Back to Journals » Clinical Ophthalmology » Volume 14
Normative Values of Corneal Spherical Aberration, Pupil Size, and Other Key Refractive and Topographic Parameters in a Large Cohort of Egyptian Cataract Surgery Candidates
Authors Elkitkat RS, Fouad YA ![]() , Shams A
, Shams A ![]() , Hamza I
, Hamza I
Received 26 October 2020
Accepted for publication 3 December 2020
Published 31 December 2020 Volume 2020:14 Pages 4571—4577
DOI https://doi.org/10.2147/OPTH.S288738
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rania Serag Elkitkat,1– 3 Yousef A Fouad,1 Abdelrhman Shams,1 Ismail Hamza1
1Ophthalmology Department, Faculty of Medicine, Ain Shams University, Cairo, Egypt; 2Watany Eye Hospital, Cairo, Egypt; 3Watany Research and Development Center, Cairo, Egypt
Correspondence: Abdelrhman Shams
Faculty of Medicine, Ain Shams University, Cairo, Egypt
Tel +201222131012
Email [email protected]
Purpose: To determine the spherical aberration, pupil size, and other key refractive and topographic parameters in a large cohort of Egyptian cataract surgery candidates, and to investigate any existent relations between the spherical aberration and other possibly related parameters.
Methods: This is a cross-sectional, descriptive study that was conducted at Ain Shams University Hospitals, Cairo, Egypt. The study was performed on the right eyes of 1658 cataract surgery candidates. The mean corneal spherical aberration [Z4] and the pupil diameter, both photopic [P. Pupil] and mesopic [M. Pupil], were measured by the Oculus Keratograph 3, while the white-to-white corneal diameter [WTW], average keratometric readings [average K], axial length measurements [AL] and Anterior Chamber Depth [ACD] were all obtained from the IOL Master 500.
Results: The mean age was 65 ± 11.3 years. The mean value of the Z4 was +0.26 ± 0.12 μm [95% Confidence Interval “CI” (0.2570– 0.2681)]. The mean values of the measured parameters were: P. Pupil 2.43 ± 0.87 mm [95% CI (2.3867– 2.4700)], M. Pupil 4.61 ± 0.91 mm [95% CI (4.5683– 4.6557)], WTW 11.72 ± 0.44 mm [95% CI (11.6969– 11.7394)], average K 43.89 ± 1.89 D [95% CI (43.7938– 43.9701)], AL 24.23 ± 2.21 mm [95% CI (24.1118– 24.3166)], and ACD 3.16 ± 0.43 mm [95% CI (3.1414– 3.1827)]. Weak statistically significant correlations were found between the Z4 and each of age (r = 0.049, p = 0.044), average K (r = 0.191, p < 0.001), and ACD (r = 0.122, p < 0.001). Multivariate analysis showed weaker relations between Z4 and both average K (beta coefficient= 0.091) and ACD (beta coefficient= 0.130), with an r2 = 0.024.
Conclusion: This is the first normative data report of corneal spherical aberration [Z4], pupil size, and related refractive and topographic parameters in an old Egyptian population. The detected correlations have a weak clinical relevance and negate the existence of significant relations between the Z4 and the studied refractive and topographic parameters.
Keywords: corneal spherical aberration, Z4, corneal keratography, white-to-white corneal diameter, Egyptian population
Introduction
The expanded arsenal of an ophthalmologist has got a myriad of instruments for measuring anterior segment parameters prior to intraocular surgeries. Non-contact optical biometry relies on the principle of partial coherence interferometry and has been the mainstay for intraocular lens (IOL) power calculations over the past two decades, with the IOL Master (Carl Zeiss Meditec, Germany) being the most commonly used device.1,2 Data obtained from the IOL Master include axial length (AL), anterior chamber depth (ACD), average keratometric (average K) readings, and white-to-white corneal diameter (WTW) measurements.3 Other than optical biometry, the placido-based topography systems, like the Keratograph (Oculus, Germany), can provide further in-depth information regarding the corneal topography mapping, the corneal spherical aberration (Z4) and the pupil size (photopic and mesopic).4
Nowadays, cataract surgery does not only aim to restore the Snellen acuity but it should also address the proper manipulation of the ocular spherical aberrations (via the Zernike transformations) to obtain the highest quality of visual acuity and contrast sensitivity.5 The corneal spherical aberration is commonly considered as the most important high-order aberration that is highly prevalent worldwide and has got a major impact on the visual performance.6
The corneal spherical aberration directly affects the corneal asphericity, and they both have got major influences on many anterior segment-related procedures including IOL power selection, IOL asphericity, and refractive surgeries.7,8 Previous related literature has suggested normative spherical aberration [Z4] values that range between +0.19 and +0.49 μm.9,10 Several demographic and refractive factors have been reported to influence the Z4.5,6 Ethnicity may be one crucial factor, with multiple available studies suggesting differences in corneal spherical aberration related to different ethnicities.11–14 To date, no large analysis work in the literature could report on the normative mean values of Z4 and related refractive variables in an Egyptian population. Egypt is unique in that it lies at the crossroads of two major continents, with a unique genetic profile spreading from Africa to the Middle East.15
In this work, we set out to study the corneal spherical aberration (Z4) in a large cohort of an Egyptian elderly population who were all candidates for cataract surgery. The secondary outcome was to obtain relevant refractive and topographic values in the same population and to investigate any correlation they might have to the Z4.
Patients and Methods
This is a cross-sectional, non-comparative, descriptive study. All the recruited participants sought medical services for performing cataract surgery in the period from January 2015 to January 2018. The study was conducted at Ain Shams University Hospitals, Cairo, Egypt. We excluded candidates with any topographic abnormalities like those with keratoconus or forme fruste keratoconus, any candidate with history of contact lenses fitting within the previous 2 weeks, previous refractive surgeries, previous ocular trauma or surgeries, or any evident anterior segment pathology on slit-lamp examination (including corneal scars). The study adhered to the tenets of the Declaration of Helsinki and informed consents were signed by all participants. The study protocol was approved by the Ethical Committee of Ain Shams University.
The right eyes of 1658 participants were included in the study. Slit-lamp examinations were performed for the recruited cohort. The corneal spherical aberration (Z4) value and the pupil diameter values (Photopic Pupil “P. Pupil” and Mesopic Pupil “M. Pupil”) were obtained from the Oculus Keratograph 3 (Oculus, Germany), whereas the WTW, average K, AL, and ACD were all obtained from the IOL Master 500 (Carl Zeiss Meditec, Germany). The measurements were performed by a single optometrist. The participants’ eyes were aligned along the visual axis using a central fixation light. Participants were instructed to blink in between shots to keep eyes moist.
Statistical analysis was performed using SPSS v25 (IBM, USA). Descriptive statistics were carried out including mean and – where appropriate – median value calculation together with standard deviations. Correlations were calculated between different numerical variables and were depicted in the form of Pearson correlation coefficient. Multivariate analyses were calculated for different studied numerical variables and were depicted in the form of beta coefficient, r and r2. Where appropriate, p-values were calculated and a value less than 0.05 was considered statistically significant.
Results
This cross-sectional study included 1658 right eyes of 1658 participants with naive corneas. The female to male ratio of the studied cohort was 1.6:1, and the mean age was 65 years (SD: ± 11.3 years).
The details of the measured parameters are depicted in Table 1 and Figure 1. The mean value for the Z4 was +0.26 (± 0.12) μm. The mean P. Pupil was 2.43 (± 0.87) mm, while the mean M. Pupil was 4.61 (± 0.91) mm. The mean WTW, average K, AL, and ACD were 11.72 (± 0.44) mm, 43.89 (± 1.89) D, 24.23 (± 2.21) mm, and 3.16 (± 0.43) mm, respectively.
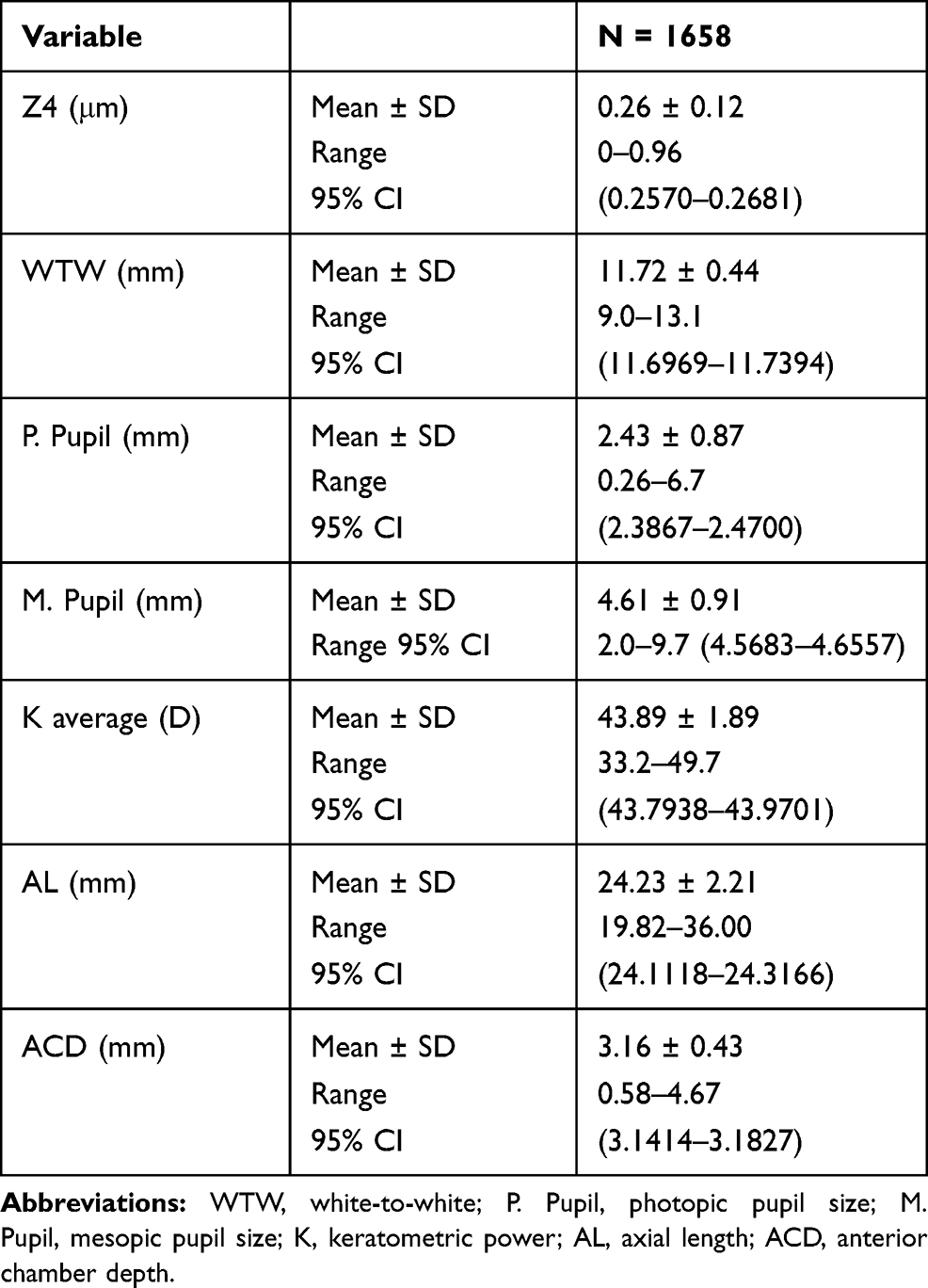 |
Table 1 Descriptive Statistics of Measured Parameters of 1658 Right Eyes |
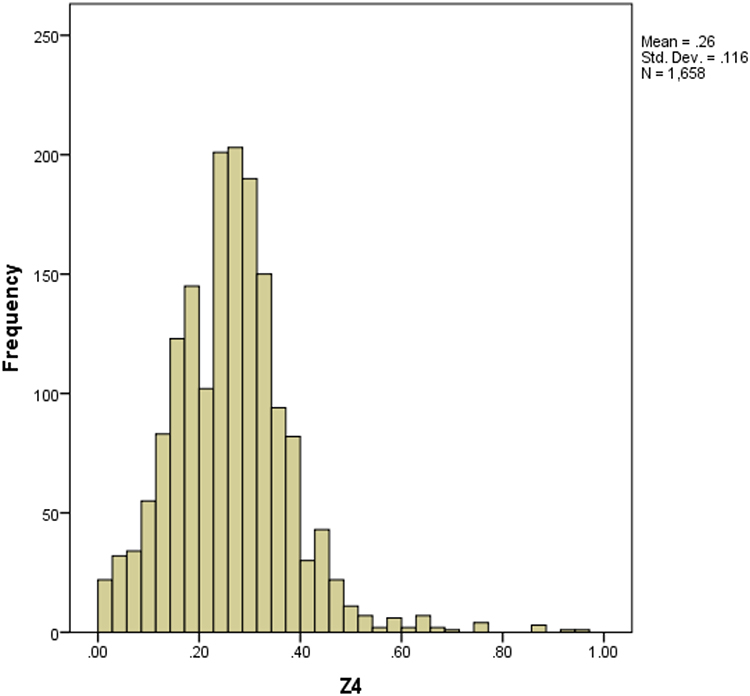 |
Figure 1 Frequency distribution curve of corneal spherical aberration (Z4) in the studied cohort. |
The correlations between the different studied parameters are detailed in Table 2. Our study results revealed positive, yet weak, statistically significant correlations between the Z4 and each of the following factors: age (r = 0.049, p = 0.044), average K (r = 0.191, p < 0.001) and ACD (r = 0.122, p < 0.001). Regarding the pupil size parameter, a statistically significant negative correlation was found between both P. Pupil and M. Pupil size and the age factor (p < 0.001), while a positive significant one was found between both pupil sizes and each of AL and ACD variables. Though all the correlations were weak ones, the strongest correlation was found between M. Pupil and ACD (r = 0.334, p <0.001).
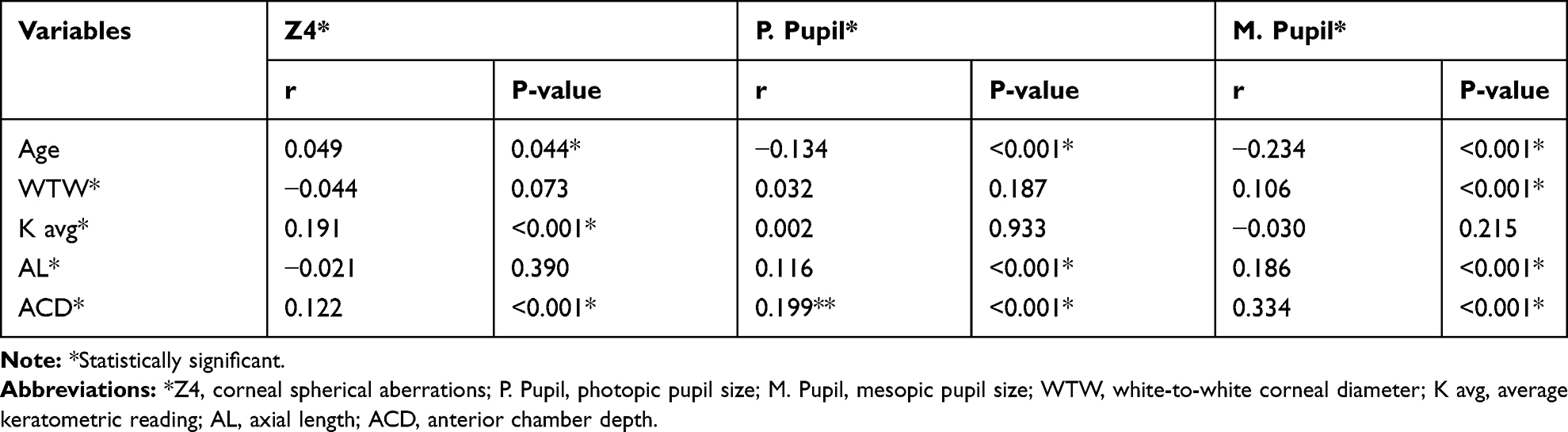 |
Table 2 Correlation Between Different Measured Variables |
Furthermore, a multivariate analysis was plotted to detect the most determining parameters that would possibly alter the Z4, which is detailed in Table 3. Our analysis revealed weak but statistically significant relations between Z4 and both average K (beta coefficient= 0.091) and ACD (beta coefficient= 0.130), with r2= 0.024.
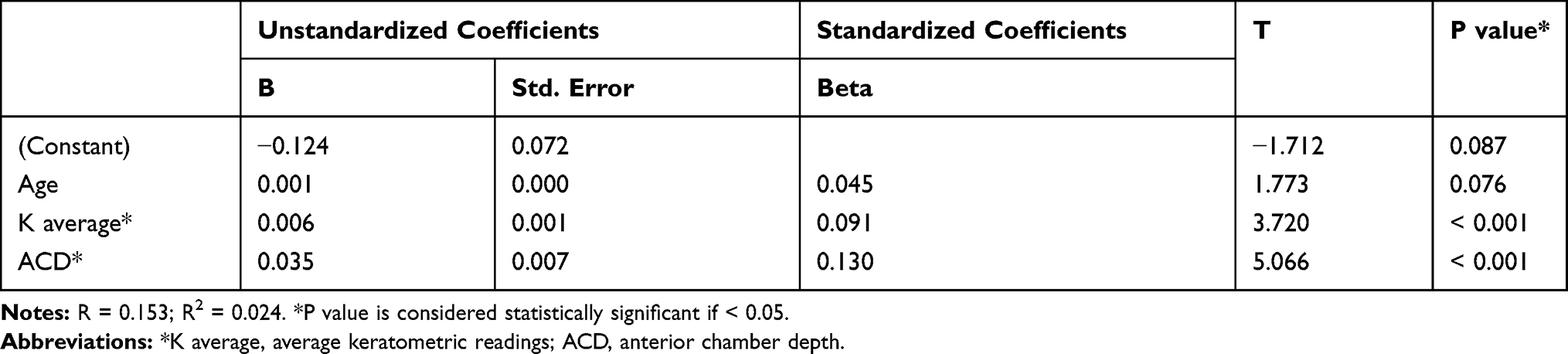 |
Table 3 Multivariate Linear Regression Analysis for the Factors Affecting the Value of Corneal Spherical Aberration (Z4) |
For the pupil size parameter, the multivariate analysis also showed weak but significant relations between both P. Pupil and M. Pupil and each of age (beta coefficient= −0.106 and −0.165, respectively) and ACD (beta coefficient = 0.135 and 0.252, respectively), with r2= 0.043 and 0.130, respectively. The results of the multivariate analyses for the pupil size are detailed in Tables 4 and 5.
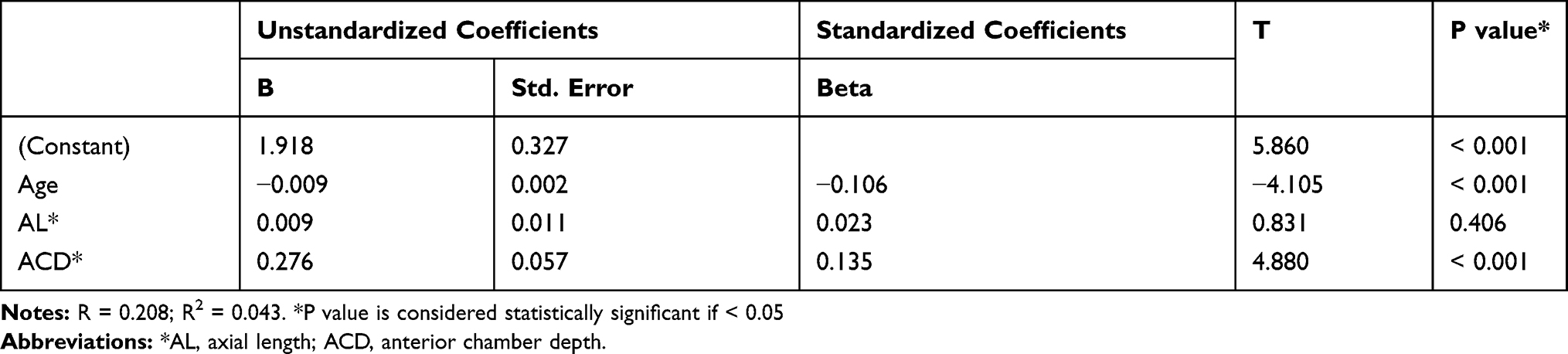 |
Table 4 Multivariate Linear Regression Analysis for the Factors Affecting the Diameter of the Photopic Pupil |
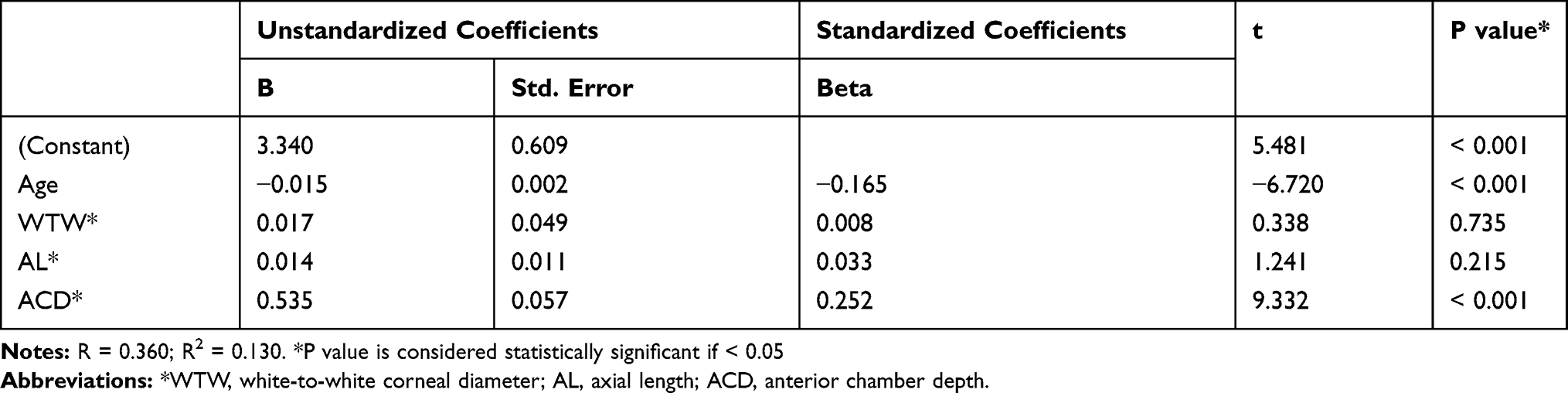 |
Table 5 Multivariate Linear Regression Analysis for the Factors Affecting the Diameter of the Mesopic Pupil |
Discussion
We report on the mean normative values of the Z4 and other key anterior segment parameters of 1658 right eyes of Egyptians who were all candidates for cataract surgery. We found that the mean Z4 in our studied sample was +0.26 (±0.12) μm, and that the Z4 was significantly (yet weakly) related to average K and ACD. To our knowledge, this is the first study to report on combined normative refractive and topographic data of a large sample of the Egyptian population.
Our reported mean Z4 value is different from the reported ranges in some studies conducted on different populations, like that conducted by Lai and colleagues11 on a Taiwanese population (with a mean Z4 of +0.31 ± 0.14 μm), another study by Lim and Fam12 on a Chinese population (mean Z4 of +0.31 (±0.11) μm), a third report by Al-Sayyari et al,13 on a Saudi population (mean Z4 +0.21 ± 0.07 μm), and a study by Shimozono and his co-workers14 on a Japanese population (mean Z4 +0.20 ± 0.10 μm). Contrarily, other studies detected very close values for the Z4 compared to our study results.5,16,17 Hence, the ethnic variations can alter the Z4 values and should be taken into consideration while planning for all the clinical implications that rely on the Z4, including but not limited to the IOL power selection, the IOL asphericity, and the refractive surgeries.
Regarding the refractive and topographic factors that may affect the Z4, we found a weak but statistically significant relation to both average K and ACD. Studies that reported correlations between Z4 and different variables had little consensus over the predictors of Z4. Lai et al,11 and Shimozono et al,14 both reported a negative significant correlation between Z4 and AL, Lim and Fam12 detected no correlations between Z4 and other refractive parameters, while Al-Sayyari et al13 reported a positive correlation between Z4 and age.
Other than ethnic variations, it is to be kept in mind that many factors may explain the varying mean Z4 measurements and the variations in the reported correlations with other parameters and should not be overlooked. Those factors may include variations in the methods of measurement and instruments used, variations in the sample size, together with variations in the studied age groups. Our studied cohort was an elderly one who were candidates for cataract surgery, and this may partially explain the variable values than other studies.
Other variables generated by our study included the mean WTW (11.72 ± 0.44), average K (43.89 ± 1.89 D), AL (24.23 ± 2.21 mm), and ACD (3.16 ± 0.43 mm). Those were all within the normative value ranges reported in the literature.18–20 Newer fourth-generation biometric formulas rely on normative values of such parameters to accurately predict the IOL power.21 Thus, our results validate the usage of such formulas in our studied population.
We also reported the mean pupil size (P. Pupil and M. Pupil) in our sample. Our mean M. Pupil size was smaller than that reported in a very large cohort of German subjects (6.45 mm),22 and a small sample of Turkish patients (6.39 mm).23 This could be attributed to the higher mean age of our participants who primarily sought medical advice for performing cataract surgery, as age is known to negatively correlate with pupil size.24 The reported dynamic pupil size has got major clinical implications in our studied population, most importantly while choosing pupil-dependent multifocal IOLs.25,26 Furthermore, both pupil size and Z4 are key factors for optimized aspheric IOL implantation.27 Paucity of studies on our population that determine such parameters validated the aim of our study, especially with the relevant clinical implications that would make benefit from the normative values of such parameters.
Though our study depicted a relation between each of the Z4, P. Pupil and M. Pupil and other related refractive and topographic parameters, both the univariate and the multivariate analyses showed weak correlation. Based on our study results, we believe that the detected relations of both the Z4 and the pupil sizes have a weak clinical relevance due to the small values of the detected correlations, which were weaker when the multivariate analyses were performed. Worthy of mention is that the detected correlations in the literature between the Z4 and the various refractive parameters were all weak ones (not exceeding 0.3 in any of the aforementioned studies). We believe that those weak correlations, should be regarded as having a weak clinical relevance, in accordance with our study results.
Limitations to our work include the single method of measurement of the Z4 and the refractive variables, the limitation of the studied age group (cataract patients, predominantly elderly), and the study being single-centered. Further studies are needed to validate our data and reinforce or reject our suggested values. Furthermore, other studies utilizing multivariate analyses are recommended to detect the strength of correlation between the studied parameters and their clinical relevance.
In conclusion, this is the first normative data report of an Egyptian population regarding the Z4 and many key refractive and topographic parameters. Further studies could reinforce whether ethnic variations in Z4 are true ones, and even larger cohorts with proper multivariate analyses would be more conclusive regarding the predictors of the Z4.
Code Availability
Not available.
Data Sharing Statement
Available from the corresponding author upon request.
Ethics Approval
The study adhered to the Tenets of the Declaration of Helsinki and was approved by the Ethical Committee of Ain Shams University.
Consent to Participate
Participants have signed consent to participate.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Drexler W, Findl O, Menapace R, et al. Partial coherence interferometry: a novel approach to biometry in cataract surgery. Am J Ophthalmol. 1998;126(4):524–534. doi:10.1016/S0002-9394(98)00113-5
2. Findl O, Drexler W, Menapace R, et al. Improved prediction of intraocular lens power using partial coherence interferometry. J Cataract Refract Surg. 2001;27(6):861–867. doi:10.1016/S0886-3350(00)00699-4
3. Dong J, Zhang Y, Zhang H, et al. Comparison of axial length, anterior chamber depth and intraocular lens power between IOLMaster and ultrasound in normal, long and short eyes. PLoS One. 2018;13(3):e0194273–e0194273. doi:10.1371/journal.pone.0194273
4. Best N, Drury L, Wolffsohn JS. Clinical evaluation of the Oculus Keratograph. Cont Lens Anterior Eye. 2012;35(4):171–174. doi:10.1016/j.clae.2012.04.002
5. Beiko GH, Haigis W, Steinmueller A. Distribution of corneal spherical aberration in a comprehensive ophthalmology practice and whether keratometry can predict aberration values. J Cataract Refract Surg. 2007;33(5):848–858. doi:10.1016/j.jcrs.2007.01.035
6. Zhang M, Qian D, Jing Q, et al. Correlations of corneal spherical aberration with astigmatism and axial length in cataract patients. J Ophthalmol. 2019;2019:4101256. doi:10.1155/2019/4101256
7. Guirao A, Tejedor J, Artal P. Corneal aberrations before and after small-incision cataract surgery. Invest Ophthalmol Vis Sci. 2004;45(12):4312–4319. doi:10.1167/iovs.04-0693
8. Fuller DG, Alperin D. Variations in corneal asphericity (q value) between african-americans and whites. Optom Vis Sci. 2013;90(7):667–673. doi:10.1097/OPX.0b013e318296befe
9. Lindsay R, Smith G, Atchison D. Descriptors of Corneal Shape. Optom Vis Sci. 1998;75(2):156–158. doi:10.1097/00006324-199802000-00019
10. Rozema JJ, Atchison DA, Tassignon MJ. Statistical eye model for normal eyes. Investig Opthalmology Vis Sci. 2011;52(7):4525. doi:10.1167/iovs.10-6705
11. Lai YJ, Yeh SI, Cheng HC. Distribution of corneal and ocular spherical aberrations in eyes with cataract in the Taiwanese population. Taiwan J Ophthalmol. 2015;5(2):72–75. doi:10.1016/j.tjo.2015.03.003
12. Lim KL, Fam HB. Ethnic differences in higher-order aberrations: spherical aberration in the South East Asian Chinese eye. J Cataract Refract Surg. 2009;35(12):2144–2148. doi:10.1016/j.jcrs.2009.06.031
13. Al-Sayyari TM, Fawzy SM, Al-Saleh AA. Corneal spherical aberration in Saudi population. Saudi J Ophthalmol. 2014;28(3):207–213. doi:10.1016/j.sjopt.2014.03.003
14. Shimozono M, Uemura A, Hirami Y, et al. Corneal spherical aberration of eyes with cataract in a Japanese population. J Refract Surg. 2010;26(6):457–459. doi:10.3928/1081597X-20100212-03
15. Keita SOY, Boyce AJ. Genetics, Egypt, and history: interpreting geographical patterns of y chromosome variation. Hist Afr. 2005;32:221–246. doi:10.1353/hia.2005.0013
16. Wang L, Dai E, Koch DD, Nathoo A. Optical aberrations of the human anterior cornea. J Cataract Refract Surg. 2003;29(8):1514–1521. doi:10.1016/S0886-3350(03)00467-X
17. Holladay JT, Piers PA, Koranyi G, et al. A new intraocular lens design to reduce spherical aberration of pseudophakic eyes. J Refract Surg. 2002;18(6):683–691.
18. Hashemi H, Khabazkhoob M, Emamian MH, et al. White-to-white corneal diameter distribution in an adult population. J Curr Ophthalmol. 2015;27(1–2):21–24. doi:10.1016/j.joco.2015.09.001
19. Almorin-Fernandez-Vigo I, Sanchez-Guillen I, Fernandez-Vigo JI, et al. Normative Pentacam anterior and posterior corneal elevation measurements: effects of age, sex, axial length and white-to-white. Int Ophthalmol. 2019;39(9):1955–1963. doi:10.1007/s10792-018-1028-6
20. Chen H, Lin H, Lin Z, et al. Distribution of axial length, anterior chamber depth, and corneal curvature in an aged population in South China. BMC Ophthalmol. 2016;16(1):47. doi:10.1186/s12886-016-0221-5
21. Darcy K, Gunn D, Tavassoli S, et al. Assessment of the accuracy of new and updated intraocular lens power calculation formulas in 10 930 eyes from the UK National Health Service. J Cataract Refract Surg. 2020;46(1):2–7. doi:10.1016/j.jcrs.2019.08.014
22. Linke SJ, Baviera J, Munzer G, et al. Mesopic pupil size in a refractive surgery population (13,959 eyes). Optom Vis Sci. 2012;89(8):1156–1164. doi:10.1097/OPX.0b013e318263c165
23. Cakmak HB, Cagil N, Simavli H, et al. Corneal white-to-white distance and mesopic pupil diameter. Int J Ophthalmol. 2012;5(4):505–509. doi:10.3980/j.issn.2222-3959.2012.04.19
24. Guillon M, Dumbleton K, Theodoratos P, et al. The effects of age, refractive status, and luminance on pupil size. Optom Vis Sci. 2016;93(9):1093–1100. doi:10.1097/OPX.0000000000000893
25. Salerno LC, Tiveron MC
26. Ouchi M, Shiba T. Diffractive multifocal intraocular lens implantation in eyes with a small-diameter pupil. Sci Rep. 2018;8(1):11686. doi:10.1038/s41598-018-30141-1
27. Du W, Lou W, Wu Q. Personalized aspheric intraocular lens implantation based on corneal spherical aberration: a review. Int J Ophthalmol. 2019;12(11):1788–1792. doi:10.18240/ijo.2019.11.19
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.