Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Nursing and PharmD Undergraduate Students’ Attitude Toward the “Do Not Resuscitate” Order for Children with Terminally Ill Diseases
Authors Abuhammad S ![]() , Muflih S
, Muflih S ![]() , Alzoubi KH
, Alzoubi KH ![]() , Gharaibeh B
, Gharaibeh B
Received 21 December 2020
Accepted for publication 28 January 2021
Published 24 February 2021 Volume 2021:14 Pages 425—434
DOI https://doi.org/10.2147/JMDH.S298384
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sawsan Abuhammad,1 Suhaib Muflih,2 Karem H Alzoubi,2 Besher Gharaibeh3
1Department of Maternal and Child Health, Jordan University of Science and Technology, Irbid, 22110, Jordan; 2Department of Clinical Pharmacy, Jordan University of Science and Technology, Irbid, 22110, Jordan; 3Department of Adult Health, Jordan University of Science and Technology, Irbid, 22110, Jordan
Correspondence: Sawsan Abuhammad Email [email protected]
Background: Nurses and Doctor of Pharmacy (pharmD) must communicate and properly documented the do not resuscitate orders for terminally ill children and their relatives. They also have to offer excellent care including more family support, assisting the child with terminally ill disease in passing on peacefully, and preventing unnecessary cardiopulmonary resuscitation. This research was aimed to survey attitudes of nursing and pharmD undergraduate students about the “do not resuscitate” order for children with terminally ill diseases.
Methods: A cross-sectional correlational design was used to study the correlation between attitude toward DNR and demographic variables. More than 400 nursing and pharmD students from Jordan University of Science and Technology were recruited in this study. All the participating students were e-mailed information regarding the study, including the web survey link.
Results: The results showed that there was a significant difference in perception toward do not resuscitate order between nursing and pharmD students (p ≤ 0.05). The pharmD students had more positive attitude toward do not resuscitate than the nursing students. Approximately, 60% of the nursing and pharmD students would disclose the need for the do not resuscitate order for children with terminally ill diseases Demographic variables were not associated with the perception toward do not resuscitate orders (p ≥ 0.05).
Conclusion: This study showed that Jordanian nursing and pharmD students are willing to learn more about different aspects of do not resuscitate orders for terminally ill children. Analyzing their responses to many items showed their misconception about do not resuscitate orders for terminally ill children.
Keywords: do not rusticate, cardiopulmonary resuscitation, nursing students, children, pharmD students
Introduction
A number of children under 20 years comprise 35% of the whole world population and 40% of the least-developed nations.1 The number of children who suffer from terminally ill diseases each year reached as high as 21 million.2 Because of the low survival rate among terminally ill pediatric patients after the administration of cardiopulmonary resuscitation CPR, a term was found, which is do not resuscitate (DNR). Although the survival rate is high after CPR for children who are suffering from terminally ill diseases, all of them died shortly after the CPR.3 The DNR decisions are made when anyone that with terminally ill disease include children refuses resuscitation, poor diagnosis, or if it is evident that the individual with terminally ill disease will not survive CPR with better life quality.4,5 The DNR order entails avoiding basic CPR, compressing the chest combined with or without concurrent ventilation, and exceptional CPR that involves defibrillation and medication.3
According to western regulations, if there is no DNR order for a child with terminally ill disease, CPR must commence within 60 seconds, and defibrillation within three minutes.3,4 Provisions of western laws dictate that for a child with terminally ill disease, the DNR decision lies with the responsible physician.5–9 The physician usually makes his final decision.10–14
Because healthcare providers such as nurses and pharmDs spend significant time with the patient,15,16 offering bedside nursing and medical attention within the several hours of their duty shift, they, frequently, start discussing DNR.7,17,18 Besides, nurses and pharmDs have been trained to properly document DNR orders for terminally ill children and to properly inform the child with terminally ill diseases and his relatives offering care, such as more family support, assisting the child with terminally ill disease in passing on peacefully, and preventing unnecessary CPR.7,15 In the Middle East, there is no consensus for nurses and pharmDs about how to practice DNR orders within since the nursing and pharmD students will be the next generation who will take care of pediatric patients. The attitudes of these students towards DNR decisions are very important. Therefore, this study aimed to survey attitudes of nursing and pharmD undergraduate students about do not resuscitate order for children with terminally ill diseases and whether differences in attitudes existed between nursing and pharmD students.
Method
This was a descriptive correlational study, utilizing an online survey to assess the attitudes of nursing and pharmD undergraduate students about the do not resuscitate orders for children with terminally ill diseases. The researchers used the G*Power software version 3.1.92 to calculate the required sample size. A significance level of 0.05, a power of 0.95, and 11th variables were used with a medium effect size of 0.15 resulting in a minimum number of subjects being 400. However, since using electronic surveys have a low response rate, the researcher sent 800 surveys to guarantee enough responses. A total of 800 nursing and pharmD undergraduate students from Jordan University of Science and Technology were contacted, where a flyer was sent to them to participate in the study. Almost 420 surveys were returned where 18 of them were excluded for missing data. Thus, the total number of surveys included in the study was 402 consist of two hundred forty-two from nursing and 160 from pharmD. Data collection began in April 2020 and closed in June 2020. The inclusion criteria for participating in the study were nursing or pharmD students enrolled at Jordan University of Science and Technology/Jordan regardless of year or gender. First- and second-year students were excluded since in these years will not expose to pediatric patients who suffering from terminally ill disease. During the survey filling, the participant was first given brief details regarding the study and its aim. Then, an online consent form was presented, and the participant was instructed to carefully read the informed consent and click on the agree button at the end of the consent form if he/she was willing to take part in the study. After that, an online survey was disseminated to the participants. Completed questionnaires were automatically saved on Qualtrics software, which is password protected and can only be accessed by the study authors.
Instrument
The web survey included two sections: first, the participants were requested to complete background information that includes age, gender, hear about DNR, discuss DNR with others, income, living area, nationality, years of education, father education, mother education, and reason may impact the decision of DNR.
The second part was based on a tool about DNR developed by Dunn.20 This tool consisted of 25 statements (items), which were scored based on a five-point Likert scale. Likert scale from 1 (not significant/probable) to 5 (very substantial/likely) was used. The total score ranged from 25 to 125. Increased score indicated more positive attitude toward DNR among children with terminally ill disease. This tool was subdivided into three categories: overall perception, expertise, and personal opinions about the issue of DNR. It was acquired from comparable research of nurses ‘perception toward DNR order in Saudi Arabia; a Cronbach alpha of 0.82 confirmed the accuracy and suitability of this questionnaire for use in the current study context.21 We followed all the required steps for the translation of the DNR measure to ensure the reliability, validity and cultural sensitivity of the translation. In our study, the DNR found to be valid and reliable with Cronbach alpha was 0.84.
Data Analysis
Statistical package for Social Sciences [SPSS], version 24 was used to conduct data analysis. A survey was excluded if it was missing more than 20% of the data. In the sample of the current study, the frequencies of missing values across all items were less than 5%. A multivariate diagnostic test was used to explore the degree of randomness in the identified missing data. The analysis revealed that the missing pattern was random (p > 0.05). Numbers, percentages, measures of central tendency, and ranges were used to represent descriptive data. The t-test was used to determine the differences in attitude between nursing and pharmDs’ students. Multiple regressions test was conducted to determine the predictors of attitude toward DNR in nursing and pharmD students. The attitude toward DNR total score was entered as an outcome variable, whereas other factors such as age and gender were entered as potential predictors after determining if there is any multicollinearity. Before conducting the multiple regressions multicollinearity diagnostic tests were conducted and multicollinearity was not found since VIF was less than 10. To control the confounders, the possible confounders were includedas variables in the regression model, in this way, the authors control for the impact of the confounding variables. Any effect that the potential confounding variable has on the dependent variable will show up in the results of the regression and allow you to separate the impact of the independent variable.
Ethical Consideration
An ethical approval was given from the Jordan University of Science and Technology IRB (2020243). The research was carried out while adhering to the national and international empirical research guidelines and regulations regarding voluntariness and anonymity of the data. Respondents agreed that the findings be published in a scientific journal. The survey did not ask questions that were deemed as sensitive or inappropriate. Since the study instruments may include some items that have the potential of eliciting negative feelings, participants were informed that they could refrain from answering any questions that may elicit distress.
Results
Demographic Characteristics
Total of 402 students participated in the study including 242 nursing and 160 pharmD students. Males were 90 (22.4%) whereas females were 312 (77.6%). Demographic characteristics of the study participants according to the group are shown in Table 1.
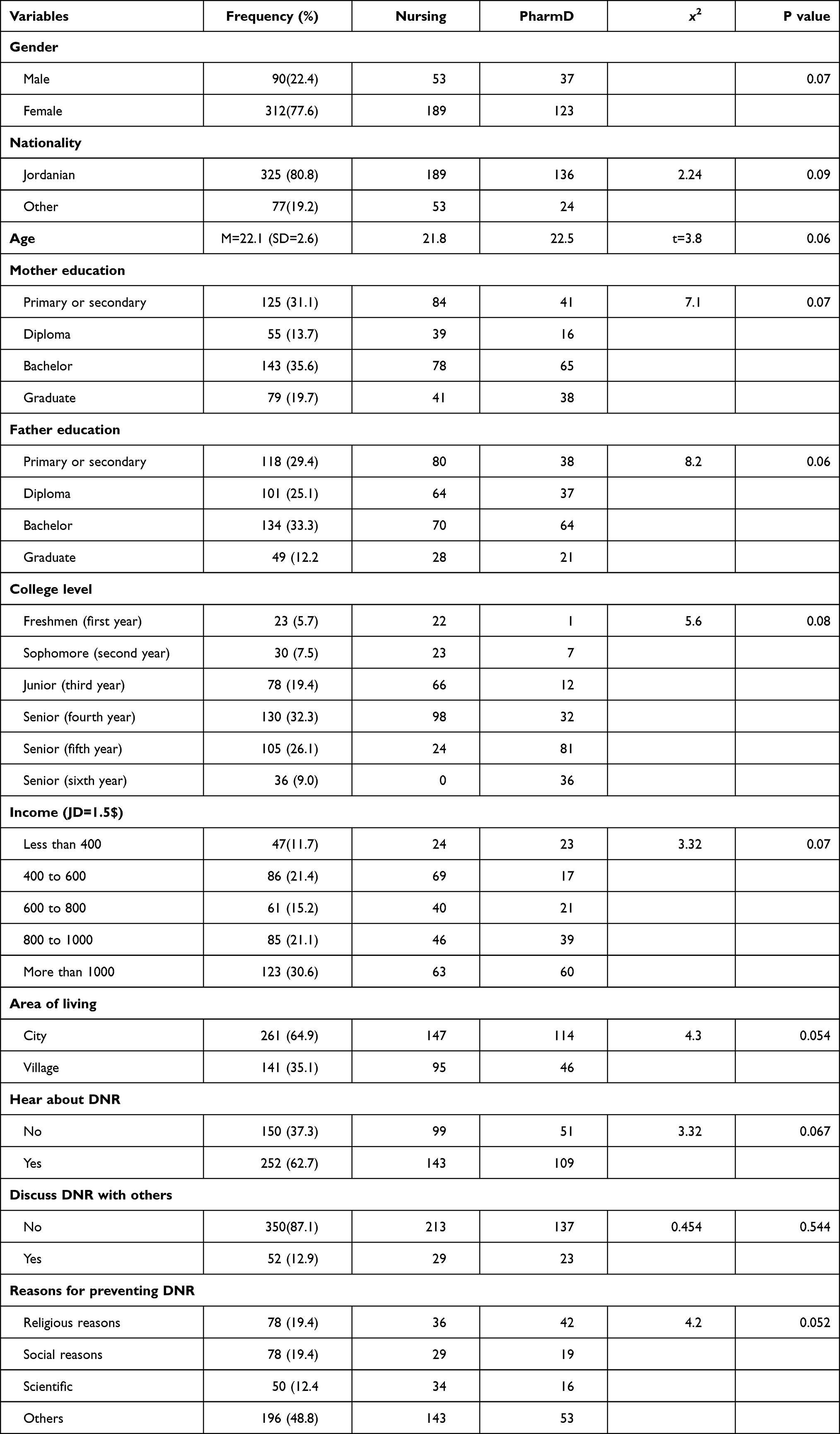 |
Table 1 Frequency Distribution of Socio-Demographic Characteristics of Undergraduate Students (n=402) |
Attitude Toward DNR Among Nursing and PharmD Students
Attitude towards DNR among nursing and pharmD students was good (M= 69.9, SD=10.3). Many students showed agreement to the following statements “DNR orders for terminally ill children help keep patients from suffering unnecessarily”, 290 (69%), and “The patient or the patient’s family must give written permission in orders for the physician to initiate DNR orders for terminally ill children”, 267 (66%). Table 2 shows the responses of the study participants regarding their perception toward DNR orders in children with terminally ill diseases.
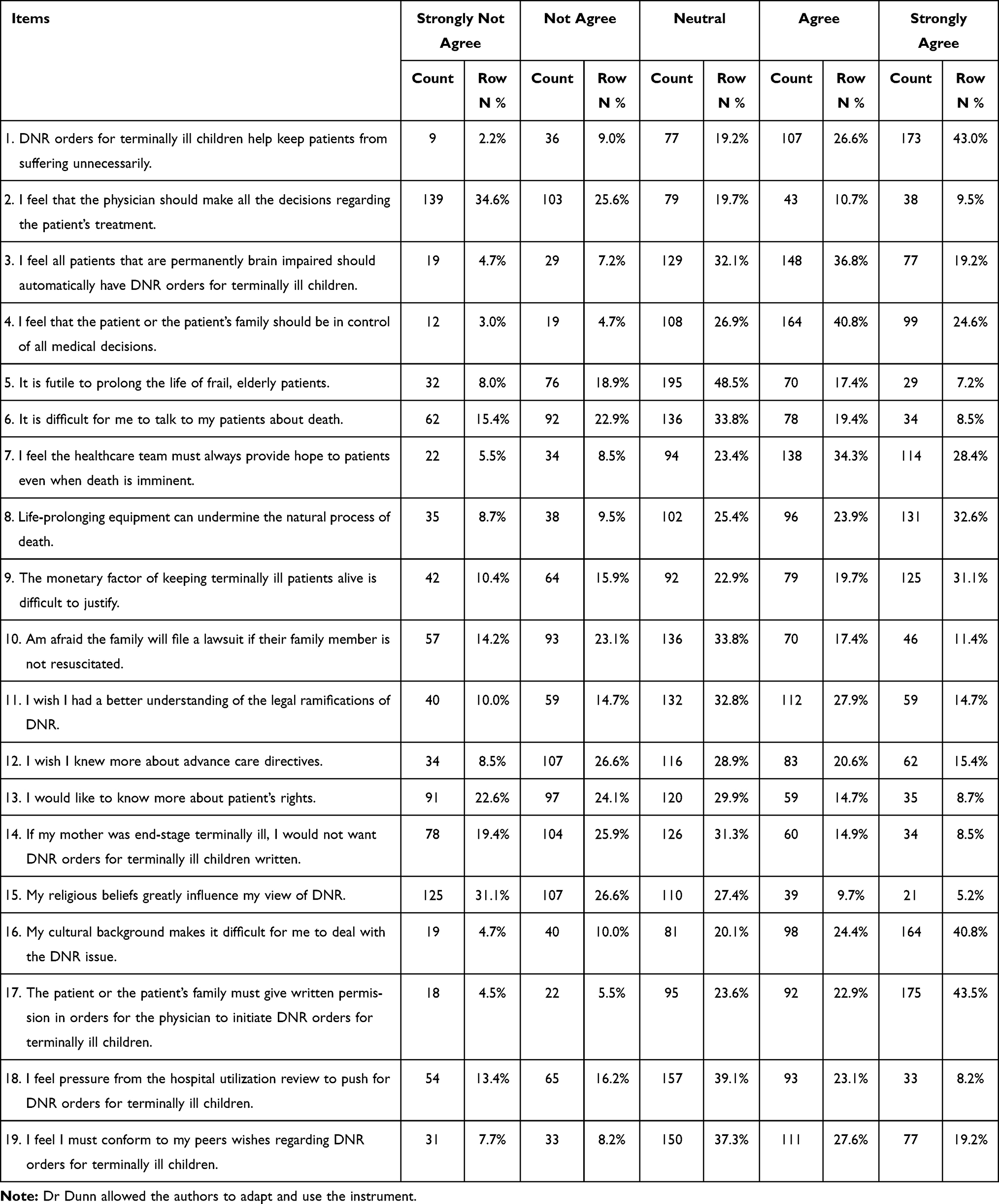 |
Table 2 Responses to DNR Items for Nursing and PharmD Students (n=402) |
Differences Between Nursing and PharmD Students Regarding DNR
The t-test was used to compare attitude toward DNR between nursing and pharmD students. For nursing students, the DNR score was M= 84.15, SD=12.8, whereas for pharmD students, the ‘DNR score was M=85.19, SD= 18.6. Thus, a significant difference in perception toward DNR orders was detected between nursing and pharmD students (t=−1.3, p=0.013).
Factors Related to Nursing and PharmD Students’ Attitudes
Multiple regressions were used to predict nursing and pharmD students’ attitude about barriers toward participation in research according to demographic variables such as age, gender, income, living place, nationality, year of education and parents’ education. Table 3 summarizes the outcomes of the multiple regression tests. All the listed factors were not associated with the perception toward DNR orders (p-value > 0.05) except prevention reasons for doing DNR for children (t=−2.180, p=0.030).
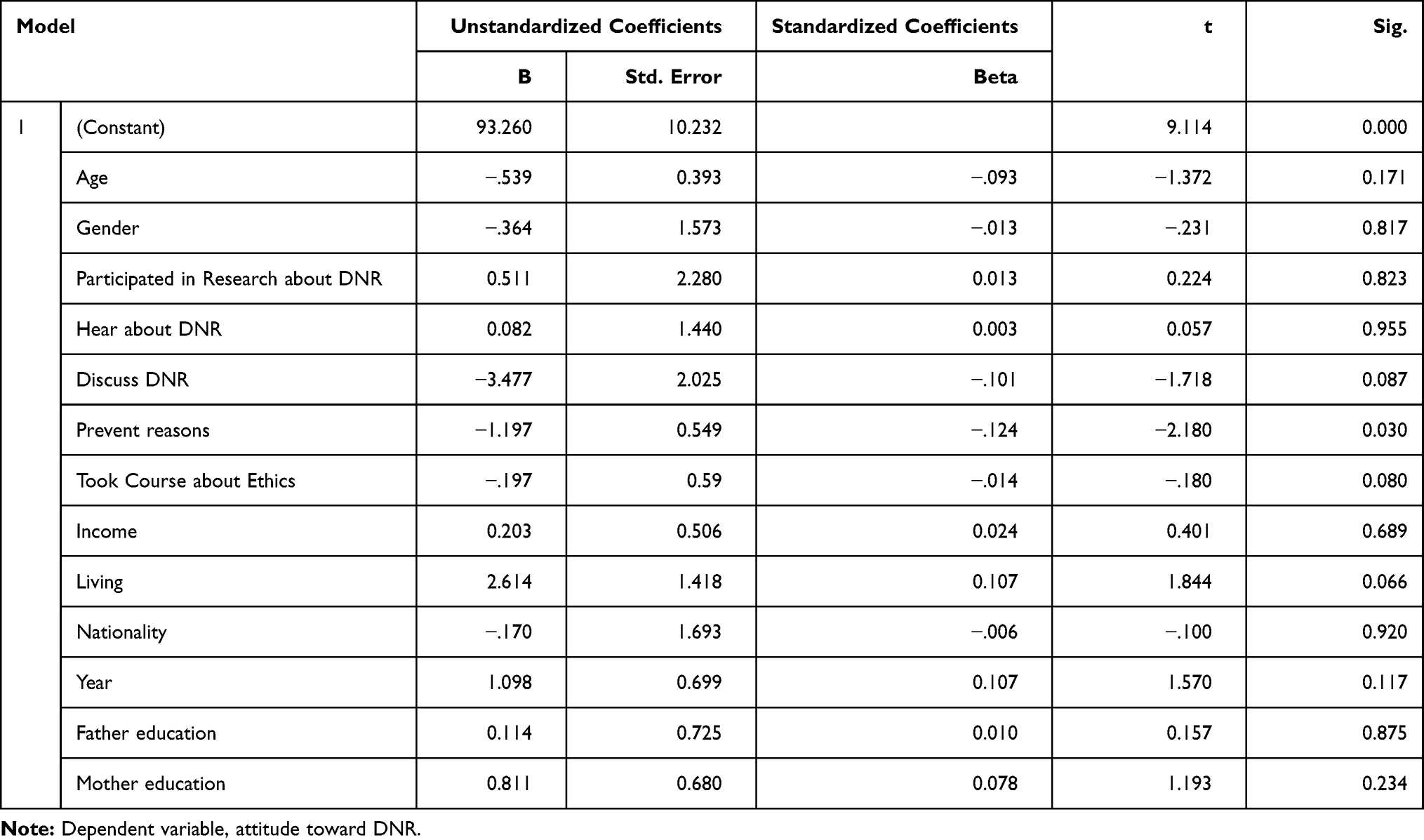 |
Table 3 Multiple Regression for Predictors of DNR of Terminally Ill Children |
Discussion
This study is the first to investigate the attitude of Jordanian nursing and pharmD students toward DNR orders for terminally ill children. This study was aimed to survey attitudes of nursing and pharmD undergraduate students about do not resuscitate order for children with terminally ill diseases, to detect whether differences in attitudes existed between nursing and pharmD student, and to determine the predictors of attitude toward DNR among nursing and pharmD. It is worth to note that the attitude towards DNR among nursing and pharmD students was good. These findings indicate that, despite favorable perspectives on a few elements, Jordanian nursing and pharmD students retain a pessimistic attitude for “DNR orders for terminally ill children” in various important elements on the “attitude on the DNR” survey.
Similarly, in a systematic literature review study, only few studies have investigated the perspectives of students regarding ‘DNR orders for terminally ill children or adults. In one study, Al- Mobeireek revealed recommendations of DNR for healthy adult patients, which were made by only 16% of Saudi physicians.23 Another study by Iyilikci found that 66% of anesthesiologists in turkey had ordered written/oral ‘DNR orders for terminally ill children.24 Another study was conducted by Varon in Singapore to study terminally ill children and to determine some misconceptions regarding “DNR orders for terminally ill children” among healthcare care providers and found there are many misconceptions among.25 These findings showed that the implementation of DNR differs based on the Muslim healthcare service providers from one country to another.
In our study, most students were agreed to the item that “I would like to know more about patient’s rights” where their religious beliefs greatly influence their attitude toward DNR (2.63, SD= 1.12). To compare our study with previous literature, the searching of the literature that no prior studies investigating the attitude toward DNR orders for terminally ill children in Jordanian nursing and pharmD students. It is noteworthy that this first study that examines the attitude of pharmD students, but there are few studies that examine medical students and nurses’ attitudes toward euthanasia (the painless killing of a patient suffering from an incurable and painful disease or in an irreversible coma).26,27 Moghadas et al26 and Rastegari-Najafabadi et al27 found that almost 50% of nurses in Iran accepted the practice of euthanasia or end of life during surgery. In another observation study, it was found that 50% of medical scholars in Iran described encouraging opinion toward the use of euthanasia or end of life techniques.28 Previous literature can be compared to the current study since most undergraduate students were from the same religion. Followed by every Islamic sects, any kind of euthanasia is not allowed.29 But “DNR orders for terminally ill children“ are not going against the fundamental Islamic regulations.30 Islam assumes life as sacred30 while comprehends death to be an unavoidable aspect of life.20 Muslims acknowledge death is authorized by God.31 Thus, treatments are not implied when they just prolong the sufferings of terminal sickness.30 Removing life-enduring remedies in that situation may appear to allow death to make its natural approach.31 Hence, the pessimistic impression of Jordanian nursing and pharmD students over “DNR orders for terminally ill children” is not explained with their religious principles and affiliations. It is noteworthy that undergraduate students are showing favorable opinion to additionally understand distinct characteristics of DNR orders for terminally ill children. On the other hand, many undergraduate students revealed that their strict religious convictions greatly impact their attitude toward DNR. One main explanation of the pessimistic approach on ”DNR orders for terminally ill children” might arise from the absence of deep understanding over DNR orders for terminally ill children. The same way earlier studies indicated that nursing and pharmD students have limited information about many ethical dilemmas.32 Though many differences in point of view are observed between Muslims, the perspectives on death remain the same.30
The multiple regression analysis was conducted in the current study to determine the factors that were associated with attitude toward DNR orders for terminally ill children among nursing and pharmD students that includes their demographic variables and other associated factors such as previous experience with DNR among terminally ill children. In our study, it was shown that these demographical characteristics were not associated substantially with the attitude of nursing pharmD students‘ attitudes toward the DNR issue among children.
Our results revealed contract results with previous studies in the same area that religious convictions significantly affect more than 70% of the undergraduate students concerning their opinion of DNR orders for terminally ill children.34 Our finding of the current study corresponds with the outcomes of several other studies in this area.34–36 In many ways, the spiritual and religious problem is generally awakened or worsened for dying patients.34 Many studies in many countries Eastern and Western have examined the influence of variables such as religion, ethics, and culture to ensure an appropriate end to life for terminally ill patients.35,36 Furthermore, consideration of the impact of culture and faith on the attitude and posture of future healthcare providers should be an essential part of any strategy to be developed to aid patients when there is a life and death situation.33 According to previous studies, ethical reasoning, and justification of DNR order in critically ill patients with prolonged suffering should be based on the clinical reality, patient preferences, quality-of-life considerations, and the likelihood of surviving cardiopulmonary resuscitation (CPR). Healthcare providers such as nurses and pharmD should use their knowledge and skills to make reasonable actions to optimize patients’ health outcomes in accordance with professional judgment. The DNR can be ethically acceptable, especially when death is welcome by the patient as a natural process of life. Since healthcare providers are portioned to communicate with patients and families about end-of-life care and the hard decisions to make with a great focus on patients’ preferences and autonomy, they may be aware of the emotional pressure they may exert on patients and family members when assisting with communication about DNR orders.38 Without prior signed DNR orders, the role of physicians can be more complex. One of the big ethical challenges of end-of-life care is withholding and withdrawing care that is unlikely to provide physiological benefits for terminally ill patients. Thus, standards for excellent care should be established to respect the autonomy of terminally ill patients at the end of life, which in turn can help physicians and other healthcare providers such as nurses to make effective decision-making without being hesitant from providing care for desperately ill patients.38,39 Based on current results, gender did not significantly influence the DNR decision. However, there is a need for more research to substantiate this claim.
Strengths and Limitations
The major strength of this study was being the first study in Jordan to survey nursing and pharmD students regarding DNR in children. The major limitation that affecting this current study is using a convenience sample. The major criticism of convenience sampling is sampling bias, and that the sample may not be representative of the entire population. Another considerable disadvantage of using a convenience sample is the limitation in generalization and inference making about the entire population. Since the sample is not representative of the population, the results of the study cannot speak for the entire population.
Implications for Practice
The outcomes of this research have suggestions for real-life exercises and could be generalized to all students in developing countries with similar situations. Results showed that Jordanian nursing and pharmD students had a good attitude toward many key aspects of DNR orders for terminally ill children. This study shows that Jordanian nursing and pharmD students were willing to learn more about different aspects of DNR orders for terminally ill children. By analyzing their responses to multiple items, misconception about DNR orders for terminally ill children was apparent. Therefore, it is important to provide education programs about DNR for those students during their study and to integrate DNR within courses in the undergraduate curricula of in nursing and PharmD. According to the study outcome, the attitude of Jordanian nursing and pharmD students about DNR orders for terminally ill children may change by such education.
Conclusion
A non-Western nation adds to knowledge as it extends our understanding of this subject in another context. The results showed that there was a significant difference in perception toward do not resuscitate order between nursing and pharmD students. The pharmD students had more positive attitude toward do not resuscitate than the nursing students. Demographic variables were not associated with the perception toward do not resuscitate orders. This study shows that Jordanian nursing and pharmD students are willing to learn more about different aspects of DNR orders for terminally ill children and analyzing their responses to many items showed their misconception about DNR orders for terminally ill children.
Abbreviations
PPC, pediatric palliative care; PCQN, Palliative Care Nursing Questionnaire; DNR, do not resuscitate orders; PharmD, Doctor of Pharmacy.
Data Sharing Statement
Data will be sent upon request from Sawsan Abuhammad at [email protected].
Ethics Approval and Consent to Participate
This research got an Approval from the Jordan University of Science and Technology IRB (#20202343). Consent form was signed by all the participants.
Acknowledgment
DNR Questionnaire was approved to use by Dunn (2000). The instrument was developed by Dr Dunn and permission was given to use it.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project was carried out as part of “The Research Ethics Education Program in Jordan” and has been supported by NIH grant number (1R25TW010026-01). The funder support data collection and fees for publication. All authors have read and approved the manuscript” and ensure that this is the case.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World population data sheet. Washington DC: Population Reference Bureau; 2014. Available from: http://www.prb.org/pdf14/2014-world-population-data-sheet_eng.pdf.
2. Connor SR, Downing J, Marston J. Estimating the global need for palliative care for children: a cross-sectional analysis. J Pain Symptom Manage. 2017;53(2):171–177. doi:10.1016/j.jpainsymman.2016.08.020
3. Burns JP, Truog RD. The DNR order after 40 years. N Engl J Med. 2016;375(6):504–506. doi:10.1056/NEJMp1605597
4. Pettersson M, Hedstrom M, Hoglund AT. Striving for good nursing care: nurses’ experiences of do not resuscitate orders within oncology and hematology care. Nurs Ethics. 2014;21(8):902–915. doi:10.1177/0969733014533238
5. Silen M, Svantesson M, Ahlstrom G. Nurses’ conceptions of decision making concerning life-sustaining treatment. Nurs Ethics. 2008;15(2):160–173. doi:10.1177/0969733007086014
6. Clements M, Fuld J, Fritz Z. Documentation of resuscitation decision-making: a survey of practice in the United Kingdom. Resuscitation. 2014;85(5):606–611. doi:10.1016/j.resuscitation.2014.02.005
7. Adhikari S, Rijal S. Attitude of doctors working in a tertiary hospital towards Do-not-resuscitate decisions. J Gen Pract Emerg Med Nepal. 2019;6(8):13–16.
8. Naghshbandi S, Salmasi S, Parsian Z, Rahmani F. Attitude of nurses in intensive care units towards Do Not Resuscitate order. J Res Clin Med. 2019;7(4):122–128.
9. Shayestefar S, Mardani-Hamooleh M, Kouhnavard M, Kadivar M. Ethical challenges in pediatrics from the viewpoints of Iranian pediatric residents. J Compr Ped. 2018;9(1).
10. Schwartz JA. Innovation in pediatric surgery: the surgical innovation continuum and the ETHICAL model. J Pediatr Surg. 2014;49(4):639–645. doi:10.1016/j.jpedsurg.2013.12.016
11. Asemani O, Parsaei H. Decisionmaking on the prolongation of the life of severely diseased newborns: reinspection of criteria. Iranian J Med Ethics Hist Med. 2012;5(5):36–52.
12. Salem A, Salem AF. Breaking bad news: current prospective and practical guideline for Muslim countries. J Cancer Educ. 2013;28(4):790–794. doi:10.1007/s13187-013-0523-8
13. Levin T, Li Y, Weiner J, Lewis F, Bartell A, Piercy J. How do-not-resuscitate orders are utilized in cancer patients: timing relative to death and communicating-training implications. Palliat Support Care. 2008;6(4):341–348. doi:10.1017/S1478951508000540
14. Duplan KL, Pirret AM. Documentation of cardiopulmonary resuscitation decisions in a New Zealand hospital: a prospective observational study. Intensive Crit Care Nurs. 2016;37:75–81. doi:10.1016/j.iccn.2016.06.005
15. Peimani M, Zahedi F, Larijani B. Do not resuscitate order across societies and the necessity of a national ethical guideline. Iranian J Med Ethics Hist Med. 2012;5(5):19–35.
16. Izadikhah A, Changiz YN, Mirshahjafarey I. Developing codes of ethics for clinical medicine educators. Iranian J Med Ethics Hist Med. 2013;6(1):37–52.
17. Jensen HI, Ammentorp J, Johannessen H, Ording H. Challenges in end-of-life decisions in the intensive care unit: an ethical perspective. J Bioeth Inq. 2013;10(1):93–101. doi:10.1007/s11673-012-9416-5
18. Mockford C, Fritz Z, George R, et al. Do not attempt cardiopulmonary resuscitation (DNACPR) orders: a systematic review of the barriers and facilitators of decision-making and implementation. Resuscitation. 2015;88:99–113. doi:10.1016/j.resuscitation.2014.11.016
19. Pfeil TA, Laryionava K, Reiter-Theil S, Hiddemann W, Winkler EC. What keeps oncologists from addressing palliative care early on with incurable cancer patients? An active stance seems key. Oncologist. 2015;20:56. doi:10.1634/theoncologist.2014-0031
20. Dunn MC. Attitudes of medical personnel toward do-not-resuscitate orders MS Dissertation. Long Beach: Department of Social Work, California State University; 2000.
21. Fallahi M, Banaderakhshan H, Abdi A, Borhani F, Kaviannezhad R, Karimpour HA. The Iranian physicians attitude toward the do not resuscitate order. J Multidiscip Healthc. 2016;9:279. doi:10.2147/JMDH.S105002
22. Mahon MM, McAuley WJ. Oncology nurses’ personal understandings about palliative care. Oncol Nurs Forum. 2010;37(3):E141–E150. doi:10.1188/10.ONF.E141-E150
23. Al-Mobeireek AF. Physicians’ attitudes towards ‘do-not-resuscitate’ orders for the elderly: a survey in Saudi Arabia. Arch Gerontol Geriat. 2000;30:151–160. doi:10.1016/S0167-4943(00)00047-9
24. Iyilikci L, Erbayraktar S, Gökmen N, Ellidokuz H, Kara H, Günerli A. Practices of anaesthesiologists with regard to withholding and withdrawal of life support from the critically ill in Turkey. Acta Anaesthesiol Scand. 2004;48:457–462. doi:10.1046/j.1399-6576.2003.00306.x
25. Varon J, Bisbal Z, Vargas B, Fromm RE, Tai DY. Cardiopulmonary resuscitation preferences among health professionals in Singapore. Crit Care Shock. 2004;7:219–225.
26. Moghadas T, Momeni M, Baghaeei M, Ahmadi S. Intensive care unit of nurses’ attitudes toward euthanasia. Iranian J Med Ethics Hist Med. 2012;5:80–86.
27. Rastegari-Najafabadi H, Sedaghat M, Saeedi Tehrani S, Aramesh K. Nurses’ attitudes Tehran of Medical University hospitals towards euthanasia. Iranian J Med Ethics Hist Med. 2010;3:37–44.
28. Tavosian A, Sedaghat M, Aramesh K. Attitudes of interns Tehran University of medical sciences towards euthanasia. Iranian J Med Ethics Hist Med. 2009;3:43–51.
29. Takrouri M, Halwani T. An Islamic medical and legal prospective of do not resuscitate order in critical care medicine. Internet J Health. 2008;7:12–16.
30. Sarhill N, LeGrand S, Islambouli R, Davis MP, Walsh D. The terminally ill Muslim: death and dying from the Muslim perspective. Am J Hosp Palliat Care. 2001;18:251–255. doi:10.1177/104990910101800409
31. Zahedi F, Larijani B, Tavakoly Bazzaz J. End of life ethical Issues and Islamic views. Iran J Allergy Asthma Immunol. 2007;6:5–15.
32. Zahedi F, Larijani B. Cancer ethics from the Islamic point of view. Iran J Allergy Asthma Immunol. 2007;6:17–24.
33. Zarghami M, Valaie N, Sartakhti AA, Mehraban M, Mahmoudi R, Moonesi FS. Attitudes of Iranian interns and residents towards euthanasia. World Appl Sci J. 2010;8:486–489.
34. Jung JY, Shin SY. Awareness and ethical attitudes about DNR of emergency department students: differences in recognition according to bioethics education. 한국산학기술학회 논문지. 2014;15(2):1074–1082. Chinese.
35. Emami-Razavi S, Ghajarzadeh M, Oryani S, Askari F, Jalilian R, Azizi S. Perspectives of Iranian medical nurses about do-not-resuscitate (DNR) orders. Acad J Surg. 2014;1(3–4):49–51.
36. Hileli I, Weyl Ben Arush M, Hakim F, Postovsky S. Association between religious and socio‐economic background of parents of children with solid tumors and DNR orders. Pediatr Blood Cancer. 2014;61(2):265–268. doi:10.1002/pbc.24712
37. American Nurses Association. Nurses’ roles and responsibilities in providing care and support at the end of life. Revised Position Statement. 2016;3(2).
38. Luce M, White B. The pressure to withhold or withdraw life-sustaining therapy from critically ill patients in the United States. Am J Respir Crit Care Med. 2007;175(11):1104–1108. doi:10.1164/rccm.200609-1397CP
39. WHO. WHOQOL: measuring quality of life. Health statistics and information systems [Internet]. Geneva: WHO; 2018. [
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.