Back to Journals » Clinical Optometry » Volume 14
OculoMotor Assessment Tool: Children Compared with Adults
Authors Eichler R, Mivtachi G, Hershkovitz-Azoulay D, Scheiman M, Ben-Eli H ![]()
Received 1 March 2022
Accepted for publication 18 May 2022
Published 27 May 2022 Volume 2022:14 Pages 75—81
DOI https://doi.org/10.2147/OPTO.S364516
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Rachel Eichler,1 Gila Mivtachi,1 Dina Hershkovitz-Azoulay,1 Mitchell Scheiman,2 Hadas Ben-Eli1,3
1Department of Optometry and Vision Science, Hadassah Academic College, Jerusalem, Israel; 2Pennsylvania College of Optometry, Salus University, Elkins Park, PA, USA; 3Department of Ophthalmology, Hadassah Medical Organization and Faculty of Medicine, Hebrew University of Jerusalem, Jerusalem, Israel
Correspondence: Hadas Ben-Eli, Department of Optometry and Vision Science, Hadassah Academic College, Neviim St. 37, Jerusalem, 9101001, Israel, Tel +972-50-4638006, Email [email protected]
Purpose: To provide additional normative data for the OculoMotor Assessment Tool (OMAT) for horizontal and vertical saccades and vergence jumps and to compare the results of children to adults.
Methods: Participants with visual acuity of logMAR ≥ 0.0 (6/6) and Randot stereopsis of at least 250 sec of arc without binocular disorders were recruited. Horizontal and vertical saccades, near point of convergence (NPC), accommodation and vergence jumps were evaluated using the OMAT. Means and standard deviations were reported for all parameters in children and adults.
Results: A total of 52 participants (ages 9– 34, mean age 17.5 ± 7.2 years) participated in this study. Statistically significant differences were found for horizontal and vertical saccades with lower mean results in children, aged 9– 18 (111.5 ± 20.9 and 112.5 ± 22.7, respectively) compared to adults, aged 19– 34 (131.6 ± 23.9 and 126.2 ± 24.2, respectively) (P = 0.002 and 0.04, respectively). The mean of the last 30 seconds of both horizontal and vertical saccades were statistically significantly lower in the children’s group (52.5 ± 10.6 and 52.1 ± 11.3, respectively) compared to the adults (63.2 ± 10.2 and 59.3 ± 13.4, respectively) (P = 0.001 and 0.04, respectively). The normative values for horizontal and vertical saccades were 119.6 ± 23.9 and 118.1 ± 24.1 saccades per minute, respectively. NPC break and recovery were 2.3 ± 2.3cm and 3.0 ± 3.3cm, respectively. The vergence jumps assessment was 79.3 ± 21.19 movements per minute.
Conclusion: Normative values for the OMAT test were found in this study for children and adults. Assessment of endurance found children norms significantly lower for horizontal and vertical saccades compared to adults.
Keywords: OculoMotor Assessment Tool, OMAT, oculomotor abilities, saccadic dysfunction, endurance
Introduction
Recent studies have demonstrated a high frequency of accommodative, vergence and eye movement disorders in children and young adults after concussion.1–4 Master et al1 evaluated 100 adolescents with a mean age of 14.5 years. Overall, 69% had one or more of the following vision diagnoses: accommodative disorders (51%), convergence insufficiency (49%), and saccadic dysfunction (29%). Scheiman et al2 performed a comprehensive oculomotor evaluation on 113 participants 11 to 17 years old, assessed 4 to 12 weeks following a diagnosed concussion. Seventy percent of the participants had at least one oculomotor diagnosis after concussion, with the most common problems being vergence disorders (60%) and accommodative disorders (57%). In a study of soldiers with a mean age of 28.6 years of age, the authors also found a high prevalence of convergence insufficiency (48%), accommodative insufficiency (48%) and eye movement dysfunction (23%).4
Studies also show that the presence of these oculomotor problems can have a negative effect on visual endurance5 and recovery from a concussion.6–8 Yaramothu et al performed a visual endurance test on 8 participants with a medical diagnosis of concussion.5 They found that vergence eye movements significantly degrade over time in concussed subjects compared to healthy controls while participating in the visual endurance test. In a study of 432 patients, Master et al reported that an abnormal accommodative amplitude predicted prolonged concussion recovery in children.7 Both Kawata et al6 and Pearce et al8 found that a receded near point of convergence is associated with prolonged recovery.
Given this high frequency, its negative effect on recovery, and the issue if endurance it is important for eye care and other health-care professionals managing patients after concussion to carefully test for these oculomotor problems with more emphasis on an endurance assessment. While clinicians can evaluate accommodation, vergence, and eye movements using traditional testing procedures, it would be useful to have a single, convenient instrument that would enable clinicians, including non-ophthalmic practitioners, to efficiently test these three areas of oculomotor function. The OculoMotor Assessment Tool (OMAT)9 is a new diagnostic tool that was developed in response to the need for a standardized testing method to accurately assess the near point of convergence, accommodative amplitude, vergence jumps, and saccadic eye movements in patients with persistent concussive symptoms. There are five tests in the OMAT, and this study concentrates on the horizontal and vertical saccades, and the vergence jumps which represent assessments assess endurance and have not been part of traditional optometric care.
At present, the Vestibular Ocular Motor Screening (VOMS)10 is commonly used to assess oculomotor function by clinicians evaluating patients with persistent symptoms post-concussion. The VOMS examination includes smooth pursuits, horizontal and vertical saccades, and near point of convergence (NPC), horizontal vestibular ocular reflex, and visual motion sensitivity. However, there are several shortcomings in the VOMS protocol, including the lack of any testing for accommodative function, and a non-standard protocol for the assessment of the NPC. The VOMS NPC protocol10 states that “the patient focuses on a small target (approximately 14-point font size) at arm’s length and slowly brings it toward the tip of their nose until double vision occurs. The distance in cm between target and the tip of nose is measured and recorded”. This protocol is inconsistent with current standard practice which was used to derive the currently accepted normative data we use in clinical practice.11–13 First, the patient should not hold the target because this may lead to a smaller NPC measurement (due proximal vergence). Second, the target size (14-point font) recommended for the VOMS is considerably larger than current recommendations.11–13 Finally, the measurement should be to the nasion not to the tip of the nose which varies in size from one patient to another. The OMAT instrument and protocol were developed to overcome the limitations of the VOMS protocol.9
Currently, only one study (USA-based) has been published with normative data.9 In Yaramothu’s study, the mean age was 20.4 years with a range of 11 to 34 years of age. Forty two out of 376 participants were children (<18 years old). The purpose of this study is to contribute to the literature by providing additional data from both children and young adults in the Israeli population. Once expected findings have been established in the normal population, the results can be used in the assessment of concussion-related vision disorders.
Methods
Participants
Participants between the ages of 9 and 34 were recruited both from the student population and patients at Hadassah Academic College (HAC) as well as patients from the private practices of the examiners. This study followed the tenets of the Helsinki declaration and received the approval of HAC ethics committee. All participants signed an informed consent form, and a parent or legal guardian of participants under 18 years of age provided informed consent. Data were coded anonymously by serial code numbers.
Inclusion and Exclusion Criteria
Male and female participants of a diverse racial and ethnic background, between the ages 9–34 years old (pediatric participants aged 9–17 years old, adult participants aged 18–34 years old) were required to have corrected visual acuity of ≥ logMAR 0.0 (6/6) in each eye. Randot stereopsis with a minimum of 250 seconds of arc was required. Exclusion criteria included vertical heterophoria of 2 prism diopters or greater, amblyopia, strabismus, or the use of medications affecting visual function and chronic diseases such as diabetes. Pregnant women and cognitively impaired individuals did not participate in this study.
The methods were verbally explained to the participants who all signed a written statement of informed consent prior to their participation (for children - assent and guardian consent). Participants were examined at Hadassah Academic College or at the private practices of the examiners. Each session lasted approximately 15 minutes per participant.
Procedures
In order to ensure participant eligibility, the examiner performed the following tests: visual acuity (using the Snellen chart at 6 meters), stereopsis at near (Randot stereotest), and cover test distance and near. The examiner then performed horizontal and vertical saccades, NPC, vergence jumps and amplitude of accommodation using the OculoMotor Assessment Tool (OMAT) (Gulden Ophthalmics, Elkins Park, PA; product no. 18009) using the same sequence for each participant with a break of one minute between each test. Each participant was examined by one examiner. All examiners were trained to use the identical OMAT procedure protocol training. The OMAT vergence bar was first placed at the participant’s nasion for all procedures and held in that position by the examiner (except the amplitude of accommodation where it was placed at the forehead above the eye being tested). For horizontal saccades, participants were instructed to look right and left between the two “X” targets. For vertical saccades, the participant was instructed to look up and down between the two “X” targets. For both horizontal and vertical saccades examiners used the instructions suggested in a previous publication.9 “This task will be for 1 minute, look back and-forth between the target ‘X’s’ as fast as you can without overshooting or undershooting the ‘X.’ I will let you know when to stop. Start by looking at left/top green ‘X.” The vergence jumps procedure required the participant to look from a vertical line placed at the “A” point (24 cm) to a near vertical line placed at the “F” point (9 cm) keeping the lines single and clear after every jump vergence movement. The following instructions were used. “This task will also be for 1 minute, look back and forth between the two target lines on the sliders as fast as you can, making sure the line is single and clear before the next jump, and to report if the lines were double. I will let you know when to stop. Start by looking at the far line”9. The examiners counted the eye movements and timed one minute by using the OMAT companion iOS and Android smartphone application. The OMAT smartphone application recorded the number of eye movements in the first 30 seconds and after 60 seconds.
The target for the NPC and accommodative amplitude was a vertical line of 20/30 letters. The patient was asked to “look at this row of letters as I bring it closer to your nose. Please let me know if the target splits into two by saying ‘Two’ I will then move the target out. Please let me know as soon as the row returns to one by saying ‘One’.” The break and recovery were recorded. For the amplitude of accommodation measurement, which was displayed in diopters on the bar, the patient was asked to put an eye patch on their left eye (standard black cloth eye patch). The instructions were as follows: “this row of letters will be brought closer towards your open right eye. Please let me know when the letters start to blur and remain blurred. The dioptric value was recorded, and the same procedure was repeated for the left eye. Examiners read the testing procedure instructions verbatim to ensure uniform administration of the tests.
This T-shaped tool is non-invasive and can be used chair-side. The OMAT (Figure 1) has two 25-cm long bars, attached to form a T-shape with magnets that can be rotated and locked. The OMAT is comprised of high-contrast white-on-black targets, as well as red and green “X” targets.
 |
Figure 1 OculoMotor Assessment Tool (OMAT). |
Sample Size
Initial pilot study was performed on 10 children and 10 adults that provided the mean and SD of the horizontal saccades needed to calculate the sample size. The mean horizontal saccades in these participants were 114.1±20.2 saccades per minute and 135.6±29.8 saccades per minute, respectively. Sample size calculation was performed using stat.ubc.ca calculator and a two tailed paired test was performed using an alpha of 0.05 and power of 0.80, hence a sample size of 14 was determined for horizontal saccades comparison.
Statistical Analysis
Means and standard deviations were reported for each continuous parameter. Normal distribution of the data was evaluated based on skewness. The results of one eye were reported for parameters where there was a correlation of 0.97 or higher between eyes. Comparison of the children and adults was done using two samples t-test. Comparison of the first and last 30 sec of the test was done using paired samples t-test. Statistically significant results were considered with α=0.05. Statistical analysis was done by SPSS 25.0 software (Chicago, IL 60606–6307).
Results
Fifty-two participants were enrolled, 28/52 were male (54%), with an age range of 9–34 years (mean 17.5±7.2 years) and 60% of the participants (n = 31) were between the ages of 9–18 years (Table 1).
 |
Table 1 Baseline Parameters Including Mean Age and Standard Deviation of All Participants and According to Gender |
The normative values per minute for horizontal and vertical saccades, the NPC break and recovery, and vergence jumps are listed in Table 2. These represent the expected norms for those parameters when using the OMAT. Statistically significant differences were found between children (9–18 years old) and adults (19–34 years old) in horizontal saccades (P = 0.002) and vertical saccades (P = 0.04). The range for horizontal saccades for children was 77–157 saccades per minute and 107–193 saccades per minute for adults. The range for vertical saccades for children was 74–151 saccades per minute and 86–173 saccades per minute for adults (horizontal: 9–18 = 111.5±20.9, 19–34 = 131.6±23.9). The decrease in the saccades between the first 30 seconds and the last 30 seconds of horizontal and vertical saccades was significant in both children (p < 0.001) and adults (p = 0.001) separately as well as together (p < 0.001). There was no significant difference between children and adults in the NPC break (P = 0.32, 9–18 = 1.8±2.0, 19–34 = 2.4±2.7), recovery (P = 0.78, 9–18 = 2.9±3.2, 19–34 = 3.2±3.5) and vergence jumps (P = 0.26, 9–18 = 82.0±23.4, 19–34 = 75.3±17.2). For vergence jumps, the difference between the first 30 seconds and the last 30 seconds was statistically significant for children (p < 0.001) and the sum of all participants (p < 0.001) but not for adults.
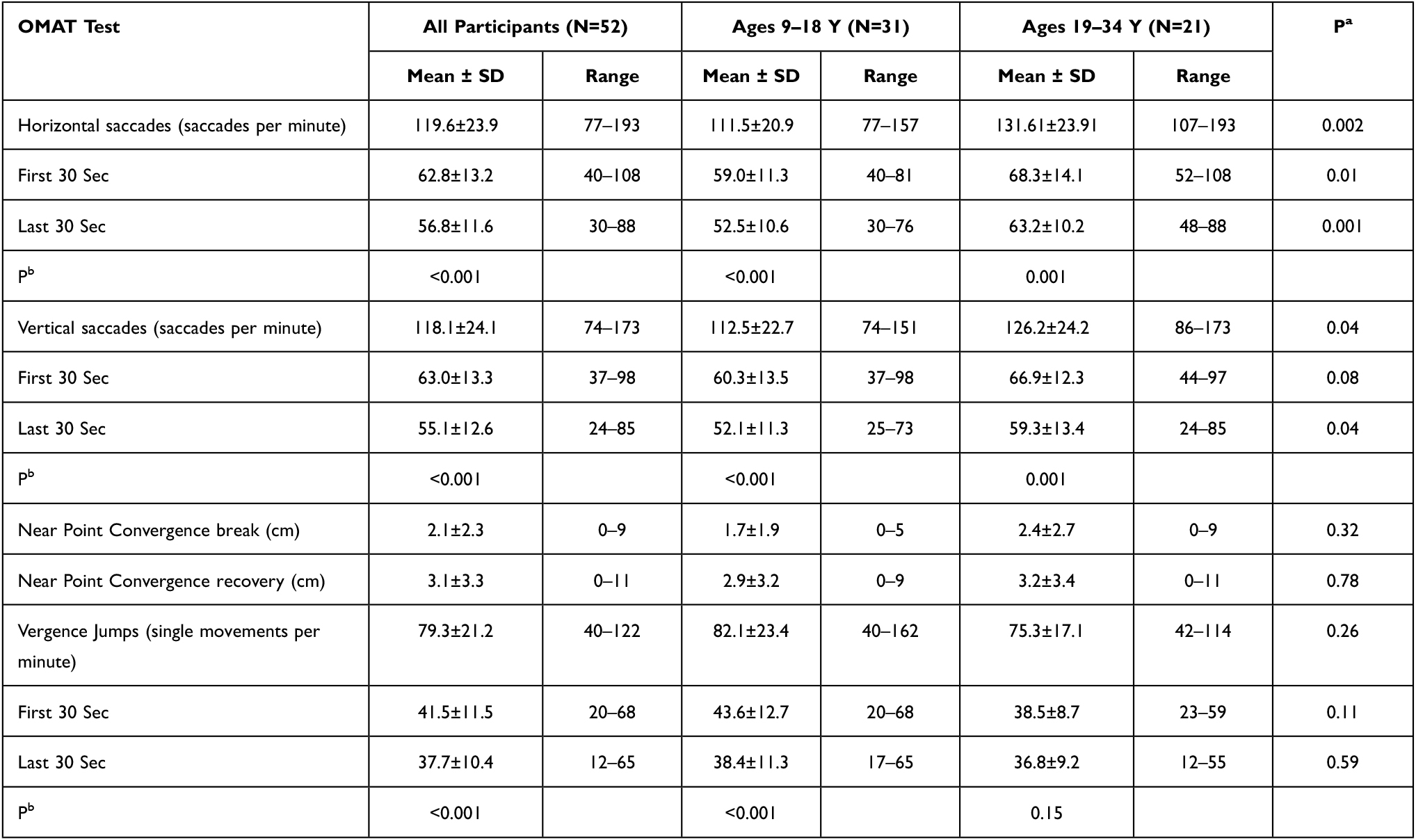 |
Table 2 Distributions of Saccades, NPC and Vergence Jumps for All Participants and According to Specified Age Groups |
Discussion
The results of this study provide additional normative data for horizontal and vertical saccades and vergence jumps using the OMAT. Unlike the recent study of Yaramothu et al,9 we found differences between children and adults and reported the data separately for each group. Statistically significant differences were found between the horizontal and vertical saccades of children and adults. The results of Yaramothu et al for horizontal saccades and vertical saccades were 133.3 ± 27.0 and 130.7 ± 25.6, respectively. One reason for this may be that the means age of children in this study was 12.1 years compared to 15.4 years in the previous study. Our results for adults were very similar for horizontal saccades and vertical saccades 131.6±23.9 and 126.2±24.2, respectively. In agreement with Yaramothu et al, we found the last 30 seconds of the horizontal and vertical saccades to be statistically significantly lower than the first 30 seconds. In the current study, the decrease in the horizontal and vertical saccades in the last 30 seconds was more significant in children. The total result for horizontal and vertical saccades was lower because children comprised 60% of the participants in our study. Yaramothu reported the fusional vergence jumps with the OMAT to be 81.7 ± 21.5. This result was very similar to our study result of 79.32±21.19, demonstrating the unique yet consistent results of the fusional vergence jumps with the OMAT.9 The results of Yaramothu et al for the first 30 seconds vergence jumps were 42.6±11.4 and the last 30 seconds were 39.1±10.7.9 Our results for adults are very similar. In the current study, the vergence jumps significantly decreased in the last 30 seconds in children.
As expected, the reported data correlates well with established norms for the NPC with an accommodative target.11 Our results were close to that of Scheiman et al, who found 2.4±2.1/4.4±3.3 cm in ages 22–37 in the U.S.11 Subtle differences are likely due to different study populations, inclusion criteria, different equipment, and target used (use of a non-accommodative target vs an accommodative testing). When compared with studies that used an accommodative target our results were only slightly lower.
Our study results suggest that the OMAT may be a suitable instrument for measuring the most frequently occurring vision disorders after concussion – binocular vision, accommodative amplitude, and saccadic eye movements. While it certainly can be used by eye care professionals, it also may be of interest as a screening tool for physicians and therapists who manage patients with persistent concussive symptoms. Of course, the OMAT test procedure could also be used in clinical practice to assess accommodative amplitude, near point of convergence, vergence facility and saccadic eye movements in the non-concussed population.
The main strength of this study is the comparison between children and adults regarding the OMAT normative data of horizontal and vertical saccades and vergence jumps. These results may be used to assess these functions in children and adults separately. Secondly, the OMAT tool was just recently published as a clinical tool to be used for concussion-related vision problems, and the current findings provide additional data that can be helpful for clinicians using this device for this purpose. The OMAT device could certainly be used in patients with accommodative and non-strabismic binocular vision disorder in the non-concussed population using these normative data.
Conclusions
The results of this study provide additional information about normative data for horizontal and vertical saccades, and vergence jumps using the OMAT. There were significant differences found between children and adults in the horizontal and vertical saccades, particularly in the last 30 seconds as well as the decrease in vergence jumps in the last 30 seconds for children.
The OMAT may be used as a convenient, all-in-one tool for measuring binocular vision, accommodative amplitude, and saccadic eye movements in the general population. In particular, the OMAT test procedure can be used in patients without concussion, it should be particularly useful for the assessment of these functions in the concussion population because three of the tests assess endurance ability which has been shown to be an important factor after concussion. Future research using a larger sample size of children and adults is recommended.
Abbreviations
OMAT, OculoMotor Assessment Tool; NPC, Near Point of Convergence; VOMS, Vestibular Ocular Motor Screening; VA, Visual Acuity; SOA, Seconds Of Arc; DEC, Decimal; Y, Years; SD, Standard Deviation; cm, Centimeter.
Consent for Publication
All authors confirm that the details of the image can be published, and that the persons providing consent have been shown the article contents to be published.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Master CL, Scheiman M, Gallaway M, et al. Vision diagnoses are common after concussion in adolescents. Clin Pediatr. 2016;55:260–267. doi:10.1177/0009922815594367
2. Scheiman M, Grady MF, Jenewein E, et al. Frequency of oculomotor disorders in adolescents 11 to 17 years of age with concussion, 4 to 12 weeks post injury. Vision Res. 2021;183:73–80. doi:10.1016/j.visres.2020.09.011
3. Raghuram A, Cotter SA, Gowrisankaran S, et al. Postconcussion: receded near point of convergence is not diagnostic of convergence insufficiency. Am J Ophthalmol. 2019;206:235–244. doi:10.1016/j.ajo.2019.04.008
4. Brahm KD, Wilgenburg HM, Kirby J, et al. Visual impairment and dysfunction in combat-injured servicemembers with traumatic brain injury. Optom Vis Sci. 2009;86:817–825. doi:10.1097/OPX.0b013e3181adff2d
5. Yaramothu C, Greenspan LD, Scheiman M, Alvarez TL. Vergence endurance test: a pilot study for a concussion biomarker. J Neurotrauma. 2019;36(14):2200–2212. doi:10.1089/neu.2018.6075
6. Kawata K, Rubin LH, Lee JH, et al. Association of football subconcussive head impacts with ocular near point of convergence. JAMA Ophthalmol. 2016;134:763–769. doi:10.1001/jamaophthalmol.2016.1085
7. Master CL, Master SR, Wiebe DJ, et al. Vision and vestibular system dysfunction predicts prolonged concussion recovery in children. Clin J Sport Med. 2018;28:139–145. doi:10.1097/JSM.0000000000000507
8. Pearce KL, Sufrinko A, Lau BC, et al. Near point of convergence after a sport-related concussion: measurement reliability and relationship to neurocognitive impairment and symptoms. Am J Sports Med. 2015;43:3055–3061. doi:10.1177/0363546515606430
9. Yaramothu C, Morris CJ, d’Antonio-Bertagnolli JV, Alvarez TL. Oculomotor assessment tool test procedure and normative data. Optom Vis Sci. 2021;98:636–643. doi:10.1097/OPX.0000000000001698
10. Mucha A, Collins MW, Elbin RJ, et al. A brief Vestibular/Ocular Motor Screening (Voms) assessment to evaluate concussions: preliminary findings. Am J Sports Med. 2014;42:2479–2486. doi:10.1177/0363546514543775
11. Scheiman M, Gallaway M, Frantz KA, et al. Near point of convergence: test procedure, target selection and expected findings. Optom Vis Sci. 2003;80:214–225. doi:10.1097/00006324-200303000-00011
12. Hayes GJ, Cohen BE, Rouse MW, De Land PN. Normative values for the nearpoint of convergence of elementary schoolchildren. Optom Vis Sci. 1998;75:506–512. doi:10.1097/00006324-199807000-00019
13. Maples WC, Hoenes R. Near point of convergence norms measured in elementary school children. Optom Vis Sci. 2007;84:224–228. doi:10.1097/OPX.0b013e3180339f44
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.