Back to Journals » Clinical Ophthalmology » Volume 13
Ocular angiostrongyliasis in Thailand: a retrospective analysis over two decades
Authors Sinawat S ![]() , Trisakul T
, Trisakul T ![]() , Choi S, Morley M
, Choi S, Morley M ![]() , Sinawat S, Yospaiboon Y, Yospaiboon Y
, Sinawat S, Yospaiboon Y, Yospaiboon Y ![]()
Received 6 February 2019
Accepted for publication 8 May 2019
Published 18 June 2019 Volume 2019:13 Pages 1027—1031
DOI https://doi.org/10.2147/OPTH.S204380
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Suthasinee Sinawat,1 Thawinee Trisakul,1 Stephanie Choi,2 Michael Morley,2 Supat Sinawat,3 Yosanan Yospaiboon1
1KKU Eye Center, Department of Ophthalmology, Khon Kaen University, Khon Kaen, Thailand; 2Harvard Medical School, Boston, MA, USA; 3Department of Physiology, Khon Kaen University, Khon Kaen, Thailand
Purpose: To elucidate the clinical manifestations, management, and visual outcomes of patients with ocular angiostrongyliasis.
Methods: This was a single-center retrospective study of patients with ocular angiostrongyliasis presenting between 1995 and 2017 at Srinagarind Hospital, Khon Kaen, Thailand. Cases were found based on a search of diagnostic codes. A total of 18 patients were diagnosed through identification of the Angiostrongylus cantonensis parasite within the eye. Medical records and ocular photography were reviewed.
Results: There were 18 cases, with a mean age of 40.7±14.2 years. All patients had a history of raw food ingestion, such as snails. Most of the patients presented with blurred vision: 13 cases (72.22%) had best-corrected visual acuity of 2/60 or worse. Only one living larva was detected in each case. The size of larvae varied widely from 2.6–12.6 mm in length. Larvae were commonly detected in the vitreous cavity. Although multiple treatment modalities were used, including focal laser, surgery, antihelminthic drugs, and steroid treatment, the majority of cases (70.6%) did not have visual improvement.
Conclusion: Focal laser is recommended to eradicate subretinal angiostrongyliasis, while laser treatment prior to surgical removal is recommended to eliminate intracameral and intravitreal angiostrongyliasis. Pulse methylprednisolone therapy may be beneficial in cases of acute optic neuritis. The visual prognosis mainly depends on ocular pathology and parasitic migration pathway.
Keywords: Angiostrongylus canthnensis, intraocular parasite, raw food, ocular angiostrongyliasis
Introduction
Human angiostrongyliasis is primarily characterized by eosinophilic meningitis. Only 1.1% of diagnosed patients develop ocular angiostrongyliasis, which is identified Angiostrongylus cantonensis in any part of the eye.1 Of 43 previous case reports, 20 cases (46.5%) originated from Thailand.2,3 Ocular findings have included lateral rectus palsy, facial palsy, glaucoma, uveitis, disk swelling, disk atrophy, retinal pigment alterations, subretinal tracks, necrotizing retinitis, and exudative retinal detachment.
Cases
This single-center retrospective study was approved by the institutional review board of Khon Kaen University. Patients with ocular angiostrongyliasis presenting between 1995 and 2017 at Srinagarind Hospital were found based on a search of diagnostic codes. A total of 18 patients were diagnosed through clinical identification of the A. cantonensis parasite within the eye. Medical records and ocular photography were reviewed. The study adhered to the tenets of the Declaration of Helsinki.
Results
There were 18 cases (ten males, eight females), with a mean age of 40.72±13.79 years. All patients had a history of raw food ingestion such as snails, fish, and shrimp. Most of the patients (88.89%) presented with a chief complaint of blurred vision. Thirteen cases (72.22%) presented with best-corrected visual acuity of 2/60 or worse. One patient presented with red eye and one with a floater. Three patients had a history of meningitis. The meningitis was active at the time of ocular diagnosis in one patient and 2–3 months earlier in two patients (Table 1). As shown in Figure 1, A. cantonensis was identified in the subtenon (5.56%), anterior chamber (22.22%), subretinal space (33.33%), and vitreous cavity (38.89.3%). Only a single living larva was detected in each patient. The size of larvae varied widely: 2.6–22.6 millimeters (mm) in length. Six from ten extracted parasites were sent to the parasitologist, and all were identified as third-stage larvae varying in size (6–12 mm in approximate length). Female larvae were bigger than male larvae. Although parasitic migration from the anterior chamber to the posterior chamber was detected in one case, three cases (75%) of intracameral angiostrongyliasis had abnormal findings in the posterior segment, such as retinal hemorrhage and retinal pigment epithelium (RPE) alteration. Eosinophilia was found in four of eleven patients (36.36%). Stool examination with concentration technique showed eggs and larvae of parasites in five of nine patients (55.56%) such as Opisthorchis egg, but no Strongylus eggs were found. Two of these five patients also had a history of taking antihelminthic drugs annually (Table 1). Humans can acquire the infection by eating undercooked snails or freshwater animals infected with the parasite, then third-stage larvae or young adult nematodes migrate to the brain or other neural tissue, such as the eye, where the parasites ultimately die.
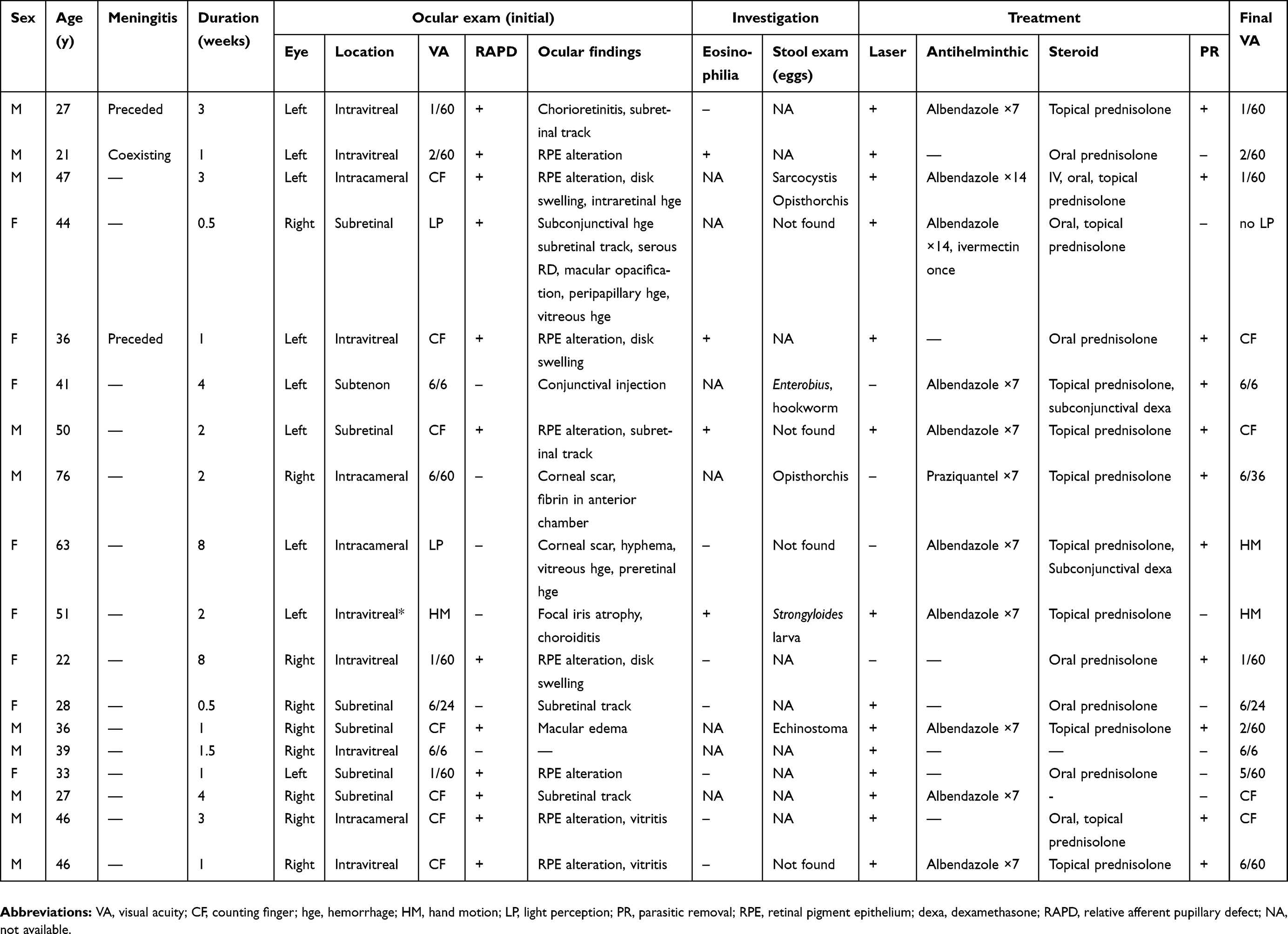 | Table 1 Patient demographic data, ocular findings, management, and visual outcome |
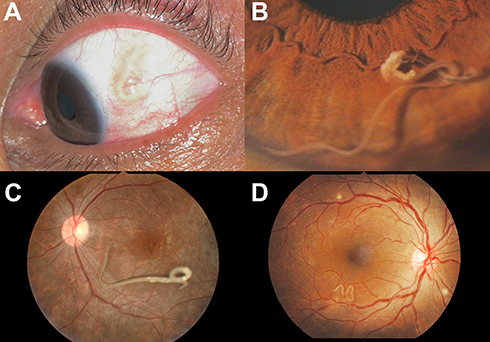 | Figure 1 Angiostrongylus cantonensis larvae in subtenon space (A), aqeous humour (B), vitreous cavity (C), and subretinal space (D). |
Multiple treatment modalities were used, including focal laser (14 cases, 77.78%), surgical removal (ten cases, 55.56%), antihelminthic drugs (eleven cases, 61.11%), and steroid treatment (16 cases, 88.89%), as shown in Table 1. Albendazole 400 mg was prescribed orally twice a day for 7–14 days. Two patients (11.11%) were prescribed antiglaucomatous drugs to control intraocular pressure. Primary laser ablation was typically applied to the pigmented gut, followed by parasitic removal. Surgical removal included subtenon removal, extraction from anterior chamber, pars plana vitrectomy, and subretinal removal through retinotomy. No postoperative complication, eg, proliferative vitreoretinopathy or retinal detachment, was detected. Various routes and types of corticosteroids were administered, depending on the site and severity of intraocular inflammation. The median follow-up was 4 weeks (0–68 weeks). One patient with subretinal angiostrongyliasis was lost to follow-up after laser treatment at first visit. Six patients had visual improvement after treatment, whereas one patient had worsened. Over half the patients were prescribed antihelminthic drugs.
Discussion
Our study is the largest case series of ocular angiostrongyliasis conducted to date. Blurred vision without headache was the most common presenting symptom, which is consistent with previous case reports. In several cases, eosinophilic meningitis was found either to coexist or precede the ocular symptoms. Two patients had a history of eosinophilic meningitis, and one had coexisting ocular and meningitis symptoms.
Laboratory studies, such as complete blood-cell count, cerebrospinal fluid analysis, and parasite-specific serum IgM/IgG antibodies, are unnecessary for the management of ocular angiostrongyliasis without meningitis, since the A. cantonensis parasite can be easily identified by its physical characteristics. Moreover, the parasitologist can distinguish male parasites from female parasites through detection of a bursa in the posterior structures; however, we found both male and female nematodes from the pathological report.4 Previous studies have found the intravitreal cavity to be the most common location of the motile larvae. In our study, the parasite was most often detected within the vitreous. However, the location of the parasite did not seem to affect the severity of the patient’s symptoms or level of visual impairment. Ocular manifestations of angiostrongyliasis are believed to occur as the larvae usually migrateto the orbit by traveling between the optic nerve and the sheath and penetrate the eye by way of the cribriform plate.5 In those eyes with intracameral A. cantonensis, retinal abnormalities are also noted, suggesting that the larvae had entered the anterior chamber from the retina.
Several treatment modalities were attempted to treat ocular angiostrongyliasis in our study, including corticosteroids, focal laser photocoagulation, and surgical removal. Unfortunately, no form or regimen of therapy appeared to improve visual function dramatically. In the majority of cases (66.67%) in our study, there was no visual improvement in best-corrected visual acuity, regardless of treatment type. The most severe case in our study presented with impaired light perception, total macular whitening, and peripapillary hemorrhage resulting from the largest parasite, which may be a young adult nematode (Figure 2). Visual acuity subsequently worsened to no light perception, despite laser treatment and pulse intravenous prednisolone injection being prescribed within 1 week. This is also the most severe case of ocular angiostrongyliasis that has been reported within the literature.
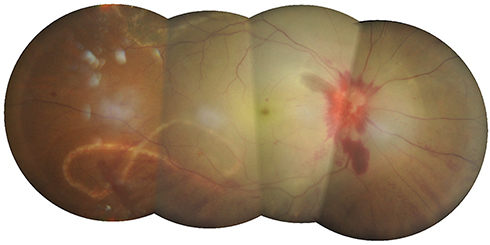 | Figure 2 Large subretinal angiostrongyliasis with severe disk hemorrhage and extensive retinal whitening. |
Migration of larvae suggests the importance of applying focal laser to the pigmented gut of the living A. cantonensis prior to surgical removal, in order to immobilize the parasite. Laser therapy can also be used to guard parasitic invasion into the posterior pole. When performing laser treatment for subretinal parasites, it is critical to avoid laser application to the macular area and optic disk.
Although antihelminthic drugs have no direct benefit for ocular angiostrongyliasis, we generally recommend their use to eradicate other possible parasites due to patients presenting with a history of eating raw freshwater animals. In experimental models, larvicidal drugs have inhibited parasitic migration from the brain. However, antihelminthic drugs should be used with caution in patients with coexisting meningitis. The death of larvae simultaneously in the brain may produce catastrophic effects from toxic substances released by the necrotic parasites.6 Fortunately, no brain reaction related to antihelminthic drugs was found in our patients. Public education campaigns in endemic areas should be considered to increase awareness of food-borne parasites.
Conclusion
Focal laser photocoagulation is recommended to eradicate subretinal angiostrongyliasis, while laser treatment prior to surgical removal is recommended to eliminate intracameral and intravitreal angiostrongyliasis. Pulse methylprednisolone therapy may be beneficial in cases of acute optic neuritis. Antihelminthic drugs should be used with caution in patients with coexisting meningitis. The visual prognosis mainly depends on ocular pathology and parasitic migration pathway. This retrospective study adds important information to previous reports in the literature.
Acknowledgments
We would like to express our gratitude to Dr Wipada Laovirojjanakul for sharing pictures of the subconjunctival parasite. An abstract of this paper was presented as a poster at the 12th Asia-Pacific Vitreo-Retinal Society Congress with interim findings and at the 34th Congress of Asia-Pacific Academy of Ophthalmology.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sawanyawisuth K, Kitthaweesin K, Limpawattana P, et al. Intraocular angiostrongyliasis: clinical findings, treatments and outcomes. Trans R Soc Trop Med Hyg. 2007;101:497–501.
2. Diao Z, Wang J, Qi H, et al. Human ocular angiostrongyliasis: A literature review. Trop Doct. 2011;41:76–78. doi:10.1258/td.2010.100294
3. Sinawat S, Yospaiboon Y, Sinawat S. Subretinal angiostrongyliasis-induced optic neuritis. Clin Ophthalmol. 2013;7:977–979. doi:10.2147/OPTH.S43565
4. Kumar V, Kyprianou I, Keenan JM. Ocular angiostrongyliasis: removal of a live nematode from the anterior chamber. Eye. 2005;19:229–230. doi:10.1038/sj.eye.6701442
5. Sinawat S, Sanguansak T, Angkawinijwong T, et al. Ocular angiostrongyliasis: clinical study of three cases. Eye. 2008;22:1446–1448. doi:10.1038/sj.eye.6702590
6. Cuckler AC, Egerton JR, Alicata JE. Therapeutic effect of thiabendazole on Angiostrongylus cantonensis infections in rats. J Parasitol. 1965;51:392–396. doi:10.2307/3275961
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.