Back to Journals » Clinical Ophthalmology » Volume 19
Nurse-Led Model in Diabetic Retinopathy Screening: An Exploratory Scoping Review of Nurses’ Roles and Contributions
Authors Chen C, Pazo EE ![]() , Liu H
, Liu H ![]() , Liu J
, Liu J ![]()
Received 19 June 2025
Accepted for publication 31 October 2025
Published 27 November 2025 Volume 2025:19 Pages 4335—4347
DOI https://doi.org/10.2147/OPTH.S548241
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yousef Fouad
Chen Chen, Emmanuel Eric Pazo, Hua Liu, Juping Liu
Tianjin Key Laboratory of Retinal Functions and Diseases, Tianjin Branch of National Clinical Research Center for Ocular Disease, Eye Institute and School of Optometry, Tianjin Medical University Eye Hospital, Tianjin, People’s Republic of China
Correspondence: Juping Liu, Tianjin Key Laboratory of Retinal Functions and Diseases, Tianjin Branch of National Clinical Research Center for Ocular Disease, Eye Institute and School of Optometry, Tianjin Medical University Eye Hospital, Tianjin, People’s Republic of China, Email [email protected]
Purpose: As the growing number of diabetic retinopathy (DR), the demands for screening requests and eye care services are expected to increase. While different screening models have been reported, there are several articles in literature of nurse-led DR screening. The purpose of this review was to define the roles and contributions of nurses in DR screening, identify the necessary supports required, and address the challenges that need to be resolved.
Methods: The literature search for the included articles was performed in the following databases: PubMed, CINAHL, Cochrane, Embase, and Web of Science. This search was conducted from the start of May 2025. Two reviewers independently screened all articles. If predefined inclusion criteria were met, the studies were further descriptive content, and data were summarized and individually evaluated.
Results: From a total of 126 citations, 15 articles were selected for inclusion in the final review. Currently, nine countries globally are actively developing and implementing nurse-led DR screening models, with Australia leading in the number of such programs. Our search of literatures demonstrated the roles and contributions of nurse-led DR screening encompass research and leadership, consultancy, health management, technical expertise, and data collection. The supports required and challenges faced include transforming traditional screening models, providing adequate training, securing financial resources, and enhancing career motivation.
Conclusion: The nurse-led model is a promising approach in DR screening that integrates eye examinations, diabetes education, data collection and fundus imaging within a single encounter, thereby improving efficiency and lowering costs. It may thus be considered a scalable approach for the future expansion of screening programs.
Keywords: nurse, led, diabetic retinopathy, DR, screening
Introduction
DR, a complication of diabetes mellitus (DM), is characterized by progressive retinal microvascular damage that compromises visual function.1 Anticipated trends indicate a substantial increase in the global prevalence and disease burden of DR in the coming decades.2 Current projections indicate that the number of affected individuals will rise from approximately 103 million in 2020 to 130 million by 2030, with a further increase expected to reach 161 million by 2045.2 This marked growth is expected to place additional strain on existing healthcare systems and resources, which are already under considerable pressure.
DR often presents asymptomatically in initial phases.2–4 Often, by the time diabetic patients undergo a fundus examination in a hospital, their condition has already advanced to moderate or severe non-proliferative DR (NPDR).5 With 60% of type 2 diabetes patients developing retinopathy after two decades disease of duration.1 However, according to the International Diabetes Federation, only approximately half of individuals with diabetes are aware of their DR status.6 Given the asymptomatic nature of early-stage progression and the potential for preserving vision through timely intervention, routine DR screening is established as a critical risk management strategy to safeguard eye health and prevent vision impairment.2,4 More alarmingly, the response rate for DR screening is a matter of significant concern. Fewer than 50% of diabetic patients undergo DR screening even in developed countries.7 Moreover, among underserved populations, the lack of access to eye specialists has resulted in annual screening rates as low as 10% to 20%.7
Despite global recommendations promoting systematic retinal screening and organized eye care for individuals with diabetes,3,8–11 the rising global prevalence of DR has intensified shortages in ophthalmic professionals, thereby constraining the capacity to fulfill increasing demands for DR screening.12,13 The insufficient screening coverage resulting from this may lead to a series of adverse clinical outcomes, such as the complication of the screening process, poor management of chronic diseases, and uneven allocation of medical resources.7 Therefore, strengthening and standardizing DR Screening strategies has become a key issue that urgently needs to be addressed in the current field of public health.12–14 In previous DR screening practices, the field has engaged a range of professionals such as ophthalmologists, primary care physicians, optometrists, vision technicians, nurses, and pharmacists.15 These individuals have been recognized for their potential roles in screening activities.15 However, due to the persistent shortage of medical staff and uneven allocation of resources, the large-scale promotion of screening services still faces significant obstacles.8,9
Recent practices had shown that enabling nurses to undertake part of the DR Screening responsibilities through systematic training can effectively enhance the service efficiency and patient turnover capacity of the overburdened retinal medical system.6,12,16,17 Although international experience and pilot programs have demonstrated that the nurse-led screening model is effective in identifying and managing the risk of DR, currently, no systematic framework offers a comprehensive description of the core roles and contributions of the nurse-led DR model or the full range of outcomes it generates. This review therefore evaluates its international dissemination, synthesizes the key roles and contributions of nurses within the model, clarifies clinical, organizational, economic and experiential outcomes, and explores the challenges and supports that shape its implementation.
Methods
Scoping review offers a broad-based methodology, accommodating diverse research designs and integrating varied perspectives and theoretical frameworks. This approach was undertaken following the methodological framework initially proposed by Arksey and O’Malley,18 subsequently refined by Levac and colleagues.19 The five-step process outlined: (1) defining the research objectives; (2) locating pertinent studies; (3) screening and selecting sources; (4) systematically extracting and organizing data; (5) synthesizing, interpreting, and presenting findings. This iterative structure ensures methodological rigor while maintaining flexibility to address expansive research aims.18
Step 1: Defining the research objectives
What roles and responsibilities do nurses undertake in the nurse-led screening models for DR worldwide?
Step 2: Locating pertinent studies
A systematic literature search was conducted in PubMed, CINAHL, Cochrane, Embase, and Web of Science (from start to May 2025). The search terms were as follows: DR OR diabetic retinopathy AND nurse AND led.
Step 3: Screening and selecting sources
Steps 4 and 5: Systematically extracting and organizing data, presenting findings
During the title and abstract screening phase to determine the literature that meets the criteria, we used the following process:
First, two reviewers independently conducted a preliminary screening of the article’s title and abstract. This step aims to identify relevant literature for the research topic. A third reviewer then independently reviewed the selection process and resolved any disagreements between the first two reviewers to ensure consistency and accuracy of the selection criteria.
After the initial screening, the selected articles were further evaluated by two reviewers responsible for determining whether the articles meet the eligibility criteria for inclusion in the study. The articles included indicated the nurse’s leading role in DR screening. In addition, we held a project group meeting to discuss and evaluate the relevance and applicability of the papers. These meetings aimed to ensure that a consensus could be reached on including literatures before and during data extraction. Through this meticulous and collaborative process, we strived to provide the rigor of the selection process and the high quality of the literatures.
The initial data extraction phase involved a comprehensive examination by the primary author to determine the specific nature, type, and extent of research on the focal topic. This examination culminated in the compilation of a comprehensive table of articles that encapsulated purpose, design, methodologies, primary characters, and pivotal findings. As the review progressed, including various items in the data extraction tables was subject to rigorous scrutiny and refinement through discussions among all contributing authors. The authors carefully noted, thoroughly compared, and thoroughly discussed emerging patterns and themes. Figure 1 presents the PRISMA flow diagram for our review. The papers were excluded from the title and abstract screening, full-text screening, evaluation of relevance, and data extraction stages mainly because they were outside our aims.
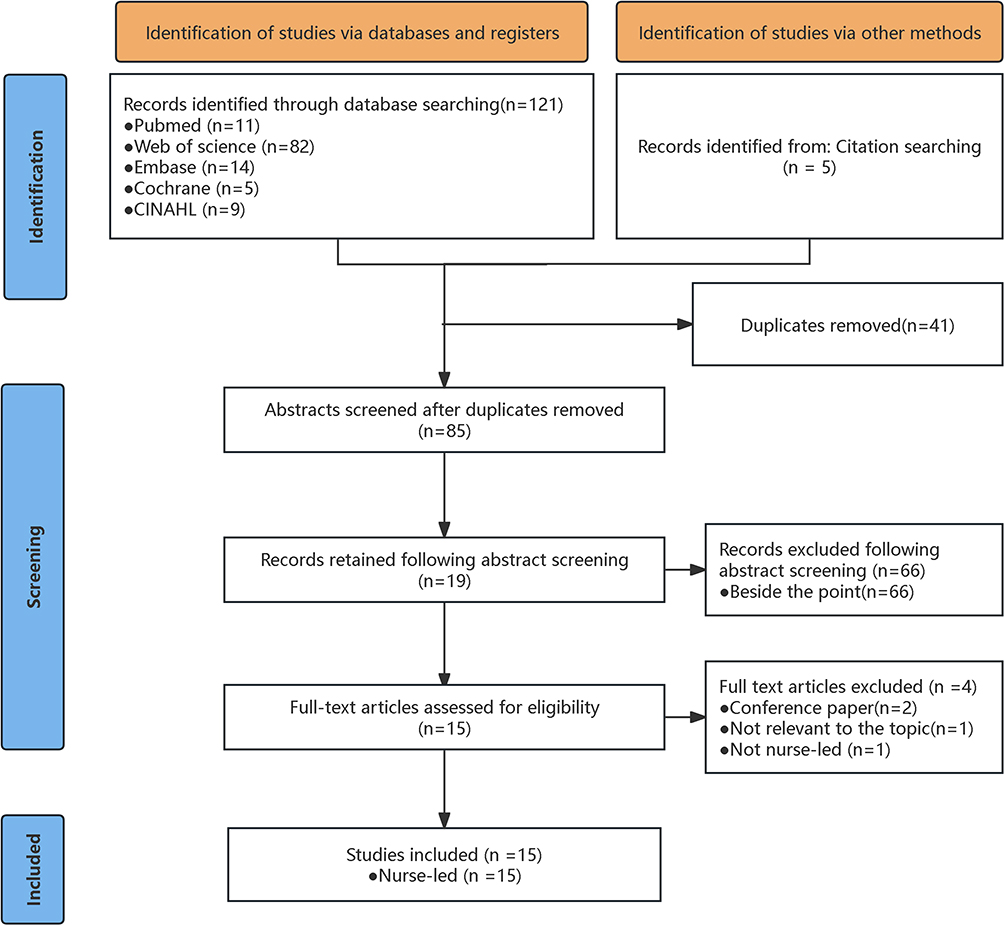 |
Figure 1 PRISMA flowchart of systematic study identification and inclusion process. |
Results
Study Characteristics
A total of 15 studies were published over an extended period from 2005 to 2025 (Table 1).3,9–11,20–30 Currently, 9 countries worldwide are actively exploring nurse-led screening models for DR. Figure 2 shows the geographical distribution of the included studies. Five studies (33.3%) were conducted in Australia,3,10,11,25,30 two studies (13.3%) were conducted in Canada,21,23 two studies (13.3%) were conducted in the USA,27,29 and the remaining six studies were conducted in the UK,22 Brazil,20 India,28 France,26 Spain,24 and Tanzania.9 Regarding institutional affiliations, the majority of first authors were affiliated with academic institutions (n=11, 73.3%),3,10,11,20–22,24,25,27,29 while the remainder were associated with hospital systems (n=4, 26.7%).9,25,26,28 Among the 15 analyzed nurse-led studies, seven utilized observational designs (6.7%),9,11,21,25–28 only one randomized controlled trial (6.7%),29 four conducted pre-post intervention analyzes (26.7%),3,10,20,24 one performed a retrospective cohort investigation (6.7%),23 one engaged in qualitative exploration (6.7%)30 and one presented a study protocol (6.7%).22
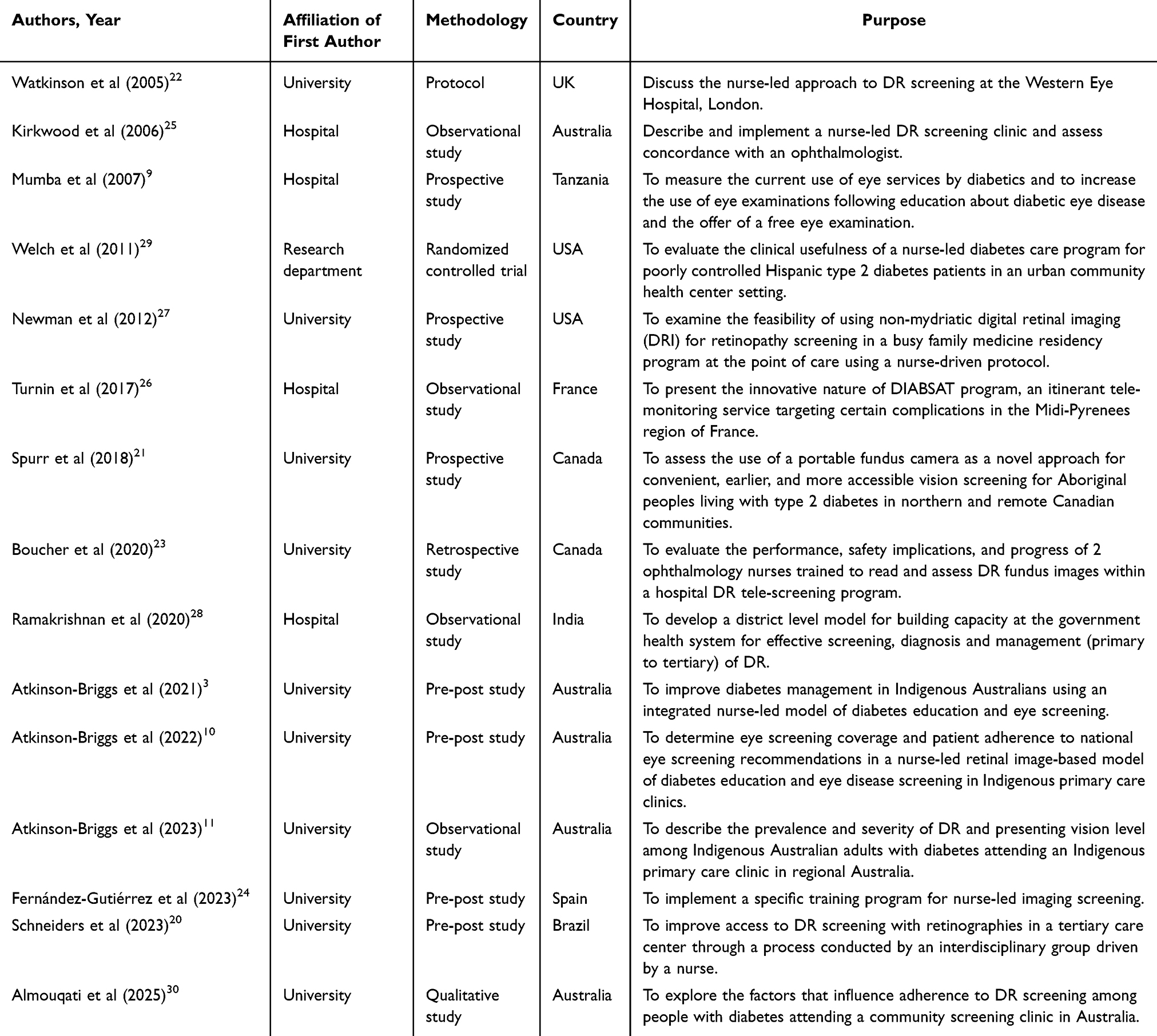 |
Table 1 Summary of Studies’ Characteristics |
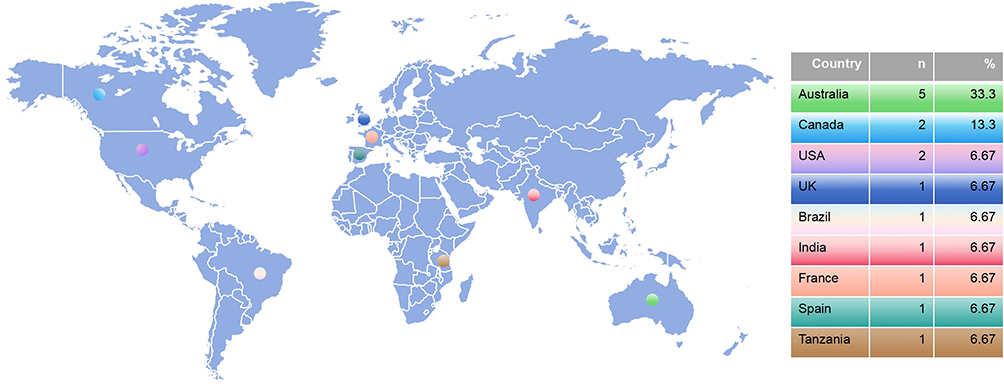 |
Figure 2 Geographical distribution of the included studies. |
Key Themes
Key themes identified include the feasibility of nurses with extended skills working within DR screening, as well as the roles and contributions to DR screening. The identified roles and contributions included research and leadership, consultant, health manager, technician, and data collector (Table 2 and Figure 3).
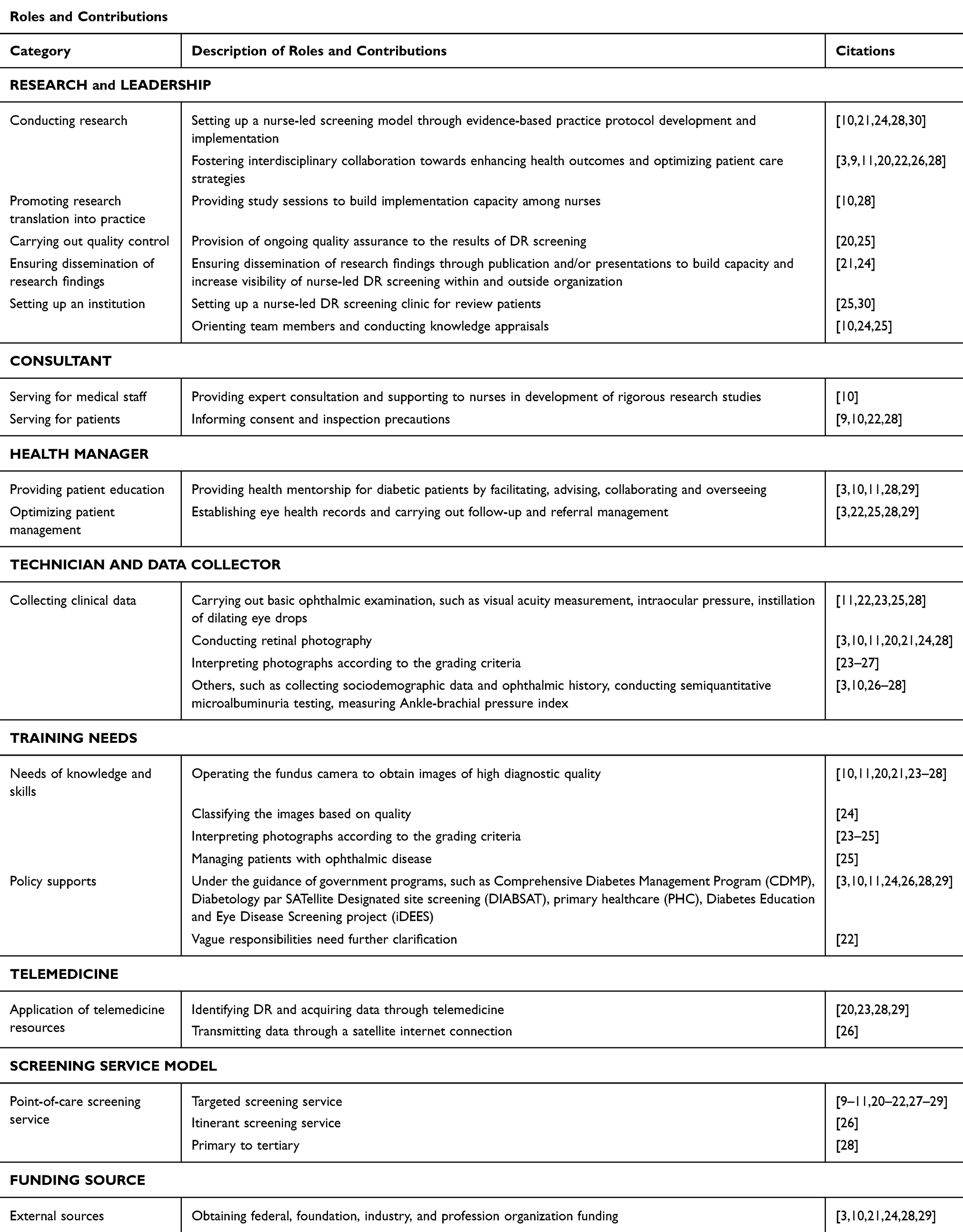 |
Table 2 Thematic Categories Characterizing the Nurse’s Roles and Critical Contributions in DR Screening |
 |
Figure 3 Roles and contributions in nurse-led model of DR screening. |
Research and Leadership
Experienced nurses frequently assumed multiple responsibilities as clinical experts, academic researcher and leader of programs. They were expected to engage closely with other program members and participants by conducting clinical research meetings to ensure the effective collection and management of patient biological samples, the gathering of study data, and the execution of informed consent processes.3,11,22,24,28,30,31 To enhance implementation capacity among nursing staff, this role also involved organizing study sessions and educational programs.10,28 Furthermore, this role encompasses ongoing quality assurance measures related to DR screening results, which are crucial for maintaining both integrity and reliability throughout the screening process.24,25
The Plan-Do-Study-Act (PDSA) cycle, as a commonly used tool for improving the quality of medical services, can promote quantifiable improvements when effectively applied to clinical process interventions.20,32 In Brazil, an interdisciplinary team led by an advanced practice nurse implemented iterative PDSA cycles in DR screening to develop the referral protocol, train the multidisciplinary team, and subsequently revisit the data to refine each step. Refinement with PDSA was iterative.20,32 Over six months, the team introduced tailored appointments and comprehensive assessments, then looped back to the data after every cycle. DR screening coverage among people with diabetes rose significantly and the re-engineered information system simultaneously accelerated clinical decisions while reducing safety risks.10
Running parallel to routine clinical commitments, a stand-alone nurse-led DR screening clinic now provided clear evidence of an expanded professional scope, recognized as key members of the multidisciplinary workforce.10,11,25,30,33 This clinic was designed to operate upstream of physician-led interventions, and serves as the single portal through which image acquisition, grading, triage and brief counselling occur in one episode, shortening the patient journey and protecting sight.25,30 Insights from semi-structured interviews carried out in this setting have identified both enablers and obstacles to attendance, yielding actionable data for service refinement.32 Senior nurses also oriented new staff and undertook performance reviews, measured that safeguard team efficiency and keep clinical targets in view.10,24,25,30 By embedding nurse-led DR screening clinics within chronic disease management pathways, the model ensured that only patients whose images reveal sight-threatening DR (STDR) or uncertain disease were referred to the ophthalmologists.25,30 This allocation preserved limited specialist time for patients requiring urgent interventions, reduced avoidable referrals and strengthened overall system efficiency.
Health Consultant and Manager
Within nurse-led DR screening programs, each nurse functioned simultaneously as a health consultant and care manager who translates evidence into daily practice.10
Certified diabetes nurse educators (CDNEs) weaved retinal imaging into routine self-management sessions by explaining glycemic control and DR pathogenesis, constructing a risk-stratified screening calendar, and agreeing on an individualized prevention plan during the same consultation.9,10,22,28 This single-encounter approach closed the gap between glucose advice and eye care and raised screening uptake from 29% to 47% within six months, while the average interval between retinal assessments fell from 4.8 months to same-day completion.9 Although these figures remained below population targets, they demonstrated that a nurse-anchored one-stop service can rapidly expand retinal evaluation coverage.
As a health manager, the nurses served as the clinical linchpin by standardizing electronic eye-health records, conducting longitudinal data audits to detect early changes in DR status, and triggering timely escalation when required.3 They also reframed epidemiological risk into accessible language, empowering patients to become informed partners who adhere to appointments, follow treatment plans, and adopt sight-preserving behaviors.3,10,11 These responsibilities contributed to sustained quality improvements through the PDSA cycle and supported the cost-effectiveness required for program scalability.
To advance health equity, nurses adapted their communication style for racially and ethnically diverse populations.34 Australian Indigenous participation in DR screening remains low, limiting access to timely therapy.3,10,11 Leveraging the regular nurse-patient consultation and adopting culturally sensitive education can embed screening into usual care, facilitate prompt DR identification, and streamline referral for sight-threatening disease.3,10,11 By acquiring retinal images during the diabetes visit, the same nurse removed the need for a separate ophthalmology appointment. Patients could complete both assessments in one episode and leave the clinic without further delay, while workflow efficiency was enhanced by reducing reliance on specialists’ appointment waiting lists.9 A pragmatic South African cohort study quantified the attainable gain.9
Technician and Data Collector
Nurses, in their dual capacity as technicians and data collectors, fulfilled pivotal roles indispensable to the effective execution and success of the screening process.35 They undertook various technical and data management tasks, which are instrumental in bolstering patient care and research endeavors. Nurses were primarily responsible for carrying out basic ophthalmic examinations,11,22,23,25,28 and gathering sociodemographic data and ophthalmic history from patients,3,10,26–28 which include essential procedures such as measuring visual acuity, assessing intraocular pressure, and instilling dilating eye drops.
Recent studies indicated that additional significant responsibilities include performing retinal photography3,10,11,20,21,24,28 and interpreting the resulting images in accordance with established grading criteria.23–27 In Australia, empirical practice demonstrated that ophthalmic nurse practitioners achieve both sensitivity and specificity exceeding 90% for the detection of STDR, indicating that virtually every affected eye can be identified under their care.25 Nurses working in non-communicable disease (NCD) clinics completed certified training in retinal photography and subsequently delivered screening to 75% of all people with diabetes enrolled at their respective sites.28 In Canada, it had been demonstrated that nurses are able to accurately to assess and identify DR and maintain a high degree of consistency with doctors (k=0.67).21
Unfortunately, no additional themes could be identified due to the limited number of publications available in this field and the relatively narrow scope of content.
Discussion
To our knowledge, this is the first paper to synthesize and analyze the literatures on the influence of nurse-led screening on DR screening practices and to delineate nurses’ roles and contributions to DR screening. According to the temporal and geographical distribution of the included studies, this not only reflects the growing global burden of diabetes and DR but also highlights the crucial role of nurses in mitigating this public health.13 Despite their potential, nurses, as frontline healthcare managers, are often confined to traditional clinical tasks rather than broader roles in disease prevention, early diagnosis, health education, and chronic care management.14 This review highlights that nurse-led DR screening models remain underexplored in clinical practice.
The Differences Among Nurse-Led and Other Screening Models for DR
The growing burden of DR necessitates innovative and scalable screening models that extended beyond the conventional approach. Compared with other non-ophthalmologist based screening approaches, such as those led by primary care physicians, optometrists, vision technicians, or pharmacists, the nurse-led models demonstrated distinct advantages in clinical integration, patient accessibility and diagnostic performance.
Nurses, particularly those working in NCD clinics, had been effectively trained as fundus photographers and image evaluators.28 Studies reported that ophthalmic nurse practitioners achieve excellent sensitivity (93%) and specificity (91%) in detecting any DR, with an ability to identify all cases of STDR.25 This performance was comparable to, and in some contexts superior to, other non-ophthalmologist screeners. For instance, while primary care physicians using non-mydriatic handheld cameras showed sensitivities above 90% for referable DR,36 their engagement may be limited by logistical constraints such as imaging costs, lack of interest in ophthalmic diagnosis, and the need for coordination with reading centers.15 Optometrists, vision technicians, and pharmacists had been effectively incorporated into DR screening initiatives.37,38 In many communities, optometrists and vision technicians often served as the primary contact points for eye care, with trained optometrists demonstrating sensitivity rates of 88%–95% in detecting sight-threatening conditions.37,39 Pharmacist-led screening, although a relatively new approach, provided high accessibility due to the frequency of patient interactions.38 However, their roles were generally limited to ocular health or medication-related services. Vision technicians played a vital role in remote areas under the “Refract, Recognize, Refer” framework,37 while pharmacists contributed through a modified “Medicine, Recognize, Refer” model in regions where other healthcare professionals were scarce.38 Despite these contributions, such models lacked the comprehensive clinical expertise and integration with routine diabetes care that nurse-led models inherently provide.
Advantages in Nurse-Led DR Screening
As care delivery paradigms continue to evolve, nurse-led models had emerged as conceptual frameworks that operationalize nursing expertise through primary responsibility for patient-centered care coordination, outcome optimization, holistic health strategies, and interdisciplinary collaboration.40 These structured care approaches, now integrated into diverse health policy agendas in some countries and regions, demonstrated particular efficacy in chronic disease management by aligning practice-based protocols with localized care realities.41,42 Although the specific expansion of nurses’ roles and contributions varies among original articles, the overall pattern is clear. In remote and rural areas, the expansion of registered nurses’ roles in diabetes care has demonstrated a substantial impact on community disease management, as evidenced by Morgan.13 In this context, the nurse-led DR screening models have been piloted internationally across diverse settings, demonstrating proven efficacy.
Optimizing the Accessibility of Medical Resources
Primarily, the nurse-led approach facilitated the decentralization of care by extending screening capacity beyond the ophthalmology clinic, thereby enhancing accessibility for patients, especially in underserved or remote regions where specialist services may be limited.10,21 Due to the limited availability of ophthalmologists, nurse-led screening models can increase throughput by allowing nurses to conduct preliminary screenings, triage patients more efficiently, and refer only those requiring advanced care to specialists.22 This approach maximized the use of healthcare resources and reduces the burden on specialty services.10
To our knowledge, DIABSAT was the only itinerant program in France that concurrently screens for ophthalmological, renal, neuropathic and peripheral vascular complications of diabetes.26 By using satellite links to transmit data in real time from geographically isolated areas that lack broadband, the initiative first reached populations without any regular medical cover. Its core function, however, was to strengthen existing healthcare structures and to foster coordination among professionals, while explicitly preserving rather than replacing recommended specialist follow-up. The adoption of nurse-led point-of-care fundus photography without mydriasis could alleviate the burden on diabetic patients associated with scheduling screening appointments, double the participation rate of screening, and increase the number of screenings from 161 cases per year to 330 cases.27
Patient-Centered Engagement and Cultural Alignment
Furthermore, nurse-led models were inherently more patient-centered.33 By incorporating education and counseling as core components of the screening process, these models fostered greater patient engagement and satisfaction. They empowered patients to take an active role in their health management, while also emphasizing the importance of preventive care measures and compliance with screening recommendations.3 This proactive approached contrasts with the often more reactive nature of traditional models, which may not emphasize education and support to the same extent. Nurse-led models can lead to better adherence to national screening guidelines and improved patient outcomes, such as higher screening rates and lower instances of missed appointments.10 The adaptability and scalability of nurse-led models also allowed them to be tailored to the specific cultural and socio-economic contexts of various populations, particularly in indigenous communities,21 thereby enhancing their effectiveness in diverse settings.43
During the COVID-19 pandemic, Atkinson-Briggs and colleagues embedded a nurse-led DR screening program within Indigenous communities.10 Before any intervention, nurses delivered culturally tailored, one-to-one education on retinal imaging, thereby establishing both relevance and trust. They then initiated intensive lifestyle coaching, facilitated structured discussions of clinical risk factors, and negotiated individualized targets while concurrently integrating diabetes self-management training. Compared with standard education, this approach introduced clear innovations. At the main site, 79% of people with diabetes underwent retinal photography. Despite subsequent lockdown, 76% attended scheduled DR follow-up on time, and 91% of Indigenous participants reported very high satisfaction.10 A systematic review highlights that nurse-led diabetes management may achieve superior clinical outcomes in glycemic control and biomarker improvement compared to physician-led care, with notable cost-effectiveness.44 In a point-of-care DR imaging survey, the mean satisfaction score on a 10-point Likert scale was 8.6.27 Respondents repeatedly praised the convenience of undergoing retinal imaging during their routine diabetes visit, avoiding an additional eye appointment, and highlighted the associated cost savings.27
Cost-Effectiveness Nursing Care
Nurse-led models offered advantages in terms of cost efficiency. Current DR screening models, including facility-based point-of-care systems and mobile itinerant units, required strategic integration of structural supports to optimize their localized implementation while addressing context-specific challenges. Point-of-care screening was typically conducted in medical facilities such as ophthalmology clinics, primary care centers, or endocrinology practices.9–11,20–22,27–29 This model facilitated the pooling of resources and expertise, thereby enhancing the efficiency of screenings. Itinerant screening offered convenient services for patients with diabetes through mobile inspection units staffed with qualified personnel and equipped with specialized tools to access remote areas.26 DIABSAT was a nurse-led Itinerant screening program, more cost-effective compared to the eye screening program in Burgundy,45 with a cost reduction of approximately 40 euros per person.26 Moreover, the DIABSAT examination extended beyond ophthalmology by including assessments for other diabetes-related complications, such as kidney disease.26
By allowing nurses to provide DR screening and management at lower operational costs, this approach reduces the economic and human resource demands of other models.44 The nurse-led models represent a transformative change in healthcare delivery, aligning with contemporary efforts to expand access to essential services and support comprehensive management of chronic diseases.3,21 As such, its integration into healthcare systems stands to significantly enhance the quality and efficiency of DR screening programs worldwide.
Challenges and Supports
The implementation of nurse-led DR screening models is confronted with four interrelated challenges. First, while the engagement and advancement of nurse-led initiatives are essential, they cannot be conducted in isolation and should be regarded as one component of a broader sector-wide evaluation. Second, mastery of endocrinology fundamentals, imaging protocols and classification criteria is expected, yet no standardized competency framework for case management or referral decisions has been adopted. Third, global nursing shortages mean that DR screening is frequently added to already full workloads, raising questions about the sustainable enhancement of motivation. Fourth, chronic under-funding hampers both research continuity and technological innovation, with only six identified studies reporting adequate financial support for protocol optimisation.3,10,21,24,28,29
As nurses now form the largest health workforce segment, their active participation in future eye-care delivery is not optional but essential.6 To close the identified gaps, health systems should integrate DR screening into routine nursing roles through establishing well-defined competency frameworks, allocating dedicated time, and ensuring sustained funding. Inter-professional collaboration should be prioritized so that nurses perform screening and initial grading while physicians retain oversight of complex or sight-threatening cases.46,47 Development of continuous professional is essential because literature consistently highlights four core domains for nursing practice in DR programs. These are fundus camera operation and image quality control, retinal image interpretation and grading, and evidence-based management of patients with DR.10,11,20,21,23–28 These skills are rarely covered in standard nursing curricula. Without structured education and real-time mentorship, nurses may report low confidence and inconsistent performance.24
Technological innovation is reshaping DR screening, with nurse-led models playing a leading role in this advancement. Portable fundus cameras and smartphone-based ophthalmoscopes now enable nurses to capture high-quality retinal images in rural clinics, community halls or patients’ homes, facilitating early detection in underserved regions where ophthalmic services are scarce.48,49 Although, only five studies in the current review specifically examined satellite data transmission and other telemedicine solutions under resource-limited conditions,20,23,26,28,29 their findings indicated that reliable telemedicine plus rational resource allocation are the promotion for compliance of screening. By integrating artificial intelligence-supported diagnostic systems, nurses could independently conduct initial grading and generate timely, accurate referrals for specialist care, thereby shortening the interval between lesion detection and treatment initiation while reducing the socioeconomic burden of diabetes-related visual loss.3,10,11,20,21,24,28 A scalable training model that combines large-volume image assessment, iterative feedback from experienced graders and periodic re-certification was delivered through clinical simulators that provide a risk-free setting for repeated practice.25,50 Online platforms, such as those used in Denmark further, enable nurses to certificate and update credentials without leaving clinical posts.50 In Australia, an ophthalmic nurse practitioner who had completed board-approved extra training was authorized to order investigations, prescribe therapeutics and refer to other specialists, illustrating how formal accreditation can extend the nurse role while maintaining patient safety.25
Sustained policy supports are now required to secure funding streams and formalize nurse competency certification. Across the Asia-Pacific region, governments are embedding non-ophthalmologist screening within primary care systems and financing annual eye examinations as core diabetes indicators.51 Multi-country initiatives such as CDMP, DIABSAT, PHC and iDEES have written nurse roles into official service descriptors and allocated recurrent budgets for training, equipment and quality assurance,51 thereby creating replicable blueprints for task-shifting in retinal care while preserving physician oversight for complex cases.
At the individual level, a professional certification register linked to title promotion could reward nurses who complete accredited courses in fundus photography, image interpretation and chronic-disease management.16 The UK had already piloted such a scheme, providing institutional recognition for expanded practice.52 Performance-based subsidies tied to screening volume or referral accuracy can translate new skills into tangible salary gains, while telemedicine dashboards and AI decision support heighten nurses’ sense of autonomy and control.53,54 Together, these measures strengthened professional identity, enhanced patient care quality and secured the workforce needed for scalable, nurse-led DR screening.
Limitations
Although a broad overview of nurse-led DR screening models was provided, it inevitably captured only a partial representation of the full spectrum of nursing roles and failed to reflect a standardized division of responsibilities. Data on cost and compliance were explicitly reported in only a limited number of studies, while the majority focused primarily on assessing the feasibility of expanding nursing roles in screening, without providing detailed metrics on adherence or economic implications. The gap reflected a genuine paucity of published studies rather than any deficiencies in the formulation of the question or eligibility criteria. We therefore proposed that future research adopt primary methodologies such as national surveys, expert consensus forums, or direct field observation, to capture unpublished experience and establish baseline metrics that are currently lacking in the existing literatures.
Conclusion
This scoping review aims to map the current roles, contributions, advantages, and challenges of the nurse-led models in DR screening as described in the global literatures, and to determine whether cost-effectiveness data and adherence metrics are utilized to guide program implementation. The nurse-led model is a promising approach that integrates diverse resources, including eye examinations, diabetes education, data collection, and fundus imaging, thereby improving screening efficiency and reducing costs. Unfortunately, the available evidence in the literature remains limited and fragmented. Most of the reports simply explored the feasibility of expanding nursing roles to conduct retinal photography, while standardized competency frameworks, compliance rates, and economic analyses were rarely presented.
Future research should therefore prioritize the collection of primary data on the current nurse-led DR screening workforce, quantify the clinical and economic benefits associated with each nursing cadre, and conduct comparative analyzes of performance across rural, urban, and resource-limited settings. Comparative studies should further examine how nurse-led initiatives could complement ophthalmologists, optometrists, and AI-supported grading systems, and how the combined workforce could collectively accelerate progress toward achieving international goals for blindness reduction. Research should also evaluate real-world policy, financing support, and digital-health platforms that enhance uptake and must offer implementable improvements for people with diabetes worldwide. Finally, it is essential to clarify the collaborative mechanisms among government agencies, training institutions, professional care organizations, and ophthalmic care departments to effectively attract, retain, and rationally allocate nursing personnel, thereby positioning them as key contributors to future DR screening initiatives.
Acknowledgments
We want to thank all members of the Clinic Research Center and the Nursing Department of Tianjin Medical University Eye Hospital.
Funding
Funded by 2024 Tianjin Nursing Society Research Project (tjhlky2024QN06).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sun H, Saeedi P, Karuranga S, et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
2. Teo ZL, Tham YC, Yu M, et al. Global prevalence of diabetic retinopathy and projection of burden through 2045: systematic review and meta-analysis. Ophthalmology. 2021;128(11):1580–1591. doi:10.1016/j.ophtha.2021.04.027
3. Atkinson‐Briggs S, Jenkins A, Keech A, Ryan C, Brazionis L. A model of culturally‐informed integrated diabetes education and eye screening in indigenous primary care services and specialist diabetes clinics: study protocol. J Adv Nurs. 2021;77(3):1578–1590. doi:10.1111/jan.14734
4. Das T, Takkar B, Sivaprasad S, et al. Recently updated global diabetic retinopathy screening guidelines: commonalities, differences, and future possibilities. Eye. 2021;35(10):2685–2698. doi:10.1038/s41433-021-01572-4
5. He J, Cao T, Xu F, et al. Artificial intelligence-based screening for diabetic retinopathy at community hospital. Eye. 2020;34(3):572–576. doi:10.1038/s41433-019-0562-4
6. Machin HM, Daniell M, Entwistle LI, et al. A scoping review on determining australian nurse engagement in eye care settings. Clin Ophthalmol. 2023;17:393–401. doi:10.2147/opth.S391734
7. Hazin R, Colyer M, Lum F, Barazi MK. Revisiting diabetes 2000: challenges in establishing nationwide diabetic retinopathy prevention programs. Am J Ophthalmol. 2011;152(5):723–729. doi:10.1109/TMI.2015.2506902
8. Li X, Tan T-E, Wong TY, Sun X. Diabetic retinopathy in China: epidemiology, screening and treatment trends—A review. Clin Exper Ophthalmol. 2023;51(6):607–626. doi:10.1111/ceo.14269
9. Mumba M, Hall A, Lewallen S. Compliance with eye screening examinations among diabetic patients at a tanzanian referral hospital. Ophthalmic Epidemiol. 2007;14(5):306–310. doi:10.1080/09286580701272079
10. Atkinson‐Briggs S, Jenkins A, Ryan C, Brazionis L. Mixed diabetic retinopathy screening coverage results in indigenous Australian primary care settings: a nurse‐led model of integrated diabetes care. J Adv Nurs. 2022;78(10):3187–3196. doi:10.1111/jan.15163
11. Atkinson-Briggs S, Jenkins A, Keech A, Ryan C, Brazionis L. Prevalence of diabetic retinopathy and reduced vision among indigenous Australians in the nurse-led integrated diabetes education and eye screening study in a regional primary care clinic. Intern Med J. 2023;53(7):1188–1195. doi:10.1111/imj.15625
12. Sinclair SH, Schwartz S. Diabetic retinopathy: new concepts of screening, monitoring, and interventions. Surv Ophthalmol. 2024;69(6):882–892. doi:10.1016/j.survophthal.2024.07.001
13. Morgan PA, Smith VA, Berkowitz TSZ, et al. Impact of physicians, nurse practitioners, and physician assistants on utilization and costs for complex patients. Health Aff. 2019;38(6):1028–1036. doi:10.1377/hlthaff.2019.00014
14. Silpa-archa S, Limwattanayingyong J, Tadarati M, Amphornphruet A, Ruamviboonsuk P. Capacity building in screening and treatment of diabetic retinopathy in Asia-Pacific region. Indian J Ophthalmol. 2021;69(11):2959–2967. doi:10.4103/ijo.IJO_1075_21
15. Rani PK, Takkar B, Das T. Training of nonophthalmologists in diabetic retinopathy screening. Indian J Ophthalmol. 2021;69(11):3072–3075. doi:10.4103/ijo.IJO_1117_21
16. Machin H, Daniell M, Entwistle L, et al. Australian nurse engagement in eye care: a national survey. Clin Ophthalmol. 2024;18:1829–1840. doi:10.2147/opth.S463743
17. Michelotti MM, Abugreen S, Kelly SP, et al. Transformational change: nurses substituting for ophthalmologists for intravitreal injections - a quality-improvement report. Clin Ophthalmol. 2014;8:755–761. doi:10.2147/opth.S59982
18. A H, Om L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
19. Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5(1):69. doi:10.1186/1748-5908-5-69
20. Schneiders J, Telo GH, Lavinsky D, Dos Reis MA, Corrêa BG, Schaan BD. Organizational intervention to improve access to retinopathy screening for patients with diabetes mellitus: health care service improvement project in a tertiary public hospital. Prim Care Diabetes. 2023;17(4):354–358. doi:10.1016/j.pcd.2023.05.007
21. Spurr S, Bullin C, Bally J, Trinder K, Khan S. Nurse-led diabetic retinopathy screening: a pilot study to evaluate a new approach to vision care for Canadian Aboriginal peoples. Int J Circumpolar Health. 2018;77(1):1422670. doi:10.1080/22423982.2017.1422670
22. Watkinson S, Chetram N. A nurse-led approach to diabetic retinal screening. Nurs Times. 2005;101(36):32–34.
23. Boucher MC, Nguyen MTD, Qian J. Assessment of training outcomes of nurse readers for diabetic retinopathy telescreening: validation study. JMIR Diabetes. 2020;5(2):e17309. doi:10.2196/17309
24. Fernández-Gutiérrez DÁ, Núñez-Marrero J, Martínez-Alberto CE, et al. Knowledge of diabetic retinopathy among primary care nurses performing fundus photography and agreement with ophthalmologists on screening. Nurs Rep. 2023;13(3):1064–1076. doi:10.3390/nursrep13030093
25. Kirkwood BJ, Coster DJ, Essex RW. Ophthalmic nurse practitioner led diabetic retinopathy screening. Results of a 3-month trial. Eye. 2006;20(2):173–177. doi:10.1038/sj.eye.6701834
26. Turnin M-C, Schirr-Bonnans S, Chauchard M-C, et al. DIABSAT telemedicine itinerant screening of chronic complications of diabetes using a satellite. Telemed J E Health. 2017;23(5):397–403. doi:10.1089/tmj.2016.0185
27. Newman R, Cummings DM, Doherty L, Patel NR. Digital retinal imaging in a residency-based patient-centered medical home. Fam Med. 2012;44(3):159–163.
28. Ramakrishnan R, Abdul Khadar SM, Srinivasan K, Kumar H, Vijayakumar V. Diabetes mellitus in the Tamil Nadu state-noncommunicable diseases nurse model in diabetic retinopathy screening. Indian J Ophthalmol. 2020;68(Suppl 1):S78–S82. doi:10.4103/ijo.IJO_1987_19
29. Welch G, Allen NA, Zagarins SE, Stamp KD, Bursell S-E, Kedziora RJ. Comprehensive diabetes management program for poorly controlled hispanic type 2 patients at a community health center. The Diabetes Educator. 2011;37(5):680–688. doi:10.1177/0145721711416257
30. Almouqati F, Daire J, Catanach C, deSousa JL, Quill S, Estai M. Factors associated with adherence to diabetic retinopathy screening among patients attending a nurse-led community clinic in australia: a qualitative study. Nurs Rep. 2025;15(1):23. doi:10.3390/nursrep15010023
31. Iriarte‐Roteta A, Lopez‐Dicastillo O, Mujika A, et al. Nurses’ role in health promotion and prevention: a critical interpretive synthesis. J Clin Nurs. 2020;29(21–22):3937–3949. doi:10.1111/jocn.15441
32. Christoff P. Running PDSA cycles. Curr Probl Pediatr Adolesc Health Care. 2018;48(8):198–201. doi:10.1016/j.cppeds.2018.08.006
33. Procter S, Wilson PM, Brooks F, Kendall S. Success and failure in integrated models of nursing for long term conditions: multiple case studies of whole systems. Int J Nurs Stud. 2013;50(5):632–643. doi:10.1016/j.ijnurstu.2012.10.007
34. Macias-Konstantopoulos WL, Collins KA, Diaz R, et al. Race, healthcare, and health disparities: a critical review and recommendations for advancing health equity. West J Emerg Med. 2023;24(5):906–918. doi:10.5811/westjem.58408
35. Schultz MA, Walden RL, Cato K, et al. Data science methods for nursing-relevant patient outcomes and clinical processes: the 2019 literature year in review. Comput Inform Nurs. 2021;39(11):654–667. doi:10.1097/cin.0000000000000705
36. Farley TF, Mandava N, Prall FR, Carsky C. Accuracy of primary care clinicians in screening for diabetic retinopathy using single-image retinal photography. Ann Fam Med. 2008;6(5):428–434. doi:10.1370/afm.857
37. Rao GN, Khanna RC, Athota SM, Rajshekar V, Rani PK. Integrated model of primary and secondary eye care for underserved rural areas: the L V Prasad eye institute experience. Indian J Ophthalmol. 2012;60(5):396–400. doi:10.4103/0301-4738.100533
38. Coronado AC, Zaric GS, Martin J, Malvankar-Mehta M, Si FF, Hodge WG. Diabetic retinopathy screening with pharmacy-based teleophthalmology in a semiurban setting: a cost-effectiveness analysis. CMAJ Open. 2016;4(1):E95–E102. doi:10.9778/cmajo.20150085
39. Ramasamy K, Mishra C. Capacity building for diabetic retinopathy screening by optometrists in India. Indian J Ophthalmol. 2021;69(3):482. doi:10.4103/ijo.IJO_3716_20
40. Johnson C, Ingraham MK, Stafford SR, Guilamo-Ramos V. Adopting a nurse-led model of care to advance whole-person health and health equity within Medicaid. Nurs Outlook. 2024;72(4):102191. doi:10.1016/j.outlook.2024.102191
41. Aldahmashi H, Maneze D, Molloy L, Salamonson Y. Nurses’ adoption of diabetes clinical practice guidelines in primary care and the impacts on patient outcomes and safety: an integrative review. Int J Nurs Stud. 2024;154:104747. doi:10.1016/j.ijnurstu.2024.104747
42. Wilson PM, Kendall S, Brooks F. Nurses’ responses to expert patients: the rhetoric and reality of self-management in long-term conditions: a grounded theory study. Int J Nurs Stud. 2006;43(7):803–818. doi:10.1016/j.ijnurstu.2005.10.011
43. Rajalakshmi R, Prathiba V, Rani PK, Mohan V. Various models for diabetic retinopathy screening that can be applied to India. Indian J Ophthalmol. 2021;69(11):2951–2958. doi:10.4103/ijo.IJO_1145_21
44. Crowe M, Jones V, Stone MA, Coe G. The clinical effectiveness of nursing models of diabetes care: a synthesis of the evidence. Int J Nurs Stud. 2019;93:119–128. doi:10.1016/j.ijnurstu.2019.03.004
45. Beynat J, Charles A, Astruc K, et al. Screening for diabetic retinopathy in a rural French population with a mobile non-mydriatic camera. Diabetes Metab. 2009;35(1):49–56. doi:10.1016/j.diabet.2008.07.002
46. Vázquez-Calatayud M, Errasti-Ibarrondo B, Choperena A. Nurses’ continuing professional development: a systematic literature review. Nurse Educ Pract. 2021;50:102963. doi:10.1016/j.nepr.2020.102963
47. Redwood T, Ward A, Ali T, O’Dell C, Poole C, Rebaudo D. Continued professional development (CPD) provision for nurses: a qualitative exploration. Heliyon. 2024;10(12):e32582. doi:10.1016/j.heliyon.2024.e32582
48. Wang S, Jin K, Lu H, Cheng C, Ye J, Qian D. Human visual system-based fundus image quality assessment of portable fundus camera photographs. IEEE Trans Med Imaging. 2016;35(4):1046–1055. doi:10.1109/tmi.2015.2506902
49. Singh A, Cheyne K, Wilson G, Sime MJ, Hong SC. On the use of a new monocular-indirect ophthalmoscope for retinal photography in a primary care setting. N Z Med J. 2020;133(1512):31–38.
50. Andersen JKH, Hubel MS, Savarimuthu TR, Rasmussen ML, Sørensen SLB, Grauslund J. A digital online platform for education and certification of diabetic retinopathy health care professionals in the Region of Southern denmark. Acta Ophthalmol. 2022;100(5):589–595. doi:10.1111/aos.15123
51. Resnikoff S, Lansingh VC, Washburn L, et al. Estimated number of ophthalmologists worldwide (international council of ophthalmology update): will we meet the needs? Br J Ophthalmol. 2020;104(4):588–592. doi:10.1136/bjophthalmol-2019-314336
52. Simcock P, Kingett B, Mann N, Reddy V, Park J. A safety audit of the first 10 000 intravitreal ranibizumab injections performed by nurse practitioners. Eye. 2014;28(10):1161–1164. doi:10.1038/eye.2014.153
53. Padhy SK, Takkar B, Chawla R, Kumar A. Artificial intelligence in diabetic retinopathy: a natural step to the future. Indian J Ophthalmol. 2019;67(7):1004–1009. doi:10.4103/ijo.IJO_1989_18
54. Scanzera AC, Beversluis C, Potharazu AV, et al. Planning an artificial intelligence diabetic retinopathy screening program: a human-centered design approach. Front Med. 2023;10:1198228. doi:10.3389/fmed.2023.1198228
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.