:800–802. | ||
Sciarretta V, Pasquini E, Tesei F, Modugno GC, Farneti G. Endoscopic sinus surgery for the treatment of maxillary sinus atelectasis and silent sinus syndrome. J Otolaryngol. 2006;35:60–64. | ||
Cardesin A, Escamilla Y, Romera M, Molina JA. Single surgical step for endoscopic surgery and orbital reconstruction of a silent sinus syndrome. Acta Otorrinolaringol Esp. 2013;64:297–299. | ||
Brandt MG, Wright ED. The silent sinus syndrome is a form of chronic maxillary atelectasis: a systematic review of all reported cases. Am J Rhinol. 2008;22(1):68–73. | ||
Rose GE, Sandy C, Hallberg L, Moseley I. Clinical and radiologic characteristics of the imploding antrum, or “silent sinus,” syndrome. Ophthalmology. 2003;110:811–818. | ||
Sivasubramaniam R, Sacks R, Thornton M. Silent sinus syndrome: dynamic changes in the position of the orbital floor after restoration of normal sinus pressure. J Laryngol Otol. 2011;125(12):1239–1243. | ||
Thomas RD, Graham SM, Carter KD, Nerad JA. Management of the orbital floor in silent sinus syndrome. Am J Rhinol. 2003;17(2):97–100. | ||
Soparkar CN, Patrinely JR, Davidson JK. Silent sinus syndrome-new perspectives? Ophthalmology. 2004;111:414–415. [author reply 415–416]. | ||
Cobb AR, Murthy R, Cousin GC, et al. Silent sinus syndrome. Br J Oral Maxillofac Surg. 2012;50:e81–e85. | ||
Sesenna E, Oretti G, Anghinoni ML, Ferri A. Simultaneous management of the enophthalmos and sinus pathology in silent sinus syndrome: a report of three cases. J Craniomaxillofac Surg. 2010;38(6):469–472. | ||
Rapidis AD, Liarikos S, Ntountas J, Patel BC. The silent sinus syndrome: report of 2 cases. J Oral Maxillofac Surg. 2004;62:1028–1033. | ||
Mavrikakis I, Detorakis ET, Yiotakis I, Kandiloros D. Nonsurgical management of silent sinus syndrome with hyaluronic acid gel. Ophthal Plast Reconstr Surg. 2012;28(1):e6–e7. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.