Back to Journals » Clinical and Experimental Gastroenterology » Volume 19
Omalizumab-Induced Remission and Steroid Withdrawal in Refractory Eosinophilic Gastroenteritis with Severe Hypereosinophilia: A Case Report
Authors Du Z, Zhou W ![]() , Li J, Ma L, Zhu Q, Zhi Y
, Li J, Ma L, Zhu Q, Zhi Y ![]()
Received 6 May 2025
Accepted for publication 1 December 2025
Published 12 January 2026 Volume 2026:19 533173
DOI https://doi.org/10.2147/CEG.S533173
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Andreas M. Kaiser
Zhirong Du,1 Weixun Zhou,2 Ji Li,3 Li Ma,4 Qingli Zhu,4 Yuxiang Zhi1
1Department of Allergy, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing Key Laboratory of Precision Medicine for Diagnosis and Treatment of Allergic Disease, National Clinical Research Center for Dermatologic and Immunologic Diseases, Beijing, 100730, People’s Republic of China; 2Department of Pathology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Beijing, 100730, People’s Republic of China; 3Department of Gastroenterology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Beijing, 100730, People’s Republic of China; 4Department of Ultrasound, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Beijing, 100730, People’s Republic of China
Correspondence: Yuxiang Zhi, Department of Allergy, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing Key Laboratory of Precision Medicine for Diagnosis and Treatment of Allergic Disease, National Clinical Research Center for Dermatologic and Immunologic Diseases, Beijing, 100730, People’s Republic of China, Email [email protected]
Abstract: Eosinophilic gastroenteritis (EGE) is a rare, immune-mediated disorder characterized by pathological eosinophilic infiltration of the gastrointestinal tract. Corticosteroids are the primary treatment for EGE, but managing patients who are corticosteroid-dependent can be challenging. This report describes a 33-year-old female patient with EGE and severe hypereosinophilia, who was corticosteroid-dependent and had been on long-term oral corticosteroids for 5 years with an increasing maintenance dose. The patient achieved effective treatment with omalizumab without adverse reactions. This case provides evidence for the efficacy and safety of omalizumab in patients with corticosteroid-dependent eosinophilic gastroenteritis and severe hypereosinophilia.
Keywords: eosinophilic gastroenteritis, hypereosinophilia, omalizumab
Introduction
Eosinophilic gastrointestinal diseases (EGIDs) represent a group of chronic inflammatory conditions marked by the abnormal accumulation of eosinophils in various segments of the gastrointestinal tract.1–3 Among these, eosinophilic esophagitis (EoE) is the most prevalent and well-characterized subtype. Non-esophageal forms of EGIDs encompass eosinophilic gastritis (EoG), eosinophilic enteritis (EoN), and eosinophilic colitis (EoC).2–5 EoG and EoN were historically collectively referred to as eosinophilic gastroenteritis (EGE).6 EGE is a rare condition, the prevalence is 3–8 per 100000 individuals,7,8 and its incidence is increasing.9 The rising incidence is partly attributed to improved diagnosis and awareness, though environmental and lifestyle changes that disrupt immune regulation may also contribute to an actual increase. Corticosteroids are the primary treatment for EGE,10 but 48.8% of patients with EGE were glucocorticoid dependent.11 The precise mechanisms underlying the reliance of EGE on glucocorticoids remain elucidated. Glucocorticoid dependence in EGE is primarily driven by chronic eosinophilic inflammation and dysregulated immune responses, particularly involving Th2 cytokines such as IL-4, IL-5, and IL-13.12,13 These cytokines promote eosinophil recruitment, survival, and activation in the gastrointestinal mucosa, leading to tissue damage and persistent symptoms, which may result in a dependence on glucocorticoids to control eosinophil-mediated tissue injury.
Prolonged corticosteroid use is associated with a range of potential adverse effects, including hypertension, diabetes, and osteoporosis, which impair quality of life.14 Immunomodulators such as azathioprine and 6-mercaptopurine may be used as steroid-sparing agents. However, their efficacy requires further validation in more studies.9 Omalizumab, a humanized monoclonal antibody targeting the high-affinity IgE receptor, binds to free IgE, preventing its attachment to IgE receptors on mast cells, basophils, and eosinophil, has shown promise in reducing peripheral eosinophilia and alleviating symptoms in patients with EGE.15,16 However, available data are limited, and its therapeutic efficacy remains debated.15 Additionally, there are no reports on the use of omalizumab to treat eosinophilic gastroenteritis with severe hypereosinophilia. Here, we report a case of glucocorticoid-dependent EGE with severe hypereosinophilia, that was successfully resolved with omalizumab and report no adverse effect.
Case Presentation
A 33-year-old female patient presented with abdominal pain, ascites and peripheral blood eosinophilia, was diagnosed with eosinophilic gastroenteritis for 9 years. The patient had a history of hyperthyroidism and was treated with oral methimazole since 2012. The patient denied any history of rhinitis, asthma or eczema. In December 2022, she visited our allergy and hematology department for the first time due to glucocorticoid dependency over the past 7 years.
In 2013, the patient experienced abdominal pain and eosinophilia, which responded well to glucocorticoid therapy. The corticosteroids were tapered and discontinued after one month.
However, in 2017, abdominal pain recurred along with ascites, and laboratory tests revealed significantly elevated peripheral blood eosinophils (13 × 109/L). Esophageal biopsy revealed features of acute and chronic inflammation, with no evidence of eosinophilic infiltration. A duodenal biopsy showed acute and chronic mucosal inflammation with superficial erosion and infiltration of lymphocytes, plasma cells, and eosinophils (>25/HPF). Biopsy specimens obtained from the transverse colon revealed chronic mucosal inflammation with lymphoid follicle formation and multifocal eosinophilic infiltration (>25/HPF). Ascitic fluid analysis revealed a large number of eosinophils and a small number of lymphocytes. The patient underwent further extensive evaluation, including stool tests for parasites, H. pylori testing, antinuclear antibodies, antineutrophil cytoplasmic antibodies, chest CT, bone marrow aspiration, and biopsy to rule out parasitic infections, autoimmune diseases and hematological diseases, confirming a diagnosis of eosinophilic gastroenteritis.
From 2017 to 2020, the patient’s condition remained stable with a daily oral dose of 5 mg prednisone. In September 2020, abdominal pain, ascites, and eosinophilia recurred despite this maintenance dose. Increasing the glucocorticoid dose controlled the symptoms, and the minimum effective dose of prednisone was adjusted to 10 mg daily, which was maintained for 2 years. Unfortunately, in September 2022, the disease relapsed, with peripheral blood eosinophils rising to 15.0 × 109/L. Gastrointestinal pathology showed mild active inflammation in the descending duodenum, with an increase in eosinophils in the deeper layers of the mucosa, some located in the mucosal muscle layer, and occasional infiltration of the epithelium (Figure 1A–C). Prednisone was increased to 40 mg daily and gradually reduced to 25 mg daily by December 2022, when she first presented to our department. The total serum immunoglobulin (Ig) E level was elevated (1090kU/L), with specific IgE positive to mugwort (w6, 0.6 kUA/L) and house dust mite mix 1 (ds1, 0.47 kUA/L); all food sIgE tests were negative. To facilitate glucocorticoid tapering, imatinib was initiated at 0.4 g daily. Methimazole was discontinued following radioactive iodine therapy for hyperthyroidism to rule out its potential effect on eosinophils. Six months later, glucocorticoids were tapered and discontinued, meanwhile the patient adherent to a six-food elimination diet (6-FED). However, dull lower abdominal pain recurred, and peripheral blood eosinophils increased to 1.12 × 109/L within 2 weeks. One month later, peripheral blood eosinophils surged to 21.03 × 109/L. Intestinal ultrasound revealed thickening of the stomach, ascending colon, and transverse colon, as well as abdominal lymphadenopathy and a small amount of ascitic fluid. Serum IgE levels were markedly elevated (989 kU/L). Omalizumab was initially administered at a dose of 300 mg every four weeks. After 8 weeks, the abdominal pain resolved and peripheral blood eosinophil levels dropped to 3.79 × 109/L. By 16 weeks, eosinophil levels further declined to 0.59 × 109/L. The dosing interval was subsequently extended to 300 mg every six weeks. However, peripheral blood eosinophil levels increased slightly after two treatments, the dosing frequency was reverted to 300 mg every four weeks for 6 months, and eosinophil levels stabilized between 0.8 and 2.81 × 109/L. The dosing interval was then extended again to every six weeks, with a total of two injections, during which peripheral blood eosinophil levels remained stable at 0.38 to 0.57 × 109/L (Figure 2). Intestinal ultrasound re-examination showed no significant thickening of the small intestine or colon walls. Fourteen months after the initiation of omalizumab treatment, gastroscopic biopsy re-examination showed that the eosinophils in the gastrointestinal tissue decreased to normal levels, with chronic inflammation in the descending duodenum, accompanied by lymphocyte infiltration (Figure 1D–F). The patient did not report any adverse reactions.
 |
Figure 1 Pathological findings in this patient. (A–C) Biopsy at disease flare, shows that mild active inflammation in the descending duodenum, with an increase in eosinophils in the deeper layers of the mucosa, some located in the mucosal muscle layer, and occasional infiltration of the epithelium. (D–F) Biopsy after 16 months of omalizumab treatment, shows that eosinophils in the gastrointestinal tissue decreased to normal levels, with chronic inflammation in the descending duodenum, accompanied by lymphocyte infiltration. |
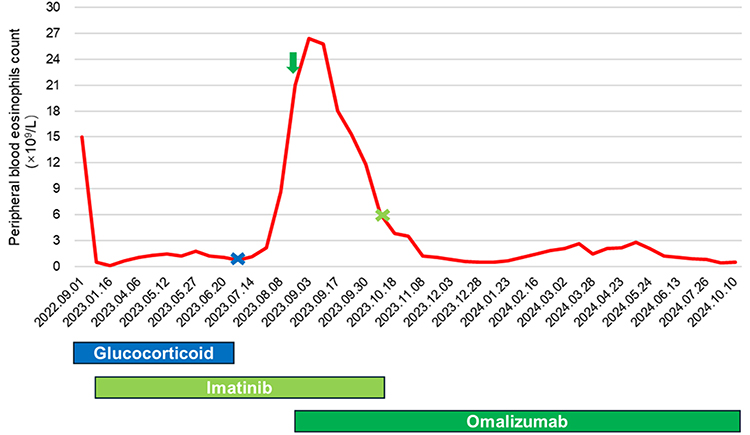 |
Figure 2 Peripheral Blood Eosinophil Count Over Time with Treatment Interventions. This graph depicts the peripheral blood eosinophil count (×109/L) from September 2022 to October 2024. The timeline of treatments is indicated by distinct colors: glucocorticoid (blue), imatinib (light green), and omalizumab (dark green). The blue “X” marks the cessation of glucocorticoid treatment, the light green “X” denotes the discontinuation of imatinib, and the dark green arrow signifies the initiation of omalizumab therapy. |
Discussion and Conclusions
Herein, we report a case of glucocorticoid-dependent eosinophilic gastroenteritis with severe hypereosinophilia. Given the documented association between carbimazole and eosinophilic gastroenteritis in rare cases,17 the drug was stopped post-radioactive iodine therapy to rule out its effects on eosinophils. However, the disease still relapsed. Omalizumab was subsequently administered and effectively induced and maintained remission. The efficacy of Omalizumab in the treatment of eosinophilic gastroenteritis remains uncertain, with limited studies reporting its effectiveness.15,16 However, its efficacy in patients with concomitant severe hypereosinophilia has not yet been reported. Therefore, our case confirms the therapeutic effect of Omalizumab in glucocorticoid-dependent eosinophilic gastroenteritis with severe hypereosinophilia and highlights its potential as a treatment option in patients.
EGE is characterized by abdominal pain, diarrhea, nausea, and vomiting.10,18 Abnormally increased eosinophil infiltration in the stomach and bowel is a key histopathological characteristic.9 Although 80% of patients with EGE show elevated peripheral eosinophil counts, the average level is 1000 cells/μL,11,19,20 severe hypereosinophilia is rare. Corticosteroids are the mainstay of treatment for EGE.10 However, 48.8% of patients were glucocorticoid dependent. Given the adverse effects of long-term corticosteroid use and refractory status, other therapies, including omalizumab, have been explored.10,21
Omalizumab has been approved by the FDA for the prevention of food allergies.22 Studies have shown that it may facilitate the up-dosing phase of food immunotherapy and reduces the risk of allergic reactions during treatment.23 A single-center study reported that omalizumab reduced peripheral eosinophilia and improved clinical symptoms in patients with EGE. However, the reduction in tissue eosinophil counts did not achieve statistical significance.15 In contrast, two case studies documented complete normalization of both clinical symptoms and tissue eosinophilia following omalizumab treatment.16,24. Given the heterogeneity of EGE, small study sizes, and potential publication bias, larger cohort studies are needed for definitive confirmation of omalizumab’s efficacy and to discover predictive biomarkers. There are no reports on the use of omalizumab for treating eosinophilic gastroenteritis with severe hypereosinophilia. Omalizumab treatment in our patient resulted in a favorable clinical response, characterized by symptomatic improvement, reduced peripheral blood eosinophil count, enhanced endoscopic findings, and histologic remission. The treatment was well-tolerated with no adverse events observed. This outcome suggests a potential involvement of IgE-mediated pathways in the pathogenesis of EGE in this case. Omalizumab was found to play a unique role in reducing co-stimulatory molecules expression on eosinophil and serum eotaxin-1 levels in severe allergic asthmatics.25 The mechanism of omalizumab in the treatment of EGE remains elusive. Omalizumab has a favorable safety profile compared to systemic corticosteroids. However, its high cost may limit accessibility, and clinical response can be variable due to the heterogeneity of EGE. Given the heterogeneous and complex pathogenesis of EGE, further studies are essential to identify which patient subgroups are most likely to benefit from biologic therapy and to determine predictive factors for a favorable clinical response. Importantly, as omalizumab is used off-label in EGE, no standardized dosing regimen or frequency has been established. Therefore, additional research is urgently needed to establish optimized, disease-specific dosing protocols and treatment intervals. Our report suggested significant improvement in glucocorticoid-dependent eosinophilic gastroenteritis with severe hypereosinophilia after treatment with Omalizumab, and provided evidence for the potential of anti-IgE therapy in the treatment of eosinophilic gastroenteritis, even with severe hypereosinophilia. In addition, further research and clinical trials are needed to validate the effectiveness and safety of Omalizumab.
Ethics and Consent
Written informed consent has been provided by the patient to have the case details and any accompanying images published. The patient acknowledged that no personally identifiable information would be disclosed. This study was reviewed and approved by the Institutional Review Board of Peking Union Medical College Hospital. The case details are provided as open-access and do not require institutional approval for access.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by National High Level Hospital Clinical Research Funding (2022-PUMCH-B-090).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rothenberg ME, Hottinger SKB, Gonsalves N, et al. Impressions and aspirations from the FDA GREAT VI workshop on eosinophilic gastrointestinal disorders beyond eosinophilic esophagitis and perspectives for progress in the field. J Allergy Clin Immunol. 2022;149(3):844–6. doi:10.1016/j.jaci.2021.12.768
2. Low EE, Dellon ES. Review article: emerging insights into the epidemiology, pathophysiology, diagnostic and therapeutic aspects of eosinophilic oesophagitis and other eosinophilic gastrointestinal diseases. Aliment Pharmacol Ther. 2024;59(3):322–340. doi:10.1111/apt.17845
3. Dellon ES, Gonsalves N, Abonia JP, et al. International consensus recommendations for eosinophilic gastrointestinal disease nomenclature. Clin Gastroenterol Hepatol. 2022;20(11):2474–2484e2473. doi:10.1016/j.cgh.2022.02.017
4. Kinoshita Y, Sanuki T. Review of Non-Eosinophilic Esophagitis-Eosinophilic Gastrointestinal Disease (Non-EoE-EGID) and a case series of twenty-eight affected patients. Biomolecules. 2023;13(9):1417. doi:10.3390/biom13091417
5. Wright BL, Abonia JP, Abud EM, et al. Advances and ongoing challenges in eosinophilic gastrointestinal disorders presented at the CEGIR/TIGERs symposium at the 2024 American academy of allergy, asthma & immunology meeting. J Allergy Clin Immunol. 2024;154(4):882–892. doi:10.1016/j.jaci.2024.07.022
6. Marasco G, Visaggi P, Vassallo M, et al. Current and novel therapies for eosinophilic gastrointestinal diseases. Int J Mol Sci. 2023;24(20):15165. doi:10.3390/ijms242015165
7. Jensen ET, Martin CF, Kappelman MD, Dellon ES. Prevalence of eosinophilic gastritis, gastroenteritis, and colitis: estimates from a national administrative database. J Pediatr Gastroenterol Nutr. 2016;62(1):36–42. doi:10.1097/MPG.0000000000000865
8. Mansoor E, Saleh MA, Cooper GS. Prevalence of Eosinophilic gastroenteritis and colitis in a population-based study, from 2012 to 2017. Clin Gastroenterol Hepatol. 2017;15(11):1733–1741. doi:10.1016/j.cgh.2017.05.050
9. Li K, Ruan G, Liu S, et al. Eosinophilic gastroenteritis: pathogenesis, diagnosis, and treatment. Chin Med J. 2023;136(8):899–909. doi:10.1097/CM9.0000000000002511
10. Chen PH, Anderson L, Zhang K, Weiss GA. Eosinophilic Gastritis/Gastroenteritis. Curr Gastroenterol Rep. 2021;23(8):13. doi:10.1007/s11894-021-00809-2
11. Li KW, Ruan GC, Liu S, et al. Long-term prognosis and its associated predictive factors in patients with eosinophilic gastroenteritis. World J Gastroenterol. 2024;30(2):146–157. doi:10.3748/wjg.v30.i2.146
12. Shoda T, Wen T, Caldwell JM, et al. Molecular, endoscopic, histologic, and circulating biomarker-based diagnosis of eosinophilic gastritis: multi-site study. J Allergy Clin Immunol. 2020;145(1):255–269. doi:10.1016/j.jaci.2019.11.007
13. Caldwell JM, Collins MH, Stucke EM, et al. Histologic eosinophilic gastritis is a systemic disorder associated with blood and extragastric eosinophilia, TH2 immunity, and a unique gastric transcriptome. J Allergy Clin Immunol. 2014;134(5):1114–1124. doi:10.1016/j.jaci.2014.07.026
14. Volmer T, Effenberger T, Trautner C, Buhl R. Consequences of long-term oral corticosteroid therapy and its side-effects in severe asthma in adults: a focused review of the impact data in the literature. Eur Respir J. 2018;52(4). doi:10.1183/13993003.00703-2018
15. Foroughi S, Foster B, Kim N, et al. Anti-IgE treatment of eosinophil-associated gastrointestinal disorders. J Allergy Clin Immunol. 2007;120(3):594–601. doi:10.1016/j.jaci.2007.06.015
16. Du Z, Wang Z, Zhou W, Yin J, Zhi Y. Eosinophilic gastritis and gluten-sensitive enteropathy manifested as hypoproteinemia and treated with omalizumab: a case report. Allergy Asthma Clin Immunol. 2024;20(1):19. doi:10.1186/s13223-024-00878-8
17. Hafidh K, Kazmi T, Alhaj A, Nazir Z. Carbimazole-induced eosinophilic gastroenteritis in a young female with abdominal pain and ascites: a case report. J Med Case Rep. 2024;18(1):559. doi:10.1186/s13256-024-04866-9
18. Sato H, Honma T, Owaki T, Tominaga K, Yokoyama J, Terai S. Clinical and pathological profile of eosinophilic gastroenteritis. Eur J Gastroenterol Hepatol. 2019;31(2):157–162. doi:10.1097/MEG.0000000000001241
19. Gonsalves N. Eosinophilic gastrointestinal disorders. Clin Rev Allergy Immunol. 2019;57(2):272–285. doi:10.1007/s12016-019-08732-1
20. Chang JY, Choung RS, Lee RM, et al. Talley NJ: a shift in the clinical spectrum of eosinophilic gastroenteritis toward the mucosal disease type. Clin Gastroenterol Hepatol. 2010;8(8):
21. Dellon ES, Spergel JM. Biologics in eosinophilic gastrointestinal diseases. Ann Allergy Asthma Immunol. 2023;130(1):21–27. doi:10.1016/j.anai.2022.06.015
22. Casale TB, Fiocchi A, Greenhawt M. A practical guide for implementing omalizumab therapy for food allergy. J Allergy Clin Immunol. 2024;153(6):1510–1517. doi:10.1016/j.jaci.2024.03.019
23. Riggioni C, Oton T, Carmona L, Du Toit G, Skypala I, Santos AF. Immunotherapy and biologics in the management of IgE-mediated food allergy: systematic review and meta-analyses of efficacy and safety. Allergy. 2024;79(8):2097–2127. doi:10.1111/all.16129
24. Han D, Lee JK. Severe asthma with eosinophilic gastroenteritis effectively managed by mepolizumab and omalizumab. Ann Allergy Asthma Immunol. 2018;121(6):742–743. doi:10.1016/j.anai.2018.07.030
25. Yan H, Sun L, Ni Y, et al. Effective omalizumab treatment influenced eosinophil function in severe allergic asthmatics. J Thorac Dis. 2023;15(6):3115–3125. doi:10.21037/jtd-22-1818
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.