Back to Journals » Journal of Healthcare Leadership » Volume 18
Nursing Students’ Experiences of in situ Simulation Training in Leadership Practice: A Qualitative Explorative Study
Authors Eid HR ![]() , Raaen AH, Grevskott T
, Raaen AH, Grevskott T ![]() , Bjørgum M, Myrvold LM, Øvereng IA
, Bjørgum M, Myrvold LM, Øvereng IA ![]() , Lysfjord EM
, Lysfjord EM ![]()
Received 21 February 2026
Accepted for publication 6 May 2026
Published 8 June 2026 Volume 2026:18 604428
DOI https://doi.org/10.2147/JHL.S604428
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Pavani Rangachari
Hege Rasmussen Eid,1 Ann Helen Raaen,2,* Torhild Grevskott,2,* Marthe Bjørgum,3,* Line Merete Myrvold,4,* Ingunn Almli Øvereng,4,* Else Marie Lysfjord1
1Faculty of Nursing and Health Sciences, Nord University, Namsos, Norway; 2Faculty of Nursing and Health Sciences, Nord University, Levanger, Norway; 3Faculty of Nursing and Health Sciences, Nord University, Bodø, Norway; 4Nord-Trøndelag Health Trust, Namsos Hospital, Namsos, Norway
*These authors contributed equally to this work
Correspondence: Hege Rasmussen Eid, Faculty of Nursing and Health Sciences, Nord University, Postbox 474, Namsos, 7801, Norway, Email [email protected]
Purpose: Developing leadership and management skills among nursing students is increasingly recognized as essential for their future roles as professional nurses. Meanwhile, simulation-based learning has emerged as a valuable pedagogical approach in nursing education. This study aimed to explore third-year nursing students’ experiences of in situ simulation training in leadership practice.
Methods: A qualitative explorative design was used. Nursing students (n = 26) participated in focus group interviews after completing simulation training. Data was collected using semi-structured interview guides; content analysis was conducted to identify key themes.
Results: Three themes emerged: prepared for reality, beneficial learning, and development of leadership competence. The themes showed how, by engaging in realistic scenarios, students gained deeper self-insight, strengthened their ability to connect theory with practice, and developed greater confidence in managing complex clinical situations.
Conclusion: In situ simulation appears to be an effective approach for enhancing nursing students’ leadership competence and professional development. The findings suggest that simulation supports the formation of professional identity and facilitates the transition from education to nursing practice.
Keywords: nursing leadership, simulation, clinical placement, nursing students
Introduction
Teaching leadership and management skills is an integral part of nursing education as they underpin students’ preparedness for their future roles as professional nurses.1 Rapidly changing roles and increasing expectations regarding healthcare quality amplify the need for effective nursing leadership within health services.2 In this context, decisive nursing leadership plays a significant role, as it influences critical processes as in task delegation and coordination of clinical work.3 From a systems perspective, improved task distribution within health and care services has been identified as crucial for achieving sustainable services, underscoring leadership competence as a prerequisite for successful implementation.4 Specifically, the transfer of tasks between personnel and professional groups requires leadership competence, transparent decision-making processes, and regular quality control.5 The absence of these prerequisites can undermine the potential benefits of task distribution, compromise quality, and, in the worst case, pose a risk to patient safety.6 In Norway, the Directorate for Higher Education and Competence has proposed national guidelines for nursing education,7 replacing the 2019 regulation. While leadership was previously described as a part of general competence, the new guidelines elevate it to a distinct area of competence, representing a significant strengthening of expectations compared to the previous regulation. The guidelines introduce explicit requirements for comprehensive knowledge of leadership and organizational structures, embedding leadership throughout the curriculum in both theory and practice. Students are expected to develop skills in leading, prioritizing, and coordinating healthcare services, with a strong emphasis on patient safety, quality improvement, and interdisciplinary collaboration.
Newly qualified nurses typically face a range of challenges in transitioning from students to professional nurses. Increasingly complex patient cases and specialized healthcare systems demand advanced knowledge and strong self-management skills.8–10 Research suggests that many newly qualified nurses feel underprepared for this complexity, often experiencing insecurity and uncertainty regarding patient care and independent work.11,12 These challenges can lead to doubts about remaining in the profession.13
A recent review by Costa et al14 highlights that fostering leadership competencies require structured, student-centered pedagogical methods and systematic evaluations. Curriculum reform and innovative teaching strategies are needed to prepare nursing students for future leadership roles.14 Against this background, simulation-based learning (SBL) is recognized as a valuable pedagogical approach in nursing education. SBL is effective as it tries to imitate real situations, enabling students to apply knowledge and develop practical skills in a safe environment.15 Compared to traditional classroom-based teaching, SBL can reduce the gap between theory and practice. By creating opportunities for experienced nurses, new graduates, and students to learn together,16 it also provides training in interprofessional collaboration and communication, which are key factors in preventing adverse events in healthcare.17
Previous reviews suggest that SBL in relation to nursing leadership and management education could foster key competencies such as delegation, teamwork, collaboration, decision making, problem solving, and communication within a safe learning environment.18 Similar conclusions are drawn in a more recent review by Riaz and Tabassum,19 which indicates that SBL is a feasible approach for leadership training among undergraduate students and may enhance students’ leadership-related skills and confidence.19 Nevertheless, the number of included studies remains small.18,19 Taken together, these findings point to a clear need for further research examining how SBL can support leadership practice in nursing education. This study aims to explore third-year nursing students’ experiences of in situ simulation training in leadership practice to shed light on the use of simulation as a pedagogical approach to leadership.
Method
This study employed an exploratory qualitative design to explore students’ experiences of learning and leadership development through simulation-based training20 and was reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ).21
Context and Research Design
This study is based on a project which was conducted from January 2023 to December 2025. This was a collaboration project between a university and two hospitals in the middle of Norway. The project aimed to explore the possibility of improving bachelor students’ abilities to develop their leadership competence through in situ simulation.
During the final semester, the bachelor students at the university perform a five-week clinical practice in nursing leadership and service development.22 The key themes in the learning outcomes are quality and patient safety, service development and innovation, understanding organizational structure and workflow, prevention of adverse events and user involvement, and interdisciplinary collaboration.
An important task in the project was to develop realistic simulation scenarios based on clinical, student, and pedagogical experiences. The collaboration involved project leaders and students from the university, as well as nurses from both hospitals. Scenario development took place in two phases: first, the group split into two teams and created initial scenarios in separate workshops; then, the full group met to discuss, refine, and select the final scenarios. These were further improved, documented in facilitator guides, and shared in a common Teams workspace accessible to all participants. Altogether, six scenarios were developed, one example is illustrated in Figure 1.
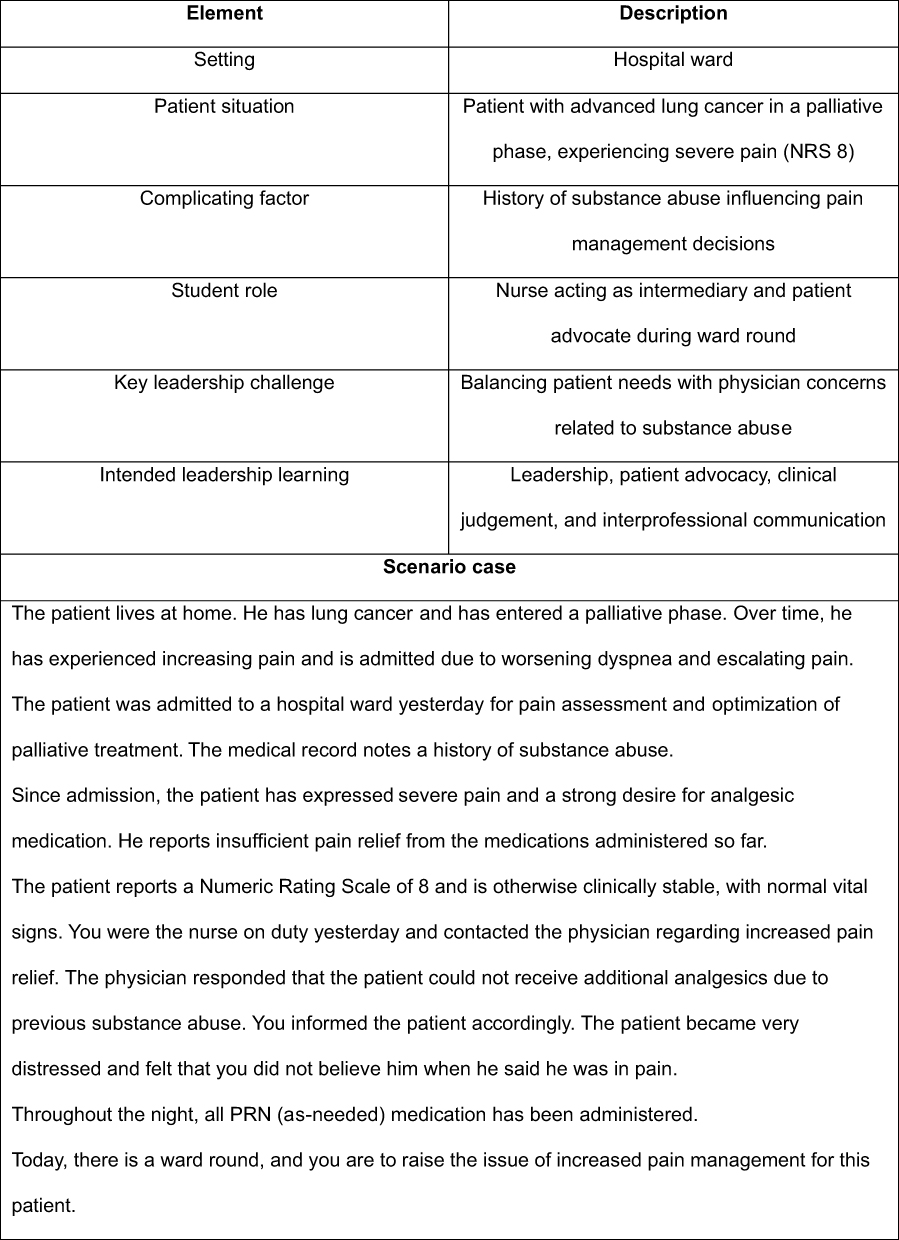 |
Figure 1 Example of scenario for simulation. |
Nurses with facilitator education from both hospitals and the university acted as facilitators and were responsible for conducting the simulations. The sessions were held in hospital environments at both hospitals and designed to be “in situ”. Prior to the simulation day, students received a letter with practical details, facilitator names, learning outcomes, and a clear message that the simulation focused on learning rather than assessment. Each simulation group consisted of 7–9 students. The project spanned two years and included two cohorts in their final semester of clinical practice in nursing leadership and service development (spring 2023 and spring 2024). Simulations were conducted during these semesters, with each simulation day comprising two or three scenarios. All activities—briefing, scenario execution, and debriefing—took place in the same room, with facilitators, simulators, and responders present throughout.
Following completion of the simulations, researchers conducted focus group interviews with students (26 in total).
Participants and Settings
Participants were recruited from the project by the first and the third author. The participants received verbal and written information about the project prior to their clinical practice. They also received verbal and written information about the opportunity for participating in the focus group interviews and that participation was voluntary. The participants were ensured that the participation of the simulation was not a part of the assessment of them in the clinical practice. All the students that were undertaking their clinical practice at the hospital wards included in the project were invited to participate in focus group interviews. In 2023, 20 students were invited and 9 participated. In 2024, 36 students were invited and 17 participated. The participants consisted of final semester bachelor students in nursing at the university, who were about to finish clinical practice in nursing leadership and service development. All participants provided informed consent through signed documentation. An overview of the participants is provided in Table 1.
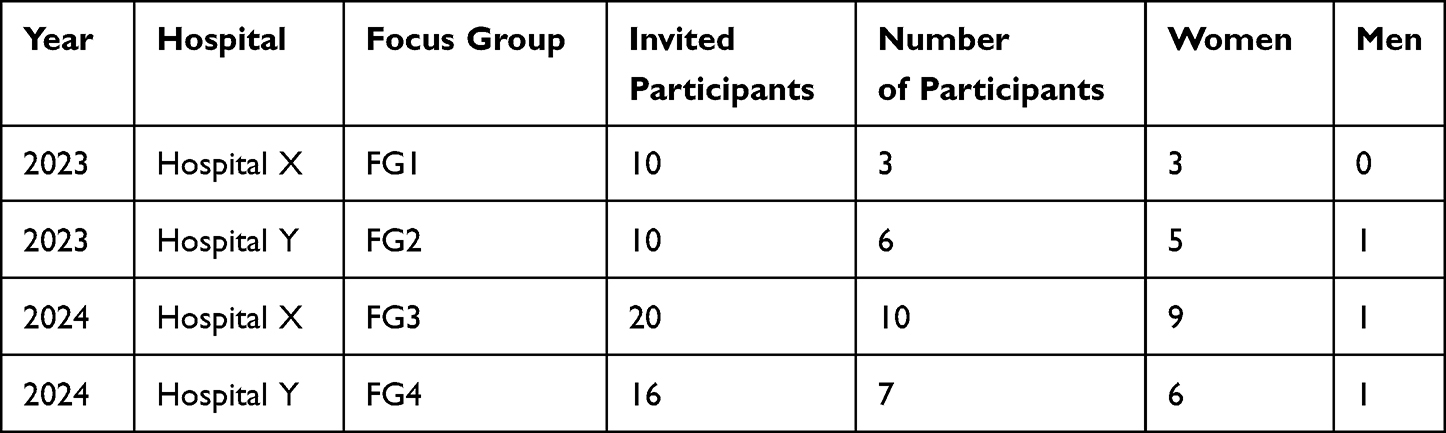 |
Table 1 Overview of Focus Group Interviews and Participants |
Data Collection
Data was gathered through four focus group interviews. Focus group interviews were conducted during the final days of the clinical placement, after formal assessment of the students had been completed. During spring 2023, focus group interviews 1 (FG1) and 2 (FG2) comprised participants performing their clinical practice in both hospitals respectively. Similarly, during spring 2024, focus group interviews 3 (FG3) and 4 (FG4) comprised participants performing their clinical practice in both hospitals, respectively. FG1, 2, 3, and 4 consisted of 3, 6, 10, and 7 students, respectively (n=26 in total) (Table 1). FG2 was performed by using Teams due to practical reasons, while FG1, FG3 and FG4 was performed by physical meeting with the students. The focus group interviews were performed by authors 1, 2, 3, and 4. Author 1 holds a Ph.D., authors 2, 3 and 4 are university lecturers, all employed at the university. Author 2 and 3 had participated in the simulations with the students. The interviews, lasting from 45–60 minutes, were recorded and transcribed using Nettskjema software.23 The interviews were conducted and transcribed in Norwegian language.
Ethics
The participants received both verbal and written information about the study and signed written confirmation of informed consent. The consent included permission for the publication of anonymized responses and direct quotes. Participation was voluntary, and the participants had the right to withdraw from the study at any time without consequences. The research protocol was approved by the SIKT (Norwegian Agency for Shared Services in Education and Research, ref nr: 835638).
Analysis
We conducted content analysis on the transcribed material, following the method of Graneheim and Lundman,24 which focuses on the manifest meaning in the material and results and aims to identify subcategories and categories through a close-to-text analysis.24 Firstly, all authors read the transcribed material and reflected together to obtain a sense of the whole. Then authors 1, 2 and 7 separately read the transcribed material and identified meaning units, which were words, sentences, or statements that related to the aim of the study. Author 1 and 2 participated in the focus group interviews, author 7 did not participate in the focus group interviews. In the next step, they discussed the identified meaning units and decided whether they were relevant to the aim of the study. Then they sorted the identified meaning units (which were related through their content and context) into sub-categories. Thereafter, they sorted the identified sub-categories, grouping those that were related into categories, and translated the meaning units, subcategories and categories into English language. Finally, authors 1, 2, 3, 4, 5, 6 and 7 read and reflected together upon the categories who represent the findings in the study. An example illustrating the analytic process is presented in Table 2.
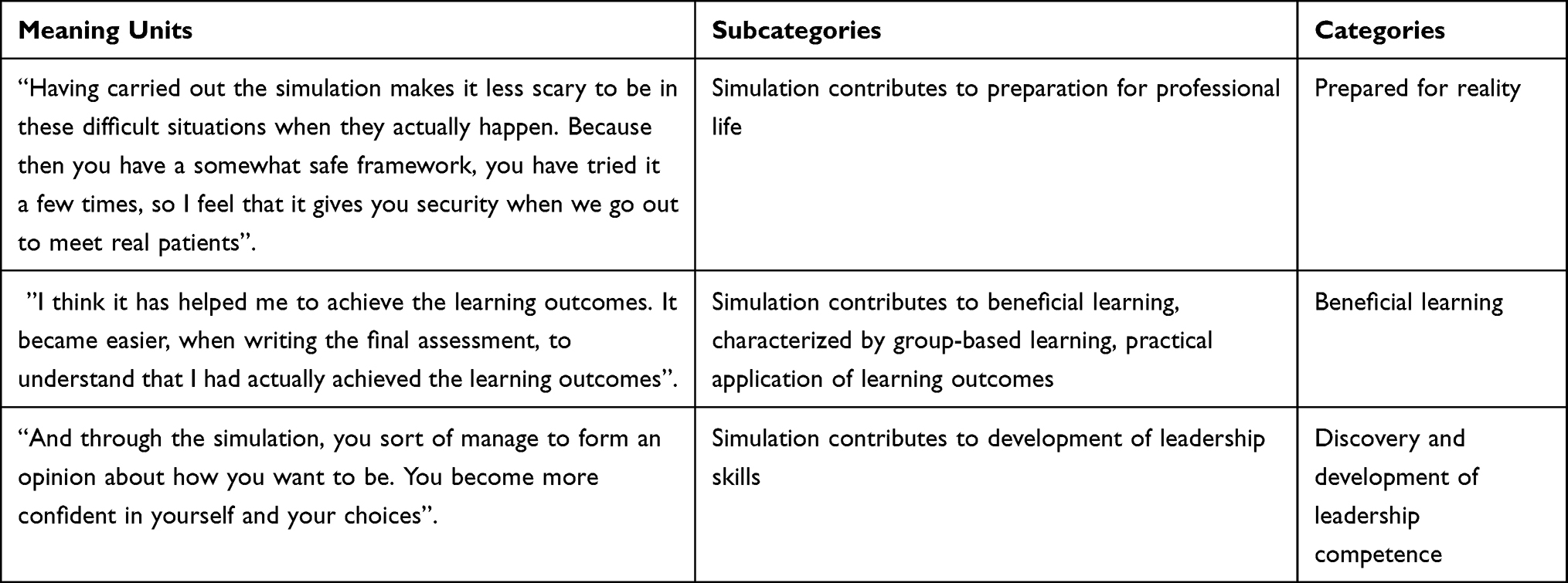 |
Table 2 Example of Content Analysis approach |
Findings
The content analysis identified three themes: prepared for reality, beneficial learning, and development of leadership competence. This section discusses each theme and illustrates them with extracts from the interviews.
Prepared for Reality
Participants emphasized the critical role of realistic simulation in fostering a sense of preparedness and confidence when encountering complex clinical situations. Engaging in simulations within safe and structured environments was perceived as instrumental in developing professional readiness. One participant described how prior simulation experience contributed to their sense of security:
Having gone through the simulation makes it less frightening to face these difficult situations when they actually happen. Because you’ve had the chance to try it a few times in a safe setting, I feel it gives a sense of security when we’re going out to meet real patients. (FG1)
Several students acknowledged the limitations of clinical placements in exposing students to the full range of possible situations they may encounter as nurses. Simulation was regarded as a vital supplement to these limitations of practice-based learning:
There are things that happen during one shift that don’t happen during another. Some situations are quite rare, and suddenly, you’re in it as a nurse, and you’ve never encountered it in practice before. (FG1)
Similarly, another student noted,
I appreciate being given the opportunity to simulate cases that we might not encounter until we enter working life, and to already have some experience of what it is like to be in situations that can at times feel somewhat uncomfortable. (FG3)
Simulations were seen as reflective of the inherent unpredictability in professional nursing practice, where quick decisions often need to be made without prior notice. As one participant noted,
There’s some learning in being thrown into it as well, because when we enter the workforce, no one is going to prepare you. We’re nearing the end [of our education], so maybe it’s good to have been thrown into it a bit. (FG1)
This sentiment was echoed by others who appreciated the opportunity to test their clinical reasoning in unexpected scenarios:
I think it’s a really smart approach. Because it’s true—we don’t know what kind of cases we’ll encounter when we start working. So, it’s good that we get to test ourselves a bit before we actually enter the workplace. (FG1)
This early exposure is particularly important given the emotional demands of nursing, where newly qualified nurses must learn to navigate challenging interactions, including dealing with distressed relatives, while managing their own emotional responses.
In this way, simulation exercises play a crucial role in preparing nursing students for the unpredictable and often challenging realities of clinical practice. Participants highlighted how repeated exposure to difficult situations in a controlled and safe environment reduced the fear associated with encountering such scenarios in real life. Students reported that engaging in simulation training for challenging situations fostered a sense of confidence. One student emphasized,
Going through the simulation makes it less frightening to face these difficult situations when they actually occur. You have already practiced them a few times in a safe environment, and I feel that this gives me confidence when we are about to meet real patients. (FG1)
Importantly, simulation not only familiarizes students with clinical scenarios but also supports the development of personal coping strategies and confidence. It provides tools that help individuals who may naturally feel apprehensive about confronting difficult situations. One participant noted,
Simulation can help those who feel anxious by providing them with tools and the opportunity to test them in advance. This way, you know more about what to expect in working life, and you may feel more confident when facing yourself, colleagues, patients, and the workplace … enabling them to approach their future roles with greater assurance and comfort, both for themselves and for those they care for. (FG3)
In addition to emotional preparedness, simulation contributed to expanding students’ practical skillsets and problem-solving abilities. One of the students conveyed,
You carry more tools in your toolbox when you encounter such a situation … then you do not have only one way of solving it, but several different approaches. (FG2)
Acting as the patient’s spokesperson is a central part of the nurse’s professional role, yet this can be experienced as a challenging activity, particularly for newly graduated or in-training nurses. As one participant expressed,
I do find it difficult sometimes, when you come in as a nurse, and you’re supposed to be the spokesperson for your patient. (FG3)
This highlights the emotional and professional weight of advocating for the patient’s needs and rights, especially in situations where nurses must engage with other healthcare professionals who may have differing perspectives.
One of the scenarios involved a patient in a palliative phase due to advanced lung cancer, admitted for pain management. The patient had a history of substance use and reported inadequate pain relief. A nurse had contacted the physician the previous day to request additional analgesics, but the request was declined due to the patient’s history. The patient was distressed and felt that no-one believed he was experiencing pain. During ward round, the nursing student (simulating as nurse) was expected to raise the issue of pain management. One of the students described her experience of holding the nursing role in this scenario as follows:
Yes, I was thinking about staying professional and not saying something like, “Surely you understand that Schedule III–IV drugs won’t help!” I had to stay factual and say something like, “I’ve given a lot of Schedule II medications without satisfactory effects—do you think Schedule III–IV will work?” I’m not sure I would have discussed it like that with a doctor in real life. (FG4)
This case also shows how simulation fostered empathy and ethical awareness. Another participant emphasized trust and compassion:
The patient did not feel believed in this case. The patient felt that we questioned everything and withheld care because he was a former substance abuser. I feel that much of what we have learned is that patients should not be in pain—especially not at the end of life. It is more about quality of life than quantity. (FG4)
These insights illustrate how simulation can deepen students’ understanding of patient-centered care and the complexities of symptom management at the end of life.
Overall, these reflections show that training and rehearsal, encountered through simulation, are important arenas for developing the courage and communication skills required to effectively take on the role of patient advocate. Simulation enhanced confidence, communication, and ethical awareness in the participants through realistic and emotionally challenging scenarios, helping them to develop resilience and practical skills. Simulation also provided a safe space to practice patient advocacy and professional dialogue, preparing the participants for clinical practice with competence and clarity.
Beneficial Learning
The students reported that the simulation supported their understanding of learning outcomes. They noted that the learning outcomes in the final clinical placement differed significantly from those in earlier placements and were perceived as difficult to grasp and achieve. Several participants expressed that the simulation made these learning outcomes more recognizable; this experience was useful when they wrote their assessment papers during their placement:
After the simulation, it became easier when I had to write the final assessment to actually understand that I have achieved the learning outcomes. (FG1)
The students also described the simulation as a foundation for understanding academic theory and applying it in their own context. One participant expressed that the simulation contributed to a clearer understanding of theory when revisiting academic texts:
I think you learn so much from simulation that makes sense if you read about it afterwards, because it’s difficult when you first read it. And then you have simulation and then, in a way, for me, a greater understanding. And then you can go back to your book and say, “Oh, now I understand what it says”. In a way, you get something to build on. So, I think simulations are good both for this subject, but also for disease learning, anatomy, and all those subjects. It helps us see the whole picture. (FG1)
The students also expressed a sense of enhanced understanding and confidence gained through the simulation experience, which provided them with more substantial knowledge, making the learning process more tangible and realistic. This hands-on approach made it easier for them to grasp and retain information:
I feel like I have more substance after simulation. Then I have, in a way, experienced it for real, even though it’s not real. At least for me, it’s much easier to learn when I have done something. (FG4)
Students described the simulation as a collaborative learning environment where they could observe others, give and receive feedback, and reflect together. This supported their ability to analyze situations and engage in constructive dialogue. Several students expressed a preference for SBL over traditional study assignments. They stated that simulations offered a more engaging and meaningful learning experience, describing how the practical nature of the simulation helped them understand and retain academic content more effectively:
I would much rather have simulation than study assignments. You learn so much more from simulation than sitting at home and just writing, reading from the book and referring to sources that I have done a million times before. Simulation goes much deeper. (FG4)
Students described how participating in simulation supported their learning by strengthening their ability to critically assess and evaluate situations during clinical placement. In one of the scenarios, a nurse discovered that a close colleague had not replaced the peripheral venous catheters with several patients, resulting in infections. The nurse felt uncomfortable reporting this as a deviation, and in the scenario, she discussed with colleagues whether it should be reported or not. One colleague argued against reporting it, while another argued in favor. During simulation of this scenario, the students recognized the importance of documenting deviations to prevent future occurrences and viewed this as an opportunity for collective learning and improvement, even if reporting the deviation may have felt uncomfortable:
I argued that it might be wise to document the deviation, considering the future and that it shouldn’t happen again, that it could be a little wake-up call for everyone. (FG4)
In summary, participants reported that the simulation enhanced their understanding of learning outcomes, helped them connect theory with practice, and increased their confidence. The hands-on, collaborative nature of the simulation made learning more meaningful and easier to recall.
The experience also strengthened their ability to critically evaluate clinical situations and recognize the importance of actions such as documenting deviations.
Development of Leadership Competence
The simulation of the scenario centered on deviation management clarified that such reporting is intended to address systemic issues rather than individual shortcomings, thereby fostering a shift in perspective from personal accountability to organizational learning. Moreover, the simulation served to normalize and reduce apprehension associated with reporting deviations, as students became more aware of its constructive role in promoting transparency and continuous improvement within healthcare systems.
I was thinking about quality development work in such a big way, but then you realize that it can actually just be about reporting deviations, because those forces you to sharpen up or address routines. We received a new perspective on what quality development work really is about. (FG1)
Students found that participating in SBL activities contributed to a deeper understanding of the nature of leadership and highlighted key aspects to prioritize in their continued professional development:
The simulation helped provide insight into what leadership actually is, what our focus is, what we need to act on, and what we should prioritize. (FG3)
Students clearly described how the simulation heightened their awareness of others’ behavior, including both verbal and non-verbal communication. This increased attentiveness contributed to a deeper self-awareness regarding how they themselves might be perceived in a leadership role when interacting with colleagues. In this way, the simulation supported the ongoing development of their leadership style, as well as their ability to lead both themselves and others:
Leadership roles that you can recognize yourself in—like, “Oh … I don’t want to be like that”. When you simulated the supervisor or something … and then you realize what it might actually feel for the other person. So yeah, it’s something that reminds you that you need to work on becoming a different kind of leader. (FG2)
Students described how the simulation provided hands-on experience in organizing and facilitating departmental meetings, and how it helped them identify key elements necessary for creating a constructive and inclusive meeting environment, regardless of the topic being addressed. The emphasis was on establishing a safe and open atmosphere that encouraged participation and sharing of perspectives. Furthermore, students became increasingly aware of individual behaviors and body language, and how these non-verbal cues influenced group dynamics. This heightened awareness contributed to greater self-reflection on their own presence and conduct in leadership contexts:
The experience of organizing a meeting, how to include everyone, but also that it’s possible to talk to each person beforehand, so maybe people dare to say more about what’s really going on. yeah, a lot of good things came up during the debrief afterwards. So, you get kind of a psychoanalysis of how people behaved, both the good and the bad. I didn’t notice any change in body language from the “role-holder”, but you saw it, and the others could see it too, so it gave me something to think about. (FG2)
Students emphasized that participation in the simulation contributed to increased self-confidence and a stronger sense of autonomy. They expressed that the experience made them more likely to trust their own decisions in their future roles as nurses, as it fostered a greater sense of independence and professional readiness:
I don’t think we would have had the same reflections without the simulation. I don’t think we would have brought out the same perspective without it. And through simulation, you kind of form an idea of how you want to be yourself. You become, in a way, more confident in yourself and in your choices. (FG1)
In summary, the simulation deepened participants’ insights into leadership by increasing their awareness of quality improvement processes, communication, behavior, and their own leadership style. Through practicing meeting facilitation and observing group dynamics, they gained a clearer sense of how to create inclusive and constructive environments. Overall, the simulation strengthened the participants’ confidence, autonomy, and readiness to make informed decisions in future nursing roles.
Discussion
This section places the three themes identified in content analysis—prepared for reality, beneficial learning, and development of leadership competence—in context, describing their connections with findings from other relevant literature and practical implications.
Prepared for Reality
The findings suggest that participants perceived simulation-based leadership training as a vital form of preparation for future professional roles, supporting their readiness for the realities of the workplace. Exposure to realistic scenarios involving team leadership, unforeseen events, and decision-making under pressure appears to have strengthen participants’ confidence and self-efficacy. These findings are consistent with previous research indicating that simulation-based leadership education enhances decision-making, communication, and prioritization skills in complex clinical settings.25,26 At the same time, it is important to note that simulation represents an artificial learning environment, and participants are aware that the situation does not involve real patients or real clinical consequences. This artificiality may influence how leadership challenges are experienced and should be considered when interpreting the findings. On the other hand, the participants reported that opportunities to practice leadership in comparable situations were limited in clinical practice. From this perspective, simulation-based training may offer a particularly valuable, and in some cases the only, structured opportunity to develop such competencies.
SBL also supplements theoretical learning; as concluded in Daneshfar and Moonaghi’s review,27 SBL plays a significant role in narrowing the theory-practice gap. The review highlights that realistic, structured simulations, particularly high-fidelity formats, enhance students’ clinical competence by improving decision-making, confidence, practical skills, and the ability to integrate theoretical knowledge into practice. Additionally, simulation fosters empathy and communication skills through patient-centered scenarios. Among the various approaches, high-fidelity simulation and well-designed scenarios with guided debriefing were found most effective, while emerging methods such as virtual reality and gamification show promise for engagement and experiential learning.27
Another important contribution of the findings is that simulations seemed to reframe participants’ understanding of patient safety incidents (PSIs) as a collective and system-oriented practice, rather than exercise in individual blame.
According to Espin et al’s review,28 students identify fear of negative consequences, focus on individual rather than systemic factors, and other nurses’ perceptions as barriers for reporting PSIs.28 This is supported by the findings of Gradišnik et al,29 who also highlight the need for developing a professional culture shared by universities and healthcare institutions regarding PSI reporting, in order to support open communication and reflection Such an environment can increase students’ confidence in reporting PSIs, preparing future nurses to prioritize patient safety.29 Our findings suggest that simulation may contribute to such a professional culture.
Our participants valued the opportunity to practice patient advocacy during simulation. This role, central to nursing practice, was often perceived as challenging, particularly when it involved negotiating with other healthcare professionals. Through simulating advocating adequate pain management for a palliative patient with a history of substance use, participants experienced the complexity of balancing professionalism, communication, and patient rights. Participants reported that these simulations helped them develop confidence and strategies for speaking up on behalf of patients, a skill they were unsure they would have been able to apply effectively in real clinical settings without prior practice. This finding aligns with theoretical perspectives on patient advocacy, which emphasize the nurse’s role in safeguarding patient rights and mediating between patients and other healthcare professionals. Abbasinia et al30 identify “mediating” as a key attribute of advocacy, involving communication of patient preferences and needs to the healthcare team. Professional competence, effective communication skills, self-confidence, and autonomy are fundamental prerequisites for nurses to successfully advocate for their patients.30
Beneficial Learning
The findings indicate that participants were aware of the limitations of clinical practice`s exposure to complex leadership situations. Simulation was therefore viewed as a meaningful mechanism for bridging this gap by enabling deliberate practice and reflection on leadership challenges in controlled, realistic settings. SBL has emerged as a transformative pedagogical strategy in healthcare education, particularly in addressing the persistent gap between theoretical instruction and clinical practice. This gap often stems from the limited opportunities students have to apply classroom knowledge in real-world settings, especially in complex, high-risk, or ethically sensitive scenarios.31 Simulation cases targeting difficult-to-practice situations offer a realistic, safe, and structured environment where students can develop clinical reasoning, apply theoretical concepts, and build confidence. The mechanisms through which simulation bridges the theory–practice gap are multifaceted and deeply impactful.32
One of the most significant advantages of SBL is its ability to replicate clinical situations that are rare, unpredictable, or ethically challenging, such as being the patient’s spokesman. Other situations might be acute care, emergency scenarios, managing multiple patients, and leading interprofessional teams under time pressure.19 By practicing during simulation, students may gain the competence needed to respond effectively when such situations arise in real work life.33
The simulations in our study can be classified as low-fidelity simulations. High-fidelity simulations, which mimic real-life clinical environments with advanced technology and detailed scenarios, entail substantially higher costs related to technical equipment, maintenance, and personnel training.34 Several studies demonstrate that simulation fidelity is not necessarily decisive for knowledge acquisition among nursing students.34–36 This potentially addresses a recurring concern regarding simulation as a pedagogical approach, namely the financial burden associated with equipment, technology, instructors, and facilities.37 In the present project, costs were minimal because the simulation did not involve advanced medical equipment and was facilitated by clinical supervisors and educators with facilitator competence.
Notably, SBL, as an active and engaging learning approach, may be more effective than traditional clinical placements, where students tend to observe rather than actively participate. Simulation therefore supports a holistic learning process, enabling students to bridge abstract concepts with concrete actions.38 Critical thinking and decision-making are core competencies in healthcare, yet they are challenging to cultivate through didactic instruction alone. SBL encourages learners to prioritize tasks, assess risks, and communicate effectively with team members. The iterative nature of simulation, where students can repeat scenarios and refine their approaches, supports the development of clinical judgment.33 In a scenario simulating leadership-related issues (as implemented in the present study), this often involves time-sensitive decisions, unpredictable patient or colleague responses, and requiring students to adapt and think on their feet. Students in our study reported increased self-confidence after engaging in SBL. Increased confidence translates into greater preparedness and autonomy in clinical settings, ultimately enhancing patient care outcomes.38 The debrief was highlighted as particularly important for the learning process by participants. Debriefing is a critical component of SBL that reinforces learning and bridges the gap between theory and practice. This reflective process helps learners internalize lessons, recognize areas for improvement, and understand the rationale behind clinical decisions. Debriefing also fosters a culture of openness and continuous learning, encouraging students to view errors as opportunities for growth. By linking theoretical knowledge to experiential insights, debriefing solidifies the educational value of simulation and enhances its impact on professional development.31
Development of Leadership Competence
The findings show that participation in simulation training provided students with new insights into learning outcomes related to leadership competence, and helped them discover new dimensions in leadership, self-leadership, and their own roles and responsibilities within it. According to a recent review by Abdul-Rahim et al,1 simulation is an important and safe method for helping nursing students develop leadership and management skills1 Our findings show that successful simulations depend on a safe environment, professionalism of facilitators, and relevant scenarios. The need for careful design with realistic scenarios, preferably developed in collaboration with clinicians, is emphasized by other studies.1,27 In this way, the design of the scenarios and simulations in our study could have been the underlying reason behind the students’ new insights into leadership and learning outcomes.
This aligns with Vygotsky’s sociocultural perspective on learning, which claims that learning does not occur in isolation within the individual, but through interaction with others and the cultural context. Vygotsky’s concept of the “zone of proximal development” highlights the importance of guidance and support from more knowledgeable others (teachers or peers) in the learning process. Learning occurs not only through direct instruction, but also through observation and participation in cultural practices.39 Social interaction is essential for the development of higher mental functions, and language serves as a tool for thinking.40 The sociocultural view of learning also emphasizes the significance of context and the tools used in the learning process, and how these contribute to the development of knowledge and skills.41
Our findings show that students experienced a greater sense of security during the simulation sessions compared to previous experiences in campus settings. This increased psychological safety was attributed to factors such as smaller group sizes, the explicit clarification that the simulation was not part of formal assessment, previous experience of simulation learning on campus, and the presence of the facilitators. The fact that students were less worried about performing this simulation than former simulations may indicate that they achieved “team psychological safety”,42 a condition in which team members feel safe to take interpersonal risks, such as asking questions, admitting mistakes, and sharing ideas, without fear of being humiliated or punished. Team psychological safety is built on mutual respect and trust and differs from group cohesion, which can lead to “groupthink”. When psychological safety is high, learning and innovation increase because people feel free to be open and collaborate. This is essential for the team’s development and performance.42
Methodological Considerations
This study employed a qualitative design to explore students’ experiences of learning and leadership development through simulation-based training. The chosen design was considered appropriate for gaining in-depth insight into how students perceived, interpreted, and reflected on their learning experiences in a complex educational and clinical context. Several strategies were employed to enhance trustworthiness, including careful consideration of interviewer roles, reflexive discussions within the research team, and systematic analytic procedures. Nevertheless, as with all qualitative research, it cannot be fully ruled out that the research context, interactional dynamics, and the researchers’ involvement may have influenced the data and interpretations. Despite efforts to reduce potential interviewer bias and power imbalances, such influence cannot be entirely excluded. Even if the students received rich information about the project, the simulation and the voluntarily of participation in the focus group interviews, they might still have felt pressured to respond in a certain way due to the teacher’s position of authority, leading them to withhold criticism and provide responses they believe the teacher expects. This dynamic can influence the honesty of student responses and, consequently, the reliability of the data. However, the responsibility for daily assessment during clinical practice rested with nurses (clinical supervisors) at the wards who were not involved in the interviews. Also, the credibility of the study is strengthened by the fact that students independently communicated to clinical supervisors, peers, and other instructors in various contexts that the leadership simulation was valuable for learning. The data material was characterized by rich and detailed descriptions, including both positive experiences and critical reflections on existing teaching and learning approaches. The presence of critical perspectives suggests that participants felt able to express their views openly. This aligns with findings from the interviews and increases our confidence that the focus group data reflect the students’ genuine experiences. The authors analyzing the material represented varying degrees of involvement in the simulation and data collection, which may have both enriched the analysis through multiple perspectives and reduced the risk of bias. At the same time, such variation may also have influenced how the data were interpreted, underscoring the importance of collaborative reflection and discussion of emerging findings. Transparency was further supported through detailed descriptions of the analytic process and the use of illustrative quotations, enabling readers to follow the analytic reasoning and assess the grounding of the findings in the data.
Implications for Practice and Future Research
These findings highlight the need for universities and clinical settings to co-create realistic simulation scenarios in nursing leadership to ensure relevance, quality, and consistent learning outcomes. Joint ownership and initiative from both partners are essential to secure alignment with real clinical demands when it comes to nursing leadership. Simulations should be planned and performed within a psychologically safe learning environment and facilitated by experienced educators who can guide the debrief, reflection, and feedback. Future research may benefit from longitudinal and mixed-method designs to further explore the transfer and sustainability of leadership learning from simulation-based training.
Conclusion
This study suggests that in situ SBL is a valuable approach for developing nursing students’ leadership competence and strengthening their professional growth. Through realistic and emotionally engaging scenarios, students gained deeper insight into their own leadership behavior, enhanced their ability to integrate theory with practice, and developed greater confidence in handling complex clinical situations. The simulation experience also supported the formation of professional identity by helping students explore their role as leaders, colleagues, and advocates for patient safety. Overall, the findings show that simulation offers a meaningful and supportive arena for practicing decision-making, communication, and accountability, and thereby contributes to the transition from education to professional nursing, giving students adequate leadership competence.
Funding
The project was funded by The Liaison Committee for Education, Research and Innovation in Central Norway, reference number 2023/229-2806/2023 The funding for the article processing charges was provided by Nord University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Abdul-Rahim HZ, Sharbini SH, Ali M, Hashim SH, Abdul-Mumin KH. Leadership and management skills for student nurses: a scoping review. BMC Nurs. 2025;24(1):111. doi:10.1186/s12912-024-02603-7
2. Sethi S, Chaturvedi DV, Kataria DP. A review of upskilling in the healthcare sector with special emphasis on nurses: life sciences. Int J Life Sci Pharma Res. 2023;13(special issue 6):L1–14. doi:10.22376/ijlpr.2023.13.4.SP6.L1-L11
3. Putri P, Afandi A. The positive impact of delegation in nursing: a literature review. DNurs Health J. 2023;4:58–66.
4. Wang B-L, Batmunkh M-U, Samdandash O, Divaakhuu D, Wong W-K. Sustainability of nursing leadership and its contributing factors in a developing economy: a study in Mongolia. Front Public Health. 2022;10:900016. doi:10.3389/fpubh.2022.900016
5. Leong SL, Teoh SL, Fun WH, Lee SWH. Task shifting in primary care to tackle healthcare worker shortages: an umbrella review. Eur J Gen Pract. 2021;27(1):198–210. doi:10.1080/13814788.2021.1954616
6. Malterud K, Aamland A, Fosse A. How can task shifting put patient safety at risk? A qualitative study of experiences among general practitioners in Norway. Scand J Prim Health Care. 2020;38(1):24–32. doi:10.1080/02813432.2020.1714143
7. Forskrift om nasjonal retningslinje for sykepleierutdanning [Regulation on the National Curriculum for Nursing Education]. FOR-2019-03-15-412. 2019.
8. Dogan P, Sendir M. Effect of different simulation methods in nursing education on critical thinking dispositions and self-efficacy levels of students. Think Skills Creat. 2022;45:101112. doi:10.1016/j.tsc.2022.101112
9. Hornstrup C, Storch J. Sammenhengende ledelse, tjenester og løsninger: relasjonell kapasitet i arbeidet med komplekse velferdsutfordringer. 1. utgave. ed. Kommuneforlaget AS; 2021.
10. Oh S, Lim J. Developing and evaluating a camp-style leadership enhancement program for nursing students. J Korean Acad Nurs Adm. 2019;25:52. doi:10.11111/jkana.2019.25.1.52
11. Oddvang TKK, Loftfjell A-LG, Brandt LM, Sørensen K. Nursing students’experience of learning ethical competence and person-centered care through simulation. Int Pract Dev J. 2021;11(2):Article7.
12. Thomas C, Hodson-Carlton K, Ryan M. Preparing nursing students in a leadership/management course for the workplace through simulations. Clin Simul Nurs. 2011;7(3):e99–e104. doi:10.1016/j.ecns.2010.06.005
13. Kyllingstad L, Kristoffersen M. Nyutdannede sykepleieres tanker om egen fremtid i sykepleieryrket. Nord Sygepl Forsk. 2022;12(4):1–14. doi:10.18261/nsf.12.4.5
14. Costa P, Sousa JP, Nascimento T, et al. Leadership development in undergraduate nursing students: a scoping review. Nurs Rep. 2025;15(5):160. doi:10.3390/nursrep15050160
15. Alharbi A, Nurfianti A, Mullen RF, McClure JD, Miller WH. The effectiveness of simulation-based learning (SBL) on students’ knowledge and skills in nursing programs: a systematic review. BMC Med Educ. 2024;24(1):1099. doi:10.1186/s12909-024-06080-z
16. Brown KM, Rode JL. Leadership development through peer-facilitated simulation in nursing education. J Nurs Educ. 2018;57(1):53–57. doi:10.3928/01484834-20180102-11
17. Oksavik WS, Heen C, Heggdal K. Faktorer som påvirker kommunikasjon og samspill i kirurgiske team med betydning for pasientsikkerhet – belyst fra operasjonssykepleierens ståsted. Klin Sygepleje. 2021;35(1):3–22. doi:10.18261/issn.1903-2285-2021-01-02
18. Labrague LJ. Use of simulation in teaching nursing leadership and management course: an integrative review. Sultan Qaboos Univ Med J. 2021;21(3):344–353. doi:10.18295/squmj.4.2021.007
19. Riaz S, Tabassum M. Effects of simulation-based education on improving leadership skills in medical and nursing students: a systematic review. J Exp Clin Med. 2024;40(4):783–791.
20. Polit DF, Beck CT. Essentials of Nursing Research: Appraising Evidence for Nursing Practice.
21. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
22. Nord University. Clinical Practice: nursing Management and Service Development, Community and/or Specialist Health Care Services. [Internet]. In. Available From: Clinical Practice: Nursing Management and Service Development, Community and/or Specialist Health Care Services | Nord.no - PRA2031. Bodø,Norway:Nord University
23. University of Oslo. Nettskjema. [Internet]. Oslo, Norway: University of Oslo; Available from: https://nettskjema.no/?lang=en.
24. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. doi:10.1016/j.nedt.2003.10.001
25. Jeffries P. Simulation in Nursing Education. Wolters Kluwer Health; 2020.
26. Tosterud R. Simulation used as a learning approach in nursing education: Students’ experiences and validation of evaluation questionnaires. Doctoral thesis, comprehensive summary. Karlstads universitet; 2015.
27. Daneshfar M, Moonaghi HK. The impact of clinical simulation on bridging the theory–practice gap in nursing education: a systematic review. BMC Med Educ. 2025;25(1):1216. doi:10.1186/s12909-025-07790-8
28. Espin S, Sears N, Indar A, Duhn L, LeGrow K, Thapa B. Nursing students’ experiences of patient safety incidents and reporting: a scoping review. J Nurs Educ Pract. 2019;10:26–35.
29. Gradišnik M, Fekonja Z, Vrbnjak D. Nursing students’ handling patient safety incidents during clinical practice: a retrospective qualitative study. Nurse Educ Today. 2024;132:105993. doi:10.1016/j.nedt.2023.105993
30. Abbasinia M, Ahmadi F, Kazemnejad A. Patient advocacy in nursing: a concept analysis. Nurs Ethics. 2020;27(1):141–151. doi:10.1177/0969733019832950
31. Brown JE. Graduate nurses’ perception of the effect of simulation on reducing the theory-practice gap. SAGE Open Nurs. 2019;5:2377960819896963. doi:10.1177/2377960819896963
32. Newton R, Krebs A. Bridging the theory-practice gap using simulation to teach care of patients with disabilities. Teach Learn Nurs. 2020;15(4):233–236. doi:10.1016/j.teln.2020.04.003
33. Koukourikos K, Tsaloglidou A, Kourkouta L, et al. Simulation in clinical nursing education. Acta Inform Med. 2021;29(1):15–20. doi:10.5455/aim.2021.29.15-20
34. Kardong-Edgren S, Anderson M, Michaels J. Does simulation fidelity improve student test scores? Clin Simul Nurs. 2007;3(1):e21–e24. doi:10.1016/j.ecns.2009.05.035
35. Lapkin S, Levett-Jones T. A cost-utility analysis of medium vs. high-fidelity human patient simulation manikins in nursing education. J Clin Nurs. 2011;20(23–24):3543–3552. doi:10.1111/j.1365-2702.2011.03843.x
36. Lapkin S, Levett-Jones T, Bellchambers H, Fernandez R. Effectiveness of patient simulation manikins in teaching clinical reasoning skills to undergraduate nursing students: a systematic review. Clin Simul Nurs. 2010;6(6):e207–e222. doi:10.1016/j.ecns.2010.05.005
37. Aggarwal R, Mytton OT, Derbrew M, et al. Training and simulation for patient safety. Qual Saf Health Care. 2010;19 Suppl 2:i34–43. doi:10.1136/qshc.2009.038562
38. Alrashidi N, Pasay An E, Alrashedi MS, et al. Effects of simulation in improving the self-confidence of student nurses in clinical practice: a systematic review. BMC Med Educ. 2023;23(1):815. doi:10.1186/s12909-023-04793-1
39. Rogoff B. The Cultural Nature of Human Development. Oxford University Press; 2003.
40. Wertsch JV. Voices of the Mind: A Sociocultural Approach to Mediated Action. Harvard University Press; 1993.
41. Lave J, Wenger E. Situated Learning: Legitimate Peripheral Participation. Cambridge University Press; 1991.
42. Edmondson A. Psychological safety and learning behavior in work teams. Adm Sci Q. 1999;44(2):350–383. doi:10.2307/2666999
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.