Back to Journals » Clinical Ophthalmology » Volume 19
Ocular Surface Alteration on Corneal Endothelial Decompensation and Descemet’s Membrane Endothelial Keratoplasty
Authors Ma M, Dong X, Wu J, Peng J, Guo R, Yu Y, Xu C, Ouyang C, Huang T
Received 25 November 2024
Accepted for publication 8 April 2025
Published 26 August 2025 Volume 2025:19 Pages 2977—2984
DOI https://doi.org/10.2147/OPTH.S508390
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Minglu Ma,* Xiaojuan Dong,* Jing Wu, Jiayin Peng, Ruilin Guo, Yi Yu, Chenjia Xu, Chen Ouyang, Ting Huang
State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-sen University, Guangdong Provincial Key Laboratory of Ophthalmology and Visual Science, Guangdong Provincial Clinical Research Center for Ocular Diseases, Guangzhou, 510060, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ting Huang, State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-sen University, Guangdong Provincial Key Laboratory of Ophthalmology and Visual Science, Guangdong Provincial Clinical Research Center for Ocular Diseases, Room 1507, Clinical Building, Zhongshan Ophthalmic Center, Sun Yat-sen University, 7 Jinsui Road, Tianhe District, Guangzhou, 510060, People’s Republic of China, Tel +86 13682205425, Fax +86 20 87333566, Email [email protected]
Objective: To explore alterations in tears and ocular surface throughout Descemet’s Membrane Endothelial Keratoplasty (DMEK), thereby offering valuable insights for clinical intervention.
Methods: This study was conducted on 84 patients (84 eyes) with CED and received DMEK who visited the Zhongshan Ophthalmic Center of Sun Yat-sen University from April 2022 to January 2024. All patients were evaluated preoperatively and 1, 3, 6, and 12 months postoperatively, with 31 patients (31 eyes) post-24 months above. This cohort was then compared against a normal control of 21 individuals (21 eyes). Main clinical outcomes included lipid layer thickness (LLT), blink counts and partial blink rate (PBR) measured by Lipiview interferometer, in vivo confocal microscopy (IVCM) was used to detect the density of epithelial wing cells, leukocytes, subbasal dendritic cells (DCs) and endothelial cells.
Results: Compared with normal control, LLT was decreased at 6 months (P = 0.053); total blink counts were significantly higher at 36 months (P < 0.05) after DMEK, while LLT was significantly lower (P < 0.05). Utilizing IVCM, an increased leukocytes density was identified in CED patients, which correlated positively with Log MAR visual acuity (r = 0.261, P = 0.04) and inversely with epithelial wing cells density (r = − 0.319, P = 0.009). Leukocytes density decreased to comparable level at postoperative 3 months (P = 0.11). Subbasal DCs density was still higher at 6 months postoperatively (P < 0.05), while there was no difference at 12 months after DMEK (P > 0.05).
Conclusion: Abnormalities of LLT can occur at different stages after DMEK. Besides, the immune reaction on cornea is still active within 6 months after DMEK.
Plain Language Summary:
Plain Language Summary: What is already known on this topic:
DMEK had earned a reputation for its significantly reduced complication rates and lower incidence of graft rejection when compared to other forms of corneal transplantation.
What this study adds: Following DMEK, abnormalities in the LLT could emerge, and the immune response within the cornea remained active.
How this study might affect research, practice or policy: The study serves as a reminder to clinical doctors to closely monitor for postoperative corneal inflammation within first six months following DMEK, and to be vigilant about potential meibomian gland dysfunction during long-term follow-up periods.
Keywords: Descemet’s membrane endothelial keratoplasty, lipid layer thickness, blinking, corneal inflammatory cells
Introduction
Tear film serves as a critical interface between corneal epithelium and environment, with an average thickness of approximately 6μm.1 Lipid layer of tear film originates from meibomian gland, and possesses a remarkably thin layer of just 100 nm.2 Characterized by its low surface tension, lipid layer facilitates even distribution of tears, offering a uniform refractive medium and impeding tear evaporation.3 The instability of tear film is related to LLT and functionality of the meibomian glands.4 Changes in the diffusion of lipid layer and localized thinning attributable to meibomian gland disorders can precipitate tear film instability.2 In addition, quality of tear film is a determinant of PBR, with spontaneous blinking engaging in intricate interactions with ocular surface.4
CED and endothelial keratoplasty (EK) are recognized as triggers for tear film instability, which in turn can induce alterations in homeostatic balance and structural integrity of ocular surface, which might cause corneal inflammation.5 The development of IVCM has facilitated the detailed examination of ocular surface,6 encompassing a comprehensive view of cellular and neural components. Beyond endothelium, stromal and endothelium, there is an important group of cells known as antigen-presenting cells (APCs), including dendritic cells (DCs) and macrophages, which play a crucial role in corneal immune response.7,8 DCs, typically found at a depth of 35–60μm within corneal epithelium, serve as sentinels for environmental changes and professional APCs.9 IVCM has revealed the coexistence of DCs and leukocytes under certain immune-mediated inflammatory conditions.10 However, current research predominantly concentrates on the shifts in tear secretion and corneal nerve integrity in penetrating keratoplasty (PK) and deep anterior lamellar keratoplasty (DALK), with little attention given to dynamics of tear secretion and corneal cellular density in CED and DMEK. Therefore, this study focuses on exploring the dynamic changes of ocular surface following DMEK in CED patients, particular emphasis on variations in LLT, blinking, and corneal inflammatory cells, providing a reference for clinical intervention.
Methods
Patient Data
Patient demographics are summarized in Table 1. Inclusion Criteria: Without regard to gender or ethnicity, ages over 18 years old; CED with refractory to medical treatment; first-time recipient of EK; patients with full compliance in follow-up. Exclusion Criteria: Individuals with monocular vision; history of previous corneal surgery; concurrent active ocular inflammation; systemic conditions compromising surgical safety, including uncontrolled cardiac or cerebrovascular disorders and severe systemic infections; uncontrolled systemic connective tissue or rheumatic immune diseases; severe psychiatric conditions, such as anxiety and depression; systemic illnesses like diabetes and thyroid dysfunction; pregnant or lactating women; patients unable to cooperate with surgery and regular follow-up; potential risk of complications after DMEK such as graft detachment, secondary glaucoma, and filamentary keratitis. Data was collected from 84 cases of CED patients underwent DMEK, which 31patients (31 eyes) underwent DMEK 2 years above. All patients visited Zhongshan Ophthalmic Center of Sun Yat-sen University from April 2022 to January 2024, as well as 21 normal individuals (21 eyes). This study was approved by the Ethics Committee of the Zhongshan Ophthalmic Center of Sun Yat-sen University (Approval No: 2022KYPJ145), and all patients provided informed consent and signed informed consent forms. All patients underwent a series of standardized ocular evaluations, including BCVA, Lipiview interferometer, non-contact tonometry, Schirmer I test (without anesthesia), and IVCM. These assessments were meticulously conducted by expert investigators H.T. and M.ML. both before and after DMEK. Clinical outcomes included BCVA, intraocular pressure, SIT; LLT, PBR measured by Lipiview interferometer. IVCM was used to scan cornea and calculated density of epithelial wing cells, leukocytes, subbasal dendritic cells (DCs) and endothelial cells (Figure 1). Besides, patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
 |
Table 1 Baseline Characteristics of Patients |
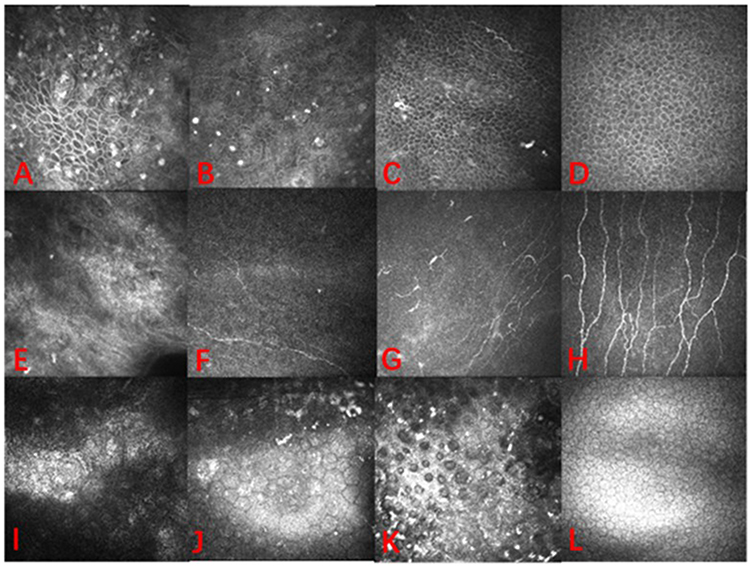 |
Figure 1 IVCM images of epithelium layer, subbasal layer, and endothelium in patients with different types of CED (virus subgroup: (A, E and I) intraocular surgery subgroup: (B, F and J) endothelial dystrophy subgroup: (C, G and K) normal control group: (D, H and L)). Leukocytes are defined as high-reflectivity cells located within wing and basal epithelial cell layers, characterized by absence of dendritic structures and diameter of 12–15μm. |
Surgical Technique
DMEK was performed by the same ophthalmic expert. The donor scleral corneal tissue was stored in EUSOL-C corneal storage solution (Alchimia, Padova, Italy) at 4°C. If there were complications such as cataract, anterior/posterior synechia of the iris, surgery was completed as needed, such as phacoemulsification, intraocular lens implantation, and iridotomy. DMEK referred to the described technique of Melles,11 where the graft was pre-stripped with a diameter of 7.50 to 8.0 mm and stained with trypan blue (Vision blue, D.O.R.C., Zuidland, the Netherlands). Peripheral iridotomy was performed at 6 o’clock of scleral limbus. Triple-folded graft was inserted into anterior chamber through a custom-made syringe (E.Janach S.r.I., Como, Italy), and graft was unfolded. Anterior chamber was filled with filtered sterilized air or inert gas (16% C3F8).
Postoperative Medication
Tacrolimus, three times a day, for 36 months; prednisolone acetate ophthalmic solution, four times a day for the first postoperative month; twice a day for the second postoperative month; once a day for the third postoperative month; fluorometholone 0.02% ophthalmic solution, four times a day for the fourth to twelfth postoperative months, once a day for the thirteenth to twenty-fourth postoperative months; artificial tears: four times a day, for 36 months.
Data Analysis
All data were collected using Microsoft Excel and imported into IBM SPSS Statistics 26 (SPSS.NY.USA). The Shapiro–Wilk test (S-W test) was used to test the normality of continuous variables. Data that met the normal distribution were represented as mean ± standard deviation ( ), while continuous data that did not meet the normal distribution were represented as median (interquartile range). Categorical variable data were represented by absolute numbers and relative frequency (p). For data that met the normal distribution, Student’s t-test was used to analyze the statistical differences between two groups, and data that did not meet the normal distribution were analyzed using the Wilcoxon Mann–Whitney rank-sum test. A P-value less than 0.05 was considered to indicate a statistically significant difference.
), while continuous data that did not meet the normal distribution were represented as median (interquartile range). Categorical variable data were represented by absolute numbers and relative frequency (p). For data that met the normal distribution, Student’s t-test was used to analyze the statistical differences between two groups, and data that did not meet the normal distribution were analyzed using the Wilcoxon Mann–Whitney rank-sum test. A P-value less than 0.05 was considered to indicate a statistically significant difference.
Results
This study retrospectively analyzed 84 patients (84 eyes) with CED and received DMEK who visited the Zhongshan Ophthalmic Center of Sun Yat-sen University from April 2022 to January 2024, with 31 patients (31 eyes) of 24 months and above of follow-up, as well as 21 normal individuals (21 eyes). Patients with CED were divided into three subgroups: 11 patients (11 eyes) caused by virus, 51 patients (51 eyes) caused by intraocular surgery, and 22 patients (22 eyes) due to endothelial dystrophy. Foundational demographic is presented in Table 1.
Ocular Surface Changes
LLT decreased at 6 months (P = 0.053) and 36 months (P = 0.016) postoperatively (Figure 2A), while there was no significant change in LLT at 1 month, 3 months, 12 months, and 24 months after DMEK (P > 0.05), comparing to normal control. Besides, the number of complete blinks significantly increased at 36 months after DMEK (P = 0.016, Figure 2B). Moreover, PBR significantly increased at 3 months and 12 months after DMEK (P < 0.05). At 12 months post-DMEK, LLT showed a negative correlation with number of partial blinks (R = −0.465, p = 0.029).
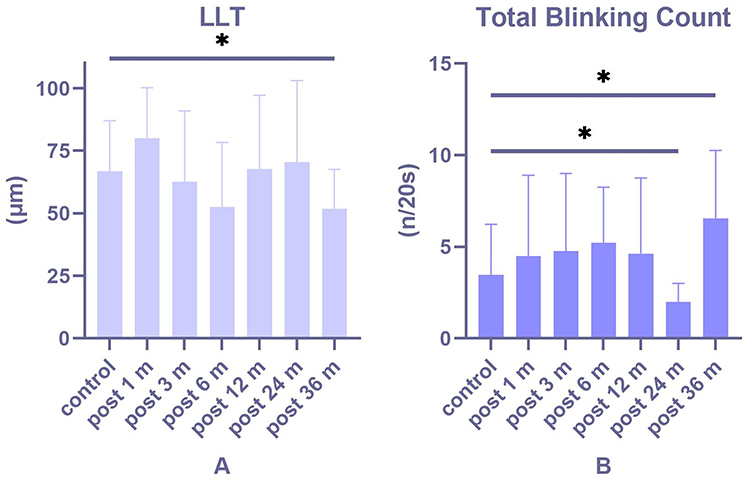 |
Figure 2 Postoperative data versus normal control (A) LTT decreased at 36 months of follow-up comparing to normal control. (B) Total blinking count is instable in post-24 months and above. *p < 0.05. |
Changes in Various Layers of Corneal Cells
In CED patients, comparing to normal control, density of epithelial cells and endothelial cells in cornea decreased in all subgroups (P < 0.05); density of leukocytes in epithelium increased in all subgroups (P ≤ 0.05); DCs density decreased in virus (P = 0.000), while it increased in intraocular surgery and endothelial dystrophy subgroup (P < 0.05).
For postoperative data versus normal control, density of leukocytes increased significantly at 1 month of follow-up (P = 0.000), while there were no significant changes 3 months and beyond (P > 0.05); within 6 months after DMEK, DCs density increased significantly (P < 0.05). And 12 months and above postoperatively, there were no significant changes in DCs density (P > 0.05).
Visual Acuity and Intraocular Pressure
Compared to normal control group, Log MAR visual acuity of patients with CED (P < 0.001) and post-DMEK (P < 0.005) were worse. And there was no significant changes in intraocular pressure.
In all patients with CED, Log MAR visual acuity was negatively correlated with density of epithelial wing cells (Figure 3A). It was positively correlated with leukocytes density (Figure 3B). What is more, density of epithelial wing cells was negatively correlated with leukocytes density (Figure 3C). In initial month following DMEK, corneal endothelial cell loss did not appear to be correlated with donor corneal endothelial cells. However, by 12-month postoperative mark, a significant positive correlation emerges between these two variables (r = 0.552, P = 0.022).
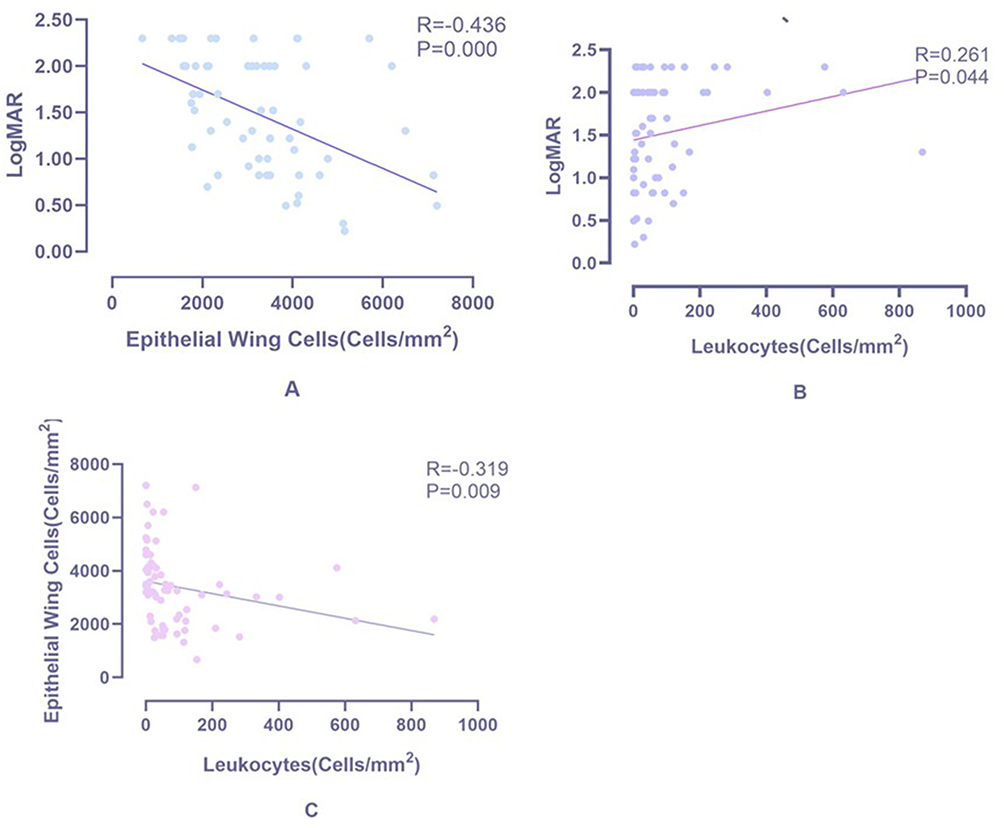 |
Figure 3 Scatter plots among leukocytes, epithelial wing cells and Log MAR visual acuity. (A) display a negative correlation between Log MAR and epithelial wing cells (r = −0.436, p = 0.000), while (B) is positive one between Log MAR and leukocytes (r = 0.261, p = 0.044). Finally, (C) shows when leukocytes increase, there is a decrease in epithelial wing cells (r = −0.319, p = 0.009). |
Discussion
In advanced CED, intricate ocular surface conditions characterized by corneal edema and subepithelial bullae can trigger active inflammation of ocular surface, while tear secretion and lipid layer, as well as complete and partial blinking, have not demonstrated significant deviations from normal. DMEK, which involves excision of compromised corneal endothelium, progressively ameliorate ocular status of CED patients.
The deterioration of dry eye parameters after keratoplasty, such as tear film breakup time, corneal fluorescein staining, SIT, and LLT, has been previously reported.12,13 We conducted a comprehensive assessment of tear secretion, complete and partial blinking frequency, and PBR after DMEK.
Our investigation revealed no significant deviations in tear secretion after DMEK. However, tear secretion was found to be nearing lower threshold of normalcy in 24 months and above post-DMEK. Notably, we identified disturbances in meibomian gland secretion and blinking frequency, both in early and mediate postoperatively phase timeframe.
Changes in meibomian gland function after DMEK are influenced by various factors. The change in LLT in early period of DMEK is similar to cataract surgery.14 First, neural feedback pathway appears to be compromised. Given that meibomian glands are enveloped by a rich network of cholinergic parasympathetic nerve fibers, they are likely integral to this feedback mechanism.15 DMEK inevitably damages corneal nerves, disrupting the feedback pathway of lacrimal functional unit, causing early postoperative neural dysregulation of meibomian glands and leading to abnormal secretion. Subsequently, alterations in blinking frequency have been observed. Moreover, the negative correlation between LLT and frequency of partial blinking at 12 months of follow up was observed, which demonstrated that partial blinking affects spread of lipid layer, increasing excessive evaporation16 and leading to tear film instability.
In medium term after DMEK, abnormalities in meibomian gland secretion may be related to insufficient eyelid hygiene and postoperative medication usage. Insufficient eyelid hygiene after keratoplasty can lead to deterioration of meibomian gland function. A diligent eyelid hygiene regimen can mitigate the presence of lipid by-products and lipophilic bacteria along eyelid margin, consequently diminishing MMP-9 levels and enhancing lipid quality, which can ameliorate meibomian gland dysfunction (MGD).17–19 Patients are typically advised against eyelid cleaning due to the risk of inflicting mechanical trauma on ocular surface after keratoplasty. Insufficient eyelid hygiene, leading to lipid stagnation and gland obstruction, may result in changes in meibomian gland function after DMEK. Additionally, the impact of medication time and preservatives on meibomian gland has been reported,20 and prolonged application of preserved eye drops after DMEK can also lead to abnormal meibomian gland secretion. Therefore, even if complete blinking frequency increased compensatorily after 36 months post-DMEK, LLT remains at a low level. Therefore, for patients after DMEK, it is imperative to initiate comprehensive blink exercises early on, uphold strict eyelid hygiene, and minimize exposure to preservative-laden eye drops to ensure tear film stability and prevent occurrence of MGD.
In three subgroups of patients with CED, there is a significant decrease in epithelial wing cells and endothelial cells density, and inflammatory cells are observed in corneal epithelium. These leukocytes have been previously reported in patients with Sjögren’s syndrome, and their density is higher in patients with higher corneal fluorescein staining scores.21 Due to the lack of in vivo studies, we cannot determine the specific type of leukocytes. However, morphological characteristics of leukocytes suggest that a large proportion of these highly reflective cells may be polymorphonuclear neutrophils (PMNs). Our study found that leukocytes density is positively correlated with Log MAR visual acuity and negatively correlated with epithelial wing cells density. In individuals afflicted with CED, a diminished density of endothelial cells culminates in development of corneal edema and formation of subepithelial bullae. Concurrently, there is a notable upsurge in presence of leukocytes, while a decline is observed in density of corneal epithelial cells. Changes in leukocytes suggest that they are involved in pathophysiology of epithelial changes in CED, and dynamic assessment of leukocytes can serve as an indicator of severity of ocular surface damage in CED. At various stages after DMEK, a significant reduction in leukocytes compared to preoperative levels can be observed, which may be due to removing diseased endothelium and Descemet’s membrane, significantly improving corneal microenvironment. This intervention is instrumental in gradual reversal of ocular surface damage and in mitigating inflammation of ocular surface.
DCs, situated in the corneal subbasal membrane, serve as proficient antigen-presenting entities, pivotal to vigilance of ocular immunity. They are adept at engulfing, processing, and presenting antigens, which can incite immune inflammatory responses on ocular surface.22 Our research dynamically monitors dynamic changes of dendritic cells (DCs) in the context of DMEK. It was observed that in CED, DCs density remains elevated up to 6 months post-surgery, then experiences a marked reduction by 12 months, and sustains a diminished state thereafter. Preoperative corneal inflammation induced by CED maintains DCs at a high level; in early postoperative phase, influenced by DMEK and robust immune reaction of cornea, DCs do not exhibit a significant reduction relative to preoperative levels. It is 6 months above that corneal microenvironment begins to heal and stabilize. These insights underscore the necessity for clinical doctors to closely monitor corneal inflammatory responses and the risk of allograft rejection, particularly within the first 6 months following DMEK.
As a specialized procedure within EK, DMEK is characterized by a notable enhancement in endothelial cells at each subsequent follow-up when compared to baseline preoperatively. The correlation between endothelial cell loss and donor endothelial cell density proves previous research, which experimental studies have shown that donor endothelial cells can promote inflammation and allograft rejection reactions as targets of immune response.23 Furthermore, isolated corneal endothelial transplants are known to elicit potent cytotoxic responses.24 Therefore, donor corneal endothelial cells exert an influence on post-DMEK endothelial cell attrition. Achieving an optimal equilibrium between donor cell density and recipient acceptance is a critical subject that merits further rigorous investigation in EK.
Limitation
There are still many limitations in this study. For instance, research on meibomian glands still requires integration of more parameters to assess changes in morphology and secretion characteristics. In addition, there is a lack of longer-term postoperative observations to elucidate changes in tear fluid and corneal microstructure after DMEK.
Conclusion
Following DMEK, LLT of tear film tends to be abnormally attenuated at various postoperative stages. Despite an observed increase in total blinking frequency during extended follow-up periods, this does not seem to enhance LLT. This reduction in LLT implies that patients may not be able to rely solely on their own regulatory mechanisms to stabilize tear film, necessitating more proactive clinical interventions. Moreover, in early postoperative phase, a heightened density of inflammatory cells within epithelium and subbasal layer is observed when compared to normal conditions. This observation underscores the importance of closely monitoring immune response within first 6 months after DMEK. To mitigate the risk of transplant rejection, it is imperative that clinical management includes a robust pharmaceutical strategy.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of the Zhongshan Ophthalmic Center Review Board. Ethics number:2022KYPJ145. Written informed consent was obtained from all patients after the nature and possible consequences of the study were explained.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The project from the Natural Science Research Foundation of Guangdong Province of China (grant No. 2021A1515010309): design of the study and collection, analysis, and interpretation of data. The project from the Young Scientists Fund of the National Natural Science Foundation of China (grant No. 81900865): write the manuscript and pay for a professional language editing service.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Bai Y, Ngo W, Khanal S, et al. Human precorneal tear film and lipid layer dynamics in meibomian gland dysfunction. Ocular Surf. 2021;21:250–256. doi:10.1016/j.jtos.2021.03.006
2. Pflugfelder SC, Stern ME. Biological functions of tear film. Exp Eye Res. 2020;197:108115. doi:10.1016/j.exer.2020.108115
3. Sabeti S, Kheirkhah A, Yin J, et al. Management of meibomian gland dysfunction: a review. Surv Ophthalmol. 2020;65(2):205–217. doi:10.1016/j.survophthal.2019.08.007
4. Vidal-Rohr M, Craig JP, Davies LN, et al. Classification of dry eye disease subtypes. Contact Lens Anterior Eye. 2024;47(5):102257. doi:10.1016/j.clae.2024.102257
5. Müller LJ, Marfurt CF, Kruse F, et al. Corneal nerves: structure, contents and function. Exp Eye Res. 2003;76(5):521–542. doi:10.1016/s0014-4835(03)00050-2
6. Cruzat A, Qazi Y, Hamrah P. In vivo confocal microscopy of corneal nerves in health and disease. Ocular Surf. 2017;15(1):15–47. doi:10.1016/j.jtos.2016.09.004
7. Mobeen R, Stapleton F, Chao C, et al. Corneal epithelial dendritic cell density in the healthy human cornea: a meta-analysis of in-vivo confocal microscopy data. Ocular Surf. 2019;17(4):753–762. doi:10.1016/j.jtos.2019.07.001
8. Hamrah P, Huq SO, Liu Y, et al. Corneal immunity is mediated by heterogeneous population of antigen-presenting cells. J Leukocyte Biol. 2003;74(2):172–178. doi:10.1189/jlb.1102544
9. Jamali A, Kenyon B, Ortiz G, et al. Plasmacytoid dendritic cells in the eye. Prog Retinal Eye Res. 2021;80:100877. doi:10.1016/j.preteyeres.2020.100877
10. Blautain B, Rabut G, Dupas B, et al. Multimodal approach in dry eye disease combining in vivo confocal microscopy and HLA-DR expression. Trans Vision Sci Technol. 2024;13(8):39. doi:10.1167/tvst.13.8.39
11. Melles GR, Ong TS, Ververs B, et al. Descemet membrane endothelial keratoplasty (DMEK). Cornea. 2006;25(8):987–990. doi:10.1097/01.ico.0000248385.16896.34
12. Kim KY, Chung B, Kim EK, et al. Changes in ocular surface and meibomian gland after penetrating keratoplasty. BMC Ophthalmol. 2021;21(1):85. doi:10.1186/s12886-021-01851-4
13. Meyer JJ, Gokul A, Wang MTM, et al. Alterations in the ocular surface and tear film following keratoplasty. Sci Rep. 2022;12(1):11991. doi:10.1038/s41598-022-16191-6
14. Zhang K, Zhang S, Yu J, et al. Changes of the tear film lipid layer thickness after cataract surgery in patients with diabetes mellitus. Acta ophthalmologica. 2021;99(2):e202–e08. doi:10.1111/aos.14565
15. Girard E, Bernard V, Minic J, et al. Butyrylcholinesterase and the control of synaptic responses in acetylcholinesterase knockout mice. Life Sci. 2007;80(24–25):2380–2385. doi:10.1016/j.lfs.2007.03.011
16. Darwish T, Brahma A, Efron N, et al. Subbasal nerve regeneration after penetrating keratoplasty. Cornea. 2007;26(8):935–940. doi:10.1097/ICO.0b013e3180de493f
17. Green-Church KB, Butovich I, Willcox M, et al. The international workshop on meibomian gland dysfunction: report of the subcommittee on tear film lipids and lipid-protein interactions in health and disease. Invest Ophthalmol Visual Sci. 2011;52(4):1979–1993. doi:10.1167/iovs.10-6997d
18. Romero JM, Biser SA, Perry HD, et al. Conservative treatment of meibomian gland dysfunction. Eye Contact Lens. 2004;30(1):14–19. doi:10.1097/01.Icl.0000095229.01957.89
19. Guillon M, Maissa C, Wong S. Symptomatic relief associated with eyelid hygiene in anterior blepharitis and MGD. Eye Contact Lens. 2012;38(5):306–312. doi:10.1097/ICL.0b013e3182658699
20. Lee SY, Lee K, Park CK, et al. Meibomian gland dropout rate as a method to assess meibomian gland morphologic changes during use of preservative-containing or preservative-free topical prostaglandin analogues. PLoS One. 2019;14(6):e0218886. doi:10.1371/journal.pone.0218886
21. Wolffsohn JS, Recchioni A, Hunt OA, et al. Optimising subjective grading of corneal staining in Sjögren’s syndrome dry eye disease. Ocul Surf. 2024;32:166–172. doi:10.1016/j.jtos.2024.03.005
22. Csorba A, Maneschg OA, Resch MD, et al. Examination of corneal microstructure in the quiescent phase of vernal keratoconjunctivitis using in vivo confocal microscopy. Eur J Ophthalmol. 2023;33(1):196–202. doi:10.1177/11206721221099778
23. Huang T, Lee EJ, Planck SR, et al. The effects of corneal endothelium on graft survival in a murine model of lamellar keratoplasty. Ophthal Res. 2012;47(3):128–134. doi:10.1159/000330271
24. Skelsey ME, Mayhew E, Niederkorn JY. CD25+, interleukin-10-producing CD4+ T cells are required for suppressor cell production and immune privilege in the anterior chamber of the eye. Immunology. 2003;110(1):18–29. doi:10.1046/j.1365-2567.2003.01676.x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.