Back to Journals » Risk Management and Healthcare Policy » Volume 13
Obstetric Telephone Triage
Authors Engeltjes B ![]() , Wouters E
, Wouters E ![]() , Rijke R, Scheele F
, Rijke R, Scheele F ![]()
Received 20 August 2020
Accepted for publication 14 October 2020
Published 5 November 2020 Volume 2020:13 Pages 2497—2506
DOI https://doi.org/10.2147/RMHP.S277464
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Bernice Engeltjes,1,2 Eveline Wouters,3 Rudy Rijke,2 Fedde Scheele1
1Athena Institute of Transdisciplinary Research, VU University Amsterdam, Amsterdam, the Netherlands; 2School of Health Care Studies, Rotterdam University of Applied Sciences, Rotterdam, the Netherlands; 3Department of Tranzo, School of Social and Behavioral Sciences, Tilburg University, Tilburg, the Netherlands
Correspondence: Bernice Engeltjes
School of Health Care Studies, Rotterdam University of Applied Sciences, Rochussenstraat 198, Rotterdam 3015 EK, the Netherlands
Tel +31 6 41804881
Email [email protected]
Objective: Little is known about obstetric telephone triage: the methods used to prioritize the severity of symptoms of obstetric emergency and other unplanned care requests originating by telephone. In large-scale obstetric units, there is a need for an evidence-based triage guideline. The aim of this study was to develop an obstetric guideline for telephonic triage.
Design, Setting and Participants: A multi-phase multi-center study was performed with consecutive drafts of the triage guideline using four focus groups, four observations of training sessions and two expert consultations based on the Delphi method. The study was performed in ten hospitals in the Netherlands. The obstetric care professionals involved were gynecologists, midwives, nurses, doctor’s assistants, team managers and application managers. After each focus group, each observation and each expert consultation, an interpretative analysis was undertaken. Based on these analyses, the obstetric telephone triage guideline was drafted.
Measurements and Results: The designed guideline describes the primary symptoms presented, five prioritization categories and several descriptors. Consensus (> 90%) was reached during the second expert consultation. Fifty-seven (91.9%) participants stated that the obstetric telephone triage guideline was clinically complete, correct, user-friendly and well designed, and 61 (98.4%) participants judged that the newly designed triage guideline was ready to use in daily practice.
Key-Conclusions and Implications for Practice: An evidence-based guideline for obstetric telephone triage was developed through a multi-phase multi-center study with all stakeholders. The guideline was found to be clinically complete, correct, well-designed and user-friendly. It provides a uniform and concrete basis for assessing the severity of the symptoms of obstetric emergency and other unplanned care requests originating by telephone. It also provides a good basis to further develop this evidence-based guideline for telephone triage by continuous registration of all calls.
Keywords: midwifery, obstetric telephone triage, triage guideline, unplanned telephone obstetric care
Introduction
In the Netherlands, the geographical concentration of acute obstetric care has led to an increase in the number of pregnant women per location. On average, obstetric emergency care departments in Dutch hospitals receive 20 to 30 telephone calls from pregnant women per day. During these calls, midwives, nurses or doctor’s assistants use their obstetric knowledge and experience to determine the severity of the complaints and the necessity and urgency for a physical consultation with an obstetrician or a midwife. This telephone triage is a medical procedure that is currently not performed in a uniform manner due to lack of specific guidelines.1–3
Evidence suggests that uniformity of triage would have a favorable effect on the safety and efficacy of emergency care.4 In general healthcare, triage systems such as the Manchester Triage System (MTS), the Emergency Severity Index (ESI) and the guidelines of the Dutch Triage Standard (NTS) contain background information about presenting symptoms and prioritization codes, which aim to indicate the maximum acceptable medical waiting time.5,6 However, as they do not address the physiological changes in pregnancy, the triage systems for general emergency care are not specific enough for unplanned obstetric care requests of pregnant women.7 For this reason, the Rotterdam Obstetric Triage System (ROTS) has been developed between 2007 and 20138,9 (articles in Dutch). In the same period one of the first obstetric triage systems – the Obstetric Triage Acuity Scale (OTAS) – evolved in Canada.10,11 In the United States, the Maternal Fetal Triage Index (MFTI) has been developed, which is based on the ESI.12 In Switzerland, an obstetric section has been added to the general Swiss Emergency Triage Scale (SETS).7
It is important to note however that these guidelines have all been developed to classify the urgency of care requests by means of physical (face-to-face) triage. Nonetheless, in practice most women call first to ask whether it is necessary to have a check-up. Telephone triage has many positive aspects, such as efficacy and uniformity, both for care professionals and for women. Challenges exist because of the lack of a clinical perspective during the telephone call and because the lack of specific diagnostic information, eg, blood pressure. Ideally, a triage guideline should be usable on both occasions.3,13 The aim of this study was to develop an obstetric guideline for telephonic triage.
Materials and Methods
Design
A multi-phase multi-center study was performed with consecutive drafts of the telephone triage guideline using four focus groups, four observations of training sessions and two expert consultations based on the Delphi method.14,15 After focus group, and/or observation and the Delphi round, interpretative analysis was undertaken. Based on these analyses, a new version of the obstetric telephone triage guideline was drafted (Table 1).
 |
Table 1 Schematic Overview of the Consecutive Phases of Development of the Telephone Triage Guideline |
The aims of the focus group discussions were 1) to investigate the current procedures for unplanned telephone consultations, 2) to evaluate the applicability, value and limitations of the physical triage system ROTS for telephone triage and 3) to determine quality themes for obstetric telephone triage.
For the observations, the objectives were 1) to evaluate the usability of the triage guideline, and 2) to correct incompleteness and inaccuracies.
In the digital expert consultation (Delphi rounds) the objectives were 1) to formulate an obstetric telephone triage guideline based on sufficient consensus and 2) to test and optimize the transferability of the guideline (Table 1).
Participants
During the focus groups, observations and Delphi rounds, participants represented a broad range of obstetric care professionals: nursing personnel (specialized nurses, general nurses and doctor’s assistants), medical personnel (gynecologists, residents, physician assistants and, clinical midwives) and supporting services personnel (policy makers, managers and management team leaders, application managers).
Focus Groups
Focus groups consisted of six to nine care professionals from four different hospitals (three general hospitals and one academic hospital). The first author (BE) had the role of observer during all focus groups. The moderator was a psychologist or a policy maker. Topics to be discussed were chosen according to Wester and Peters16 (Table 2). All focus groups were verbatim transcribed.
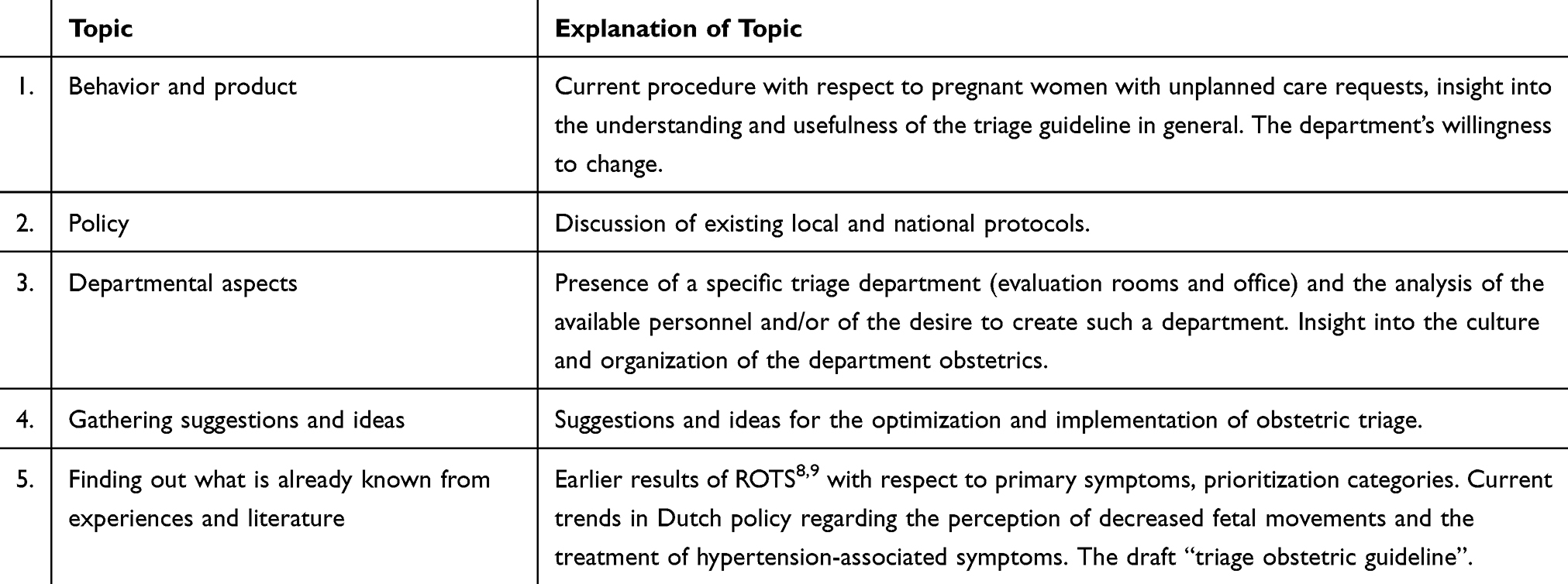 |
Table 2 Overview of Topics for the Focus Groups and Explanation |
Transcripts of the focus groups were analyzed with respect to themes. Meaningful sections of text were coded via open coding, axial coding, codes/topics and subcodes/subtopics.17 After each focus group, a summary was written and presented to the participants for their review (member check). Each focus group ended with adjustments of the draft guideline.
Observations of Training Sessions
Four triage training sessions were observed. During each training session, twelve obstetric care professionals applied the triage guideline draft (Table 1) to twenty cases, which were purposefully chosen from practice. Mild, moderate and severe cases were included. The first and second training sessions were conducted with a group of intended users (nurses and doctor’s assistants). In the third and fourth training sessions, the group was expanded to include all obstetric care professionals (gynecologists, clinical midwives, nurses, and doctor’s assistants). The training sessions were led by a psychologist, and the roles of the pregnant women were played by actors. Any lack of clarity that became apparent during these observations regarding the usefulness of the triage guideline was corrected and changes were incorporated into the obstetric triage guideline draft (version 2 and 3) (Table 1).
Delphi Method
The Delphi rounds were executed until consensus was achieved, with consensus being defined as at least 90% agreement.14,15
All participants of the focus groups of the four hospitals were invited to participate in the Delphi rounds. To test and optimize transferability of the triage guideline, in addition also participants from six other hospitals were selected (Table 1). The optimal number of participants was 60. Taking non-responders into account, 75 care professionals were invited to participate in the first Delphi round. For the second Delphi round, all professionals of the first Delphi round were invited again to participate. Those who had not responded to the invitation for the first round were asked if they were willing to participate this time. In the second round, 69 care professionals were invited.
The Delphi rounds were held according to the theory of van Zolingen en Klaassen (2002).15 During the first expert consultation, 75% of the questions were open-ended questions about obstetric triage.14,15,18 The analyses of the results from the first Delphi round were discussed and summarized by the research group (BE, EW, RR, FS) based on the quality themes formulated during the focus group discussions. The interpretations of the feedback were incorporated into the next version of the obstetric triage guideline (Version 5, Table 1). During the second Delphi round, interpretations of the first round were shared with participants. During this second round, mainly close-ended and more in-depth questions were asked.
Before sending the questions to all participants of the Delphi rounds, the questions were pretested by independent experts who had not previously participated in the study. The questions were presented along with the obstetric telephone triage guideline in PDF format (Table 1). The first Delphi round was held between March 26th and April 19th 2017 and the second Delphi round was held between June 16th and July 14th 2017.
Ethical Approval
The study was approved by the Medical Research Ethics Committees United (MEC-U) and the Medical Ethics Committee of Leiden University Medical Center (LUMC, 2016) Act (W.16.053 and P17.075/PG/pg).
Results
In total, 30 care professionals participated in the focus groups. During four training sessions, 48 care professionals were observed. In the first Delphi round, 62 (82.7%) of the 75 invitees participated, and in the second Delphi round, 62 (89.9%) of the 69 invitees responded (Table 3). The average age and number of years of work experience in clinical obstetrics were equal in both rounds. Of the 62 participants of each round, 57 (91.9%) took part in both Delphi rounds. About half of the participants of the Delphi rounds had also previously participated in the focus groups, while the other half had no previous acquaintance with the subject of triage and the obstetric triage guideline. The average age and number of years of work experience among participants were equal in both rounds.
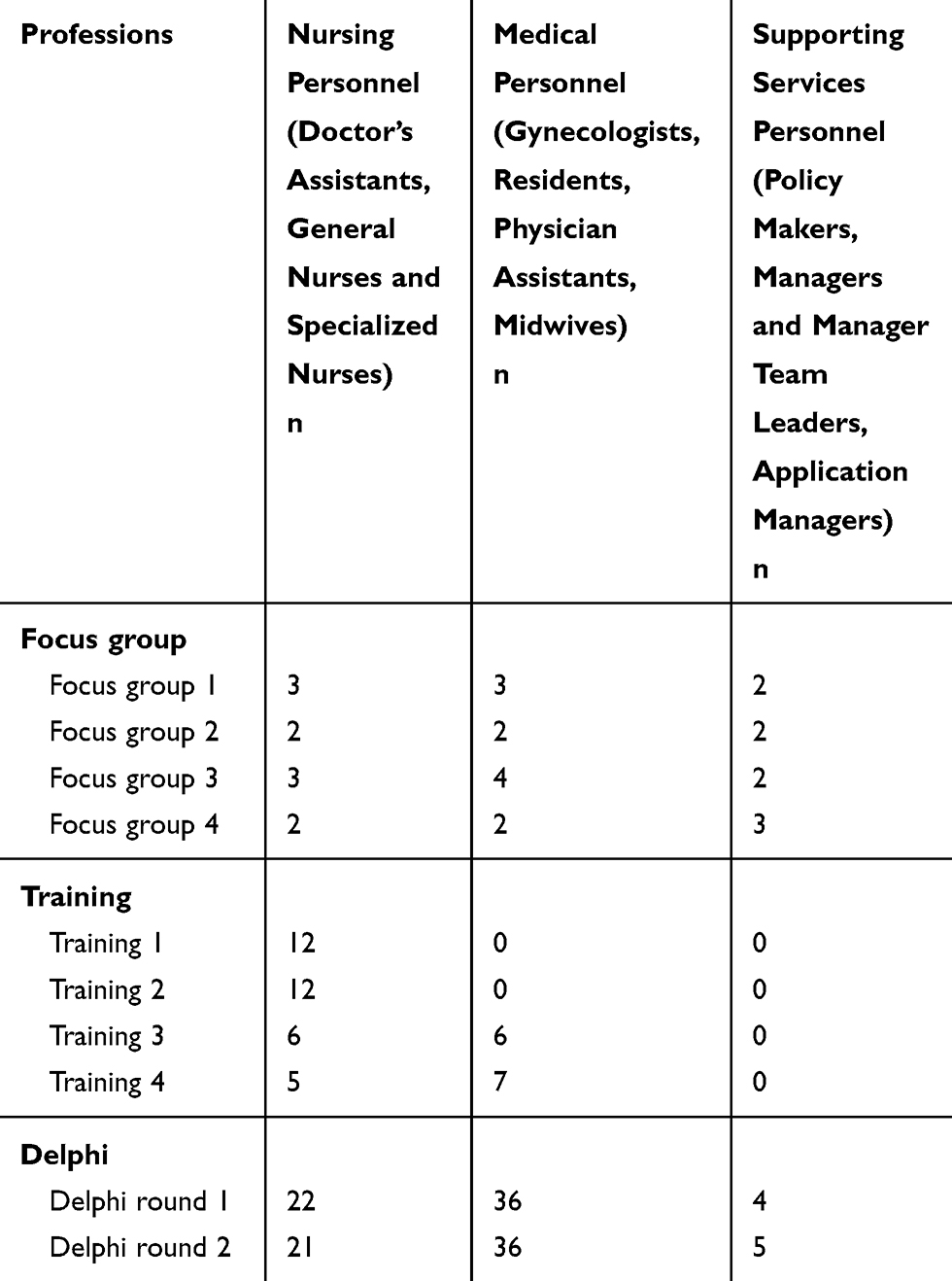 |
Table 3 Participants in the Focus Groups, Triage Training & Delphi Rounds |
Focus Groups
Current Procedure of Unplanned Care
During the focus groups, it became clear that the existing procedure for prioritizing unplanned care differed within hospitals, depending on which professional was on call. Also differences existed between hospitals with respect to logistics and care content. Care professionals stated that it was necessary to develop a structured approach, not only because of the increased number of consultations in recent years but also because of a lack of transparency in the telephone triage process.
According to the current procedure, most pregnant women called the nurse or doctor’s assistant on duty. Based on this call, sometimes the pregnant woman was advised to come to the hospital immediately. In other cases, the nurses or doctor’s assistants considered, based on their knowledge, a consultation not necessary and advised the patient to stay at home. It was not always clear if a midwife or gynecologist was consulted during this decision-making process.
Departmental Aspects
Two hospitals had a stand-alone triage department. At two other hospitals, the delivery room or outpatient clinic was used for triage.
Current Policy and Ideas for Implementation
The participants were aware of the lack of a standard policy for unplanned telephone obstetric triage at the national level. At the local level, various protocols were used, with different levels of details.
Evaluation ROTS
The participants of the focus groups agreed that the already existing physical triage system (ROTS) could be used as the basis for the telephone triage guideline. In their opinion the lack of the clinical perspective during the telephone call and of certain specific information, such as blood pressure, adjustments to this physical triage system were necessary, in order to make it suitable for telephone triage.
Based on information gained from the focus groups, unplanned obstetric care requests over the telephone could be grouped into five categories resulting in the following presenting symptoms: fluid loss, vaginal bleeding, abdominal pain, concerned pregnant/non-somatic symptoms and other physical symptoms. After discussion, consensus on these categories was reached within each focus group.
In order to design a working triage guideline, prioritization categories were determined. The first focus group came up with four prioritization categories; Resuscitation & life threatening, Emergency, Urgent, Non-urgent (Figure 1). Focus group 2 added the category “self-care advice”, in line with both practical experience and general emergency care.
 |
Figure 1 Triage guideline - overview of presenting symptoms and prioritization categories (U= urgency). |
Quality Criteria
After analyzing the focus group discussions, two quality criteria for the telephone triage guideline were identified. These quality criteria were 1) clinical correctness and completeness and 2) user-friendliness and supportive design. User-friendliness should be achieved by developing an application in the electronic patient record. The design should support the recognition of the presenting symptoms and prioritization categories. To this end, participants recommended the use of colors and symbols, as well as an intuitive arrangement of the categories.
Observations of Triage Training Sessions
During the training sessions, care professionals (Tables 1 and 3) were observed as they applied the obstetric telephone triage guideline (versions 1 and 2) to various cases in daily practice. Based on these observations, changes were made to the applied version of the triage guideline to increase its clinical correctness, completeness, design and user-friendliness. For example, “duration of pregnancy” was added to the descriptor “fewer fetal movements”. Also “pregnancy unconfirmed by ultrasound” was added to the descriptor “light vaginal bleeding”. In addition, the contents were displayed in a different lay-out.
Delphi Method
Consensus was reached during the second Delphi round, as 57 (91.9%) of the 62 participants considered the obstetric triage guideline to be complete, correct, user-friendly and well designed. Sixty-one (98.4%) participants regarded the newly designed triage guideline and judged it was ready to implement the telephone triage in daily practice (Figures 1 and 2).
 |
Figure 2 Complete triage guideline - overview of presenting symptoms and prioritization categories (U= urgency). |
Clinical Correctness and Completeness
After the first Delphi round, the clinical correctness was regarded as good by 44 participants (71.0%). Suggested additions were incorporated into the obstetric triage guideline, for instance ‘limbs and hands’ was added to the “itch” descriptor. In the second Delphi round, the obstetric triage guideline was regarded as correct by 55 participants (88.7%).
The obstetric triage guideline (version 4) was judged as clinically complete by 55 participants (88.7%) after the first Delphi round. Only a few additions were incorporated into the triage guideline, such as more information about the “breakdown of vital parameters” diagram. During the second Delphi round, 54 participants (85.7%) stated that the obstetric triage guideline (version 5) was sufficiently complete. Five participants who did not deem the obstetric triage guideline to be complete stated that minor additions and a few corrections to the content of the self-care advice were necessary.
User-Friendliness and Design
During the first Delphi round, the PDF version of the triage guideline was rated as user-friendly by 25 (41.6%) participants. During the second Delphi round, 59 (95.9%) participants considered the obstetric triage guideline to be user-friendly. The design was rated as good and attractive by 47 (75.8%) participants of the first Delphi round. During the second Delphi round, 61 (98.4%) participants stated that the design was sufficient.
Various points of improvement were suggested by the participants, most of which were related to support the user-friendliness in the form of digital aids and posters. Participants also indicated that the user-friendliness could be increased by developing a specific training and implementation program. The obstetric triage guideline was amended in response to the feedback submitted during the first Delphi round. Suggestions were also made with respect to improving digital support and designing posters, including a schematic overview of all presenting symptoms (Figure 2). A schematic overview of a structured triage consultation was designed (Figure 3).
 |
Figure 3 Schematic overview of telephone triage. |
Discussion
Using a multi-phase study, a telephone triage guideline for unplanned obstetric care by telephone was developed in co-creation with professionals. Consensus was reached and the guideline was judged ready for transfer into obstetric practice. To the best of our knowledge, the present study is the first to explore consensus on the content and design of obstetric triage by telephone.
In the development of this telephone triage guideline, all relevant stakeholders were involved. Involvement and co-creation with stakeholders in the developmental phase of a service-design has been recognizes in literature to be of great importance in order to successfully implement innovations in daily practice.19,20
Our findings suggest that when introducing changes to clinical practice such as the implementation of a new working method in the department, involving new tasks and responsibilities, the chances of success will be improved by training of those affected by the change, in our case the triage nurses. This should receive attention during the implementation phase of the guideline. An important aspect is to develop a contextual thinking capacity, ie, to be able to take into account specific circumstances, contexts and complexity.21 Previous studies7,10 also found that investments need to be made in the learning capacity of triage specialists so that they can properly operate within the digital environment of triage. The need for training and incorporation of the triage guideline into the electronic patient records used were also an important outcome of the focus groups and the first Delphi round. Furthermore, training and supervision during implementation need to be developed as an important part of achieving a high-quality, properly functioning triage guideline.3,5,7,22,23
The obstetric telephone triage guideline was developed as a tool to be used by triage nurses. If used correctly, the guideline should not reduce professional autonomy or responsibility. Given the current defensive culture within healthcare, any deviation from a guideline can be experienced as an ethical dilemma.24 Attention must be paid to this fact if this guideline becomes part of obstetric care. The guideline should be used based on a combination of professional insight and patient preferences in accordance with the concept of evidence-based practice.25 Users clinical insight and the feeling that something is “not right” should be taken into account when making decisions.26,27 Research on general emergency care has shown that this “not-right” feeling is important and constitutes a legitimate reason for changing the prioritization category.4,28
A strength of this study was the use of different research methods that were continually analyzed and evaluated (triangulation).29 In addition, all professional groups equally participated in the focus groups, training sessions and Delphi rounds, with a high level of response. In this study the minimum degree of consensus required was set at 90%.
Due to a strong demand for a telephone obstetric triage guideline3, our study has a high degree of clinical relevance. In the Netherlands, the use of this obstetric telephone triage guideline is rapidly expanding. And a structured approach to unplanned obstetric care requests has also become one of the quality marks in accreditation guidelines for hospital care. Our study shows that it is possible to use an inclusive framework to ensure that clinical professionals can work jointly to develop a high-quality, clinical correct and complete telephone triage guideline, with corresponding scientific evaluations. For the international field, this triage guideline may serve as a useful tool or as an example to be tailored to local culture and context.
Having reached consensus about the content of the obstetric telephone triage guideline, the next step will be to examine its reliability and diagnostic validity. The validity of the triage guidelines used in general emergency care was found to vary significantly.5 To provide clarity about the validity of the obstetric telephone triage guideline, a prospective observational study at various hospitals is under construction as recommended.5,29,30
Conclusion
Using the existing obstetric physical triage system ROTS as a basis, we developed an obstetric telephone triage guideline, which was judged by professional users to be clinically complete, correct, well-designed and user-friendly.
Clinical Trial Registry
Not applicable.
Abbreviations
ESI, Emergency Severity Index; MFTI, Maternal Fetal Triage Index; MTS, Manchester Triage System; NTS, Dutch Triage Standard; OTAS, Obstetric Triage Acuity Scale; ROTS, Rotterdam Obstetric Triage System; SETS, Swiss Emergency Triage Scale.
Ethical Approval and Consent
The study was approved by the Medical Research Ethics Committees United (MEC-U) and the Medical Ethics Committee of Leiden University Medical Center (LUMC, 2016) Act (W.16.053 and P17.075/PG/pg). The study was submitted to and approved in 2016 by the daily Boards MEC-U and the Medical Ethics Committee of Leiden University Medical Center (LUMC, 2016). As a result of these reviews, the boards declared that the rules laid down in the Medical Research Involving Human Subjects Act (also known by its Dutch abbreviation WMO) do not apply to the study. No additional approval was requested for the current study since it is not based upon a clinical study or patient data. All participants gave digital-informed consent to use the data for analyses. All data were anonymously processed. Participants were able to resign at any time, without any statement of reasons.
Acknowledgments
The authors wish to thank all participating obstetric professionals of the following ten hospitals: OLVG Amsterdam, Leiden University Medical Center, Leiden, Amphia hospital Breda, Elisabeth Tweesteden hospital Tilburg, Jeroen Bosch hospital ‘s Hertogenbosch, Ziekenhuisgroep Twente (ZGT) Almelo- Hengelo, Tjongerschans hospital Heerenveen, Erasmus Medical Center Rotterdam, Albert Schweitzer hospital Dordrecht and Amstelland hospital Amstelveen. The authors also wish to thank Ageeth N. Rosman (PhD), Doug J. Cronie (PhD), Nicole Y.C. Steemers (MD), Lisette van Hulst for feedback and editing assistance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation. And took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Author BE has a personal grant for teachers, Netherlands Organization for Scientific Research (NWO) Award number 023.009.030.
Disclosure
The authors declare that they have no competing interests.
References
1. Poeran J, Borsboom GJ, de Graaf JP, et al. Does centralisation of acute obstetric care reduce intrapartum and first-week mortality? An empirical study of over 1 million births in the Netherlands. Health Policy (New York). 2014;117(1):28–38. doi:10.1016/j.healthpol.2014.03.009
2. Wiegers TA, Borst JD. Organization of Emergency Care in Obstetric Care. Utrecht: NIVEL; 2010.
3. Bailey CM, Newton JM, Hall HG. Telephone triage in midwifery practice: a cross-sectional survey. Int J Nurs Stud. 2019;91:110–118. doi:10.1016/j.ijnurstu.2018.11.009
4. van Ierland Y, van Veen M, Huibers L, Giesen P, Moll HA. Validity of telephone and physical triage in emergency care: the Netherlands Triage System. Fam Pract. 2011;28(3):334–341. doi:10.1093/fampra/cmq097
5. Gratton RJ, Bazaracai N, Cameron I, et al. Acuity assessment in obstetrical triage. J Obstet Gynaecol Can. 2016;38(2):125–133. doi:10.1016/j.jogc.2015.12.010
6. Huibers L, Giesen P, Wensing M, Grol R. Out-of-hours care in western countries: assessment of different organizational models. BMC Health Serv Res. 2009;9:105.
7. Veit-Rubin N, Brossard P, Gayet-Ageron A, et al. Validation of an emergency triage scale for obstetrics and gynaecology: a prospective study. BJOG. 2017;124(12):1867–1873. doi:10.1111/1471-0528.14535
8. Thijsse E, Caluwe R, van der Velden IHM. Attention for obstetric triage. Dutch Midwifery J. 2007;32:28–29.
9. Engeltjes B, Dahrs H, van der Noll M, Rijke RPC. Obstetric triage ready for implementation into obstetric practice. Med Contact (Bussum). 2014;69:1528–1530.
10. Smithson DS, Twohey R, Rice T, Watts N, Fernandes CM, Gratton RJ. Implementing an obstetric triage acuity scale: interrater reliability and patient flow analysis. Am J Obstet Gynecol. 2013;209(4):287–293. doi:10.1016/j.ajog.2013.03.031
11. Paisley KS, Wallace R, DuRant PG. The development of an obstetric triage acuity tool. MCN Am J Matern Child Nurs. 2011;36(5):290–296. doi:10.1097/NMC.0b013e318226609c
12. Ruhl C, Scheich B, Onokpise B, Bingham D. Content validity testing of the maternal fetal triage index. J Obstet Gynecol Neonatal Nurs. 2015;44(6):701–709. doi:10.1111/1552-6909.12763
13. Manning NA, Magann EF, Rhoads SJ, Ivey TL, Williams DJ. Role of telephone triage in obstetrics. Obstet Gynecol Surv. 2012;67(12):810–816. doi:10.1097/OGX.0b013e318277dd9c
14. Keeney S, Hasson F, McKenna HP. A critical review of the Delphi technique as a research methodology for nursing. Int J Nurs Stud. 2001;38(2):195–200. doi:10.1016/S0020-7489(00)00044-4
15. van Zolingen SJ, Klaassen CA. Selection processes in a Delphi study about key qualifications in senior secondary vocational education. Technol Forecast Soc Change. 2002;70:317–340. doi:10.1016/S0040-1625(02)00202-0
16. Wester F, Peters V. Qualitative Analyzes. Coutinho; 2004.
17. Boeije H. Analysis in Qualitative Research. Sage Publications Ltd; 2009.
18. Hasson F, Keeney S, McKenna H. Research guidelines for the Delphi survey technique. J Adv Nurs. 2000;32(4):1008–1015.
19. Carr D, Howells A, Chang M, Hirji N, English A. An integrated approach to stakeholder engagement. Healthc Q. 2009;12(sp):62–70. doi:10.12927/hcq.2009.20754
20. Coiera E. Four rules for the reinvention of health care. BMJ. 2004;328(7449):1197–1199. doi:10.1136/bmj.328.7449.1197
21. Vansteenkiste M, Simons J, Lens W, Sheldon KM, Deci EL. Motivating learning, performance, and persistence: the synergistic effects of intrinsic goal contents and autonomy-supportive contexts. J Pers Soc Psychol. 2004;87(2):246–260. doi:10.1037/0022-3514.87.2.246
22. Zachariasse JM, Seiger N, Rood PP, et al. Validity of the Manchester Triage System in emergency care: a prospective observational study. PLoS One. 2017;12(2):e0170811. doi:10.1371/journal.pone.0170811
23. Moth G, Huibers L, Christensen MB, Vedsted P. Out-of-hours primary care: a population-based study of the diagnostic scope of telephone contacts. Fam Pract. 2016;33(5):504–509. doi:10.1093/fampra/cmw048
24. Nordhaug M, Nortvedt P. Justice and proximity: problems for an ethics of care. Health Care Anal. 2011;19(1):3–14. doi:10.1007/s10728-010-0159-3
25. Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn’t. 1996. Clin Orthop Relat Res. 2007;455:3–5.
26. Rew L, Barrow EM. State of the science: intuition in nursing, a generation of studying the phenomenon. ANS Adv Nurs Sci. 2007;30(1):E15–25. doi:10.1097/00012272-200701000-00011
27. Stolper E, Van de Wiel M, Van Royen P, Van Bokhoven M, Van der Weijden T, Dinant GJ. Gut feelings as a third track in general practitioners’ diagnostic reasoning. J Gen Intern Med. 2011;26(2):197–203. doi:10.1007/s11606-010-1524-5
28. van Veen M, Steyerberg EW, Ruige M, et al. Manchester triage system in paediatric emergency care: prospective observational study. BMJ. 2008;337:a1501. doi:10.1136/bmj.a1501
29. Moll HA. Challenges in the validation of triage systems at emergency departments. J Clin Epidemiol. 2010;63(4):384–388. doi:10.1016/j.jclinepi.2009.07.009
30. Seiger N, van Veen M, Almeida H, et al. Improving the Manchester Triage System for pediatric emergency care: an international multicenter study. PLoS One. 2014;9(1):e83267. doi:10.1371/journal.pone.0083267
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.