Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 17
Novel Therapies in Primary Central Nervous System Lymphoma
Authors Wakim M ![]() , Mezher M, Perez-Perez A, Maharaj A, Odia Y
, Mezher M, Perez-Perez A, Maharaj A, Odia Y ![]() , Ahluwalia MS, Linhares Y
, Ahluwalia MS, Linhares Y ![]()
Received 19 October 2024
Accepted for publication 17 May 2025
Published 28 May 2025 Volume 2025:17 Pages 97—117
DOI https://doi.org/10.2147/CPAA.S501065
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Arthur E. Frankel
Michel Wakim,1,* Mariana Mezher,2,* Ariel Perez-Perez,3 Arun Maharaj,3 Yazmin Odia,3 Manmeet S Ahluwalia,1,3 Yuliya Linhares1,3
1Herbert Wertheim College of Medicine, Florida International University, Miami, FL, USA; 2Faculty of Medical Sciences, Lebanese University, Beirut, Lebanon; 3Miami Cancer Institute, Baptist Health South Florida, Miami, FL, USA
*These authors contributed equally to this work
Correspondence: Yuliya Linhares, Translational Medicine, Florida International University, Chief of Lymphoma Services, Miami Cancer Institute, 8900 N Kendall Dr, Miami, FL, 33176, USA, Tel +1-310-795-6849, Email [email protected]
Abstract: Primary central nervous system lymphoma (PCNSL) is a rare, aggressive, extranodal lymphoma exclusively located in the central nervous system. High-dose methotrexate (HD-MTX)-based chemotherapy combination regimens are now the standard of care for the upfront treatment of PCNSL and are used in a salvage setting but are toxic and cumbersome to administer because of the need for inpatient supportive care. While the incidence of PCNSL is increasing in the aging population, a significant proportion of patients are unable to follow HD-MTX protocols owing to performance status and organ dysfunction. Consolidative autologous stem cell transplant or whole-brain radiation therapy improves progression-free survival at the cost of short- and long-term toxicities. Induction of low toxicity and consolidative and salvage therapeutic options are lacking. Due to its unique biology, PCNSL presents an exciting opportunity for the development of novel therapies with improved efficacy and toxicity. In this review, we focus on the biology of PCNSL and novel chemotherapeutics, including targeted and immunotherapeutic agents as well as cellular therapies. Expert Opinion summary: Given the lack of low-toxicity standard treatments for PCNSL, the outcomes for aging PCNSL patients remain suboptimal. Current research has focused on introducing targeted immunotherapies into the induction, salvage, and consolidation treatments of PCNSL.
Keywords: primary central nervous system lymphoma (PCNSL), high-dose methotrexate (HD-MTX) in PCNSL, targeted therapy in PCNSL, immunotherapy in PCNSL, Bruton tyrosine kinase (BTK) signaling pathway in PCNSL, chimeric antigen receptor T cells (CARTs) in PCNSL
Introduction
Primary central nervous system lymphoma (PCNSL) is an aggressive extranodal lymphoma that exclusively originates in the central nervous system (CNS), leptomeningeal compartment, or eyes. It constitutes approximately 2% of all primary brain tumors and less than 1% of non-Hodgkin’s lymphoma (NHL).1 PCNSL is more prevalent in immunocompromised patients such as patients affected by HIV/AIDS and those on immunosuppressive therapies.2 About 90% of PCNSLs are diffuse large B cell lymphomas (DLBCLs) and express B cell markers including CD20, CD19, CD79a, and immunoglobulin light chains.3
The annual incidence of PCNSL is 0.3 to 0.6 cases per 100,000 persons and has been increasing worldwide. For example, the incidence of PCNSL in the United States (US) increased 5 times from 1975 to 2017.1,4 The incidence of PCNSL increases with age and has been rising in patients over 70 years old (yo).5
Traditionally, PCNSL has been treated with HD-MTX-based regimens, owing to its excellent CNS penetration. Single agent HD-MTX produces 30–52% complete remission (CR) rate with overall survival (OS) and progression-free survival (PFS) less than one year in patients who do not achieve CR.6–8 HD-MTX administration is cumbersome requiring hospitalization for high volume hydration, leucovorin rescue administration, and monitoring of MTX levels. HD-MTX has the potential to cause significant renal, liver, and lung toxicities. Approximately 36% of patients treated with HD-MTX based therapy relapse after achieving CR. Patients with relapsed or refractory disease respond poorly to currently available chemotherapy regimens with survival ranging between 0.5 to 40.5 months.9 Combining HD-MTX based therapy with a monoclonal anti-CD 20 antibody rituximab improved outcomes in some studies but did not yield a significant benefit in others.8,10,11
HD-MTX in combination with alkylators, as well as other chemotherapeutic agents, has demonstrated a PFS advantage over HD-MTX alone, making combination regimens the standard of care for newly diagnosed PCNSL. The choice of the multiagent HD-MTX-based alkylator-containing induction regimen is institution-dependent, with the historical preference of Rituximab-Methotrexate-Procarbazine-Vincristine (R-MPV) and Methotrexate-Rituximab-Temozolomide in the US, and Methotrexate-Cytarabine-Temozolomide-Rituximab (MATRix) in Europe.12–14 Despite the increased toxicity of combination regimens, CR rates are still mostly disappointing (Table 1).11–13,15–18
 |
Table 1 High Dose Methotrexate-Based Regimens for PCNSL |
Without consolidation, only patients who achieve CR can have prolonged PFS.8 Post- HD-MTX induction consolidation therapies, such as whole brain radiation therapy (WBRT) and autologous stem cell transplantation (ASCT), have been investigated to increase remission durability. However, both offer efficacy at the expense of significant toxicity. At 2 years, PFS was 63% with WBRT and 87% with ASCT consolidative approach. WBRT negatively affects cognitive function, whereas ASCT puts patients at risk of hematologic toxicities, infections, and transplant-related mortality.15,21,22 Illerhaus et al recently reported the results of a randomized controlled trial comparing post-induction R-DeVIC (rituximab, dexamethasone, etoposide, ifosfamide, carboplatin) chemotherapy consolidation with high-dose thiotepa-based conditioning, followed by ASCT. At a median follow-up of 45.3 months there was a significant PFS difference in favor of ASCT, with 79% of transplanted patients and 52% of chemotherapy consolidated patients being progression-free at 3 years post-randomization (p= 0.0001, HR 0.396), solidifying consolidative ASCT as a standard of care for newly diagnosed PCNSL patients who otherwise meet transplant organ function and performance status criteria. Additionally, the long-term follow up of newly diagnosed immunocompetent patients with PCNSL treated with R-MPV followed by thiotepa-busulfan-cyclophosphamide (TBC) conditioning and ASCT in responders demonstrated excellent efficacy with 5-, 10-, and 15-year PFS and OS of 80.8% in 26 transplanted patients.23 In a recent Memorial Sloan Kettering Cancer Center retrospective analysis, in patients with complete response to consolidation, only R-MPV induction was associated with improved PFS, as compared to MPV or other regimens (Table 1). 20,24
Despite the introduction of rituximab to the front-line regimens, the use of multiagent induction chemotherapy, and the adoption of ASCT as the front-line consolidative standard of care, PCNSL prognosis continues to lag behind that of DLBCL, with a median PFS of 10.2 months median OS of 25.3 months, and median OS of relapsed patients as low as 6.1 months according to a recent report of the French oculo-cerebral lymphoma network.25
A Memorial Sloan Kettering Cancer Center PCNSL survival analysis included data from 1973 to 2013 and demonstrated that the median OS of PCNSL patients doubled from 12.5 months in the 1970s to 26 months in 2010, while the survival of patients ≥ 70 yo was unchanged (6 months in the 1970s vs 7 months in the 2010s). Survival improvement in younger patients was likely due to the introduction of HD-MTX followed by consolidation including ASCT as a standard of care for fit patients.26,27 Lack of improvement in survival of older patients pointed out the need for the development of novel treatment regimens for those who are not candidates for the intensive therapy.28 Most of the studies on novel therapeutics in PCNSL date from the end of 2010s to 2020s (see reference list). Unfortunately, there is no PCNSL survival statistics available for this time period. We are hopeful that the incorporation of novel therapeutics into PCNSL regimens improves patient survival, especially the survival of those with R/R disease and those who are not candidates for HD-MTX based induction and ASCT consolidation.
In recent years, the treatment of systemic DLBCL has been revolutionized with novel therapies, including antibodies (tafasitamab), bispecific T cell engagers (mosenutizumab), antibody-drug conjugates (loncastuximab), and chimeric antigen receptor T cells (CARTs); however, progress in PCNSL has been lagging behind.29–32 Most of the novel DLBCL therapies lack sufficient CNS penetration to be effective in PCNSL. Patients with secondary CNS lymphoma (SCNSL) involvement, from whom insights into therapeutic efficacy and safety in the CNS can be gained, are frequently excluded from clinical trials because of their potential for rapid clinical deterioration. Additionally, PCNSL is a rare disease, and many excellent PCNSL clinical trials have been closed early owing to poor accrual.
PCNSL presents an exciting opportunity for the development of novel therapies owing to its unique biology and the need for effective blood–brain barrier (BBB) penetration. The key targetable features of PCNSL biology are mutations in B cell receptor (BCR) or toll-like receptor (TLR) pathways which lead to nuclear factor kappa B (NF-κB) activation, which subsequently prevents terminal B cell differentiation and apoptosis and facilitates immune escape. Additionally, PCNSL has unique tumor microenvironment and is characterized by immune evasion.33,34
Additionally, the existing standard treatments are of suboptimal efficacy, cumbersome to administer, and toxic, creating the need for convenient treatments with lower toxicity and higher efficacy. Therefore, effective, and tolerable salvage regimens are needed. Elderly patients and those with compromised organ function are frequently not candidates for HD-MTX-based regimens or are unable to complete enough cycles due to toxicities. Additionally, these patients are frequently not candidates for consolidative ASCT. Regimens with lower toxicity and higher efficacy are urgently required in vulnerable populations.
Substantial efforts have been made to understand the molecular mechanisms underlying PCNSL, generating interest in the use of targeted therapies for upfront and RR-PCNSL treatment. In this review, we focus on PCNSL biology as related to the discussed therapies and the newly studied agents in ongoing and completed clinical trials, ranging from chemotherapeutic drugs to targeted therapies.
Novel Therapies for PCNSL
Pemetrexed
Pemetrexed is a novel antifolate chemotherapeutic that is approved by the Food and Drug Administration (FDA) for use in mesothelioma and recurrent non-small cell lung cancer (Pemetrexed package insert). It targets more than one site in folate metabolism by interrupting purine synthesis via thymidylate synthase and dihydrofolate reductase inhibition and pyrimidine synthesis via glycinamide ribonucleotide formyltransferase and aminoimidazole carboxamide formyltransferase inhibition.35 Pemetrexed has the same ability to penetrate the CNS as methotrexate but is less toxic and does not require hospital admission for supportive care. Unfortunately, pemetrexed is rarely used by oncologists in PCNSL settings despite its known activity and inclusion in the NCCN guidelines for relapsed or refractory diseases (NCCN guidelines). Dexamethasone before and after pemetrexed administration, as well as folic acid and cyanocobalamin maintenance therapy, are obligatory for the prevention of pemetrexed toxicity (Pemetrexed package insert). Pemetrexed activity has been reported in multiple clinical trials in both treatment-naïve and RR-PCNSL patients, including those with PCNSL refractory to HD-MTX.
Twelve treatment-naïve PCNSL patients over 65 yo were treated with pemetrexed, with 10 responding and four achieving CR. The median OS was 19.5 months, and the estimated 1-year and 2-year survival rates were 66.7% and 41.7%, respectively. No neurotoxicity or treatment-related death was observed. Side effects were mild and included leukocytopenia, anemia, fatigue, rash, and vomiting. The results of this trial are promising for the elderly population because minimizing toxicity is particularly challenging in this age group and, suboptimal therapy remains a problem.36
In a Phase I pemetrexed trial for the treatment of RR PCNSL, 14 patients were evaluated for their response. ORR was 57.1%, and the disease control rate (DCR), including CR + PR+ SD was 71.4%. The 6-month PFS and 12-month PFS were 35.7% and 21.4%, respectively, with a median PFS of 4.2 months and median OS of 44.5 months. The estimated 1-year, 2-year, and 5-year survival rates were 78.6%, 64.3%, and 35.7%, respectively. A maximum tolerated dose (MTD) of 900 mg/m2 was administered every two weeks. The main adverse observed were fatigue and cytopenia.37
Another prospective trial evaluated pemetrexed 900 mg/m2 every three weeks in RR PCNSL. Eleven patients with a median age of 69.8 yo and an average KPS of 70% (10–100%) were treated; 10 had failed prior HD-MTX. CR rate, ORR, and DCR were 36%, 55%, and 91%, respectively. The 6-month PFS was 45%, median PFS was 5.7 months, and median OS was 10.1 months. Importantly, responses occurred in patients in whom HD-MTX failed, suggesting that methotrexate exposure does not preclude a response from pemetrexed. In addition, responses were observed in patients who failed multiple prior treatments, including ASCT. Overall, the treatment was well-tolerated, with the most common adverse events (AEs) being hematologic events.14
Zhang et al retrospectively analyzed the outcomes of pemetrexed salvage at 900 mg/m2 every 3 weeks in 18 patients with RR-PCNSL and 12 patients with SCNSL. For PCNSL and SCNSL, ORR, CR rate and median PFS were 64.7%, 64.7%, 5.8 months and 58.3%, 16.6% and 2.5 months respectively. Grade ≥3 AEs included leukopenia 16.7%), neutropenia 3.3%), and fatigue in 10.0%). Pemetrexed was well tolerated and showed activity in RR-PCNSL, although responses were not durable, with less favorable results in SCNSL.38
Twenty-seven HD-MTX HD-MTX-resistant PCNSL were treated with pemetrexed in combination with rituximab. CR, PR, and SD rates were 22.2%, 40.7%, and 29.6%, respectively, with an ORR of 62.9% and DCR of 92.5%. PFS was 6.9 months, and the median OS was 11.2 months.39
Pemetrexed in combination with lenalidomide was studied in patients with RR PCNSL in whom two or more therapeutic regimens failed. Thirty-eight patients were treated with an ORR of 68.4% and median PFS and OS of 6 and 18 months.40
In summary, pemetrexed is active in RR PCNSL, including HD MTX failures, with CR reported from 22.2 to 64.7% and ORR 55–64.7%. In contrast to HD-MTX, pemetrexed is administered in the outpatient setting and has an excellent toxicity profile with no neurotoxicity, treatment-related deaths, or non-hematologic toxicity over grade 4 observed in most studies. Pemetrexed is an excellent candidate as an antifolate backbone in combination with targeted and immunomodulatory therapies and is now used in multiple PCNSL clinical trials (Table 2).
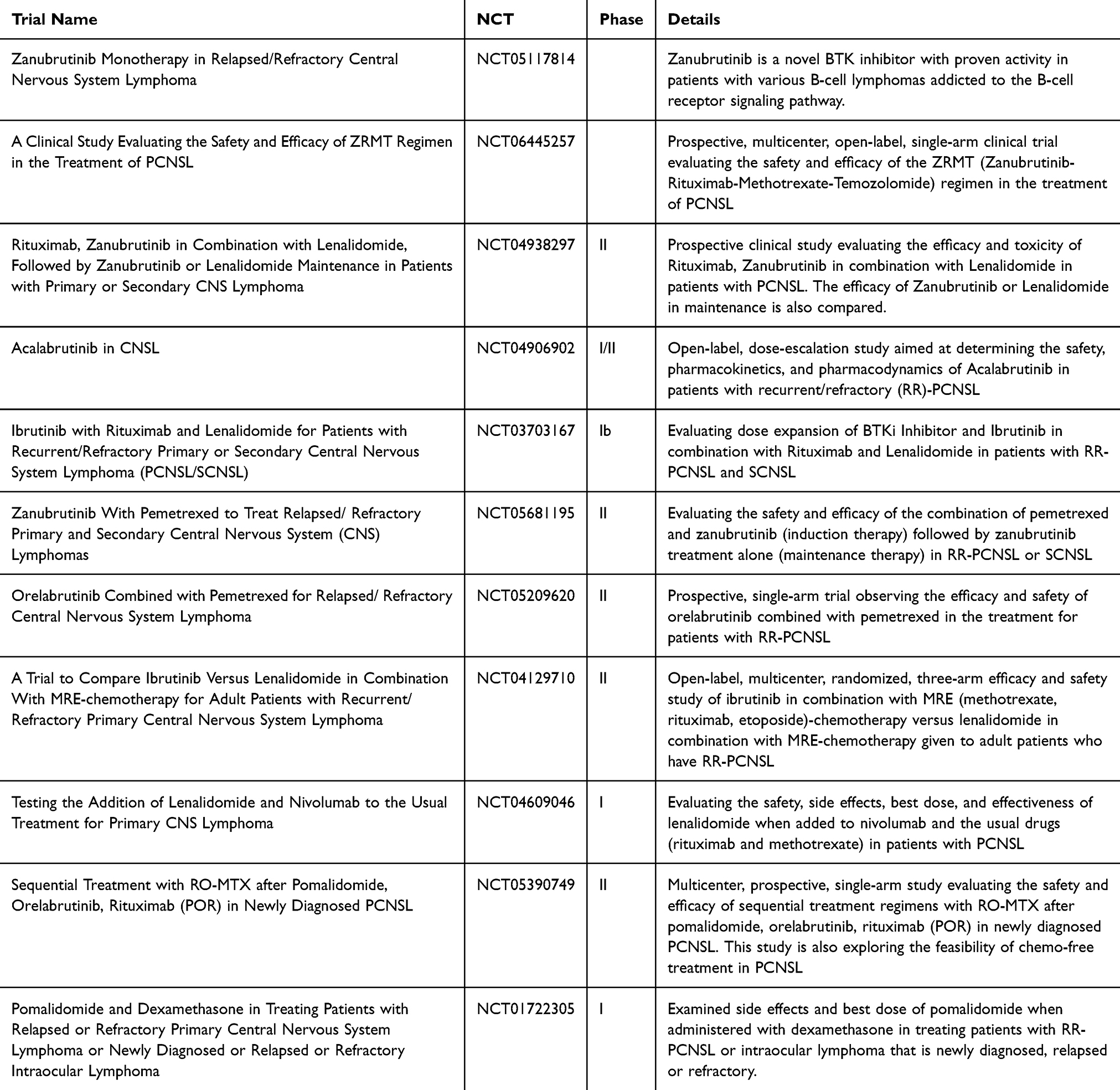 |
Table 2 Novel Therapy Trials for PCNSL |
Rituximab
Rituximab is a chimeric monoclonal antibody that targets CD20 cell surface proteins. When combined with CHOP (cyclophosphamide, doxorubicin, oncovin, and prednisone), it increased DLBCL EFS and OS by 15–20% becoming a standard of care.41 PCNSLs express CD20 in over 90% of cases, making rituximab an attractive therapeutic choice in PCNSL.34 Rituximab is a large 145 kD molecule with poor BBB penetration. At 375 mg/m2 IV, rituximab CSF concentrations were 0.1% of plasma.42 Homogeneous enhancement with gadolinium suggests that the BBB is disrupted in PCNSL. In patients with active leptomeningeal disease, the CSF concentration of rituximab is 3–4% of the serum concentration, suggesting that BBB disruption allows for rituximab penetration and prompts further studies on rituximab in PCNSL.43
The randomized Phase 2 IELSG32 (MATRix) trial confirmed the benefit of rituximab in upfront PCNSL regimens. Patients were randomized to receive HD-MTX-cytarabine with or without rituximab, in addition to rituximab-HD-MTX-cytarabine and thiotepa (MATRix). MATRix arm performed best with 49% of patients achieving CR, while CR rate was numerically higher in patients treated with rituximab-HD-MTX-cytarabine versus HD-MTX-cytarabine without rituximab (23 vs 30%).19 Interestingly, on 7-year follow-up, HD-MTX-cytarabine-rituximab arm demonstrated overall survival advantage over HD-MTX-cytarabine arm with 7-year OS at 37% and 21% accordingly, HR 0.64 (p=0.04).44 Rituximab is now included in most used first line regimens such as R-MPV, MRT, and MATRix with excellent ORRs at 77%, 97%, and 87%, respectively.12,18,19
Some experts still consider the role of rituximab to be controversial, as no studies have demonstrated its PFS or OS advantages. In a retrospective registry study, there was an increase in ORR in patients receiving R-MPV versus MPV (77 vs 53%; p = 0.03), but there was no difference in PFS or OS. This could be because the patients were older (median age, 68 yo), had poor KPS at 60%, and received three cycles of high-dose cytarabine consolidation, which led to increased hematologic toxicity.45
Despite some studies demonstrating the safety and activity of intraventricular rituximab within the leptomeninges, intraocular compartments, and small parenchymal lesions, its use remains under investigation.46
Bruton Kinase Inhibitors
DLBCL is classified into three subtypes based on gene expression profile: (i) germinal center B-cell-like (GCB), (ii) activated B-cell-like (ABC), and (iii) type 3.47 ABC-DLBCLs have a higher frequency of concomitant or isolated myeloid differentiation primary response gene MYD88L265P and CD79B mutations as well as BCL6 fusions and NOTCH1 and NOTCH2 mutations and carry worse prognosis.48 CD79B and MYD88 double mutant DLBCL is further classified as MCD DLBCL, is almost universally of the ABC subtype, carries inferior prognosis, and is enriched in lymphomas with extranodal involvement, including breast, testes, and nervous system.48,49 Both CD79B and MYD88 signaling leads to NF-kB pathway activation. Over 85% of PCNSL originate from ABC origin. 96% of PCNSL have mutations in the NF-κB gene network, with the CD79B (83%) and MYD88 (76%) mutants being most common, and 67% are reported to be double mutant MCD DLBCL.50,51
Upon Toll-like and interleukin receptor stimulation, the MYD88 adaptor protein activates JAK/STAT3 signaling and NF-kB, whereas MYD88L265P mutant constitutively activates the NF-κB signaling pathway, promoting B-cell survival and growth.52
Interplay of the BCR-CD79B pathway and MYD88 signaling is crucial for understanding the therapeutic targeting of the NF-kB pathway via Bruton Tyrosine Kinase (BTK) inhibition (Figure 1). BCR stimulation activates BTK via CD79A and CD79B heterodimers. Activated BTK preferentially forms a complex with MYD88L265P mutant, signaling to CARD11 and subsequently activating the NF-κB pathway. BTK inhibition resulted in decreased formation of the MYD88-BTK complex with CD79B and MYD88 double mutants, benefitting the most from BTK inhibition. Recently, the MYD88-TLR9-BCR (My-T-BCR) supercomplex was identified in ABC-DLBCL, PCNSL, and Waldenstrom’s macroglobulinemia (WM). My-T-BCR promotes lymphomagenesis by activating the mammalian target of rapamycin (mTOR) and NF-κB pathways and correlates with responsiveness to BTK inhibition. My-T-BCR is a novel therapeutic target and could be used as a biomarker for predicting the efficacy of BTKis as well as a classifier of B-NHL.53,54
 |
Figure 1 Targeting NF-κB Signaling Network in Primary CNS Lymphoma. Most PCNSLs harbor mutations in NF-κB signaling network leading to its aberrant activation. CD79B, which is a part of the BCR complex, and MYD88, an adaptor protein downstream of Toll-like receptor, are most frequently mutated. BCR and TLR signaling is transmitted by BTK. Activated BTK preferentially forms complex with MYD88L265P mutant, signaling to CARD11 and activating NF-κB pathway. Additionally, CARD11 gain-of-function mutations can lead to constitutive NF-κB activation. BTK is a therapeutic target in PCNSL which is inhibited by small molecule BTK inhibitors. Syk kinase is one of the kinases that activates BTK upon BCR activation and is a therapeutic target in PCNSL. TLR activation leads to the formation of myddosome complex which incorporates several proteins including IRAK4, which is inhibited by small molecule emavusertib (CA4948). Upon BCR activation, BTK contributes to the activation of PI3K-mTOR signaling pathways which is targeted by buparlisib and temsirolimus respectively. TNFAIP3 is a tumor suppressor gene that can be mutated or inactivated in PCNSL leading to increased NF-κB activity. IMiDs inhibit NF-κB by promoting the degradation of key transcription factors and directly suppressing NF-κB activation. Original Figure: Mendez JS, Grommes C. Treatment of primary central nervous system lymphoma: from chemotherapy to small molecules. Am Soc Clin Oncol Educ Book. 2018;38:604–615. DOI: 10.1200/EDBK_200829. Created in BioRender. (2025) https://BioRender.com/apoqnuq. Abbreviations: TLR, toll-like receptor; BCR, B cell receptor; CD79B, immunoglobulin-associated beta; Y196, tyrosine residue at gene position 196; MYD88, myeloid differentiation primary response 88. L265P, amino acid substitution leucine to proline at position 265 in the MYD88 Toll/interleukin-1 receptor (TIR) domain; SYK, spleen tyrosine kinase; IRAK, interleukin 1 receptor associated kinase 1; CA4948, kinase inhibitor; BTK, Bruton tyrosine kinase; PIP3, Phosphatidylinositol (3,4,5)-trisphosphate; PTEN, phosphatase and tensin homolog deleted on chromosome-10; PI3K, phosphatidylinositol 3-kinase; CARD11, Caspase recruitment domain family, member 11; BCL-10, B-cell lymphoma/leukemia 10; MALT1, mucosa-associated lymphoid tissue lymphoma translocation gene 1; TNFAIP3, tumor necrosis factor alpha-induced protein 3; IMiDs, immunomodulatory drugs; NFκB, nuclear factor kappa-light-chain-enhancer of activated B cells. |
Systemic ABC-DLBCL lymphomas with MYD88L265P mutation are more prone to CNS relapse, with 53% of patients with the mutation relapsing in CNS at five years and almost 100% of wild type (WT) patients living CNS relapse-free, suggesting that the MYD88 L265P mutation plays a critical role in the ability of DLBCL cells to invade CNS. Given the interplay of the BCR, BTK, and MYD88 signaling, BTKis are being actively investigated in the treatment of B-NHLs, demonstrating higher responses in MYD88 L265P mutant tumors.52,55 PCNSL is enriched in MYD88 mutations, with various studies showing an average 60.8% (33–100%) of PCNSL carrying MYD88 L265P mutation, making BTK inhibition an attractive therapeutic opportunity in PCNSL.54
First Generation Bruton Kinase Inhibitors
Ibrutinib is the first oral small-molecule covalent irreversible BTKi inhibitor. Ibrutinib binds covalently to the cysteine residue C481 at the BTK active site, leading to irreversible BTK inhibition and blockage of NF-kB activation, thus having a particularly significant activity in RR ABC-DLBCL with both CD79B and MYD88 L265P mutations.56 Mouse studies have demonstrated that ibrutinib rapidly penetrates the BBB with a brain-to-plasma ratio of 0.7.57 Ibrutinib was studied alone and in combination for the treatment of RR-PCNSL with multiple trials currently ongoing.
Ibrutinib was safe and effective in a phase I/II dose escalation study of patients with RR-PCNSL. The MTD was 840 mg/day. A clinical response was noted in 10 of the 13 patients including five CRs and five PRs, yielding a median PFS of 4.6 months. One non-responder had a missense mutation within the coiled-coil domain of CARD11, which promotes BTK-independent activation of NF-κB, and incomplete responders had a CARD11 (R337Q) mutation or inactivating lesions in TNFAIP3, a negative regulator of NF-κB.58,59
In a Phase II study of 560 mg daily ibrutinib in RR-PCNSL and ocular lymphoma patients, disease control was 70% in 44 evaluable patients, including 10 CRs, 17 PRs, and five stable diseases (SD). With a median follow-up of 25.7 months, the median PFS and OS were 4.8 months and 19.2 months, respectively. Thirteen patients received ibrutinib treatment for more than 12 months. Two patients developed pulmonary aspergillosis (PA). The clinical response to ibrutinib appears to be independent of gene mutations in the BCR pathway. Responses were observed in all compartments of the CNS with an ibrutinib concentration in the CSF above the efficacy threshold level at a steady state.60
In summary, PCNSL demonstrated a much higher response to ibrutinib than systemic DLBCL, where the pooled OR and CR to ibrutinib monotherapy were 41.6% and 15.2%.61 CARD11 coiled-coiled domain R179Q mutation facilitated complete resistance to ibrutinib, while CD79B mutations were associated with partial ibrutinib resistance. This is consistent with the observation that ibrutinib-resistant ABC-DLBCs upregulate the expression of CD79B. CD79B mutations are frequently associated with MYD88 mutations in PCNSL and attenuate BTK “addiction” by providing a redundant survival signal that is independent of NF-κB via the upregulation of phosphoinositide 3-kinase (PI3K)/mTOR signaling. In vitro, mTOR or PI3k inhibition is synergistic with ibrutinib and leads to cell death in CD79B mutant PCNSL.58 It is crucial to overcome BTKi resistance in upfront combination regimens to improve the outcomes, which can be achieved by combining BTKis with other chemotherapeutic agents or targeted therapies such as PI3K inhibitors. There are multiple ongoing RR-PCNSL clinical trials of ibrutinib in combination with other agents including checkpoint inhibitors (CPIs) and immunomodulators. Alternatively, next-generation non-covalent BTK inhibitors, such as pirtobrutinib, offer increased efficacy and reduced toxicity in the setting of B-cell malignancies and warrant exploration in CNSL settings.
Lionakis et al performed a proof-of-concept phase Ib study of ibrutinib monotherapy followed by ibrutinib plus temozolomide, etoposide, liposomal doxorubicin, dexamethasone, and rituximab chemotherapy (DA-TEDDi-R) combined with intraventricular cytarabine in patients with RR and newly diagnosed PCNSL. Eighteen patients were treated with ibrutinib, and 16 underwent TEDDi-R. Ibrutinib monotherapy showed clinical activity in 94% of patients, with 83% of patients reaching PRs. DA-TEDDi-R subsequently produced CRs in 86% of patients, which included eight patients who were free of disease at a median of 15.5 (range, 8–27) months follow-up. Ibrutinib had significant CSF penetration with CSF/plasma ratio of 28.7%, while liposomal doxorubicin CSF penetration was low but unexpectedly had measurable concentrations during the entire treatment cycle, suggesting a depot effect in the CNS. Two patients developed invasive aspergillosis during ibrutinib monotherapy, and an additional 5 patients developed aspergillosis on TEDDi-R. One case of Pneumocystis jiroveci pneumonia was reported. The high incidence of aspergillosis during this trial was attributable to ibrutinib since ibrutinib monotherapy was administered. Further studies demonstrated that Btk-/- mice have a higher mortality from pulmonary aspergillosis, demonstrating a role for BTK in innate fungal immune surveillance, suggesting that inhibition of BTK by ibrutinib contributed to the high incidence of aspergillosis, perhaps in concert with glucocorticoids.56 Those results prompted further consideration for fungal prophylaxis in future ibrutinib studies. A phase II study of 2 weeks of ibrutinib treatment for two weeks followed by TEDDi-R in ibrutinib responders and TEDD-R in ibrutinib-refractory patients was conducted using universal isavuconazole fungal prophylaxis. Patients with untreated or RR-LBCL with CNS with or without systemic involvement were included. 57% of patients were ibrutinib-responsive. ORR for TEDDi-R were 92%, CR 77%, TEDD-R ORR was 45%, and 28%. One-year PFS and OS were significantly higher in ibrutinib-responsive versus ibrutinib-resistant tumors at 54.7% versus 17.6% (p < 0.002) and 76.7% versus 47.1% (p = 0.08), respectively. 88% of ibrutinib-responsive tumors were CD10 negative and had TEDDi-R ORR of 83%, with 70% CR rate. There were no opportunistic infections.62
In a Phase 1 B trial, Grommes et al combined ibrutinib with HD-MTX and rituximab in CNSL patients. Ibrutinib was continued after the completion of induction therapy until disease progression, intolerable toxicity, or death. The combination was well tolerated, and no dose-limiting toxicity was observed. Twelve of the 15 patients responded with sustained tumor responses associated with the clearance of circulating tumor DNA from the cerebrospinal fluid (CSF).63
To develop a less toxic salvage regimen, temozolomide and ibrutinib have been combined by French investigators. In 13 RR PCNSL and nine SCNSL patients, the best ORR was 55%, including three CRs. With a median follow-up of 18.2 months, the median PFS was 5.3 and the OS 8.9 months. Four patients experienced serious infectious complications, but none developed aspergillosis.64
Ibrutinib alone or in combination with rituximab, with or without HD-MTX, is now included in the NCCN guidelines for the treatment of RR-PCNSL, which constitutes a huge step forward in the utilization of targeted therapies for PCNSL (NCCN).
Given the toxicity, suboptimal complete response rate, and high rate of relapse without consolidation with high HD-MTX-containing induction regimens, the introduction of BTKi into front-line regimens may be of value.
In a phase 1 trial, 16 patients, newly diagnosed with PCNSL, were treated daily with 560mg ibrutinib combined with MTX 3.5 g/m2 and rituximab (375 mg/m2 I-MR). After four cycles, the responders underwent ASCT followed by ibrutinib or lenalidomide maintenance. ORR to induction was 94%, with 50% of patients achieving CR. Five patients proceeded to HSCT. At a median follow-up of 24.5 months, median PFS and OS were not achieved, and the estimated 3-year OS and PFS were 88.9% and 86.5%. No grade 4 AEs were observed. I-MR appeared to be safe and effective and resulted in excellent 3-year PFS with only 30% of patients undergoing ASCT, warranting further investigation in a front-line setting.65
In a phase II trial, ibrutinib (560 mg/day) was combined with MTX 3.5 g/m2 and temozolomide 150 mg/m2 d1-d5 (MIT) every three weeks. Patients <65 yo proceed to ASCT. Ibrutinib maintenance lasted for up to 2 years. The ORR was 92.9%, and the CR rate was 67.9%. Undetectable ctDNA in CSF/plasma samples was associated with CR. After a median follow-up of 7 months, the 1-year PFS and OS were 88.9% and 100%. Given its excellent preliminary safety and efficacy, this regimen requires further investigation in larger trials.66
Owing to off-target kinase inhibition, ibrutinib has multiple side effects, including arrhythmias and bleeding. The development of drug resistance is common and is facilitated by the C481S mutation in BTK, which hampers the interaction between ibrutinib and BTK, as well as by mutations in PLCg2, CARD11, and CXCR4. Next-generation BTK inhibitors are being developed to overcome these limitations.57
Second Generation Bruton Kinase Inhibitors
As a first-generation BTKi, ibrutinib binds covalently to BTK and other kinases, including members of the TEC kinase family, such as ITK, EGFR, JAK3, and HER2, leading to off-target toxicities. More selective second-generation BTK inhibitors, including zanubrutinib, acalabrutinib, and tirabrutinib, were developed to ameliorate off-target effects.57 These molecules form an irreversible covalent bond with BTK Cys-481 with high selectivity and exhibit minimal inhibition of TEC, EGFR, and Src family kinases.67
Zanubrutinib is a small, potent second-generation BTKi with a highly selective target-binding profile.68 In a Phase III trial of zanubrutinib versus ibrutinib for CLL/SLL, patients treated with zanubrutinib had significantly lower rates of atrial fibrillation (2.5% vs 10.1%) and overall lower rates of cardiac events, major hemorrhages, and AEs leading to treatment discontinuation or death.69 Zanubrutinib is FDA approved for treatment of multiple B cell malignancies including CLL, marginal zone lymphoma (MZL), WM, and follicular lymphoma (label (fda.gov)). Zanubrutinib proved to be effective in both mutant and WT MYD88 WM. MYD88 WT WM patients responded poorly to ibrutinib, with none of the MYD88 WT patients treated with ibrutinib in a phase II trial. Twenty-six MYD88WT WM patients and two with unknown or inconclusive MYD88 mutational status were assigned to receive zanubrutinib in the ALPINE trial sub-study. Zanubrutinib induced VGPR in 27%, major response in 50%, and ORR in 81% of these patients.70–72 Genetic similarity between WM and PCNSL and its activity in both MYD88 mutant and MYD 88WT WM prompted further investigation of zanubrutinib for the treatment of PCNSL.
The first study to demonstrate the effectiveness of zanubrutinib-containing regimens in different DLBCL subtypes, particularly those with CNS involvement, was Zhang’s retrospective case series of 13 patients. Eight patients had ocular lymphoma with brain involvement in 4/8 cases, 2/5 patients with systemic DLBCL had brain involvement, and 8/13 patients had an RR disease. Four regimens combining 160mg zanubrutinib with other chemotherapeutic agents were evaluated in this study, demonstrating tolerability and efficacy. Eleven patients responded, and ten achieved CR; the DOR was 12 (9–14) months. Zanubrutinib had an excellent BBB penetration with the mean peak concentration in CSF at 2941.1 pg/mL and the corrected mean CSF/plasma ratio based on 94% protein binding at 42.7% ± 27.7%.73
Thus, zanubrutinib may have activity against HD-MTX-resistant PCNSL. Cheng et al reported a case of a patient with PCNSL whose disease progressed after two cycles of lenalidomide HD-MTX-rituximab. The patient was subsequently treated with zanubrutinib combined with HD-MTX- rituximab and achieved remission after 3 cycles.74 In another case series, 3 patients with ocular PCNSL relapses, two of whom were first treated with HD-MTX based therapy, achieved CR with zanubrutinib.75
Zanubrutinib has an improved safety profile compared to ibrutinib, excellent BBB penetration, and can be safely combined with cytotoxics. Given its preliminary activity in PCNSL and CNSL with ocular involvement, we designed a clinical trial that combined pemetrexed with zanubrutinib to treat patients with RR-PCNSL and SCNSL (Table 2). Further studies on zanubrutinib activity in B-cell lymphomas with CNS involvement are ongoing (Table 2).
Tirabrutinib was approved for the treatment of RR-PCNSL in Japan in March 2020. In a phase I/II trial, tirarutinib was administered to 44 patients with RR PCNSL at escalating doses up to 480 mg po daily. No DLTs were observed. A grade 5 AE (pneumocystis pneumonia) was observed in one patient, and the MTD was not reached at 480 mg. ORR was 64%, and all 4 patients achieved CR/CRu at 480 mg. The median PFS was 11.1 at 480 mg. Median OS was not achieved. The ORR was similar among patients harboring CARD11, MYD88, and CD79B mutations and the corresponding wild types.76 Ibrutinib is currently being studied as a single agent for RR PCNSL and in combination with HD-MTX-based regimens for newly diagnosed PCNSL in a PROSPECT trial (NCT04947319).
Currently, there is no published data available on acalabrutinib BBB penetration and activity of acalabrutinib in CNS lymphoma. Several ongoing clinical trials have explored the activity of acalabrutinib in PCNSL and B cell lymphomas with CNS involvement (Table 2).
Orelabrutinib, a novel second-generation BTKi approved in China for the treatment of RR lymphoma, demonstrated good CNS penetration and activity in PCNSL both alone and in combination.77,78
A novel highly selective BTKi JDB175 has shown high brain penetration (%, Cbrain/Cplasma) rate at 49.2%, which is much higher than that of orelabrutinib, zanubrutinib, tirabrutinib, and ibrutinib. It has demonstrated activity against lymphoma cell lines in vitro and was active in a mouse model of CNS lymphoma without excess toxicity. Thus, JDB175 is a promising candidate for human PCNSL trials.79
PI3K/mTOR Inhibitors
mTOR is a serine-threonine protein kinase that is part of the PI3K–related kinase family.80 The PI3K/AKT/mTOR signaling pathway presents an excellent therapeutic target as it controls growth, proliferation, differentiation, apoptosis, and metabolism and plays an important role in the development of malignancies, including lymphomas. Thus, PI3K/mTOR upregulation may be associated with poor prognosis in PCNSL.81
CD79 mutations are associated with incomplete PCNSL tumor responses. CD79B mutants showed increased expression of mTOR-related genes and PI3K/mTOR activation markers. Treatment of these tumors with a PI3K inhibitor resulted in cell death, indicating that the PI3K–mTOR signaling axis is constitutively activated and promotes survival in CD79B-mutant PCNSL. Robust CD79B mutant death occurs not with PI3K selective inhibitors but with inhibition of both p110a and p110d isoforms, indicating that both isoforms provide redundant survival signals in CD79B mutant PCNSL cells. The mTOR inhibitor INK128 combined with ibrutinib synergistically induced cell death associated with mTOR inhibition but not NF-κB inhibition, suggesting that the PI3K–mTOR survival signal is independent of BTK/NF-κB signaling. The combination of BTK and PI3K/mTOR inhibitors may augment BTK inhibitor response in CD79B -mutant human PCNSLs.58
The small-molecule mTOR inhibitor temsirolimus, as well as buparlisib, a pan-PI3K inhibitor, have demonstrated suboptimal clinical activity and poor CNS penetration in CNSL trials.82,83 The buparlisib derivative bimiralisib (PQR309) is an oral, small-molecule inhibitor of both PI3K and mTOR that was designed to overcome the limitations of crossing the BBB.84,85 Bimiralisib’s activity against lymphoma cell lines was observed in combination with multiple other targeted therapies, which prompted the study of its effects on PCNSL. A phase II clinical trial of bimiralisib in 21 patients with RR-PCNSL was completed, and the results have been reported (NCT02669511).
A phase IB/II Study Combining the PI3K inhibitors copanlisib and ibrutinib in patients with RR PCNSL is ongoing (NCT03581942). An update on six patients treated with the combination reported a manageable toxicity profile and ORR of 67% with 1 CR, 3 PR, and 1 SD after a median follow-up of 180 days.86 Further exploration of mTOR inhibition in combination with other therapies in PCNSL is warranted.
Immunomodulatory Drugs
Immunomodulatory drugs (IMiDs) target cereblon, which is the substrate-binding subunit of Cullin-RING E3 ubiquitin ligase 4 (CRL4CRBN) that mediates ubiquitination and proteasomal degradation of target proteins. IMiDs alter the substrate specificity of CRBN, leading to the degradation of proteins responsible for tumor survival. Degradation of the IKAROS transcription factor is promoted, which in turn leads to inhibition of MYC and IRF4 expression and subsequent inhibition of the NF-kB and PI3K/mTOR signaling pathways.87–89 Additionally, IMiDs alter the lymphoma microenvironment and stimulate T and NK cell expansion (Figure 2).90–92 Molecular targeting combined with excellent CNS penetration makes lenalidomide and pomalidomide promising candidates in PCNSL.90
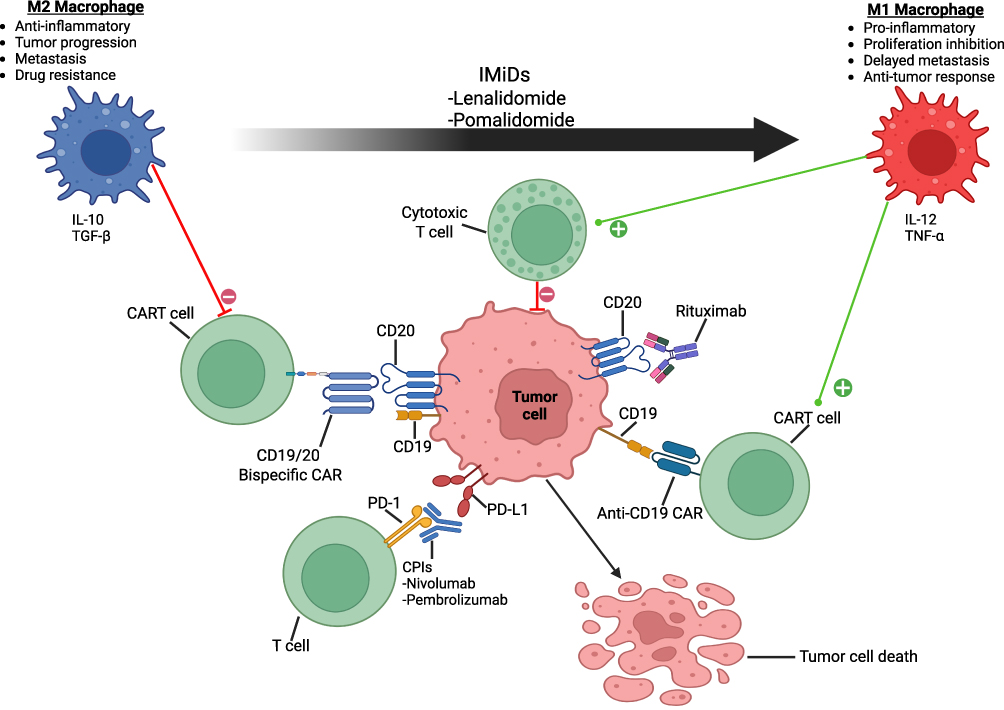 |
Figure 2 Immunotherapies and the Role of Microenvironment in Primary Central Nervous System Lymphoma. The tumor microenvironment in PCNSL is characterized by an interplay of immune cells and stromal cells which influence PCNSL growth and response to therapies. The PCNSL tumor microenvironment is characterized by the infiltration of TAMs and tumor-infiltrating lymphocytes, including cytotoxic T cells, and is considered to be an immunosuppressive environment with a high expression of immune checkpoints such as PD-1 and their ligands. TAMs can be polarized into M1 (anti-tumor) or M2 (pro-tumor) phenotypes. M1 polarized macrophages produces cytokines such as IL-12 and TNF-α, which stimulate CART activity and promote the activation of cytotoxic T cells, enhancing the anti-tumor response. M2 polarized macrophages secrete IL-10 and TGF-β creating an immunosuppressive microenvironment which blunts immune responses, promotes tumor growth, and reduces CART efficacy. Increased ratio of M1/M2-like TAMs has been associated with better PCNSL outcomes. IMiDs stimulate polarization of M2-like macrophages towards M1 phenotype therefore enhancing antitumor immune response. CPIs block immune checkpoints, such as the binding of PD-1 to its ligands, enabling an immune antitumor response. PCNSLs frequently have increased expression of PD-L1 and PD-L2 which contributes to the sensitivity of PCNSLs to CPIs. CD19-targeted CARTs have shown promise in PCNSL, while the activity of CARTs targeting both CD19 and CD20 in PCNSL is being studied. Most PCNSLs are CD20+ subtypes of DLBCL. CD20-directed monoclonal antibody rituximab binds CD20 on PCNSL cells and contributes to the improvement in PCNSL survival when added to chemotherapy backbone. Created in BioRender. (2025) https://BioRender.com/6lx7nif. Abbreviations: PCNSL, primary central nervous system lymphoma; TAM, tumor-associated macrophages; PD-1, programmed cell death protein 1; IL, interleukin; TNF-α, tumor necrosis factor-alpha; CART, chimeric antigen receptor T cells; TGF-β, transforming growth factor-beta; IMiDs, immunomodulatory drugs; CPI, checkpoint inhibitor; PD-L1, programmed death ligand 1; CD, cluster of differentiation; DLBCL, diffuse large B cell lymphoma. |
Lenalidomide has been evaluated as a single agent in combination with other therapies in multiple CNS lymphoma clinical trials. A phase 1 study of 14 patients investigated the lenalidomide and lenalidomide rituximab (R2) combination in patients with RR-PCNSL. The ORR was 68%, and the median PFS was 6 months. Among patients with brain parenchymal lymphoma, the response rate was 60%, and among those with leptomeningeal disease, CR to lenalidomide was 33%. In general, lenalidomide was well-tolerated as monotherapy and with rituximab, with no unexpected toxicities.93 In another phase 2 clinical trial, R2 was studied in 45 patients with RR-PCNSL or primary intravitreal lymphoma. Induction therapy consisted of eight 28-day cycles of R2 followed by lenalidomide maintenance. The median PFS and OS were 7.8 months and 17.7 months, respectively. As observed in previous studies of this combination, neutropenia was the main toxicity and remained manageable. The maximum response to R2 was obtained during the first 4 months of therapy.94
Owing to its immunomodulatory effects, lenalidomide has been used as maintenance therapy in patients with PCNSL. Twenty-two patients aged > 65 yo with PCNSL who achieved >PR to MRT induction and subsequently received low-dose lenalidomide maintenance therapy were retrospectively analyzed. The patient did not undergo ASCT or WBRT consolidation. During a median follow-up of 47 months, the median maintenance time was 14 months. The median PFS was 84 months, and the median OS was not reached. There was only one death due to PCNSL. Maintenance was well tolerated, with mild-to-moderate fatigue and insomnia being the most common side effects.95 The IMiD-based maintenance strategy merits further investigation. The safety and efficacy of lenalidomide and nivolumab for methotrexate-based induction and maintenance are currently under investigation (NCT04609046) (Table 2).
A retrospective analysis of 14 RR-PCNSL patients treated with a combination of lenalidomide, rituximab, and ibrutinib (R2I) reported the best response to CR in 4/14 patients and PR in 4/14 patients. R2I was discontinued due to toxicity in 3/14 patients. Toxicity-related deaths were not observed. These results support further investigations of R2I in R/R PCNSL.96
R2I was further investigated for the treatment of RR PCNSL and SCNSL in an ongoing phase IB trial. Ibrutinib and lenalidomide were administered at escalating doses according to the 3+3 design. Rituximab was administered for six cycles at 500mg/m2, lenalidomide for 12 cycles, and ibrutinib was continued. The combination was well tolerated, and no Aspergillus infection was observed. After a median follow-up of 6.9 months, ORR was achieved in 13/15 of the patients, including 4 CRs. The median PFS was 3.03 months overall and not yet reached for dose 4 level with 1/6 patients progressing with a median follow-up of 5 months.97
Multiple investigations attempting to add immunomodulators to frontline chemotherapy for PCNSL are ongoing. Twelve patients, newly diagnosed with PCNSL, were treated with lenalidomide, rituximab, and methotrexate (R2-MTX) induction followed by R2 consolidation in a phase II study. ORR was achieved in 11/12 with 9 CRs. At a median follow-up of 11.3 months, only one patient had PD. Overall, the regimen was well tolerated and a promising addition to the front-line PCNSL armamentarium.98
Pomalidomide, a novel, third-generation IMiD, has shown excellent CNS penetration at 40%) and significant therapeutic activity against CNSL in murine models. It exhibits dual anti-lymphoma activity via direct cytotoxicity and modulation of the tumor immune microenvironment by converting the polarization status of tumor-associated macrophages (TAMs) from M2 to M1 phenotype (Figure 2). Pomalidomide/dexamethasone followed by pomalidomide maintenance was evaluated in a phase I study for the treatment of RR-PCNSL and PVRL. The dose of pomalidomide used was 5mg. ORR was 43% (9/21) with a median PFS of 5.3 months. Grade 3/4 toxicity was hematologic in 38.1% and non-hematologic in 33.3%.90,99 Pomalidomide is now in NCCN guidelines for the treatment of RR PCNSL (NCCN 2022).
In summary, the preliminary data suggest that IMiD combination regimens are safe and effective. Chemotherapy-free BTKi/IMiD combinations may provide therapeutic opportunities for RR PCNSL patients and those who are not candidates for cytotoxic regimens.
Selinexor
Selinexor (KTP-330) is a selective inhibitor of nuclear export (SINE) that binds and inactivates Exportin-1 (XPO-1). XPO-1 facilitates the nuclear export of regulatory proteins, including tumor suppressors, such as p53, IkB, and p21, and is overexpressed in hematological malignancies. XPO-1 inhibition results in nuclear retention and activation of tumor suppressor proteins, leading to apoptosis. Selinexor inhibits BCR and NF-kB signaling in lymphoma cells. In preclinical studies, GCB and ABC-DLBCL cell lines were equally sensitive to selinexor. In addition, selinexor was found to be synergistic with ibrutinib. Selinexor increased survival and reduced tumor growth in ABC-DLBCL cerebral xenograft mouse models.100 In a phase II study, an ORR of 28% in RR-DLBCL was demonstrated, which led to selinexor’s FDA approval for this indication. Selinexor toxicities included cytopenia, nausea, fatigue, and infections.101
A 55 yo patient with DLBCL who developed an isolated HD-MTX-refractory CNS relapse after several lines of cytotoxic chemotherapy achieved clinically meaningful PR with selinexor 60mg twice a week. Selinexor was discontinued due to fatigue and anorexia with subsequent rapid progression in CNS.102 Several preclinical studies demonstrated that selinexor is synergistic with BTKis, and the combination can repair the immune microenvironment.99,103,104 Five newly diagnosed patients were treated with a novel HD-MTX-Selinexor-BTKi regimen with 100% CRR, durable remissions, and good tolerability.103 Overall, preclinical and clinical evidence prompts further studies of selinexor in CNS lymphoma.
Checkpoint Inhibitors
Immune evasion and spread into “immune-privileged” sites such as the CNS, eyes, testes, and breast is a unifying feature of MCD-DLBCLs, prompting the exploration of immunotherapies in this DLBCL subtype.49 CPIs block immune checkpoints, such as the binding of programmed cell death protein 1 (PD-1) to its ligands, enabling an immune antitumor response (Figure 2).92 Several mechanisms might contribute to the sensitivity of PCNSLs to CPIs. Programmed cell death protein ligand (PD-L) 1 and PD-L2 are encoded on chromosome 9p21.1 and bind to the PD-1 receptor on T cells, blocking T cell activation, which leads to tumor immune evasion. PCNSLs frequently exhibit 9p24.1 copy gains and translocation, leading to increased PD-L1 and PD-L2 expression. 13% of PCNSLs have unique translocations in the PD-L1 loci.105–107 Additionally, aberrant somatic hypermutation (aSHM) leads to increased tumor mutational load in DLBCLs and PCNSLs. aSHM causes transition mutations, with the C to G substitution being more common. The increased mutational load due to aSHM combined with increased PD-L expression may lead to PCNSL sensitivity to CPIs.108 Additionally, tumor-associated macrophages (TAMs) may play a role in PCNSL sensitivity to CPIs. There are two macrophage lineages with different immunophenotype and function, M1 and M2. M1 macrophages are pro-inflammatory and are involved in direct microbial killing. They also have anti-tumor activity via promoting anti-tumor immune responses partially via activating Th1 cells. M2 macrophages promote tumorigenesis as they inhibit anti-tumor responses of M1 and Th1 cells and recruit and activate Tregs and Th2 cells. It has been demonstrated that PCNSL prognosis varies depending on the number and immunophenotype of TAMs. Predominance of TAMs with M2 immunophenotype is common in PCNSL and is associated with worse prognosis.109 M2 macrophages can reduce CPI efficacy via upregulating PD-L1 expression in the tumor, recruiting Tregs and high jacking anti-PD-1 antibodies.110,111 At the same time, TAMs can express PD-1 and become active against tumor cells with this checkpoint inhibition.112 Four patients with RR PCNSL and one with CNS relapse of primary testicular lymphoma were treated with nivolumab, resulting in four CRs and one PR. Three patients remained progression-free at 13+ to 17+ months. In another small study, 8 patients with PCNSL, including 2 treatment-naive patients, received nivolumab. Seven patients responded, and 3 achieved CR. Two-year PFS, OS were 26% and 44% with median OS and PFS of 12 months. There was one case of pseudoprogression followed by CR.113
In a phase II study, 50 patients with RR PCNSL, including nine with PVRL, were treated with pembrolizumab. ORR was 26%, and 10% of patients had stable disease. 1/9 PVRL patient responded. After a median follow-up of 6.7 months, the median PFS was 2.6 months, with a 6-month PFS of 29.8% and a 6-month OS of 60.4%. In the responders, the median DOR was estimated to be 10 months. Pembrolizumab was well tolerated, and there were no toxic deaths.114
Owing to their excellent safety profiles and immunomodulatory effects, CPIs have been studied in combination with BTK inhibitors, IMIDs, and chemotherapeutics (Table 2). Several studies have explored CPIs in maintenance settings (Table 3).
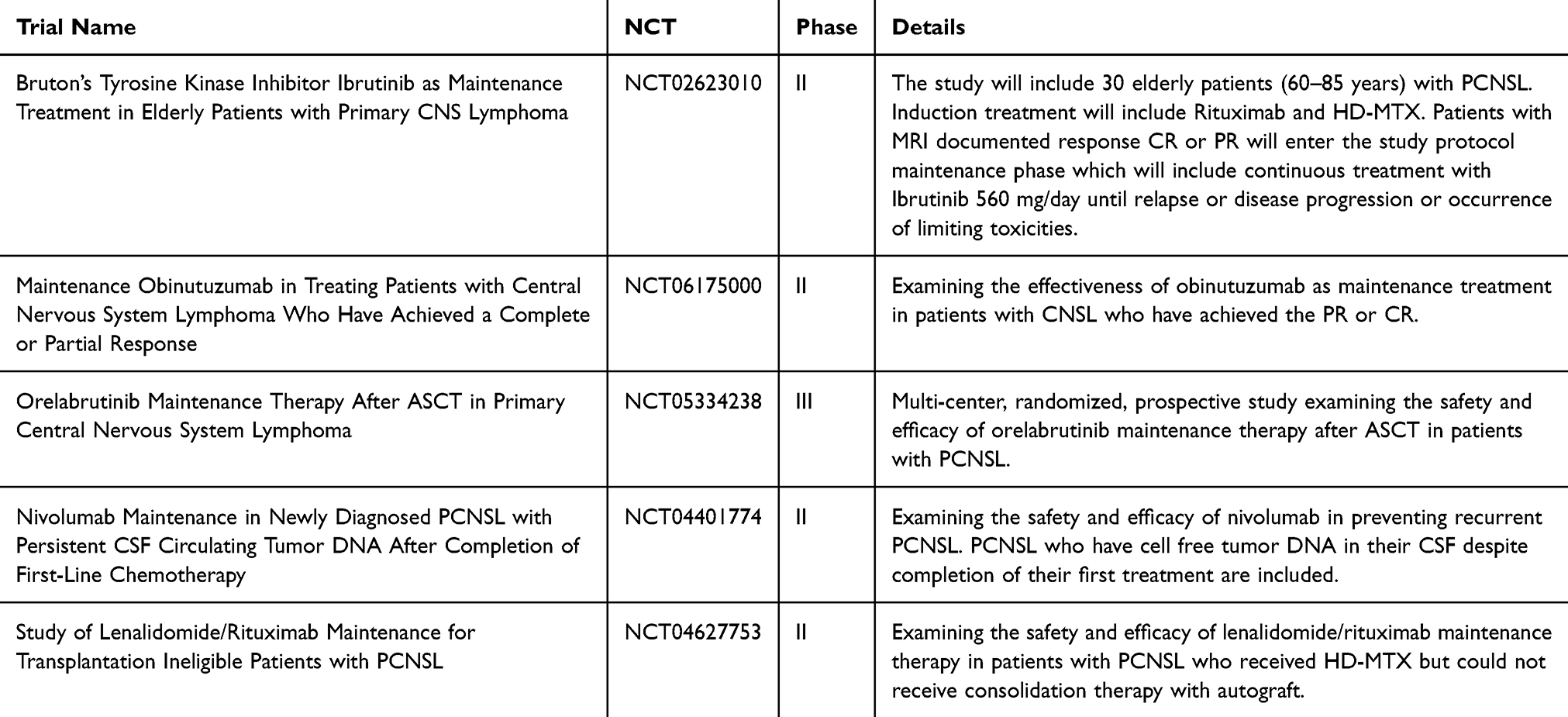 |
Table 3 Maintenance Therapy for PCNSL |
Chimeric Antigen Receptor Therapy
In non-ASCT candidates, RR PCNSL prognosis is dismal, with a median OS of 6.8 months and with 1- and 5-year OS rates of 38% and 18%. ASCT recipients do significantly better with 1 and 5-year OS rates of 74% and 52%.25 CART therapies have the potential to provide a long-standing remission in patients who are not ASCT candidates due to chemo-refractory disease or other factors.
CART immunotherapy has revolutionized the treatment of RR B cell malignancies. CARTs are autologous or allogeneic T cells that have been genetically engineered for MHC-unrestricted binding to a specific antigen on target cancer cells, such as pan-B cell marker CD19, which is expressed on most B cell leukemias and lymphomas (Figure 2).115,116 Autologous CD19-directed CARTs (CD19-CARTs) are FDA-approved for B cell malignancies, including ALL, DLBCL, follicular, and mantle cell lymphomas, but patients with PCNSL have been excluded from most landmark trials because of the fear of potential immune effector cell-associated neurotoxicity syndrome (ICANS). CD19-CARTs administered intravenously were detectable in the CSF, suggesting that they can migrate into the CNS. Some patients with active PCNSL and SCNSL treated with CARTs achieved durable remission. The immunosuppressive brain microenvironment influences PCNSL pathophysiology, linking low immune infiltration to poor prognosis and posing a challenge for immunotherapies in PCNSL. Multiple CART trials for RR PCNSL and SCNSL are currently ongoing (Table 4).117–119
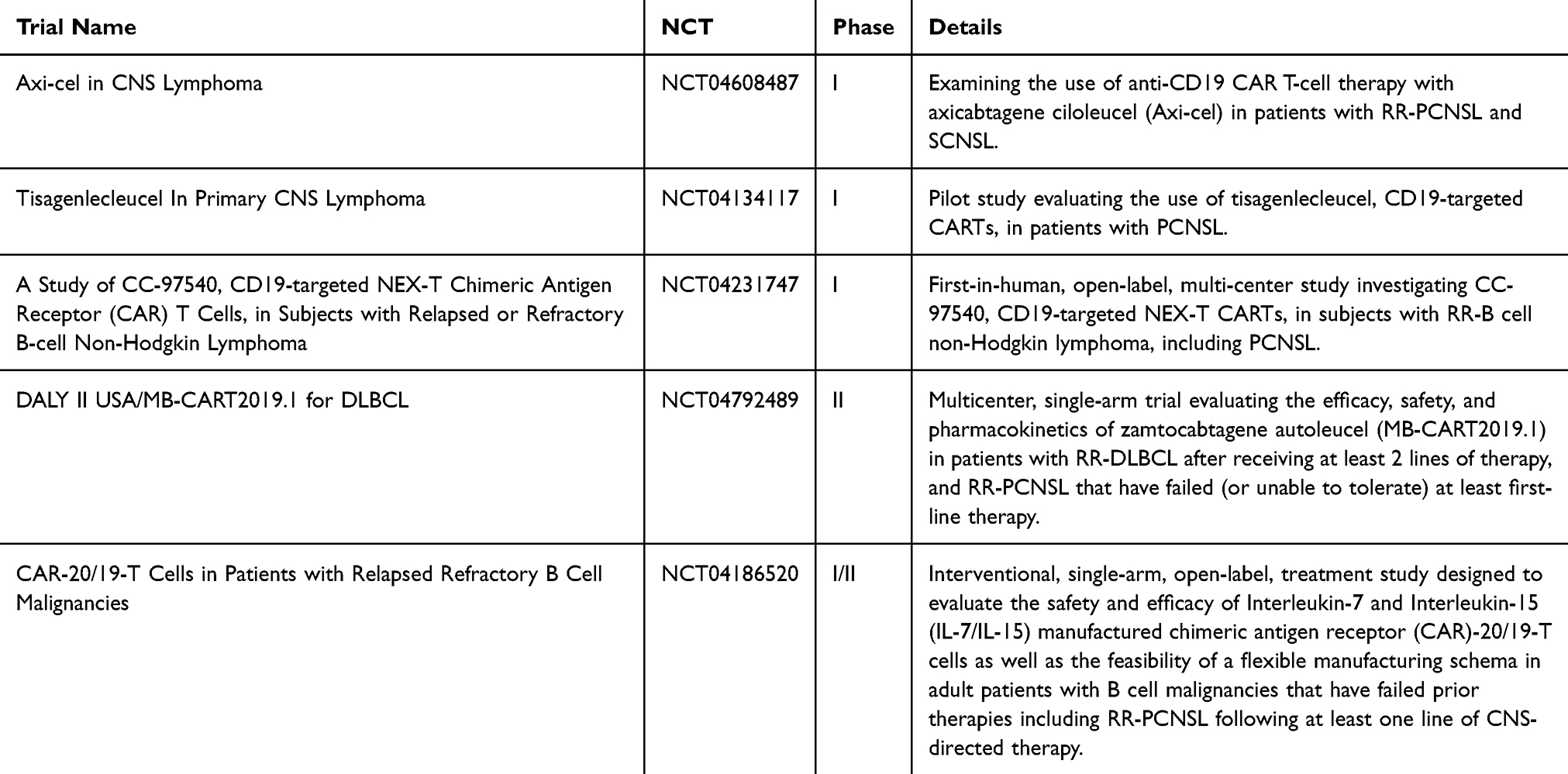 |
Table 4 CART Trials for PCNSL |
As part of a larger clinical trial, five patients with PCNSL were treated with CD19CAR-CD28-CD3zeta-EGFRt-expressing Tn/mem-enriched T lymphocytes. Three patients achieved CR and two achieved SD. All the patients developed grade ≥ 1 cytokine release syndrome (CRS) and ICANS. This study demonstrated the safety and feasibility of CD19 CARTs for PCNSL.117
In another trial, 12 heavily pretreated patients were treated with tisa-cel. Seven out of the 12 patients developed grade 1 CRS, and 5/12 developed ICANS, with only one case of grade 3 ICANS. With a median follow-up of 12.2 months, 7/12 patients demonstrated a response to CR. There were no treatment-related deaths. Tisa-cel has also been detected in the CNS. Remission was sustained in of 3/7 responders demonstrating overall safety and efficacy in patients with highly refractory PCNSL.120
In the US, PCNSL is a specific contraindication for CARTs, whereas there is no such contraindication in Europe. The outcomes of patients with PCNSL treated with CARTs from the French National LOC network database were analyzed. Patients with PCNSL who were not eligible for ASCT and received third-line therapy other than CARTs served as controls (N= 247). Twenty-seven patients were leukapherezed, and 25 received CARTs. All but one patient received bridging therapy, and 14 responded. The median patient age was 68 yo, and 20% of the patients had ECOG 3–4. Sixteen subjects received tisa-cel and 9 axi-cel. The median number of previous treatments was three, and 14/25 patients had previous ASCT. Best responses was CR in 64% and PR in 16%. Patients who responded to bridging therapy and were in CR or PR prior to CARTs had a significantly higher CR rate at 86% vs 36% (p = 0.02). Two patients showed a pseudoprogression. The 12-month RFS rate after CART cell infusion was 79% in patients with CR or PR before CART cell infusion, versus 24% in patients with SD or PD (p= 0.02). The 12-month RFS after CART cell infusion in patients who achieved CR after CART cells was 87%. The 12-month PFS and OS from CART cell infusion were 46% and 55%, respectively. All patients who did not achieve CR with CARTs progressed by 10 months post-therapy. 92% of patients experienced CRS, and 68% experienced neurotoxicity (20% grade ≥3, 36% required ICU transfer). Three patients experienced toxicity lasting over 3 months, with one toxic death, signaling greater CART neurotoxicity than systemic NHL. There was significantly improved median PFS and OS in CART patients at 8.4 months and 21.2 months versus controls (median PFS: 3 months; median OS: 4.7 months; p< 0.001). This real-life study of the largest reported PCNSL patient cohort treated with CARTs demonstrates the feasibility of CART treatment in heavily pretreated PCNSL patients and, most importantly, the potential for prolonged PFS and possible cure in this patient population.121
The retrospective analysis of one of the largest cohorts of RR PCNSL patients who received commercial CARTs including tisa-cel and axi-cel was recently published. Twenty four patients with the median age of 57 yo (range, 25–81) were included, 23 were evaluable for response. Subjects received the median of 4 prior therapies (range, 1–10), 50% had prior ASCT. The ORR was 61% by day 100, with 48% of patients achieving CR. The median follow up from the CART infusion was 26 months (range, 3–38). The 1- and 2- year PFS and OS were 48% and 55%, and 28% and 50% respectively. There was no non-relapse mortality. CRS occurred in 66.7% of patients, with no grade ≥3 CRS. ICANS occurred in 33% of patients with 2 patients who received tisa-cel experiencing grade ≥3 ICANS. These results demonstrate lower activity of CARTs in PCNSL as compared to systemic lymphoma. This may be due to PCNSL immune evasion via increased PD-L1 expression or shorted CART persistence in CNS prompting the development of CART combination or consolidative regimens with IMiDs, CPIs or BTKis.122
Given the efficacy and safety signals, more CART trials are now available for patients with PCNSL, including trials of FDA-approved axi-cel, tisa-cel, and liso-cel. Zamtocabtagene autoleucel (MB-CART2019.1), a bispecific CART targeting both CD19 and CD20, has been explored in patients with PCNSL (Figure 2). International trials of CD19 and CD20 CARTs for the treatment of SCNSL and PCNSL have demonstrated the safety and efficacy of CART and are ongoing (Table 4).123 Novel strategies need to be developed to overcome the brain immunosuppressive microenvironment to facilitate CART efficacy.
Role of Surgery in the Current Treatment Landscape of PCNSL
Surgery is not considered a primary treatment modality for PCNSL since it is often multifocal and involves deep brain structures. PCNSL is exquisitely sensitive to methotrexate and radiation making the role of surgery questionable altogether.124 Traditionally, a diagnostic biopsy has been preferred to a complete resection of a lesion to minimize morbidity.125 A retrospective analysis suggested that complete surgical resection was associated with improved OS; however, the patients were not stratified by performance status or the number of lesions.126 Additionally, in a meta-analysis, patients who underwent resection were more likely to be younger and have a single superficial lesion, introducing potential selection bias.127 While one retrospective study demonstrated improved OS in younger patients with solitary lesions who underwent surgical resection, a different retrospective analysis demonstrated no improvement of OS or PFS with the surgical resection of solitary PCNSL.128,129 Further prospective studies are needed to define the role of surgery in PCNSL. There are no retrospective or prospective studies that address the role of surgery in combination with novel chemotherapeutics.
Expert Opinion on Emerging Therapies in Primary Central Nervous System Lymphoma
With the incorporation of rituximab and alkylators into the HD-MTX based induction therapy and addition of the thiotepa-based high dose therapy and ASCT consolidative therapy, PCNSL outcomes have improved dramatically for the younger and fit transplant candidate patients.12 With a median diagnosis age of 65 yo, the past decade has seen a marked increase in PCNSL among the elderly, especially in those aged 70 to 79 yo, with over 20% of all PCNSL cases occurring in patients aged ≥80 yo.5 PCNSL outcomes in older patients who are not transplant candidates remain dismal.130 Current frontline therapies, such as HD-MTX, while effective, are associated with significant toxicities and require inpatient administration. This can be particularly burdensome for elderly patients, leading to psychosocial distress, extended hospital stay, rehabilitation costs, and treatment delays due to de-conditioning. The need for re-conditioning between treatment cycles can lead to treatment delays, increasing the overall morbidity and treatment failure rate.131 This underscores the necessity for more tolerable outpatient induction, salvage, and maintenance regimens.
The dependence of PCNSL on aberrantly activated BCR signaling axis and, subsequently, the NF-κB pathway has opened the door for well-tolerated oral targeted therapies. Multiple BTK inhibitors, including ibrutinib, tirabrutinib, and zanubrutinib, have shown efficacy and safety in PCNSL as single agents as well as in combination.56,63,131,132 Immunomodulators, including lenalidomide and pomalidomide, exploit the importance of NF-κB pathway in PCNSL and can be safely combined with BTK inhibitors.90,94,96,97,99 PI3K inhibitors may be synergistic with BTK inhibitors, prompting combination trials.58 Despite efficacy, PCNSL is well-tolerated, quickly develops resistance to above mentioned targeted therapies, leading to short PFS. Therefore, novel combination regimens are required to overcome the development of pathway inhibitor resistance. The multitargeted antifolate agent pemetrexed is a valuable alternative to methotrexate as a PCNSL chemotherapeutic backbone because of its known activity in RR PCNSL, excellent side effect profile, and outpatient administration.14,40 Just as rituximab eventually became a standard component of PCNSL induction regimens, we expect BTK inhibitors, IMiDs, and checkpoint inhibitors to eventually lead to frontline PCNSL regimens. Similarly, to the trends in systemic DLBCL, there is an opportunity for salvage PCNSL regimens to be entirely constituent of novel targeted well-tolerated outpatient pharmaceuticals.
Post-induction maintenance therapies may improve the outcomes of patients who are not candidates for ASCT consolidation. Ibrutinib and lenalidomide have shown promise as maintenance agents, while other BTK inhibitors, immunomodulators, and checkpoint inhibitors are currently being explored in maintenance trials (Table 3).66,95,133
Despite initial toxicity concerns, CART therapy has proven to be an effective and safe salvage option for RR-PCNSL.121 In the future, CARTs may offer a consolidative option to non-ASCT candidates. Multiple CART constructs, including novel bispecific CD19/CD20 CART cells, are currently under investigation (Table 4).
With ongoing advancements in targeted therapies and CART cells, the shift from traditional inpatient chemotherapy to more manageable outpatient regimens for PCNSL is becoming a reality. Further research should focus on well-tolerated outpatient targeted therapies to improve the disease-related quality of life and outcomes for patients with PCNSL.
Disclosure
Dr. Yuliya Linhares is a consultant with Acrotech, ADCT, BMS, GenMab, Genentech, Kyowa Kirin, Novartis, and Pfizer and received research funding from BeiGene Therapeutics, Miltenyi, ADCT, and Genentech, personal fees from astra zeneca, personal fees from Gilead. Dr Ariel Perez-Perez reports Speaker Bureau from Gilead Kite, consulting from AbbVie, outside the submitted work. Dr Yazmin Odia reports personal fees from Pharpoint, personal fees from GammaTile, grants from Cantex, grants from Exelixis, outside the submitted work. Dr Manmeet Ahluwalia reports personal fees from Bayer, personal fees from Xoft, personal fees from Anheart Therapeutics, personal fees from Apollomics, personal fees from Viewray, personal fees from Cairn Therapeutics, personal fees from Theraguix, personal fees from MenariniRicerche, personal fees from Autem therapeutics, personal fees from Sumitomo Pharma Oncology, personal fees from GT Medical Technologies, personal fees from Incyte, personal fees from Servier Pharmaceuticals, personal fees from Allovir, personal fees from EquilliumBio, personal fees from VBI Vaccines, personal fees from Modifibiosciences, personal fees from Bugworks, grants from Pfizer, stock options from Trisalus Lifesciences, stock options from Mimivax, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Ostrom QT, Cioffi G, Gittleman H. et al. CBTRUS statistical report: primary brain and other central nervous system tumors diagnosed in the United States in 2012-2016. Neuro Oncol. 2019;21(5):v1–v100. doi:10.1093/neuonc/noz150
2. Grommes C, Rubenstein JL, DeAngelis LM, et al. Comprehensive approach to diagnosis and treatment of newly diagnosed primary CNS lymphoma. Neuro Oncol. 2019;21(3):296–305. doi:10.1093/neuonc/noy192
3. Shao L, Xu C, Wu H, et al. Recent Progress on Primary Central Nervous System Lymphoma-From Bench to Bedside. Front Oncol. 2021;11. doi:10.3389/fonc.2021.689843
4. Haldorsen IS, Krossnes BK, Aarseth JH, et al. Increasing incidence and continued dismal outcome of primary central nervous system lymphoma in Norway 1989–2003: time trends in a 15‐year national survey. Cancer. 2007;110(8):1803–1814. doi:10.1002/cncr.22989
5. Liu Y, Yao Q, Zhang F. Diagnosis, prognosis, and treatment of primary central nervous system lymphoma in the elderly population. Int J Oncol. 2021;58(3):371–387. doi:10.3892/ijo.2021.5180
6. Batchelor T, Carson K, O’Neill A, et al. Treatment of primary CNS lymphoma with methotrexate and deferred radiotherapy: a report of NABTT 96-07. J Clin Oncol. 2003;21(6):1044–1049. doi:10.1200/JCO.2003.03.036
7. Neuro-Oncology Working Group of the German Society, Herrlinger U, Küker W, Uhl M, et al. NOA-03 trial of high-dose methotrexate in primary central nervous system lymphoma: final report. Ann Neurol. 2005;57(6):843–847. doi:10.1002/ana.20495.
8. Holdhoff M, Ambady P, Abdelaziz A, et al. High-dose methotrexate with or without rituximab in newly diagnosed primary CNS lymphoma. Neurology. 2014;83(3):235–239. doi:10.1212/WNL.0000000000000593
9. Jahnke K, Thiel E, Martus P, et al. Relapse of primary central nervous system lymphoma: clinical features, outcome and prognostic factors. J Neurooncol. 2006;80(2):159–165. doi:10.1007/s11060-006-9165-6
10. Birnbaum JT, Stadler EA, von Baumgarten L, et al. Rituximab significantly improves complete response rate in patients with primary CNS lymphoma. J Neurooncol. 2012;109(2):285–291. doi:10.1007/s11060-012-0891-7
11. Bromberg JEC, Issa S, Bakunina K, et al. Rituximab in patients with primary CNS lymphoma (HOVON 105/ALLG NHL 24): a randomised, open-label, phase 3 intergroup study. Lancet Oncol. 2019;20(2):216–228. doi:10.1016/S1470-2045(18)30747-2
12. Omuro A, Correa DD, DeAngelis LM, et al. R-MPV followed by high-dose chemotherapy with TBC and autologous stem-cell transplant for newly diagnosed primary CNS lymphoma. Blood. 2015;125(9):1403–1410. doi:10.1182/blood-2014-10-604561
13. Nagle SJ, Shah NN, Ganetsky A, et al. Long-term outcomes of rituximab, temozolomide and high-dose methotrexate without consolidation therapy for lymphoma involving the CNS. Int J Hematol Oncol. 2017;6(4):113–121. doi:10.2217/ijh-2017-0020
14. Raizer JJ, Rademaker A, Evens AM, et al. Pemetrexed in the treatment of relapsed/refractory primary central nervous system lymphoma. Cancer. 2012;118(15):3743–3748. doi:10.1002/cncr.26709
15. Houillier C, Taillandier L, Dureau S, et al. Radiotherapy or Autologous Stem-Cell Transplantation for Primary CNS Lymphoma in Patients 60 Years of Age and Younger: results of the Intergroup ANOCEF-GOELAMS Randomized Phase II PRECIS Study. J Clin Oncol. 2019;37(10):823–833. doi:10.1200/JCO.18.00306
16. Pels H, Schmidt-Wolf IG, Glasmacher A, et al. Primary central nervous system lymphoma: results of a pilot and phase II study of systemic and intraventricular chemotherapy with deferred radiotherapy. J Clin Oncol. 2003;21(24):4489–4495. doi:10.1200/JCO.2003.04.056
17. Ferreri AJ, Reni M, Foppoli M, et al. High-dose cytarabine plus high-dose methotrexate versus high-dose methotrexate alone in patients with primary CNS lymphoma: a randomised phase 2 trial. Lancet. 2009;374(9700):1512–1520. doi:10.1016/S0140-6736(09)61416-1
18. Rubenstein JL, Hsi ED, Johnson JL, et al. Intensive chemotherapy and immunotherapy in patients with newly diagnosed primary CNS lymphoma: CALGB 50202 (Alliance 50202). J Clin Oncol. 2013;31(25):3061–3068. doi:10.1200/JCO.2012.46.9957
19. Ferreri AJ, Cwynarski K, Pulczynski E, et al. Chemoimmunotherapy with methotrexate, cytarabine, thiotepa, and rituximab (MATRix regimen) in patients with primary CNS lymphoma: results of the first randomisation of the International Extranodal Lymphoma Study Group-32 (IELSG32) phase 2 trial. Lancet Haematol. 2016;3(5):e217–27. doi:10.1016/S2352-3026(16)00036-3
20. Illerhaus G, Ferreri A, Binder M, et al. Consolidative HCT-ASCT is Superior to Non-Myeloablative Chemo-Immunotherapy in Newly-Diagnosed PCNSL - Updated Results of the Randomized Phase III MATRix/IELSG43 Trial [abstract]. Hematol Oncol. 2023;41(S2):41–43. doi:10.1002/hon.3163_15
21. Thiel E, Korfel A, Martus P, et al. High-dose methotrexate with or without whole brain radiotherapy for primary CNS lymphoma (G-PCNSL-SG-1): a phase 3, randomised, non-inferiority trial. Lancet Oncol. 2010;11(11):1036–1047. doi:10.1016/S1470-2045(10)70229-1
22. Houillier C, Dureau S, Taillandier L, et al. Radiotherapy or Autologous Stem-Cell Transplantation for Primary CNS Lymphoma in Patients Age 60 Years and Younger: long-Term Results of the Randomized Phase II PRECIS Study. J Clin Oncol. 2022;40(32):3692–3698. doi:10.1200/JCO.22.00491
23. Therkelsen KE, Schaff LR, Nandakumar S, Omuro AM, DeAngelis LM, Grommes C. Long-term outcomes in primary CNS lymphoma after R-MVP and high-dose chemotherapy with autologous hematopoietic stem cell transplant. Neurology. 2023;101(7):e710–6. doi:10.1212/WNL.0000000000207490
24. Tringale KR, Scordo M, Yahalom J, et al. Evolving consolidation patterns and outcomes for a large cohort of patients with primary CNS lymphoma. Blood Adv. 2024;8(24):6195–6206. doi:10.1182/bloodadvances.2024013780
25. Houillier C, Soussain C, Ghesquières H, et al. Management and outcome of primary CNS lymphoma in the modern era: an LOC network study. Neurology. 2020;94(10):e1027–e1039. doi:10.1212/WNL.0000000000008900
26. Mendez JS, Ostrom QT, Gittleman H, et al. The elderly left behind-changes in survival trends of primary central nervous system lymphoma over the past 4 decades. Neuro Oncol. 2018;20(5):687–694. doi:10.1093/neuonc/nox187
27. Kaji FA, Martinez‐Calle N, Bishton MJ, et al. Improved survival outcomes despite older age at diagnosis: an era‐by‐era analysis of patients with primary central nervous system lymphoma treated at a single referral centre in the United Kingdom. Br J Haematol. 2021;195(4):561–570. doi:10.1111/bjh.17747
28. Burns EA, Sanchez CG, Mathur S, et al. Long term outcomes in older patients with primary central nervous system lymphoma: an analysis of the Texas Cancer Registry. Ann Hematol. 2023;102(5):1111–1120. doi:10.1007/s00277-023-05140-6
29. Duell J, Maddocks KJ, González-Barca E, et al. Long-term outcomes from the Phase II L-MIND study of tafasitamab (MOR208) plus lenalidomide in patients with relapsed or refractory diffuse large B-cell lymphoma. Haematologica. 2021;106(9):2417–2426. doi:10.3324/haematol.2020.275958
30. Budde LE, Sehn LH, Matasar M, et al. Safety and efficacy of mosunetuzumab, a bispecific antibody, in patients with relapsed or refractory follicular lymphoma: a single-arm, multicentre, phase 2 study. Lancet Oncol. 2022;23(8):1055–1065. doi:10.1016/S1470-2045(22)00335-7
31. Caimi PF, Ai W, Alderuccio JP, et al. Loncastuximab tesirine in relapsed or refractory diffuse large B-cell lymphoma (LOTIS-2): a multicentre, open-label, single-arm, phase 2 trial. Lancet Oncol. 2021;22(6):790–800. doi:10.1016/S1470-2045(21)00139-X
32. Westin JR, Kersten MJ, Salles G, et al. Efficacy and safety of CD19-directed CAR-T cell therapies in patients with relapsed/refractory aggressive B-cell lymphomas: observations from the JULIET, ZUMA-1, and TRANSCEND trials. Am J Hematol. 2021;96(10):1295–1312. doi:10.1002/ajh.26301
33. Ferreri AJ, Calimeri T, Cwynarski K, et al. Primary central nervous system lymphoma. Nat Rev Dis Primers. 2023;9(1):29. doi:10.1038/s41572-023-00439-0
34. von Roemeling C, Ferreri AJ, Soussain C, Tun HW, Grommes C. Targets and treatments in primary CNS lymphoma. Leuk Lymphoma. 2024;65(8):1055–1067. doi:10.1080/10428194.2024.2342560
35. Shih C, Chen VJ, Gossett LS, et al. LY231514, a pyrrolo [2,3-d] pyrimidine-based antifolate that inhibits multiple folate-requiring enzymes. Cancer Res. 1997;57(6):1116–1123.
36. Han S, Wang M, Liu B, et al. Pemetrexed for primary central nervous system lymphoma in the elderly. Clin Transl Oncol. 2016;18(2):138–143. doi:10.1007/s12094-015-1345-4
37. Dietrich J, Versmee L, Drappatz J, et al. Pemetrexed in Recurrent or Progressive Central Nervous System Lymphoma: a Phase I Multicenter Clinical Trial. Oncologist. 2020;25(9):747–e1273. doi:10.1634/theoncologist.2020-0489
38. Zhang JP, Lee EQ, Nayak L, et al. Retrospective study of pemetrexed as salvage therapy for central nervous system lymphoma. J Neurooncol. 2013;115(1):71–77. doi:10.1007/s11060-013-1196-1
39. Zhao HT, Chen J, Shi SB, et al. Pemetrexed plus rituximab as second-line treatment for primary central nervous system lymphoma. Med Oncol. 2015;32(1):351. doi:10.1007/s12032-014-0351-7
40. Ma J, Lin Z, Ding T, et al. Pemetrexed Plus Lenalidomide for Relapsed/Refractory Primary Central Nervous System Lymphoma: a Prospective Single-Arm Phase II Study. Front Oncol. 2022;12:938421. doi:10.3389/fonc.2022.938421
41. Pfreundschuh M, Trümper L, Osterborg A, et al. CHOP-like chemotherapy plus rituximab versus CHOP-like chemotherapy alone in young patients with good-prognosis diffuse large-B-cell lymphoma: a randomised controlled trial by the MabThera International Trial (MInT) Group. Lancet Oncol. 2006;7(5):379–391. doi:10.1016/S1470-2045(06)70664-7
42. Rubenstein JL, Rosenberg J, Damon L High-dose methotrexate plus rituximab (Anti-CD20) monoclonal antibody in the treatment of primary CNS lymphoma [abstract]. Soc Neuro-Onc; fourth annual meeting. 1999.
43. Shah GD, Yahalom J, Correa DD, et al. Combined immunochemotherapy with reduced whole-brain radiotherapy for newly diagnosed primary CNS lymphoma. J Clin Oncol. 2007;25(30):4730–4735. doi:10.1200/JCO.2007.12.5062
44. Ferreri AJM, Cwynarski K, Pulczynski E, et al. Long-term efficacy, safety and neurotolerability of MATRix regimen followed by autologous transplant in primary CNS lymphoma: 7-year results of the IELSG32 randomized trial. Leukemia. 2022;36(7):1870–1878. doi:10.1038/s41375-022-01582-5
45. Houillier C, Ghesquières H, Chabrot C, et al. Rituximab, methotrexate, procarbazine, vincristine and intensified cytarabine consolidation for primary central nervous system lymphoma (PCNSL) in the elderly: a LOC network study. J Neurooncol. 2017;133(2):315–320. doi:10.1007/s11060-017-2435-7
46. Fraser E, Gruenberg K, Rubenstein JL. New approaches in primary central nervous system lymphoma. Chin Clin Oncol. 2015;4(1):11. doi:10.3978/j.issn.2304-3865.2015.02.01
47. Alizadeh AA, Eisen MB, Davis RE, et al. Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature. 2000;403(6769):503–511. doi:10.1038/35000501
48. Schmitz R, Wright GW, Huang DW, et al. Genetics and Pathogenesis of Diffuse Large B-Cell Lymphoma. N Engl J Med. 2018;378(15):1396–1407. doi:10.1056/NEJMoa1801445
49. Wright GW, Huang DW, Phelan JD, et al. A probabilistic classification tool for genetic subtypes of diffuse large B cell lymphoma with therapeutic implications. Cancer Cell. 2020;37(4):551–568. doi:10.1016/j.ccell.2020.03.015
50. Nakamura T, Tateishi K, Niwa T, et al. Recurrent mutations of CD79B and MYD88 are the hallmark of primary central nervous system lymphomas. Neuropathol Appl Neurobiol. 2016;42(3):279–290. doi:10.1111/nan.12259
51. Radke J, Ishaque N, Koll R, et al. The genomic and transcriptional landscape of primary central nervous system lymphoma. Nat Commun. 2022;13(1):2558. doi:10.1038/s41467-022-30050-y
52. Nishimura N, Takeuchi K, Asaka R, et al. MYD88 L265P mutation detected by digital PCR as a prognostic factor in patients with diffuse large B-cell lymphoma in rituximab era. Leuk Res. 2020;97:106426. doi:10.1016/j.leukres.2020.106426
53. Phelan JD, Young RM, Webster DE, et al. A multiprotein supercomplex controlling oncogenic signalling in lymphoma. Nature. 2018;560(7718):387–391. doi:10.1038/s41586-018-0290-0
54. de Groen RAL, Schrader AMR, Kersten MJ, et al. MYD88 in the driver’s seat of B-cell lymphomagenesis: from molecular mechanisms to clinical implications. Haematologica. 2019;104(12):2337–2348. doi:10.3324/haematol.2019.227272
55. Dimopoulos MA, Trotman J, Tedeschi A, et al. Ibrutinib for patients with rituximab-refractory Waldenström’s macroglobulinaemia (iNNOVATE): an open-label substudy of an international, multicentre, phase 3 trial. Lancet Oncol. 2017;18(2):241–250. doi:10.1016/S1470-2045(16)30632-5
56. Lionakis MS, Dunleavy K, Roschewski M, et al. Inhibition of B Cell Receptor Signaling by Ibrutinib in Primary CNS Lymphoma. Cancer Cell. 2017;31(6):833–843. doi:10.1016/j.ccell.2017.04.012
57. Low JT, Peters KB. Ibrutinib in Primary Central Nervous System Diffuse Large B-Cell Lymphoma. CNS Oncol. 2020;9(1):CNS51. doi:10.2217/cns-2019-0022
58. Grommes C, Pastore A, Palaskas N, et al. Ibrutinib unmasks critical role of Bruton tyrosine kinase in primary CNS lymphoma. Cancer Discov. 2017;7(9):1018–1029. doi:10.1158/2159-8290.CD-17-0613
59. Wilson WH, Young RM, Schmitz R, et al. Targeting B cell receptor signaling with ibrutinib in diffuse large B cell lymphoma. Nat Med. 2015;21(8):922–926. doi:10.1038/nm.3884
60. Soussain C, Choquet S, Blonski M, et al. Ibrutinib monotherapy for relapse or refractory primary CNS lymphoma and primary vitreoretinal lymphoma: final analysis of the phase II ‘proof-of-concept’ iLOC study by the Lymphoma study association (LYSA) and the French oculo-cerebral lymphoma (LOC) network. Eur J Cancer. 2019;117:121–130. doi:10.1016/j.ejca.2019.05.024
61. Hou K, Yu Z, Jia Y, et al. Efficacy and safety of ibrutinib in diffuse large B-cell lymphoma: a single-arm meta-analysis. Crit Rev Oncol Hematol. 2020;152:1.
62. Roschewski M, Simard J, Melani C, et al. Phase 2 Study of Ibrutinib with Temozolomide, Etoposide, Liposomal Doxorubicin, Dexamethasone, Rituximab (TEDDI-R) for Secondary CNS Lymphoma. Hematol Oncol. 2023;41(S2):44–46. doi:10.1002/hon.3163_17
63. Grommes C, Tang SS, Wolfe J, et al. Phase 1b trial of an ibrutinib-based combination therapy in recurrent/refractory CNS lymphoma. Blood. 2019;133(5):436–445. doi:10.1182/blood-2018-09-875732
64. Renaud L, Bossard JB, Terriou L. Treatment with Temozolomide and Ibrutinib in Recurrent/Refractory Primary (PCNSL) and Secondary CNS Lymphoma (SCNSL) [abstract]. Blood. 2020;136(Suppl 1):23–24. doi:10.1182/blood-2020-138764
65. Guo Y, Lan X, Chang X, et al. Ibrutinib in Combination with Rituximab and High-Dose Methotrexate in Newly Diagnosed Primary Central Nervous System Lymphoma Patients [abstract]. Blood. 2021;138(1):1416. doi:10.1182/blood-2021-147742
66. Wang X, Shan C, Huang H, et al. A Prospective Study of Methotrexate in Combination with Ibrutinib and Temozolomide (MIT) in Newly Diagnosed Primary CNS Lymphoma [abstract]. Blood. 2022;140(Suppl 1):6606–6607. doi:10.1182/blood-2022-169608
67. Shirley MB. Tyrosine Kinase Inhibitors in B-Cell Malignancies: their Use and Differential Features. Target Oncol. 2022;17(1):69–84. doi:10.1007/s11523-021-00857-8
68. Guo Y, Liu Y, Hu N, et al. Discovery of Zanubrutinib (BGB-3111), a Novel, Potent, and Selective Covalent Inhibitor of Bruton’s Tyrosine Kinase. J Med Chem. 2019;62(17):7923–7940. doi:10.1021/acs.jmedchem.9b00687
69. Hillmen P, Eichhorst B, Brown JR, et al. Zanubrutinib Versus Ibrutinib in Relapsed/Refractory Chronic Lymphocytic Leukemia and Small Lymphocytic Lymphoma: interim Analysis of a Randomized Phase III Trial. J Clin Oncol. 2023;41(5):1035–1045. doi:10.1200/JCO.22.00510
70. Treon SP, Gustine J, Meid K, et al. Ibrutinib monotherapy in symptomatic, treatment-naïve patients with Waldenström macroglobulinemia. J Clin Oncol. 2018;36(27):2755–2761. doi:10.1200/JCO.2018.78.6426
71. Treon SP, Meid K, Gustine J, et al. Long-term follow-up of previously treated patients who received ibrutinib for symptomatic Waldenstrom’s macroglobulinemia: update of pivotal clinical trial [abstract]. Blood. 2017;130(Suppl 1):1.
72. Dimopoulos M, Sanz RG, Lee HP, et al. Zanubrutinib for the treatment of MYD88 wild-type Waldenström macroglobulinemia: a substudy of the phase 3 ASPEN trial. Blood Adv. 2020;4(23):6009–6018. doi:10.1182/bloodadvances.2020003010
73. Zhang Y, Li Y, Zhuang Z, et al. Preliminary Evaluation of Zanubrutinib-Containing Regimens in DLBCL and the Cerebrospinal Fluid Distribution of Zanubrutinib: a 13-Case Series. Front Oncol. 2021;11:760405. doi:10.3389/fonc.2021.760405
74. Cheng Q, Wang J, Lv C, et al. Successful Management of a Patient with Refractory Primary Central Nervous System Lymphoma by Zanubrutinib. Onco Targets Ther. 2021;14:3367–3372. doi:10.2147/OTT.S309408
75. Wang L, Guan W, Peng X. Targeting Bruton Tyrosine Kinase With Zanubrutinib for Treatment of Vitreoretinal Lymphoma: report of 3 Cases. Front Oncol. 2021;11:676792. doi:10.3389/fonc.2021.676792
76. Narita Y, Nagane M, Mishima K, et al. Phase I/II study of tirabrutinib, a second-generation Bruton’s tyrosine kinase inhibitor, in relapsed/refractory primary central nervous system lymphoma. Neuro Oncol. 2021;23(1):122–133. doi:10.1093/neuonc/noaa145
77. Wu JJ, Wang WH, Dong M, et al. Orelabrutinib-Bruton tyrosine kinase inhibitor-based regimens in the treatment of central nervous system lymphoma: a retrospective study. Invest New Drugs. 2022;40(3):650–659. doi:10.1007/s10637-022-01219-5
78. Qiao L, Liu Q, Huang C. Orelabrutinib versus ibrutinib for patients with refractory/relapsed primary central nervous system lymphoma: an efficacy and safety analysis. Medicine. 2023;102(27):e33880. doi:10.1097/MD.0000000000033880
79. Xia Y, Li X, Jiang N, et al. A novel Bruton’s tyrosine kinase inhibitor JDB175 shows potent efficacy to suppress central nervous system lymphoma. MedComm. 2023;4(6):e424. doi:10.1002/mco2.424
80. Illerhaus G, Schorb E, Kasenda B. Novel agents for primary central nervous system lymphoma: evidence and perspectives. Blood. 2018;132(7):681–688. doi:10.1182/blood-2018-01-791558
81. Zhang X, Wu Y, Sun X, et al. The PI3K/AKT/mTOR signaling pathway is aberrantly activated in primary central nervous system lymphoma and correlated with a poor prognosis. BMC Cancer. 2022;22(1):190. doi:10.1186/s12885-022-09275-z
82. Korfel A, Schlegel U, Herrlinger U, et al. Phase II Trial of Temsirolimus for Relapsed/Refractory Primary CNS Lymphoma. J Clin Oncol. 2016;34(15):1757–1763. doi:10.1200/JCO.2015.64.9897
83. Grommes C, Pentsova E, Schaff LR, et al. Preclinical and clinical evaluation of Buparlisib (BKM120) in recurrent/refractory Central Nervous System Lymphoma. Leuk Lymphoma. 2023;64(9):1545–1553. doi:10.1080/10428194.2023.2223734
84. Beaufils F, Cmiljanovic N, Cmiljanovic V, et al. 5-(4,6-Dimorpholino-1,3,5-triazin-2-yl)-4-(trifluoromethyl)pyridin-2-amine (PQR309), a Potent, Brain-Penetrant, Orally Bioavailable, Pan-Class I PI3K/mTOR Inhibitor as Clinical Candidate in Oncology. J Med Chem. 2017;60(17):7524–7538. doi:10.1021/acs.jmedchem.7b00930
85. Bohnacker T, Prota AE, Beaufils F, et al. Deconvolution of Buparlisib’s mechanism of action defines specific PI3K and tubulin inhibitors for therapeutic intervention. Nat Commun. 2017;8(1):14683. doi:10.1038/ncomms14683
86. Grommes C, Gavrilovic I, Miller AM, et al. Phase Ib of Copanlisib in Combination with Ibrutinib in Recurrent/Refractory Primary CNS Lymphoma (PCNSL). Blood. 2019;134(Suppl 1):1598. doi:10.1182/blood-2019-126214
87. Zhu YX, Shi CX, Bruins LA, et al. Identification of lenalidomide resistance pathways in myeloma and targeted resensitization using cereblon replacement, inhibition of STAT3 or targeting of IRF4. Blood Cancer J. 2019;9(2):19. doi:10.1038/s41408-019-0173-0
88. Bjorklund CC, Lu L, Kang J, et al. Rate of CRL4(CRBN) substrate Ikaros and Aiolos degradation underlies differential activity of lenalidomide and pomalidomide in multiple myeloma cells by regulation of c-Myc and IRF4. Blood Cancer J. 2015;5(10):e354. doi:10.1038/bcj.2015.66
89. Grommes C, Nayak L, Tun HW, et al. Introduction of novel agents in the treatment of primary CNS lymphoma. Neuro Oncol. 2019;21(3):306–313. doi:10.1093/neuonc/noy193
90. Li Z, Qiu Y, Personett D, et al. Pomalidomide shows significant therapeutic activity against CNS lymphoma with a major impact on the tumor microenvironment in murine models. PLoS One. 2013;8(8):e71754. doi:10.1371/journal.pone.0071754
91. Hideshima T, Ogiya D, Liu J, et al. Immunomodulatory drugs activate NK cells via both Zap-70 and cereblon-dependent pathways. Leukemia. 2021;35(1):177–188. doi:10.1038/s41375-020-0809-x
92. Alcantara M, Fuentealba J, Soussain C. Emerging landscape of immunotherapy for primary central nervous system lymphoma. Cancers. 2021;13(20):5061. doi:10.3390/cancers13205061
93. Rubenstein JL, Geng H, Fraser EJ, et al. Phase 1 investigation of lenalidomide/rituximab plus outcomes of lenalidomide maintenance in relapsed CNS lymphoma. Blood Adv. 2018;2(13):1595–1607. doi:10.1182/bloodadvances.2017014845
94. Ghesquieres H, Chevrier M, Laadhari M, et al. Lenalidomide in combination with intravenous rituximab (REVRI) in relapsed/refractory primary CNS lymphoma or primary intraocular lymphoma: a multicenter prospective ‘proof of concept’ phase II study of the French Oculo-Cerebral lymphoma (LOC) Network and the Lymphoma Study Association (LYSA). Ann Oncol. 2019;30(4):621–628. doi:10.1093/annonc/mdz032
95. Tsang M, Cleveland J, Cerejo MC, et al. Survival and Patient-Reported Outcomes of Older Adults with Primary Central Nervous System Lymphoma on Low-Dose Lenalidomide. Blood. 2020;136(Suppl 1):21–22. doi:10.1182/blood-2020-143070
96. Houillier C, Chabrot CM, Moles-Moreau MP, et al. Rituximab-Lenalidomide-Ibrutinib Combination for Relapsed/Refractory Primary CNS Lymphoma A Case Series of the LOC Network. Neurol. 2021;97(13):628–631. doi:10.1212/WNL.0000000000012515
97. Grommes C, Piotrowski A, Pentsova E, et al. Phase Ib Trial with Dose Expansion of the Bruton’s Tyrosine Kinase (BTK) Inhibitor, Ibrutinib, in Combination with Rituximab and Lenalidomide in Patients with Refractory/Recurrent Primary Central Nervous System Lymphoma (PCNSL) and Refractory/Recurrent Secondary Central Nervous System Lymphoma (SCNSL). Blood. 2020;136(Suppl 1):48.
98. Yuan X, Liang Y, Liu H, et al. Lenalidomide, Rituximab and Methotrexate (R2-MTX) in Newly Diagnosed Primary Central Nervous System Lymphoma [abstract]. Blood. 2021;138(Suppl 1):2491. doi:10.1182/blood-2021-145565
99. Tun HW, Johnston PB, DeAngelis LM, et al. Phase 1 study of pomalidomide and dexamethasone for relapsed/refractory primary CNS or vitreoretinal lymphoma. Blood. 2018;132(21):2240–2248. doi:10.1182/blood-2018-02-835496
100. Crespo M, Carabia J, Jiménez I, et al. XPO1 Inhibition by Selinexor Synergizes with BCR Inhibition, Blocks Tumor Growth and Prolongs Survival in a Bioluminescent Animal Model of Primary Central Nervous System Lymphoma. Blood. 2016;128(22):463. doi:10.1182/blood.V128.22.463.463
101. Kalakonda N, Maerevoet M, Cavallo F, et al. Selinexor in patients with relapsed or refractory diffuse large B-cell lymphoma (SADAL): a single-arm, multinational, multicentre, open-label, phase 2 trial. Lancet Haematol. 2020;7(7):e511–e522. doi:10.1016/S2352-3026(20)30120-4
102. Bobillo S, Abrisqueta P, Carpio C, et al. Promising activity of selinexor in the treatment of a patient with refractory diffuse large B-cell lymphoma and central nervous system involvement. Haematologica. 2018;103(2):e92–e93. doi:10.3324/haematol.2017.181636
103. Li L, Yang W, Ye R, et al. Combination of Selinexor with BTK Inhibitor for Central Nervous System Diffuse Large B-Cell Lymphoma, Possible Mechanisms and Therapeutic Potential Exploration [abstract]. Blood. 2023;142(Suppl 1):3010. doi:10.1182/blood-2023-184371
104. Zheng X, Wang C, Chen F, et al. Zanubrutinib delays selinexor resistance evolution in biopsy sample-derived primary central nervous system lymphoma models. iScience. 2024;27(5):109799. doi:10.1016/j.isci.2024.109799
105. Chapuy B, Roemer MG, Stewart C, et al. Targetable genetic features of primary testicular and primary central nervous system lymphomas. Blood. 2016;127(7):869–881. doi:10.1182/blood-2015-10-673236
106. Berghoff AS, Ricken G, Widhalm G, et al. PD1 (CD279) and PD-L1 (CD274, B7H1) expression in primary central nervous system lymphomas (PCNSL). Clin Neuropathol. 2014;33(1):42–49. doi:10.5414/NP300698
107. Furuse M, Kuwabara H, Ikeda N, et al. PD-L1 and PD-L2 expression in the tumor microenvironment including peritumoral tissue in primary central nervous system lymphoma. BMC Cancer. 2020;20(1):277. doi:10.1186/s12885-020-06755-y
108. Lebrun L, Allard-Demoustiez S, Salmon I. Pathology and new insights in central nervous system lymphomas. Curr Opin Oncol. 2023;35(5):347–356. doi:10.1097/CCO.0000000000000978
109. Nam SJ, Kim S, Kwon D, et al. Prognostic implications of tumor-infiltrating macrophages, M2 macrophages, regulatory T-cells, and indoleamine 2, 3-dioxygenase-positive cells in primary diffuse large B-cell lymphoma of the central nervous system. Oncoimmunol. 2018;7(7):e1442164. doi:10.1080/2162402X.2018.1442164
110. Zhang H, Liu L, Liu J, et al. Roles of tumor-associated macrophages in anti-PD-1/PD-L1 immunotherapy for solid cancers. Molec Cancer. 2023;22(1):58. doi:10.1186/s12943-023-01725-x
111. Xiang X, Wang J, Lu D, Xu X. Targeting tumor-associated macrophages to synergize tumor immunotherapy. Signal Transduct Target Ther. 2021;6(1):75. doi:10.1038/s41392-021-00484-9
112. Pages-Geli C, Medina D, Hernandez C, et al. Macrophages Play a Key Role in Controlling Tumor Growth and Response to Immunotherapy in Primary Central Nervous System Lymphoma. Blood. 2023;142:1642. doi:10.1182/blood-2023-180719
113. Gavrilenko AN, Volkov NP, Shmidt DI, et al. Nivolumab in Primary CNS Lymphoma and Primary Testicular Lymphoma with CNS Involvement: single Center Experience [abstract]. Blood. 2020;136(Suppl 1):4. doi:10.1182/blood-2020-138924
114. Hoang-Xuan K, Houot R, Soussain C, et al. First Results of the Acsé Pembrolizumab Phase II in the Primary CNS Lymphoma (PCNSL) Cohort. Blood. 2020;136(Suppl 1):15–16. doi:10.1182/blood-2020-141773
115. Wagner DL, Fritsche E, Pulsipher MA, et al. Immunogenicity of CAR T Cells in Cancer Therapy. Nat Rev Clin Oncol. 2021;18(6):379–393. doi:10.1038/s41571-021-00476-2
116. Al-Juhaishi T, Ahmed S, Al-Juhaishi T. Selecting the Optimal CAR-T for the treatment of B-Cell Malignancies. Curr Hematol Malig Rep. 2021;16(1):32–39. doi:10.1007/s11899-021-00615-7
117. Siddiqi T, Wang X, Blanchard MS, et al. CD19-directed CAR T-cell therapy for treatment of primary CNS lymphoma. Blood Adv. 2021;5(20):4059–4063. doi:10.1182/bloodadvances.2020004106
118. Karschnia P, Rejeski K, Winkelmann M, et al. Toxicities and Response Rates of Secondary CNS Lymphoma After Adoptive Immunotherapy With CD19-Directed Chimeric Antigen Receptor T Cells. Neurology. 2022;98(21):884–889. doi:10.1212/WNL.0000000000200608
119. Alame M, Cornillot E, Cacheux V, et al. The immune contexture of primary central nervous system diffuse large B cell lymphoma associates with patient survival and specific cell signaling. Theranostics. 2021;11(8):3565–3579. doi:10.7150/thno.54343
120. Frigault MJ, Dietrich J, Gallagher K, et al. Safety and efficacy of tisagenlecleucel in primary CNS lymphoma: a phase 1/2 clinical trial. Blood. 2022;139(15):2306–2315. doi:10.1182/blood.2021014738
121. Choquet S, Soussain C, Azar N, et al. CAR T-cell therapy induces a high rate of prolonged remission in relapsed primary CNS lymphoma: real-life results of the LOC network. Am J Hematol. 2024;99(7):1240–1249. doi:10.1002/ajh.27316
122. Mercadal S, Ahn KW, Allbee-Johnson M, et al. Outcomes of patients with primary central nervous system lymphoma following CD19-targeted chimeric antigen receptor T-cell therapy. Haematologica. 2024;110(1):218.
123. Liu R, Cheng Q, Kang L, et al. CD19 or CD20 CAR T Cell Therapy Demonstrates Durable Antitumor Efficacy in Patients with Central Nervous System Lymphoma. Hum Gene Ther. 2022;33(5–6):318–329. doi:10.1089/hum.2021.249
124. Citterio G, Reni M, Gatta G, Ferreri AJ. Primary central nervous system lymphoma. Crit Rev Oncol Hematol. 2017;113:97–110. doi:10.1016/j.critrevonc.2017.03.019
125. Schaff LR, Grommes C. Primary central nervous system lymphoma. Blood. 2022;140(9):971–979. doi:10.1182/blood.2020008377
126. Chojak R, Koźba-Gosztyła M, Polańska K, et al. Surgical resection versus biopsy in the treatment of primary central nervous system lymphoma: a systematic review and meta-analysis. J Neurooncol. 2022;160(3):753–761. doi:10.1007/s11060-022-04200-7
127. Li G, Hou X, Fu Y, et al. Association between surgery and increased survival in primary central nervous system lymphoma: a retrospective cohort study. Sci Rep. 2025;15(1):3816. doi:10.1038/s41598-025-88351-3
128. Lee C, Byeon Y, Kim GJ, et al. Assessing the effect of cytoreduction on solitary, resectable lesions in primary central nervous system lymphoma. Cancers. 2025;17(6):917. doi:10.3390/cancers17060917
129. Schellekes N, Barbotti A, Abramov Y, et al. Resection of primary central nervous system lymphoma: impact of patient selection on overall survival. J Neurosurg. 2021;135(4):1016–1025. doi:10.3171/2020.9.JNS201980
130. Alzahrani N. The effect of hospitalization on patients’ emotional and psychological well-being among adult patients: an integrative review. Appl Nurs Res. 2021;61:151488. doi:10.1016/j.apnr.2021.151488
131. Yonezawa H, Narita Y, Nagane M, et al. Three-year follow-up analysis of phase 1/2 study on tirabrutinib in patients with relapsed or refractory primary central nervous system lymphoma. Neurooncol Adv. 2024;6(1):vdae037. doi:10.1093/noajnl/vdae037
132. Wang N, Chen FL, Pan L, et al. Clinical outcomes of newly diagnosed primary central nervous system lymphoma treated with zanubrutinib-based combination therapy. World J Clin Oncol. 2023;14(12):606–619. doi:10.5306/wjco.v14.i12.606
133. Vu K, Rubenstein J, Mannis GN, et al. Low-Dose Lenalidomide Maintenance after Induction Therapy in Older Patients with Primary CNS Lymphoma. Br J Haematol. 2019;186(1):180–183. doi:10.1111/bjh.15787
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.