Back to Journals » Drug Design, Development and Therapy » Volume 19
Obinutuzumab is Effective as an Initial Treatment for PLA2R-Associated Primary Membranous Nephropathy: A Retrospective, Single-Center Trial
Authors Li XQ, Liu Y, Cai ZY, Lv TG, Hao J
Received 13 March 2025
Accepted for publication 1 July 2025
Published 11 July 2025 Volume 2025:19 Pages 5961—5972
DOI https://doi.org/10.2147/DDDT.S527661
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Tuo Deng
Xue-Qi Li,1 Yang Liu,1 Ze-Yu Cai,1 Tie-Gang Lv,2 Jian Hao1
1Department of Medicine, Division of Nephrology, The Affiliated Hospital of Inner Mongolia Medical University, Hohhot, Inner Mongolia Autonomous Region, 010050, China; 2Department of Medicine, Division of Radiology, The Affiliated Hospital of Inner Mongolia Medical University, Hohhot, Inner Mongolia Autonomous Region, 010050, People’s Republic of China
Correspondence: Jian Hao, Department of Medicine, Division of Nephrology, The Affiliated Hospital of Inner Mongolia Medical University, No. 1 North Passage Road, Huimin District, Hohhot, Inner Mongolia Autonomous Region, 010050, People’s Republic of China, Tel +8613704751021, Email [email protected]
Background: Membranous nephropathy (MN) can cause nephrotic syndrome. B cells contribute to MN, but available treatments are often inadequate. We addressed this treatment gap by analyzing the effect of obinutuzumab in patients with primary MN (PMN).
Methods: Forty-seven PMN patients were followed for six months, with 25 receiving obinutuzumab and 22 (control) receiving rituximab. Treatment response was assessed by 24-h urine total protein (24-h UTP), serum albumin (ALB), and other indicators. Immunologic remission was assessed by measurement of anti-phospholipase A2 receptor autoantibodies (PLA2R autoAbs).
Results: Relative to baseline, the obinutuzumab group had significant decreases of PLA2R autoAbs (83.40 [55.90– 344.36] vs 0.41 [0.17– 1.20] RU/mL), 24-h UTP (8.90 [7.15– 13.80) vs 1.82 [1.12– 3.43] g/day), and B cells (312.61 [202.00– 406.12) vs 0 [0– 0] cells/μL), and a significant increase of serum ALB (25.90 [20.85– 28.70] vs 42 [39.7– 45.3] g/L) after six months. Nineteen of the evaluable patients (76% [55– 91%]) achieved immunological remission at three months, 20 (80% [60– 93%] achieved immunological remission at six months, and 16 (64% [42– 83%] achieved partial response (PR) at three-months. After six-months, no patients achieved complete remission, but 19 (76% [55– 91%]) achieved PR. Before the second dose of obinutuzumab, the CD19+ B cell count in 20 patients (80%) [60%– 93%] was less than 1 cell/μL, and 18 patients had counts of 0 cells/μL. At the 6-month follow-up, the rituximab and obinutuzumab groups had no significant differences in immunological remission (80% vs 64%; OR: 2.29 [0.62– 8.47]; P=0.211) or clinical remission (76% vs 59%; OR: 2.19 [0.63– 7.66]; P=0.215]. No patients experienced serious adverse events.
Conclusion: This retrospective analysis suggests that obinutuzumab may have potential as an initial therapeutic option for patients with PMN, although larger controlled studies are needed for confirmation.
Keywords: obinutuzumab, PLA2R, membranous nephropathy, proteinuria
Introduction
Membranous nephropathy (MN) is one of the most common causes of nephrotic syndrome in China and elsewhere. Although kidney biopsy results are considered the gold standard for diagnosis of MN, positivity for phospholipase A2 receptor (PLA2R) autoantibodies (autoAbs) in serum samples is considered a specific marker of primary MN (PMN).1–3 Because B cells produce these autoAbs, there is a pathophysiological rationale for using treatments that target B cell lineages to prevent the production and deposition of these autoAbs. AutoAbs against other proteins also contribute to the pathogenesis of MN. Most patients with PMN have antibodies against a conformation-dependent epitope in PLA2R. PLA2R only occurs at low levels in normal podocytes, but occurs at high levels in the immune deposits of patients with PMN, indicating that PLA2R contributes to the pathogenesis of MN.3–6
The treatment of MN primarily relies on targeting of B cell lymphocytes by immunosuppressants,1,7 and anti-CD20 monoclonal antibodies are of particular interest due to their mechanisms of action. Based on their functional characteristics, therapeutic anti-CD20 monoclonal antibodies can be classified as Type I or Type II. Type I antibodies (eg, rituximab, ofatumumab) eliminate B cells through potent complement-dependent cytotoxicity (CDC) and clustering of lipid rafts, but only lead to a weak induction of apoptosis. In contrast, Type II antibodies (eg, obinutuzumab, tositumomab) have robust and direct effects on apoptosis and homotypic cell aggregation, weak CDC activity, but more comprehensive depletion of B cells. Although both types of antibodies have comparable efficacy in terms of antibody-dependent cellular cytotoxicity (ADCC), clinical studies suggest that obinutuzumab may provide better B cell clearance than rituximab and ofatumumab.8–10 Notably, recent randomized controlled trials (RCTs) of patients with MN reported that rituximab was superior to cyclosporine and led to fewer adverse effects.11 Despite the effectiveness of rituximab in many MN patients, over one-third of these patients may experience treatment failure, and management of these unresponsive patients is a significant challenge. Type II antibodies are a potential strategy to address this challenge.12,13 The functional differences of these two types of therapeutic antibodies primarily stem from distinct epitope recognition rather than antibody affinity or isotype, providing a theoretical basis for precision therapy in MN. Recent studies showed that obinutuzumab may be more effective in the depletion of B cells than rituximab and ofatumumab.7
Several studies have documented better responses to obinutuzumab than rituximab in patients with certain B cell malignancies (follicular lymphoma and chronic lymphocytic leukemia).14–16 There is also evidence that obinutuzumab is effective for treatment of patients with MN. Ongoing randomized controlled trials are investigating the effect of obinutuzumab in adults with MN.3,17
Based on evidence from previous case series that examined the effect of obinutuzumab as a rescue therapy for MN, we examined the effect of this mAb as an initial treatment for MN. More specifically, we analyzed the efficacy and safety of obinutuzumab by performing a retrospective analysis of PMN patients from Northern China, 25 of whom received obinutuzumab and 22 of whom received rituximab.
Methods
Study Cohort and Ethical Approval
This hospital-based retrospective observational descriptive study analyzed 47 patients with PMN at the First Affiliated Hospital of Inner Mongolia Medical University (Hohhot) from January 2023 to December 2024 (Figure 1). All patients received obinutuzumab or rituximab therapy at least twice during hospitalization. Twenty-five patients (53%) received obinutuzumab as an initial treatment; 22 other patients (47%) received rituximab as an initial treatment, but 2 of them switched to obinutuzumab because of rituximab resistance. All patients were followed for at least six months. The follow-up time was defined as the time from the first dose of the treatment drug to the date of visit.
 |
Figure 1 Patient disposition. |
The inclusion criteria were age of 18 to 80 years; diagnosis of PMN by a PLA2R autoAb test; estimated glomerular filtration rate (eGFR) of at least 30 mL/min/1.73 m2 based on the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula; and receipt of infusional obinutuzumab or rituximab. The exclusion criteria were receipt of dialysis, negative results for the anti-PLA2R autoAb (<2 RU/mL),14 use of other immunosuppressants, inadequate follow-up, and another major illness that may affect the accuracy of the PLA2R autoAb test. These other illnesses included any malignancy, acute infection, autoimmune disease, rapidly progressive glomerulonephritis, and severe kidney impairment (eGFR < 30 mL/min/1.73 m2 or need for kidney transplant).
Clinical data from all patients were recorded before receipt of obinutuzumab or rituximab and during follow-ups after drug initiation. Obinutuzumab was diluted in 1000 mL normal saline. The dose of the initial infusion was 1000 mg, and the time from the first to second infusion was typically 2 to 3 weeks. Each infusion was administered at 50 mg/h during the first 2 h, and then at 100 mg/h during the following 9 h. Before each infusion, 5 mg of intravenous dexamethasone sodium phosphate with 12.5 mg of intramuscular promethazine hydrochloride was administered to minimize infusion-related adverse reactions. Rituximab was administered using the same methods. In addition, nine patients who received obinutuzumab received infusions of human serum albumin (ALB) to correct very low serum levels.
The Ethics Review Committee of our institution provided ethical approval for this study (approval ID: ID-KY2025022) and each patient signed a written informed consent document prior to receipt of the treatment drug. This retrospective analysis was performed in accordance with the Declaration of Helsinki, and all procedures were in accordance with relevant guidelines and regulations.
Data Collection
The basic information and laboratory data of all patients were collected from the hospital information system and supplementary records. This basic information included age, sex, systolic blood pressure (SBP), diastolic blood pressure (DBP), presence of hypertension, and presence of diabetes. The laboratory indices included serum PLA2R autoAb, 24-h urine total protein (24-h UTP), serum ALB, serum total protein (TP), hemoglobin (Hb), CD19+ B cell count, serum creatinine (Scr), eGFR, urea nitrogen (BUN), uric acid (UA), total cholesterol (TC), triglycerides (TG), low density lipoprotein (LDL), high density lipoprotein (HDL), and serum IgG. The PLA2R autoAb level was measured using a chemiluminescence immunoassay (ELISA, Biomerieux, France) at baseline (before treatment) and at 1, 3, and 6 months after onset of treatment. Immunologic remission was defined as a decrease of the serum PLA2R autoAb titer to below 2 RU/mL. Clinical remission (CR) included complete clinical remission (CCR) and partial clinical remission (PCR). CCR was defined as a reduction in the 24-h UTP to below 0.3 g/day, normal serum albumin, and stable kidney function. PCR was defined as decrease of 50% or more in the 24-h UTP relative to baseline, a 24-h UTP below 3.5 g/day, improvement or normalization of serum albumin, and stable kidney function.
Statistical Analysis
Categorical variables are expressed as count and percentage. Continuous variables are expressed as mean (standard deviation, SD) if they had normal distributions and median (interquartile range, IQR) if they had non-normal distributions. Data analyses were performed using SPSS Statistics version 26 (IBM) and GraphPad Prism version 10.2 (GraphPad Software). For comparisons of values before and after treatment, the independent two-sample t-test was used for continuous variables that had normal distributions, and the paired-samples Wilcoxon or Mann–Whitney test was used for continuous variables that had non-normal distributions. The significance of changes over time was analyzed using analysis of variance (ANOVA). Kaplan-Meier curves were used to present the probability of achieving remission based on PLA2R autoAb and 24-h UTP. Multivariable-adjusted Cox regression analysis was conducted to evaluate the association between age, sex, Scr, eGFR, ALB, hypertension and diabetes with final remission outcomes (data not shown). A two-sided P value below 0.05 was considered significant. All figures were generated using GraphPad Prism.
Results
Baseline Characteristics of PMN Patients Who Received Obinutuzumab or Rituximab (Control)
We included 47 patients with PMN in this study. A total of 25 patients received obinutuzumab as an initial treatment and 22 received rituximab (control) at our center between January 2023 and December 2024 (Table 1). The median (IQR) age was 51 years (40.50–64) in the obinutuzumab group and 63 years (55–69) in the rituximab group (P = 0.059). The two groups had no statistically significant differences in sex, baseline SBP, DBP, hypertension, and diabetes (all P > 0.05). Meanwhile, analysis of the laboratory data also indicated the two groups had no significant differences in Hb, BUN, eGFR, ALB, uric acid, CHO, TG, LDL, HDL, IgG, 24-h UTP, CD19+ B cell count, and, PLA2R antibody titer (all P > 0.05).
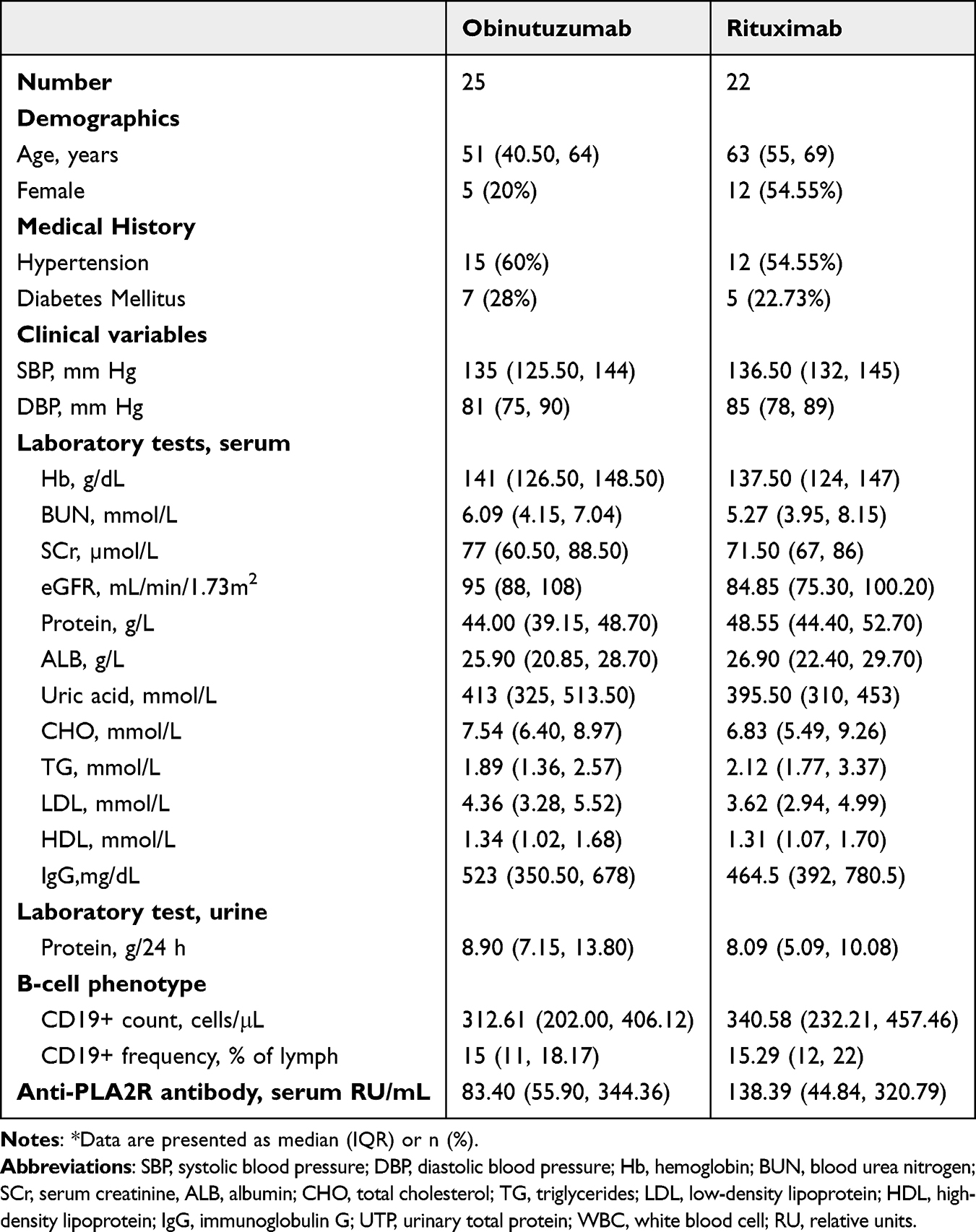 |
Table 1 Clinical Characteristics of PMN Patients Included in This Study* |
Timing of Response to Obinutuzumab
We assessed the timing of the response to obinutuzumab by analysis of clinical data recorded at baseline, and at the one month, three-month, and six-month follow-ups (Figure 2). Compared to baseline, the PLA2R autoAb titer, B-cell count, and 24-h UTP were significantly lower at one month, three months, and six months (all P < 0.001); the eGFR was significantly greater at three months and six months (P < 0.05); the serum ALB and LDL were significantly greater at one month, three months and six months (all P < 0.001). Thus, these patients experienced a rapid clinical improvement after receipt of obinutuzumab.
 |
Figure 2 Levels of PLA2R autoAb (A), C19+ B cells (B), 24-h UTP (C), eGFR (D), serum ALB (E), and LDL (F) before and after administration of obinutuzumab. Each value indicates mean ±SD. *P<0.05, ***P<0.001, ****P<0.0001, ns: not significant. |
Further analysis (data not shown) demonstrated that approximately 80% of the obinutuzumab patients achieved immunologic remission with no rebound of the serum PLA2R autoAb titer and had no need for additional treatment. The depletion of B cells was especially notable At day 20, the median circulating B cell count was 0 cells/μL (0% of all lymphocytes); 18 patients had no detectable peripheral B cells; and the other five patients had an average B cell count of 1.20 cells/μL (0.31% of all lymphocytes). The effect of obinutuzumab on durable depletion of peripheral B cells appeared to be greatest in patients with higher baseline levels of 24-h UTP, serum PLA2RAb titer, and B cell count.
Obinutuzumab vs Rituximab
We then compared changes in the levels of PLA2R autoAb, 24-h UTP, CD19+ B cell count, ALB, eGFR, and LDL between the obinutuzumab and rituximab groups (Figure 3). Overall, both groups had rapid declines in the PLA2R autoAb titer after treatment initiation. However, at follow-up periods of 1-month and 3-months, patients in the obinutuzumab group had slightly lower levels, although there was no rebound in either group. Patients receiving obinutuzumab had a continuous and sustained decline of the CD19+ B cell count, but patients in the rituximab had a slight rebound in this variable at the 3-month follow-up. The levels of eGFR and ALB were greater in the obinutuzumab group (both P < 0.05) and the LDL level was lower in the obinutuzumab group at the 1-month follow-up (P < 0.05), although the two groups had similar LDL levels at the 3-month and 6-month follow-ups.
 |
Figure 3 Levels of PLA2R autoAb (A), C19+ B cells (B), 24-h UTP (C), eGFR (D), serum ALB (E), and LDL (F) in patients who received rituximab (n = 22) or obinutuzumab (n = 25). *P<0.05. |
We also compared clinical and immunological remission in the two groups (Figure 4). At the 6-month follow-up, 20 patients in the obinutuzumab group (80% [95% CI: 60–93%]) and 14 patients in the rituximab group (64% [95% CI: 42–83%]), achieved immunologic remission, with no significant difference (OR: 2.29 [95% CI: 0.62–8.47]; P = 0.211). Also at the 6-month follow-up, 19 patients in the obinutuzumab group (76% [95% CI: 55–91%]) and 13 patients in the rituximab group (59% [95% CI: 36–79%]) achieved clinical remission, with no significant difference (OR: 2.19 [95% CI: 0.63–7.66; P = 0.215).
 |
Figure 4 Kaplan Meier analysis of clinical remission (A) and immunological remission (B) in patients who received rituximab or obinutuzumab. Clinical remission included complete clinical remission and partial clinical remission. |
Obinutuzumab in Patients with Rituximab-Resistant PMN
Two patients who received two initial treatments with rituximab (infusion at 25 mL/h for the first hour, with a progressive increase every 30 min to a maximum of 400 mg/h) with 5 mg of IV dexamethasone sodium phosphate and 12.5 mg of IM promethazine hydrochloride to minimize infusion-related reactions (as in the obinutuzumab infusion regimen). However, these two patients experienced rituximab resistance, defined as failure to achieve CR or PR based on the presence of proteinuria at least six months after the last dose (Figure 5). At the time of admission, each patient had a PLA2R autoAb titer above 300.00 RU/mL, a 24-h UTP of approximately 10 g/day, serum ALB below 30 g/dL, and average number of B cells of 213/μL (10% of all lymphocytes).
 |
Figure 5 Clinical course of PMN in two patients: patient A (A) and patient B (B) who initially received rituximab, developed rituximab resistance, and then switched to obinutuzumab. |
Patient A was a 78-year-old male. The laboratory markers in this patient improved after the beginning of rituximab treatment, but they subsequently deteriorated (Figure 5A). This patient initiated obinutuzumab treatment when the PLA2R autoAb titer was 37.97 RU/mL, the 24-h UTP was 20.40 g/day, and the B cell count was 44.85 cells/μL (3.98% of all lymphocytes). This patient received two doses of obinutuzumab over a 6-month period. At the final follow-up (1 month after the last dose of obinutuzumab), the PLA2R autoAb titer was 3.52 RU/mL, the 24-h UTP was 3.60 g/day, and the B cell count was 0 cells/µL (0% of all lymphocytes).
Patient B was a 70-year-old male. The laboratory markers in this patient improved somewhat after the beginning of rituximab treatment, but remained elevated (Figure 5B). In particular, the PLA2R autoAb titer decreased from 461.83 to 57.40 RU/mL, the 24-h UTP decreased from 10.08 to 5.38 g/day, and the B cell count increased from 0 cells/μL (0% of all lymphocytes) to 3 cells/µL (1% of all lymphocytes). This patient therefore initiated obinutuzumab because of the persistently elevated 24 h UTP and PLA2R autoAb titer. After three months, the PLA2R autoAb titer was 11.93 RU/mL, the 24-h UTP was 1.19 g/day, and the B cell count was 0 cells/µL (0% of all lymphocytes).
Thus, both patients who had rituximab-resistant PMN achieved immunologic remission and PR after obinutuzumab therapy.
Discussion
This study describes 47 patients with PLA2R-associated PMN, with 25 patients receiving obinutuzumab as an initial treatment and 22 patients receiving rituximab (control). Previous case reports found that obinutuzumab had promising efficacy in treating patients with complex, refractory MN, such as IgG4-associated MN, semaphorin 3b-associated MN, and MN accompanied by severe chronic kidney disease.18–21 Clinical trials during the previous decade showed that rituximab was effective for patients with PLA2R-associated MN, and this led to its use as first-line therapy.11,21,22 Rituximab is a chimeric mAb that has an immunoglobulin variable region and a human immunoglobulin G1 heavy chain. It is a type I mAb that binds to the CD20 antigen of B cells during maturation, but not precursor cells. Rituximab typically decreases the level of B cells after about six months, and affects memory B cells for more than 1 year. Rituximab increases complement-dependent cytotoxicity (CDC) by clustering CD20 within lipid rafts, leading to antibody-dependent cell-mediated cytotoxicity (ADCC).23,24
Obinutuzumab is also a humanized type II mAb that binds to the CD20 antigen of B cells. However, obinutuzumab was designed to bind an overlapping epitope of CD20 in a different orientation, thus preventing internalization of the CD20 antibody complex. Obinutuzumab is also glycosylated, and this increases its affinity for the FcgRIII (CD16) antigen on B cells. Compared with rituximab, obinutuzumab has an increased affinity for effector cells, greater antibody-dependent cell cytotoxicity, and its effect is less dependent on CDC. Obinutuzumab thus elicits a stronger apoptotic response in B cells and increased lysosome-mediated cytotoxicity. It is less dependent on high levels of the B cell activating factor (BAF) than rituximab, and therefore leads to a greater depletion of memory B cells, which have more resistance to rituximab.15,17,25,26
Our study of 25 patients who received obinutuzumab as an initial treatment for PMN indicated significant responses after one month. At that time, the average serum PLA2R autoAb titer was 9.41 RU/mL, seven patients achieved immunologic remission (<2 RU/mL), and 2 patients had an autoAb titer of 0 RU/mL. Also after 1 month, the average 24-h UTP was 4.43 g/day; nine patients (36%) [95% CI:18–57%] achieved PR; the B cell count was 0 cells/μL in 18 patients and was greatly reduced in the other patients; and the average serum ALB level was 34.15 g/L and 8 patients had levels above 35 g/L.
At the three month follow-up, the average serum PLA2R autoAb titer was 2.35 RU/mL, 19 patients achieved immunologic remission (<2 RU/mL), and four patients had titers of 0 RU/mL. Although 16 patients (64%) [95% CI:42–83%] achieved PR, the 24-h UTP of six patients increased slightly. The B cell count increased in three patients (1.26, 0.31, and 0.56 cells/μL), and was 0 cells/µL or unchanged in the other patients. The average serum ALB level at this time was 38.44 g/L and 20 patients had levels above 35 g/L.
At the 6-month follow-up, the average serum PLA2R autoAb titer was 0.62 RU/mL; 20 patients achieved immunologic remission (<2 RU/mL); and 1 patient had a titer of 0 RU/mL. The patients who did not achieve immunologic remission nonetheless had improved clinical data. The average 24-h UTP was 2.15 g/day, PR was achieved in 19 (76%) [95% CI:55–91%]patients, the average serum ALB was 42.43 g/L and was greater than 35 g/L in 24 patients, and the average B cell count remained low.
Our results thus provide a rationale for using obinutuzumab as a treatment for PLA2R-associated PMN. First, most of the patients who received obinutuzumab as an initial treatment achieved immunologic remission and most also achieved PR. The 2 patients who switched to obinutuzumab due to rituximab resistance also achieved immunologic remission or PR, and obinutuzumab had better effectiveness than rituximab.
Second, obinutuzumab led to the depletion of B cells in all patients. After one month, the median B cell count was below 1 cell/μL, after three months the median B-cell count of 20 patients (80%) was 0 cells/μL, and the B cell count remained low thereafter.
Third, compared to rituximab, obinutuzumab led to significantly better improvements of eGFR and ALB, and superior maintenance of long-term effectiveness. Although no statistically significant differences were observed between the two treatments regarding PLA2R autoAbs, 24-h UTP, CD19+ B-cells, and LDL, the figures indicate that obinutuzumab was at least as effective as rituximab. In addition, two patients who received rituximab initially experienced a favorable response but eventually developed rituximab-resistance. For these two patients, obinutuzumab appeared to be a suitable alternative. Other observational studies found that a rapid response was associated with a favorable long-term kidney outcome.12,13,23
Fourth, none of our 25 patients experienced infusion-related reactions, and the kidney vein thrombosis of two patients who received rituximab resolved after administration of obinutuzumab. Previous clinical trials of rituximab reported that some patients developed infections, neutropenia, lupus nephritis, and heart problems.5,13,27 In contrast, our study cohort, even those with rituximab resistance, exhibited good tolerance of obinutuzumab. However, the short follow-up period and small sample size are the limitations of this study, and these limit the generalizability of our results. Future long-term follow-up studies with large samples are needed.
Previous studies that examined the effect of obinutuzumab in patients with PMN reported serious and non-serious adverse events, including the need for additional hospitalization and life-threatening or organ-threatening events. Several events, including headache, tachycardia, nausea, and hypertension, were common after the first infusion.1,14 None of our patients required admission for infection or had infusion-related reactions (treatment-related adverse events that occurred within 24 h of infusion). Moreover, two of our patients who initially had kidney vein thrombosis experienced resolution of this condition after obinutuzumab infusion. We observed no serious adverse events during the study period, and obinutuzumab had a generally acceptable safety profile. Other studies also found that obinutuzumab-associated depletion of B cells was not associated with serious safety events, suggesting that obinutuzumab may be a more tolerable option for patients who cannot tolerate rituximab or other medications. However, there is limited evidence regarding the long-term safety of obinutuzumab when used as a treatment for MN. It is important to acknowledge treatment-related complications can occur as the follow-up time increases.
Conclusions
Our retrospective cohort study showed that obinutuzumab appeared to be effective and safe when used as an initial treatment for patients with PLA2R-associated PMN. In addition, PMN patients who received obinutuzumab as an initial treatment had better responses than those who initially received rituximab. Obinutuzumab therefore has potential as an initial treatment for PMN, but further large studies are needed to more directly assess its effect relative to existing therapies.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The Ethics Review Committee of First Affiliated Hospital of Inner Mongolia Medical University provided ethical approval for this study (approval ID: ID-KY2025022) and all patients signed a written informed consent document prior to receipt of obinutuzumab. This retrospective analysis was performed in accordance with the Declaration of Helsinki, and all procedures were in accordance with relevant guidelines and regulations.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (No. 82260146), Inner Mongolia Natural Science Foundation (No. 2022MS08036), the Program for Young Talents of Science and Technology in Universities of Inner Mongolia Autonomous Region (No. NJYT- 23-068), Medical and Health Science and Technology Plan of Health Commission of Inner Mongolia Autonomous Region (No. 202201253), and Inner Mongolia Medical University General program (No. YKD2021MS034 and ZY20242126).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Su X, Wu B, Tie X, et al. Obinutuzumab as initial or second-line therapy in patients with primary membranous nephropathy. Kidney Int Rep. 2024;9:2386–2398. doi:10.1016/j.ekir.2024.05.004
2. Cattran DC, Brenchley PE. Membranous nephropathy: integrating basic science into improved clinical management. Kidney Int. 2017;91:566–574. doi:10.1016/j.kint.2016.09.048
3. Klomjit N, Fervenza FC, Zand L. Successful treatment of patients with refractory PLA(2)R-associated membranous nephropathy with obinutuzumab: a report of 3 cases. Am J Kidney Dis. 2020;76:883–888. doi:10.1053/j.ajkd.2020.02.444
4. Wu F, Zhang Y, Cui W, et al. Development and validation of a discrimination model between primary PLA2R-negative membranous nephropathy and minimal change disease confirmed by renal biopsy. Sci Rep. 2021;11:18064. doi:10.1038/s41598-021-97517-8
5. Deng L, Xu G. Update on the application of monoclonal antibody therapy in primary membranous nephropathy. Drugs. 2023;83:507–530. doi:10.1007/s40265-023-01855-y
6. Beck LH, Bonegio RG, Lambeau G, et al. M-type phospholipase A2 receptor as target antigen in idiopathic membranous nephropathy. N Engl J Med. 2009;361:11–21. doi:10.1056/NEJMoa0810457
7. Furie RA, Aroca G, Cascino MD, et al. B-cell depletion with obinutuzumab for the treatment of proliferative lupus nephritis: a randomised, double-blind, placebo-controlled trial. Ann Rheum Dis. 2022;81:100–107. doi:10.1136/annrheumdis-2021-220920
8. Beers SA, Chan CH, James S, et al. Type II (tositumomab) anti-CD20 monoclonal antibody out performs type I (rituximab-like) reagents in B-cell depletion regardless of complement activation. Blood. 2008;112:4170–4177. doi:10.1182/blood-2008-04-149161
9. Beers SA, Chan CH, French RR, Cragg MS, Glennie MJ. CD20 as a target for therapeutic type I and II monoclonal antibodies. Semin Hematol. 2010;47:107–114. doi:10.1053/j.seminhematol.2010.01.001
10. Cragg MS, Glennie MJ. Antibody specificity controls in vivo effector mechanisms of anti-CD20 reagents. Blood. 2004;103:2738–2743. doi:10.1182/blood-2003-06-2031
11. Fervenza FC, Appel GB, Barbour SJ, et al. Rituximab or cyclosporine in the treatment of membranous nephropathy. N Engl J Med. 2019;381:36–46. doi:10.1056/NEJMoa1814427
12. Freeman CL, Sehn LH. A tale of two antibodies: obinutuzumab versus rituximab. Br J Haematol. 2018;182:29–45. doi:10.1111/bjh.15232
13. Hu X, Zhang M, Xu J, et al. Comparison of obinutuzumab and rituximab for treating primary membranous nephropathy. Clin J Am Soc Nephrol. 2024;19:1594–1602. doi:10.2215/CJN.0000000000000555
14. Lin Y, Han Q, Chen L, et al. Obinutuzumab in refractory membranous nephropathy: a case series. Kidney Med. 2024;6:100853. doi:10.1016/j.xkme.2024.100853
15. Sethi S, Kumar S, Lim K, Jordan SC. Obinutuzumab is effective for the treatment of refractory membranous nephropathy. Kidney Int Rep. 2020;5:1515–1518. doi:10.1016/j.ekir.2020.06.030
16. Hudson R, Rawlings C, Mon SY, Jefferis J, John GT. Treatment resistant M-type phospholipase A2 receptor associated membranous nephropathy responds to obinutuzumab: a report of two cases. BMC Nephrol. 2022;23:134. doi:10.1186/s12882-022-02761-3
17. Hao J, Wang J, Zhou P, Xu R, Chen X. Obinutuzumab in untreated primary membranous nephropathy: an observational case series. Nephrology (Carlton). 2024;29:709–716. doi:10.1111/nep.14331
18. Conversano E, Debiec H, Colucci M, Emma F, Ronco P, Vivarelli M. A child with semaphorin 3b-associated membranous nephropathy effectively treated with obinutuzumab after rituximab resistance. Pediatr Nephrol. 2024;39:305–308. doi:10.1007/s00467-023-06085-8
19. Ginthör NE, Artinger K, Pollheimer MJ, Stradner MH, Eller K. Membranous nephropathy associated with immunoglobulin G4-related disease successfully treated with obinutuzumab. Clin Kidney J. 2022;15:564–566. doi:10.1093/ckj/sfab250
20. Naik S, Shukla S, Av N, et al. Obinutuzumab in refractory phospholipase A2 receptor-associated membranous nephropathy with severe CKD. Kidney Int Rep. 2023;8:942–943. doi:10.1016/j.ekir.2023.01.035
21. Ramachandran R, Prabakaran R, Priya G, et al. Immunosuppressive therapy in primary membranous nephropathy with compromised renal function. Nephron. 2022;146:138–145. doi:10.1159/000518609
22. Keri KC, Blumenthal S, Kulkarni V, Beck L, Chongkrairatanakul T. Primary membranous nephropathy: comprehensive review and historical perspective. Postgrad Med J. 2019;95:23–31. doi:10.1136/postgradmedj-2018-135729
23. Basu B, Angeletti A, Islam B, Ghiggeri GM. New and old anti-CD20 monoclonal antibodies for nephrotic syndrome. Where we are? Front Immunol. 2022;13:805697. doi:10.3389/fimmu.2022.805697
24. Lundberg S, Westergren E, Smolander J, Bruchfeld A. B cell-depleting therapy with rituximab or ofatumumab in immunoglobulin A nephropathy or vasculitis with nephritis. Clin Kidney J. 2017;10:20–26. doi:10.1093/ckj/sfw106
25. Edelmann J, Dokal AD, Vilventhraraja E, et al. Rituximab and obinutuzumab differentially hijack the B cell receptor and NOTCH1 signaling pathways. iScience. 2021;24:102089. doi:10.1016/j.isci.2021.102089
26. Reddy V, Klein C, Isenberg DA, et al. Obinutuzumab induces superior B-cell cytotoxicity to rituximab in rheumatoid arthritis and systemic lupus erythematosus patient samples. Rheumatology. 2017;56:1227–1237. doi:10.1093/rheumatology/kex067
27. Zhang Y, Sun J, Gao J, et al. Case report: one case of refractory membranous nephropathy with hypokalemia after rituximab infusion was switched to obinutuzumab without recurrence of hypokalemia. Front Pharmacol. 2024;15:1347880. doi:10.3389/fphar.2024.1347880
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.