Back to Journals » Clinical Interventions in Aging » Volume 20
Older Patients’ Postoperative Neurocognitive Recovery: A Narrative Review
Authors Nilsson U ![]() , Amirpour A, Lampi M
, Amirpour A, Lampi M ![]() , Guenna Holmgren A, Markovic G, Zecevic E
, Guenna Holmgren A, Markovic G, Zecevic E ![]() , Nömm M, Drakenberg A, Claesson Lingehall H, Damén T, Martinik A, Saarijärvi M, Bergman L, Eckerblad J
, Nömm M, Drakenberg A, Claesson Lingehall H, Damén T, Martinik A, Saarijärvi M, Bergman L, Eckerblad J
Received 9 August 2025
Accepted for publication 1 December 2025
Published 16 December 2025 Volume 2025:20 Pages 2579—2591
DOI https://doi.org/10.2147/CIA.S559531
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Ulrica Nilsson,1 Anahita Amirpour,1 Maria Lampi,1– 3 Amina Guenna Holmgren,1 Gabriela Markovic,4,5 Ernad Zecevic,1,6 Marcus Nömm,2,6 Anna Drakenberg,7,8 Helena Claesson Lingehall,7,8 Tor Damén,9,10 Anna Martinik,10 Markus Saarijärvi,1,11 Lina Bergman,1 Jeanette Eckerblad1 On behalf of PeriBrainCare
1Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, Stockholm, Sweden; 2Department of Clinical Science, Intervention and Technology (CLINTEC), Karolinska Institute, Stockholm, Sweden; 3Department of Upper Abdominal Diseases, Karolinska University Hospital, Stockholm, Sweden; 4Department of Clinical Sciences, Danderyd University Hospital, Karolinska Institutet, Stockholm, Sweden; 5Department of Rehabilitation Medicine, Danderyd University Hospital, Stockholm, Sweden; 6Perioperative Medicine and Intensive Care, Karolinska University Hospital, Stockholm, Sweden; 7Faculty of Medicine and Health, School of Health Sciences, Örebro University, Örebro, Sweden; 8Department of Cardiothoracic and Vascular Surgery, Örebro University Hospital, Örebro, Sweden; 9Department of Anaesthesiology and Intensive Care Medicine, Institute of Clinical Sciences, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; 10Department of Cardiothoracic Anaesthesia and Intensive Care, Sahlgrenska University Hospital, Gothenburg, Sweden; 11Department of Cardiology, Danderyd Hospital, Stockholm, Sweden
Correspondence: Ulrica Nilsson, Email [email protected]
Abstract: Perioperative neurocognitive disorders, including postoperative delirium, delayed neurocognitive recovery and mild/major postoperative neurocognitive disorder, are common complications that affect older adults after surgery. Postoperative delirium, which occurs in 10– 60% of major surgery patients, can increase the risk of delayed neurocognitive recovery and postoperative neurocognitive disorder, which affects 10– 25% of patients. Preoperative and postoperative assessment of neurocognitive functioning typically involve the use of screening tools, such as Mini-Cog or 4AT. Despite the availability of evidence-based cognitive screening tools, many patients remain undiagnosed in clinical settings. Both postoperative delirium and postoperative neurocognitive disorder can lead to long-term cognitive and emotional complications, such as forgetfulness, trouble with initiating tasks, and mood disturbances. Next of kin experience considerable distress when witnessing delirium in a family member, a situation that is frequently exacerbated by a lack of information from health care professionals. Ethical challenges arise when cognitive impairment impacts patients’ decision-making capacity, raising concerns about autonomy, use of restraints, and resource allocation. Informing patients about their risk of postoperative neurocognitive disorder before surgery is vital; however, it is not standardized in clinical practice. Further, there is a notable lack of interventions aimed at promoting neurocognitive recovery, with most guidelines relying on expert consensus. This narrative review therefore aims to explore recent advances in perioperative neurocognitive recovery, focusing on symptomatology, patient and next of kin experiences, assessments, care interventions and ethical aspects.
Keywords: postoperative neurocognitive decline, postoperative delirium, patient experiences, next of kin, delayed neurocognitive recovery
Background
Life expectancy is increasing worldwide, and the number of older adults (≥65 years) is growing rapidly, particularly those aged 85 and older.1 Advancing age is associated with a higher prevalence of mild cognitive impairment and dementia.2 Concurrently, a growing proportion of older adults are undergoing surgery, largely due to medical advances that make complex procedures feasible and safe in this age group. This increase is particularly common for procedures such as knee and hip replacements, cardiac surgeries, bladder surgeries, and prosthetic lens implantation. On average, surgical patients are 14.5 years older than the general population, reflecting the increasing representation of older adults among surgical cohorts.3 Despite the growing number of older adults undergoing surgery, post-surgical hospital stays remain relatively short, with an average duration of five days.3 This leaves a substantial portion of postoperative recovery to take place at home.4
During this recovery phase, patients often have to manage co-occurring symptoms and illnesses on their own, and if possible, with support from their next of kin.4,5 Postoperative complications in older patients are more likely to be medical than surgical, with perioperative neurocognitive disorders being a common issue.6 Furthermore, over 50% of the older population experiences multimorbidity, further complicating recovery and hindering their ability to resume daily activities.7 It has been suggested that early recognition of postoperative neurocognitive decline, along with the provision of comprehensive care for older patients, may improve outcomes.8 This narrative review, therefore, aims to explore recent advances in perioperative neurocognitive recovery, focusing on symptomatology, patient and next of kin experiences, assessments, care interventions and ethical aspects.
Perioperative Neurocognitive Disorder
Neurocognitive decline is the most common complication following otherwise uneventful surgery.9 It is characterized by a reversible decline in cognitive performance compared to baseline levels prior to surgery. The factors contributing to the onset of neurocognitive decline are numerous and complex. Among the various theories presented, the neuroinflammation hypothesis stands out as the most significant. This theory posits that surgery initiates a systemic inflammatory response that compromises the blood-brain barrier, results in neuronal harm, and subsequently causes postoperative neurocognitive decline.10–12 Additionally, the combination of chronic low-oxygen conditions associated with aging and sudden hypoxic events, along with the stress of surgery, can contribute to these issues. Surgery can exacerbate hypoxia due to factors such as reduced blood circulation, inadequate ventilation, fluid accumulation in the lungs, and blood loss.13 Other proposed mechanisms for postoperative cognitive decline include cerebral hypoperfusion, the presence of cerebral microemboli, and hemodynamic changes, particularly following cardiac surgery.14
The risk of postoperative neurocognitive decline is especially pronounced in patients over the age of 65 who have pre-existing cognitive disorders, depression, poor functional status, frailty, and those undergoing a longer duration of surgery.15–19 Previous literature shows that background health conditions or injuries that lead to surgery may impact cognitive performance.20 The prevalence of MCI prior to surgery in older patients is estimated to be between 7%-25%,21 and many older patients are unaware of their cognitive impairment before surgery. Studies show a high prevalence of unrecognized cognitive impairment: 37% in elective non-cardiac surgeries and 50% in emergency surgeries22 and preoperative cognitive impairment is associated with a higher risk of postoperative neurocognitive decline and medical complications for both cardiac23 and non-cardiac surgeries.16,24
Various cognitive domains can be affected, including memory, attention, information processing, and executive functions.25 Following the nomenclature of if present within seven days after surgery, it is defined as postoperative delirium (POD). The incidence of POD after major surgery is between 10% and 60%26–28 and typically develops within a few hours to days and is often reversible. Three subtypes can be distinguished: hyperactive (eg, hypervigilance, agitation, aggression); hypoactive (eg, lethargy, decreased psychomotor performance); and mixed, with symptoms common to both of the above.26,29 The hypoactive and mixed subtypes are the most common but can often remain undiagnosed without use of screening tests.28,30 It is essential to recognize that these conditions should not be viewed as dichotomous. Rather, they exist on an ordinal spectrum of severity, similar to pain, which can be measured using a scale (NRS: 0–10).31 Additionally, symptoms of POD that do not fully meet the diagnostic criteria for delirium are often referred to as subsyndromal delirium, representing a less pronounced or more subtle manifestation compared to full delirium.32 Emergence delirium (ED) is a state of cognitive decline that should be viewed independently from postoperative delirium (POD). ED generally occurs right as a patient starts to regain consciousness from general anesthesia and typically lasts between 5 to 15 minutes.33 Pre-existing undetected cognitive issues prior to the surgery can elevate the risk of ED in older patients, especially those with hearing impairments.34 The occurrence of ED serves as a significant indicator of POD.33,35 If cognitive decline occurs within 30 days after surgery, it is referred to as delayed neurocognitive recovery (dNCR). If it persists up to one year after surgery, it is classified as postoperative neurocognitive disorder (p-NCD).31,36–38 The cognitive changes associated with dNCR/p-NCD can vary from mild to severe, impacting one or more cognitive functions. These changes are often reversible but can last from a few weeks to several years.39 The incidence of dNCR/p-NCD is between 10 and 25%,26 Figure 1.
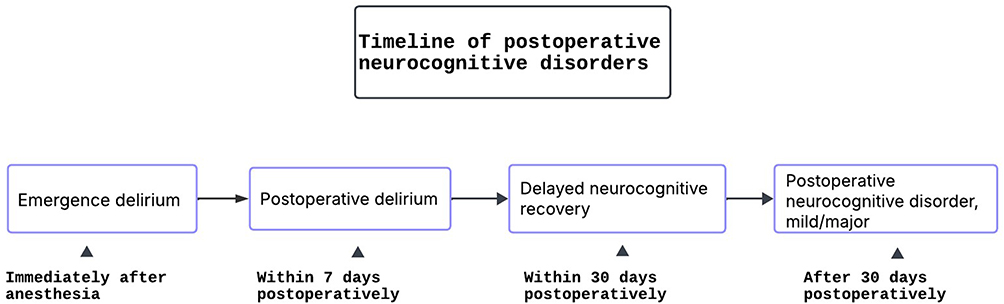 |
Figure 1 Timeline of postoperative neurocognitive disorders. |
Both POD and dNCR/p-NCD negatively impact the quality of life and are linked to a higher risk of morbidity and mortality.8,31 Several studies have investigated the relationship between POD and dNCR/p-NCD, but the results remain conflicting. It is still unclear whether POD constitutes an independent risk factor for delayed or persistent neurocognitive dysfunction dNCR/p-NCD, which would suggest that patients who develop POD in the postoperative phase31 are at increased risk of subsequent cognitive decline. According to Brown et al,40 these patients may exhibit a more pronounced reduction in processing speed one year after surgery, indicating a potential link between acute and long-term neurocognitive outcomes. However, further longitudinal studies are needed to clarify causal relationships and underlying mechanisms.
Patient Experiences and Cognitive Symptoms
Patients who experience POD, describe that the symptoms often fluctuate, and that it can be challenging to stay oriented to the environment and time of day. Being in a delirious state can feel like a strange world of dreams with hallucinations and delusions. These hallucinations can be connected to earlier experiences in life or nightmares, such as being chased and threatened with one’s life, trapped in a cage, trying to cry for help but not being heard or seen, watching a blood pressure cuff turn into a bomb, or seeing the next of kin hurt. Conversely, hallucinations can also be pleasant and amusing. Moreover, the delirious state feels like a parallel world, a crossroad between reality and a surreal state and one can experience feeling completely clear and lucid, despite being in a surreal state.41–44
POD changes the patient’s sense of their surroundings and ability to perform tasks as usual, patients may feel detached and disconnected, which can be distressing44 and worry about the negative impact on their next of kin and healthcare professionals (HCP). Further, patients may feel ashamed and apologize for their behavior.45 Therefore, past delirium becomes a painful memory that could bother patients for a long time42,45 and essential to acknowledge that the patients’ experiences are hallucinations. POD can also have long-term cognitive impacts on the individual, including difficulties with orientation, forgetfulness, reduction in energy, misplacing items, reading challenges, slowed cognitive processing and feelings of sadness.42,44 This makes it challenging to distinguish between cognitive complications caused by POD, symptoms from dNCR /p-NCD, and those related to cognitive ageing or dementia.
Patients with dNCR/p-NCD frequently experience a range of cognitive symptoms, such as problems with intellectual functioning, concentration issues, subjective concerns about cognitive abilities, and memory deficits.31 These issues can significantly affect their recovery and daily lives. Additionally, cognitive difficulties may also be present in patients who have not been diagnosed with dNCR/p-NCD.46,47 Cognitive difficulties are symptoms, signs, and problems that patients experience in the postoperative period, including memory loss, difficulties executing daily tasks, engaging in social activities or housework, decreased focus, and fatigue.5,47 Patients can express this state as “not being the same since the surgery”48,49 and often attributing it to medications. Further, emotional reactions including anger outbursts, sadness and anxiety are related to cognitive difficulties.5,47,49 Earlier research49–51 indicate POD and dNCR/p-NCD are strongly associated with a decrease in independence due to impaired daily activities, and depression, which subsequently reduces autonomy and self-capacity.51
Next of Kin Experiences of Their Family Members’ Cognitive Symptoms
Next of kin experience significant distress when witnessing POD in a family member. This distress is often heightened by observing personality changes in their state, deterioration in medical conditions, and behaviors such as anger outbursts, paranoia and irrationality.52,53 Unexpected emotional and behavioral changes due to POD can lead to increased anxiety and fear among next of kin. They often experience intense, alternating feelings of distress, especially when they have difficulties recognizing their family member, who has become unfamiliar as a result of these changes.54 Next of kin struggle with the uncertainty about whether the delirium could become permanent.53,55 A lack of information about POD in general, and their family members’ specific needs in particular, can lead to individuals creating their own explanations for their family members’ symptoms. Such explanations include blaming sleep deprivation56 or medications, resulting in a feeling of loss of control.54 However, providing accurate information, before the surgery and during an episode, can alleviate some of their distress and help them better manage the situation.56 Guiding next of kin on how to best support the patient is crucial in easing their emotional burden.57 Furthermore, as next of kin plays a key role in assisting HCPs by helping tailor care and identifying new symptoms they need to be kept well-informed.55
Next of kin expect professional support in the discharge process as patients at times are sent home with POD symptoms.56 After discharge, changes in neurocognitive function can affect family dynamics, often leading to grief and frustration for the next of kin.58 But also increased anxiety about the long-term effects and the recurring risk of POD, especially since some patients had already experienced memory deterioration.54 This is particularly challenging for older couples dealing with multimorbidity, which can limit their ability to care for each other.58 However, next of kin experience of their family members’ cognitive symptoms are rarely studied, in particular regarding dNCR/p-NCD.
Assessment of Neurocognitive Function
Understanding the difference between “neuropsychological assessment” and “cognitive screening” is imperative. Although often used interchangeably, these terms refer to two distinct evaluations. Neuropsychological assessments are comprehensive, standardized evaluations conducted by clinicians with training in neuropsychology, considering clinical, demographic, and medical factors. In contrast, cognitive screening tests focus on selected neurocognitive domains and use pre-specified cut-off scores. While these tests do not replace neuropsychological assessments, they are valuable in busy clinical settings for identifying at-risk patients.59,60
Preoperative Assessment and Screening of Neurocognitive Function
An ideal preoperative cognitive screening tool should take ≤5 min to conduct, have high sensitivity and specificity, and be validated in the preoperative geriatric population. Examples of such screening tools are Rapid Cognitive Screening (RCS), Six-Item Screener (SIS) and Mini-Cog61 (Table 1). Traditionally, the Mini-Mental State Examination (MMSE)62 has been used as the standard screening tool for dementia. However, it cannot fully capture cognitive deficits observed in MCI for all populations and is limited by a ceiling effect.62–66 A more sensitive test for detecting cognitive impairment is the Montreal Cognitive Assessment (MoCA)67,68 (Table 1). However, the level of education can affect the results from both MMSE and MoCA as well as age, emotional status, and gender.69
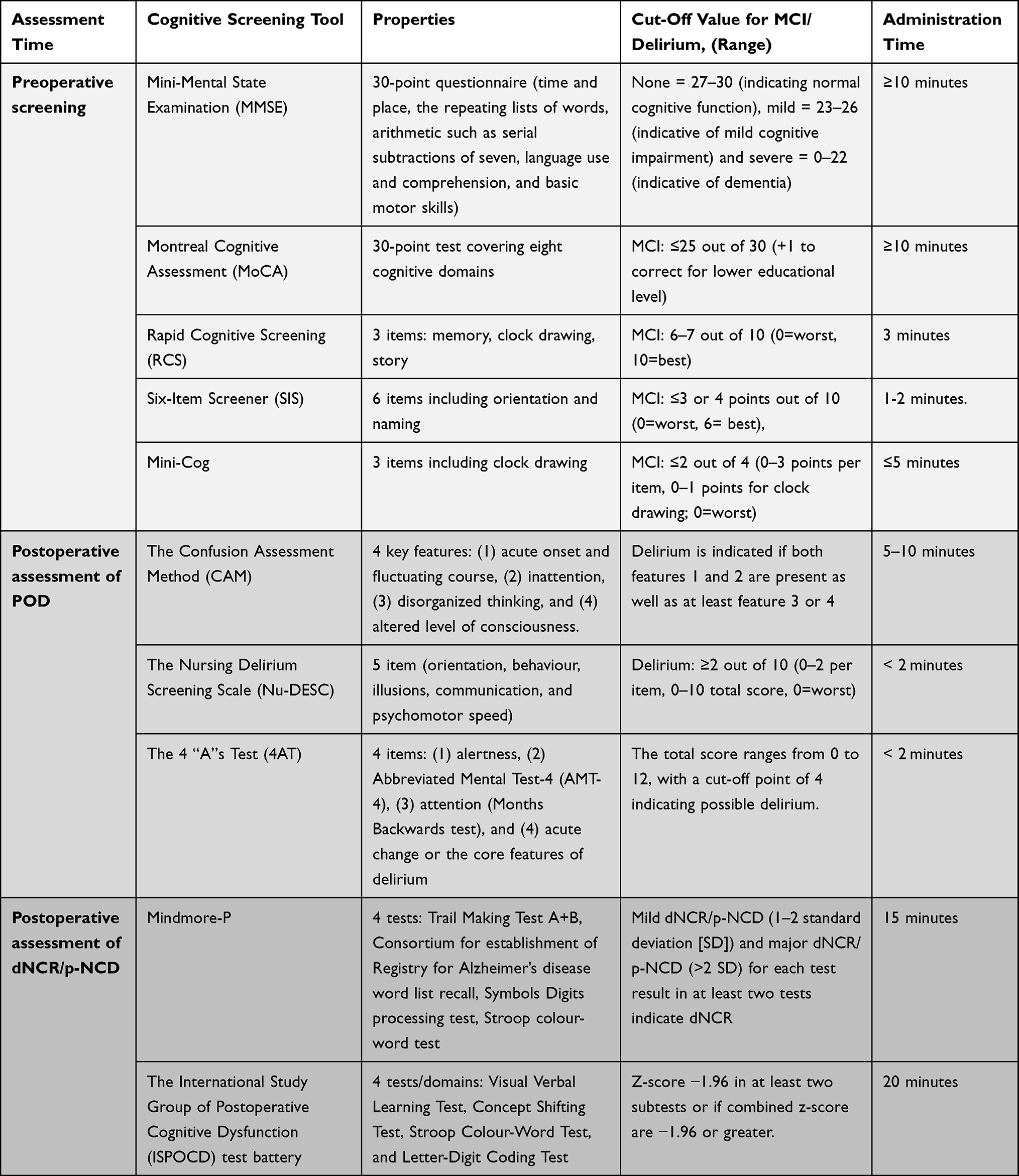 |
Table 1 Example of Cognitive Screening Tools and and Their Characteristics for Assessing Cognitive Decline Before and After Surgery |
The best time to perform a baseline assessment is 1–2 weeks before surgery, at the preoperative visit.20,70 However, it is important to know that cut-off scores used in cognitive screening can limit outcome analyses as cut-off scores do not inherently consider the patient’s cognitive strengths and weaknesses. Therefore, it is encouraged to integrate screening tools with interdisciplinary team engagement and consultation.59
Postoperative Assessment of POD
Delirium diagnosis according to the DSM requires a comprehensive assessment of several complex and, at times, subjective criteria (eg, consciousness, attention, cognition, and temporal course). Many POD assessment tools—such as the Confusion Assessment Method (CAM), the 4AT, or the Nursing Delirium screening scale (Nu-DESC)—are designed to rapidly screen for or identify delirium, rather than to replace a full diagnostic evaluation based on DSM criteria. Yet, early detection is crucial to treating it effectively. Routine screening is recommended by several guidelines for clinical practice and is emphasized to be more important than the actual diagnosis for POD care.2,17,31,60,71 Nurses play a pivotal role in the early detection of postoperative delirium due to their continuous, round-the-clock monitoring and clinical assessment of patients throughout the perioperative period. Therefore, it has been emphasised that nurses should have access to a user-friendly screening tool for assessing delirium.42,72–74
The Confusion Assessment Method (CAM) is a commonly used tool for identifying delirium.75 However, routine screenings may not be practical because the use of CAM takes a relatively long time and requires professional training to make an accurate assessment.72,76,77 An easy-to-use clinical tool that requires no specific training for detecting delirium is the 4 “A”s Test (4AT) consisting of four items73,78 (Table 1). Moreover, the Nursing Delirium Screening Scale (Nu-DESC) is an observational tool to detect and monitor delirium79 (Table 1). As with many other delirium screening instruments, Nu-DESC does not require any patient performance, which might be a disadvantage. But due to its short duration of approximately one minute, it can be more readily adaptable in clinical practice.72,73 The Nu-DESC consists of five domains79 in which the fifth domain, “psychomotor retardation,” can be helpful in detecting hypoactive delirium.73 This is a more subtle form of delirium that is easily overlooked.42,73 However, it has been reported that nurses have had difficulty interpreting hypoactive delirium using Nu-DESC, leading to underdiagnosis.41 Additionally, Confusion Assessment Method-Intensive Care Unit (CAM-ICU) and Intensive Care Delirium Screening Checklist (ICDSC) are the most common delirium assessment tools for critically ill intensive care patients in clinical practice.80 Such tools enable the early detection of POD in patients who undergo prolonged mechanical ventilation after surgery.
Postoperative Assessment of dNCR/p-NCD
Neurocognitive tests are required to detect impairment in neurocognitive function. The timing of postoperative assessments is a crucial factor that influences the incidence rates of neurocognitive decline. Research follow-up periods have ranged from one day to five years after surgery.20 In a Statement of Consensus (CS) from 1995, Murkin et al recommend that studies on dNCR /p-NCD have at least one cognitive follow-up assessment postoperatively.81 It is advisable to delay testing for patients experiencing postoperative complications that could lead to fatigue or decreased motivation. However, not having a standardized time-point for measuring postoperative neurocognitive function after surgery can lead to a significant methodological issue. This is because dNCR /p-NCD may be more prevalent in patients who are unable or unwilling to undergo testing at the usual time of discharge.70 The CS recommends using a specific set of tests called the “core battery” to assess cognitive abilities, which include verbal memory, attention, and psychomotor ability.81 However, there has been heterogeneity in the methodology used to study dNCR /p-NCD and a large variety of diagnostic rules since the publication of the 1995 Consensus Statement.82 When conducting neurocognitive assessments, balancing the desire to evaluate multiple domains with practical considerations is important. For instance, if a patient is about to undergo surgery or has physical limitations, the tests should not be too demanding or lengthy. This is because lengthy assessments can lead to poor performance due to pain or fatigue, or the patient may lose interest. Many commonly used assessment batteries may not be suitable for routine clinical practice due to their resource-intensive and burdensome nature.20
A well-established test in research for the assessment of postoperative neurocognitive function in patients is the neuropsychological test battery developed by the International Study Group of Postoperative Cognitive Dysfunction (ISPOCD).70,82,83 Montreal Cognitive Assessment (MoCA) has also been used in research to assess postoperative cognitive function. ISPOCD and MoCA evaluate different cognitive abilities, such as memory, executive functions, and visuospatial skills70,83,84 (Table 1).
Digital cognitive assessments offer numerous benefits in both remote and healthcare settings. They reduce the workload of healthcare practitioners, simplify repeat testing, and improve cost and time efficiency. Older adults are increasingly using both smartphones and tablets. Adopting this technology for cognitive screening in various settings is feasible, even for older adults with no prior experience with touchscreen technology.85,86 Additionally, they can provide screening to underserved and under-resourced populations since their adaptability to multiple languages helps address healthcare disparities.86,87 Examples of digital self-administered tests comparable to analogue tests such as ISPOCD and MoCA are Mindmore,85 XpressO,88 and Geras Solutions cognitive tests.87 However, according to the Diagnostic and Statistical Manual for Mental Disorders, fifth edition, DSM-5,29 diagnosing dNCR/p-NCD requires subjective cognitive complaints from the patient, informant, or clinician, objective evidence from neurocognitive tests, and changes or decline in instrumental activities of daily living (IADL).36,89
Next of Kin Assessment of dNCR/p-NCD
Assessment of dNCR/p-NCD by a next of kin is considered a more reliable measure than patients’ self-assessment.90 The Cognitive Failures Questionnaire-for-Others (f-CFQ) is an eight-item questionnaire designed for next of kin to assess the frequency of failures in daily living related to memory, attention, action, and perception.91 However, the assessment of next of kin regarding their family members’ cognitive symptoms, particularly in relation to dNCR/p-NCD, is rarely studied, and no research has been found concerning POD.
Care Interventions for POD
Recommended care interventions for POD include preoperative screening and identification of risk factors.2,92 Patients and their next of kin should receive information about the signs, symptoms, risk factors, and outcomes of POD. They should also be guided on how to identify and manage delirium early. A “Getting to know you” form can help collect personal information about the patient, such as the names of their next of kin, assistive devices, profession, hobbies, and preferred terms for activities. This information can assist frontline professionals in assessing and understanding cognitive functions during the postoperative recovery period.2,93 Understanding the causes and treatments of POD and communicating with others can help individuals cope with their experience.42
Postoperative care is crucial for reducing the risk of POD. Strategies to prevent POD include orienting the patient to time and place, maintaining regular communication with them, allowing time for understanding and responses, keeping explanations simple, rephrasing if necessary94 and asking straight and concrete questions.57 However, if the patient experiences POD, it can be challenging for them to articulate their thoughts clearly, leading HCPs to view them as suspicious and paranoid toward the staff. As a result, patients may appear to endure their struggles silently, coming across as introverted and difficult to engage with.57 In such cases, family members can act as mediators to facilitate communication between the nurse and the patient.54 Therefore, allowing a next of kin or caregiver to accompany the patient into the post-anesthesia care unit is beneficial.95,96 Encouraging early mobilization is also advantageous67,74,96,97 however, physical signs that may be perceived as symptoms of hypoactive delirium can include patients appearing extremely fatigued and being difficult to motivate for mobilization.57
Additionally, creating a supportive environment – such as allowing the patient to sit upright, minimizing unnecessary noise, and providing access to glasses and hearing aids – is essential.95 Identifying and treating hypoxia, hypotension, pain, hypothermia, infection, urinary retention, and inability to void are critical as well.2,74,95–97 Having an empathic approach and providing emotional support can also be effective in caring for a patient suffering from POD.92 A critical task is to maintain the patient’s circadian rhythm. To reduce disturbances during sleep, it is important to minimize nighttime inspections and limit noise from the corridor and medical equipment. To help prevent patients from feeling isolated at night, doors can be left open, and delirious patients can be placed in rooms closer to the nursing desk. Furthermore, engaging in daytime activities, such as physiotherapy, has been found to improve sleep quality at night.57
Care Interventions for dNCR/p-NCD
Current evidence does not sufficiently determine whether preoperative cognitive training has a positive impact on dNCR/p-NCD and POD.98–100 Cognitive function training includes programs with structured exercises aimed at improving specific cognitive tasks. These exercises focus on enhancing performance across various cognitive areas, such as memory, attention, and executive function.101 Cognitive training can encompasses a wide range of approaches, including traditional paper-and-pen exercises that promote cognitive engagement, as well as modern digital programs that use interactive platforms to facilitate learning and memory enhancement. Among these, complex cognitive tasks challenge individuals through puzzles and problem-solving activities, while sensorimotor integrative training combines physical movements with cognitive tasks to enhance both mental and motor function. Additionally, advancements in technology have led to the use of virtual reality applications, which create immersive environments for cognitive training, and psychotherapeutic techniques that integrate biosensor feedback to help monitor and improve cognitive performance in real-time. Presently, computer-based cognitive training stands out as the most widely used method.99,100 However, cognitive training can lead to feelings of being overwhelmed, technical difficulties, and constraints related to preoperative timelines, which may increase anxiety and apprehension, especially among older patients.102
Treatment and support should extend beyond the hospital setting and continue after discharge. Patients and their next of kin should not be left to navigate the burdens of perioperative neurocognitive disorders without assistance. Caring for these patients requires a multidisciplinary approach where HCPs collaborate with the patients and their next of kin to develop tailored interventions. Perioperative neurocognitive disorders can significantly impact a patient´s quality of life, affecting their activity of daily living, engaging in social activities, or maintaining independence.44 Therefore, appropriate follow-up care and support for both patients and next of kin are essential.
Ethical Challenges
Providing care for patients with impaired cognitive functions presents several ethical challenges. One major issue is that perioperative neurocognitive disorders can compromise a patient’s ability to make informed healthcare decisions, if the patient suffers from communication and behavioral problems92 particularly if cognitive difficulties are prolonged. The fluctuating nature of POD complicates the assessment of a patient’s decision-making capacity.103 In cases of hyperactive and mixed subtypes of delirium, patients may exhibit disturbing behaviors such as aggression or and violence,103 which can endanger both themselves and the HCPs.92 Additionally, delirious patients may resist treatment, leading HCP to consider using physical or chemical restraints.104 The use of restraints raises ethical dilemmas due to violations of personal integrity and autonomy, as well as potential adverse effects on the patient.105,106
If a patient temporarily or permanently loses their decision-making capacity and refuses treatment, legal grounds for restraint exist only if justified by a severe psychiatric condition. This situation poses challenges for patients with long-term cognitive impairment who do not meet these criteria, increasing the risk of inadequate healthcare under current regulations. Consequently, there is a significant risk that patients with impaired decision-making capacity who refuse treatment will not receive the necessary healthcare.107 Another ethical issue involves resource allocation and prioritization of patients with POD compared to other patients needing care. If POD leads to prolonged hospital stays or increased healthcare needs post-surgery, it can strain healthcare resources.108 Therefore, timely interventions and treatment strategies for this patient group are crucial.
Ethical considerations also arise regarding the balance between the potential benefits of surgery and the risk of cognitive decline, especially in older patients or those with pre-existing cognitive impairment. Additionally, the right to know is a fundamental human right.109 Patients at risk should be thoroughly informed about the risk of postoperative neurocognitive decline before surgery. They should receive individually tailored information that is easy to understand and meaningful.109 Accurately predicting individual risk is challenging, and if patients are not fully informed about the likelihood of cognitive difficulties after surgery, it may lead to inadequate informed consent. Another ethical concern is how to manage the results of screening for POD and dNCR/p-NCD. Simply identifying patients having POD or dNCR/p-NCD without a treatment or support plan is ethically unjustifiable.
Future Perspectives
Perioperative neurocognitive disorders are a significant health issue for older patients, particularly those undergoing major surgery. Delirium is increasingly recognized as a multifactorial and multidisciplinary clinical challenge, particularly in the context of perioperative care and geriatric medicine.110 The effective use of screening instruments to identify neurocognitive complications requires adequate knowledge and, consequently, that HCP receive appropriate training and education. Conducting screening alone is insufficient; results must be accurately interpreted, systematically followed up, and integrated into routine clinical practice. For screening to be meaningful, a structured protocol is essential, whereby results are actively sought, thoroughly documented, and utilized as a basis for ongoing clinical decision-making.41,77,110
While reliable and sensitive instruments are available for preoperative screening and postoperative detection of these complications, clinical routines for assessing neurocognitive function remain inadequate. Barriers to screening-tool implementation are related to HCPs’ limited knowledge of cognitive complication, their competency in using the tools and management of cognitive complications. There are also team collaboration related and organizational barriers to consider. A perioperative neurocognitive recovery is a multifaceted issue, it require an interprofessional team approach to education, identification, and management.111 We recommend that future research focus on strategies to enhance the implementation of evidence-based interventions for detecting neurocognitive complications and supporting patients with cognitive difficulties after surgery. This requires applying theoretical approaches from implementation science to understand the barriers and facilitators to changing practices in the perioperative setting.112
Although guidelines exist for preventing and managing POD, knowledge about the effectiveness and timing of care interventions for dNCR/p-NCD is limited. Unlike POD, which occurs soon after surgery, dNCR/p-NCD often manifests when patients are at home, managing neurocognitive symptoms independently, or with support from their next of kin.112 Given the short duration of inpatient care, patients must oversee their recovery, relying on their self-care capacity to navigate daily life. Effective self-care involves knowledge of symptom management, monitoring, and coping strategies.113 By assessing and discussing these strategies, HCPs can increase patients’ self-efficacy in coping with their conditions.114
To enhance surgical follow-up, we propose a “brain and function check in”. This would involve clinicians gathering information and asking specific questions about cognitive function, and any psychological symptoms that have emerged or changed during the postoperative period. It should also assess the implications of these changes on a functional level, from both patient’s and next of kin’s perspective. If needed, a multidisciplinary team could then provide support, including neurocognitive training, education, home assistance or cognitive behavioral therapy.
Conclusions
The global population is aging, and older adults undergoing surgery are at risk of various postoperative complications. Among these, POD and dNCR/p-NCD are particularly concerning, as they can have severe and potentially life-threatening effects. HCP must provide optimal care by preventing and minimizing perioperative neurocognitive disorders through evidence-based practices and careful monitoring. However, there is a knowledge gap regarding functional status, symptom experiences, and the use of restraints related to postoperative neurocognitive decline. Additionally, we need to better understand the experiences of patients’ next of kin and how to effectively support patients dealing with these disorders.
Addressing ethical challenges requires a multidisciplinary approach that includes HCP, policymakers, patients, and their families. We must collaborate to develop strategies and clinical practices that promote the well-being and rights of older patients experiencing postoperative neurocognitive decline, while considering their individual needs, capacities, and vulnerabilities.
Funding
Strategic area in health care science, SFO-V, Dr no: 2021-01095, 3-1074/2024 and 2-3226/2023. The Swedish Research Council Dr no: 2023-02089.
Disclosure
The authors declare no competing interests.
References
1. Bloom DE. Population 2020. Finance Development. 2020;0057(001):A002.
2. Peden CJ, Miller TR, Deiner SG, Eckenhoff RG, Fleisher LA. Improving perioperative brain health: an expert consensus review of key actions for the perioperative care team. Br J Anaesth. 2021;126(2):423–432. doi:10.1016/j.bja.2020.10.037
3. Fowler AJ, Abbott TEF, Prowle J, Pearse RM. Age of patients undergoing surgery. Br J Surg. 2019;106(8):1012–1018. doi:10.1002/bjs.11148
4. Nilsson U, Gruen R, Myles PS. Postoperative recovery: the importance of the team. Anaesthesia. 2020;75:e158–e64. doi:10.1111/anae.14869
5. Bergman L, Guenna Holmgren A, Nilsson U, Amirpour A, Conte H, Eckerblad J. The bumpy road to recovery: older adults’ experiences during the first year after hip replacement surgery - a longitudinal qualitative study. BMC Geriatr. 2025;25(1):483. doi:10.1186/s12877-025-06155-6
6. Lester PE, Ripley D, Grandelli R, Drew LA, Keegan M, Islam S. Interdisciplinary protocol for surgery in older persons: development and implementation. J Am Med Dir Assoc. 2022;23(4):555–562. doi:10.1016/j.jamda.2022.01.070
7. Marengoni A, Angleman S, Melis R, et al. Aging with multimorbidity: a systematic review of the literature. Ageing Res Rev. 2011;10(4):430–439. doi:10.1016/j.arr.2011.03.003
8. Suraarunsumrit P, Srinonprasert V, Kongmalai T, et al. Outcomes associated with postoperative cognitive dysfunction: a systematic review and meta-analysis. Age Ageing. 2024;53(7). doi:10.1093/ageing/afae160
9. Goldberg TE, Chen C, Wang Y, et al. Association of delirium with long-term cognitive decline: a meta-analysis. JAMA Neurol. 2020;77(11):1373–1381. doi:10.1001/jamaneurol.2020.2273
10. Zhang M, Yin Y. Dual roles of anesthetics in postoperative cognitive dysfunction: regulation of microglial activation through inflammatory signaling pathways. Front Immunol. 2023;14:1102312. doi:10.3389/fimmu.2023.1102312
11. Safavynia SA, Goldstein PA. The role of neuroinflammation in postoperative cognitive dysfunction: moving from hypothesis to treatment. Front Psychiatry. 2018;9:752. doi:10.3389/fpsyt.2018.00752
12. X-x T, Qiu -L-L, Sun J. Research progress on the role of inflammatory mechanisms in the development of postoperative cognitive dysfunction. Biomed Res Int. 2021;2021(1):3883204. doi:10.1155/2021/3883204
13. Snyder B, Simone SM, Giovannetti T, Floyd TF. Cerebral hypoxia: its role in age-related chronic and acute cognitive dysfunction. Anesth Analg. 2021;132(6):1502–1513. doi:10.1213/ANE.0000000000005525
14. Vu T, Smith JA. An update on postoperative cognitive dysfunction following cardiac surgery. Front Psychiatry. 2022;13:884907. doi:10.3389/fpsyt.2022.884907
15. Huang H, Li H, Zhang X, et al. Association of postoperative delirium with cognitive outcomes: a meta-analysis. J Clin Anesth. 2021;75:110496. doi:10.1016/j.jclinane.2021.110496
16. Chen L, Au E, Saripella A, et al. Postoperative outcomes in older surgical patients with preoperative cognitive impairment: a systematic review and meta-analysis. J Clin Anesth. 2022;80:110883. doi:10.1016/j.jclinane.2022.110883
17. Curtis MS, Forman NA, Donovan AL, Whitlock EL. Postoperative delirium: why, what, and how to confront it at your institution. Curr Opin Anaesthesiol. 2020;33(5):668–673. doi:10.1097/ACO.0000000000000907
18. Chen YQ, Qin J. Modified frailty index independently predicts postoperative delirium and delayed neurocognitive recovery after elective total joint arthroplasty. J Arthroplasty. 2021;36(2):449–453. doi:10.1016/j.arth.2020.07.074
19. Cheng H, Ling Y, Li Q, et al. Association between modified frailty index and postoperative delirium in patients after cardiac surgery: a cohort study of 2080 older adults. CNS Neurosci Ther. 2024;30(6):e14762. doi:10.1111/cns.14762
20. Piggin LH, Newman SP. Measuring and monitoring cognition in the postoperative period. Best Pract Res Clin Anaesthesiol. 2020;34(1):e1–e12. doi:10.1016/j.bpa.2018.11.002
21. Petersen RC, Lopez O, Armstrong MJ, et al. Practice guideline update summary: mild cognitive impairment: report of the guideline development, dissemination, and implementation subcommittee of the american academy of neurology. Neurology. 2018;90(3):126–135.
22. Kapoor P, Chen L, Saripella A, et al. Prevalence of preoperative cognitive impairment in older surgical patients.: a systematic review and meta-analysis. J Clin Anesth. 2022;76:110574. doi:10.1016/j.jclinane.2021.110574
23. Au E, Thangathurai G, Saripella A, et al. Postoperative outcomes in elderly patients undergoing cardiac surgery with preoperative cognitive impairment: a systematic review and meta-analysis. Anesth Analg. 2023;136(6):1016–1028. doi:10.1213/ANE.0000000000006346
24. Viramontes O, Luan Erfe BM, Erfe JM, et al. Cognitive impairment and postoperative outcomes in patients undergoing primary total hip arthroplasty: a systematic review. J Clin Anesth. 2019;56:65–76. doi:10.1016/j.jclinane.2019.01.024
25. Evered LA, Silbert BS. Postoperative cognitive dysfunction and noncardiac surgery. Anesth Analg. 2018;127(2):496–505. doi:10.1213/ANE.0000000000003514
26. Migirov A, Chahar P, Maheshwari K. Postoperative delirium and neurocognitive disorders. Curr Opin Crit Care. 2021;27(6):686–693. doi:10.1097/MCC.0000000000000882
27. Rengel KF, Pandharipande PP, Hughes CG. Postoperative delirium. La Presse Médicale. 2018;47(4):e53–e64. doi:10.1016/j.lpm.2018.03.012
28. Swarbrick C, Partridge J. Evidence‐based strategies to reduce the incidence of postoperative delirium: a narrative review. Anaesthesia. 2022;77:92–101. doi:10.1111/anae.15607
29. Association AP. Diagnostic and Statistical Manual of Mental Disorders: DSM-5: American Psychiatric Association. Washington, DC; 2013.
30. Radkowski P, Oniszczuk H, Fadrowska-Szleper M, Onichimowski D. Decoding the neurological sequelae of general anesthesia: a review. Med Sci Monit. 2024;30:e942740.
31. Dilmen OK, Meco BC, Evered LA, Radtke FM. Postoperative neurocognitive disorders: a clinical guide. J Clin Anesth. 2024;92:111320. doi:10.1016/j.jclinane.2023.111320
32. Serafim RB, Soares M, Bozza FA, et al. Outcomes of subsyndromal delirium in ICU: a systematic review and meta-analysis. Crit Care. 2017;21(1):179. doi:10.1186/s13054-017-1765-3
33. Lee S-J, Sung T-Y. Emergence agitation: current knowledge and unresolved questions. Korean J Anesthesiol. 2020;73(6):471–485. doi:10.4097/kja.20097
34. Yu TS, Hung KC. Hearing impairment and postoperative emergence agitation. J Clin Anesth. 2024;94:111394. doi:10.1016/j.jclinane.2024.111394
35. Fields A, Huang J, Schroeder D, Sprung J, Weingarten T. Agitation in adults in the post-anaesthesia care unit after general anaesthesia. Br J Anaesth. 2018;121(5):1052–1058. doi:10.1016/j.bja.2018.07.017
36. Evered L, Silbert B, Knopman DS, et al. Recommendations for the nomenclature of cognitive change associated with anaesthesia and surgery—2018. Anesthesiology. 2018;129:872–879. doi:10.1097/ALN.0000000000002334
37. Kong H, Xu LM, Wang DX. Perioperative neurocognitive disorders: a narrative review focusing on diagnosis, prevention, and treatment. CNS Neurosci Ther. 2022;28(8):1147–1167. doi:10.1111/cns.13873
38. Plas M, Rotteveel E, Izaks GJ, et al. Cognitive decline after major oncological surgery in the elderly. Eur J Cancer. 2017;86:394–402. doi:10.1016/j.ejca.2017.09.024
39. Varpaei HA, Farhadi K, Mohammadi M, Khafaee Pour Khamseh A, Mokhtari T. Postoperative cognitive dysfunction: a concept analysis. Aging Clin Exp Res. 2024;36(1):133. doi:10.1007/s40520-024-02779-7
40. Brown CHT, Probert J, Healy R, et al. Cognitive decline after delirium in patients undergoing cardiac surgery. Anesthesiology. 2018;129(3):406–416. doi:10.1097/ALN.0000000000002253
41. Lingehall HC, Smulter N, Engström KG, Gustafson Y, Olofsson B. Validation of the Swedish version of the nursing delirium screening scale used in patients 70 years and older undergoing cardiac surgery. J Clin Nurs. 2013;22(19–20):2858–2866. doi:10.1111/j.1365-2702.2012.04102.x
42. Falk A, Stenman M, Kåhlin J, Hultgren R, Nymark C. Suffering in silence - Cardiac surgery patients recalling hypoactive delirium a qualitative descriptive study. Intensive Crit Care Nurs. 2023;79:103493. doi:10.1016/j.iccn.2023.103493
43. Instenes I, Gjengedal E, Eide LSP, Kuiper KKJ, Ranhoff AH, Norekvål TM. “Eight days of nightmares … “ - Octogenarian patients’ experiences of postoperative delirium after transcatheter or surgical aortic valve replacement. Heart Lung Circ. 2018;27(2):260–266. doi:10.1016/j.hlc.2017.02.012
44. Cohen CL, Atkins KJ, Evered LA, Silbert BS, Scott DA. Examining subjective psychological experiences of postoperative delirium in older cardiac surgery patients. Anesth Analg. 2023;136(6):1174–1181. doi:10.1213/ANE.0000000000006226
45. Claesson Lingehall H, Smulter N, Olofsson B, Lindahl E. Experiences of undergoing cardiac surgery among older people diagnosed with postoperative delirium: one year follow-up. BMC Nurs. 2015;14:17. doi:10.1186/s12912-015-0069-7
46. Dijkstra JB, Jolles J. Postoperative cognitive dysfunction versus complaints: a discrepancy in long-term findings. Neuropsychol Rev. 2002;12:1–14. doi:10.1023/A:1015404122161
47. Amirpour A, Bergman L, Markovic G, Liander K, Nilsson U, Eckerblad J. Understanding neurocognitive recovery in older adults after total hip arthroplasty-neurocognitive assessment, blood biomarkers and patient experiences: a mixed-methods study. BMJ Open. 2025;15(1):e093872. doi:10.1136/bmjopen-2024-093872
48. Leslie M. The post-op brain. Science. 2017;356(6341):898–900. doi:10.1126/science.356.6341.898
49. Li L, Dohan D, Smith AK, Whitlock EL. “It was a great brain, and I miss it”: lay perspectives on postoperative cognitive dysfunction. Br J Anaesth. 2023;130(5):567–572. doi:10.1016/j.bja.2023.02.003
50. Gearhart SL, Do EM, Owodunni O, Gabre-Kidan AA, Magnuson T. Loss of independence in older patients after operation for colorectal cancer. J Am Coll Surg. 2020;230(4):573–582. doi:10.1016/j.jamcollsurg.2019.12.021
51. Deiner S, Liu X, Lin H-M, et al. Does postoperative cognitive decline result in new disability after surgery? Ann Surg. 2021;274(6):e1108–e1114. doi:10.1097/SLA.0000000000003764
52. Day J, Higgins I. Adult family member experiences during an older loved one’s delirium: a narrative literature review. J Clin Nurs. 2015;24(11–12):1447–1456. doi:10.1111/jocn.12771
53. Schmitt EM, Gallagher J, Albuquerque A, et al. Perspectives on the delirium experience and its burden: common themes among older patients, their family caregivers, and nurses. Gerontologist. 2019;59(2):327–337. doi:10.1093/geront/gnx153
54. Jing D, Weijing S, Yiyu Z. Patients’ and family members’ dyadic experience of post-operative delirium in the intensive care unit: a qualitative study. Nurs Crit Care. 2025;30(2):e13297. doi:10.1111/nicc.13297
55. Meilak C, Biswell E, Willis R, Partridge J, Dhesi J. A qualitative exploration of the views of patients and their relatives regarding interventions to minimize the distress related to postoperative delirium. Int J Geriatr Psychiatry. 2020;35(2):230–249. doi:10.1002/gps.5241
56. Meyer G, Mauch M, Seeger Y, Burckhardt M. Experiences of relatives of patients with delirium due to an acute health event - A systematic review of qualitative studies. Appl Nurs Res. 2023;73:151722. doi:10.1016/j.apnr.2023.151722
57. Hallberg Kristensen A, Nymark C, Stenman M, Falk A. Registered nurses’ experiences of caring for patients with hypoactive delirium after cardiac surgery - A qualitative study. Intensive Crit Care Nurs. 2024;84:103757. doi:10.1016/j.iccn.2024.103757
58. Connors MH, Seeher K, Teixeira-Pinto A, Woodward M, Ames D, Brodaty H. Mild cognitive impairment and caregiver burden: a 3-year-longitudinal study. Am J Geriatr Psychiatry. 2019;27(11):1206–1215. doi:10.1016/j.jagp.2019.05.012
59. Arias F, Wiggins M, Urman RD, et al. Rapid in-person cognitive screening in the preoperative setting: test considerations and recommendations from the Society for Perioperative Assessment and Quality Improvement (SPAQI). J Clin Anesth. 2020;62:109724. doi:10.1016/j.jclinane.2020.109724
60. Block CK, Johnson-Greene D, Pliskin N, Boake C. Discriminating cognitive screening and cognitive testing from neuropsychological assessment: implications for professional practice. Clin Neuropsychol. 2017;31(3):487–500. doi:10.1080/13854046.2016.1267803
61. Tran J, Nimojan T, Saripella A, et al. Rapid cognitive assessment tools for screening of mild cognitive impairment in the preoperative setting: a systematic review and meta-analysis. J Clin Anesth. 2022;78:110682. doi:10.1016/j.jclinane.2022.110682
62. Devenney E, Hodges JR. The mini-mental state examination: pitfalls and limitations. Pract Neurol. 2017;17(1):79–80. doi:10.1136/practneurol-2016-001520
63. van Steenoven I, Aarsland D, Hurtig H, et al. Conversion between mini‐mental state examination, montreal cognitive assessment, and dementia rating scale‐2 scores in Parkinson’s disease. Mov Disord. 2014;29(14):1809–1815. doi:10.1002/mds.26062
64. Kasten M, Bruggemann N, Schmidt A, Klein C. Validity of the MoCA and MMSE in the detection of MCI and dementia in Parkinson disease. Neurology. 2010;75(5):478–479. doi:10.1212/WNL.0b013e3181e7948a
65. Ciesielska N, Sokołowski R, Mazur E, Podhorecka M, Polak-Szabela A, Kędziora-Kornatowska K. Is the Montreal Cognitive Assessment (MoCA) test better suited than the Mini-Mental State Examination (MMSE) in mild cognitive impairment (MCI) detection among people aged over 60? Meta-analysis. Psychiatr Pol. 2016;50(5):1039–1052. doi:10.12740/PP/45368
66. Jia X, Wang Z, Huang F, et al. A comparison of the Mini-Mental State Examination (MMSE) with the Montreal Cognitive Assessment (MoCA) for mild cognitive impairment screening in Chinese middle-aged and older population: a cross-sectional study. BMC Psychiatry. 2021;21(1):485. doi:10.1186/s12888-021-03495-6
67. Sanjanwala RM, Hiebert B, Kent D, Warren S, Grocott H, Arora RC. A quality improvement initiative to reduce postoperative delirium among cardiac surgery patients. Geriatrics. 2021;6(4):111. doi:10.3390/geriatrics6040111
68. Carson N, Leach L, Murphy KJ. A re-examination of Montreal Cognitive Assessment (MoCA) cutoff scores. Int J Geriatr Psychiatry. 2018;33(2):379–388. doi:10.1002/gps.4756
69. Chun CT, Seward K, Patterson A, Melton A, MacDonald-Wicks L. Evaluation of available cognitive tools used to measure mild cognitive decline: a scoping review. Nutrients. 2021;13(11):3974. doi:10.3390/nu13113974
70. Rasmussen LS, Larsen K, Houx P, Skovgaard LT, Hanning CD, Moller JT. The assessment of postoperative cognitive function. Acta Anaesthesiol Scand. 2001;45(3):275–289. doi:10.1034/j.1399-6576.2001.045003275.x
71. Hasan TF, Kelley RE, Cornett EM, Urman RD, Kaye AD. Cognitive impairment assessment and interventions to optimize surgical patient outcomes. Best Pract Res Clin Anaesthesiol. 2020;34(2):225–253. doi:10.1016/j.bpa.2020.05.005
72. Kim S, Choi E, Jung Y, Jang I. Postoperative delirium screening tools for post-anaesthetic adult patients in non-intensive care units: a systematic review and meta-analysis. J Clin Nurs. 2023;32(9–10):1691–1704. doi:10.1111/jocn.16157
73. Jeong E, Park J, Lee J. Diagnostic test accuracy of the 4AT for delirium detection: a systematic review and meta-analysis. Int J Environ Res Public Health. 2020;17(20):7515. doi:10.3390/ijerph17207515
74. Chróinín D N, Chuan A. Post-operative delirium in the patient with hip fracture: the journey from hospital arrival to discharge. Front Med. 2022;9:1080253. doi:10.3389/fmed.2022.1080253
75. Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med. 1990;113(12):941–948. doi:10.7326/0003-4819-113-12-941
76. Olbert M, Eckert S, Mörgeli R, Kruppa J, Spies CD. Validation of 3-minute diagnostic interview for CAM-defined Delirium to detect postoperative delirium in the recovery room: a prospective diagnostic study. Eur J Anaesthesiol. 2019;36(9):683–687. doi:10.1097/EJA.0000000000001048
77. Smulter N, Lingehall HC, Gustafson Y, Olofsson B, Engström KG. Validation of the confusion assessment method in detecting postoperative delirium in cardiac surgery patients. Am J Crit Care. 2015;24(6):480–487. doi:10.4037/ajcc2015551
78. Tieges Z, Maclullich AMJ, Anand A, et al. Diagnostic accuracy of the 4AT for delirium detection in older adults: systematic review and meta-analysis. Age Ageing. 2021;50(3):733–743. doi:10.1093/ageing/afaa224
79. Gaudreau JD, Gagnon P, Harel F, Tremblay A, Roy MA. Fast, systematic, and continuous delirium assessment in hospitalized patients: the nursing delirium screening scale. J Pain Symptom Manage. 2005;29(4):368–375. doi:10.1016/j.jpainsymman.2004.07.009
80. Diao Y, Yu X, Zhang Q, Chen X. The predictive value of confusion assessment method-intensive care unit and intensive care delirium screening checklist for delirium in critically ill patients in the intensive care unit: a systematic review and meta-analysis. Nurs Crit Care. 2024;29(6):1224–1235. doi:10.1111/nicc.13064
81. Murkin JM, Newman SP, Stump DA, Blumenthal JA. Statement of consensus on assessment of neurobehavioral outcomes after cardiac surgery. Ann Thorac Surg. 1995;59(5):1289–1295. doi:10.1016/0003-4975(95)00106-U
82. Borchers F, Spies CD, Feinkohl I, et al. Methodology of measuring postoperative cognitive dysfunction: a systematic review. Br J Anaesth. 2021;126:1119e27. doi:10.1016/j.bja.2021.01.035
83. Moller J, Cluitmans P, Rasmussen L, et al. Long-term postoperative cognitive dysfunction in the elderly: ISPOCD1 study. Lancet. 1998;351(9106):857–861. doi:10.1016/S0140-6736(97)07382-0
84. Vide S, Gambús PL. Tools to screen and measure cognitive impairment after surgery and anesthesia. Presse Med. 2018;47(4 Pt 2):e65–e72. doi:10.1016/j.lpm.2018.03.010
85. Amirpour A, Eckerblad J, Bergman L, Nilsson U. Comparing analog and digital neurocognitive tests with older adults: a study of the ISPOCD battery vs. a digital test battery from mindmore. BMC Geriatr. 2024;24(1):34. doi:10.1186/s12877-023-04648-w
86. Thompson LI, Kunicki ZJ, Emrani S, et al. Remote and in-clinic digital cognitive screening tools outperform the MoCA to distinguish cerebral amyloid status among cognitively healthy older adults. Alzheimer’s Dementia. 2023;15(4):e12500.
87. Bloniecki V, Hagman G, Ryden M, Kivipelto M. Digital screening for cognitive impairment - a proof of concept study. J Prev Alzheimer’s Dis. 2021;8(2):127–134. doi:10.14283/jpad.2021.2
88. Klil-Drori S, Bodenstein KC, Sun S, et al. Montreal Cognitive Assessment (MoCA) XpressO: validation of a digital self-administered cognitive prescreening tool. J Am Geriatr Soc. 2024;72(8):2516–2522. doi:10.1111/jgs.18902
89. Aldecoa C, Bettelli G, Bilotta F, et al. Update of the European society of anaesthesiology and intensive care medicine evidence-based and consensus-based guideline on postoperative delirium in adult patients. Eur J Anaesthesiol. 2024;41(2):81–108. doi:10.1097/EJA.0000000000001876
90. Kastaun S, Gerriets T, Schwarz NP, et al. The relevance of postoperative cognitive decline in daily living: results of a 1-year follow-up. J Cardiothorac Vasc Anesth. 2016;30(2):297–303. doi:10.1053/j.jvca.2015.12.008
91. Broadbent DE, Cooper PF, FitzGerald P, Parkes KR. The cognitive failures questionnaire (CFQ) and its correlates. Br J Clin Psychol. 1982;21(1):1–16. doi:10.1111/j.2044-8260.1982.tb01421.x
92. Azizoğlu H. Experiences of cardiovascular surgery intensive care nurses in the care of patients with postoperative cognitive dysfunction: a qualitative study. Inquiry. 2025;62:469580251332061. doi:10.1177/00469580251332061
93. Deeken F, Sánchez A, Rapp MA, et al. Outcomes of a delirium prevention program in older persons after elective surgery: a stepped-wedge cluster randomized clinical trial. JAMA Surgery. 2022;157(2):e216370–e. doi:10.1001/jamasurg.2021.6370
94. Nilsson U, Bergman L. “Never the same” after surgery: postoperative delirium and early postoperative cognitive decline. J Perianesth Nurs. 2021;36(3):321–322. doi:10.1016/j.jopan.2021.03.005
95. White S, Griffiths R, Baxter M, et al. Guidelines for the peri‐operative care of people with dementia: guidelines from the Association of Anaesthetists. Anaesthesia. 2019;74(3):357–372. doi:10.1111/anae.14530
96. Zhao Y, Quon A, Luke K, Tivis LJ. Impact of nursing interventions on discharge disposition in patients with postoperative delirium. Nursing. 2023;53(11):51–57. doi:10.1097/01.NURSE.0000978892.66327.23
97. Hshieh TT, Yang T, Gartaganis SL, Yue J, Inouye SK. Hospital elder life program: systematic review and meta-analysis of effectiveness. Am J Geriatric Psychiatry. 2018;26(10):1015–1033. doi:10.1016/j.jagp.2018.06.007
98. Lau KT, Chiu LCS, Fong JSY, Chan AKM, Ho KM, Lee A. Preoperative cognitive training for the prevention of postoperative delirium and cognitive dysfunction: a systematic review and meta-analysis. Perioper Med. 2024;13(1):113. doi:10.1186/s13741-024-00471-y
99. Zhang R, Zhu C, Chen S, Tian F, Huang P, Chen Y. Effects of cognitive training on cognitive function in patients after cardiac surgery: a systematic review and meta-analysis of randomized controlled trials. Medicine. 2024;103(44):e40324. doi:10.1097/MD.0000000000040324
100. Zhao L, Guo Y, Zhou X, Mao W, Li L. Preoperative cognitive training improves postoperative cognitive function: a meta-analysis and systematic review of randomized controlled trials. Front Neurol. 2023;14:1293153. doi:10.3389/fneur.2023.1293153
101. Guglietti B, Hobbs D, Collins-Praino LE. Optimizing cognitive training for the treatment of cognitive dysfunction in Parkinson’s disease: current limitations and future directions. Front Aging Neurosci. 2021;13:709484. doi:10.3389/fnagi.2021.709484
102. Ishizawa Y. Preoperative cognitive optimization and postoperative cognitive outcomes: a narrative review. Clin Interv Aging. 2025;20:395–402. doi:10.2147/CIA.S505388
103. van Velthuijsen EL, Zwakhalen SMG, Mulder WJ, Verhey FRJ, Kempen G. Detection and management of hyperactive and hypoactive delirium in older patients during hospitalization: a retrospective cohort study evaluating daily practice. Int J Geriatr Psychiatry. 2018;33(11):1521–1529. doi:10.1002/gps.4690
104. Teece A, Baker J, Smith H. Identifying determinants for the application of physical or chemical restraint in the management of psychomotor agitation on the critical care unit. J Clin Nurs. 2020;29(1–2):5–19. doi:10.1111/jocn.15052
105. Evans D, Wood J, Lambert L. Patient injury and physical restraint devices: a systematic review. J Adv Nurs. 2003;41(3):274–282. doi:10.1046/j.1365-2648.2003.02501.x
106. Joebges S, Mouton-Dorey C, Ricou B, Biller-Andorno N. Coercion in intensive care, an insufficiently explored issue-a scoping review of qualitative narratives of patient’s experiences. J Intensive Care Soc. 2023;24(1):96–103. doi:10.1177/17511437221091051
107. Guenna Holmgren A, von Vogelsang AC, Lindblad A, Juth N. Restraint in somatic healthcare: how should it be regulated? J Med Ethics. 2024. doi:10.1136/jme-2023-109240
108. Leslie DL, Inouye SK. The importance of delirium: economic and societal costs. J Am Geriatr Soc. 2011;59(Suppl 2):S241–3. doi:10.1111/j.1532-5415.2011.03671.x
109. Inkeroinen S, Virtanen H, Stolt M, Leino-Kilpi H. Patients’ right to know: a scoping review. J Clin Nurs. 2023;32(15–16):4311–4324. doi:10.1111/jocn.16603
110. Marcantonio ER. Delirium in hospitalized older adults. N Engl J Med. 2017;377(15):1456–1466. doi:10.1056/NEJMcp1605501
111. Bianchi LA, Harris R, Fitzpatrick JM. Barriers to healthcare professionals recognizing and managing delirium in older adults during a hospital stay: a mixed-methods systematic review. J Adv Nurs. 2024;80(7):2672–2689. doi:10.1111/jan.16018
112. Nilsen P. Making sense of implementation theories, models and frameworks. Implement Sci. 2015;10:53. doi:10.1186/s13012-015-0242-0
113. Riegel B, Jaarsma T, Lee CS, Strömberg A. Integrating symptoms into the middle-range theory of self-care of chronic illness. ANS Advanc Nurs Sci. 2019;42(3):206. doi:10.1097/ANS.0000000000000237
114. Wolf A, Fors A, Ulin K, Thorn J, Swedberg K, Ekman I. An eHealth diary and symptom-tracking tool combined with person-centered care for improving self-efficacy after a diagnosis of acute coronary syndrome: a substudy of a randomized controlled trial. J Med Internet Res. 2016;18(2):e40. doi:10.2196/jmir.4890
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.