Back to Journals » Clinical Interventions in Aging » Volume 21
Nutrition and Aging in Iran: A Critical Analysis of Policy Responses
Authors Nabizadeh Bonab Y ![]() , Hosseini S, Barzegar A
, Hosseini S, Barzegar A
Received 23 December 2025
Accepted for publication 28 June 2026
Published 9 July 2026 Volume 2026:21 589780
DOI https://doi.org/10.2147/CIA.S589780
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Yalda Nabizadeh Bonab, Samira Hosseini, Ali Barzegar
Department of Community Nutrition, Faculty of Nutrition and Food Sciences, Tabriz University of Medical Sciences, Tabriz, Iran
Correspondence: Yalda Nabizadeh Bonab, Email [email protected]
Background: Iran is undergoing a rapid demographic transition toward population aging, which poses significant challenges for the health system, social protection mechanisms, and food and nutrition policies. Despite the well-established role of nutrition in healthy aging, its integration into aging-related policies in Iran has not been comprehensively examined. Although national nutrition frameworks exist, they remain fragmented and insufficiently operationalized for the elderly. As this demographic transition in Iran, its struggle to integrate nutrition into aging policies mirrors challenges faced by many other lower-middle-income countries.
Objective: This study evaluates the coherence, implementation capacity, and strategic alignment of Iran’s aging-related policies concerning nutritional needs.
Methods: This comprehensive review of secondary data is a descriptive analytical policy was conducted using qualitative content analysis. The study examined national policy documents, demographic indicators, and regulatory frameworks published between 2011 and 2025, focusing on five key dimensions: policy convergence, age-specific characteristics, implementation mechanisms, monitoring, and equity.
Results: Findings reveal a significant structural imbalance; vast majority (over 70%) of analyzed documents prioritize curative medical interventions over preventive nutritional strategies. Critical gaps identified include the absence of age-specific dietary guidelines, fragmented screening protocols, and a lack of intersectoral coordination between health and social welfare sectors.
Conclusion: Unlike successful integrated models such as Thailand’s community-based approach, Iran’s framework is characterized by fragmentation. To mitigate the health risks of aging, a paradigm shift is required, moving from generalized health policies toward “nutrition-sensitive” aging strategies that integrate systematic screening and localized, preventive interventions into the national policy landscape. Although the findings are context-specific, the framework applied in this study may be adapted by other middle-income countries to assess geriatric nutrition policies within their own health system and policy contexts.
Keywords: healthy aging, nutrition policy, geriatric nutrition, food security, demographic transition, content analysis
Introduction
Population aging represents one of the most transformative demographic shifts of the twenty-first century. According to the United Nations, the global population aged 60 and older is projected to double by 2050, exceeding two billion individuals.1 This transition imposes substantial pressure on health systems, social protection frameworks, and public policy infrastructures, particularly in low and middle-income countries undergoing rapid demographic transitions.2,3
Iran is currently experiencing one of the most accelerated aging processes within the Middle East and North Africa (MENA) region. Driven by declining fertility rates, increasing life expectancy, and an ongoing epidemiological transition, projections indicate that by 2050, approximately 25–26% of Iran’s population will be aged 60 or older.1 This demographic surge presents critical challenges to the long-term sustainability of healthcare financing, social welfare systems, and long-term care provisions.
Nutritional adequacy is a fundamental determinant of healthy aging and the preservation of functional ability. Targeted dietary intake is essential for maintaining muscle mass, mitigating frailty and sarcopenia, bolstering immune function, and reducing the prevalence of non-communicable diseases. However, older adults face heightened vulnerability to malnutrition due to a complex interplay of physiological senescence, polypharmacy, diminished appetite, social isolation, and economic constraints.4,5 Research underscores malnutrition in older populations as a pressing global health concern,6,7 necessitating specialized nutritional interventions. Furthermore, regional data from the WHO-EMRO highlights specific nutritional vulnerabilities within the elderly population in Iran.8
Despite the clinical importance of nutrition, a significant disconnect exists between demographic trends and policy responses. While the National Document on Elderly Care in Iran serves as a pivotal framework for fostering healthy aging, there remains a critical oversight regarding the integration of specialized geriatric nutrition within broader health and welfare mandates. Although the document aims to optimize quality of life, addressing nutritional determinants requires more than generalized welfare; it demands specific, evidence-based nutritional policies.9 Recent legal analyses suggest that, despite international commitments, the domestic regulatory landscape lacks the necessary specificity to protect the nutritional rights of the elderly as a distinct demographic group.10
Furthermore, aligning national efforts with global benchmarks set by organizations such as the WHO and the UN1,3,11–14 is essential for developing robust, evidence-based strategies. Integrating clinical, legal, and international dimensions is therefore vital for a holistic assessment of Iran’s capacity to address these needs.8,15,16 To this end, this study employs a multi-dimensional approach: first, evaluating the nutritional status of older adults in Iran through secondary data (Section 2); second, conducting a systematic review of national laws and policy frameworks (Section 3); and finally, utilizing qualitative content analysis to identify policy strengths, structural gaps, and strategic opportunities (Section 4).15,16
The remainder of this article is organized as follows: The methodology regarding policy document identification and analysis is detailed in the subsequent section. This is followed by a presentation of findings concerning nutritional policies for the elderly in Iran. Finally, the discussion evaluates these findings against existing literature, identifies key policy gaps, and concludes with practical recommendations and implications for future research.
Nutritional Status of Older Adults in Iran
Malnutrition and Nutritional Risk
Evidence from national and regional studies indicates a significant prevalence of malnutrition and associated nutritional risks among the Iranian elderly. Community-based studies employing validated instruments, such as the Mini Nutritional Assessment (MNA), have reported malnutrition prevalence rates ranging from 6% to 15%, with a substantially larger proportion of the population categorized as being at high risk of malnutrition.16,17 This vulnerability is further exacerbated in institutionalized settings, where prevalence rates have been reported to exceed 20%, highlighting the heightened risks faced by older adults in long-term care environments.6 Clinically, malnutrition in this demographic is closely linked to increased hospitalization rates, functional decline, frailty, and elevated mortality.4 Furthermore, the interplay of socioeconomic determinants, including low income, limited educational attainment, social isolation, and inadequate support systems, serves as a critical predictor of poor nutritional outcomes.18,19 These findings suggest that nutritional interventions in Iran must extend beyond clinical settings to address the underlying socioeconomic vulnerabilities embedded in the aging process.
Dietary Quality and Micronutrient Deficiencies
Beyond caloric insufficiency, the quality of dietary intake among Iranian older adults reveals widespread micronutrient deficiencies. Assessment data indicates significant inadequacies in essential nutrients, including vitamin D, calcium, folate, zinc, selenium, and potassium.20 Vitamin D deficiency, in particular, remains a widespread public health concern, driven by limited dietary fortification and insufficient sun exposure.8 Concurrently, a shift toward diets high in sodium, refined carbohydrates, and saturated fats has contributed to the rising prevalence of hypertension, cardiovascular diseases, and type 2 diabetes among this population.21,22 This pattern characterizes a “dual burden of malnutrition”, where nutrient deficiencies coexist with diet-related chronic metabolic diseases. This complexity necessitates a more nuanced policy approach that moves beyond simple food security to encompass comprehensive nutritional quality and dietary management.
Policy and Legal Frameworks Related to Nutrition and Aging in Iran
Legal and Constitutional Context
The constitutional framework of the Islamic Republic of Iran provides a normative foundation for the protection of health, social welfare, and human dignity across the life course, including for older adults. The constitutional provisions regarding the Right to Social Security explicitly recognize the entitlement of all citizens to social protection and public support in situations such as old age, disability, unemployment, and economic vulnerability. In parallel, the principles of Economic Justice and the Provision of Basic Needs emphasize the state’s responsibility to ensure access to essential necessities, including adequate food, housing, healthcare, and education as core components of social justice and equitable development.
Despite these constitutional commitments, adequate nutrition is not articulated as an independent and enforceable legal right. Rather, food security and access to sufficient, safe food are implicitly embedded within broader welfare and subsistence principles. This indirect legal framing has contributed to the marginalization of nutrition, particularly geriatric nutrition within binding policy instruments and statutory laws, resulting in fragmented interventions and limited institutional accountability.15
At the international level, Iran is a State Party to several human rights instruments that explicitly recognize nutrition and health as fundamental rights. The Article on the Right to an Adequate Standard of Living, Including Adequate Food, contained in the International Covenant on Economic, Social and Cultural Rights, affirms the right of every individual to adequate food and freedom from hunger. Additionally, the Article on the Right to the Highest Attainable Standard of Physical and Mental Health in the same Covenant underscores the obligation of governments to address the underlying determinants of health, including nutrition, food security, and access to safe and sufficient diets throughout the life course, with particular attention to vulnerable populations such as older adults.
Furthermore, global development frameworks reinforce these rights-based commitments. The Sustainable Development Goal on Ending Hunger and Achieving Food Security, alongside the goal of Ensuring Healthy Lives and Promoting Well-being at All Ages, explicitly link nutrition, health, and social equity, highlighting the importance of inclusive food and health systems that respond to demographic aging.1 The World Health Organization, through the Global Strategy and Action Plan on Ageing and Health, identifies adequate nutrition as a key determinant of functional ability, independence, and quality of life in older age, calling for integrated and legally supported nutrition-sensitive policies.12 Similarly, the Food and Agriculture Organization (FAO) emphasizes nutrition-sensitive social protection as a critical policy instrument for safeguarding food security among older adults in rapidly aging societies.23
Overall, while constitutional and international legal frameworks establish broad protections related to health and social welfare, the absence of explicit recognition of adequate nutrition, particularly in the context of aging, limits the effectiveness of policy responses. Strengthening the legal articulation of the right to adequate food and nutrition in older age, through clearer statutory language and alignment with international rights-based instruments, could significantly enhance policy coherence, accountability, and nutritional equity within Iran’s food and health systems.
National Nutrition Policies
Iran has established national nutrition policies aimed at improving dietary quality and reducing nutrition-related non-communicable diseases (NCDs) at the population level. A key policy instrument in this domain is the development of Food-Based Dietary Guidelines (FBDGs), formulated with technical support from the Food and Agriculture Organization (FAO) and the World Health Organization (WHO). These guidelines promote balanced diets, reduced intake of salt and sugar, and increased consumption of fruits, vegetables, legumes, and whole grains, aligning with international recommendations for healthy eating patterns.11,23
However, Iran’s FBDGs adopt a general population approach and do not provide age-specific dietary guidance tailored to the physiological and functional changes associated with aging. Critical nutritional considerations for older adults, such as altered energy and protein requirements, micronutrient bioavailability, sarcopenia, frailty, and diet-related chronic conditions, are not explicitly addressed, thereby limiting the applicability of the guidelines for promoting healthy aging.12,23
In parallel, Iran has implemented national micronutrient interventions, including universal salt iodization and vitamin D supplementation programs, which have contributed to the prevention of iodine deficiency disorders and widespread vitamin D insufficiency. While these initiatives indirectly benefit older adults, they are primarily designed as population-wide or risk-group interventions and are not embedded within a comprehensive geriatric nutrition or healthy aging framework.8,12
Overall, although Iran’s national nutrition policies provide an important foundation for improving general dietary patterns and addressing key micronutrient deficiencies, they insufficiently account for the specific nutritional needs of an aging population. Integrating age-sensitive dietary recommendations into FBDGs and aligning nutrition policies with healthy aging strategies could enhance policy coherence and improve nutritional and functional outcomes among older adults.
Integrated Elderly Health Care Program
The Integrated Elderly Health Care Program, implemented nationwide through Iran’s primary health care (PHC) system, constitutes the most direct and structured policy intervention specifically targeting the health needs of older adults. Launched by the Ministry of Health and Medical Education (MOHME), the program aims to promote healthy aging through a comprehensive package of preventive, promotive, and referral-based services for individuals aged 60 years and older.24 Core components include periodic health assessments, screening for chronic diseases and functional limitations, lifestyle counseling, basic nutritional screening, and referral to higher levels of care when indicated.
Within this framework, nutrition is formally recognized as a key determinant of healthy aging and is incorporated into routine service delivery. Nutritional components include the assessment of body mass index (BMI), screening for undernutrition and obesity, basic dietary counseling, and general advice on healthy eating patterns. In principle, the program offers a valuable institutional platform for integrating nutrition into elder care at the community level, particularly given the extensive coverage and accessibility of Iran’s PHC network, including rural and underserved areas.8,24
However, evidence from process evaluations and implementation studies suggests that the effectiveness of the program’s nutrition-related components remains limited by several systemic and implementation barriers. Although nutritional screening is formally included in routine care, it is often delivered as a brief, standardized activity rather than as a comprehensive, person-centered assessment that informs individualized intervention and follow-up.16 This limitation is compounded by the fact that frontline health workers are typically responsible for screening without specialized training in geriatric nutrition. Consequently, their capacity to detect clinically nuanced issues, such as early-stage undernutrition, sarcopenia-related risks, micronutrient deficiencies, and hydration imbalances remains constrained.
Furthermore, the absence of standardized, age-specific nutrition protocols and formalized referral pathways limits the program’s ability to translate screening results into targeted and sustained dietary interventions. The scarcity of dietitians or geriatric nutrition specialists within the primary care setting further weakens the link between initial screening and effective clinical management. As a result, nutritional care remains largely embedded within a broader biomedical agenda focused on chronic disease control, while the preventive and functional dimensions of nutrition, essential for maintaining independence and quality of life, receive comparatively less attention.12,23 This structural and workforce-related gap helps explain why malnutrition can persist at substantial levels despite the existence of a national program dedicated to elderly health.
Overall, while the Integrated Elderly Health Care Program represents a critical policy opportunity for embedding nutrition into routine elder care, its current implementation falls short of realizing its full potential. Strengthening the nutrition dimension through specialized workforce training, the development of standardized geriatric nutrition guidelines, improved monitoring mechanisms, and stronger linkages with social protection and food assistance schemes could substantially enhance its impact on the nutritional status and healthy aging outcomes of older adults in Iran.
International Policy Context
International policy frameworks increasingly recognize nutrition as a foundational component of healthy aging and functional ability. The World Health Organization’s Decade of Healthy Ageing (2021–2030) explicitly highlights nutrition as critical to maintaining intrinsic capacity, preventing frailty, and supporting independence among older adults.11 Evidence from both high-income and middle-income countries demonstrates that effective aging policies integrate age-specific dietary guidelines, routine nutritional screening, targeted supplementation, and social nutrition support to address vulnerability and promote health equity across the life course.1,6
Comparative policy analyses reveal that countries with advanced healthy aging strategies, such as Japan, Sweden, and Germany, adopt a multisectoral approach in which nutrition is embedded across healthcare, social protection, and food system policies. These strategies typically include geriatric-specific dietary recommendations, standardized nutrition assessment protocols in primary care, the integration of specialized dietitians into elder care services, and social programs ensuring access to nutritionally adequate foods for older adults.5,7 Such integrative approaches have been associated with improved functional outcomes, reduced prevalence of undernutrition, and enhanced quality of life among aging populations.
While much attention is focused on high-income countries, the evolving landscape in middle-income countries provides more direct benchmarks for developing nations. For instance, Thailand, a nation navigating rapid demographic shifts, has moved toward a holistic, community-based model where nutrition is intrinsically linked to functional health. Although a singular, codified national nutrition policy for older adults may not be explicitly documented, substantial evidence indicates a policy trajectory that embeds nutritional considerations within comprehensive geriatric care.25–27 This is manifested through the routine implementation of nutritional risk screening, tailored interventions for dysphagia, the provision of texture-modified foods, and dedicated support for individuals experiencing frailty. The Thai experience serves as a valuable case study, demonstrating how middle-income countries can adapt global best practices to their specific socio-economic and healthcare contexts, moving away from siloed nutritional interventions toward integrated care.
In contrast, Iran’s policy landscape remains comparatively fragmented in this domain. While existing national nutrition policies and primary health care (PHC) programs provide general dietary guidance and micronutrient interventions, there is a notable lack of intersectoral integration between health, social welfare, food security, and long-term care services. This fragmentation constrains the capacity of current policies to address the multidimensional nutritional needs of older adults or to leverage nutrition as a core preventive tool within broader healthy aging strategies.8,12,23 To bridge this gap, Iran would benefit from adopting age-specific national dietary guidelines, formalizing nutritional assessment and counseling within elder care protocols, and fostering enhanced intersectoral coordination, measures increasingly recognized as essential components of international healthy aging frameworks.
Content Analysis of Nutrition-Related Aging Policies
Document Selection and Analysis
To ensure a rigorous and representative assessment, a systematic selection of policy documents was conducted. Documents were identified through a targeted search of official repositories from key decision-making bodies in Iran, including the Plan and Budget Organization, the Ministry of Health and Medical Education (MOHME), and the Organization for Social Welfare, Rehabilitation and Welfare Services.
The selection followed a two-stage process:
- Inclusion Criteria: Documents were included if they were: (a) officially published at the national level; (b) addressed health, aging, nutrition, or social welfare; and were published between 2011 and 2025.
- Exclusion Criteria: Documents were excluded if they were purely statistical reports, regional/provincial guidelines, or non-binding internal memos.
A total of 12 documents met these criteria and were subjected to semi-quantitative content analysis to evaluate the prevalence of nutrition-specific targets and the orientation (preventive vs. curative) of aging-related policies.
Coding Procedures
A systematic thematic coding process was employed to analyze the selected policy documents. Initially, an open coding phase was conducted to identify recurring themes and key concepts related to elderly nutritional policies. This was followed by axial coding to establish connections between these themes and the overarching policy frameworks. Finally, selective coding was used to refine the categories into a cohesive set of findings. To ensure the objectivity of the content analysis and minimize researcher bias, several measures were implemented. This included a rigorous application of the predefined inclusion and exclusion criteria and the use of a structured coding scheme. Furthermore, the analysis was cross-referenced with multiple policy documents to ensure that the interpretations remained grounded in the actual text of the policies rather than subjective assumptions.
Analytical Framework
A comprehensive qualitative content analysis was conducted on national policy documents addressing aging, health, and nutrition in Iran, with a particular focus on policies affecting older adults. The analytical approach employed a deductive framework informed by the World Health Organization’s conceptual models of healthy aging, including the Global Strategy and Action Plan on Ageing and Health (2015–2030) and the Decade of Healthy Ageing framework (2021–2030). These frameworks emphasize the multidimensional nature of aging, highlighting the interaction between intrinsic capacity, functional ability, environmental factors, and social determinants of health, with nutrition identified as a central determinant of health, independence, and quality of life in older age.11,12
The Content Analysis Examined Policy Documents Across Five Key Dimensions
Policy Coherence and Integration
This dimension assessed whether national policies demonstrated alignment and synergy between health, nutrition, social protection, and aging strategies. Emphasis was placed on identifying intersectoral linkages that enable coordinated interventions across multiple ministries and agencies, consistent with WHO recommendations for integrated health and social systems for older adults.8,11
Target Specificity
Policies were evaluated for their clarity in defining target populations, particularly whether nutrition interventions explicitly addressed the unique physiological, metabolic, and functional needs of older adults, such as protein adequacy, micronutrient sufficiency, and prevention of sarcopenia or frailty. Age-specificity in policy objectives is considered a critical factor in enhancing the relevance and effectiveness of interventions.1,6
Implementation Mechanisms
This dimension explored the presence of operational frameworks, resource allocation, workforce responsibilities, and service delivery channels for nutrition-related aging interventions. Emphasis was placed on identifying structured processes for integrating nutrition into primary health care, community-based elder programs, and social support schemes.16,24
Monitoring and Evaluation (M&E)
Policies were analyzed for embedded M&E systems capable of tracking implementation progress, measuring outcomes, and informing iterative policy adjustments. Particular attention was given to indicators of nutrition status among older adults, coverage of nutrition services, and effectiveness of intersectoral coordination.12,23
Equity Considerations
The framework assessed whether policies explicitly addressed disparities in access to nutrition and health services among vulnerable subpopulations of older adults, including low-income groups, rural residents, and women. Equity-oriented policy design is emphasized in international frameworks as essential to reduce health inequalities and promote inclusive aging.8,23
Using this structured analytical framework, each policy document was systematically coded and evaluated to identify strengths, gaps, and opportunities for enhancing nutrition-sensitive interventions for older adults. The deductive approach allowed for comparative assessment of Iranian national policies against international best practices, highlighting areas where policy coherence, specificity, implementation capacity, and equity considerations require improvement.1,6
Overall, this analytical framework provides a robust basis for identifying critical policy gaps in geriatric nutrition, informing recommendations for evidence-based, age-specific, and equity-oriented policy interventions in Iran.
Results
Key Findings
The semi-quantitative content analysis of Iran’s national policy documents regarding aging, health, and nutrition revealed several critical patterns and systemic gaps.
First, a profound imbalance exists between curative and preventive policy orientations. Of the 12 primary policy documents analyzed, approximately 70% focused predominantly on medicalized frameworks, such as disease management and curative interventions, while less than 30% explicitly addressed preventive, nutrition-based strategies for healthy aging. This suggests that geriatric nutrition is frequently treated as a secondary or implicit concern rather than a central pillar in the design of national health and social policies.8,16
Second, the analysis identified a lack of measurable and age-specific nutrition targets. While existing initiatives, such as the Integrated Elderly Health Care Program, incorporate basic nutritional counseling, the reviewed frameworks showed very low incidence of standardized, mandatory systems for tracking dietary quality, protein intake, or micronutrient sufficiency specifically for the older population. The absence of robust monitoring and evaluation (M&E) mechanisms limits accountability and impedes evidence-based policy adjustments.12,23
Third, significant gaps were identified in addressing the nexus between food insecurity and socioeconomic disparities. Despite well-established evidence linking food insecurity to malnutrition, frailty, and cognitive decline,1,6,28 the analyzed policies contained no specific provisions or targeted mandates to ensure equitable access to nutrient-dense foods for vulnerable elderly cohorts. Critical social determinants including income insecurity, limited mobility, and rural residence were inadequately integrated into the analyzed policy objectives.
Fourth, existing micronutrient programs (eg, universal salt iodization and vitamin D supplementation) exhibit a designed for the general population rather than older adults. The analysis revealed that in 8 out of 12 reviewed nutrition programs, interventions were formulated for the general population without being embedded within a geriatric-specific framework.8,23 This lack of age-specificity fails to account for critical physiological transitions in later life, such as altered nutrient absorption, sarcopenia, and reduced energy requirements, which are essential for maintaining functional independence.1,6
Finally, intersectoral coordination remains highly fragmented. The content analysis demonstrated a lack of integrated mandates between the health, social welfare, and food security sectors in 60% of the reviewed documents. This fragmentation prevents the emergence of a coherent, multisectoral framework, thereby reducing the potential synergy between primary healthcare, social protection, and community-based nutrition support.8,11
The transition from general elderly welfare to enforceable nutritional rights remains incomplete in Iran. Despite broad policy objectives,9 there is a significant legal gap in protecting the specific nutritional needs of the elderly within the domestic framework, particularly when compared to international legal instruments.10
Overall, these findings indicate that while aging has been integrated into Iran’s national policy agendas, nutrition-specific programming remains under-prioritized and inadequately operationalized. The transition from a curative-centric to a preventive-geriatric model is required to achieve nutrition equity and functional well-being among the elderly.
Policy Implications and Recommendations
The findings of this content analysis underscore an urgent need for a paradigm shift in Iran’s aging policies, transitioning from fragmented, curative-oriented approaches toward integrated, evidence-based, and equity-oriented nutritional frameworks.1,11 To address the identified gaps, we propose a tiered hierarchy of recommendations, categorized by their implementation urgency and scope:
Tier 1: Immediate Clinical and Operational Interventions (Short-Term)
The most pressing priority is the clinical operationalization of nutrition within the existing healthcare infrastructure.
- Systematic Screening: Routine nutritional screening must be integrated into primary healthcare (PHC) services for older adults. This should utilize validated tools to assess dietary intake, anthropometric indicators, and functional outcomes, facilitating the timely identification of malnutrition.8,24
- Referral Pathways: Effective screening must be coupled with structured referral pathways to dietitians and community nutrition programs to ensure that identified needs translate into actionable care.8,24
- Workforce Capacity: To support these clinical changes, immediate efforts should be directed toward enhancing the capacity of the healthcare workforce. Training physicians, nurses, and community health workers in geriatric nutrition and functional assessment is essential for delivering age-appropriate care.1,12
Tier 2: Structural and Regulatory Frameworks (Medium-Term)
Once clinical protocols are established, the focus must shift toward creating a formal regulatory environment conducive to sustainable nutritional support.
- National Geriatric Guidelines: There is a critical need to develop national, age-specific dietary guidelines. These must move beyond general population advice to address the unique physiological needs of older adults, such as protein adequacy for sarcopenia prevention, micronutrient sufficiency, and hydration management.6,23
- Measurable Targets: Policymakers should transition from qualitative goals to measurable, time-bound nutrition targets to ensure accountability and enable evidence-based monitoring and evaluation.6,23
Tier 3: Socioeconomic and Intersectoral Integration (Long-Term)
The final tier involves addressing the systemic determinants of nutrition through broad-scale social and political integration.
- Social Nutrition Support: To tackle socioeconomic disparities, social protection systems must be linked to nutrition outcomes. This includes targeted food assistance, subsidies for nutrient-dense foods,29 and community-based meal programs for vulnerable elderly cohorts.7,11
- Intersectoral Governance: Long-term success requires a formal, multisectoral framework that synchronizes the efforts of the health, social welfare, and food security sectors. Such coordination is vital to ensure that nutrition-sensitive programs are embedded within the broader national aging strategy, thereby promoting equity and maximizing functional well-being.11,23
As synthesized in Table 1, although Iran has established a robust PHC infrastructure for elderly care, a critical misalignment persists between general health policies and the specialized nutritional requirements of an aging population. This gap is further detailed through a five-dimensional analysis of the current policy landscape.
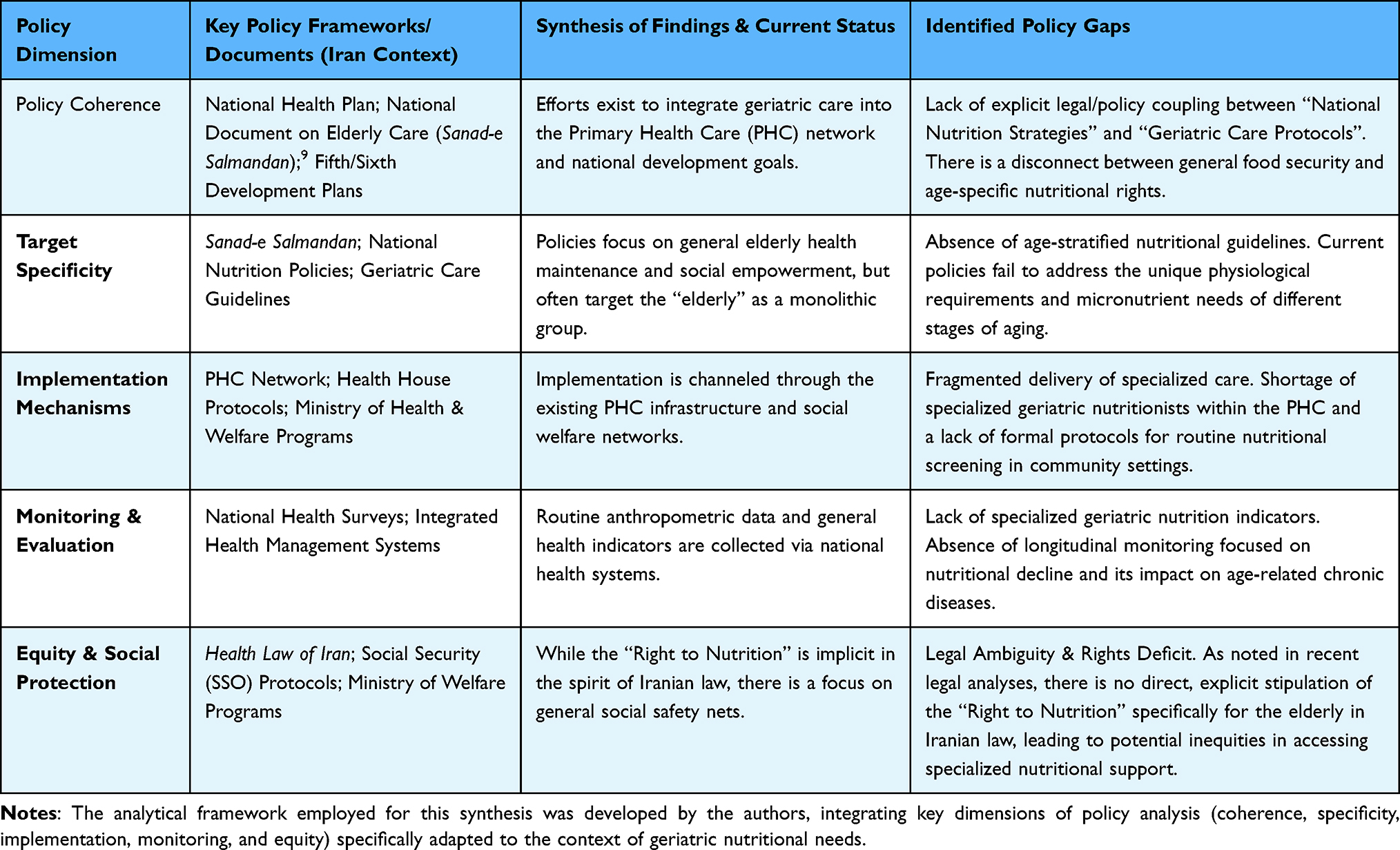 |
Table 1 Synthesis of Policy Frameworks, Identified Gaps, and Alignment with the 5-Dimensional Analytical Model |
While the National Document on Elderly Care in Iran provides a comprehensive strategic roadmap encompassing social empowerment, economic security, and health promotion, it exhibits a notable “implementation gap” regarding specialized nutritional interventions. Although the document emphasizes the holistic well-being of the elderly, it lacks granular, age-specific protocols required to bridge the gap between general food security and the complex micronutrient requirements of the aging population. Consequently, the strategic objectives outlined in the National Document remain largely aspirational in the context of geriatric nutrition, primarily due to the absence of integrated clinical and community-based nutritional guidelines.9
Study Limitations
This study has several limitations that should be acknowledged. First, the analysis was primarily based on publicly available policy documents; thus, it may not have captured internal ministerial reports, strategic memos, or non-public administrative guidelines that could offer further nuances regarding the implementation of geriatric nutrition programs. Second, while the study evaluates the formal policy landscape, it does not assess the actual fidelity of policy implementation at the grassroots level or the lived experiences of older adults and healthcare providers. Finally, the rapid pace of policy shifts in response to demographic transitions may require periodic updates to this analysis. Despite these limitations, this study provides a comprehensive baseline for understanding the current status and addressing the systemic gaps in Iran’s geriatric nutrition policy.
Conclusion
Iran is undergoing a rapid demographic transition that necessitates the integration of nutrition as a central pillar of aging policy.8,11,23 While foundational frameworks like the Integrated Elderly Health Care Program exist, our analysis highlights that current nutrition-related objectives for older adults remain fragmented and insufficiently operationalized, limiting the health system’s capacity to optimize functional ability and quality of life.1,6,8,16,24
To bridge these gaps, Iran should further align its national aging policies with international frameworks, such as the WHO Decade of Healthy Ageing (2021–2030). A prioritized, tiered pathway is recommended: starting with the integration of routine nutritional screening and workforce training; advancing to the development of formal geriatric nutrition guidelines; and ultimately, sustaining these efforts through robust intersectoral governance and social protection measures.1,8,11,12,24
In conclusion, embedding nutrition at the core of aging policy is a strategic imperative for reducing socioeconomic inequalities and fostering sustainable, functional aging in Iran.1,7,23 Furthermore, the five-dimensional analytical framework presented in this study encompassing policy coherence, target specificity, implementation mechanisms, monitoring and evaluation, and equity offers a replicable roadmap for researchers in other middle-income countries to systematically evaluate and strengthen their own geriatric nutrition policies.1,11
Disclosure
The authors report no conflicts of interest in this work.
References
1. United Nations, Department of Economic and Social Affairs, Population Division. World Population Ageing 2023. New York: United Nations; 2023.
2. Bloom DE, Chatterji S, Kowal P, et al. Macroeconomic implications of population ageing and selected policy responses. Lancet. 2015;385(9968):649–10. doi:10.1016/S0140-6736(14)61464-1
3. Beard JR, OfficerA, Araujo de Carvalho I, et al. The World report on ageing and health: a policy framework for healthy ageing Lancet. 2016; ;387(10033):2145–2154. doi:10.1016/S0140-6736(15)00516-4
4. Morley JE. Undernutrition in older adults. Fam Pract. 2012;29(Suppl 1):i89–i93. doi:10.1093/fampra/cmr054
5. Volkert D, Beck AM, Cederholm T, et al. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin Nutr. 2019;38(1):10–47. doi:10.1016/j.clnu.2018.05.024
6. Kaiser MJ, Bauer JM, Rämsch C, et al. Frequency of malnutrition in older adults: a multinational perspective using the mini nutritional assessment. J Am Geriatr Soc. 2010;58(9):1734–1738. doi:10.1111/j.1532-5415.2010.03016.x
7. Hickson M. Malnutrition and ageing. Postgrad Med J. 2006;82(963):2–8. doi:10.1136/pgmj.2005.037564
8. WHO Regional Office for the Eastern Mediterranean. A strategy for active, healthy ageing and old age care in the Eastern Mediterranean Region 2006-2015. Available from: https://www.emro.who.int/elderly-health/strategy/ageing-health-strategy.html.
9. Tehran: Secretariat of the National Council of the Elderly. سند ملی سالمندان + نهایی [National Document for the Elderly] Available from: https://snce.ir/?page_id=23369.
10. Malekshah A. The status of the right to nutrition for the elderly in Iranian law and international instruments. Health Law J. 2025;3(3):21.
11. World Health Organization. Decade of Healthy Ageing 2021–2030. Geneva: WHO; 2020.
12. World Health Organization. (2015). World Report on Ageing and Health. Geneva: WHO.
13. Organisation for Economic Co-operation and Development. The Economic Benefit of Promoting Healthy Ageing and Community Care. Available from: https://www.oecd.org/en/publications/the-economic-benefit-of-promoting-healthy-ageing-and-community-care_0f7bc62b-en.html.
14. Cederholm T, Jensen GL, Correia MITD, et al. GLIM criteria for the diagnosis of malnutrition–a consensus report from the global clinical nutrition community. J Cachexia Sarcopenia Muscle. 2019;10(1):207–217. doi:10.1016/j.clnu.2018.08.002
15. Samouei R, Keyvanara M, et al. Aging, Health System, Challenge, Future, Iran, Qualitative Research. Iranian Journal of Ageing. 2022;16:4 608–623 Persian. doi:10.32598/sija.2022.3270.1
16. Foroumandi E, Alizadeh M, Khodayari-Zarnaq R, et al. Process evaluation of a national elderly nutrition–care program in Iran. Risk Manag Healthcare Policy. 2020;13:2347–2358. doi:10.2147/RMHP.S261121
17. Amirkalali B, Sharifi F, Fakhrzadeh H, Mirarefin M, Ghaderpanahi M, Larijani B . Evaluation of the Mini Nutritional Assessment in the elderly, Tehran, Iran. Public Health Nutr. 2010 ;13(9):1373–1379. doi:10.1017/S1368980010000303
18. Payette H, Shatenstein B. Determinants of healthy eating in community-dwelling elderly people. Canad J Public Health. 2005;96(Suppl 3):S27–S31.
19. Lee JS, Frongillo EA. Nutritional and health consequences of food insecurity among older adults. J Nutr. 2001;131(5):1503–1509. doi:10.1093/jn/131.5.1503
20. Kheirandish M, Dastsouz, F, Azarbad, A, et al. The association between dietary patterns and metabolic syndrome among Iranian adults, a cross-sectional population-based study (findings from Bandare-Kong non-communicable disease cohort study). BMC Endocr Disord. 2024, ;24():
21. Micha R, Peñalvo JL, Cudhea F, et al. Association between dietary factors and mortality from heart disease, stroke, and type 2 diabetes. JAMA. 2017;317(9):912–924. doi:10.1001/jama.2017.0947
22. Ariya M, Shahraki HR, Farjam M, et al. Dietary inflammatory index and metabolic syndrome in Iranian population (Fasa Persian Cohort Study). Sci Rep. 2020;10(1):16762. doi:10.1038/s41598-020-73844-0
23. Food and Agriculture Organization of the United Nations. Food-Based Dietary Guidelines: Iran. Rome: FAO; 2015.
24. Ministry of Health and Medical Education (MOHME). Integrated Elderly Health Care Program (SIB System). Tehran: MOHME; 2018.
25. Vicerra PM, De Pano JC, Estanislao JM. Nutrition status of lower-income older adults in Thailand during COVID-19 pandemic. Asian J Soc Health Behav. 2022;5(4):147–153. doi:10.4103/shb.shb_150_22
26. Harnirattisai T, Vuthiarpa S, Pawloski LR, et al. Nutritional health risk (food security) in Thai older adults and related factors. Nutrients. 2024;16(16):2703. doi:10.3390/nu16162703
27. Larpsombatsiri K. Policies on health of older adults in Thailand. In
28. Zarei M, Qorbani M, Djalalinia S et al. Food insecurity and dietary intake among elderly population: a systematic review. Int J Prev Med. 2021;12:8. doi:10.4103/ijpvm.IJPVM_61_19
29. Darmon N, Drewnowski A. Contribution of food prices and diet cost to socioeconomic disparities in diet quality. Am J Clin Nutr. 2015;92(5):1185–1192.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.