Back to Journals » Clinical Optometry » Volume 18
Occult Retinal Abnormalities Detected by Routine Optical Coherence Tomography in Comprehensive Eye Examination: A Clinic Dataset
Authors Yau Z, Sum RWM, Lam AK ![]()
Received 26 March 2026
Accepted for publication 30 May 2026
Published 9 June 2026 Volume 2026:18 612221
DOI https://doi.org/10.2147/OPTO.S612221
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Chris Lievens
Zoe Yau, Rita WM Sum, Andrew KC Lam
School of Optometry, The Hong Kong Polytechnic University, Hong Kong SAR, People’s Republic of China
Correspondence: Andrew KC Lam, School of Optometry, The Hong Kong Polytechnic University, Hong Kong SAR, People’s Republic of China, Email [email protected]
Purpose: Optical coherence tomography (OCT) is a widely utilized ophthalmic imaging technique commonly used in clinical practice. The axial resolution of modern commercial OCT devices is at the micron level, facilitating the detection of retinal problems that may be unable to be detected in conventional dilated fundus examination (DFE). We evaluated the efficacy of integrating OCT as a routine ophthalmic procedure for identifying occult retinal abnormalities using a university clinical dataset.
Methods: The University Optometry Clinic initiated routine OCT screening as part of comprehensive eye examinations at no additional cost in summer 2025. An ophthalmic assistant captured OCT images of patients aged 40 years or older under natural pupils before the optometrist consultation. A retrospective analysis was conducted based on these OCT images acquired with a concurrent review of electronic medical records.
Results: Overall, 1398 patients underwent routine OCT examinations in two months. Thirty-two patients were excluded because of bilateral suboptimal image quality attributed to undilated pupils. The three most common occult retinal abnormalities not identified by conventional DFE but revealed by OCT were partial posterior vitreous detachment (81 patients, 5.9%), epiretinal membrane, ERM (46 patients, 3.4%), and peripapillary intrachoroidal cavitation (43 patients, 3.1%). Other abnormalities identified by OCT included pigment epithelial detachment, thin retinal nerve fiber layer, focal choroidal excavation (FCE), and idiopathic central serous chorioretinopathy (ICSC). A more serious abnormality included lamellar holes. Patients with ERM (p < 0.001) and lamellar hole (p < 0.001) were older than those without. FCE (p = 0.003) and ICSC (p = 0.009) were more commonly occurred in male.
Conclusion: Some occult retinal abnormalities were identified using OCT alone, but not discernible by conventional DFE. These mild abnormalities were unlikely to have serious consequence which may not affect clinical management. OCT examination might not be regarded as a necessary routine procedure.
Keywords: optical coherence tomography, comprehensive eye examination, posterior vitreous detachment, epiretinal membrane, dilated fundus examination, ophthalmic imaging
Introduction
Optical coherence tomography (OCT) is a widely utilized imaging technique in the ophthalmic field.1,2 It is more commonly applied in neuro-ophthalmology,3,4 and during ophthalmic surgeries.5,6 Ly et al proposed that OCT should be utilized as an adjunctive diagnostic test rather than as a standard procedure.7 Their review covered the usage of OCT and its limitations in age-related macular degeneration, diabetic retinopathy and diabetic macular edema, and glaucoma. Furthermore, OCT technology has been emerging rapidly in recent years. Ahmed et al proposed that OCT examination should be regarded as a standard preoperative procedure prior to cataract surgery.8,9 Although only 14% of clinical undetectable pathology were identified when OCT was employed preoperatively, the excellent safety profile and cost-effectiveness of OCT supported it being a routine preoperative workup. Fouad et al underscored the necessity of conducting OCT before cataract surgery in older adults, especially those with diabetes mellitus.10 Around one-fifth of the eyes had an occult macular pathology on OCT. Paul et al suggested that the regular implementation of OCT in optometric practice could facilitate the earlier identification of glaucoma.11 However, further studies are required to detect the false positive detection rate. Hood et al pointed out problems of reference databases used in commercially available OCT devices.12 Hence, they proposed using OCT scans obtained by optometrists in a clinical setting from healthy eyes to serve as reference database. Another application of OCT is the incorporation of routine OCT in tele-health programme.13
The Optometry Clinic of the School of Optometry at The Hong Kong Polytechnic University is a teaching clinic where eye examinations are mainly conducted by senior optometry students. Staff optometrists provide private eye examinations with higher consultation fees. Additionally, several clinical OCT device models are available. Staff optometrists perform OCT examinations as needed, and patients are required to pay additional examination fees. In summer 2025, the clinic incorporated routine OCT examination using an entry-level OCT device (Topcon Maestro2 3D OCT-1, Topcon, Japan). All patients aged 40 years or older registered with our staff optometrists underwent OCT examinations conducted by ophthalmic assistants. This is regarded as a component of the pre-consultation testing battery.
We believe that qualified optometrists should be able to pick up important retinal abnormalities even without doing OCT. Hence, occult retinal abnormalities identified by OCT might not have significant clinical impact. This study aimed to evaluate the efficacy of integrating OCT as a routine ophthalmic procedure for identifying occult retinal abnormalities that were not discernible by conventional comprehensive eye examination, using a university clinical dataset.
Materials and Methods
Participants
Patients aged of 40 years or older, consulting staff optometrists at the Optometry Clinic of the School of Optometry, The Hong Kong Polytechnic University, during June and July in 2025 underwent routine OCT examinations with natural pupils. All patients provided informed consent for the use of their examination results for teaching and research purposes. This study was approved by the Institute Review Board of The Hong Kong Polytechnic University (HSEARS20250924004) and adhered to the principles of the Declaration of Helsinki.
Study Design
This was a retrospective, single-center study of patient records from our electronic medical records. Upon appointment registration at the reception counter, ophthalmic assistants who received training administered pre-consultation testing battery for every patient. The pre-consultation testing battery comprised auto-refraction, non-contact tonometry, and focimetry for those wearing spectacles. Since retinal pathologies were more common in older people, routine OCT examinations were conducted only in patients aged 40 years or above, using the Topcon Maestro2 model. Imaging was performed using the 3D Wide (H) mode, which captured a 12 mm × 9 mm area encompassing both the macula and the optic disc. The scanning resolution was 512×128 pixels, corresponding to a transverse resolution of 23.4 µm horizontally and 70.3 µm vertically. The axial resolution was 6µm. The scanning speed of the 3D Wide (H) mode was 50,000 scans/s. The results included 128 horizontal B-scan images and circumpapillary retinal nerve fiber layer (RNFL) thickness. Signal strengths were at least 30 or above according to the recommendation of the manufacturer. Following the OCT scan, a fundus photograph was obtained to complement the structural data with a color image of the retina. An automated scanning protocol was employed without the use of mydriatic agents.
All staff optometrists conducted the eye examinations as usual. Best-corrected visual acuity (BCVA) was evaluated using a logMAR chart. Intraocular pressure measurements were performed and anterior ocular health was evaluated. Slit-lamp biomicroscopy was conducted with dilated pupils, unless contraindicated for pupil dilation. During dilated fundus examination (DFE), a 90-D lens was used, and the optic disc, macula, and peripheral retina were scanned. Binocular indirect ophthalmoscopy was conducted with a 20-D lens. At the end of the above examinations, optometrists were allowed to access images acquired by the routine OCT examinations. Any occult retinal abnormalities observed by OCT imaging but no retinal pathology detected in biomicroscopic fundus and binocular indirect ophthalmoscopic examinations were marked. Patients without occult retinal pathologies were set as another group. Staff optometrists arranged follow-up appointments, if necessary, for relevant occult retinal abnormalities identified from the OCT images. An independent optometrist retrieved patient examination records from the electronic medical records.
Statistical Analysis
Descriptive information was gathered regarding the number of eyes with occult retinal abnormalities that were not identified on comprehensive eye examinations. The frequencies of different abnormalities were determined based on the number of patients assessed. Statistical analyses were performed using SPSS (version 27.0, IBM Corp., Armonk, NY, USA). Normality of the data was checked using the Kolmogorov–Smirnov test. Continuous variables were expressed as mean ± standard deviation. The chi-square was used in the analysis of categorical two-group data. Non-parametric test was conducted to evaluate the distribution of variables between groups.
Results
A total of 1398 patients underwent routine OCT examinations before seeing the optometrists. The OCT image quality was poor in 32 patients, and their results were excluded from the analysis. Among the remaining 1366 patients, 215 of them (15.7%) had occult retinal abnormalities identified only by the OCT imaging. Some patients had more than one abnormality. Table 1 summarizes these abnormalities and their frequencies. There was no difference in age between patients with and without occult retinal abnormalities except those patients with epiretinal membrane (ERM) and lamellar hole were older.
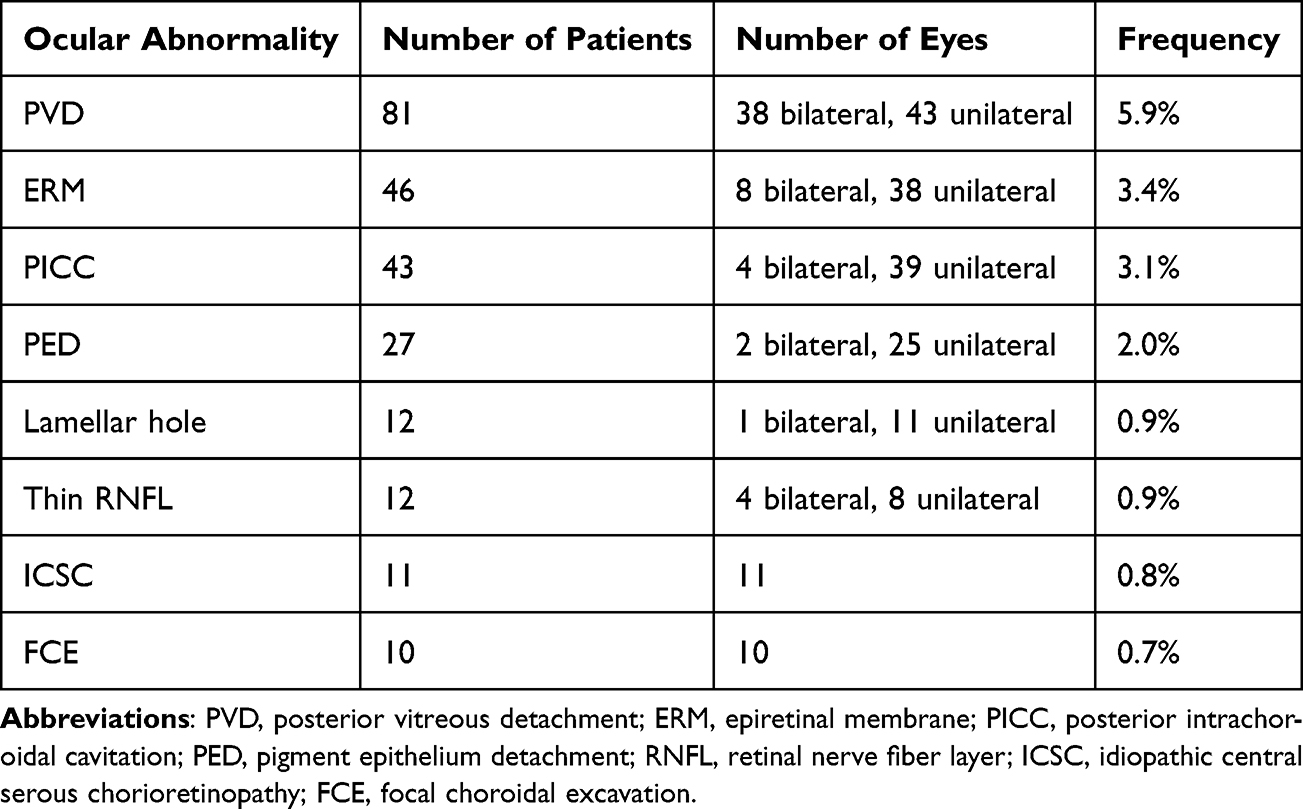 |
Table 1 Common Occult Retinal Abnormalities Identified from OCT in 1366 Patients |
Focal choroidal excavation (FCE) and idiopathic central serous chorioretinopathy (ICSC) tended to be more commonly in male (Table 2).
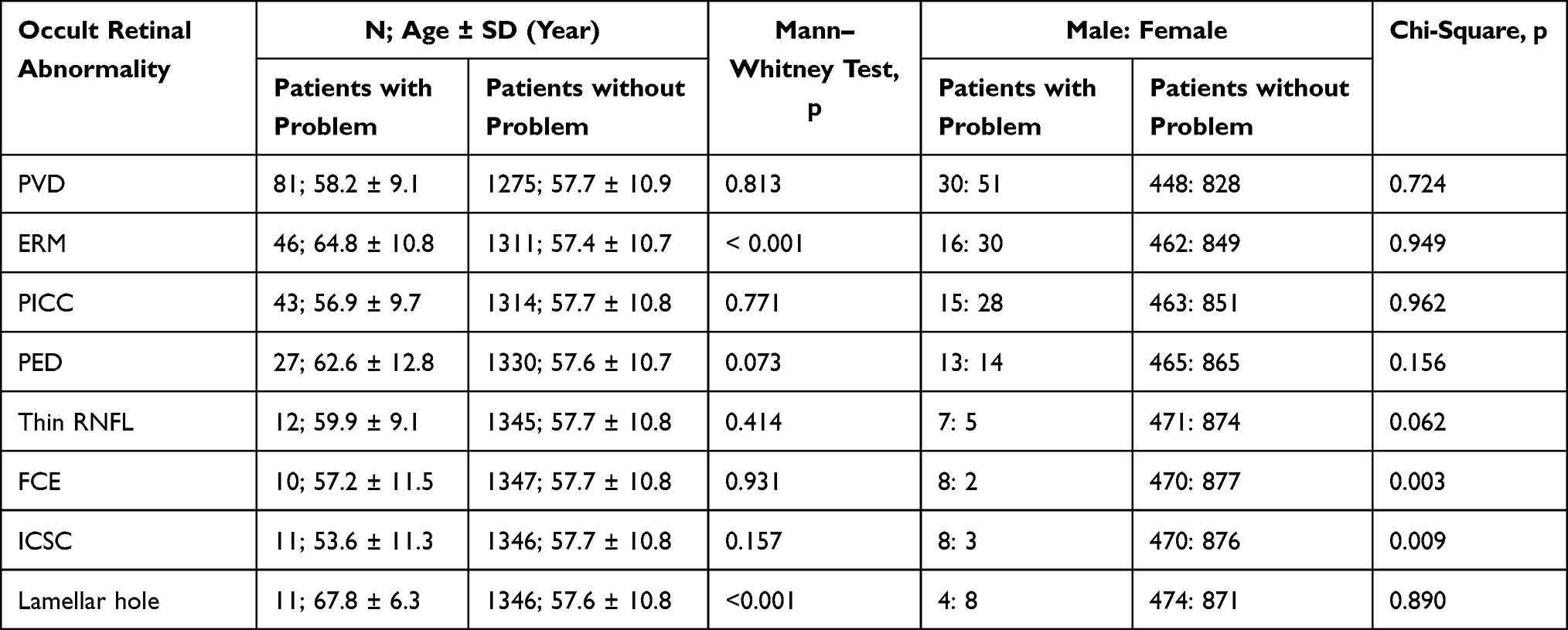 |
Table 2 Age of Patients with and without the Occult Ocular Abnormalities, and Gender Distribution |
Common occult retinal abnormalities found in this study are shown. Figures 1–5 are peripapillary intrachoroidal cavitation (PICC). Figure 6 is retinal pigment epithelium detachment (PED). Figures 7 and 8 are idiopathic central serous chorioretinopathy (ICSC).
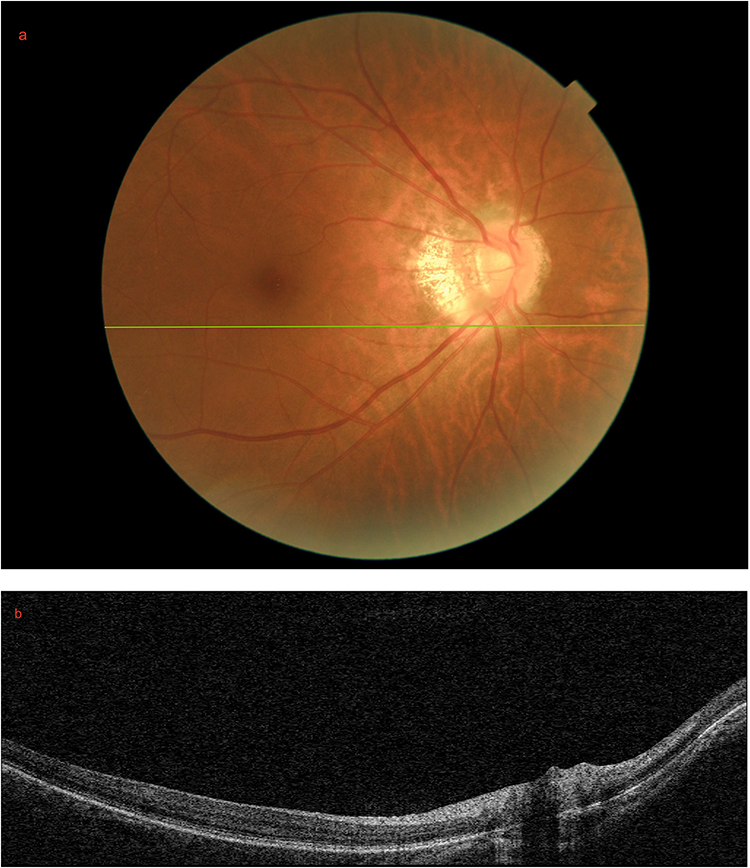 |
Figure 1 A patient with peripapillary intrachoroidal cavity. (a) Fundus photo of a patient with a lesion inferior to the optic disc; (b) B-scan OCT of the green line in (a) showing a peripapillary intrachoroidal cavity. |
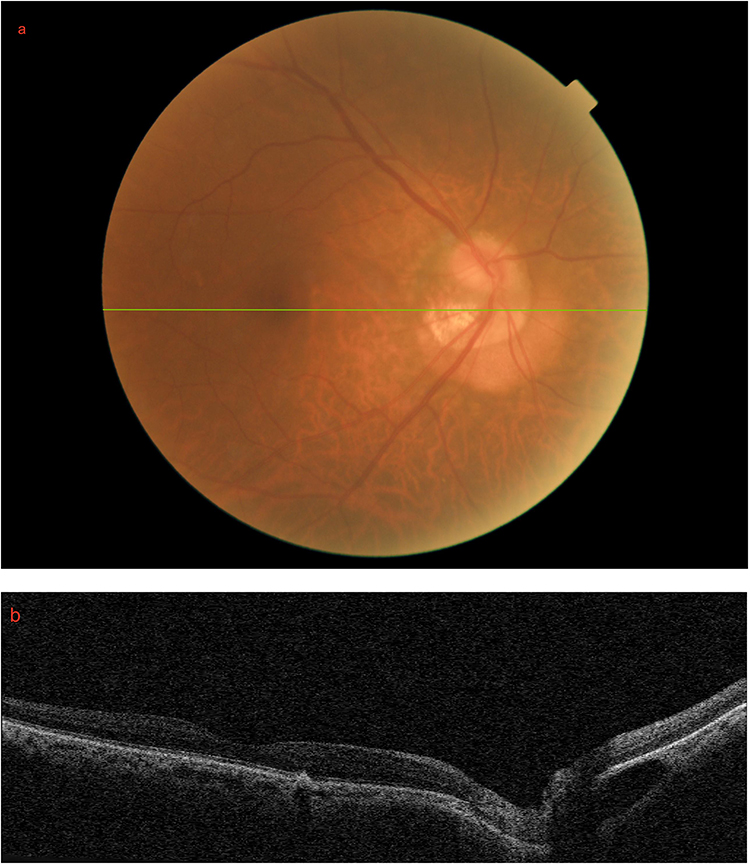 |
Figure 2 A second patient with peripapillary intrachoroidal cavity (a) Fundus photo of a patient with a lesion inferior to the optic disc; (b) B-scan OCT of the green line in (a) showing a peripapillary intrachoroidal cavity inferior to the disc. There is an area of reticular pseudodrusen in the fovea region. |
 |
Figure 3 A third patient with peripapillary intrachoroidal cavity. (a) Fundus photo of a patient with a lesion inferior to the optic disc; (b) B-scan OCT of the green line in (a) showing a peripapillary intrachoroidal cavity inferior to the disc. There is a tiny serous pigment epithelium detachment at the macular region. |
 |
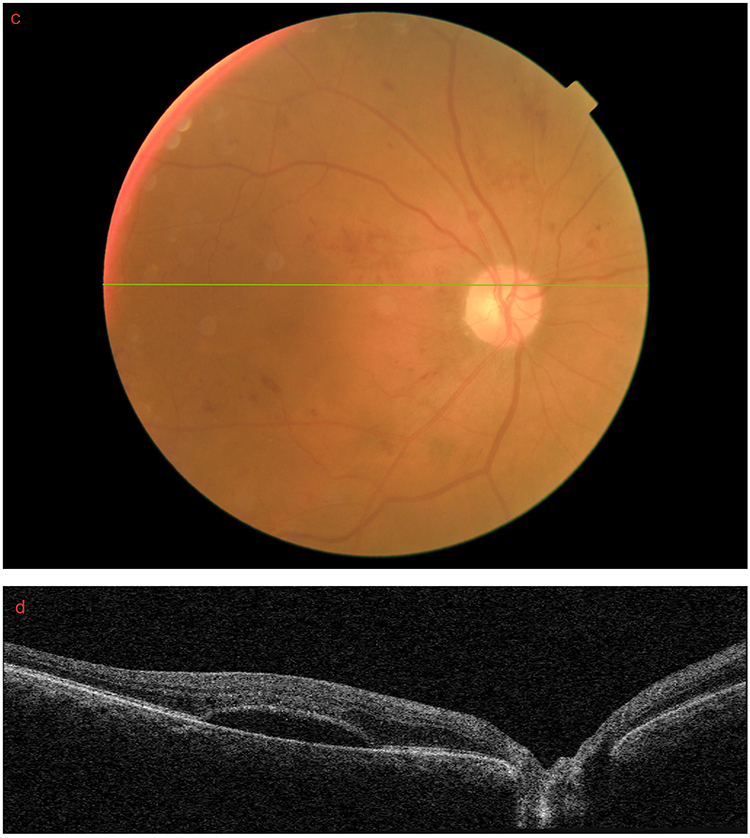
Figure 4 A fourth patient with peripapillary intrachoroidal cavity. (a) Fundus photo of a patient with a lesion at the inferior part of the optic disc; (b) B-scan OCT of the green line in (a) showing a peripapillary intrachoroidal cavity inferior to the disc. |
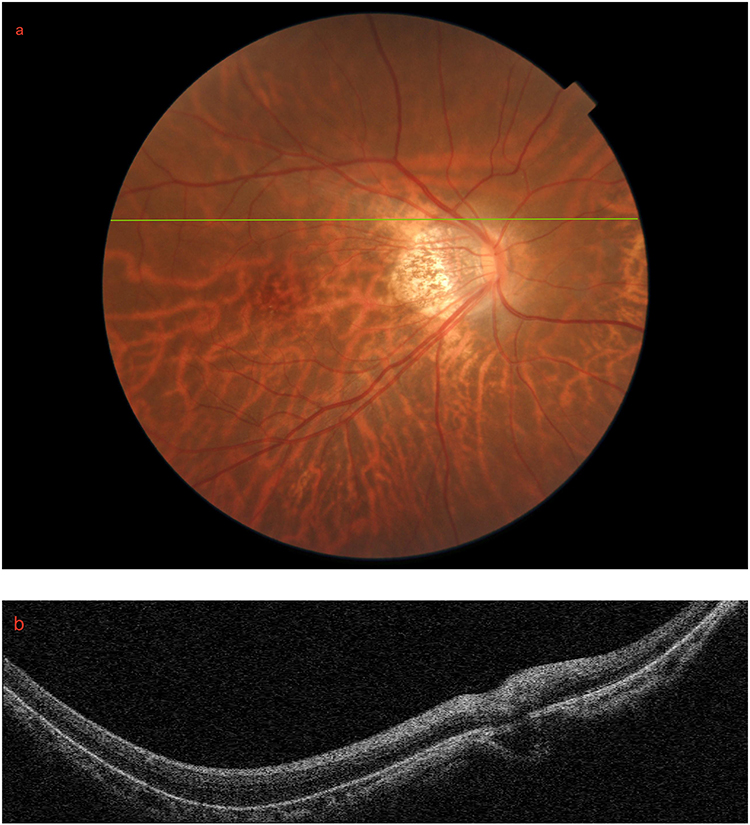 |
Figure 5 A fifth patient with peripapillary intrachoroidal cavity. (a) Fundus photo of a patient with a lesion superior to the optic disc; (b) B-scan OCT of the green line in (a) showing a peripapillary intrachoroidal cavity superior to the disc. |
 |
Figure 6 A patient with retinal pigment epithelium detachment. (a) Fundus photograph of a patient with a lesion at the inferior perimacular region; (b) B-scan OCT of the green line in (a) showing a serous pigment epithelium detachment. |
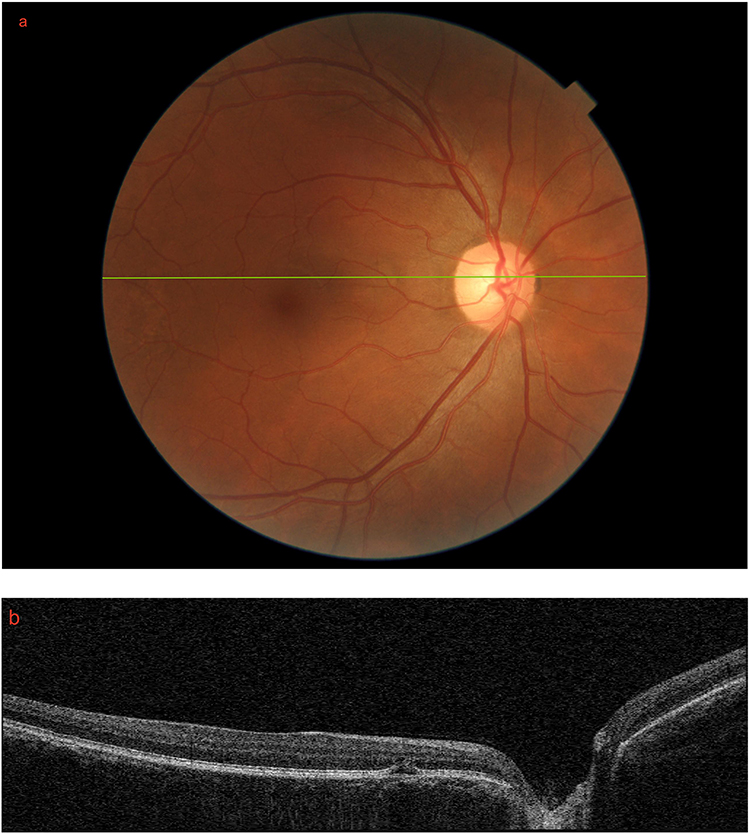 |
Figure 7 A patient with idiopathic central serous chorioretinopathy. (a) Fundus photograph of a patient with a lesion along the papillomacular bundle; (b) B-scan OCT of the green line in (a) showing serous detachment. |
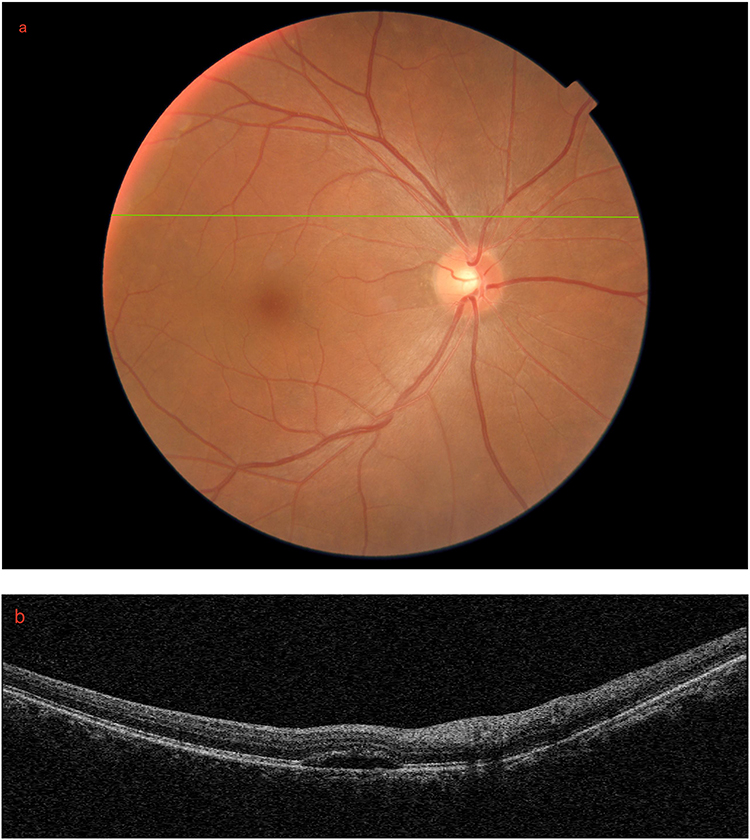 |
Figure 8 Another patient with idiopathic central serous chorioretinopathy. (a) Fundus photograph of a patient with a lesion at the superior perimacular region; (b) B-scan OCT of the green line in (a) showing serous detachment. |
Figure 9 was a patient with both serous detachment and cystoid macular edema (CME). Figure 10 is an example of two patients with thin RNFL. Examples of lamellar holes are shown in Figures 11 and 12. Figure 13 is an example of focal choroidal excavation.
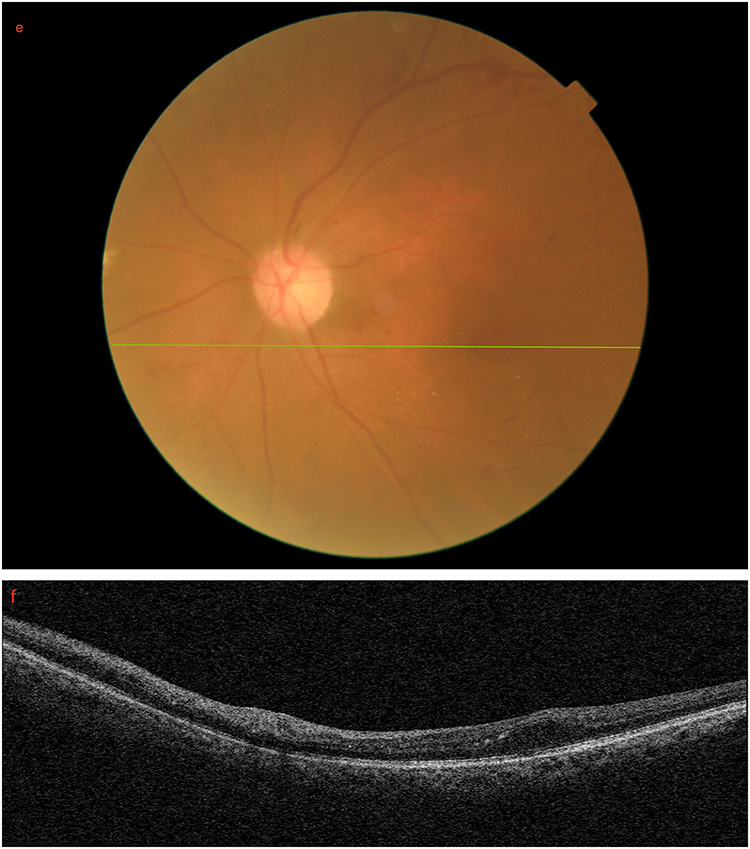
Figure 9 A patient with both serous detachment and cystoid macular edema. (a) Fundus photograph of a diabetic patient’s right eye with non-proliferative diabetic retinopathy; (b) B-scan OCT of the green line in (a) showing cystoid macular edema; (c) Fundus photo of the same patient with OCT at the foveal region; (d) B-scan OCT of the green line in (c) showing serous detachment; (e) Fundus photo of the same patient’s left eye; (f) B-scan OCT of the green line in (e) showing cystoid macular edema at the paramacular region. Figure 9 continued. Figure 9 continued.
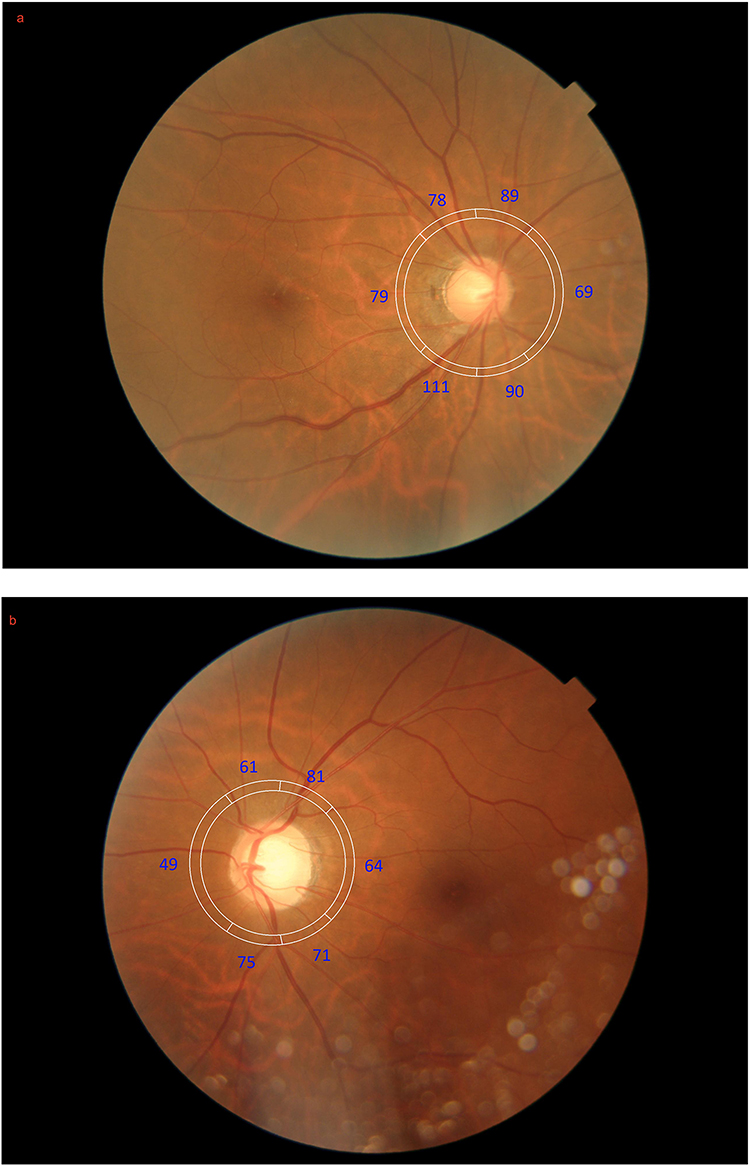 |
Figure 10 Two patients with thin retinal nerve fiber layer (RNFL). (a) A patient with an unusually thin RNFL at the superior temporal region in the right eye. The blue numbers are RNFL thickness value in microns; (b) Another patient with an unusually thin RNFL in both the superior and inferior temporal regions in the left eye. The blue numbers are RNFL thickness value in microns. |
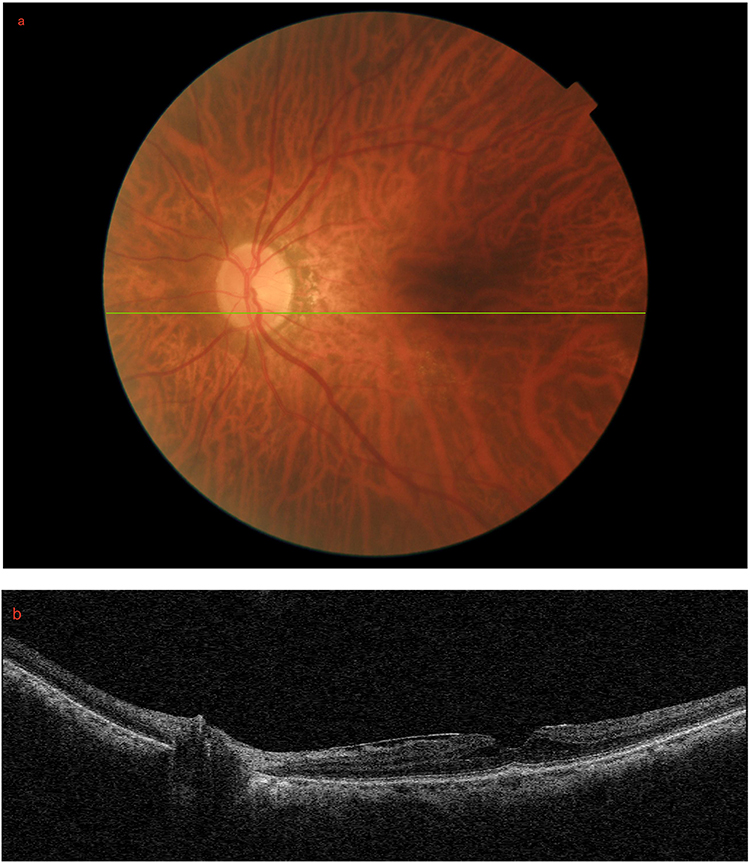 |
Figure 11 A patient with a lamellar hole. (a) Fundus photo of a patient’s fovea; (b) B-scan OCT of the green line in (a) showing a tractional lamellar hole with epiretinal membrane. |
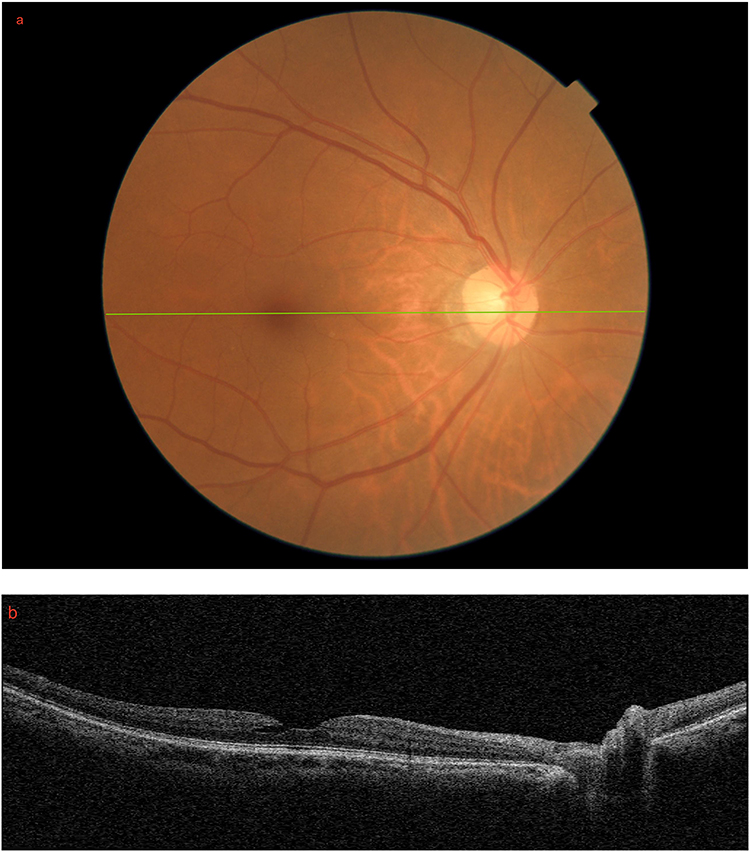 |
Figure 12 Another patient with a lamellar hole. (a) Fundus photo of a patient’s fovea; (b) B-scan OCT of the green line in (a) showing a degenerative lamellar hole. |
 |
Figure 13 A patient with focal choroidal excavation. (a) Fundus photo of a patient’s fovea; (b) B-scan OCT of the green line in (a) showing focal choroidal excavation. |
Discussion
OCT is an ideal imaging modality for identifying ocular lesions. The three most common occult retinal abnormalities missed in the comprehensive eye examination but identified in the pre-consultation OCT examination were posterior vitreous detachment (PVD), ERM, and PICC. Our optometrists were unable to detect them during the comprehensive eye examination but they were identified by OCT imaging. This was likely because the patients had good BCVA and the abnormalities were mild. Weill et al reported that age-related macular degeneration (AMD) and ERM are the two most common pathologies missed in a normal macular slit-lamp biomicroscopy in patients scheduled for cataract surgery.9 Other similar studies also found a high prevalence of vitreoretinal interface abnormalities.8,10 Icoz and Icoz14 found that ERM was the most common occult retinal pathologies detected by OCT imaging, followed by AMD.
Detection of mild asymptomatic PVD is difficult through DFE because the vitreous is a transparent and invisible gel. It is conceivable that there is a high prevalence of PVD on OCT examination using cross-sectional B-scan images. In the past, PVD was reported to occur after the sixth decade of life.15 Tsukahara et al employed wide-angle OCT and found that PVD occurred in patients as young as 21 years of age with a very mild stage.16 The detachment mainly occurs in the paramacular to peripheral regions. Hayashi et al suggested that PVD can be detected even in children during their first or second decade of life through montaged OCT imaging.17 When PVD is associated with symptoms such as the onset of flashes and floaters, the risk of retinal tears or vitreous hemorrhage is high.18 Recent studies reported that up to 25% of patients with acute PVD had complications including lattice degeneration, vitreous hemorrhage, and retinal breaks without or with detachment during DFE.19,20 Eighty-one patients (5.9%) with PVD identified through pre-consultation OCT did not report seeing floaters. Thirty-eight patients had a bilateral PVD. Mild detachment may have been missed because it was either far from the fovea or at a very mild stage. For acute symptomatic PVD without concurrent retinal tears, 7.39% of patients develop retinal lesions several years later.21 Hence, repeated examination is important to identify similar abnormalities in the fellow eye.22,23 These studies focused on acute symptomatic PVD. Further investigations are required to determine whether asymptomatic PVD has a similar rate of delayed retinal abnormalities.
Forty-six patients (3.4%) had mild ERM, which was not identified from comprehensive eye examination. ERM was bilateral in eight patients. The ERM can occur idiopathically in the macular or at the paramacular regions due to PVD. The former is commonly known as macular pucker. It can be identified from structural evaluations, such as distorted retinal vessels in the fundus examination, as well as functional evaluations, such as metamorphopsia from the Amlser chart. It has a prevalence rate of 7% to 11.8%.24,25 The International Vitreomacular Traction Study Group has defined and classified different stages of vitreomacular adhesion and traction based on anatomy without regard to symptoms.26 These 46 patients were asymptomatic, and no sign of ERM was noted on fundus examination. Mild ERM was detected only on OCT images. Several macular problems can occur owing to excessive traction on the inner retinal surface. In addition to ERM, there are pseudoholes, lamellar holes, and full-thickness macular holes. The ERM is formed during vitreoschisis, with vitreous separation from the inner retinal surface, which triggers the proliferation of glial cells and histiocytes. Mild ERM or ERM that do not involve the macula may not cause any symptoms. Early diagnosis of mild ERM is important for practitioners to issue Amsler charts for patient self-monitoring. Gelormini et al found that ERM could affect near visual performance, including near BCVA and reading speed.27 Surgical treatment involves removing the ERM or together with the internal limiting membrane.28 However, it remains controversial, because of the potential postoperative complications associated with the surgery.29,30
PICC was first described by Freund et al using time-domain OCT.31 It is a complication mainly observed in highly myopic eyes. It normally appears as a yellow-orange lobular lesion at the edge of the optic disc. OCT can highlight abnormalities at the intrachoroidal location, thereby earning its current name.32 In our study, 43 patients (3.1%) had PICC, four of which were bilateral. We found that PICC occurred more commonly in a region inferior to the optic disc (Figures 1–4), rather than superior to the optic disc (Figure 5). Eyes with PICC could have visual field defects or retinoschisis between the subretinal or intraretinal space and the PICC cavity.33 Huang et al found that PICC was more prevalent in myopic eyes with open-angle glaucoma.34 Our patients with PICC had healthy neural rim.
PED is a relative common feature in eyes with ICSC or AMD. In our study, 27 patients (2.0%) with mild PED in the perimacular region were identified by the pre-consultation OCT, with no signs on fundus examination. The impact on the fovea was considered minimal. Lewis noted that tiny serous PEDs can be too small to detect on routine fundus examination.35 Our findings were consistent with this observation (Figure 6). Pre-consultation OCT also identified tiny ICSC close to the macula (Figure 7), and perimacular region (Figure 8). Younger patients with PED could be a benign lesion, whereas older patients could be associated with AMD with possible hemorrhagic sequelae.36 Zayit-Soudry et al wrote a comprehensive review on different types of PED.37 Serous PED usually appears yellow-orange with a reddish halo of subretinal fluid, whereas drusenoid PED is more orange-gray. Fibrovascular PED is difficult to identify from colour fundus photography unless there is haemorrhage associated with it.38 A small PED with heterogeneous internal reflectivity and a connected double-layer sign on OCT may suggest a polypoidal lesion in polypoidal choroidal vasculopathy (PCV).39 Hence, patients with PED require more frequent monitor including the issue of an Amsler chart.
OCT is useful to differentiate different causes of macular thickening. There was a diabetic patient with systemic hypertension and hyperlipidemia. Apart from non-proliferative diabetic retinopathy in each eye, this patient had both serous detachment and CME in one eye but just CME in the other eye (Figure 9). Management of serous detachment and CME are different. The former can be recovered on its own or through photodynamic therapy if it cannot be resolved spontaneously while the latter requires anti-vascular endothelial growth factor therapy. Hence, an accurate diagnosis is important.
Our scan modality included measurement of the circumpapillary RNFL. There were 12 patients with RNFL thinning at the superior or inferior temporal regions than the database of the OCT system. Figure 10 is an example. Glaucoma workup including high resolution OCT and perimetry was advised to these patients to further evaluation the cause of RNFL thinning. Six of them returned and three patients were eventually referred to ophthalmologists due to normal tension glaucoma (Table 3). Six patients did not return for glaucoma workup. It was unknown if they did have thin RNFL, or simply a false-positive for thin RNFL, ie. red disease.40 Practitioners may measure circumpapillary RNFL to screen for glaucoma. Kim and Park41 advocated the incorporation of three-dimensional neuroretinal rim measurement to reduce the false-positive rate for glaucoma diagnosis. Utilization of OCT for screening glaucoma patient remains controversial. High-risk populations may be worth for OCT examination for early diagnosis of glaucoma.42 However, more examinations such as evaluation of the neural rim, perimetry, Bruch’s membrane opening-minimum rim width, etc, should be considered to better diagnose glaucoma.43
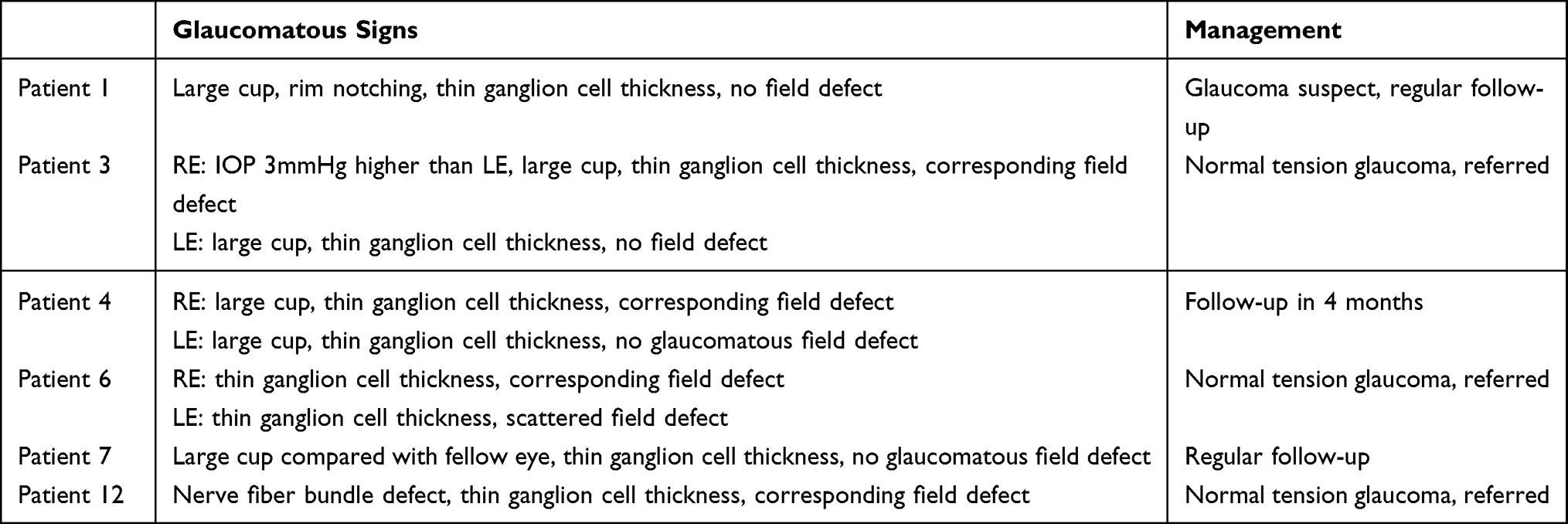 |
Table 3 Six Out of 12 Patients with Thin Retinal Nerve Fiber Layer Thickness from Optical Coherence Tomography Returned for Glaucoma Work-Up |
Twelve patients had lamellar holes. Our dataset did not have patients with full-thickness macular hole. Development of lamellar hole could be due to progressive contraction of ERM.44 Govetto et al45 divided lamellar macular holes into tractional (Figure 11) and degenerative types (Figure 12), with the former one highly associated with ERM. Surgical intervention may not be necessary, particularly if there is no epiretinal proliferation.46 Kim et al also reported that vision was stable in tractional macular holes even without surgical intervention.47 Other abnormalities picked up by OCT included reticular pseudodrusen (Figure 2) and focal choroidal excavation (Figure 13).
Hood et al suggested that a real-world reference database could be created by using OCT scans of healthy patients from optometry sites.12 We obtained good number of OCT scans in just two months. Further analyses of these images with the use of artificial intelligence may facilitate the generation of a validated real-world reference database. Regarding the use of OCT in tele-health programme, a pilot study has shown good patient convenience and adherence.13
There are limitations of this study. This study involved one single optometry clinic. This clinic-based, self-selected cohort cannot represent the general population in Hong Kong. These individuals could be more health conscious and may have higher socioeconomic or educational status. These occult retinal abnormalities could be mild and patients could be asymptomatic in this primary care setting. We did not aim to study prevalence of different ocular abnormalities. Purpose of this study is to evaluate usefulness of OCT in a primary care setting. The reported frequencies indicated occult retinal abnormalities that were missed in comprehensive eye examination but identified from OCT.
Conclusion
Vision screening is common for paediatric group,48,49 whereas ocular health screening is more important in older population.50,51 Most of the ocular health screening rely on fundus photography incorporating digital technology,52 and artificial intelligence.53 Although some occult retinal pathologies were detected, there was no alternation on patient management because these retinal pathologies were very mild (eg. PVD and ERM), away from the macula (eg. PED), or no serious consequence (eg. FCE and PICC). Hence, routine OCT examinations might not be necessary as a routine procedure.
Study Approval
This research adhered to the principles of the Declaration of Helsinki and its ethical guidelines. Approval for this study was granted by the Institute Review Board of The Hong Kong Polytechnic University (HSEARS20250924004).
Acknowledgments
We would like to thank Editage (www.editage.com) for English language editing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Qin J, An L. Optical coherence tomography for ophthalmology imaging. Adv Exp Med Biol. 2021;3233:197–19. doi:10.1007/978-981-15-7627-0_10
2. Zeppieri M, Marsili S, Enaholo ES, et al. Optical Coherence Tomography (OCT): a brief look at the uses and technological evolution of ophthalmology. Medicina. 2023;59(12):2114. doi:10.3390/medicina59122114
3. Minakaran N, de Carvalho ER, Petzold A, et al. Optical coherence tomography (OCT) in neuro-ophthalmology. Eye. 2021;35(1):17–32. doi:10.1038/s41433-020-01288-x
4. Ge JY, Teo ZL, Loo JL. Recent advances in the use of optical coherence tomography in neuro-ophthalmology: a review. Clin Exp Ophthalmol. 2024;52(2):220–233. doi:10.1111/ceo.14341
5. Muijzer MB, Schellekens P, Beckers HJM, et al. Clinical applications for intraoperative optical coherence tomography: a systematic review. Eye. 2022;36(2):379–391. doi:10.1038/s41433-021-01686-9
6. Lang SJ, Heinzelmann S, Böhringer D, et al. Indications for intraoperative anterior segment optical coherence tomography in corneal surgery. Int Ophthalmol. 2020;40(10):2617–2625. doi:10.1007/s10792-020-01442-0
7. Ly A, Phu J, Katalinic P, et al. An evidence-based approach to the routine use of optical coherence tomography. Clin Exp Optom. 2019;102(3):242–259. doi:10.1111/cxo.12847
8. Ahmed TM, Siddiqui MAR, Hussain B. Optical coherence tomography as a diagnostic intervention before cataract surgery-a review. Eye. 2023;37(11):2176–2182. doi:10.1038/s41433-022-02320-y
9. Weill Y, Hanhart J, Zadok D, et al. Patient management modifications in cataract surgery candidates following incorporation of routine preoperative macular optical coherence tomography. J Cataract Refract Surg. 2021;47(1):78–82. doi:10.1097/j.jcrs.0000000000000389
10. Fouad YA, ElGwaily AM, Shaaban YM. Screening for occult macular pathology prior to cataract surgery using optical coherence tomography. Clin Ophthalmol. 2025;19:317–324. doi:10.2147/opth.S507995
11. Paul JP, McGuinness MB, Ashby BD, et al. Increased glaucoma case-finding through routine optical coherence tomography in optometry practice. J Glaucoma. 2024;33(5):347–354. doi:10.1097/ijg.0000000000002339
12. Hood DC, Durbin M, Lee C, et al. Toward a real-world optical coherence tomography reference database: optometric practices as a source of healthy eyes. Optom Vis Sci. 2023;100(8):499–506. doi:10.1097/opx.0000000000002049
13. Ashrafzadeh S, Gundlach BS, Tsui I. Implementation of teleretinal screening using optical coherence tomography in the veterans health administration. Telemed J E Health. 2021;27(8):898–904. doi:10.1089/tmj.2021.0118
14. Icoz M, Gurturk Icoz SG. Importance of optical coherence tomography before cataract surgery. BMC Ophthalmol. 2024;24(1):339. doi:10.1186/s12886-024-03622-3
15. Novak MA, Welch RB. Complications of acute symptomatic posterior vitreous detachment. Am J Ophthalmol. 1984;97(3):308–314. doi:10.1016/0002-9394(84)90628-7
16. Tsukahara M, Mori K, Gehlbach PL, et al. Posterior vitreous detachment as observed by wide-angle OCT imaging. Ophthalmology. 2018;125(9):1372–1383. doi:10.1016/j.ophtha.2018.02.039
17. Hayashi A, Ito Y, Takatsudo Y, et al. Posterior vitreous detachment in normal healthy subjects younger than age twenty. Invest Ophthalmol Vis Sci. 2021;62(13):19. doi:10.1167/iovs.62.13.19
18. Gishti O, van den Nieuwenhof R, Verhoekx J, et al. Symptoms related to posterior vitreous detachment and the risk of developing retinal tears: a systematic review. Acta Ophthalmol. 2019;97(4):347–352. doi:10.1111/aos.14012
19. Patel PR, Minkowski J, Dajani O, et al. Analysis of posterior vitreous detachment and development of complications using a large database of retina specialists. Ophthalmol Retina. 2023;7(3):203–214. doi:10.1016/j.oret.2022.11.009
20. Driban M, Chhablani J. Clinical findings in acute posterior vitreous detachment. Graefes Arch Clin Exp Ophthalmol. 2022;260(11):3465–3469. doi:10.1007/s00417-022-05708-4
21. Jindachomthong KK, Cabral H, Subramanian ML, et al. Incidence and risk factors for delayed retinal tears after an acute, symptomatic posterior vitreous detachment. Ophthalmol Retina. 2023;7(4):318–324. doi:10.1016/j.oret.2022.10.012
22. Uhr JH, Obeid A, Wibbelsman TD, et al. Delayed retinal breaks and detachments after acute posterior vitreous detachment. Ophthalmology. 2020;127(4):516–522. doi:10.1016/j.ophtha.2019.10.020
23. Hikichi T. Time course of posterior vitreous detachment in the second eye. Curr Opin Ophthalmol. 2007;18(3):224–227. doi:10.1097/ICU.0b013e3281299022
24. Fung AT, Galvin J, Tran T. Epiretinal membrane: a review. Clin Exp Ophthalmol. 2021;49(3):289–308. doi:10.1111/ceo.13914
25. Kim JS, Kim M, Kim SW. Prevalence and risk factors of epiretinal membrane: data from the Korea National Health and Nutrition Examination Survey VII (2017–2018). Clin Exp Ophthalmol. 2022;50(9):1047–1056. doi:10.1111/ceo.14164
26. Duker JS, Kaiser PK, Binder S, et al. The International Vitreomacular Traction Study Group classification of vitreomacular adhesion, traction, and macular hole. Ophthalmology. 2013;120(12):2611–2619. doi:10.1016/j.ophtha.2013.07.042
27. Gelormini F, Ricardi F, Parisi G, et al. Visual performance and predictive OCT biomarkers in epiretinal membrane assessment: beyond distance visual acuity. Invest Ophthalmol Vis Sci. 2025;66(1):31. doi:10.1167/iovs.66.1.31
28. Matoba R, Morizane Y. Epiretinal membrane: an overview and update. Jpn J Ophthalmol. 2024;68(6):603–613. doi:10.1007/s10384-024-01127-6
29. Matoba R, Morizane Y. Surgical treatment of epiretinal membrane. Acta Med Okayama. 2021;75(4):403–413. doi:10.18926/amo/62378
30. Pike D, Mandelcorn ED, Sheidow T, et al. Inner-limiting-membrane peeling in epiretinal membrane surgery: an evolving surgical trend. Can J Ophthalmol. 2020;55(2):e72–e74. doi:10.1016/j.jcjo.2019.07.016
31. Freund KB, Ciardella AP, Yannuzzi LA, et al. Peripapillary detachment in pathologic myopia. Arch Ophthalmol. 2003;121(2):197–204. doi:10.1001/archopht.121.2.197
32. Toranzo J, Cohen SY, Erginay A, et al. Peripapillary intrachoroidal cavitation in myopia. Am J Ophthalmol. 2005;140(4):731–732. doi:10.1016/j.ajo.2005.03.063
33. Ehongo A, Bacq N. Peripapillary Intrachoroidal Cavitation. J Clin Med. 2023;12(14):4712. doi:10.3390/jcm12144712
34. Huang J, Luo N, Ye L, et al. Peripapillary intrachoroidal cavitation in myopic eyes with open-angle glaucoma: association with myopic fundus changes. Graefes Arch Clin Exp Ophthalmol. 2025. doi:10.1007/s00417-025-06822-9
35. Lewis ML. Idiopathic serous detachment of the retinal pigment epithelium. Arch Ophthalmol. 1978;96(4):620–624. doi:10.1001/archopht.1978.03910050316004
36. Klein ML, Obertynski H, Patz A, et al. Follow-up study of detachment of the retinal pigment epithelium. Br J Ophthalmol. 1980;64(6):412–416. doi:10.1136/bjo.64.6.412
37. Zayit-Soudry S, Moroz I, Loewenstein A. Retinal pigment epithelial detachment. Surv Ophthalmol. 2007;52(3):227–243. doi:10.1016/j.survophthal.2007.02.008
38. Silva VB, Brockhurst RJ. Hemorrhagic detachment of the peripheral retinal pigment epithelium. Arch Ophthalmol. 1976;94(8):1295–1300. doi:10.1001/archopht.1976.03910040167009
39. Wang Y, Bo Q, Jia H, et al. Small dome-shaped pigment epithelium detachment in polypoidal choroidal vasculopathy: an under-recognized sign of polypoidal lesions on optical coherence tomography? Eye. 2022;36(4):733–741. doi:10.1038/s41433-020-01390-0
40. Chong GT, Lee RK. Glaucoma versus red disease: imaging and glaucoma diagnosis. Curr Opin Ophthalmol. 2012;23(2):79–88. doi:10.1097/ICU.0b013e32834ff431
41. Kim YW, Park KH. Diagnostic accuracy of three-dimensional neuroretinal rim thickness for differentiation of myopic glaucoma from myopia. Invest Ophthalmol Vis Sci. 2018;59(8):3655–3666. doi:10.1167/iovs.18-24283
42. Johnson NA, Gupta P, Lee T, et al. The use of optical coherence tomography for early glaucoma screening in a population of patients with diabetes. Ophthalmic Epidemiol. 2024;31(2):145–151. doi:10.1080/09286586.2023.2214929
43. Yusof AMZ, Othman O, Tang SF, et al. Diagnostic evaluation of optical coherence tomography parameters in normal, preperimetric and perimetric glaucoma patients. Int J Ophthalmol. 2022;15(11):1782–1790. doi:10.18240/ijo.2022.11.08
44. Michalewski J, Michalewska Z, Dzięgielewski K, et al. Evolution from macular pseudohole to lamellar macular hole - spectral domain OCT study. Graefes Arch Clin Exp Ophthalmol. 2011;249(2):175–178. doi:10.1007/s00417-010-1463-1
45. Govetto A, Dacquay Y, Farajzadeh M, et al. Lamellar macular hole: two distinct clinical Entities? Am J Ophthalmol. 2016;164:99–109. doi:10.1016/j.ajo.2016.02.008
46. Ko J, Kim GA, Lee SC, et al. Surgical outcomes of lamellar macular holes with and without lamellar hole-associated epiretinal proliferation. Acta Ophthalmol. 2017;95(3):e221–e226. doi:10.1111/aos.13245
47. Kim KM, Woo SJ, Park SJ, et al. Natural history of tractional lamellar macular hole. Retina. 2026;46(1):93–97. doi:10.1097/iae.0000000000004659
48. Crippa J, Flaherty M, Silveira S. Towards a national pre-school vision screening programme. J Paediatr Child Health. 2022;58(6):948–952. doi:10.1111/jpc.15971
49. Oke I, Slopen N, Galbraith AA, et al. Gaps in the vision screening pathway for school-aged US Children. JAMA Ophthalmol. 2024;142(3):268–270. doi:10.1001/jamaophthalmol.2023.6316
50. Kolomeyer AM, Szirth BC, Shahid KS, et al. Software-assisted analysis during ocular health screening. Telemed J E Health. 2013;19(1):2–6. doi:10.1089/tmj.2012.0070
51. Sinclair SH, Schwartz S. Diabetic retinopathy: new concepts of screening, monitoring, and interventions. Surv Ophthalmol. 2024;69(6):882–892. doi:10.1016/j.survophthal.2024.07.001
52. Wu X, Wu Y, Tu Z, et al. Cost-effectiveness and cost-utility of a digital technology-driven hierarchical healthcare screening pattern in China. Nat Commun. 2024;15(1):3650. doi:10.1038/s41467-024-47211-w
53. Arenas-Cavalli JT, Abarca I, Rojas-Contreras M, et al. Clinical validation of an artificial intelligence-based diabetic retinopathy screening tool for a national health system. Eye. 2022;36(1):78–85. doi:10.1038/s41433-020-01366-0
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.