Back to Journals » Patient Preference and Adherence » Volume 9
Nurse-led intensive interventions improve adherence to continuous positive airway pressure therapy and quality of life in obstructive sleep apnea patients
Authors Chen X, Chen W, Hu W, Huang K, Huang J, Zhou Y, Wang Y
Received 20 June 2015
Accepted for publication 27 October 2015
Published 26 November 2015 Volume 2015:9 Pages 1707—1713
DOI https://doi.org/10.2147/PPA.S90846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Naifeng Liu
Xiaofen Chen,1 Weiting Chen,1 Weijie Hu,2 Kui Huang,3 Jing Huang,4 Yu Zhou5
1Hospital of Stomatology, Wenzhou Medical University, Wenzhou, 2People Hospital of Tiantai, Taizhou, 3Department of Orthodontics, Hospital of Stomatology, Wenzhou Medical University, Wenzhou, 4The Second Affiliated Hospital Zhejiang University School of Medicine, Hangzhou, 5Department of Orthodontics, Hospital of Stomatology, Wenzhou Medical University, Wenzhou, People’s Republic of China
Background: Continuous positive airway pressure (CPAP) is widely recommended for the treatment of sleep apnea/hypopnea syndrome (SAHS), but its usage by patients is very low. The aim of this study was to assess intensive educational programs and nursing support for the improvement of CPAP use and outcomes in SAHS patients.
Methods: Eighty new SAHS patients were randomized to receive nurse-led intensive interventions or usual support at hospital and home. The main outcome measure was CPAP use; changes in sleeping, symptoms, mood, and quality of life were also assessed after 12 months of treatment.
Results: All outcome measures were improved after treatment in both groups. However, patients receiving intensive support with significantly higher CPAP use (higher daily CPAP usage by 2.2 hours/day) had greater improvements in SAHS symptoms and mood (P<0.05). The intervention group further showed an improvement in the Short Form-36 domains of mental and physical health (P<0.05).
Conclusion: The CPAP usage and quality of life can be significantly improved by nurse-led intensive program in obstructive sleep apnea patients.
Keywords: CPAP, quality of life, SAHS, compliance
Introduction
Obstructive sleep apnea (OSA) is a common sleep disorder, and continuous positive airway pressure (CPAP) is the most effective treatment for this disease, but its success is closely related to the patients’ compliance rate. Annually, 20%–30% of patients stop using CPAP within the first 2 weeks after receiving CPAP treatment and ~30% of patients stop using within 6 months.1,2
There are an increasing number of articles on the effects of interventions on CPAP compliance, when recognizing the importance of compliance rates in the OSA population.3–6 Strategies include technological, educational, pharmacological, psychosocial, and multidimensional approaches. Although some strategies have proved to be effective in improving CPAP usage, orthodontic application was not suitable and cost-effectiveness was high. To date, one of the standard care for OSA patients is patient education.7 Additionally, it may play an important role in deciding to accept CPAP treatment for OSA patients.8 Bandura also found that patients’ education is not only a fact that influences the health behavior but also a critical part to committing to the behavior.9
Many single-center studies have showed that the compliance could be improved by patient education.10,11 American Academy of Sleep Medicine Adult Obstructive Sleep Apnea stressed the importance of patient education in the treatment of OSA patients.7 Therefore, patient education, especially how much complexity is required in the education program, is becoming a more and more important strategy for improving CPAP use. Is it sufficient to provide the explanation and the written material to improve the CPAP use or should we set up multiple educational programs for the OSA patients who need to receive CPAP treatment? The answers to these questions are contradictory and need to be further investigated.
Improving obstructive sleep apnea syndrome (OSAS) and patients’ quality of life is the most important target of treatment. Many studies had shown that although it is difficult, the quality of life can be improved by CPAP treatment.4,12,13 However, how the patient’s education improves the quality of life has not been studied clearly.14–17 Thus, the effect of education needs to be examined in more number of patients, so that the results can be more widely applicable and acceptable.
Therefore, the aim of the present study was to assess a simple educational input on improving CPAP compliance and quality of life in OSAS patients.
Materials and methods
This study was designed as a randomized, single-blinded, prospective trial of nurse-led intensive vs standard support in new OSA patients who were first to receive CPAP therapy. The Stomatology Hospital Ethics Committee approved this research. All the included subjects gave written informed consent, and they were unaware of the type of treatment they received: “intensive” or “standard” support.
Subjects
Subjects were recruited in May and August 2012 from three sleep disorder clinics in Zhejiang, People’s Republic of China. Inclusion criteria were: 1) apneas plus hypopneas >15/hour; 2) daytime sleepiness; 3) two major symptoms of the syndrome; 4) lived within 100 miles from Zhejiang. Individuals were excluded if: 1) previously received CPAP therapy; 2) suffering with chronic obstructive pulmonary disease, asthma, or neurological problems. At last, 80 consecutive patients with sleep apnea/hypopnea syndrome (SAHS) met the inclusion criteria.
Protocol
The included patients were randomized into two groups via a predetermined balanced block which was generated by tossing a coin: standard support group and intensive support group. Patients were blinded to the allocation and did not know to which group they were assigned.
Upon enrollment, each subject completed a self-administered Epworth sleepiness scale (ESS) with a validated measure of daytime sleepiness, and the following information was collected: the subjects’ attained level of education, occupation (subsequently classified as blue collar, white collar, or other), the approximate family income (within six categorical levels), whether the subject lived alone, whether the subject understood “what CPAP is and why (he or she) needs it”, and whether the subject had a close friend or relative who had used CPAP. Additional variables, obtained through polysomnography, included Apnea–Hypopnea Index, lowest oxygen saturation recorded, CPAP pressure assigned after a CPAP titration study, and (for most patients) multiple sleep latency test (MSLT) to record mean sleep latency.
Eligible patients were recommended to wear CPAP machine (Sullivan S6, Sydney, NSW, Australia) as long as possible when they were sleeping. The plastic strip was designed to hide the CPAP clock-timers. Patients were not aware of the presence of clock-timer during treatment; both nurse, who recorded the clock-timer, and patients were blinded to the group allocation. Patients could contact us for help, such as asking for support and questions about treatment, by telephone at any time during the treatment duration.
Intervention
We developed a series of patient education support intervention programs that we thought would be easy to apply in the standard clinical trial. Twenty-five nurses were involved in this multicenter trial. The intervention included the following support protocol:
- Hospital health education: before treatment, nurses showed patients a 30-minute educational video that explained the pathogen, mechanism, risks, benefit, and treatment methods for SAHS; personalized guidance: a nurse used different teaching methods for different people, to enable the patients to select the method convenient for them and use it as long as possible; and an SASH Health education Manual was issued.
- Patient self-management interventions, including: 1) within 5 days after receiving CPAP treatment, the nurses contacted the patients and held a 15-minute interview to find out if they faced any problems and offered help by telephone. 2) In order to reduce the problems caused by treatment, the nurses made home visits to the patients after CPAP treatment was initiated. 3) Adjustment in patient’s lifestyle, such as guiding patients to adjust their diet, reduce the intake of high-calorie foods, try to keep the health life, and increase activity in daily life, was suggested. 4) Psychological intervention, informing patients of the importance of maintaining a good mental state for disease rehabilitation, and teaching the patients methods and techniques on how to respond to anxiety and depression.
Patients had to have an appointment with the sleep physician within 1 month of the initiation of CPAP treatment. Each consultation lasted ~30 minutes, which included clinical examination, answering of queries raised by the patients, and offering help.
Control group
Patients who did not receive the intervention were also required to have an appointment with the sleep physician at 1, 3, 6, and 12 months. Each consultation lasted ~30 minutes, which included clinical examination, answering any questions, and offering help. If the patients had any questions, they could contact the nurse by telephone within office hours.
Outcome measurements
The data regarding the usage of CPAP by the patients were recorded and handled with professional software (ResMed SCAN 5.3, NSW, Australia) at each clinical visit.
All subjects underwent a daytime function testing at the beginning and after 12 months of the initiation of CPAP treatment. Function testing included the following steps: an in-house questionnaire was given to assess the severity of sleep apnea symptoms; Epworth and Stanford sleepiness scales were calculated to assess sleepiness; mood was evaluated using the Hospital Anxiety and Depression Scale; and quality of life was measured by the Short Form-36.
Data and statistical analysis
An intention-to-treat (ITT) analysis was applied. The unpaired t-test and chi-square test were used for baseline analysis in the two groups. The unpaired t-test was also used for comparison between intervention and control group. The paired t-test was used for assessing improvement of variables from baseline. Statistical significance was set at P<0.05. All statistical analyses were performed with SPSS17.0 software (SPSS Inc., Chicago, IL, USA).
Results
Among the 85 enrolled subjects, five did not agree to participate, leaving 80 subjects who completed the protocol and formed the basis for this report. Any dropout was registered (Figure 1).
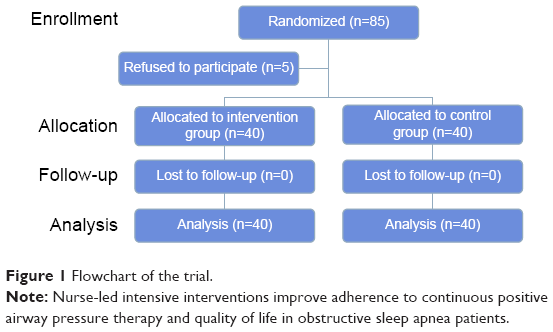 | Figure 1 Flowchart of the trial. |
At baseline, we did not find any significant difference between the intensive support and standard support groups in all outcome measures (Table 1).
 | Table 1 Patients’ baseline characteristics |
CPAP usage
The average compliance was 2.2 hours (51%) longer among subjects in the intensive support group than those in the standard support group; this difference was statistically significant between the two groups (Table 2 and Figure 2).
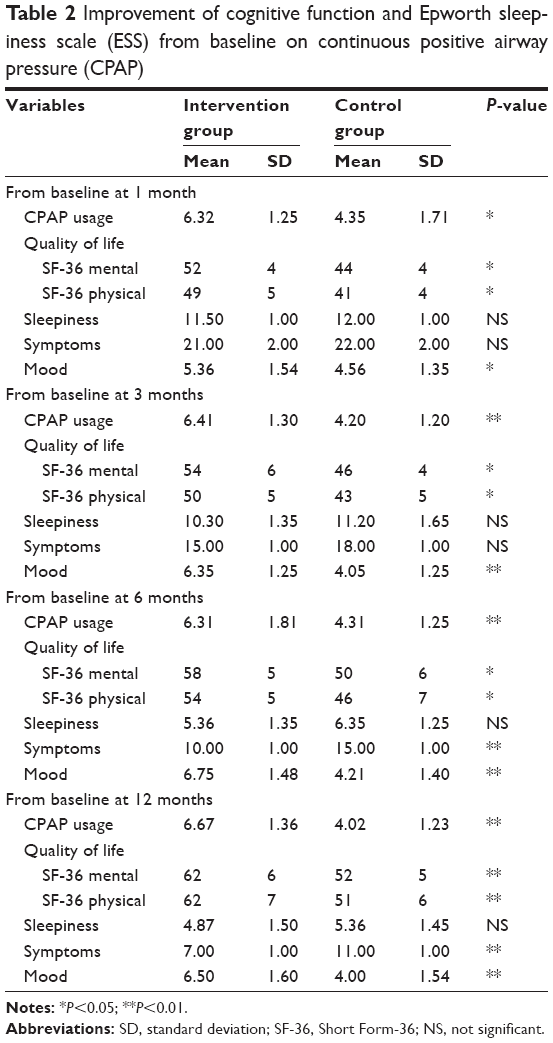 | Table 2 Improvement of cognitive function and Epworth sleepiness scale (ESS) from baseline on continuous positive airway pressure (CPAP) |
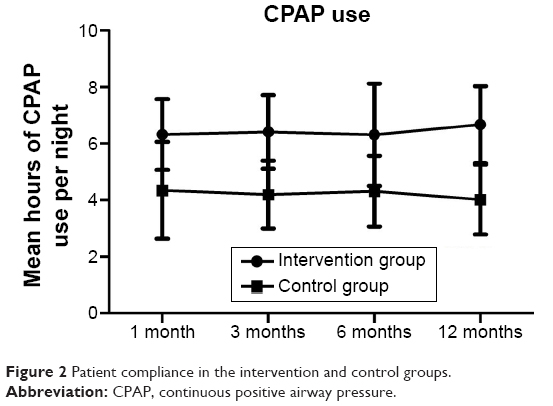 | Figure 2 Patient compliance in the intervention and control groups. |
Quality of life
The quality of life was significantly improved after CPAP treatment in both the groups. Moreover, after 12 months of treatment, the outcome was significantly different between the groups (Table 2 and Figure 3). This shows that both mental and physical health significantly improved in the intervention group over the control group. This improvement was maintained until 12 months.
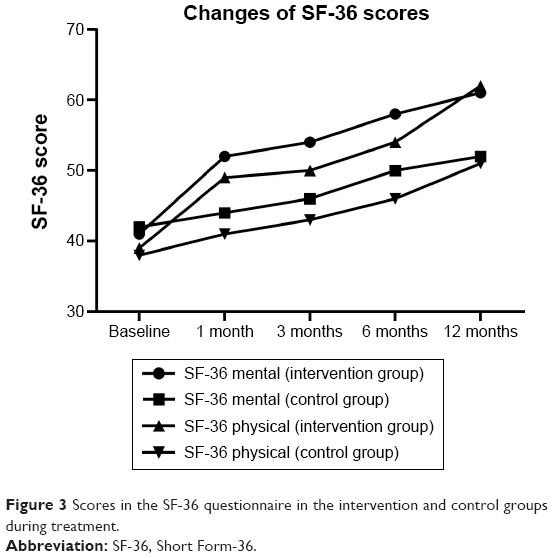 | Figure 3 Scores in the SF-36 questionnaire in the intervention and control groups during treatment. |
Sleepiness
ESS significantly decreased from 1 to 12 months (P<0.001) in both the groups. Although the scores of ESS were not significantly different between the two groups, control group reported higher values than the intervention group (Table 2 and Figure 4).
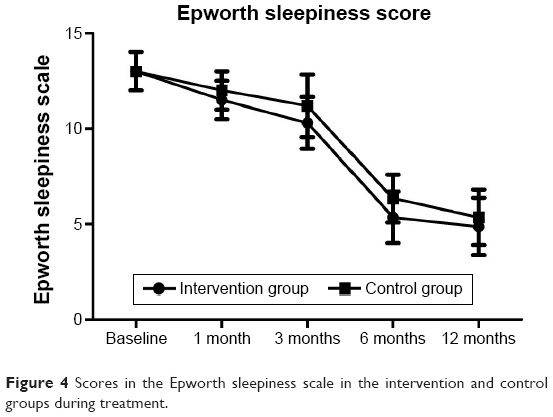 | Figure 4 Scores in the Epworth sleepiness scale in the intervention and control groups during treatment. |
Symptoms
Symptom scores significantly decreased from 1 to 12 months (P<0.001) in both groups. Symptom scores were reported to be higher in the control group than in the intervention group, and significantly lower symptom scores were observed at 6 and 12 months in the intervention group than the control group (Table 2 and Figure 5).
 | Figure 5 Scores of the symptoms in the intervention and control groups during treatment. |
Mood
Mood scores significantly increased from 1 to 12 months (P<0.001) in the intervention group. Mood scores were reported to be higher in the intervention group than in the control group, and the difference was significant between the two groups (Table 2 and Figure 6).
 | Figure 6 Scores of mood in the intervention and control groups during treatment. |
Discussion
This randomized controlled trial showed that nurse-led interventions can increase compliance with CPAP and alleviate symptoms, benefit mood, and improve quality of life in SAHS patients. The results of this study showed that nurse-led intensive support could significantly improve CPAP usage and quality of life in SASH patients.
To the best of our knowledge, the current intervention is one of the simplest among reported obstructive sleep apnea-hypopnea syndrome (OSASH) education programs to enhance adherence to CPAP use and improve quality of life in OSASH.3–6 Additionally, the duration of this study was 12 months, which was much longer than other similar studies.3,4 It was long enough to assess the impact of this intervention over standard care on the changes of quality of life and usage of CPAP. The results indicated that our education program achieved a significant improvement in quality of life and CPAP usage, and other studies have come to a similar conclusion.1,4,18–21 Only a few studies showed significant improvements in quality of life in the intervention group, compared to the control group.18,19 This may be because of the small effect of sizes and differences between the samples in different studies.
In this study, we found that our intensive support could significantly improve CPAP use and achieve better results compared to standard support. The mean CPAP usage was higher than that reported by Pepin et al22 in a European study and that of Kribbs et al23 in an American population. Apart from different patient populations, this can also be explained by the following reasons: educational programs on OSA and CPAP, practical CPAP education, and a clinical review and home visits by our nurses. Finally, all our patients had to buy the CPAP appliance by themselves, and this may have been a motivating factor. These are essential factors to achieve better CPAP use in our study. Thus, we had reasons to believe that long-term follow-up of patients will eventually show that intervention must be repeated or reinforced to maintain an initial effect. However, studies suggest that CPAP compliance at the first month could reliably predict compliance of treatment with CPAP at 3 or 6 months.23,24 These data, combined with our results, supported proactive intervention to improve compliance at the time CPAP is first prescribed.
Many studies had been conducted to improve CPAP compliance in patients.15,25,26 Fletcher and Luckett25 conducted a randomized crossover study to measure objective CPAP usage with regular telephone support or standard support. Their results found that the CPAP usage was not significantly different between the two groups. However, in this study, the patients received no additional support or frequent supportive telephone calls in the first stage of trial, which may obscure any beneficial effects. In another study, Chervin et al15 tried to assess the CPAP usage between educational and phone call. Although the difference was not statistically significant, we need to be cautious about this conclusion. Because not only the baseline level was inconsistent, but also this study exist measure bias which CPAP usage was not measure by machine. Likar et al26 conducted a study to examine the effect of the education support on CPAP usage by conducting a nonrandomized retrospective study. They suggested that education support could improve CPAP usage.
It is inevitable for most of the patients to have difference complicance in patients who completely reject or accept the machine treatment, especially in the first night. It is difficult to make a precise tactic to accommodate each patient, especially for patients who are unwilling to cooperate. So the tactic of education is integrant; at the same time, telephone support and educational literature cannot be ignored.15 With regard to patients having practical issues, they can provide their compliance by recognizing psychological factors or CPAP-related tolerance problems in early treatment stage.27 It was an advantage that benefits patients who had joined the conferences. A retrospective study by Likar et al reported that 29% of the outpatients who in their 2 hours meeting had a chance to monitor the equipment and were given education and support on symptom management would use CPAP for at least 2 hours every night. Thus, it could be a useful way to enhance the patients’ compliance.26 Similarly, the group of help by themselves could be helpful. According to the studies by others authors, the home visit may be more necessary. The finding from Hoy et al demonstrated that educational program, just like home visit, could increase the usage of CPAP by 1.5 hours every night.14 Therefore, homecare visits make an important contribution to encourage the patients to conform to this therapy. In this study, different groups received different levels of education pertaining to CPAP. The more complement the input the better compliance they had, which was positively correlated with clinical improvement. It was evident that once the input time was conducted over 4 hours, the quality of life, and clinical symptoms would be improved in OSASH patients. In accordance with Hoy’s finding, a conclusion was drawn that the degree of education did influence the efficiency of treatment. Since other studies had given the relationship between education level and compliance in the ANTADIR network, so what we got was not study-related results.13,23,28
However, a few studies were conducted to assess the changes of the quality of life in SASH patients who received CPAP therapy. The present study revealed that nurse-led intensive support significantly improved the quality of life compared to standard support. The reason was that additional support from our nurses may lead to better compliance and acquired confidence compared to standard support in some patients. Hoy et al14 reported similar results that patients who received education from the medical contact group had better compliance than patients who received information from their partner.
The improvement in mood and symptom was important to patients as it may enhance the motivation to receive CPAP treatment. In this study, we found that compliance was significantly higher in nurse-led intensive group than standard support group; this difference continued after 12 months of treatment. The reason may be the extra support helped patients to handle any problem when they used CPAP appliance and improved the motivation to CPAP treatment.
This study was a multicenter trial that was conducted in three centers. The follow-up of patients was long and complete. However, the study had certain limitations, which included small sample size. In retrospect, block randomization would have been a better design strategy. To improve the study of multiple explanatory variables and their interaction with intervention, future studies should include hundreds rather than tens of patients. Second, the nurses were not blinded to the patients, which may have caused inadvertent bias. We did our best to eliminate this bias. But it may not be the reason for the difference between the two groups. Finally, this study followed up the patients for only 12 months, whereas patients who need CPAP treatment are usually believed to be receiving a lifelong therapy. Therefore, in the future we need to conduct longer-term observations and have larger sample sizes, to assess whether the benefit of sleepiness and cognitive function caused by nurse-led intensive support was continued.
In this study, we did not include a cost–benefit analysis; the reason for this was that such analyses are highly dependent on the price of CPAP appliances, the distance between hospital and the patient’s home, and, in particular, local costs that may vary in different areas. However, in order to make the comparisons, the extra costs of the intervention group were ~500 RMB per patient, which was 1/10 of that in other sleep centers.
Conclusion
The nurse-led intensive support can significantly improve CPAP compliance and quality of life.
Disclosure
The authors report no conflicts of interest in this work.
References
Stepnowsky CJ, Marler MR, Paulau J, Brooks JA. Social-cognitive correlates of CPAP adherence in experienced users. Sleep Med. 2006;7(4):350–356. | ||
Engleman HM, Wild MR. Improving CPAP use by patients with the sleep apnoea/hypopnoea syndrome (SAHS). Sleep Med Rev. 2001;7(5):81–99. | ||
Lai AY, Fong DY, Lam JC, Weaver TE, Ip MS. The efficacy of a brief motivational enhancement education program on CPAP in OSA: a randomized controlled trial. Chest. 2014;146(3):600–610. | ||
Hui DSC, Chan JKW, Choy DKL, et al. Effects of augmented continuous positive airway pressure education and support on compliance and outcome in a Chinese population. Chest. 2000;117:1410–1416. | ||
Wang W, He G, Wang M, et al. Effects of patient education and progressive muscle relaxation alone or combined on adherence to continuous positive airway pressure treatment in obstructive sleep apnea patients. Sleep Breath. 2012;64:0149–1057. | ||
Deng T, Wang Y, Sun M, et al. Stage-matched intervention for adherence to CPAP in patients with obstructive sleep apnea: a randomized controlled trial. Sleep Breath. 2013;17:791–801. | ||
Epstein LJ, Kristo D, Strollo PJ, et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5(3):263–276. | ||
Sawyer AM, Canamucio A, Moriarty H, Weaver TE, Richards K, Kuna ST. Do cognitive perceptions influence CPAP use? Patient Educ Couns. 2011;85(1):85–91. | ||
Bandura A. Health promotion by social cognitive means. Health Educ Behav. 2004;31(2):143–164. | ||
La Piana GE, Scartabellati A, Chiesa L. Long-term adherence to CPAP treatment in patients with obstructive sleep apnea: importance of educational program. Patient Prefer Adherence. 2011;5:555–562. | ||
Wickwire EM, Lettieri CJ, Cairns AA, Collop NA. Maximizing positive airway pressure adherence in adults: a common-sense approach. Chest. 2013;144(2):680–693. | ||
Sforza E, Janssens JP, Rochat T, Ibanez V. Determinants of altered quality of life in patients with sleep-related breathing disorders. Eur Respir J. 2003;21(4):682–687. | ||
Meslier N, Lebrun T, Grillier-Lanoir V, et al. A French survey of 3,225 patients treated with CPAP for obstructive sleep apnoea: benefits, tolerance, compliance and quality of life. Eur Respir J. 1998;12(1):185–192. | ||
Hoy CJ, Vennelle M, Kingshott RN, Engleman HM, Douglas NJ. Can intensive support improve continuous positive airway pressure use in patients with the sleep apnea/hypopnea syndrome? Am J Respir Crit Care Med. 1999;159:1096–1100. | ||
Chervin RD, Theut S, Bassetti C, Aldrich MS. Compliance with nasal CPAP can be improved by simple interventions. Sleep. 1997;20(4):284–289. | ||
Flemons WW, Reimer MA. Measurement properties of the Calgary Sleep Apnea Quality of Life Index. Am J Respir Crit Care Med. 2002;165:159–164. | ||
Mok WYW, Lam CLK, Lam B, Cheung MT, Yam L, Ip MS. A Chinese version of the Sleep Apnea Quality of Life Index was evaluated for reliability, validity, and responsiveness. J Clin Epidemiol. 2004;57:470–478. | ||
Olsen S, Smith SS, Oei TPS, Douglas J. Motivational interviewing (MINT) improves continuous positive airway pressure (CPAP) acceptance and adherence: a randomized controlled trial. J Consult Clin Psychol. 2012;80:151–163. | ||
Damjanovic D, Fluck A, Bremer H, Müller-Quernheim J, Idzko M, Sorichter S. Compliance in sleep apnoea therapy: influence of home care support and pressure mode. Eur Respir J. 2009;33:804–811. | ||
Wang Y, Gao W, Sun M, Chen B. Adherence to CPAP in patients with obstructive sleep apnea in a Chinese population. Respir Care. 2012;57:238–243. | ||
Basoglu OK, Midilli M, Midilli R, Bilgen C. Adherence to continuous positive airway pressure therapy in obstructive sleep apnea syndrome: effect of visual education. Sleep Breath. 2012;16:1193–1200. | ||
Pepin J, Krieger J, Rodenstein D, et al. Effective compliance during the first 3 months of continuous positive airway pressure: a European prospective study of 121 patients. Am J Respir Crit Care Med. 1999;160:1124–1129. | ||
Kribbs NB, Pack AI, Kline R, et al. Objective measurement of patterns of nasal CPAP use by patients with obstructive sleep apnea. Am Rev Respir Dis. 1993;147:887–895. | ||
Reeves-Hoche MK, Meek R, Zwillich C. Nasal CPAP: an objective evaluation of patient compliance. Am J Respir Crit Care Med. 1994;149(1):149–154. | ||
Fletcher EC, Luckett RA. The effect of positive reinforcement on hourly compliance in nasal continuous positive airway pressure users with obstructive sleep apnea. Am Rev Respir Dis. 1991;143(5):936–941. | ||
Likar LL, Panciera TM, Erickson AD, Rounds S. Group education sessions and compliance with nasal CPAP therapy. Chest. 1997;111(5):1273–1277. | ||
Zozula R, Rosen R. Compliance with continuous positive airway pressure therapy: assessing and improving treatment outcomes. Curr Opin Pulm Med. 2001;7(6):391–398. | ||
Veale D, Chailleux E, Hoorelbeke-Ramon A, et al. Mortality of sleep apnoea patients treated by nasal continuous positive airway pressure registered in the ANTADIR observatory. Eur Respir J. 2000;15(2):326–331. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.