Back to Journals » Clinical Ophthalmology » Volume 16
Normative Data of Macular Thickness Using Spectral Domain Optical Coherence Tomography for Healthy Jordanian Children
Authors Jammal HM ![]() , Al-Omari R
, Al-Omari R ![]() , Khader Y
, Khader Y ![]()
Received 20 August 2022
Accepted for publication 11 October 2022
Published 20 October 2022 Volume 2022:16 Pages 3571—3580
DOI https://doi.org/10.2147/OPTH.S386946
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hisham M Jammal,1 Rami Al-Omari,2 Yousef Khader3
1Department of Ophthalmology, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan; 2Department of Ophthalmology, Faculty of Medicine, Yarmouk University, Irbid, Jordan; 3Department of Public Health, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan
Correspondence: Hisham M Jammal, Department of Ophthalmology, Faculty of Medicine, Jordan University of Science and Technology, PO Box 1099, Irbid, 21110, Jordan, Tel +962-2-7201000, Fax + 962-2-7095123, Email [email protected]
Purpose: To report normative values of macular thickness and volume by spectral-domain optical coherence tomography (SD-OCT) in the eyes of healthy Jordanian children aged 6– 16 years and assess the correlation of macular parameters with age, sex, and refractive error.
Patients and Methods: This observational study included 144 eyes of 144 healthy children. All children underwent comprehensive ocular examination and cycloplegic refraction. Average macular thickness, macular volume, central subfield thickness (CST), and macular thickness for all the Early Treatment Diabetic Retinopathy Study (ETDRS) quadrants were obtained using Primus SD-OCT (Carl Zeiss Meditec).
Results: The study group consisted of 68 boys and 76 girls with a mean age (SD) of 10.8 (3.0) years. The mean (SD) spherical equivalent refraction (SER) was 0.56 (1.73) diopters (range: − 4.75 to 4.75). The mean of macular average thickness was 277.2± 12.5 μm, and the mean of the central subfield thickness was 246.7± 16.8 μm. In multivariate analysis, all macular parameters except the central subfield thickness (CST) correlated positively with the SER. Boys had significantly higher CST than girls (p=0.008). None of the macular parameters were correlated with age.
Conclusion: Normative data of macular thickness for healthy Jordanian children were established for sex and age groups using SD-OCT.
Keywords: central subfield thickness, macular thickness, normative data, pediatric OCT, Primus OCT
Introduction
Optical coherence tomography (OCT) is a well-established method for acquiring high-resolution images of the retina and optic disc. Its main advantages include being noninvasive, objective, reliable, with good repeatability and reproducibility1 in both adult and pediatric populations. Besides providing a morphological assessment of the retina and optic disc, it also provides accurate quantitative measurements that help diagnose and monitor the progression or response to treatment of many retinal pathologies.
Despite the expected difficulties when performing OCT in children, where it requires a certain degree of cooperation and attention, OCT has proven to be well tolerated in children and has many clinical applications in pediatric retinal and optic disc pathologies.2
Different OCT machines come preloaded with normative data on retinal parameters for adults (18 years and older) derived from certain ethnic groups, but not for children, and this may limit the value of OCT in the pediatric setup since the diagnosis of early retinal or optic disc pathologies requires knowledge of normal OCT values of the studied tissue. Many published papers reported such normative data on macular thickness and volume in normal children among different ethnic groups using spectral-domain OCT (SD-OCT), and the reported data varied with race and other factors, however, only two reports come from the Middle East.3,4 To the best of our knowledge, normative macular thickness OCT data for Jordanian children have not been published previously.
The purpose of this study was to report normative data on macular thickness and volume measured by SD-OCT in normal eyes of healthy children in Jordan and assess its correlation with age, sex, and refractive error.
Materials and Methods
Design and Study Population
An observational study was performed on 144 consecutive healthy Middle Eastern children aged between 6 and 16 years who presented to a comprehensive ophthalmic outpatient clinic in Irbid, Jordan. The study adhered to the tenets of the Helsinki declaration and was approved by the Jordan University of Science and Technology Institutional Review Board. Informed written consent was signed by parents (guardian) of the participating children.
The participating children attended the eye clinic for routine refraction, or for vision screening on the request of parents or school, and were healthy, born term (≥37 weeks gestational age), with no history of systemic metabolic or CNS diseases, no history of ocular abnormalities such as retinal or optic nerve pathology, corneal diseases, strabismus, amblyopia, glaucoma, no history of significant ocular trauma and no history of intraocular surgery. Children were also included if they had monocular best corrected visual acuity of 1.0 in both eyes (Snellen’s chart or the Tumbling E chart), normal anterior and posterior segment examination, and no abnormality of extraocular motility and ocular alignment examination.
We excluded children with high refractive errors of more than ± 5 diopters of spherical equivalent refraction (SER), anisometropia >1.5 diopters SER, children with abnormally looking foveal reflex, optic discs with a cup/disc ratio >0.5 (or >0.2 asymmetry between the two eyes), optic disc anomalies such as a tilted disc, and uncooperative children for OCT imaging.
Demographic data was recorded including age, sex, general medical history, and family history of inherited ophthalmic diseases. The children were separated into three groups according to age; group 1: <10, group 2: 10–12, and group 3: >12 years.
Ocular Examination
All participating children underwent a standard ophthalmic examination. Best corrected visual acuity was recorded monocularly using the Snellen’s chart or the Tumbling E chart, followed by assessment of ocular alignment, extraocular motility testing, and anterior segment examination with a slit lamp. All children underwent cycloplegic refraction using cyclopentolate 1% eye drops instilled in each eye 10 minutes apart. Cycloplegic refraction was measured 50 minutes after the last drop using an autokeratorefractometer (ARK-1s, Nidek, Aichi, Japan), which provides the median of at least 3 measurements. Astigmatism was recorded as the negative cylinder and spherical equivalent refraction was calculated according to the equation: SER = sphere power +(1/2 cylinder power). Dilated fundus examination was then performed using slit-lamp biomicroscopy and indirect ophthalmoscopy.
OCT Measurement
The Primus SD-OCT machine (Carl Zeiss Meditec AG, Germany, model 200, software version 3.0) was used to acquire macular OCT images through the dilated pupil. It acquires retinal images using a super luminescent diode with a wavelength of 840 nm at a scanning speed of 12,000 A-scans per second and has an axial tissue resolution of 5 μm and a transverse resolution of ≤20 μm. The device has been shown to have good repeatability and reproducibility for both normal and diseased eyes.5 Additionally, there was a substantial equivalence between the PRIMUS 200 and Cirrus HDOCT Model 4000,5 and a substantial level of agreement in normative limits between normative databases of Primus 200 and Cirrus for the measurement parameters obtained from a given subject.6
The macular thickness analysis scan protocol generates a cube of data through a 6 mm square grid centered on the fovea by acquiring a series of 32 horizontal scan lines each composed of 512 A-scans. The machine displays the thickness measurements over a circular map which is a modified ETDRS (Early Treatment Diabetic Retinopathy Study) Grid and calculates the total macular volume and overall macular average thickness for the ILM-RPE tissue layer over the entire 6 mm square scanned area. The modified ETDRS grid map shows overall average thickness in nine sectors. This circular map is automatically centered on the fovea and is composed of three concentric circles: the central circle with a diameter of 1 mm corresponding to the foveal central 1mm circle, and its thickness is referred to as Central Subfield Thickness (CST), the inner circle, 3 mm in diameter, and the outer circle 6 mm in diameter. Both inner and outer circles are divided into superior, nasal, inferior and temporal quadrants. The macular thickness analysis map obtained by the Primus OCT of the measured and calculated macular parameters is shown in Figure 1.
 |
Figure 1 Macular thickness analysis map. Cube volume: macular volume, cube avg thickness: average macular thickness. |
All OCT scans were performed by a single experienced operator utilizing the same OCT machine and during the same day of conducting ocular examination and cycloplegic refraction. The right eye was scanned first followed by the left eye. Internal fixation light was used, and the procedure carried out in a dim room. Three to four images were taken for each eye and then reviewed individually by the operator. Images with poor signal strength (less than 7/10), poorly centered, those with motion artifacts, and images with dark areas were excluded with the purpose of having at least 2 images with acceptable quality.
The two authors reviewed all images and by consensus, selected the image with the highest signal strength, best centration, and no missing data.
Statistical Analysis
The data from the left eye were used for analysis and were analyzed using the Statistical Package for the Social Sciences (SPSS) version 26 (IBM corporation, Armonk, NY, USA). The normality of distributions for the measured macular parameters were tested using the Shapiro–Wilk test. Mean (± standard deviation) as well as 5th and 95th percentiles were used to describe the macular parameters. Percentages were used to describe categorical variables. Pearson correlation was used to test the correlation between the measured macular parameters and other variables. The generalized linear model (GLM) multivariate procedure was used for testing the effect of different variables on macular parameters. The GLM Multivariate procedure provided regression analysis and analysis of variance for multiple macular parameters by sex, age, and SER. A p-value of less than 0.05 was considered statistically significant.
Results
The data on the left eyes of 144 children (68 boys and 76 girls) were analyzed. Their age ranged from 6 years to 16 years with a mean (SD) age of 10.8 (3.0) years. A total of 49 (34%) children aged <10 years, 49 (34%) aged between 10 and 12 years, and 46 (31.9%) aged >12 years. The mean (SD) spherical equivalent refraction was 0.56 (1.73) diopters (Range: −4.75 to 4.75). Table 1 shows sex and spherical equivalent refraction according to age groups. The mean of macular average thickness was 277.2±12.5 μm, and the mean of the central subfield thickness was 246.7±16.8 μm. The macular thickness measurements in the 9 ETDRS grid sectors, the average macular thickness, and the total macular volume according to age groups and sex are shown in Table 2.
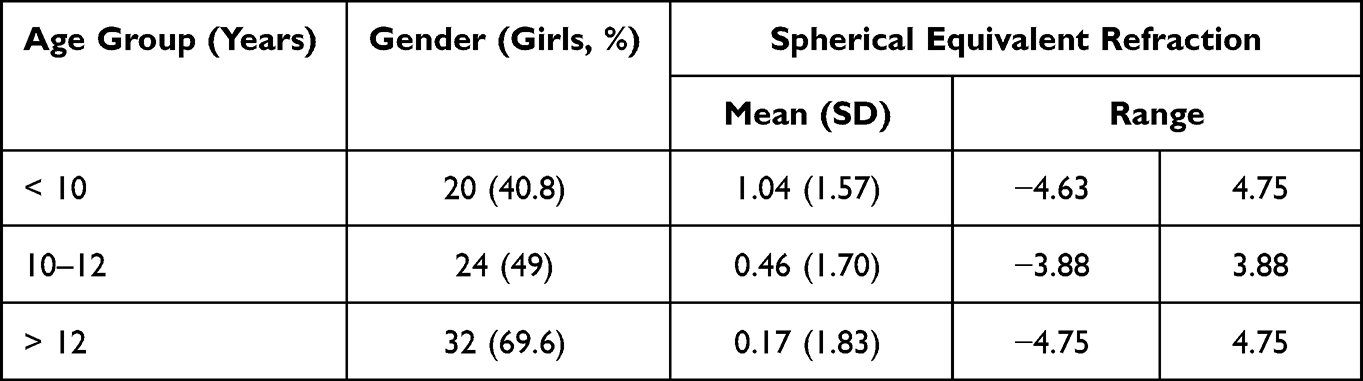 |
Table 1 Sex and Spherical Equivalent Refraction According to Age Groups |
 |
Table 2 Normative Values of Macular Parameters According to Sex and Age Groups |
All the macular measurements, average macular thickness, and the total macular volume were weakly and positively correlated with the SER (p<0.05) except the central subfield thickness (p =0.79).
Using the GLM Multivariate Analysis (Table 3), age was not significantly associated with all studied macular parameters. There was no significant sex difference in all parameters, except for central subfield thickness. The adjusted mean of central subfield thickness was significantly higher in boys (250.68 μm (95% CI: 246.68, 254.68)) compared to girls (243.06 μm (95% CI: 239.29, 246.84)). As the SER increased, all macular parameters, except central subfield thickness, significantly increased. There was no significant interaction between age, sex, and SER for all macular parameters. The overall sex, age, and SER adjusted means of all macular parameters are shown in Table 4.
 |
Table 3 Multivariate Analysis of the Association Between Macular Measurements and Sex, Age, and Spherical Equivalent Refraction |
 |
Table 4 Sex, Age, and Spherical Equivalent Refraction Adjusted Means of All Macular Parameters |
Discussion
Optical coherence tomography has become an established and indispensable method for the diagnosis and monitoring of many retinal and optic nerve diseases in the pediatric population, however the technique is still underutilized in this population because of expected difficulties when performing the test and more importantly, lack of normative database.2 Although OCT in children proved to be repeatable and reproducible,1 normative data are still not provided by the OCT manufacturers in their machines for subjects younger than 18 years, and therefore, the provision of such data is still a necessity.7 The current study reported the normative data for macular thickness and macular volume in a sample of healthy Middle Eastern children from Jordan and examined the effect of sex, age, and refractive errors on these data.
In the current study, the mean of macular average thickness was 277.2±12.5 μm, and the mean of the central subfield thickness was 246.7±16.8 μm. Those measurements were comparable to those reported by studies that used the Cirrus SD-OCT,3,8–13 which ranged from 271 μm to 289 μm for the macular average thickness, and from 235 μm to 255 μm for the central subfield thickness. In particular, our results for the macular average thickness and CST were very close to those reported by Al-Haddad3 (279.6±12.5 μm, 249.1±20.2 μm, respectively) in the only study performed using Cirrus SD-OCT on a sample of Middle Eastern children from Lebanon, with nearly similar age distribution (10.7±3.1 years). Similarly, the means of the inner and outer ETDRS grid quadrants from the current study were comparable to those from the other studies using Cirrus SD-OCT.3,8–13 Although OCT measurements from different machines cannot be used interchangeably, the Primus SD-OCT machine used in the current study and the Cirrus SD-OCT are both made by the same manufacturer, use the same technology, and both machines provided very similar mean values of macular parameters when a comparative analysis was performed for both machines.5 The average macular thickness and CST were found to be less in general when compared to those reported by studies conducted using the Spectralis SD-OCT,14–18 which is known to give higher values due to different measurement algorithms and software used in different machines.19 It is important to note that the value of comparisons between the current study’s results and those of other research may be limited by the influence of age range, refractive error state, type and size of the studied sample, ethnicity, and methodology.
Regarding age, the current study sample involved a wide range of ages but excluded those younger than 6 years for the expected lack of cooperation. We did not find a significant association between age and the measured macular parameters, in line with several previous reports.12,14,20–24 However, other studies reported a relation between age and the following: CST,8,9,11,15,17,18,25 specific segmented retinal layers,26–28 macular volume,17,18 all macular parameters,3,13 and CST in black but not white children.29 These results are variable regarding the measured anatomical area and therefore, cannot be generalized. A longitudinal study design would be preferable for establishing a relationship between age and macular characteristics.
We found a significantly higher CST in boys than girls, but other macular parameters showed no sex difference. Many studies reported a sex difference particularly in CST, with males showing higher values than females,3,4,8–11,13,21 while other studies reported no difference, and we found no reports showing higher values in females regarding macular parameters. This sex difference is also noted in the adult population,30,31 however Wexler31 found that this sex difference became non-significant in subjects older than 43 years and suggested that sex difference in the younger adults (<43 years) is due to gonadal hormonal effect.
The spherical equivalent refractive (SER) error was positively correlated with all the macular parameters measured in this study but showed no correlation with the CST. The results of association between SER and macular parameters from previous research are variable. While positive correlation was reported between SER and various macular parameters in several studies,3,10,13,18,21,32,33 it is interesting to note that all of these studies, except the study by Huynh et al32 showed either a negative correlation10,13,21,33 or no correlation with the CST.3,18 Additionally, several authors4,8,12,14,16,17 reported no association between SER and any of the measured macular parameters, including the CST. It is still unclear why the CST remains normal or even thicker with smaller SER, but the explanation by Wakitani34 seems a plausible one, in which decreased peripheral retinal thickness in myopia may act as a compensatory mechanism to preserve central macular thickness.
The current study has a limitation in that it is single-center, clinic-based rather than multi-center, hospital-based design which would reduce selection bias. Another limitation is that ocular axial length was not measured, and therefore the effect of axial length and ocular magnification could not be assessed.
Conclusion
The current study presented normative data on macular thickness measurements in healthy Jordanian children aged 6–16 years using SD-OCT. In general, these data were comparable to those from the Middle East, and other regions internationally. The effect of age and refraction needs to be further assessed by longitudinal studies as both factors continuously change with time. Finally, we recommend that OCT manufacturers include normative database in their OCT machines through carefully designed, international multicenter studies.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board at the Jordan University of Science and Technology (Reference number 26-140-2021). Informed consent was obtained from all subjects (guardians) involved in the study.
Author Contributions
All authors made a significant contribution to the conception, study design, execution, acquisition of data, analysis and interpretation; took part in drafting, revising and critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Larsson E, Molnar A, Holmstrom G. Repeatability, reproducibility and interocular difference in the assessment of optic nerve OCT in children—a Swedish population-based study. BMC Ophthalmol. 2018;18. doi:10.1186/s12886-018-0940-x
2. Maccora KA, Sheth S, Ruddle JB. Optical coherence tomography in paediatric clinical practice. Clin Exp Optom. 2019;102(3):300–308. doi:10.1111/cxo.12909
3. Al-Haddad C, Barikian A, Jaroudi M, Massoud V, Tamim H, Noureddin B. Spectral domain optical coherence tomography in children: normative data and biometric correlations. BMC Ophthalmol. 2014;14. doi:10.1186/1471-2415-14-53
4. Ali AN, Farag RK, Wahab TAAE, Ghanem AA. Macular and retinal nerve fiber layer analysis by optical coherence tomography in normal children. ARC J Ophthalmol. 2018;3(1):17–28.
5. Carl Zeiss Meditec Primus 200 OCT 501(k) premarket report of FDA. Available from: https://www.accessdata.fda.gov/cdrh_docs/pdf16/K163195.pdf.
6. Patel KR, Ganesh Babu TC, Natesh S. Comparative analysis: to assess the level of agreement between PRIMUS (ZEISS India) and CIRRUS (ZEISS Dublin CA) SD-OCT Normative Database limits. Invest Ophthalmol Vis Sci. 2016;57(12):4229.
7. Banc A, Ungureanu MI. Normative data for optical coherence tomography in children: a systematic review. Eye. 2020;35(3):714–738. doi:10.1038/s41433-020-01177-3
8. Barrio-Barrio J, Noval S, Galdos M, Ruiz-Canela M, Bonet E, Capote M. Multicenter Spanish study of spectral-domain optical coherence tomography in normal children. Acta Ophthalmol. 2013;91(1):e56–e63. doi:10.1111/j.1755-3768.2012.02562.x
9. Katiyar V, Mugdha K, Bangwal S, Gupta SK. Normative macular Cirrus spectral domain optical coherence tomography data in Indian pediatric population. Egypt Retin J. 2013;1(3):50. doi:10.4103/2347-5617.143818
10. Chen S, Wang B, Dong N, Ren X, Zhang T, Xiao L. Macular measurements using spectral-domain optical coherence tomography in Chinese myopic children. Investig Ophthalmol Vis Sci. 2014;55(11):7410–7416.
11. Queiros T, Freitas C, Guimaraes S. Normative database of optical coherence tomography parameters in childhood. Acta Med Port. 2015;28(2):148–157.
12. Molnar A, Holmstrom G, Larsson E. Macular thickness assessed with spectral domain OCT in a population-based study of children: normative data, repeatability and reproducibility and comparison with time domain OCT. Acta Ophthalmol. 2015;93(5):470–475. doi:10.1111/aos.12695
13. Guragac FB, Totan Y, Guler E, Tenlik A, Ertugrul IG. Normative spectral domain optical coherence tomography data in healthy Turkish children. Semin Ophthalmol. 2017;32(2):216–222. doi:10.3109/08820538.2015.1053625
14. Turk A, Ceylan OM, Arici C, et al. Evaluation of the nerve fiber layer and macula in the eyes of healthy children using spectral-domain optical coherence tomography. Am J Ophthalmol. 2012;153(3):552–559.e1. doi:10.1016/j.ajo.2011.08.026
15. Yanni SE, Wang J, Cheng CS, et al. Normative reference ranges for the retinal nerve fiber layer, macula, and retinal layer thicknesses in children. Am J Ophthalmol. 2013;155(2):354–360.e1. doi:10.1016/j.ajo.2012.08.010
16. Lee JWY, Yau GSK, Woo TTY, Lai JSM. The association between macular thickness and peripapillary retinal nerve fiber layer thickness in Chinese children. Medicine. 2015;94:e567.
17. Perez-Garcia D, Ibanez-Alperte J, Remon L, Cristobal JA, Sanchez-Cano A, Pinilla I. Study of spectral-domain optical coherence tomography in children: normal values and influence of age, sex, and refractive status. Eur J Ophthalmol. 2016;26(2):135–141. doi:10.5301/ejo.5000665
18. Passani A, Sframeli AT, Posarelli C, et al. Macular spectral-domain optical coherence tomography values and correlations in healthy children. Int Ophthalmol. 2019;39(11):2449–2457. doi:10.1007/s10792-019-01085-w
19. Sander B, Al-Abiji HA, Kofod M, Jørgensen TM. Do different spectral domain OCT hardwares measure the same? Comparison of retinal thickness using third-party software. Graefes Arch Clin Exp Ophthalmol. 2015;253(11):1915–1921. doi:10.1007/s00417-015-3075-2
20. Eriksson U, Holmstrom G, Alm A, Larsson E. A population-based study of macular thickness in full-term children assessed with Stratus OCT: normative data and repeatability. Acta Ophthalmol. 2009;87(7):741–745. doi:10.1111/j.1755-3768.2008.01357.x
21. Zhang Z, He X, Zhu J, Jiang K, Zheng W, Ke B. Macular measurements using optical coherence tomography in healthy Chinese school age children. Invest Ophthalmol Vis Sci. 2011;52(9):6377–6383. doi:10.1167/iovs.11-7477
22. Sushil O, Vaibhav J, Reena S, Brijesh S, Dipendra S. OCT normative database of macula in the paediatric population. Indian J Clin Exp Ophthalmol. 2015;1(4):238. doi:10.5958/2395-1451.2015.00021.9
23. Nigam B, Garg P, Ahmad L, Mullick R. OCT based macular thickness in a normal Indian pediatric population. J Ophthalmic Vis Res. 2018;13(2):144–148. doi:10.4103/jovr.jovr_51_17
24. Read SA, Alonso-Caneiro D, Vincent SJ, Paul F. Longitudinal changes in macular retinal layer thickness in pediatric populations: myopic vs non-myopic eyes. PLoS One. 2017;12(6):e0180462. doi:10.1371/journal.pone.0180462
25. Read SA, Collins MJ, Vincent SJ, Alonso-Caneiro D. Macular retinal layer thickness in childhood. Retina. 2015;35(6):1223–1233. doi:10.1097/IAE.0000000000000464
26. Rotruck JC, House RJ, Freedman SF, et al. Optical coherence tomography normative peripapillary retinal nerve fiber layer and macular data in children 0–5 years of age. Am J Ophthalmol. 2019;208:323–330. doi:10.1016/j.ajo.2019.06.025
27. Munoz-Gallego A, Cruz J, Rodriguez-Salgado M, Torres-Pena JL, Lucas-Viejo B, Ortueta-Olartecoechea A. Assessment of macular ganglion cell complex using optical coherence tomography: impact of a paediatric reference database in clinical practice. Clin Exp Ophthalmol. 2018;47(4):490–497. doi:10.1111/ceo.13418
28. Galdos M, Barrio-Barrio J, Noval S, et al. Multicenter macular ganglion cell analysis: normative paediatric reference range. Acta Ophthalmol. 2014;92(4):e326–327. doi:10.1111/aos.12316
29. El-Dairi MA, Asrani SG, Enyedi LB, Freedman SF. Optical coherence tomography in the eyes of normal children. Arch Ophthalmol. 2009;127(1):50–58. doi:10.1001/archophthalmol.2008.553
30. Wong ACM, Chan CWN, Hui SP. Relationship of gender, body mass index, and axial length with central retinal thickness using optical coherence tomography. Eye. 2005;19(3):292–297. doi:10.1038/sj.eye.6701466
31. Wexler A, Sand T, Elsås TB. Macular thickness measurements in healthy Norwegian volunteers: an optical coherence tomography study. BMC Ophthalmol. 2010;10(1):13. doi:10.1186/1471-2415-10-13
32. Huynh SC, Wang XY, Rochtchina E, Mitchell P. Distribution of macular thickness by optical coherence tomography: findings from a population-based study of 6-year-old children. Investig Ophthalmol Vis Sci. 2006;47(6):2351–2357.
33. Sultan M, Hamza SA, Shah MA, Khan MN, Saeed N. Comparison of macular thickness between highly myopic and normal children aged 5 to 8 years using optical coherence tomography. J Postgrad Med Inst. 2018;32:76–79.
34. Wakitani Y, Sasoh M, Sugimoto M, Ito Y, Ido M, Uji Y. Macular thickness measurements in healthy subjects with different axial lengths using optical coherence tomography. Retina. 2003;23(2):177–182. doi:10.1097/00006982-200304000-00007
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.