Back to Journals » Patient Preference and Adherence » Volume 19
Obesity Medication Treatment Perspectives Among People with Overweight or Obesity
Authors Ostrominski JW, Chhibber A, Kuti EL, Clark B ![]() , Donato BM
, Donato BM ![]()
Received 30 July 2025
Accepted for publication 4 September 2025
Published 13 September 2025 Volume 2025:19 Pages 2887—2899
DOI https://doi.org/10.2147/PPA.S555622
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
John W Ostrominski,1– 3 Anindit Chhibber,4 Effie L Kuti,4 Brendan Clark,4 Bonnie MK Donato4
1Division of Cardiovascular Medicine, Brigham and Women’s Hospital, Boston, MA, USA; 2Division of Endocrinology, Diabetes and Hypertension, Brigham and Women’s Hospital, Boston, MA, USA; 3Division of Cardiovascular Medicine and Obesity Medicine, Harvard Medical School, Boston, MA, USA; 4HEOR Value Demonstration, Boehringer Ingelheim Pharmaceuticals, Inc., Ridgefield, CT, USA
Correspondence: Anindit Chhibber, Boehringer Ingelheim Pharmaceuticals, Inc., 900 Ridgebury Road, Ridgefield, CT, USA, Email [email protected]
Background: Obesity is a complex, chronic condition associated with multiple health complications. While obesity medications (OMs), particularly GLP-1 receptor agonists (GLP-1RAs), have demonstrated significant clinical benefits, real-world insights into patient experiences with these therapies remain limited. This study evaluated patients’ behaviors and experiences with OMs, including their financial impact; and aimed to identify key decision points for seeking and receiving treatment with OMs.
Methods: Individuals were recruited from a national database to complete a 20-minute online survey between July 8 and July 18, 2024. Eligible participants were adults aged 21 years or older with a body mass index (BMI) of ≥ 30 kg/m2, or ≥ 27 kg/m2 with at least one obesity-related complication (ORC) and were currently using an OM. Participants reported their experiences with OMs, motivations and barriers for treatment, challenges, interactions with HCPs and financial challenges with OMs.
Results: 100 people with obesity (PwO) participated in the survey. The median age of the respondents was 46 years. Most PwO (94%) had at least one comorbidity in addition to overweight/obesity, and 58% were more concerned about obesity compared with other health conditions. Most PwO (91%) were currently using GLP-1RAs and had previously attempted a median of 3 unique weight management strategies prior to OM initiation. Primary drivers for OM initiation were long-term health improvement (58%) and functional enhancement (53%). Major barriers included insurance restrictions (38%), concerns about side effects (37%), and cost (31%). While on OMs, most (88%) PwO reported a positive experience, citing significant benefits on body weight and appetite reduction; 9% were neutral and 3% reported a negative experience. Participants with longer durations of reported treatment more often reported positive experiences (79% among those with ≥ 6 months of therapy; 51% among those with < 6 months of therapy). The study also found that 56% of PwO expected to be on their current OM for a limited period, with 20% anticipating less than a year and 28% anticipating less than two years. The anticipated treatment duration among PwO varied with reported out-of-pocket (OOP) costs. Communication with HCPs frequently addressed side effects and administration, but discussions about treatment duration and lifestyle integration were less consistent.
Conclusion: This study highlights the multifaceted experiences of PwO in managing obesity, particularly regarding OM use. The findings underscore the importance of early intervention, robust patient-provider communication, equitable access, and financial support to optimize treatment outcomes. Addressing systemic barriers, stigma, education, and access challenges will be essential to maximize the utility of obesity pharmacotherapy in clinical practice.
Keywords: obesity, obesity medications, treatment perspectives
Introduction
Obesity is a multifactorial chronic disease characterized by excess or abnormal adiposity with implications for health and well-being.1,2 According to the World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC), overweight is defined as a body mass index (BMI) of 25.0–29.9 kg/m², while obesity is defined as a BMI of ≥30.0 kg/m².3,4 In recent decades, the prevalence of obesity has increased sharply in the United States and worldwide.5,6 According to the CDC, the prevalence of obesity in the US increased from 31% in the 1999–2002 period to a striking 42% in 2017–20185,6 and is projected to reach 58% by 2035.7 Obesity is also linked to a myriad of chronic conditions, which contribute to excess morbidity and mortality. These include type 2 diabetes,8–10 cardiovascular disease,11–13 liver disease,14 chronic kidney disease,15 musculoskeletal disorders,16–18 site specific cancers,19,20 and dementia.21 Furthermore, large observational studies have shown that obesity is associated with a higher risk of premature death compared to individuals with a healthy weight.22 The increased morbidity and mortality associated with obesity have positioned its prevention and treatment as a leading public health priority. In this context, approaches to obesity treatment have evolved significantly, and now span behavioral and lifestyle interventions, highly efficacious obesity medications (OMs), and metabolic and bariatric surgery.
Given the growing body of evidence establishing their wide-ranging benefits on health outcomes and health-related quality of life, glucagon-like peptide-1 receptor agonists (GLP-1RAs) have emerged as transformative options for people with excess adiposity23–27 and related complications, including cardiovascular disease,28–30 chronic kidney disease,28–30 type 2 diabetes,31–33 and metabolic dysfunction-associated steatotic liver disease.34,35 Although the uptake of GLP-1RA-based therapies has been rapid,36 and OMs are increasingly recommended in clinical practice guidelines as part of comprehensive strategies to address important health risks in people with obesity (PwO), their adoption and utilization remains low, with only 1% of eligible patients receiving an OM.37
The practical understanding of the experiences of people taking OMs remains limited,38 and further evidence may inform shared decision-making, identify barriers to care, and uncover opportunities for practice improvement. In this contemporary survey of PwO taking OMs, we aimed to 1) evaluate patients’ behaviors and experiences with OMs, including their financial impact; and 2) identify key decision points for seeking and receiving treatment with OMs.
Methods
This was a cross-sectional, exploratory survey study conducted among PwO in the United States. PwO were recruited to complete a 20-minute online survey between July 8–18, 2024. Eligible participants were adults aged 21 years or older with a BMI of ≥30 kg/m2, or ≥27 kg/m2 with at least one obesity-related complication (ORC) and were currently using an OM. Individuals were excluded if they had participated in a clinical trial within the past 6 months, were bodybuilders or powerlifters, were pregnant, were not currently using OMs, had never used or would not consider using OMs, were covered exclusively by Medicaid or Medicare, or were aged 65 years or older without commercial insurance coverage. Sampling quotas were established (eg, mix of GLP1 users and non-users) to ensure representation from a diverse sample of US adults living with overweight or obesity. Study participants were recruited from national survey panels facilitated by HawkPartners. These panels draw respondents from multiple regions across US to ensure a nationally representative sample. The survey included questions about the patient’s health background, decisions to treat obesity, and experience with OMs and other weight loss methods, including economic burden and willingness to pay for treatment. The survey also explored the types of discussions between PwO and their healthcare professionals (HCPs) while on an OM. All responses were collected electronically through a secure survey software system and all respondents received a fair market incentive for their time.
The survey content and themes were derived from exploratory qualitative interviews conducted with a small group of PwO to understand the obesity treatment perspectives and financial impact. Prior to fielding the survey, two pre-tests were completed to refine the instrument and gather additional insights. HawkPartners designed and reviewed the survey to ensure it posed no risk to participants. Recruitment was conducted entirely online through national panels, and no direct contact with patients occurred. All participants provided consent prior to participation and participation was entirely voluntary, with respondents informed that there were no right or wrong answers and that they could choose not to participate or withdraw at any point. The data used in this study were de-identified and did not contain any identifiable protected health information (PHI). All data handling complied with the United States Department of Health and Human Services Privacy Rule requirements for de-identification, as codified at 45 C.F.R. § 164.514(b). Given that the study involved no identifiable patient data and posed minimal risk to participants, it met the criteria for exemption under federal regulations. Specifically, the research involved only the analysis of existing data and did not involve interactions with humans, as outlined in 45 C.F.R. § 46.104(d).4 Therefore, IRB review was not sought or required. Patient privacy was strictly maintained, and all procedures adhered to Health Insurance Portability and Accountability Act (HIPAA) regulations and ethical principles outlined in the Declaration of Helsinki.39
No a priori sample size calculation was conducted as this survey was designed to be hypothesis generating. The sample size was determined pragmatically, based on feasibility considerations with the aim of providing descriptive insights to inform future research. To ensure data integrity, multiple fraud countermeasures were implemented including browser fingerprinting, geolocation verification and knowledge verification checks. In addition, standard quality control procedures were implemented to exclude the responses from speeders, straight-liners, and participants providing poor-quality open-ended answers. In addition, the survey instrument was content validated by experts to ensure that the questions comprehensively and accurately captured the concepts of interest. Descriptive statistics were used to summarize survey responses: categorical variables were reported as frequencies and percentages, and continuous variables as means with standard deviations or medians with interquartile ranges.
Results
Patient Population
100 PwO participated in the survey (9% were overweight and 91% were living with obesity). The median age of the respondents was 46 [39, 57] years and most were women (57%), had self-reported white race (91%) and non-Hispanic ethnicity (84%), were employed (74%), were suburban (50%), had commercial insurance (94%), and had bachelor’s or higher level of education (53%) (Table 1). Nearly all participants were formally diagnosed with obesity (91%), with the majority being diagnosed by a primary care physician (PCP) (74%). Fewer had received a diagnosis of obesity from a weight management specialist (8%), or endocrinologist (6%) (Table 1). More than 9 in 10 (94%) had ≥1 health complication of obesity, and 58% were more concerned about obesity compared with other health conditions (Table 2). PwO also reported exploring various obesity management approaches before initiating an OM (ie, self-managed lifestyle changes, exercise plans, meal replacements, and supported lifestyle interventions); 86% had used ≥1 weight management method prior to OM treatment, with a median of 3 [1, 5] unique weight management strategies attempted prior to OM initiation. The majority of PwO were currently taking a GLP-1RA (91%) (67% semaglutide; 20% tirzepatide; and 4% liraglutide) for weight management, with 5 PwO (5%) reporting use of multiple OMs and the majority (53%) having been on their current OM for less than 6 months (Table 1).
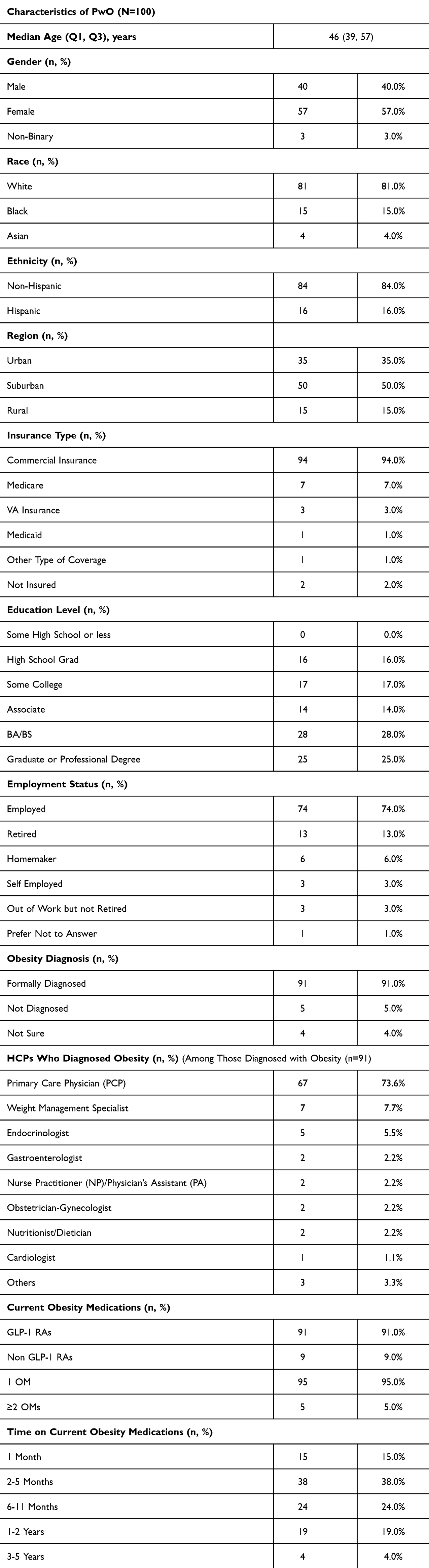 |
Table 1 Characteristics of Participants |
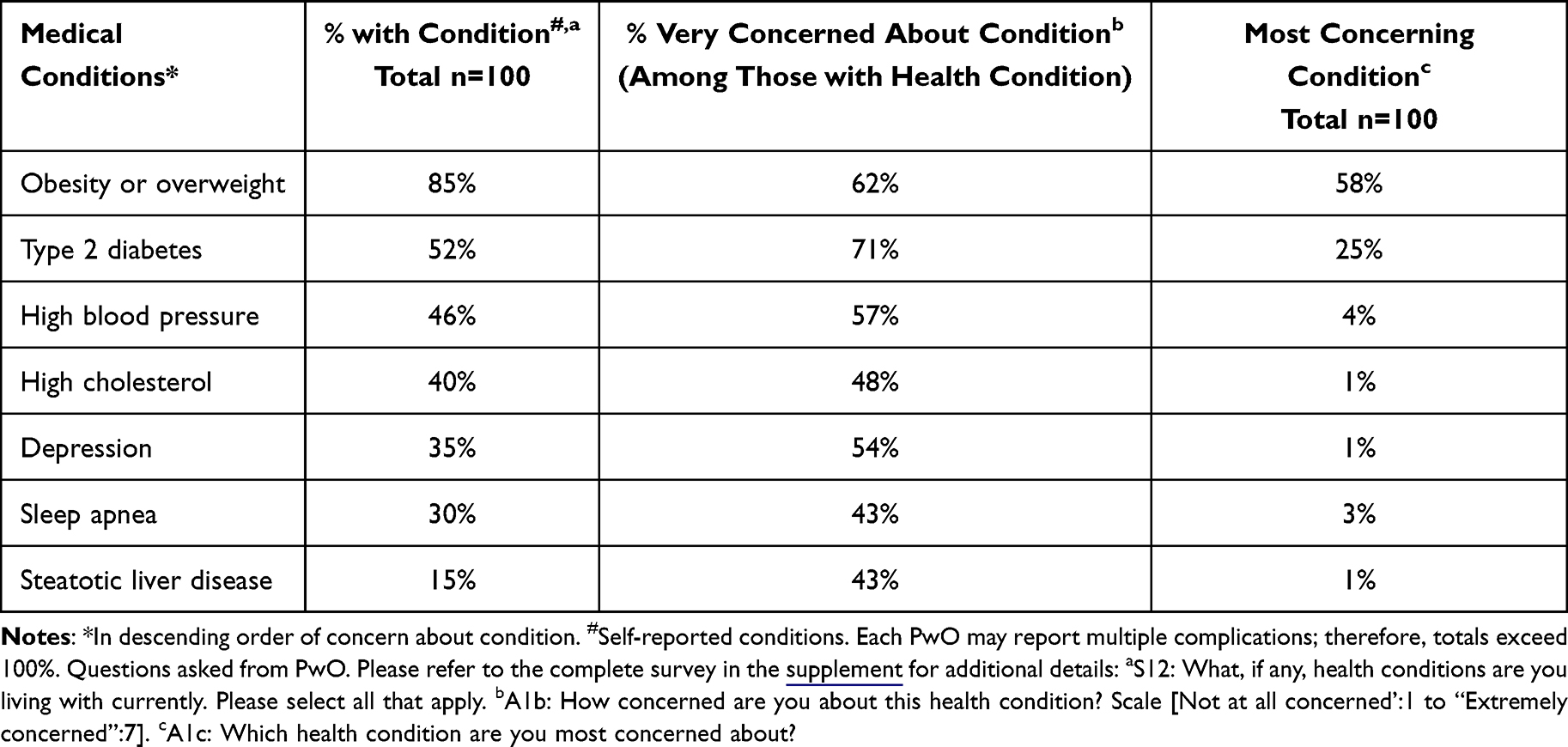 |
Table 2 Obesity and Additional Complications Among Participants |
Drivers and Barriers to Initiate OM Treatment and Key Experiences
The primary drivers for OM initiation were long-term health benefits (58%), desire to lose weight to improve activity levels (53%), and to manage other health conditions in addition to obesity (50%). Major barriers to OM treatment included insurance coverage limitations (38%), concerns about potential side effects (37%), and high costs or copays (31%) (Figure 1). While on OMs, most (88%) PwO reported a positive experience, citing significant benefits on body weight and appetite reduction; 9% were neutral and 3% reported a negative experience. Participants with longer durations of reported treatment more often reported positive experiences (79% among those with ≥6 months of therapy; 51% among those with <6 months of therapy).
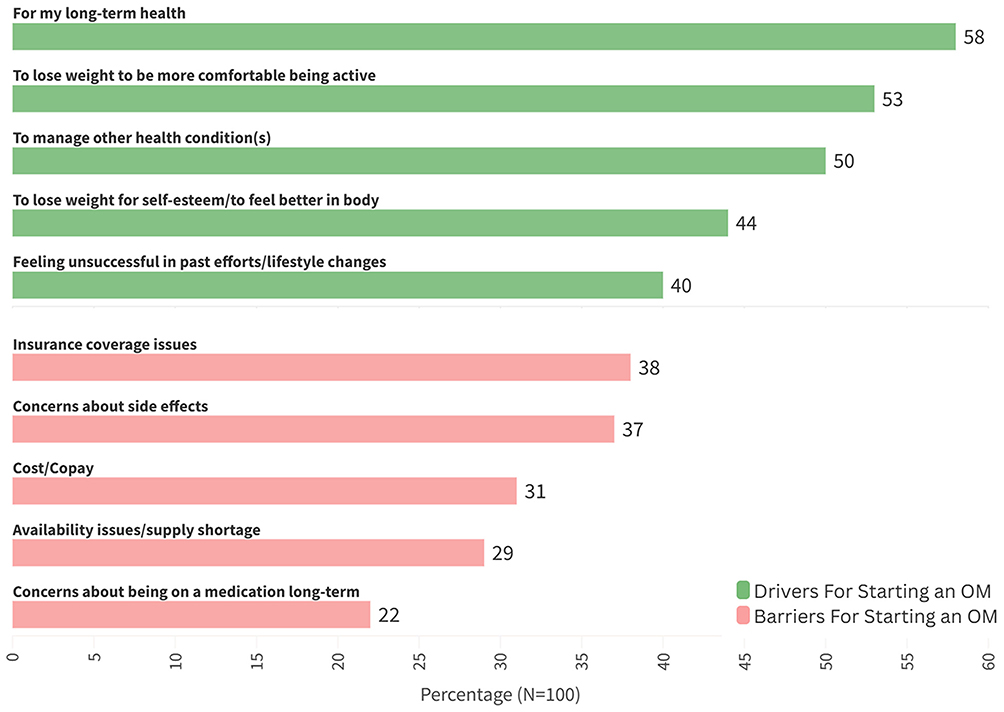 |
Figure 1 Key Drivers and Barriers for Starting an OM Among PwO. Questions asked from PwO. Please refer to the complete survey in the supplement for additional details: C8: What were the main reasons you wanted to start taking your current OM? Select all that apply. C9: What were the challenges for you before starting your current OM? Select all that apply. |
OM Discussions Between Healthcare Professionals and PwO
Results revealed alignment between HCPs and PwO on themes of side effects (HCP-initiated: 68%, PwO-initiated: 58%), long-term benefits of OMs (HCP-initiated: 58%, PwO-initiated: 37%), and medication administration (HCP-initiated: 57%, PwO-initiated: 34%). However, discussions involving concomitant lifestyle interventions appeared more commonly initiated by HCPs (HCP-initiated: 64%, PwO-initiated: 27%) (Figure 2). The study also found that 56% of PwO expect to be on their current OM for a limited period, with 20% anticipating less than a year and 28% anticipating less than two years. In addition, only 42% reported discussing anticipated treatment timelines with their HCPs, but such discussions were more common among PwO who had been taking OMs for over six months. PwO engaging in active conversations with HCPs reported less uncertainty about their treatment timeline (Among those who had discussed treatment duration with an HCP, 5% indicated they were unsure vs 40% among those who had not engaged in such discussions) (Table 3). However, even among those who discussed OM treatment timelines with their HCPs, most (64%) anticipated an OM treatment duration of ≤1-2 years.
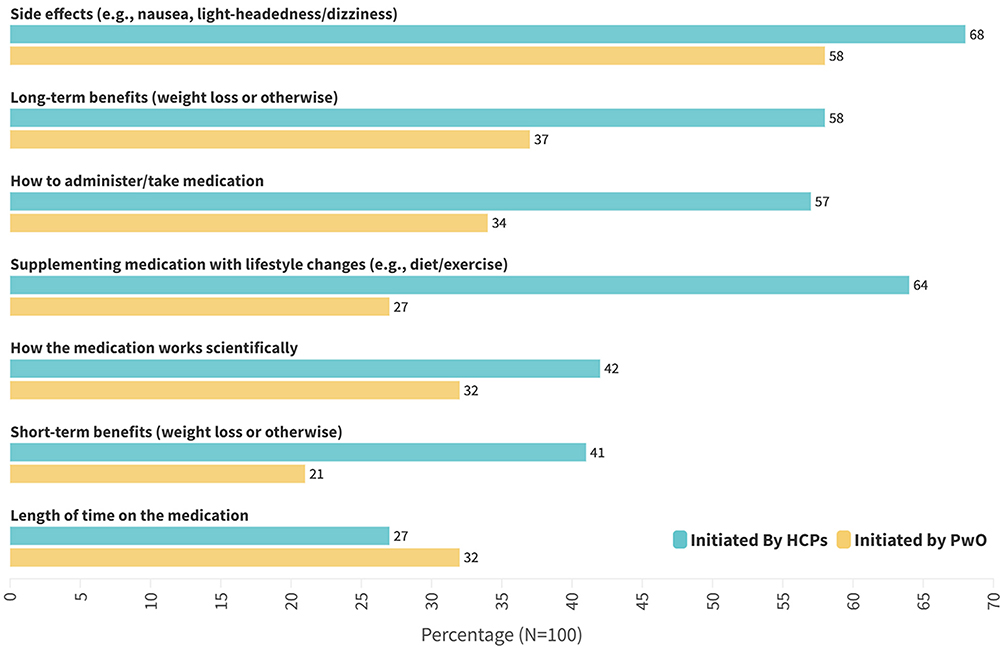 |
Figure 2 Topics of Discussion Between HCPs and PwO. Questions asked from PwO. Please refer to the complete survey in the supplement for additional details: C5: Before starting your current OM, which of the following topics did a healthcare professional discuss with you about? Select all that apply. C6: What type of questions did you ask a healthcare professional about your OM? Select all that apply. |
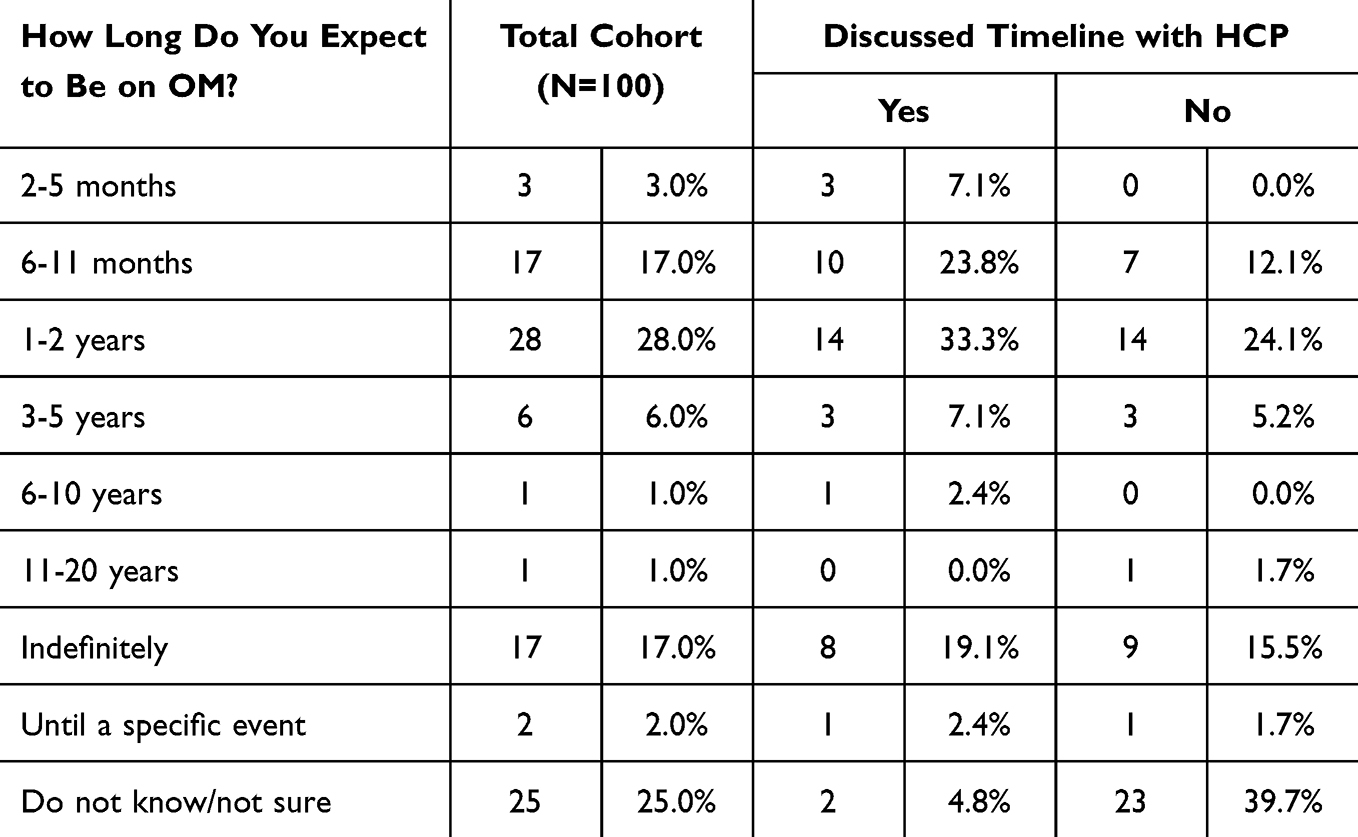 |
Table 3 HCP Discussions and Expected Duration of OM Therapy |
OM Switching Preferences
More than 1 in 5 (23%) PwO reported contemplating switching from their current OM. Among those who had considered a change, the primary drivers included the prospect of improved efficacy (22%), reduced side effects (17%), and dissatisfaction with weight loss outcomes (13%). Notably, PwO using newer-generation OMs less often considered switching to an alternative OM (Table 4).
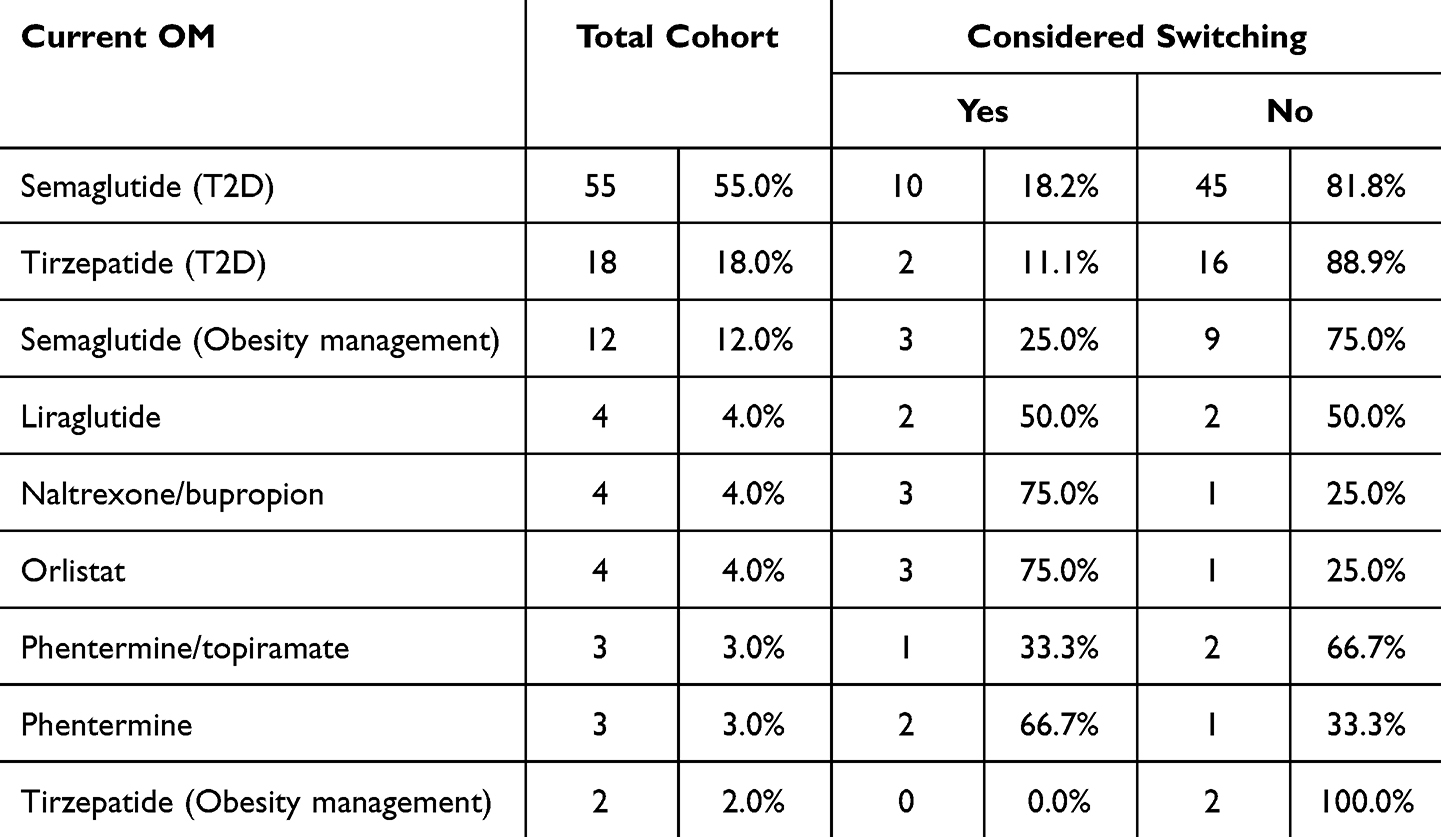 |
Table 4 Switching Preferences by OM Type |
Person-Level Financial Implications of OM Treatment
Overall, 57% of PwO reported OOP expenses of $50 or less per month for their OM, and 25% reported an OOP cost of $100 or more per month. The anticipated treatment duration among PwO varied with reported OOP costs. Among PwO who expected to use their current OM for a limited time (n=56), 41% were paying $100 or more in OOP expenses per month. In contrast, only 18% of those planning to remain on treatment indefinitely (n=17) reported OOP costs of $100 or more OOP expenses per month. Substantial individual-level variation in cost-sharing for the same OM was also observed (Table 5). For instance, OOP expenditures for semaglutide and tirzepatide ranged from $0 to $400 or more per month. In addition, 58% reported being willing to spend more on OMs over alternative interventions. However, only 59% reported being able to sustain their current OM-related expenditure for up to two years, irrespective of the income level.
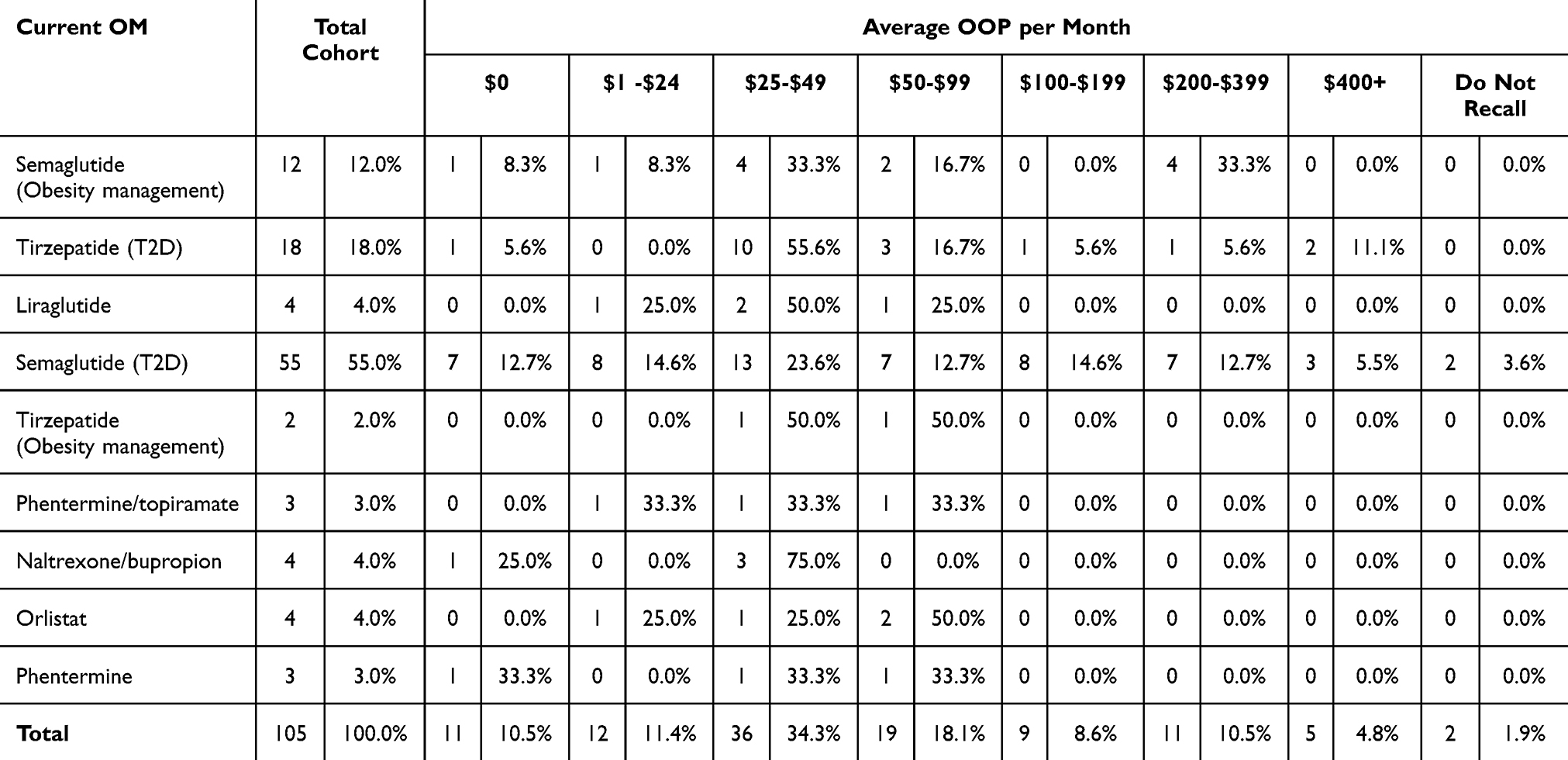 |
Table 5 Monthly OOP by OM Type |
Discussion
This study contributes to the growing body of literature exploring the real-world experiences of PwO, specifically regarding their treatment decision-making, use of OMs, perceived challenges and benefits, and financial burden associated with such treatments. The results underscore how multimorbidity, health perceptions, insurance coverage, and patient-provider communication patterns shape the uptake, continuation, and satisfaction with OMs.
Most PwO in this study were formally diagnosed with obesity, primarily by PCPs, reflecting national trends where the bulk of medical care and OM prescribing occurs in primary care settings. An analysis of 2.2 million adults in US reported that PCPs were the leading prescribers of OMs,40 a finding supported by a recent analysis showing that most OM prescriptions were issued by PCPs and advanced practice practitioner (APPs), as opposed to cardiologists, endocrinologists, general surgeons, and all other specialists.41 This highlights the critical role of PCPs, physician assistants (PAs), nurse practitioners (NPs), and advanced practice provider in frontline obesity care. Collaborative care models involving PCPs, PAs, NPs, APPs along with specialists can improve obesity outcomes.42–44 Yet, many PCPs face knowledge gaps, limited training in obesity pharmacotherapy and limited time to provide guideline-based care, all of which lead to underutilization of treatment.45–48 Future obesity care may benefit from stronger PCP-specialist collaboration, supported by education and system-level frameworks to equip PCPs for active, evidence-based obesity management.
The majority of PwO in this analysis, among whom the prevalence of complications of obesity was high, identified obesity as their primary health concern. While this might be considered unsurprising in a population treated for obesity, it suggests that clinical efforts to contextualize obesity as an upstream cause or contributor to other health conditions might inform personalized and targeted obesity treatment decisions. Such efforts should additionally incorporate psychological and social sequelae of obesity, including exposure to stigma, reduced self-esteem, and impaired daily functioning. These insights emphasize the need for healthcare providers to take a holistic approach when discussing treatment pathways, addressing not just physical health but also the emotional and psychosocial dimensions of living with obesity. By recognizing the role of weight-related concerns in patients’ lives, clinicians can foster more empathetic, personalized, and effective care.
The study revealed that most PwO attempt several distinct weight loss methods before initiating OMs. Specifically, 86% of participants reported using at least one prior weight management strategy, with a median of 3 attempts. These findings align with clinical guidelines, which recommend initial therapy with behavioral interventions such as calorie restriction, increased physical activity, and lifestyle counseling in most persons.49–51 This observation additionally underscores the relapsing and remitting nature of obesity52 and, when used in isolation, the limited health improvements with lifestyle interventions once obesity and its complications are established.53 Indeed, body weight reduction achieved through lifestyle interventions alone is rapidly counter regulated through maladaptive neurometabolic and enteroendocrine mechanisms that antagonize durable weight reduction and promote weight recurrence.54,55 This highlights the need for therapeutic approaches that consider obesity as a chronic and relapsing disease requiring timely and sustained multi-modal intervention.
A central finding of this study is the strong motivation among PwO to initiate OMs for long-term health improvement, better physical function, and complication management. This aligns with prior research showing that patients view weight loss as a critical step toward reducing disease burden and enhancing quality of life.56 Despite this motivation, financial and structural barriers significantly limit OM uptake. In this analysis, insurance coverage issues, concerns about side effects, and high OOP costs were the leading barriers to OM use, findings consistent with previous studies documenting limited OM access.57–59 Nevertheless, two-thirds of participants reported positive experiences with OMs, particularly among those who continued treatment for six months or longer. These findings reinforce the need for clinical and policy efforts to promote increased access and adherence.60,61
An important insight from the study centers on communication between PwO and their HCPs about OM treatment. While these conversations commonly addressed side effects and medication administration, discussions around integration of lifestyle interventions with pharmacotherapy were primarily initiated by HCPs. This gap emphasizes the need to ensure optimal education around concomitant use of OMs and lifestyle interventions to minimize side effects, ensure safety, and enhance achievement of health goals.62 Additionally, fewer than half of PwO discussed treatment duration and most expected therapy to last less than 2 years despite evidence from clinical trials supporting longitudinal use to maintain treatment benefits,23,26,27 including maintenance of disease control and prevention of recurrence. Those on medication for over 6 months were more likely to have had these discussions, suggesting that ongoing treatment fosters deeper communication. In addition, anticipated treatment duration appeared to be influenced by financial considerations, particularly OOP costs which aligns with prior published research work.38,63 However, the lack of early dialogue on treatment timelines represents a missed opportunity to set expectations and provide anticipatory support, with implications for premature discontinuation and subsequent clinical outcomes. These findings highlight the need for evidence-based provider training that emphasizes open, empathetic, and stigma-free communication. Optimal conversations should go beyond medication logistics to include lifestyle behaviors, emotional well-being, and long-term care planning. Research has consistently demonstrated that when patients feel heard and respected, their clinical outcomes and treatment satisfaction improve.64,65
The financial impact of OMs emerged as a significant concern, with 57% of participants paying $50 or less per month OOP, yet only 59% reporting they could sustain this cost for up to two years. These findings highlight the disconnect between willingness to pay and actual financial capacity of these PwO. The variation in cost-sharing for the same medication type may also reflect important inter-individual differences in insurance design and access, which may shape resultant OM access and health outcomes. Addressing these differences will require coordinated efforts among policymakers, payers, and clinicians to reduce financial barriers and ensure equitable access to effective obesity treatments.
This study has several strengths. It adds to a limited literature reporting on patient perspectives of OMs,38,63,66,67 capturing a broad range of factors including treatment motivations, barriers, patient-provider communication, and financial impacts. The survey design was informed by qualitative interviews and expert input, ensuring that key patient concerns and clinical insights were comprehensively assessed. The detailed exploration of multimorbidity, prior weight management efforts, and treatment adherence adds depth to the understanding of patient experiences. However, several limitations should also be acknowledged. First, selection of PwO actively receiving OM therapy may have underestimated barriers to receiving such treatment. Second, the survey respondents were predominantly White, employed or retired, and had commercial insurance. As such, the generalizability of these findings to more diverse, underinsured, or socioeconomically disadvantaged populations is uncertain. Third, the cross-sectional survey design captures patient experiences and perceptions at a single time point, which precludes assessment of longitudinal changes in treatment adherence, outcomes, or attitudes. However, the inclusion of forecasting-oriented survey questions (eg, expected treatment duration) offers some temporal insights. Fourth, self-reported data may be subject to recall bias. Lastly, this hypothesis generating study was limited by its small sample size and focus on commercially insured patients. However, despite these constraints, it provides comprehensive insights into the OM treatment experiences among PwO. Future research should focus on larger, more representative samples and incorporate longitudinal designs to enhance understanding of long-term treatment trajectories and outcomes across varied patient subgroups.
In conclusion, this study highlights the multifaceted experiences of PwO in managing obesity, particularly regarding OM use. The findings underscore the importance of early intervention, robust patient-provider communication, equitable access, and financial support to optimize treatment outcomes. As new pharmacologic agents continue to reshape the obesity treatment landscape, it is critical to ensure that these innovations translate into real-world benefits for all patients. Addressing systemic barriers, stigma, education, and communication gaps will be essential to fulfilling the promise of obesity pharmacotherapy in clinical practice.
Acknowledgments
This research was conducted in collaboration with Matthew Voghel (Analytics and Insights, BIPI US). His contributions and expertise were instrumental in supporting and completing the work.
Author Contributions
JWO contributed to data interpretation, offered critical insights, and was responsible for drafting and revising the manuscript. AC, ELK, and BC were involved in the conceptualization of the study, survey design, data interpretation, and provided critical revisions to the manuscript. BMKD oversaw the study, contributed to the interpretation of findings, and provided critical revisions to the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported and funded by Boehringer Ingelheim.
Disclosure
JWO reports grant support from National Institutes of Health. AC, ELK, BC, and BMKD are employees of Boehringer Ingelheim Pharmaceuticals, Inc. (BIPI). The authors met the criteria for authorship as recommended by the International Committee of Medical Journal Editors (ICMJE). The authors did not receive payment related to the development of the manuscript. Boehringer Ingelheim was given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations.
References
1. World Health Organization. Obesity 2025. Available from: https://www.who.int/health-topics/obesity#tab=tab_1.
2. U.S. Centers For Disease Control and Prevention. Obesity. 2025. Available from: https://www.cdc.gov/obesity/.
3. U.S. Centers For Disease Control and Prevention. Adult BMI categories. 2024 Available from: https://www.cdc.gov/bmi/adult-calculator/bmi-categories.html.
4. World Health Organization. Obesity and overweight. 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
5. GBD US Obesity Forecasting Collaborators. National-level and state-level prevalence of overweight and obesity among children, adolescents, and adults in the USA, 1990-2021, and forecasts up to 2050, Lancet. 2024;404(10469):2278–2298. PMID: 39551059. doi:10.1016/S0140-6736(24)01548-4
6. Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of obesity and severe obesity among adults: United States, 2017-2018. NCHS Data Brief. 2020; 2020(360):1–8. PMID: 32487284.
7. World Obesity Federation. World obesity atlas. 2023 Available from: https://www.worldobesity.org/resources/resource-library/world-obesity-atlas-2023.
8. Ruze R, Liu T, Zou X, et al. Obesity and type 2 diabetes mellitus: connections in epidemiology, pathogenesis, and treatments. Front Endocrinol. 2023;14:1161521. PMID: 37152942; PMCID: PMCPMC10161731. doi:10.3389/fendo.2023.1161521
9. Bhupathiraju SN, Hu FB. Epidemiology of obesity and diabetes and their cardiovascular complications. Circ Res. 2016;118(11):1723–1735. PMID: 27230638; PMCID: PMCPMC4887150. doi:10.1161/CIRCRESAHA.115.306825
10. Yu H-J, Ho M, Liu X, Yang J, Chau PH, Fong DYT. Association of weight status and the risks of diabetes in adults: a systematic review and meta-analysis of prospective cohort studies. Int J Obes Lond. 2022;46(6):1101–1113. PMID: 35197569. doi:10.1038/s41366-022-01096-1
11. Powell-Wiley TM, Poirier P, Burke LE, et al. Obesity and cardiovascular disease: a scientific statement from the American heart association. Circulation. 2021;143(21):e984–e1010. PMID: 33882682; PMCID: PMCPMC8493650. doi:10.1161/CIR.0000000000000973
12. Riaz H, Khan MS, Siddiqi TJ, et al. Association between obesity and cardiovascular outcomes: a systematic review and meta-analysis of mendelian randomization studies. JAMA Network Open. 2018;1(7):e183788. PMID: 30646365. doi:10.1001/jamanetworkopen.2018.3788
13. Kim MS, Kim WJ, Khera AV, et al. Association between adiposity and cardiovascular outcomes: an umbrella review and meta-analysis of observational and Mendelian randomization studies. Eur Heart J. 2021;42(34):3388–3403. PMID: 34333589; PMCID: PMCPMC8423481. doi:10.1093/eurheartj/ehab454
14. Li L, Liu DW, Yan HY, Wang ZY, Zhao SH, Wang B. Obesity is an independent risk factor for non-alcoholic fatty liver disease: evidence from a meta-analysis of 21 cohort studies. Obes Rev. 2016;17(6):510–519. PMID: 27020692. doi:10.1111/obr.12407
15. Pinto KRD, Feckinghaus CM, Hirakata VN. Obesity as a predictive factor for chronic kidney disease in adults: systematic review and meta-analysis. Braz J Med Biol Res. 2021;54(4):e10022. PMID: 33656052; PMCID: PMCPMC7917711. doi:10.1590/1414-431X202010022
16. Walsh TP, Arnold JB, Evans AM, Yaxley A, Damarell RA, Shanahan EM. The association between body fat and musculoskeletal pain: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2018;19(1):233. PMID: 30021590; PMCID: PMCPMC6052598. doi:10.1186/s12891-018-2137-0
17. Yoo JJ, Cho NH, Lim SH, Kim HA. Relationships between body mass index, fat mass, muscle mass, and musculoskeletal pain in community residents. Arthritis Rheumatol. 2014;66(12):3511–3520. PMID: 25185757. doi:10.1002/art.38861
18. Zheng H, Chen C. Body mass index and risk of knee osteoarthritis: systematic review and meta-analysis of prospective studies. BMJ Open. 2015;5(12):e007568. PMID: 26656979; PMCID: PMCPMC4679914. doi:10.1136/bmjopen-2014-007568
19. Chen J, Ke K, Liu Z, et al. Body mass index and cancer risk: an umbrella review of meta-analyses of observational studies. Nutr Cancer. 2023;75(4):1051–1064. PMID: 37139871. doi:10.1080/01635581.2023.2180824
20. Kyrgiou M, Kalliala I, Markozannes G, et al. Adiposity and cancer at major anatomical sites: umbrella review of the literature. BMJ. 2017;356(j477). PMID: 28246088; PMCID: PMCPMC5421437. doi:10.1136/bmj.j477
21. Nianogo RA, Rosenwohl-Mack A, Yaffe K, Carrasco A, Hoffmann CM, Barnes DE. Risk factors associated with alzheimer disease and related dementias by sex and race and ethnicity in the US. JAMA Neurol. 2022;79(6):584–591. PMID: 35532912; PMCID: PMCPMC9086930. doi:10.1001/jamaneurol.2022.0976
22. Flegal KM, Kit BK, Orpana H, Graubard BI. Association of all-cause mortality with overweight and obesity using standard body mass index categories: a systematic review and meta-analysis. JAMA. 2013;309(1):71–82. PMID: 23280227; PMCID: PMCPMC4855514. doi:10.1001/jama.2012.113905
23. le Roux CW, Steen O, Lucas KJ, Startseva E, Unseld A, Hennige AM. Glucagon and GLP-1 receptor dual agonist survodutide for obesity: a randomised, double-blind, placebo-controlled, dose-finding Phase 2 trial. Lancet Diabetes Endocrinol. 2024;12(3):162–173. PMID: 38330987. doi:10.1016/S2213-8587(23)00356-X
24. Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989–1002. PMID: 33567185. doi:10.1056/NEJMoa2032183
25. Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide once weekly for the treatment of obesity. N Engl J Med. 2022;387(3):205–216. PMID: 35658024. doi:10.1056/NEJMoa2206038
26. Rubino D, Abrahamsson N, Davies M, et al. Effect of continued weekly subcutaneous semaglutide vs placebo on weight loss maintenance in adults with overweight or obesity: the STEP 4 randomized clinical trial. JAMA. 2021;325(14):1414–1425. PMID: 33755728; PMCID: PMCPMC7988425. doi:10.1001/jama.2021.3224
27. Aronne LJ, Sattar N, Horn DB, et al. Continued treatment with tirzepatide for maintenance of weight reduction in adults with obesity: the SURMOUNT-4 randomized clinical trial. JAMA. 2024;331(1):38–48. PMID: 38078870; PMCID: PMCPMC10714284. doi:10.1001/jama.2023.24945
28. Badve SV, Bilal A, Lee MMY, et al. Effects of GLP-1 receptor agonists on kidney and cardiovascular disease outcomes: a meta-analysis of randomised controlled trials. Lancet Diabetes Endocrinol. 2025;13(1):15–28. PMID: 39608381. doi:10.1016/S2213-8587(24)00271-7
29. Neuen BL, Fletcher RA, Heath L, et al. Cardiovascular, kidney, and safety outcomes with GLP-1 receptor agonists alone and in combination with SGLT2 inhibitors in type 2 diabetes: a systematic review and meta-analysis. Circulation. 2024;150(22):1781–1790. PMID: 39210781. doi:10.1161/CIRCULATIONAHA.124.071689
30. Sattar N, Lee MMY, Kristensen SL, et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of randomised trials. Lancet Diabetes Endocrinol. 2021;9(10):653–662. PMID: 34425083. doi:10.1016/S2213-8587(21)00203-5
31. Davies M, Faerch L, Jeppesen OK, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, Phase 3 trial. Lancet. 2021;397(10278):971–984. PMID: 33667417. doi:10.1016/S0140-6736(21)00213-0
32. Rosenstock J, Wysham C, Frias JP, et al. Efficacy and safety of a novel dual GIP and GLP-1 receptor agonist tirzepatide in patients with type 2 diabetes (SURPASS-1): a double-blind, randomised, phase 3 trial. Lancet. 2021;398(10295):143–155. PMID: 34186022. doi:10.1016/S0140-6736(21)01324-6
33. Caruso I, Di Gioia L, Di Molfetta S, et al. Glucometabolic outcomes of GLP-1 receptor agonist-based therapies in patients with type 2 diabetes: a systematic review and network meta-analysis. EClinicalMedicine. 2023;64:102181. PMID: 37719418; PMCID: PMCPMC10500557. doi:10.1016/j.eclinm.2023.102181
34. Sanyal AJ, Bedossa P, Fraessdorf M, et al. A phase 2 randomized trial of survodutide in MASH and Fibrosis. N Engl J Med. 2024;391(4):311–319. PMID: 38847460. doi:10.1056/NEJMoa2401755
35. Sanyal AJ, Newsome PN, Kliers I, et al. Phase 3 trial of semaglutide in metabolic dysfunction-associated steatohepatitis. N Engl J Med. 2025;392(21):2089–2099. PMID: 40305708. doi:10.1056/NEJMoa2413258
36. Ostrominski JW, Ortega-Montiel J, Tesfaye H, et al. Trends in utilization of glucose- and weight-lowering medications after tirzepatide approval in the united states: a population-based cohort study. Ann Intern Med. 2025;178(5):620–633. PMID: 40228298. doi:10.7326/ANNALS-24-02870
37. Ostrominski JW, Wagholikar KB, Olsson K, et al. Contemporary treatment patterns of overweight and obesity: insights from the mass general Brigham health care system. Obesity. 2025;33(2):365–384. doi:10.1002/oby.24186
38. Kaplan LM, Gudzune K, Ard J, et al. Perceptions of anti-obesity medications among people with obesity and healthcare providers in the US: findings from the OBSERVE study. Obesity. 2025;33(6):1076–1086. PubMed PMID: 40275477; PMCID: PMCPMC12119403. doi:10.1002/oby.24290
39. World Medical A. World medical association declaration of Helsinki: ethical principles for medical research involving human participants, JAMA. 2025;333(1):71–74. PMID: 39425955. doi:10.1001/jama.2024.21972
40. Saxon DR, Iwamoto SJ, Mettenbrink CJ, et al. Antiobesity medication use in 2.2 million adults across eight large health care organizations: 2009-2015. Obesity. 2019;27(12):1975–1981. PMID: 31603630; PMCID: PMCPMC6868321. doi:10.1002/oby.22581
41. Berning P, Adhikari R, Schroer AE, et al. Longitudinal analysis of obesity drug use and public awareness. JAMA Network Open. 2025;8(1):e2457232. PMID: 39878977; PMCID: PMCPMC11780480. doi:10.1001/jamanetworkopen.2024.57232
42. Tsai AG, Wadden TA. Treatment of obesity in primary care practice in the United States: a systematic review. J Gen Intern Med. 2009;24(9):1073–1079. PMID: 19562419; PMCID: PMCPMC2726879. doi:10.1007/s11606-009-1042-5
43. Kushner RF, Ryan DH. Assessment and lifestyle management of patients with obesity: clinical recommendations from systematic reviews. JAMA. 2014;312(9):943–952. PMID: 25182103. doi:10.1001/jama.2014.10432
44. Fleischman A, Hourigan SE, Lyon HN, et al. Creating an integrated care model for childhood obesity: a randomized pilot study utilizing telehealth in a community primary care setting. Clin Obes. 2016;6(6):380–388. PMID: 27863024; PMCID: PMCPMC5523655. doi:10.1111/cob.12166
45. Turner M, Jannah N, Kahan S, Gallagher C, Dietz W. Current knowledge of obesity treatment guidelines by health care professionals. Obesity. 2018;26(4):665–671. PMID: 29570250. doi:10.1002/oby.22142
46. Oshman L, Othman A, Furst W, et al. Primary care providers’ perceived barriers to obesity treatment and opportunities for improvement: a mixed methods study. PLoS One. 2023;18(4):e0284474. PMID: 37071660; PMCID: PMCPMC10112804 Health (DK107456. doi:10.1371/journal.pone.0284474
47. Fruh SM, Golden A, Graves RJ, et al. Competency in obesity management: an educational intervention study with nurse practitioner students. J Am Assoc Nurse Pract. 2019;31(12):734–740. PMID: 31169791; PMCID: PMCPMC7094771. doi:10.1097/JXX.0000000000000218
48. Porter J, Boyd C, Skandari MR, Laiteerapong N. Revisiting the time needed to provide adult primary care. J Gen Intern Med. 2023;38(1):147–155. PMID: 35776372; PMCID: PMCPMC9848034. doi:10.1007/s11606-022-07707-x
49. Apovian CM, Aronne LJ, Bessesen DH, et al. Pharmacological management of obesity: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2015;100(2):342–362. PMID: 25590212. doi:10.1210/jc.2014-3415
50. Kahan S. Overweight and obesity management strategies. Am J Manag Care. 2016;22(7 Suppl):s186–96. PMID: 27356116.
51. Jastreboff AM, Kotz CM, Kahan S, Kelly AS, Heymsfield SB. Obesity as a disease: the obesity society 2018 position statement. Obesity. 2019;27(1):7–9. PMID: 30569641. doi:10.1002/oby.22378
52. Bray GA, Kim KK, Wilding JPH, World Obesity F. Obesity: a chronic relapsing progressive disease process. A position statement of the world obesity federation. Obes Rev. 2017;18(7):715–723. PMID: 28489290. doi:10.1111/obr.12551
53. Look ARG, Wing RR, Bolin P, et al. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N Engl J Med. 2013;369(2):145–154. PMID: 23796131; PMCID: PMCPMC3791615. doi:10.1056/NEJMoa1212914
54. Leibel RL, Rosenbaum M, Hirsch J. Changes in energy expenditure resulting from altered body weight. N Engl J Med. 1995;332(10):621–628. PMID: 7632212. doi:10.1056/NEJM199503093321001
55. Sumithran P, Prendergast LA, Delbridge E, et al. Long-term persistence of hormonal adaptations to weight loss. N Engl J Med. 2011;365(17):1597–1604. PMID: 22029981. doi:10.1056/NEJMoa1105816
56. Wadden TA, Webb VL, Moran CH, Bailer BA. Lifestyle modification for obesity: new developments in diet, physical activity, and behavior therapy. Circulation. 2012;125(9):1157–1170. PMID: 22392863; PMCID: PMCPMC3313649. doi:10.1161/CIRCULATIONAHA.111.039453
57. Gomez G, Stanford FC. US health policy and prescription drug coverage of FDA-approved medications for the treatment of obesity. Int J Obes. 2018;42(3):495–500. PMID: 29151591; PMCID: PMCPMC6082126. doi:10.1038/ijo.2017.287
58. Chen AS, Borden CG, Canavan ME, Ross JS, Oladele CR, Lipska KJ. Cost-related prescription drug rationing by adults with obesity. JAMA Network Open. 2024;7(11):e2433000. PMID: 39499520; PMCID: PMCPMC11539006. doi:10.1001/jamanetworkopen.2024.33000
59. Gasoyan H, Sarwer DB. Addressing insurance-related barriers to novel antiobesity medications: lessons to be learned from bariatric surgery. Obesity. 2022;30(12):2338–2339. PMID: 36190393; PMCID: PMCPMC9691525. doi:10.1002/oby.23556
60. Gleason PP, Urick BY, Marshall LZ, Friedlander N, Qiu Y, Leslie RS. Real-world persistence and adherence to glucagon-like peptide-1 receptor agonists among obese commercially insured adults without diabetes. J Manag Care Spec Pharm. 2024;30(8):860–867. PMID: 38717042; PMCID: PMCPMC11293763. doi:10.18553/jmcp.2024.23332
61. Wharton S, Haase CL, Kamran E, et al. Weight loss and persistence with liraglutide 3.0 mg by obesity class in the real-world effectiveness study in Canada. Obes Sci Pract. 2020;6(4):439–444. PMID: 32874678; PMCID: PMCPMC7448201. doi:10.1002/osp4.420
62. Lundgren JR, Janus C, Jensen SBK, et al. Healthy weight loss maintenance with exercise, liraglutide, or both combined. N Engl J Med. 2021;384(18):1719–1730. PMID: 33951361. doi:10.1056/NEJMoa2028198
63. Kaplan LM, Golden A, Jinnett K, et al. Perceptions of barriers to effective obesity care: results from the national ACTION study. Obesity. 2018;26(1):61–69. PMID: 29086529. doi:10.1002/oby.22054
64. Beach MC, Sugarman J, Johnson RL, Arbelaez JJ, Duggan PS, Cooper LA. Do patients treated with dignity report higher satisfaction, adherence, and receipt of preventive care? Ann Fam Med. 2005;3(4):331–338. PMID: 16046566; PMCID: PMCPMC1466898. doi:10.1370/afm.328
65. Flickinger TE, Saha S, Roter D, et al. Respecting patients is associated with more patient-centered communication behaviors in clinical encounters. Patient Educ Couns. 2016;99(2):250–255. PMID: 26320821; PMCID: PMCPMC5271348. doi:10.1016/j.pec.2015.08.020
66. Kaiser Family Foundation. The public’s views of new prescription weight loss drugs and prescription drug costs 2023. Available from: https://www.kff.org/health-costs/poll-finding/kff-health-tracking-poll-july-2023-the-publics-views-of-new-prescription-weight-loss-drugs-and-prescription-drug-costs/.
67. Pew Research Center. How Americans view weight-loss drugs and their potential impact on obesity in the US. 2024.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.