Back to Journals » Clinical and Experimental Gastroenterology » Volume 13
Novel Therapeutic Options for People with Ulcerative Colitis: An Update on Recent Developments with Janus Kinase (JAK) Inhibitors
Authors Troncone E, Marafini I, Del Vecchio Blanco G ![]() , Di Grazia A, Monteleone G
, Di Grazia A, Monteleone G ![]()
Received 29 January 2020
Accepted for publication 13 April 2020
Published 5 May 2020 Volume 2020:13 Pages 131—139
DOI https://doi.org/10.2147/CEG.S208020
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Andreas M. Kaiser
Edoardo Troncone, Irene Marafini, Giovanna Del Vecchio Blanco, Antonio Di Grazia, Giovanni Monteleone
Department of Systems Medicine, University of Rome “Tor Vergata”, Rome, Italy
Correspondence: Giovanni Monteleone
Dipartimento di Medicina dei Sistemi, Università di Roma “Tor Vergata”, Via Montpellier, 1, Rome 00133, Italy
Tel +390620903702
Fax +390672596391
Email [email protected]
Abstract: Crohn’s disease (CD) and ulcerative colitis (UC), the main forms of inflammatory bowel disease (IBD) in human beings, are chronic relapsing-remitting disorders of the gastrointestinal tract, which usually require lifelong therapies. For many years, IBD have been managed with corticosteroids, aminosalicylates and immunosuppressants (ie, thiopurines). The advent of biologic therapies (anti-TNF-α agents) has significantly improved the outcome of IBD patients in terms of prolonged clinical remission, corticosteroid sparing, achievement of mucosal healing and prevention of disease-related complications. Nevertheless, primary failure or loss of response to biologics occur in about 50% of patients treated with these drugs. Therefore, the need for new effective treatments for such patients has critically emerged as an urgent priority. With this regard, several small-molecule drugs (SMDs) targeting lymphocyte trafficking (ie, sphingosine-1-phosphate receptor modulators) and the JAK/STAT pathway (eg, tofacitinib) have been recently developed and tested in IBD. In particular, JAK inhibitors are oral compounds characterized by short half-life, low antigenicity and the ability to dampen several pro-inflammatory pathways simultaneously. Tofacitinib, a pan-JAK inhibitor, has shown good efficacy and safety in UC clinical trials and has been recently approved for the treatment of UC patients. In this review, we analyze the main evidence supporting the use of JAK inhibitors in UC and explore the unanswered questions about the use of this class of drug in UC.
Keywords: inflammatory bowel disease, tofacitinib, JAK/STAT pathway, small molecule drugs
Introduction
Inflammatory bowel diseases (IBD), which encompass Crohn’s disease (CD) and ulcerative colitis (UC), are inflammatory disorders of the gastrointestinal (GI) tract characterized by a chronic relapsing course and variable degrees of intestinal injury.1,2 The cause of such diseases is still unknown, but it has been hypothesized that the pathological process leading to gut damage is driven by an excessive inflammatory response against antigens of the luminal flora triggered by several environmental factors and occurring in genetically predisposed individuals.3,4 Despite sharing the generic definition of IBD, CD and UC are two distinct diseases, with important differences in immunological features, clinical presentation and disease course and, for these reasons, may require different therapeutic approaches. CD can affect the whole alimentary tract from the mouth to the anus, frequently presents with abdominal pain, diarrhea, fever or weight loss and can associate with the development of local complications such as bowel strictures, abscesses or fistulas.2 UC is an inflammatory disorder of the colonic mucosa, which starts from the rectum and can extend proximally in a continuous manner and is characterized clinically by bloody diarrhea and abdominal pain.1 Intestinal mucosa of patients with CD and patients with UC is extensively infiltrated with various immune cell populations (eg, T lymphocytes, macrophages), which produce a large amount of pro-inflammatory cytokines that eventually drive mucosal damage.5–21 For many decades, IBD have been managed with corticosteroids, 5-aminosalicylates and immunosuppressants (ie, thiopurines).22 Afterward, an increasingly understanding of the molecular mechanisms underlying the pathogenesis of IBD has progressively enriched the “conventional” therapeutic armamentarium with biological therapies, namely monoclonal antibodies targeting specific mediators involved in inflammation.23 The main representative molecules of such class are TNF-α blockers (ie, infliximab, adalimumab, certolizumab pegol, golimumab), which have been used in the last 20 years with good results for both CD and UC.24 Despite the encouraging data on clinical efficacy and mucosal healing, TNF-α antagonists are ineffective in up one-third of patients, while another third experiences loss of response after initial benefit.25–27 Furthermore, concerns about the risk of serious infections during anti-TNF-α therapies have been raised.28,29 These observations have stressed the need for new therapeutic compounds, ideally able to modulate different inflammatory pathways with good safety profile, compliance and cost-effectiveness. Consistently, new biologics have become recently available, such as anti-integrins (ie, vedolizumab) and new anti-cytokines (ie ustekinumab), while many others are under investigation.30–33
Small-molecule drugs (SMDs) represent one of the most interesting novelties in the IBD therapeutic pipeline. The main advantages of SMD over biologics rely on the short half-life, the lower risk of immunogenicity and the oral administration, which could positively affect patients’ compliance and quality of life.34 SMD targeting Janus kinase (JAK) signaling and sphingosine-1-phosphate (S1P) receptor and have been tested in IBD, and tofacitinib, a pan-JAK inhibitor, has been recently approved for UC treatment.35,36
In this review, we summarize the main evidence supporting the use of JAK inhibitors in UC and discuss the more recent clinical findings on efficacy and safety of this class of drugs.
JAK/STAT Molecules
Cytokines are soluble low-molecular-weight proteins or glycoproteins involved in the regulation of several biological activities in the immune system.37 They usually exert their biological functions through interaction with transmembrane receptors and subsequent activation of JAK and signal transducers and activators of transcription (STAT). The JAK family includes the following 4 intracellular kinases: JAK1, JAK2, JAK3 and tyrosine kinase (TYK)2.38 JAK family members associate with the intracellular domain of cytokine receptors as homodimers or heterodimers, thus combining in multiple possible associations. Following the activation, these kinases undergo dimerization and subsequent trans/auto-phosphorylation on tyrosine residues. Activation of JAK members determines, in turn, the recruitment and phosphorylation of STAT proteins (ie, STAT1, STAT2, STAT3, STAT4, STAT5 and STAT6), that finally translocate into the nucleus to regulate the transcription of several genes.38–40
The demonstration that JAK molecules mediate the activity of many inflammatory cytokines led to the development of JAK inhibitors, whose use would offer the advantage to inhibit simultaneously multiple and distinct pathways involved in the IBD-associated tissue damage.
For a detailed description of the role of each cytokine and mediator involved in either the amplification or attenuation of the IBD-associated detrimental immune response, the reader is direct toward recent reviews.37,41,42
Tofacitinib in Ulcerative Colitis: Results from Clinical Trials and Real-World Studies
Tofacitinib is a JAK inhibitor currently approved by Food and Drug Administration (FDA) and the European Medicines Agency (EMA) for the treatment of UC patients with inadequate/loss of response or intolerance to either conventional therapy or biologics.36 The compound is an oral small molecule with a 3 h half-life, originally developed as a selective inhibitor of JAK3, but subsequently defined as a pan-JAK inhibitor due to an additional binding affinity for JAK1 and, to a lesser extent, for JAK2.43 In 2012, a double-blind, randomized, placebo-controlled dose-finding Phase 2 trial evaluated the efficacy of tofacitinib in moderate-to-severe UC patients.44 One hundred ninety-four patients were randomized to tofacitinib 0.5 mg, 3 mg, 10 mg, or 15 mg or placebo twice daily for 8 weeks. The main outcomes were defined by clinical and endoscopic scoring system. The Mayo scoring system is a commonly used clinical score which ranges from 0 to 12 (higher scores indicate more severe disease) and is composed of four sub-scores for stool frequency, rectal bleeding, endoscopic findings, and Physician’s Global Assessment (each score can range from 0 to 3).45 Patients with a Mayo score ranging from 6 to 12, and an endoscopic sub-score of 2 or 3 were enrolled. The primary endpoint was clinical response at 8 weeks, defined as an absolute decrease from baseline in the Mayo score of 3 or more points. The improving of clinical score had to be accompanied by a decrease in the rectal bleeding sub-score of 1 point or more or absolute rectal bleeding sub-score of 0 or 1. Secondary endpoints were clinical remission, endoscopic response and endoscopic remission at week 8. Clinical response at 8 weeks occurred in 32% (10/31), 48% (16/33), 61% (20/33) and 78% (38/49) of patients receiving 0.5 mg, 3 mg, 10 mg and 15 mg of tofacitinib, respectively, compared to 42% (20/48) of patients receiving placebo, with a significant difference between tofacitinib 15 mg group and placebo group (95% CI, 66 to 89). Moreover, 10 mg and 15 mg groups showed a significantly higher rate of clinical remission (48% and 41%, respectively) and endoscopic remission (30% and 27%, respectively) compared to placebo (10% and 2%, respectively). The efficacy of tofacitinib in UC patients was subsequently confirmed in three Phase 3, randomized, double-blind, placebo-controlled trials: the OCTAVE Induction 1 and 2 trials and the OCTAVE Sustain trial.36 In the OCTAVE Induction 1, 122 patients with moderate-to-severe UC were randomized to receive placebo and 476 to receive tofacitinib at a dose of 10 mg twice daily. In OCTAVE Induction 2, 112 patients were randomized to receive placebo and 429 to receive tofacitinib at a dose of 10 mg twice daily. Inclusion criteria were similar to those of the phase 2 trial, and the trials included also patients who had failed anti-TNF-α therapies.36,44 The primary endpoint of the induction studies was remission, defined as a total Mayo score of ≤2, with no subscore >1 and a rectal bleeding sub-score of 0 at 8 weeks. Mucosal healing (Mayo endoscopic subscore of ≤1) at 8 weeks was one of the main secondary endpoints. The primary endpoint occurred in 18.5% of the patients (88/476) in the 10 mg tofacitinib group compared to 8.2% (10/122) in the placebo group in induction 1, and 16.6% of the patients (71/429) in the 10 mg tofacitinib group compared to 3.6% (4/112) in the placebo group in induction 2. Interestingly, tofacitinib was also effective in patients who had previously failed anti-TNF-α treatments. Moreover, mucosal healing at 8 weeks occurred in 31.3% and 28.4% of the patients in 10 mg tofacitinib group compared to 15.6% and 11.6% in the placebo group. In the OCTAVE Sustain trial, 593 patients who had a clinical response to induction therapy were randomized to placebo (198), tofacitinib 5 mg twice daily (198) or tofacitinib 10 mg twice daily (197).36 This was the first trial investigating the efficacy of tofacitinib in UC patients on a long-term period and evaluated remission rate at 52 weeks as the primary endpoint. After 52 weeks, 34.3% of the patients (68/198) in the 5 mg tofacitinib group and 40.6% (80/197) in the 10 mg tofacitinib group were in remission, compared with 11.1% (22/198) in the placebo group. Furthermore, mucosal healing occurred in significantly more patients in tofacitinib groups (37.4% and 45.7% in the 5 mg and 10 mg, respectively), compared to the placebo group (13.1%). Of note, a post-hoc analysis of the phase 3 studies showed that patients in tofacitinib groups had significant reductions from baseline in stool frequency sub-score and rectal bleeding sub-score compared to placebo starting from the third day of treatment.46 Results from phase 3 trials are summarized in Table 1. Based on the results from OCTAVE Induction 1 and 2 and OCTAVE Sustain, EMA recommends tofacitinib at the dose of 10 mg twice a day for the first 8 weeks and then 5 mg twice a week in patients with UC after failure or intolerance to conventional treatments.47 The effects of tofacitinib on health-related quality of life (HRQoL) have been evaluated using the disease-specific Inflammatory Bowel Disease Questionnaire (IBDQ) and the general Short Form-36v2® Health Survey (SF-36v2) in OCTAVE Induction 1 and 2 trial and OCTAVE Sustain trial.48 Mean changes from a baseline score of IBDQ and SF-36v2 Physical and Mental Component Summaries (PCS/MCS) were greater with tofacitinib 10 mg compared to placebo at week 8 in both induction trials. Furthermore, changes in IBDQ and SF-36v2 PCS/MCS were maintained at week 52 with both tofacitinib dosages in OCTAVE Sustain trial.48 Recently, Weisshof et al reported a real-life experience of tofacitinib in a retrospective study including 58 IBD patients (53 UC, 4 CD and 1 pouchitis).49 Notably, 93% of patients had previously failed anti-TNF-α treatments, thus representing a “difficult” IBD sub-population. Twenty-one patients (36%) achieved a clinical response and 19 (33%) achieved clinical remission. Of the 48 patients followed until week 26, 13 (27%) and 12 (25%) achieved clinical response or clinical remission, respectively. At week 52, 7 out of the remaining 26 patients (27%) were in clinical, steroid-free remission.49 A further real-world study reported the outcome of tofacitinib treatment in 38 UC patients who had previously failed anti-TNF-α and vedolizumab.50 In this cohort of refractory UC patients, survival without colectomy was 70% at week 48, and adverse events (AE) occurred in 14 (37%) patients, including 6 severe AE and an overall infection risk of 23.7% (9/38).
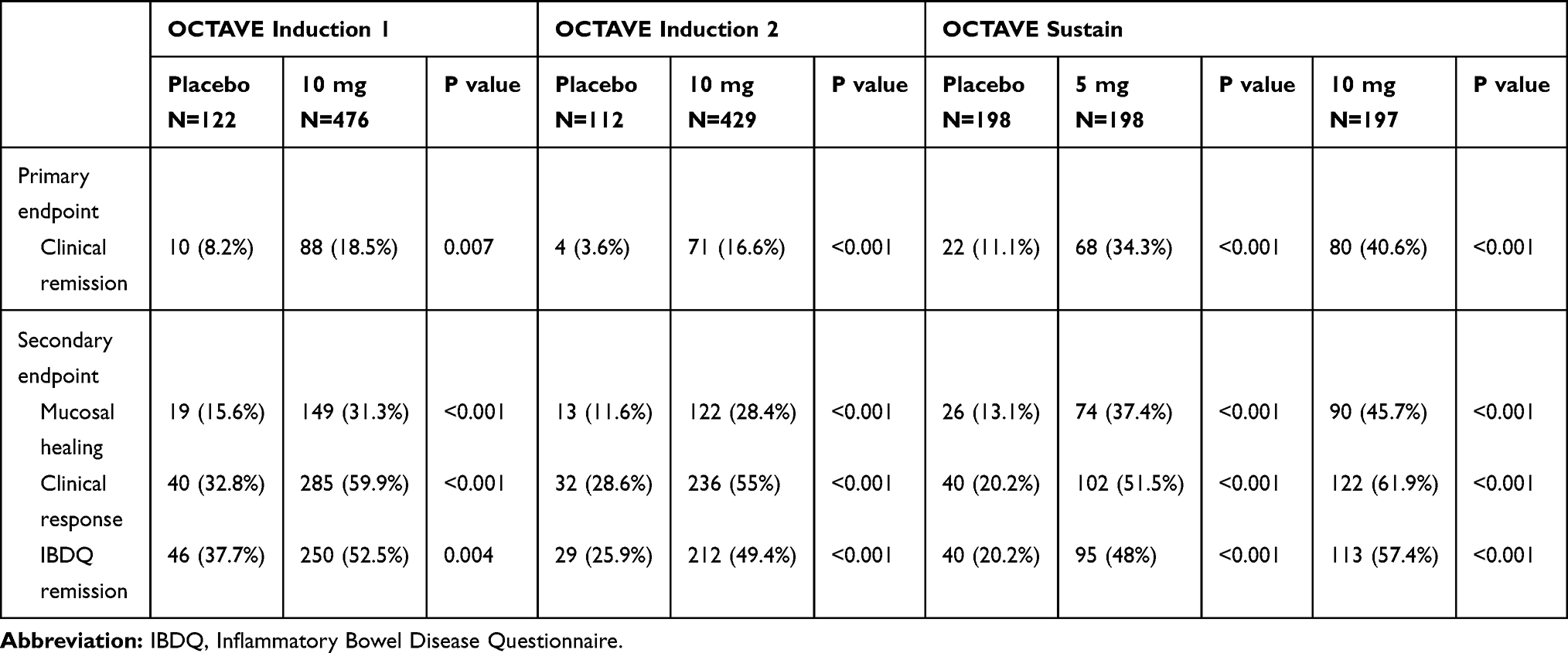 |
Table 1 Main Results from Phase 3 Studies (OCTAVE Induction 1, OCTAVE Induction 2 and OCTAVE Sustain) Evaluating Tofacitinib in Moderate-to-Severe Ulcerative Colitis (Ref 36). For Induction Trials, Endpoints Were Evaluated at 8 Weeks; for Sustain Trial, Endpoints Were Evaluated at 52 Weeks |
A recent open-label, long-term extension study of the OCTAVE trials (OCTAVE open) evaluated the efficacy and safety of tofacitinib dose escalation or de-escalation in patients receiving 5 mg or 10 mg twice daily after 52 weeks.51 Sixty-six patients receiving maintenance therapy with tofacitinib 10 mg twice daily who were in remission at week 52 underwent de-escalation at 5 mg (de-escalation group), while 57 patients who experienced an UC flare during maintenance therapy with 5 mg twice daily underwent escalation to 10 mg twice daily (escalation group). After tofacitinib de-escalation, 74.6% (47/63) maintained remission after 12 months, while after dose escalation, 35.1% (20/57) and 49.1% (28/57) were in remission at months 2 and 12, respectively.51 Although the study design and the small sample size could limit the clinical significance of these findings, this study highlights a high rate of efficacy after tofacitinib dose modulating, which could be explained with the low immunogenicity of such small molecule compared to biologics. Larger studies and longer follow-up are needed to further address this point.
Tofacitinib in Ulcerative Colitis: Safety
Given the possible wide effects on immune system and hematopoiesis secondary to JAK inhibition, great attention has been paid to the safety profile of tofacitinib since its introduction in clinical practice for immune-related disorders. Indeed, tofacitinib has been associated with an increased risk of infections, including herpes zoster, in patients with rheumatoid arthritis or psoriasis.52–55 Tofacitinib has shown an overall good safety profile in UC patients. In the phase 2 trial, few cases of influenza and nasopharyngitis were reported in both tofacitinib and placebo groups, while two cases of severe infections (one postoperative abscess and one anal abscess) were documented in patients receiving tofacitinib 10 mg.44 Mild hematological side effects were reported in 3 patients receiving tofacitinib 10 mg and 15 mg, who presented an absolute neutrophil count less than 1500 cells per cubic millimeter. Moreover, there was a dose-dependent increase in both LDL and HDL cholesterol concentrations in tofacitinib groups, which reversed after discontinuation of the study drug.44 In OCTAVE Induction 1 and 2 and OCTAVE Sustain, the rates of AE and serious AE were similar between tofacitinib groups and placebo group.36 However, in the OCTAVE Induction 1 and 2 trials, the rate of infections of any severity was higher in the 10 mg groups (23.3% and 18.2%, respectively) as compared to the placebo groups (15.6% and 15.2%). Similarly, in the OCTAVE Sustain trial, infections occurred more frequently in 5 mg and 10 mg tofacitinib groups (35.9% and 39.8%) compared to the placebo group (24.2%). Most infections were mild or moderate in severity. On the other hand, 7 patients in Induction 1 and 2 and 3 patients in OCTAVE Sustain developed serious infections, compared to only 2 serious infections in the placebo group of the Sustain trial.36 In particular, 19 cases of herpes zoster infection were reported in treatment groups among the three phase 3 trials, compared to one case in the placebo group. Main AE reported in tofacitinib groups during phase 3 trials are summarized in Table 2. All cases of herpes zoster infection in patients treated with tofacitinib have been reviewed in a work from Winthrop et al, which included the cases from the open-label study OCTAVE Open.51,56 The Authors reported 65 cases of herpes zoster infection, with an overall rate of 5.6%. Only one case of encephalitis was described, which resolved upon standard treatment, and five cases (7.7%) led to treatment discontinuation. Interestingly, multivariate analysis identified older age and prior anti-TNF-α failure as independent risk factors.56 The inhibition of interferon signaling secondary to JAK/STAT blocking may explain such an increased risk.
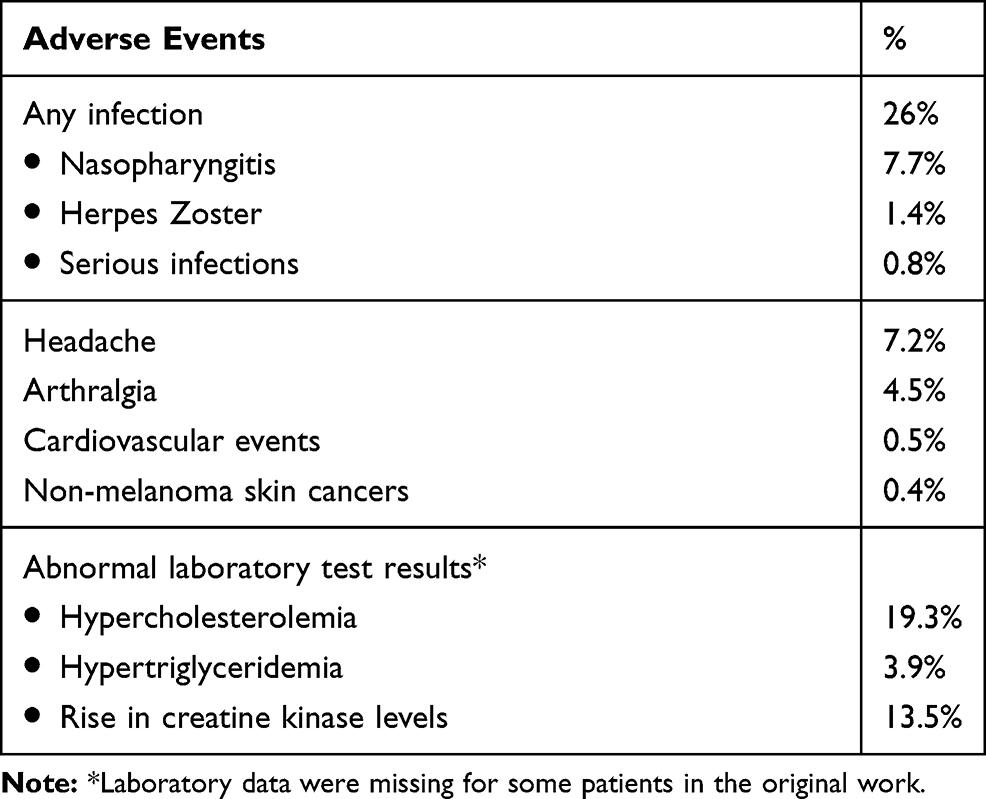 |
Table 2 Main Adverse Events Reported in Tofacitinib Groups During Phase 3 Trials (Ref 36) |
Currently, few data are available on the risk of pulmonary embolism and deep vein thrombosis in UC patients receiving tofacitinib; in particular, 5 cases were documented in OCTAVE Open cohort.57 Consistent with data emerging from the use of tofacitinib in other diseases, more cases of non-melanoma skin cancer occurred with tofacitinib as compared to placebo across the phase 3 UC trials. Moreover, six cardiovascular events occurred in the tofacitinib groups compared to no cases with placebo. This is of particular interest, considering the well-described effects of tofacitinib on the lipid profile.58 Nevertheless, evaluation of safety profile about the risk of malignancies or cardiovascular events needs a long observation time, and usually comes from post-marketing observational studies. With this regard, great help comes from the longer experience of tofacitinib (and other JAK inhibitors) in different immune-related diseases. A recent systematic review and meta-analysis from Olivera et al analyzed 82 studies comprising 66,159 patients with IBD or other immune-mediated diseases who were exposed to a JAK inhibitor.59 The authors reported an incidence rate of AEs of 42.65 per 100 person-years and of serious AEs of 9.88 per 100 person-years. Incidence rates of serious infections, herpes zoster infection, malignancy, and major cardiovascular events were 2.81 per 100 person-years, 2.67 per 100 person-years, 0.89 per 100 person-years and 0.48 per 100 person-years, respectively. However, only herpes zoster infection risk was significantly higher among patients who received JAK inhibitors.59 Pregnancies with maternal or paternal exposure to tofacitinib have been reported in UC studies, with overall 11 cases of maternal exposure and 14 cases of paternal exposure.60 Outcomes included 15 healthy newborns, 2 spontaneous abortions and 2 medical terminations, with no cases of fetal/neonatal deaths or congenital malformations. Although limited by the very small sample size, the available data suggest that prenatal exposure to tofacitinib in UC studies is similar to that reported for other tofacitinib indications and general population.60
Other JAK Inhibitors in Ulcerative Colitis
A more selective JAK inhibitor could ideally improve the safety profile and clinical efficacy. Taking advantage from the experience of multiple JAK inhibitors available for other immune-related disease, several new compounds are being tested in UC and CD.61 Peficitinib is an oral JAK inhibitor, which showed a moderate selectivity for JAK3 over JAK1, JAK2, and TYK2 in in vitro studies.62 Efficacy and safety of peficitinib in UC patients were investigated in a Phase 2b dose-ranging trial.63 Two hundred and nineteen patients with moderate-to-severe UC were randomized to 25 mg once daily (OD), 75 mg OD, 150 mg OD, 75 mg twice daily or placebo, and the primary outcome was peficitinib dose-response after 8 weeks. Secondary endpoints included clinical response, clinical remission and mucosal healing. Although a statistically significant peficitinib dose-response was not demonstrated, a higher rate of patients receiving peficitinib ≥75 mg OD achieved clinical response, remission and mucosal healing. Moreover, such an improvement was accompanied by IBDQ improvement and inflammatory biomarker normalization. The AE rate was higher in the peficitinib group compared to placebo.63
Upadacitinib is a selective JAK1 inhibitor, which has been tested in a phase 2 double-blind placebo-controlled dose-ranging randomized trial in moderate-to-severe refractory UC patients (U-ACHIEVE trial; NCT02819635). Two hundred and fifty UC patients were randomized to upadacitinib 7.5 mg (47), 15 mg (49), 30 mg (52), 45 mg (56) or placebo (46). The primary endpoint (ie, clinical remission) was met for doses of 15 mg or higher. Moreover, histologic improvement or remission were more frequent in upadacitinib-treated patients compared to placebo.64,65
Filgotinib, a selective JAK1 inhibitor, is under investigation in a phase 2b/3 in patients with moderate-to-severe UC (NCT02914522). Currently, several other selective JAK1 inhibitors, such as SHR0302 and itacitinib (NCT03675477; NCT03627052), TYK2 inhibitor, such as BMS-986165 (NCT03934216) or gut-selective pan-JAK inhibitors such as TD-1473 (NCT03635112) are under investigation, and many others are being developed by the industries.61 Excluding peficitinib, no complete publications of clinical data are currently available for the other compounds.64
Conclusions
Over the last two decades, CD and UC have been predominantly managed with “conventional” therapies and anti-TNF-α antibodies. More recently, the therapeutic armamentarium of these pathologies has been enriched by the availability of new biologics and several new SMD, which are expanding the possibilities for clinicians to manage IBD patients. In this scenario, JAK inhibitors probably represent the most promising drugs, since tofacitinib has been already approved for UC patients and several other compounds are under investigation for both UC and CD. Data from phase 3 studies are encouraging, but many issues are still unresolved. Firstly, the appearance of a new effective class of drugs raises the question about the most appropriate location in the therapeutic algorithm. Head-to-head trial would be the best strategy to compare directly two treatments, but they are very difficult and expensive to organize, due to the very large sample size needed. Therefore, in most cases, data come from clinical practice and network meta-analysis. Singh et al conducted a systematic review with network meta-analysis aimed at investigating which treatment among anti-TNF-α agents, anti-integrins (ie, vedolizumab) and JAK inhibitors performed better as first-line or second-line (that is after anti-TNF-α failure) treatment in moderate-to-severe UC patients.66 Analysis of 12 randomized controlled clinical trials including 2720 biologic-naïve patients reported that infliximab and vedolizumab were ranked highest for induction of clinical remission and mucosal healing compared to other anti-TNF-α agents and tofacitinib. Nevertheless, analysis of four randomized controlled clinical trials including 967 patients with prior exposure to anti-TNF-α reported that tofacitinib performed better for induction of clinical remission and mucosal healing compared to the other treatments.66 Therefore, these findings propose tofacitinib as the treatment of choice for the challenging class of patients with previous biologic failure. Future researches will address the possible role of tofacitinib also in acute severe ulcerative colitis.
Cost-effectiveness analysis represents another major issue when considering the appropriate place in the therapeutic algorithm of such new molecules. Chemical synthesis of SMD is simpler than biologics' synthesis, and the oral administration avoids the need for outpatient visits and dedicated staff related to drug parenteral administration. Thus, a treatment based on SMD could be theoretically cheaper compared to biologics, even though the recent advent of biosimilars makes the difference of the costs less relevant.67 Studies aimed at investigating the cost-effectiveness of JAK inhibitors in UC are still lacking, and the question remains unanswered.
Drug safety is another crucial point, which must be carefully assessed in future studies. Like many other drugs acting as immunomodulators, tofacitinib can increase the risk of infections. Most infectious AE reported in clinical trials were mild, but the risk of more severe events after prolonged therapies or in specific subsets of patients is still unknown. Moreover, a higher risk of herpes zoster infection has been clearly highlighted, and the safety and efficacy of specific vaccine will have to be investigated in UC patients receiving tofacitinib.68–70 Recently, FDA and EMA issued an alert about the risk of thrombotic and thromboembolic AE in patients receiving tofacitinib 10 mg twice a day.71,72 Whereas further studies are needed to understand the mechanisms and the magnitude of such a risk, it is recognized that JAK2 inhibition could cause hematological side effects due to the various roles of this kinase in hematopoiesis.73,74 Moreover, JAK3 inhibition leads potentially to lymphopenia and thus hypothetically to an increased risk of infection.75 Therefore, it has been hypothesized that a more selective JAK inhibition toward a JAK1 preferential inhibition (and maybe in future a selective targeting of specific STAT molecules) could improve safety and efficacy in IBD, even though conclusive evidence is still lacking. Future studies will help address this intriguing hypothesis.
Identification of predictors of response would allow optimizing treatment efficacy, safety and resource allocation through a pre-treatment stratification of patients. In this field, many efforts have been made to identify predictors of response of the currently available biologics. Considering that most of UC patients do not achieve clinical remission with tofacitinib, this topic will be of great interest also for JAK inhibitors in UC.
In conclusion, JAK inhibitors represent one of the most exciting novelties for UC management, and a positive impact for patients suffering from this condition is expected from the upcoming availability of such drugs. Safety improving and patient selection will be the hot topics for future researches.
Disclosure
Prof. Dr. Giovanni Monteleone reports personal fees from Abbvie, outside the submitted work. In addition, Prof. Dr. Giovanni Monteleone has a patent Smad7 Antisense Oligonucleotide licensed. The authors report no other conflicts of interest in this work.
References
1. Ordas I, Eckmann L, Talamini M, et al. Ulcerative colitis. Lancet. 2012;380(9853):1606–1619. doi:10.1016/S0140-6736(12)60150-0
2. Baumgart DC, Sandborn WJ. Crohn’s disease. Lancet. 2012;380(9853):1590–1605. doi:10.1016/S0140-6736(12)60026-9
3. Xavier RJ, Podolsky DK. Unravelling the pathogenesis of inflammatory bowel disease. Nature. 2007;448(7152):427–434. doi:10.1038/nature06005
4. Cho JH. The genetics and immunopathogenesis of inflammatory bowel disease. Nat Rev Immunol. 2008;8(6):458–466. doi:10.1038/nri2340
5. Neurath MF, Weigmann B, Finotto S, et al. The transcription factor T-bet regulates mucosal T cell activation in experimental colitis and crohn’s disease. J Exp Med. 2002;195(9):1129–1143. doi:10.1084/jem.20011956
6. Fuss IJ, Neurath M, Boirivant M, et al. Disparate CD4+ lamina propria (LP) lymphokine secretion profiles in inflammatory bowel disease. Crohn’s disease LP cells manifest increased secretion of IFN-gamma, whereas ulcerative colitis LP cells manifest increased secretion of IL-5. J Immunol. 1996;157(3):1261–1270.
7. Marafini I, Angelucci E, Pallone F, et al. The IL-12/23/STAT axis as a therapeutic target in inflammatory bowel disease: mechanisms and evidence in man. Dig Dis. 2015;33(Suppl 1):113–119. doi:10.1159/000437106
8. Monteleone G, Biancone L, Marasco R, et al. Interleukin 12 is expressed and actively released by crohn’s disease intestinal lamina propria mononuclear cells. Gastroenterology. 1997;112(4):1169–1178. doi:10.1016/S0016-5085(97)70128-8
9. Monteleone G, Parrello T, Luzza F, et al. Response of human intestinal lamina propria T lymphocytes to interleukin 12: additive effects of interleukin 15 and 7. Gut. 1998;43(5):620–628. doi:10.1136/gut.43.5.620
10. Macdonald TT, Monteleone G. Immunity, inflammation, and allergy in the gut. Science. 2005;307(5717):1920–1925. doi:10.1126/science.1106442
11. Fuss IJ, Heller F, Boirivant M, et al. Nonclassical CD1d-restricted NK T cells that produce IL-13 characterize an atypical Th2 response in ulcerative colitis. J Clin Invest. 2004;113(10):1490–1497. doi:10.1172/JCI19836
12. Heller F, Florian P, Bojarski C, et al. Interleukin-13 is the key effector Th2 cytokine in ulcerative colitis that affects epithelial tight junctions, apoptosis, and cell restitution. Gastroenterology. 2005;129(2):550–564. doi:10.1016/j.gastro.2005.05.002
13. Nalleweg N, Chiriac MT, Podstawa E, et al. IL-9 and its receptor are predominantly involved in the pathogenesis of UC. Gut. 2015;64(5):743–755. doi:10.1136/gutjnl-2013-305947
14. Weaver CT, Hatton RD, Mangan PR, et al. IL-17 family cytokines and the expanding diversity of effector T cell lineages. Annu Rev Immunol. 2007;25:821–852. doi:10.1146/annurev.immunol.25.022106.141557
15. Weaver CT, Elson CO, Fouser LA, et al. The Th17 pathway and inflammatory diseases of the intestines, lungs, and skin. Annu Rev Pathol. 2013;8:477–512. doi:10.1146/annurev-pathol-011110-130318
16. Bogaert S, Laukens D, Peeters H, et al. Differential mucosal expression of Th17-related genes between the inflamed colon and ileum of patients with inflammatory bowel disease. BMC Immunol. 2010;11:61. doi:10.1186/1471-2172-11-61
17. Troncone E, Marafini I, Pallone F, et al. Th17 cytokines in inflammatory bowel diseases: discerning the good from the bad. Int Rev Immunol. 2013;32(5–6):526–533. doi:10.3109/08830185.2013.823421
18. Monteleone G, Pallone F, MacDonald TT. Interleukin-21: a critical regulator of the balance between effector and regulatory T-cell responses. Trends Immunol. 2008;29(6):290–294. doi:10.1016/j.it.2008.02.008
19. Fina D, Sarra M, Fantini MC, et al. Regulation of gut inflammation and th17 cell response by interleukin-21. Gastroenterology. 2008;134(4):1038–1048. doi:10.1053/j.gastro.2008.01.041
20. Monteleone G, Monteleone I, Fina D, et al. Interleukin-21 enhances T-helper cell type I signaling and interferon-gamma production in crohn’s disease. Gastroenterology. 2005;128(3):687–694. doi:10.1053/j.gastro.2004.12.042
21. Caruso R, Fina D, Peluso I, et al. A functional role for interleukin-21 in promoting the synthesis of the T-cell chemoattractant, MIP-3alpha, by gut epithelial cells. Gastroenterology. 2007;132(1):166–175. doi:10.1053/j.gastro.2006.09.053
22. Troncone E, Monteleone G. The safety of non-biological treatments in ulcerative colitis. Expert Opin Drug Saf. 2017;16(7):779–789. doi:10.1080/14740338.2017.1340936
23. Harbord M, Eliakim R, Bettenworth D, et al. Third European evidence-based consensus on diagnosis and management of ulcerative colitis. Part 2: current management. J Crohns Colitis. 2017;11(7):769–784.
24. Cote-Daigneault J, Bouin M, Lahaie R, et al. Biologics in inflammatory bowel disease: what are the data? United European Gastroenterol J. 2015;3(5):419–428. doi:10.1177/2050640615590302
25. Gisbert JP, Panes J. Loss of response and requirement of infliximab dose intensification in crohn’s disease: a review. Am J Gastroenterol. 2009;104(3):760–767. doi:10.1038/ajg.2008.88
26. Qiu Y, Chen BL, Mao R, et al. Systematic review with meta-analysis: loss of response and requirement of anti-TNFalpha dose intensification in crohn’s disease. J Gastroenterol. 2017;52(5):535–554. doi:10.1007/s00535-017-1324-3
27. Vermeire S, Gils A, Accossato P, et al. Immunogenicity of biologics in inflammatory bowel disease. Therap Adv Gastroenterol. 2018;11:1756283X17750355. doi:10.1177/1756283X17750355
28. Nyboe Andersen N, Pasternak B, Friis-Moller N, et al. Association between tumour necrosis factor-alpha inhibitors and risk of serious infections in people with inflammatory bowel disease: nationwide Danish cohort study. BMJ. 2015;350:h2809. doi:10.1136/bmj.h2809
29. Biancone L, Annese V, Ardizzone S, et al. Safety of treatments for inflammatory bowel disease: clinical practice guidelines of the Italian Group for the Study of Inflammatory Bowel Disease (IG-IBD). Dig Liver Dis. 2017;49(4):338–358. doi:10.1016/j.dld.2017.01.141
30. Feagan BG, Rutgeerts P, Sands BE, et al. Vedolizumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2013;369(8):699–710. doi:10.1056/NEJMoa1215734
31. Sands BE, Sandborn WJ, Panaccione R, et al. Ustekinumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2019;381(13):1201–1214. doi:10.1056/NEJMoa1900750
32. Feagan BG, Sandborn WJ, Gasink C, et al. Ustekinumab as induction and maintenance therapy for crohn’s disease. N Engl J Med. 2016;375(20):1946–1960. doi:10.1056/NEJMoa1602773
33. Pagnini C, Pizarro TT, Cominelli F. Novel pharmacological therapy in inflammatory bowel diseases: beyond anti-tumor necrosis factor. Front Pharmacol. 2019;10:671. doi:10.3389/fphar.2019.00671
34. Olivera P, Danese S, Peyrin-Biroulet L. Next generation of small molecules in inflammatory bowel disease. Gut. 2017;66(2):199–209. doi:10.1136/gutjnl-2016-312912
35. Sandborn WJ, Feagan BG, Wolf DC, et al. Ozanimod induction and maintenance treatment for ulcerative colitis. N Engl J Med. 2016;374(18):1754–1762.
36. Sandborn WJ, Su C, Sands BE, et al. Tofacitinib as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2017;376(18):1723–1736. doi:10.1056/NEJMoa1606910
37. Bevivino G, Monteleone G. Advances in understanding the role of cytokines in inflammatory bowel disease. Expert Rev Gastroenterol Hepatol. 2018;12(9):907–915. doi:10.1080/17474124.2018.1503053
38. Babon JJ, Lucet IS, Murphy JM, et al. The molecular regulation of Janus kinase (JAK) activation. Biochem J. 2014;462(1):1–13. doi:10.1042/BJ20140712
39. Rawlings JS, Rosler KM, Harrison DA. The JAK/STAT signaling pathway. J Cell Sci. 2004;117(Pt 8):1281–1283. doi:10.1242/jcs.00963
40. Soendergaard C, Bergenheim FH, Bjerrum JT, et al. Targeting JAK-STAT signal transduction in IBD. Pharmacol Ther. 2018;192:100–111. doi:10.1016/j.pharmthera.2018.07.003
41. Marafini I, Sedda S, Dinallo V, et al. Inflammatory cytokines: from discoveries to therapies in IBD. Expert Opin Biol Ther. 2019;19(11):1207–1217. doi:10.1080/14712598.2019.1652267
42. Neurath MF. Cytokines in inflammatory bowel disease. Nat Rev Immunol. 2014;14(5):329–342. doi:10.1038/nri3661
43. Flanagan ME, Blumenkopf TA, Brissette WH, et al. Discovery of CP-690,550: a potent and selective Janus kinase (JAK) inhibitor for the treatment of autoimmune diseases and organ transplant rejection. J Med Chem. 2010;53(24):8468–8484. doi:10.1021/jm1004286
44. Sandborn WJ, Ghosh S, Panes J, et al. Tofacitinib, an oral Janus kinase inhibitor, in active ulcerative colitis. N Engl J Med. 2012;367(7):616–624. doi:10.1056/NEJMoa1112168
45. Schroeder KW, Tremaine WJ, Ilstrup DM. Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis. A randomized study. N Engl J Med. 1987;317(26):1625–1629. doi:10.1056/NEJM198712243172603
46. Hanauer S, Panaccione R, Danese S, et al. Tofacitinib induction therapy reduces symptoms within 3 days for patients with ulcerative colitis. Clin Gastroenterol Hepatol. 2019;17(1):139–147. doi:10.1016/j.cgh.2018.07.009
47. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/xeljanz.
48. Panes J, Vermeire S, Lindsay JO, et al. Tofacitinib in patients with ulcerative colitis: health-related quality of life in phase 3 randomised controlled induction and maintenance studies. J Crohns Colitis. 2018;12(2):145–156. doi:10.1093/ecco-jcc/jjx133
49. Weisshof R, Aharoni Golan M, Sossenheimer PH, et al. Real-world experience with tofacitinib in IBD at a tertiary center. Dig Dis Sci. 2019;64(7):1945–1951. doi:10.1007/s10620-019-05492-y
50. Lair-Mehiri L, Stefanescu C, Vaysse T, et al. Real-world evidence of tofacitinib effectiveness and safety in patients with refractory ulcerative colitis. Dig Liver Dis. 2020;52(3):268–273.
51. Sands BE, Armuzzi A, Marshall JK, et al. Efficacy and safety of tofacitinib dose de-escalation and dose escalation for patients with ulcerative colitis: results from OCTAVE open. Aliment Pharmacol Ther. 2020;51(2):271–280. doi:10.1111/apt.15555
52. Wollenhaupt J, Silverfield J, Lee EB, et al. Safety and efficacy of tofacitinib, an oral janus kinase inhibitor, for the treatment of rheumatoid arthritis in open-label, longterm extension studies. J Rheumatol. 2014;41(5):837–852. doi:10.3899/jrheum.130683
53. Yamanaka H, Tanaka Y, Takeuchi T, et al. Tofacitinib, an oral Janus kinase inhibitor, as monotherapy or with background methotrexate, in Japanese patients with rheumatoid arthritis: an open-label, long-term extension study. Arthritis Res Ther. 2016;18:34. doi:10.1186/s13075-016-0932-2
54. Bissonnette R, Iversen L, Sofen H, et al. Tofacitinib withdrawal and retreatment in moderate-to-severe chronic plaque psoriasis: a randomized controlled trial. Br J Dermatol. 2015;172(5):1395–1406. doi:10.1111/bjd.13551
55. Bachelez H, van de Kerkhof PC, Strohal R, et al. Tofacitinib versus etanercept or placebo in moderate-to-severe chronic plaque psoriasis: a phase 3 randomised non-inferiority trial. Lancet. 2015;386(9993):552–561. doi:10.1016/S0140-6736(14)62113-9
56. Winthrop KL, Melmed GY, Vermeire S, et al. Herpes zoster infection in patients with ulcerative colitis receiving tofacitinib. Inflamm Bowel Dis. 2018;24(10):2258–2265. doi:10.1093/ibd/izy131
57. Sandborn WJ, Panes J, Sands BE, et al. Venous thromboembolic events in the tofacitinib ulcerative colitis clinical development programme. Aliment Pharmacol Ther. 2019;50(10):1068–1076. doi:10.1111/apt.15514
58. Sands BE, Taub PR, Armuzzi A, et al. Tofacitinib treatment is associated with modest and reversible increases in serum lipids in patients with ulcerative colitis. Clin Gastroenterol Hepatol. 2020;18(1):123–32 e3. doi:10.1016/j.cgh.2019.04.059
59. Olivera P, Lasa J, Bonovas S, et al. Safety of Janus kinase inhibitors in patients with inflammatory bowel diseases or other immune-mediated diseases: a systematic review and meta-analysis. Gastroenterology. 2020. doi:10.1053/j.gastro.2020.01.001
60. Mahadevan U, Dubinsky MC, Su C, et al. Outcomes of pregnancies with maternal/paternal exposure in the tofacitinib safety databases for ulcerative colitis. Inflamm Bowel Dis. 2018;24(12):2494–2500. doi:10.1093/ibd/izy160
61. Ferrante M, Sabino J. Efficacy of anti-JAK inhibitors in ulcerative colitis. J Crohns Colitis. 2019. doi:10.1093/ecco-jcc/jjz202
62. Hamaguchi H, Amano Y, Moritomo A, et al. Discovery and structural characterization of peficitinib (ASP015K) as a novel and potent JAK inhibitor. Bioorg Med Chem. 2018;26(18):4971–4983. doi:10.1016/j.bmc.2018.08.005
63. Sands BE, Sandborn WJ, Feagan BG, et al. Peficitinib, an oral Janus kinase inhibitor, in moderate-to-severe ulcerative colitis: results from a randomised, phase 2 study. J Crohns Colitis. 2018;12(10):1158–1169. doi:10.1093/ecco-jcc/jjy085
64. Ma C, Lee JK, Mitra AR, et al. Systematic review with meta-analysis: efficacy and safety of oral Janus kinase inhibitors for inflammatory bowel disease. Aliment Pharmacol Ther. 2019;50(1):5–23. doi:10.1111/apt.15297
65. Sandborn WJ, Panés J, Schreiber S, et al. Efficacy and safety of upadacitinib as an induction therapy for patients with moderately-to-severely active ulcerative colitis: data from the phase 2b study U-ACHIEVE.
66. Singh S, Fumery M, Sandborn WJ, et al. Systematic review with network meta-analysis: first- and second-line pharmacotherapy for moderate-severe ulcerative colitis. Aliment Pharmacol Ther. 2018;47(2):162–175. doi:10.1111/apt.14422
67. Fiorino G, Caprioli F, Daperno M, et al. Use of biosimilars in inflammatory bowel disease: a position update of the Italian Group for the Study of Inflammatory Bowel Disease (IG-IBD). Dig Liver Dis. 2019;51(5):632–639. doi:10.1016/j.dld.2019.02.004
68. Cunningham AL, Lal H, Kovac M, et al. Efficacy of the herpes zoster subunit vaccine in adults 70 years of age or older. N Engl J Med. 2016;375(11):1019–1032.
69. Lal H, Cunningham AL, Godeaux O, et al. Efficacy of an adjuvanted herpes zoster subunit vaccine in older adults. N Engl J Med. 2015;372(22):2087–2096. doi:10.1056/NEJMoa1501184
70. Colombel JF. Herpes zoster in patients receiving JAK inhibitors for ulcerative colitis: mechanism, epidemiology, management, and prevention. Inflamm Bowel Dis. 2018;24(10):2173–2182. doi:10.1093/ibd/izy150
71. Available from: https://www.fda.gov/drugs/drug-safety-and-availability/fda-approves-boxed-warning-about-increased-risk-blood-clots-and-death-higher-dose-arthritis-and.
72. Available from: https://www.ema.europa.eu/en/news/ema-confirms-xeljanz-be-used-caution-patients-high-risk-blood-clots.
73. O’Shea JJ, Plenge R. JAK and STAT signaling molecules in immunoregulation and immune-mediated disease. Immunity. 2012;36(4):542–550. doi:10.1016/j.immuni.2012.03.014
74. Meyer SC, Keller MD, Woods BA, et al. Genetic studies reveal an unexpected negative regulatory role for Jak2 in thrombopoiesis. Blood. 2014;124(14):2280–2284.
75. Nosaka T, van Deursen JM, Tripp RA, et al. Defective lymphoid development in mice lacking Jak3. Science. 1995;270(5237):800–802. doi:10.1126/science.270.5237.800
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.