Back to Journals » Clinical Ophthalmology » Volume 19
Novel Needle for Intravitreal Injections Does Not Affect Biological Activity of Anti-VEGF Drugs
Authors Lytvynchuk L ![]() , Nolte KL, Fuezy I, Zhou W, Deissler H
, Nolte KL, Fuezy I, Zhou W, Deissler H ![]() , Deissler HL
, Deissler HL ![]()
Received 31 July 2025
Accepted for publication 18 October 2025
Published 17 November 2025 Volume 2025:19 Pages 4233—4243
DOI https://doi.org/10.2147/OPTH.S557508
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yousef Fouad
Lyubomyr Lytvynchuk,1– 3,* Kai L Nolte,1,* Isabell Fuezy,1 Wen Zhou,1,2 Helmut Deissler,4 Heidrun L Deissler1
1Department of Ophthalmology, Justus Liebig University Giessen, Giessen, Hessen, Germany; 2Department of Ophthalmology, University Hospital Giessen and Marburg GmbH, Campus Giessen, Giessen, Hessen, Germany; 3Karl Landsteiner Institute for Retinal Research and Imaging, Karl Landsteiner Society, Vienna, Vienna, Austria; 4HD/U Giessen, Giessen, Hessen, Germany
*These authors contributed equally to this work
Correspondence: Heidrun L Deissler, Department of Ophthalmology, Justus Liebig University Giessen, Friedrichstrasse 18, Giessen, 35392, Germany, Tel +49 641 985 43825, Fax +49 642 985 43890, Email [email protected]
Purpose: In this in vitro study, we investigated if the biological activity of commonly used VEGF antagonists might be affected by their passage through a newly designed 30 G needle (NDN) for intravitreal injection (IVI). To reduce the risk of intraocular inflammation compared to conventional injection with a standard hypodermic 30 G needle (SHN), the NDN contains an occluded front orifice and a side port for drug delivery, resulting in an altered direction of the injection stream.
Methods: Anti-VEGF drugs, such as ranibizumab, faricimab, and aflibercept, were passed twice through one of the two needle types to imitate IVI. To evaluate the VEGF-A-binding capacity of the un- or pretreated antagonists, VEGF-A165 was incubated with a 1– 10fold molar excess of them for 15 min at 37°C, and unbound VEGF-A was determined by ELISA. As the capture antibody and antagonists bind to the same region of the growth factor, only the non-complexed VEGF-A was measured. Biological activity of pretreated antagonists was studied by assessing their capacity to prevent VEGF-A165-induced impairment of the barrier formed by retinal endothelial cells: VEGF-A165 plus antagonists were added to the cells and, as a measure of permeability, the cell index was continuously monitored by electric cell-substrate impedance measurements for three days.
Results: Only a marginal amount of free VEGF-A, if any, was detected after incubation of the growth factor with a fourfold molar excess of any of the antagonists, independent of the drugs’ pretreatment. VEGF-A165-induced low cell index values, indicative of a dysfunctional barrier, were similarly prevented by different pretreated antagonists.
Conclusion: The passage of the proteins through NDN or SHN did neither affect efficient binding to their target, nor their capacity to prevent VEGF-A165-induced barrier dysfunction. Overall, regarding the stability of therapeutic proteins, the NDN was not inferior to the SHN, and can now be considered for evaluation in clinical studies.
Plain Language Summary: Common ocular diseases can be treated by injecting drugs into the vitreous body of the eye. Although this procedure is safe and well established, severe intraocular inflammation may occur. As this might be due to the use of a standard needle, we recently invented a novel needle with a closed tip and outlet for medication set on the needle side. We now investigated if the different flow of drug solutions out of the novel needle changed the activity of often-used anti-VEGF drugs. We found that their passage through the novel needle did not affect (1) their efficient interaction with their target or (2) their capacity to prevent barrier dysfunction in vitro. Overall, regarding the stability of anti-VEGF drugs, the novel needle is not inferior to the commonly used standard needle.
Keywords: intravitreal injection, endophthalmitis, VEGF-A, ranibizumab, faricimab, aflibercept, retinal endothelial cells
Introduction
Various ocular diseases of high socio-economic relevance, for example, age-related macular degeneration, macular edema secondary to retinal vein occlusion or diabetic retinopathy, and myopia, are accompanied by increased amounts of growth factors and cytokines in the vitreous.1–6 Of these, vascular endothelial growth factor-A (VEGF-A) plays a dominant role, and accordingly, the standard therapy comprises blocking VEGF-A-initiated signaling by intravitreal injection of VEGF-binding proteins. Fab fragment ranibizumab targets all splice variants of VEGF-A, Fc fusion protein aflibercept also complexes VEGF-B and placental growth factor (PlGF), and the bi-specific IgG faricimab additionally binds to angiopoietin-2 (Ang-2).7–14 These therapeutic proteins are usually injected intravitreally with standard hypodermic 30 gauge (G) needles (SHN) not approved for ocular use. Although intravitreal injection (IVI) is a well-established procedure, a low risk of serious vision-threatening complications, such as endophthalmitis, remains.15 Nevertheless, the number of IVIs increases worldwide every year, resulting in proportionally more cases of severe intraocular inflammation.16 Furthermore, the cumulative endophthalmitis risk per injection and eye tends to rise with an increasing number of intravitreal injections, i.e. from ~0.002% after one injection to more than 10fold after hundred injections.16 Symptoms of endophthalmitis as a consequence of IVI may differ from those of postoperative endophthalmitis after intraocular cataract, glaucoma, or vitreoretinal surgeries, and its early onset and diverse clinical presentation can lead to misdiagnosis.17 As the infection usually originates in the vitreous body, the early clinical signs may be overlooked. In such cases, infectious particles and their toxins have sufficient time to target the retina and optic nerve, causing irreversible degeneration. Although considered a rare complication, IVIs are the main cause of acute postoperative endophthalmitis because of their high frequency compared with other intraocular surgeries.18
Mechanisms of contamination of the vitreous during IVI are currently discussed, but clinical consequences of the demonstrated marked trauma to all layers of the eye wall at the entry site caused by the SHN and of ocular cell types found in needle-tip aspirates are not fully understood.19 However, histological studies revealed that a distinct linear cut remains throughout all ocular tissues passed by the tip of the 30°G SHN on its way to the vitreous.19 Therefore, intraocular inflammation can result from injection of adhering cellular material, which even could be contaminated by infectious particles, as well as from insufficient re-sealing of the entry site.19 To circumvent these problems, a 30 G needle featuring a sealed outer tip and a lateral side port for drug delivery was designed.20 Using an animal model, our group has demonstrated that penetration of the sclera with the newly designed needle (NDN) significantly reduces the risk of capturing and subsequently injecting potentially contaminated cellular material from the conjunctiva, sclera, and ciliary body.20
For the potential future use of NDN in IVIs in humans, both the safety and efficacy of drug delivery must be confirmed by thorough investigations. In particular, the altered injection stream produced by NDN may influence the biological activity of large molecules such as antibodies, and thus requires careful evaluation. Therefore, we investigated whether passage of VEGF-binding proteins through the NDN might alter their capacities to bind their target protein or to prevent VEGF-A-induced impairment of the barrier formed by immortalized microvascular endothelial cells of the bovine retina (iBREC).21–23 As model proteins we chose three VEGF antagonists frequently used in clinical practice: Ranibizumab (molecular weight 45 kDa), faricimab (140 kDa) and aflibercept (115 kDa).7,10,11,13,14
Materials and Methods
New Design of a Needle for IVI
A novel 30 G injection needle (NDN; custom-made, EP 18158 542.3, patent pending) was developed for intravitreal use (Figure 1A–C) and compared experimentally to a standard 30 G hypodermic needle (SHN; BD, Franklin Lakes, NJ, USA) (Figure 1D–F). Unlike SHN, NDN features a beveled occluded tip to eliminate dead space volume and a smooth side port for drug delivery (Figure 1B). The NDN prototype (S190630G), developed by Vitreq B.V. (Vierpolders, The Netherlands) in collaboration with Mr. Didenko (Kyiv, Ukraine), is not yet commercially available. Sterile, single-use NDN and SHN were imaged using intraoperative spectral-domain optical coherence tomography (OCT) (Rescan™ 700; Carl Zeiss Meditech AG, Jena, Germany) integrated into an OPMI Lumera 700 microscope (Carl Zeiss Meditech AG). The intraoperative OCT (iOCT) system settings were as follows: Wave length 840 nm (27000 A-scans/s; axial resolution ≤ 3.5 µm) with a 2.5 mm × 6.0 mm scan area; crosshair scans captured the needle-tip surface for analysis. The passage of liquids through the needle tips of both needle types was visualized with a solution of 0.06% trypan blue (Trypan Blue PFS, Sidapharm, Thessaloniki, Greece) (Figure 1C and F).
 |
Figure 1 Design and functional imaging of the newly designed needle (NDN) and a standard hypodermic needle (SHN). Images of (A) the NDN with a side port and (D) the SHN with a conventional front orifice (red arrows). Intraoperative OCT images of the needle tips, highlighting (B) the small side orifice of the NDN and (E) the front orifice of the SHN with a sharp inner edge (yellow arrows). Visualization of the injection jet direction out of (C) the NDN or (F) the SHN. |
VEGF-Binding Proteins
Faricimab (Vabysmo; 120 mg/mL in 3.1 mg/mL L-histidine, 1.044 mg/mL L-methionine, 1.46 mg/mL NaCl, 54.8 mg/mL D-sucrose, 0.04% polysorbate 20, pH 5.5) was purchased from Roche Pharma AG (Grenzach-Wyhlen, Germany), the Fc fusion protein aflibercept (Eylea: 40 mg/mL aflibercept in 10 mM sodium phosphate, 40 mM NaCl, 0.03% polysorbate 20, 5% sucrose, pH 6.2) from Bayer Vital GmbH Germany (Leverkusen, Germany), and ranibizumab (Lucentis: 10 mg/mL in 10 mM Histidine-HCl, 10% α,α-Trehalose 2H2O, 0.01% polysorbate 20, pH 5.5) from Novartis Pharma GmbH (Nuremberg, Germany).7–9,11–14 Recombinant human Sf21-expressed VEGF-A165 (#293VE, bio-techne, Wiesbaden, Germany) was dissolved in phosphate-buffered saline without Ca2+ and Mg2+ (PBSd; Thermo Fisher Scientific, Schwerte, Germany) at a final concentration of 100 µg/mL, and was stored at −80°C for no longer than three months.
Pretreatment of VEGF-Binding Proteins with Different Types of IVI Needles
Undiluted pharmacological formulations of the VEGF antagonists were either left untreated or 100 µL thereof were twice drawn up and dispensed through one of the needle types before being used for experiments. Repetitive passage through any of the tested cannulas mimics the process of IVI and a possible loss of biological activity should be detected with sufficiently high sensitivity. The needles were used immediately after sterilization, for which both types were rinsed several times with 70% 2-propanol and dried overnight at room temperature in a sterile environment.
Assessing Barrier Stability of Retinal Endothelial Cells by Cell Index Measurement
Generation, characterization and cultivation of telomerase-immortalized microvascular endothelial cells from bovine retina (iBREC) – established in our laboratory – have been described in great detail elsewhere.21–25 To assess the stability of a barrier formed by a monolayer of these cells, we measured the cell index with the xCELLigence RTCA DP device (Agilent, OLS, Bremen, Germany) as described in detail previously.22–28 Briefly, cells were cultured in Endothelial Cell Growth Medium MV (ECGM; #C22120, PromoCell, Heidelberg, Germany) until a confluent cell monolayer was reached three days later, indicated by a constantly high cell index (CI ~ 20).22–28 Effectors (VEGF-A165, un- or pretreated VEGF-binding proteins) were added one day after a complete exchange of the cell culture medium, and the cell index was measured every five minutes over the next three days.24 VEGF-A165 was used at a final concentration of 1.3 nM related to the dimer; final concentrations of VEGF antagonists were as follows: 0.2 µM ranibizumab, 0.1 µM faricimab or 0.1 µM aflibercept.23,24,29 Recorded cell index values (n≥5 for each condition and time point) were normalized in relation to those measured immediately before addition of the effectors (RTCA Software Pro., Version 2.6.1; Agilent), and the data were converted to graphs showing means and standard deviations with GraphPad Prism 9.4.1 (GraphPad Software, Boston, MA, USA).22–24 At the end of each experiment, integrity of the confluent monolayer was confirmed by microscopy, before cell culture supernatants were collected and stored at −80°C for further analyses.24
Determination of VEGF-A by ELISA
VEGF-A165 (final concentration of 1.3 nM) was mixed with un- or pretreated 0.8–6.5 nM ranibizumab, 0.8–13 nM faricimab or 1.3–13 nM aflibercept, respectively, and the mixtures were incubated for 15 minutes at 37°C to allow formation of the corresponding complexes. Mixtures were prepared in ECGM, which did not contain measurable amounts of VEGF-A (C(VEGF-A) ~0 pM; N>20). Then samples were diluted 1:10 in PBSd and unbound VEGF-A165 was determined with the Quantikine ELISA Human VEGF-A Immunoassay Kit (#DVE00, bio-techne) as described below. As a control, a solution of 1.3 nM VEGF-A165 was similarly processed, but these samples were diluted 1:50 in PBSd.
Unbound VEGF-A165 was also determined in the cell culture supernatants of iBREC collected after cell index measurements with cells exposed for three days to the growth factor with or without (pretreated) VEGF-binding proteins. The supernatants were not diluted except for those from the cultivation of cells exposed only to the growth factor, which were diluted 1:100 in PBSd.22–24
For all measurements, duplicate samples were processed according to the manufacturers’ instructions, and analyte-dependent absorbance was measured at 450 nm (reference wavelength: 570 nm) 20 min after addition of the stop solution with an Infinite 200Pro spectrophotometer controlled by I-control software (Tecan, Crailsheim, Germany).24 Quantification was based on standard curves generated with human recombinant VEGF-A165 (0 to 1250 pg/mL; minimal detectable dose: 19 pg/mL~0.5 pM) in parallel to the analyses of samples.
Statistical Analyses
Analysis of variance (ANOVA) followed by Tukey’s multiple comparison test was used to compare VEGF-A-specific absorbances from ELISA, the two-way ANOVA followed by Šidak’s multiple comparison test to analyze data obtained from cell index measurements. Differences resulting in p-values below 0.05 were considered significant. All statistical analyses were performed with GraphPad Prism 9.4.1; means and standard deviations are provided as numbers, graphs, or scatter plots.
Results
Unlike the SHN, which features a sharp-edged front orifice (Figure 1D and E), the NDN has a closed tip and a smooth-edged side port designed to reduce tissue trauma and cell uptake during drug delivery (Figure 1A and B). Figure 1B and E) also shows the intraoperative OCT images of both needle types. Liquids, such as solutions of VEGF-binding proteins, are released from the NDN into the vitreous through the side port at an angle of 90° relative to the longitudinal axis of the needle (Figure 1C). As this is fundamentally different from the linear flow through the SHN (Figure 1F), we investigated potential impacts on the biological activity of VEGF-binding proteins. To allow direct assessment of complex formation with VEGF-A165, the concentration range was established for each VEGF antagonist at which it most efficiently competed with the capture antibody of the used ELISA kit.30–32 The optimized conditions, under which only weak or no VEGF-specific signals indicated efficient complex formation of growth factor and antagonist, were then applied to evaluate whether passage of the VEGF-binding proteins through the NDN or a SHN affected their binding abilities. We also determined the capacity of un- or pretreated VEGF antagonists to prevent VEGF-A165-induced barrier impairment of iBREC, as assessed by cell index measurements.22–24,26,27 In these experiments, VEGF-binding proteins were used at concentrations previously shown to be effective.23,24,29
Ranibizumab
As shown in Figure 2A, concentrations of VEGF-A measured by ELISA depended on the molar ratio of ranibizumab to VEGF-A165, and at a fourfold molar excess of ranibizumab, only residual amounts of unbound VEGF-A were detected. Similar observations were made with ranibizumab after its passage through either a SHN or the NDN. (Figure 2B). Ranibizumab efficiently prevented the persistent barrier dysfunction induced by VEGF-A165 (Figure 2C), indicated by a significant decline of the normalized cell index. This was not changed by the passage of the antagonist through any of the two needle types tested (Figure 2D–F). At the end of the experiment, the concentrations of free VEGF-A in cell culture supernatants of control cells or of cells exposed to the growth factor and the un- or pretreated antagonists were below the ELISA detection limit. Supernatants of only VEGF-A-challenged iBREC then still contained 0.9 ± 0.1 nM VEGF-A (N=4; p<0.0001 compared to all other treatments).
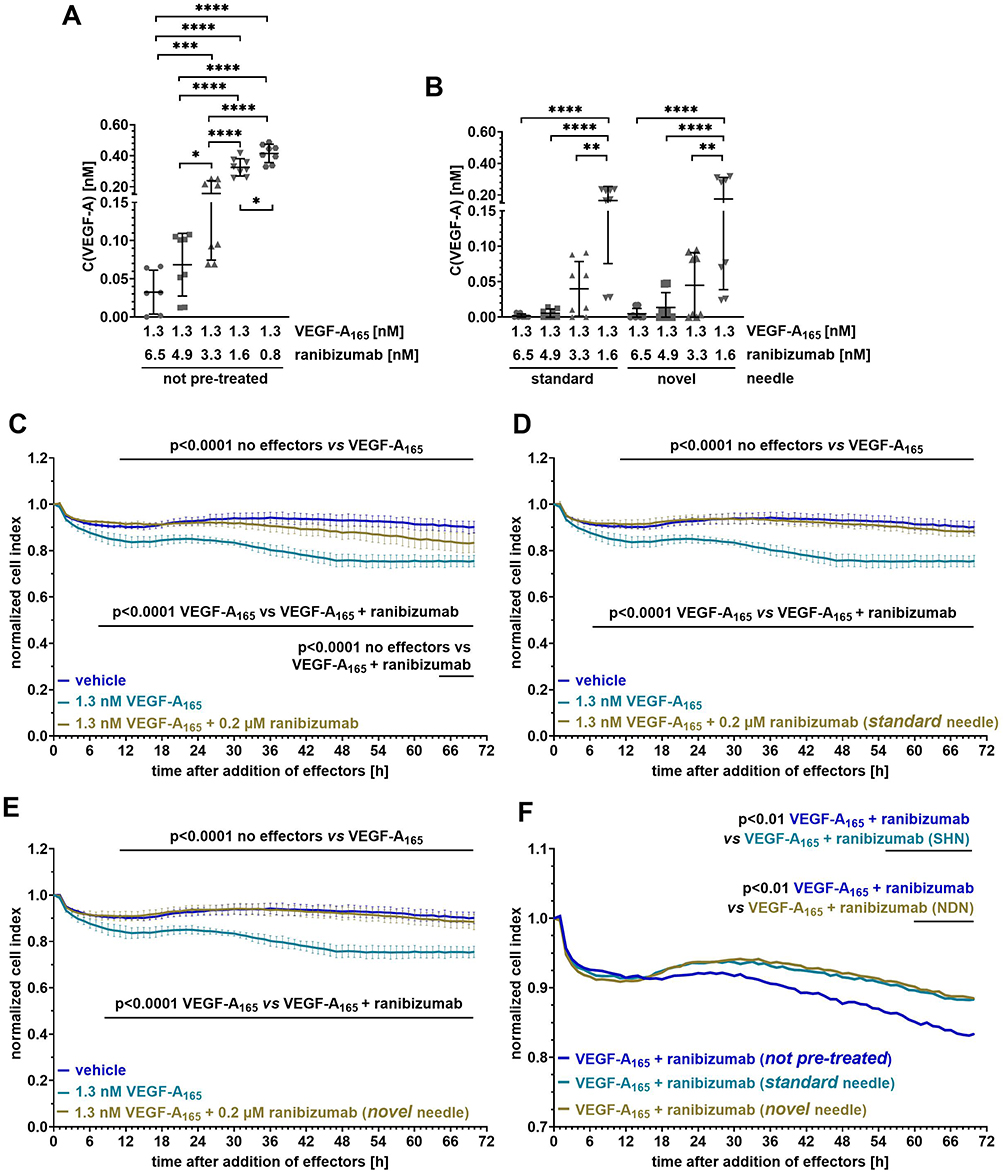 |
Figure 2 Passage of ranibizumab through the NDN or SHN did not change its typical characteristics. After incubation of VEGF-A165 with (A) untreated ranibizumab or (B) ranibizumab repeatedly passed through a needle, free growth factor was determined by ELISA. Data from independent experiments were pooled and analyzed as described in Material and Methods, and are shown as scatter plots with means ± standard deviations. *p<0.05, **p<0.01, ***p<0.001, ****) p<0.0001; only statistically significant differences are shown. All measured concentrations of free VEGF-A were very low. (C–F) Confluent monolayers of retinal endothelial cells (iBREC) were exposed to vehicle (n=6), VEGF-A165 (n=8), the growth factor plus (C and F) untreated (n=8), (D and F) SHN-treated (n=12) or (E and F) NDN-treated (n=11) ranibizumab for three days and the cell index was measured continuously. Cell index values were normalized and analyzed as described in Material and Methods. Means ± standard deviations are shown in (C–E), means only in (F). Ranibizumab efficiently prevented VEGF-A165-induced decline of cell index values which was not changed by its passage either through a SHN or the NDN. |
Faricimab
Concentrations of VEGF-A determined by ELISA also depended on the molar ratio of faricimab to the growth factor, and they were even lower than those measured with ranibizumab (Figure 3A). An at least fourfold molar excess of the VEGF antagonist was sufficient for the complete depletion of free growth factor, regardless of whether faricimab had passed through either of the two needle types (Figure 3B). Consequently, the untreated (Figure 3C) and pretreated (Figure 3D–F) antagonists similarly prevented the VEGF-A165-induced barrier impairment. Unbound VEGF-A was also not detected in cell culture supernatants of cells exposed to the growth factor together with the antagonist for three days, whereas it was still present in supernatants of VEGF-A-treated iBREC (0.62 ±0.15 pM, N=6; p<0.0001 compared to all other treatments).
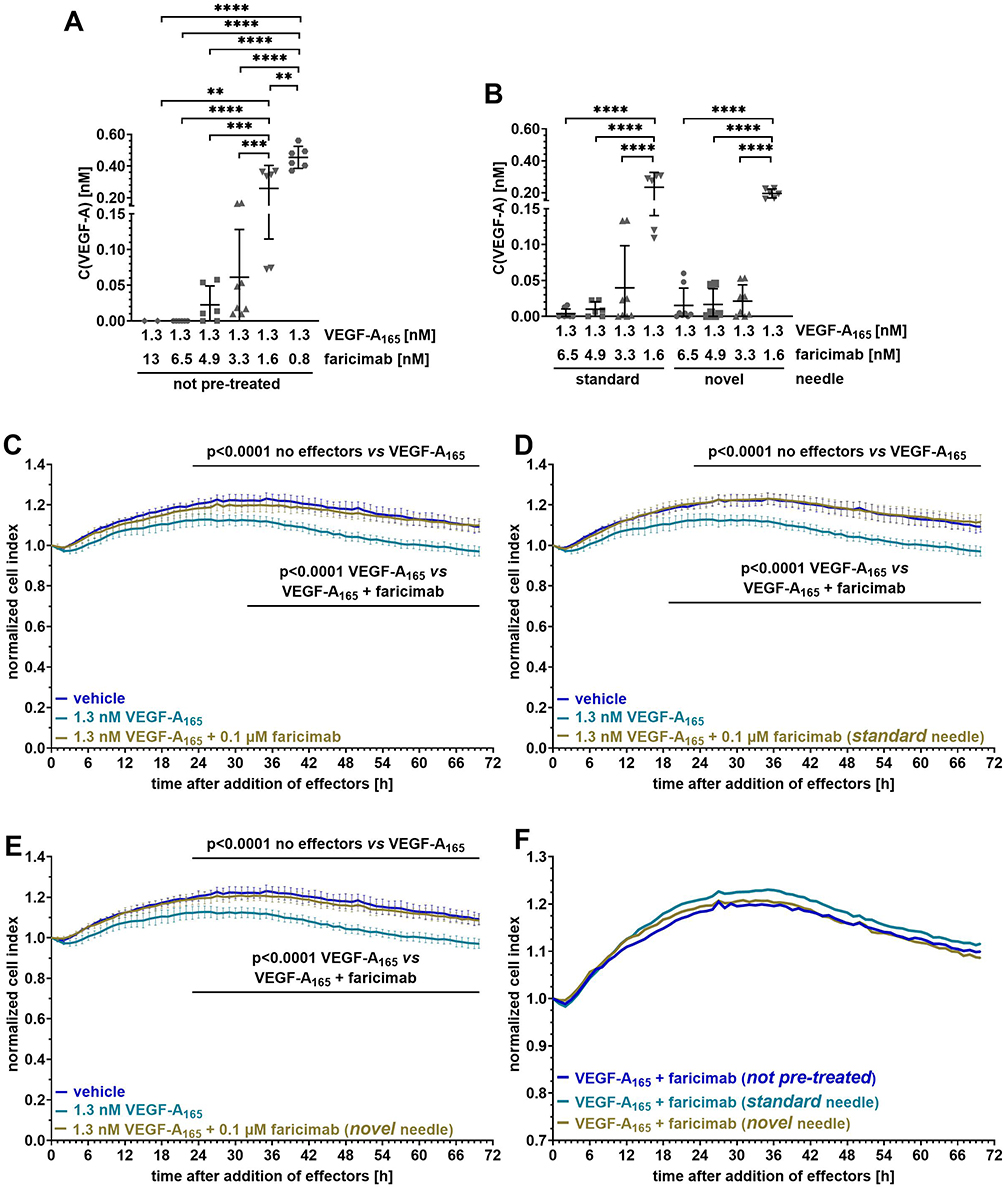 |
Figure 3 Passage through the NDN or a SHN did not alter faricimab’s properties. Free VEGF-A was determined by ELISA after incubating VEGF-A165 with (A) untreated or (B) pretreated faricimab. Data from independent experiments were pooled, analyzed and presented as described in the legend to Figure 1. **p<0.01, ***p<0.001, ****p<0.0001; only statistically significant differences are shown. Only very low concentrations of free VEGF-A were measured, independent of pretreatment of the antagonist. (C–F) The cell index was continuously measured for three days of confluent iBREC exposed to vehicle (n=5), VEGF-A165 (n=6), the growth factor plus (C and F) untreated (n=7), (D and F) SHN-treated (n=9) or (E and F) NDN-treated (n=8) faricimab, and cell index values were processed as described in the legend to Figure 1. Means ± standard deviations are shown in (C–E), means only in (F). The VEGF-A165-induced decline of the cell index values efficiently prevented by faricimab which was not changed by its passage either through a SHN or the NDN, as indicated by nearly identical curves. |
Aflibercept
At equimolar concentrations of a VEGF antagonist and VEGF-A165, markedly less VEGF-A was measured by ELISA with aflibercept than with faricimab, although residual amounts of the free growth factor were still present even at a 10fold molar excess of aflibercept (Figure 4A). However, observations made with aflibercept pretreated with SHN or NDN were similar, confirming the equivalence of the two needle types (Figure 4B). Similar to the other anti-VEGF drugs, aflibercept efficiently prevented the VEGF-A165-induced barrier breakdown (Figure 4C), with similar results when pretreated antagonists were used (Figure 4D–F). Interestingly, in contrast to our observations with ranibizumab and faricimab, residual amounts of VEGF-A were measured by ELISA in all cell culture supernatants obtained from iBREC cultures exposed to the growth factor together with aflibercept for three days (Figure 4G). However, these amounts were still significantly lower than those measured in the supernatants of VEGF-A165-exposed iBREC (Figure 4H).
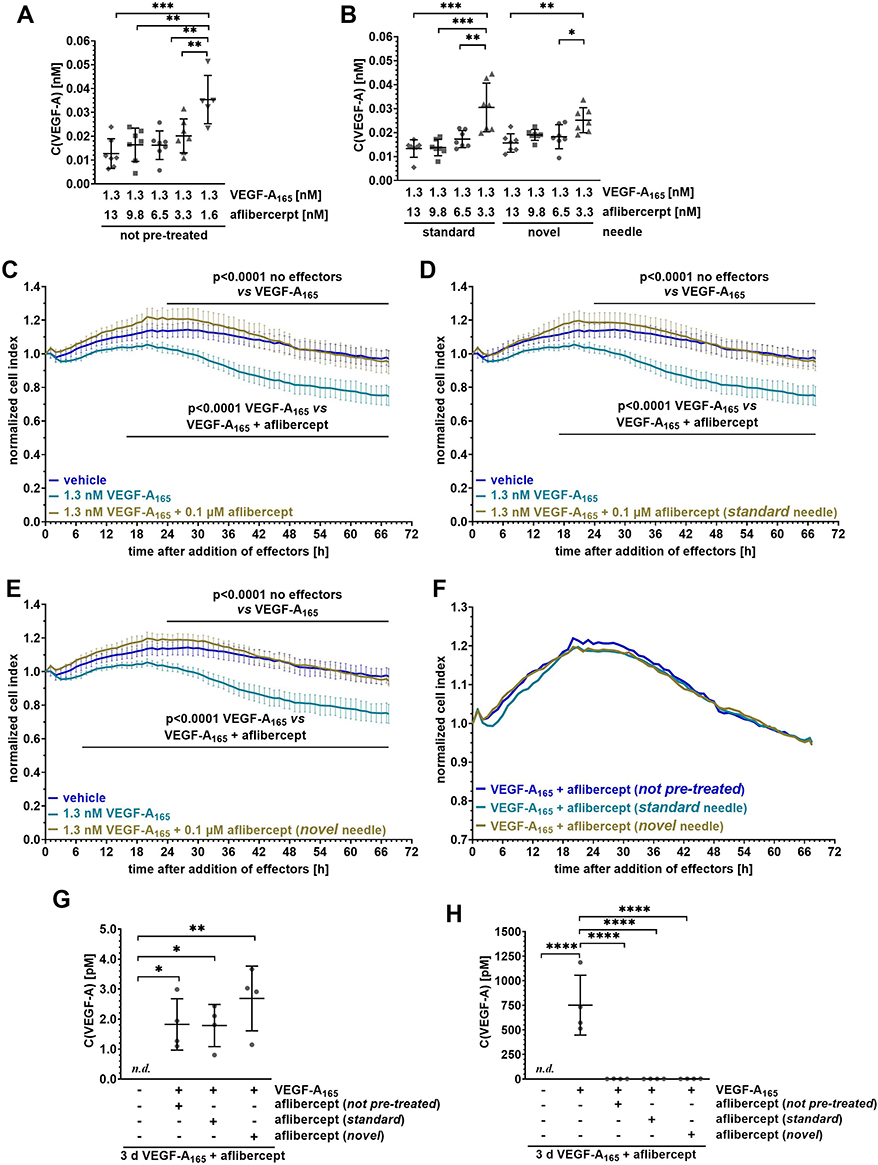 |
Figure 4 Characteristics of aflibercept were not changed by its passage through the NDN or a SHN. Competitive ELISA was used to determine free growth factor after incubation of VEGF-A165 with (A) untreated or (B) pretreated aflibercept. Data from independent experiments were pooled and processed as described above. *p<0.05, **p<0.01, ***p<0.001; only statistically significant differences are shown. All measured concentrations of free VEGF-A were very low. (C–F) Confluent iBREC were treated with vehicle (n=7), VEGF-A165 (n=6), the growth factor plus (C and F) untreated (n=6), (D and F) SHN-treated (n=10) or (E and F) NDN-treated (n=8) aflibercept for three days, and the cell index was measured continuously. Cell index values were processed as described above. Means ± standard deviations are shown in (C–F), means only in (F). Both un- and pretreated aflibercept efficiently prevented VEGF-A165-induced decline of cell index values with nearly identical results obtained in experiments with the different needle types. (G and H) Unbound VEGF-A was determined by competitive ELISA in supernatants of iBREC exposed to the growth factor with or without un- or pretreated aflibercept for three days. Pooled data were analyzed as described above. *p<0.05, **p<0.01, ****p<0.0001; only statistically significant differences are shown. n.d. not detected. Independent of pretreatment of aflibercept, residual free VEGF-A was measured in (G) supernatants of cells exposed to the growth factor and the antagonist but the amounts were still much lower than those in (H) supernatants of VEGF-A165-treated cells. |
Discussion
Ocular diseases are increasingly being treated with intravitreal injections of medications. Although severe complications such as infectious and non-infectious inflammation are rare, their absolute number is rising, prompting efforts to optimize the technique and devices. We focused on improving safety of intravitreal injections by modifying the needle tip, an area not yet systematically addressed.20 In previous studies we demonstrated that standard hypodermic needles may directly cause trauma and introduce cellular contaminants potentially leading to inflammation.19 In contrast, use of our novel needle with a closed front tip and side port was associated with reduced tissue damage in combination with comparable drug delivery, despite of a slightly higher penetration force due to prototype characteristics.20 In comparison to the tip aspirates of the SHN, those of the NDN contain ~50% less conjunctival and ciliary body cells, granulated proteins and vitreous body remnants, and it is a plausible assumption that the associated risk of inadvertent injection of potentially infectious particles is lower.20 In this study, we now investigated whether the different flow through the NDN affects the activity of commonly used VEGF-binding proteins as a contribution to the assessment of its safety in view of potential clinical use in humans.
In accordance with previous findings of others, we observed that anti-VEGF drugs ranibizumab, faricimab and aflibercept competed for binding to VEGF-A with capture antibodies of the used commercial ELISA kit.30–32 Only low concentrations of the growth factor were measured in the presence of the three antagonists, confirming the formation of stable complexes. However, the concentrations of residual free VEGF-A differed, which is likely due to the different dissociation constants of the three antagonists.13,33,34 Most importantly, pretreatment of the antagonists by passing them through any of the needle types tested did not alter the concentrations of free VEGF-A, confirming that the binding capacities of the antagonists were not affected and did not differ after lateral flow out of the NDN. Confirming our previous observations, all three anti-VEGF drugs also efficiently prevented VEGF-A165-elevated permeability of microvascular retinal endothelial cells, represented by the iBREC cell line.22–24,28 This ability was also not diminished by the passage of an antagonist solution through one of the needle types investigated. Even a moderate loss of activity of the antagonists would have been recognized because of the much lower ratio of antagonist to VEGF-A used in comparison to clinical practice.8–10,12,14 In addition, even subtle or transient changes affecting the cells’ barrier function would have been detected by highly sensitive cell index measurements.22–27 However, differences between pre- and untreated anti VEGF drugs were not observed, confirming that passage through the NDN does not alter their binding abilities.
We focused on the ability of the NDN-treated antagonists to bind to splice variant VEGF-A165 and to thereby suppress activation of its receptors and subsequent signaling, since this splice variant is the main driver in processes leading to impairment of the barrier formed by monolayers of retinal endothelial cells in vitro.35 In vivo, VEGF-A165-elevated permeability of retinal vessels eventually results in macular edema, a hallmark of various ocular diseases.36 The splice variant VEGF-A121 has only a minor effect, and VEGF-B, PlGF or Ang-2 by themselves do not alter the stability of the REC barrier in vitro.24,35,37 Although of non-human origin, iBREC that are similar to primary microvascular endothelial cells of the bovine retina, are an excellent and highly reliable in vitro model of the tight inner blood-retina barrier proofed to be useful to study the biological activity of VEGF antagonists.22,23,38,39 We believe that our very clear results based on the iBREC model are sufficient to confirm stability and maintained activity of VEGF antagonists injected with the NDN to foster its further clinical evaluation. Additional time-consuming and expensive investigations in animal models do not seem to be warranted, and therefore might also raise ethical concerns.
This in vitro study was performed to critically verify our hypothesis that the lateral injection stream out of the newly designed needle does not impair the biological activity of large therapeutic molecules, e.g. antibodies and their derivates.20 One limitation of the study is the only indirect verification by competitive ELISA of the anti VEGF drugs’ ability to bind to their target proteins.30–32 However, from the very low amounts of free VEGF-A measured, we can safely conclude that any possible sheer stress applied during passage through the NDN does not affect the antagonists’ binding efficiencies. Despite the study’s in vitro design, we do not anticipate different outcomes when the therapeutic efficacy will be evaluated after standard intravitreal injection with the NDN into the human eye. Collected data on the NDN, confirming less tissue damage, comparable drug delivery, and maintenance of drug activity as shown by this and our previous studies, now provide the basis for its clinical evaluation. Future approval and routine use of the potentially beneficial NDN will depend on the results of a sufficiently large prospective clinical study meeting all regulatory requirements. Obviously, the device then has to be manufactured under high-quality conditions that allow its initial certification and ongoing validation.
Conclusion
Passage of the VEGF-binding proteins faricimab, ranibizumab, or aflibercept through a newly designed needle with a lateral port does not affect their efficient interaction with VEGF-A165. Accordingly, the use of this delivery device does not impair the capacity of the anti-VEGF drugs to prevent VEGF-A165-induced barrier dysfunction of retinal endothelial cells. Our results clearly indicate that the newly designed needle is not inferior to the standard needle in terms of stability of therapeutic VEGF-binding proteins, complying with the approval requirements for intravitreal drug delivery.
Abbreviations
Ang-2, angiopoietin-2; ECGM, endothelial cell growth medium; iBREC, immortalized bovine retinal endothelial cells; iOCT, intraoperative OCT; IVI, intravitreal injection; NDN, newly designed 30 G needle; PBSd, phosphate-buffered saline without Ca2+ and without Mg2+ ions; OCT, optical coherence tomography; PlGF, placental growth factor; SHN, standard hypodermic 30 G needle; VEGF, vascular endothelial growth factor.
Data Sharing Statement
The original data used to support the findings of this study are either included in the article or are available from the corresponding author upon request.
Acknowledgments
This article does not contain any results of studies with human participants or animals. For this research, no external funding was received. This study is based on data presented at the ARVO Annual Meeting 2025 (Salt Lake City, USA).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Lyubomyr Lytvynchuk is the inventor of NDN and is a member of the advisory boards of Roche Pharma AG, Germany, and Bayer Vital GmbH, Germany. Lyubomyr Lytvynchuk also reports a pending patent EP18158542.3. Heidrun L. Deissler has received research funding from Roche Pharma AG (Germany). Kai L. Nolte, Isabell Fuezy, Wen Zhou, and Helmut Deissler declare no conflicts of interest in this work.
References
1. Aiello LP, Avery RL, Arrigg PG, et al. Vascular endothelial growth factor in ocular fluid of patients with diabetic retinopathy and other retinal disorders. N Engl J Med. 1994;331(22):1480–1487. doi:10.1056/NEJM199412013312203
2. Boulton M, Gregor Z, McLeod D, et al. Intravitreal growth factors in proliferative diabetic retinopathy: correlation with neovascular activity and glycaemic management. Br J Ophthalmol. 1997;81(3):228–233. doi:10.1136/bjo.81.3.228
3. Campochiaro PA. Retinal and choroidal neovascularization. J Cell Physiol. 2000;184(3):301–310. doi:10.1002/1097-4652(200009)184:3<301::AID-JCP3>3.0.CO;2-H
4. Campochiaro PA. Ocular neovascularization. J Mol Med. 2013;91(31):311–321. doi:10.1007/s00109-013-0993-5
5. Scholl S, Kirchhhof J, Augustin AJ. Pathophysiology of macular edema. Ophthalmologica. 2010;224(1):8–15. doi:10.1159/000315155
6. Klaassen I, deVries EW, Vogels IMC, et al. Identification of proteins associated with clinical and pathological features of proliferative diabetic retinopathy in vitreous and fibrovascular membrane. PLoS One. 2017;12(11):e0187304. doi:10.1371/journal.pone.0187304
7. Ferrara N, Damico L, Shams N, Lowman H, Kim R. Development of ranibizumab, an anti-vascular endothelial growth factor antigen binding fragment, as therapy for neovascular age-related macular degeneration. Retina. 2006;26(8):859–870. doi:10.1097/01.iae.0000242842.14624.e7
8. Rosenfeld PJ, Brown DM, Heier JS, et al. MARINA Study Group. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1419–1431. doi:10.1056/NEJMoa054481
9. Mitchell P, Bandello F, Schmidt-Erfurth U, et al. RESTORE study group. The RESTORE study: ranibizumab monotherapy or combined with laser versus laser monotherapy for diabetic macular edema. Ophthalmology. 2011;118(4):615–625. doi:10.1016/j.ophtha.2011.01.031
10. Wells JA, Glassman AR, Ayala AR, et al. Diabetic retinopathy clinical research network. aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N Engl J Med. 2015;372(13):1193–1203. doi:10.1056/NEJMoa1414264
11. Holash J, Davis S, Papadopoulos N, et al. VEGF-Trap: a VEGF blocker with potent antitumor effects. Proc Natl Acad Sci USA. 2002;99(17):11393–11398. doi:10.1073/pnas.172398299
12. Do DV, Nguyen QD, Boyer D, et al. da Vinci Study Group. One-year outcomes of the DA VINCI study of VEGF trap-eye in eyes with diabetic macular edema. Ophthalmology. 2012;119(8):1658–1665. doi:10.1016/j.ophtha.2012.02.010
13. Regula JT, Lundh von Leithner P, Foxton R, et al. Targeting key angiogenic pathways with a bispecific CrossMAb optimized for neovascular eye diseases. EMBO Mol Med. 2016;8(11):1265–1288. doi:10.15252/emmm.201505889
14. Wong TY, Haskova Z, Asik K, et al. YOSEMITE and RHINE investigators. Faricimab treat-and-extend for diabetic macular edema: 2-year results from the randomized Phase 3 YOSEMITE and RHINE trials. Ophthalmology. 2024;131(6):708–723. doi:10.1016/j.ophtha.2023.12.026
15. Jonas JB, Spandau UH, Rensch F, Von Baltz S, Schlichtenbrede F. Infectious and noninfectious endophthalmitis after intravitreal bevacizumab. J Ocul Pharmacol Ther. 2007;23(3):240–242. doi:10.1089/jop.2006.0146
16. Israilevich RN, Mansour H, Patel SN, et al. Risk of endophthalmitis based on cumulative number of anti-VEGF intravitreal injections. Ophthalmology. 2024;131(6):667–673. doi:10.1016/j.ophtha.2023.12.033
17. Shao EH, Yates WB, Ho IV, Chang AA, Simunovic MP. Endophthalmitis: changes in presentation, management and the role of early vitrectomy. Ophthalmol Ther. 2021;10(4):877–890. doi:10.1007/s40123-021-00406-6
18. Ong AY, Rigaudy A, Toufeeq S, et al. Intravitreal injections as a leading cause of acute postoperative endophthalmitis-a regional survey in England. Eye. 2023;37(1):163–169. doi:10.1038/s41433-021-01886-3
19. Lytvynchuk L, Sergienko A, Savytska I, et al. Comparative cyto-histological study of needle tip aspirates and entry sites after intravitreal injection using different needle types. PLoS One. 2017;12(7):e0174467. doi:10.1371/journal.pone.0174467
20. Lytvynchuk LM, Petrovski G, Dam A, et al. Novel needle for intravitreal drug delivery: comparative study of needle tip aspirates, injection stream and penetration forces. Clin Ophthalmol. 2021;15:723–734. doi:10.2147/OPTH.S297139
21. Deissler H, Deissler H, Lang GK, Lang GE. Generation and characterization of iBREC: novel hTERT-immortalized bovine retinal endothelial cells. Int J Mol Med. 2005;16(1):65–70. doi:10.3892/ijmm.16.1.65
22. Deissler HL, Lang GK, Lang GE. Inhibition of single routes of intracellular signaling is not sufficient to neutralize the biphasic disturbance of a retinal endothelial cell barrier induced by VEGF-A165. Cell Physiol Biochem. 2017;42(4):1493–1513. doi:10.1159/000479213
23. Deissler HL, Rehak M, Busch C, Wolf A. Blocking of VEGF-A is not sufficient to completely revert its long-term effects on the barrier formed by retinal endothelial cells. Exp Eye Res. 2022;216:108945. doi:10.1016/j.exer.2022.108945
24. Deissler HL, Rehak M, Lytvynchuk L. VEGF-A165a and angiopoietin-2 differently affect the barrier formed by retinal endothelial cells. Exp Eye Res. 2024;247:110062. doi:10.1016/j.exer.2024.110062
25. Busch C, Rehak M, Hollborn M, et al. Type of culture medium determines properties of cultivated retinal endothelial cells: induction of substantial phenotypic conversion by standard DMEM. Heliyon. 2021;7(1):e06037. doi:10.1016/j.heliyon.2021.e06037
26. Sun M, Fu H, Cheng H, et al. A dynamic real-time method for monitoring epithelial barrier function in vitro. Anal Biochem. 2012;425(2):96–103. doi:10.1016/j.ab.2012.03.010
27. Bischoff I, Hornburger MC, Mayer BA, Beyerle A, Wegener J, Fürst R. Pitfalls in assessing microvascular endothelial barrier function: impedance-based devices versus the classic macromolecular tracer assay. Sci Rep. 2016;6(1):23671. doi:10.1038/srep23671
28. Deissler HL, Sommer K, Lang GK, Lang GE. Transport and fate of aflibercept in VEGF-A165-challenged retinal endothelial cells. Exp Eye Res. 2020;198:108156. doi:10.1016/j.exer.2020.108156
29. Deissler HL, Lang GK, Lang GE. Capacity of aflibercept to counteract VEGF-stimulated abnormal behavior of retinal microvascular endothelial cells. Exp Eye Res. 2014;122:20–31. doi:10.1016/j.exer.2014.02.024
30. Walz JM, Boehringer D, Deissler HL, et al. Pre-analytical parameters affecting vascular endothelial growth factor measurement in plasma: identifying confounders. PLoS One. 2016;11(1):e0145375. doi:10.1371/journal.pone.0145375
31. Takahashi H, Nomura Y, Nishida J, Fujino Y, Yanagi Y, Kawashima H. Vascular endothelial growth factor (VEGF) concentration is underestimated by enzyme-linked immunosorbent assay in the presence of anti-VEGF drugs. Invest Ophthalmol Vis Sci. 2016;57(2):462–466. doi:10.1167/iovs.15-18245
32. Sumner G, Georgaros C, Rafique A, et al. 2019 Anti-VEGF drug interference with VEGF quantitation in the R&D systems human quantikine VEGF ELISA kit. Bioanalysis. 2019;11(5):381–392. doi:10.4155/bio-2018-0096
33. Lowe J, Araujo J, Yang J, et al. Ranibizumab inhibits multiple forms of biologically active vascular endothelial growth factor in vitro and in vivo. Exp Eye Res. 2007;85(4):425–430. doi:10.1016/j.exer.2007.05.008
34. Papadopoulos N, Martin J, Ruan Q, et al. Binding and neutralization of vascular endothelial growth factor (VEGF) and related ligands by VEGF Trap, ranibizumab and bevacizumab. Angiogenesis. 2012;15(2):171–185. doi:10.1007/s10456-011-9249-6
35. Deissler H, Deissler H, Lang GE. Inhibition of VEGF is sufficient to completely restore barrier malfunction induced by growth factors in microvascular retinal endothelial cells. Br J Ophthalmol. 2011;95(8):1151–1156. doi:10.1136/bjo.2010.192229
36. Qaum T, Xu Q, Joussen AM, et al. VEGF-initiated blood-retinal barrier breakdown in early diabetes. Invest Ophthalmol Vis Sci. 2001;42(10):2408–2413.
37. Deissler HL, Deissler H, Lang GK, Lang GE. VEGF but not PlGF disturbs the barrier of retinal endothelial cells. Exp Eye Res. 2013;115:162–171. doi:10.1016/j.exer.2013.07.018
38. Bosma EK, Darwesh S, Habani YI, et al. Differential roles of eNOS in late effects of VEGF-A on hyperpermeability in different types of endothelial cells. Sci Rep. 2023;13(1):21436. doi:10.1038/s41598-023-46893-4
39. Jung DM, Fuezy I, Lytvynchuk L, Deissler HL. Faricimab reverts VEGF-A165-induced impairment of the barrier formed by retinal endothelial cells. Int J Mol Sci. 2025;26(9):4318. doi:10.3390/ijms26094318
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.