Back to Journals » Medical Devices: Evidence and Research » Volume 15
Nonclinical Bench Performance Testing of a Very Low-Cost Nonelectric Bubble Continuous Positive Airway Pressure (bCPAP) and Blenders Device Designed for Newborn Respiratory Support
Received 9 February 2022
Accepted for publication 16 May 2022
Published 27 June 2022 Volume 2022:15 Pages 187—197
DOI https://doi.org/10.2147/MDER.S318218
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Patricia S Coffey, Alec Wollen
Medical Devices and Health Technologies, PATH, Seattle, Washington, USA
Correspondence: Patricia S Coffey, Medical Devices and Health Technologies, PATH, Seattle, WA, USA, Tel +1 206 285-3500, Fax +1 206 285-6619, Email [email protected]
Purpose: Bubble continuous positive airway pressure (bCPAP) is often used to treat respiratory distress experienced by some 15 million preterm infants born globally every year. In low- and middle-income countries, improvised bCPAP devices are used, often without a blender that protects the infant from the sequelae of excessive oxygen exposure.
Materials and Methods: The aim of this bench testing was to assess the mechanical safety and performance of the PATH bCPAP and blenders device, which provides a stable and reliable source of pressurized blended gas without the requirement for a source of compressed medical air or electricity. The device includes two fixed ratio blenders: a “low” blend that provides 37% oxygen and a “high” blend that provides 60% oxygen. We performed bench testing to characterize the performance of the bCPAP and blenders, including respiratory circuit verification, blender verification, conditioned humidity testing, and sound measurement.
Results: Test results for all performance variables met the acceptance criteria of our product requirement specification. The device provides a fixed ratio of air and oxygen that is consistent over the entire range of clinically relevant pressures (4 to 8 cmH2O) and remains consistent despite changes in flow (2 to 7 liters per minute). The blend is stable within ± 5% of the blenders’ nominal blend ratio when used with a 100% oxygen source, irrespective of the flow and pressure from the oxygen source or the flow and pressure of the blended gas delivered to the neonate. Sound and humidity test results were within specifications.
Conclusion: This very low-cost nonelectric bCPAP and blenders device is optimally designed to deliver a stable and reliable source of pressurized blended gas.
Keywords: hyperoxia, respiratory distress syndrome, preterm infants, noninvasive ventilation, global health, affordability, medical device design, biomedical engineering
Introduction
Every year, about 15 million babies are born prematurely, and more than 1 million babies die due to complications of preterm birth.1,2 A serious complication of preterm birth is neonatal respiratory distress syndrome (RDS) due to insufficient lung development and lack of surfactant production. More than half of preterm infants (born at 32 weeks of gestation or less) will develop RDS.3 A lifesaving treatment commonly used in high-resource facilities to treat RDS is continuous positive airway pressure (CPAP)4,5 therapy. In resource-limited settings such as low- and middle-income countries (LMICs), commercially available CPAP devices are often unaffordable, maintenance and component resupply for repair are challenging, and the required infrastructure is lacking at facility level. As an alternative, bubble CPAP (bCPAP), which is considered to be a safe and effective6–8 therapeutic intervention, is often used to treat respiratory disease in infants and children. In some LMIC inpatient care settings, bCPAP devices are improvised by assembling tubing, connectors, nasal prongs, and a water bottle as the bubbler. These improvised devices have been promoted by many groups, including the World Health Organization (WHO),9 and provide lifesaving respiratory support. However, they generally rely on a source of 100% oxygen from a cylinder, wall supply, or oxygen concentrator and lack the ability to blend air into the gas provided to the infant. While providing an immediate lifesaving benefit, high concentrations of delivered oxygen frequently cause longer term complications10 in preterm infants, including retinopathy of prematurity,11–13 chronic lung disease,14 and brain15 damage.
The currently available oxygen blenders require compressed sources of both air and oxygen (minimum 40 pounds per square inch [psi] and minimum 10 liters per minute [LPM] output) and cost about US$1000. Hospitals in well-resourced settings generally have 50 psi of compressed oxygen and air available to blend for therapeutic use, typically piped into the ward as part of the facility infrastructure.
In LMICs, oxygen, if available, is often provided by a cylinder or oxygen concentrator. WHO technical specifications for oxygen concentrators16 are available, and oxygen concentrators are used in LMICs. While the availability of oxygen is limited in LMICs, the availability of compressed air is virtually nonexistent.17 Medical air compressors are expensive, rely on electricity, and require maintenance. Nonmedical compressors typically use industrial grade lubricants in the gas pathway, which are not suitable for medical use. Thus, even where oxygen is available, providers are unable to use it safely because they have no way to achieve the desired concentration of oxygen in the gas mixture (ie, fraction of inspired oxygen [FiO2]). An appropriate oxygen blending method to improve both oxygen delivery and availability can eliminate the need for compressed air.
Low-flow therapy is effective in mild cases of hypoxemia and requires minimal equipment and training. However, more severe diseases require high-flow therapy or positive airway pressure ventilation such as bCPAP therapy. High-flow or ventilatory support therapy, when used with oxygen, needs to incorporate an air-oxygen blender to prevent the risk of hyperoxia, particularly for newborns, and be operable without a source of electricity. Some entrainment devices (such as Venturi-style blenders) are available on the market that entrain and mix room air into a high-velocity jet of oxygen and thereby obviate the need for compressed air. These devices are designed to provide blended gases to high-flow masks and are not suitable for use in applications where there is resistance in the respiratory circuit or positive airway pressure such as in neonatal bCPAP. In addition, these devices do not provide stable oxygen blend ratios at low-flow ranges, as they were designed for adults. To address this need, we designed a very low-cost, nonelectric bCPAP and oxygen blenders device that provides a stable and reliable source of pressurized blended gas for preterm newborns with RDS to reduce the risk of brain, eye, and lung damage and death without the requirement for a source of compressed medical air.
Materials and Methods
Device Design
The PATH bCPAP device drew inspiration from an improvised bCPAP device initially conceived and employed in clinical practice in India.18 Using a human-centered design approach that included input from more than 50 CPAP users from Benin, Nigeria, South Africa, and Uganda,19 we developed a bCPAP configuration and assembly instructions that employed inexpensive components commonly found in hospitals (Figure 1).
 |
Figure 1 Bubble continuous positive airway pressure (bCPAP) assembly diagram. Contents: 1) bubbler stand, 2) cannula adapter, 3) air-oxygen blenders (37% and 60%), 4) nasal cannula, 5) bubbler straw, 6) bubbler bottle, 7) bubbler bottle lid. Circuit tubing: 8) cannula adapter to straw (140 cm), 9) cannula adapter to blender (50 cm), 10) blender to oxygen (130 cm). |
To optimize the product for LMIC settings, we also designed two inline, passive air-oxygen blenders capable of providing fixed 37% and 60% blends of oxygen (Figure 2).20 The PATH bCPAP and blender device is designed to operate on oxygen cylinders, mid-to-large-sized oxygen concentrators, or central oxygen supplies piped into a wall.
 |
Figure 2 Oxygen blenders included in PATH bCPAP device. (A) PATH’s fixed-rate bCPAP blenders. (B) Blender principle of operation. Abbreviation: bCPAP, bubble continuous positive airway pressure. |
The blenders operate on a similar principle to traditional Venturi-style entrainment blenders. A pressurized source of oxygen passes through a small nozzle that crosses a gap that is open to the surrounding atmosphere. The pressure in the oxygen jet is substantially lower than that of its surroundings, resulting in entrainment of ambient air. On the far side of the gap, coaxial with the nozzle, is an opening that receives a jet of blended gases. This opening features a section of constant diameter tubing that allows for laminar flow to redevelop followed by a diffuser—a section of tubing that gradually expands in diameter—that facilitates modest pressure recovery in the blended gas, allowing this design to be used with positive pressure (eg, CPAP) therapy.
Our initial design goal was to have no custom-designed parts except for the oxygen blender. However, we identified two custom components that could increase the simplicity of manufacture and use: 1) cannula adapter and 2) bubbler stand. The cannula adapter allows the circuit tubing to connect directly to the 15 mm RAM cannula fitting. Bubbler stand features include a wide base to prevent tipping, hook for hanging the bubbler firmly in place in any position and when full of water on both large and small rails at bedside, and depth gauge.
Device Fabrication
Bormed RF825MO polypropylene random copolymer (Borealis Group, Vienna, Austria) was used to fabricate the ambient air-oxygen blender and cannula adapter parts. These components were injection molded by Protolabs, Inc. (Maple Plain, Minnesota, USA).
Test Methods
Bench testing was conducted to verify the respiratory circuit and blender performance, evaluate the device under humid conditions, and measure the sound emitted by the device while in operation. Test criteria were informed by the product requirements specification, which was developed by the product development team with input from expert users.21–23 Most but not all of our specifications align with a more recent effort that developed global product requirements specifications for newborn care in low-resource settings, including CPAP24 devices. Bench testing methods to characterize device performance are detailed below.
Respiratory Circuit Verification
We developed a procedure to verify the performance of the respiratory circuit, specifically with regard to the mean airway pressure a preterm infant patient might experience using the device. An ASL 5000 test lung (IngMar Medical, Pittsburgh, Pennsylvania, USA) was used to simulate two patient profiles: a healthy full-term (40-week) newborn weighing 3.5 kilograms and a 1-kg preterm infant. While the former is not necessarily representative of the typical use scenario (preterm with RDS), this patient profile presented a worst-case scenario, where flow demands of the patient are highest. Lung settings can be found in Table 1. The device was operated at high (5 LPM) and low (2 LPM) flow for the respective patient profiles at both 4 and 8 cm of bubbler depth and mean airway pressure (MAP) recorded. Blended flows were verified using a PFC-3000 flow analyzer (BC Biomedical, St. Charles, Missouri, USA). The testing used custom 3D-printed “noses” to fit infant and preemie RAM cannula (Neotech Products, Valencia, California, USA) sizes with no leak to the nares. Data on blender flow, pressure, and FiO2 were also collected with the analyzer. The bCPAP respiratory circuit and lung simulator were set up as shown in Figure 3.
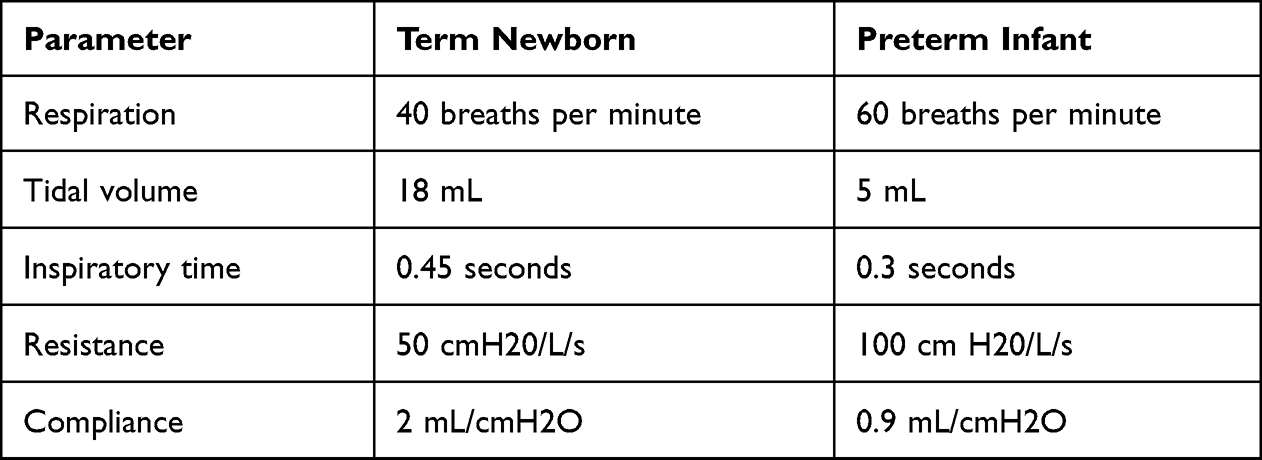 |
Table 1 Test Lung Settings Used for Respiratory Circuit Verification |
 |
Figure 3 Respiratory circuit with test lung. |
Blender Verification
This test verified the oxygen blender oxygen fractionation was accurate and stable over a specified range of flows and back pressures using source oxygen pressures provided by medium and large oxygen concentrators (defined as 8.5 and 20 psi, respectively). To speed up the process of testing at two pressures, a pressure control box was constructed using two pressure regulators and a selection switch to direct flow into either. Each regulator was set to deliver oxygen pressure that would provide flow output on the extremes of the specification (2 LPM @ 2.5 cmH2O and 7 LPM @ 15 cmH2O of pressure, respectively). The oxygen was delivered from the control box to the blender, which then flowed through the PFC-3000 flow analyzer to an adjustable positive end-expiratory pressure (PEEP) valve. Source oxygen pressure, flow, oxygen percentage, and blended pressure were measured by the flow analyzer (Figure 4).
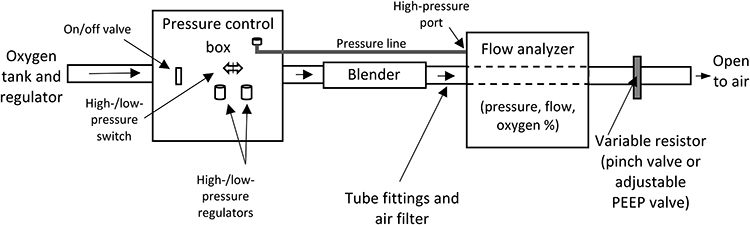 |
Figure 4 Blender verification test setup. Abbreviation: PEEP, positive end-expiratory pressure. |
Conditioned Humidity Testing
The above blender verification testing was also performed after conditioning the blenders at different environmental conditions (heat and humidity) as defined in the product requirements specification. These include two storage conditions at temperature extremes as well as an elevated humidity condition to simulate use in a tropical environment. Blenders were tested using the above procedure to gather a baseline. Afterwards, they were conditioned in an environmental chamber for 48 hours followed by immediate testing using the same procedure. Table 2 describes the test conditions.
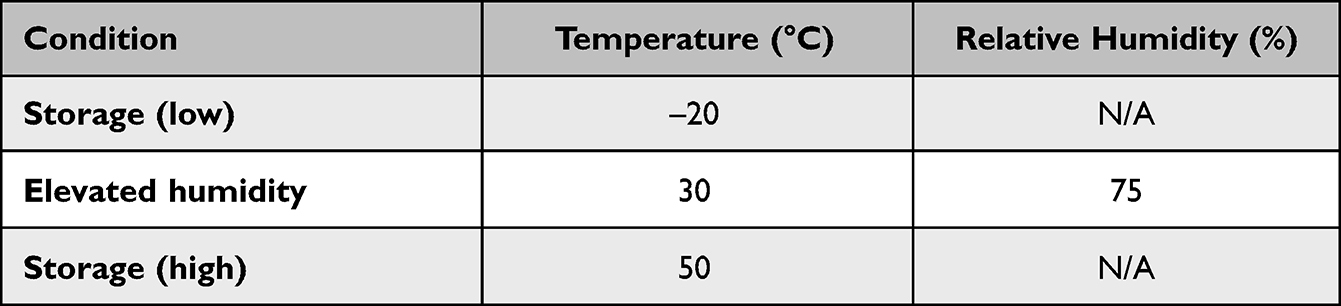 |
Table 2 Test Conditions for Blenders |
Sound Measurements
This test characterized the levels of sound generated by the device to inform its acceptability in a hospital setting. This test was intended to estimate the sound pressure level produced by the device only, and the test setup was not in compliance with International Organization for Standardization (ISO) 3746 or any equivalent standard due to lack of facilities.25 For this test, we used a room approximately 2.5 m × 3 m in dimension with two fabric-coated walls, one concrete wall, one wall composed of drywall, ceiling tiles, and a carpeted floor. The blender was oriented so that the entrainment opening was facing side to side rather than vertical to avoid blockage from the table. Test equipment included a sound meter (Sper Scientific 840014, Scottsdale, Arizona, USA), oxygen flowmeter (1MFA, Precision Medical, Northampton, Pennsylvania, USA), and tape measure (Figure 5).
 |
Figure 5 Sound measurement test setup. |
Measurement points were placed 50 cm away from the blender at the center of the table, at 120° angles from each other (Figure 5). Measurements were taken with the bubbler straw at a depth of 5 cm with a) no water in the bottle and b) water in the bubbler, partially occluding the nares to achieve a steady stream of bubbles. Sound measurements were obtained at baseline (no oxygen flow), oxygen flow at 1 LPM, and in 1-LPM oxygen increments up to 10 LPM or 50 psi, whichever came first.
Statistical Analysis
For quantitative variables, we calculated descriptive statistics using mean ± standard deviation for all sample results.
Results
All testing was completed between 2014 and 2018, and test results were documented in the design history file.
Respiratory Circuit Verification
Test results show approximately 1 cmH2O higher MAP from the respective bubbler depth set value at 2 LPM and 3.5 cmH2O higher MAP at 5 LPM compared to the specification value of 1 cmH2O. This was with 100% occlusion of the cannula in the mock nose for consistency. In clinical use, cannula will not have full occlusion, to avoid complications such as septal erosion, which will lower delivered pressure.
Blender Verification
Forty-five samples of each of the 37% and 60% blenders were used for blender verification in lab environmental conditions (22°C, 48% humidity). With the exception of one outlier, both the 60% and 37% nominal FiO2 blenders meet the acceptance criteria for both flow and FiO2 (Figure 6). One outlier had a marginally lower flow but acceptable FiO2.
 |
Figure 6 Blender FiO2 for high/low flow and pressure (n=45). Abbreviations: FiO2, fraction of inspired oxygen; n, number. |
Conditioned Humidity Testing
Ten samples of each blender were tested in the three environmental conditions outlined in the methods section. Figures 7 and 8 show the results of conditioning in terms of oxygen blend percentage and output flows relative to their results from before the 48-hour conditioning period. Most of the observed changes did not impact the ability of the blenders to meet specifications with the exception of the 37% blender at elevated temperature (50°C). In this condition, five of the ten blenders did not meet the flow specification.
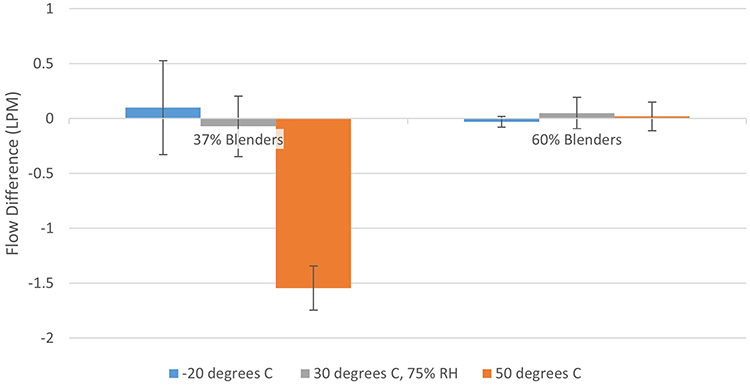 |
Figure 7 Difference in average flow before and after conditioning (LPM). |
 |
Figure 8 Difference in average FiO2 before and after conditioning (% oxygen). Abbreviations: FiO2, fraction of inspired oxygen; LPM, liter per minute; RH, relative humidity. |
Sound Measurements
The baseline measurement (no flow) of the testing setup was 37 A-weighted decibels (dBA). The 37% blender measurements averaged from 46 to 79 dBA between 1 and 7 LPM of oxygen flow, while the 60% blender measurements averaged 46 to 66 dBA over the same flow range (Figure 9). The bubbler added 2 dBA of sound pressure at 1 LPM of oxygen and was negligible (<1dBA difference) compared to the blender at 2 LPM and above.
 |
Figure 9 PATH CPAP average sound levels 50 cm away from blender. Abbreviations: bCPAP, bubble continuous positive airway pressure; dBA; A-weighted decibels; LPM, liter per minute. |
Discussion
In summary, our bench studies demonstrate that the bCPAP with blenders delivers pressures of up to 8 cmH2O and oxygen blends of 37% and 60% at typical flow rates (2 to 5 LPM) for neonatal patients. There was a slight reduction in flow capability of the 37% blender at high temperature (50°C). However, this represents a worst-case scenario, and we do not anticipate this would impact patient safety as the FiO2 was unaffected by temperature and could be compensated for with additional oxygen flow. Although our bench testing has demonstrated blend ratios down to 30%, they require an oxygen supply with higher driving pressures (> 8.5 pounds per square inch gauge). This would not be an issue for large oxygen concentrators, facility-distributed oxygen, or oxygen cylinders, but many stationary concentrators would be unable to deliver sufficient pressure. For this reason, we fixed our lower oxygen blend level at 37%.
Our blender design can be manufactured using injection molding, making low-cost production of this device extremely feasible. Injection molding is well suited for this application because it can maintain dimensional stability over thousands of parts, produce parts at relatively low cost, and be compatible with a wide spectrum of biocompatible polymers. Care must be taken to ensure that the orifices produced in the molding process are of high quality and in good alignment; flashing or distortion can result in poor performance.
Other designs of bCPAP and Venturi-type blenders are currently in various stages of development.26–28 Our circuit design is distinct in that it uses a RAM cannula for patient interface rather than nasal prongs resembling Hudson RCI® products. Our team selected a RAM cannula because this type of interface is simple to secure on the patient’s face and is likely to be more feasible in LMIC environments where nursing ratios for neonatal in-patient care are relatively high.29 Furthermore, while the fixed ratio oxygen blenders in our device are not fully adjustable, they do provide a lower blend option (37% or 60%) compared to the 60–100% noted in some designs. Limitations to our bench testing include the lack of a neonatal airway model and performance testing with different amounts of leak at the nares. The elevated 3.5 cmH2O at 5 LPM of flow could present patient risk if the nares are fully occluded, however previous studies have noted lower pressure delivery with the RAM cannula when using the manufacturer recommended 60–80% occlusion ratio at the nares.30 Also, we were not able to test FiO2 output with lower upstream oxygen concentrations (eg, from a poorly performing concentrator) so our calculations are only theoretical. Work of breathing calculations were also not performed.
Further research could be beneficial to determine user acceptability of the noise generated by the oxygen blenders, particularly the 37% blender at higher flow rates. While the level of noise is not necessarily harmful (blender is <80 dB), elevated sound levels could be annoying,31 especially at nighttime. The sound levels were measured in a nonideal environment and assume a 50-cm distance from the observer. Improper placement of the device into a warmer or otherwise nearby patient could increase sound exposure. Further research to assess the feasibility of using this device in a special care unit for small and sick newborns in an LMIC is warranted. An evaluation is currently ongoing to assess the operational feasibility, usability and acceptability of the PATH bCPAP and oxygen blenders by health care workers in Uganda. Results from this operational feasibility study will be used to inform any further design modifications.
Use of improvised bCPAP devices has been reported in Bangladesh, Nigeria,32–35 India,36 Kenya,37 Malawi,38 and Uganda.39 However, improvised devices are not standardized, and the pressures delivered are often variable.40,41 The demand for respiratory support for preterm infants in LMICs will likely be expanding due to recently released global guidance targeting the use of CPAP in at least 80% of districts as part of special care units for small and sick newborns.42,43 Adding a standardized and bench-tested low-cost bCPAP with oxygen blenders could help overcome this challenge and would be a welcome addition to respiratory newborn care options currently available in LMICs.44,45
Conclusion
These bench testing results show that this very low-cost, nonelectric bCPAP and blenders device is optimally designed to deliver a stable and reliable source of pressurized blended gas for neonatal therapies. This low-cost bCPAP device does not require assembly at the point of care and is designed to provide bCPAP therapy to newborns without the requirement of a power source (ie, electricity or battery) or a source of compressed medical air. As such, this low-cost bCPAP and blenders device is well positioned to reduce unmet need for newborn respiratory support in LMICs.
Acknowledgments
We would like to thank Eugene Saxon and Michael Eisenstein, both of whom contributed substantially to the development of this product while they were working at PATH. We also recognize the generosity and dedication of our wonderful collaborators, Adara Development, Kiwoko Hospital, Seattle Children’s Hospital, and the University of Washington, Department of Neonatology. Finally, we would like to thank Jill Sherman-Konkle, who has been a stalwart companion on this product development journey.
We acknowledge the generous funding support of the Saving Lives at Birth partners: the United States Agency for International Development, the government of Norway, the Bill & Melinda Gates Foundation, Grand Challenges Canada, and the UK government. The views expressed are the responsibility of the authors and do not necessarily reflect the views of the Saving Lives at Birth partners.
Disclosure
Both authors have been active in developing the bCPAP and blenders technology while employed at PATH. PATH and/or the authors do not hold any relevant financial or nonfinancial relationships related to this product. The authors report no other conflicts of interest in this work.
References
1. Blencowe H, Cousens S, Oestergaard MZ, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379(9832):2162–2172. doi:10.1016/S0140-6736(12)60820-4
2. World Health Organization. Preterm birth fact sheet. Available from: http://www.who.int/mediacentre/factsheets/fs363/en/.
3. Kamath BD, Macguire ER, McClure EM, Goldenberg RL, Jobe AH. Neonatal mortality from respiratory distress syndrome: lessons for low-resource countries. Pediatrics. 2011;127(6):1139–1146. doi:10.1542/peds.2010-3212
4. Ho JJ, Subramaniam P, Davis PG. Continuous positive airway pressure (CPAP) for respiratory distress in preterm infants. Cochrane Database Syst Rev. 2020;10(10):CD002271. doi:10.1002/14651858.CD002271.pub3
5. Sweet DG, Carnielli V, Greisen G, et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome – 2019 Update. Neonatology. 2019;115(4):432–450. doi:10.1159/000499361
6. Ekhaguere OA, Mairami AB, Kirpalani H. Risk and benefits of Bubble Continuous Positive Airway Pressure for neonatal and childhood respiratory diseases in Low- and Middle-Income countries. Paediatr Respir Rev. 2019;29:31–36. doi:10.1016/j.prrv.2018.04.004
7. Martin S, Duke T, Davis P. Efficacy and safety of bubble CPAP in neonatal care in low and middle income countries: a systematic review. Arch Dis Child Fetal Neonatal Ed. 2014;99(6):F495–504. doi:10.1136/archdischild-2013-305519
8. Nørgaard M, Stagstrup C, Lund S, Poulsen A. To bubble or not? A systematic review of bubble continuous positive airway pressure in children in low- and middle-income countries. J Trop Pediatr. 2020;66(3):339–353. doi:10.1093/tropej/fmz069
9. World Health Organization. Oxygen therapy for children. 2016. Available from: http://www.healthynewbornnetwork.org/hnn-content/uploads/Oxygen-Therapy-for-Children.pdf.
10. Bancalari E, Claure N. Respiratory instability and hypoxemia episodes in preterm infants. Am J Perinatol. 2018;35(6):534–536. doi:10.1055/s-0038-1637760
11. Lee J, Dammann O. Perinatal infection, inflammation, and retinopathy of prematurity. Semin Fetal Neonatal Med. 2012;17(1):26–29. doi:10.1016/j.siny.2011.08.007
12. Vanderveen DK, Mansfield T, Eichenwald EC. Lower oxygen saturation limits decrease the severity of retinopathy of prematurity. J AAPOS. 2006;10(5):445–448. doi:10.1016/j.jaapos.2006.04.010
13. Tin W, Walker S, Lacamp C. Oxygen monitoring in preterm babies: too high, too low? Paediatr Respir Rev. 2003;4:9–14. doi:10.1016/s1526-0542(02)00307-x
14. Baraldi E, Filippone M. Chronic lung disease after premature birth. N Engl J Med. 2007;357(19):1946–1955. doi:10.1056/NEJMra067279
15. Reich B, Hoeber D, Bendix I, Felderhoff-Mueser U. Hyperoxia and the immature brain. Dev Neurosci. 2016;38(5):311–330. doi:10.1159/000454917
16. World Health Organization (WHO). Technical Specifications for Oxygen Concentrators. Geneva: WHO; 2015. Available from: https://www.who.int/publications/i/item/9789241509886.
17. Egesa WI, Waibi WM. Bubble nasal continuous positive airway pressure (bNCPAP): an effective low-cost intervention for resource-constrained settings. Int J Pediatr. 2020;2020:8871980. doi:10.1155/2020/8871980
18. Jain A, DiBlasi RM, Devgan V, et al. Simple point of care continuous positive airway pressure delivery device (Jain-CPAP). BMJ Innovations. 2019;5(1):13–19. doi:10.1136/bmjinnov-2018-000339
19. Hedstrom AB, Ebels K, Eisenstein M, et al. Expanding the reach of bubble Cpap devices- results from 2015 Stakeholder Workshop in Uganda. Pediatrics. 2018;141:483. doi:10.1542/peds.141.1MA5.483
20. Research Disclosure. Oxygen Blender – public Disclosure. Research Disclosure database number 635032. Published in the March 2017 paper journal. 2017.
21. PATH. Evaluation and Preparation for Introduction of a Low-Cost, Bubble, Continuous Positive Airway Pressure Kit and Oxygen Blender for Neonates: Final Report. Seattle: PATH; 2016.
22. PATH. Development of a Low-Cost, Bubble, Continuous Positive Airway Pressure (Bcpap) Kit and Oxygen Blender. Draft Product Requirement Specifications for a bCPAP Kit and Oxygen Blender. Seattle: PATH; 2016.
23. PATH. Product Requirements Specification (DRAFT). For a Bubble CPAP Kit and Oxygen Blender. Seattle: PATH; 2018.
24. UNICEF, NEST360°. Target Product Profiles for Newborn Care in Low-Resource Settings (v1.2) Consensus Meeting Report (March 2020). 2020. Available from: https://www.unicef.org/supply/sites/unicef.org.supply/files/2020-04/TPP-newborn-care-final-report-v1-2.pdf.
25. International Organization for Standardization. Acoustics — determination of sound power levels and sound energy levels of noise sources using sound pressure — survey method using an enveloping measurement surface over a reflecting plane. (ISO Standard No. 3746:2010). Geneva: ISO; 2010. Reviewed and confirmed in 2021. Available from: https://www.iso.org/standard/52056.html.
26. Kamyar -M-M, Thomas FB, Michelle D, et al. A Low-Cost Venturi Ambient Air-Oxygen Blender for Neonatal Oxygen Therapy. Acad J Ped Neonatol. 2020;9(1):555808. doi:10.19080/AJPN.2020.08.555808
27. Dundek L, Ng M. Evaluation of a Bubble CPAP System for Low Resource Settings. Respir Care. 2021;66(10):1572–1581. doi:10.4187/respcare.08948
28. Floersch J, Hauschildt E, Keester A. A Low-Resource Oxygen Blender Prototype for Use in Modified Bubble CPAP Circuits. J Med Devices. 2020;14(1):015001. doi:10.1115/1.4045899
29. Tooke L, Ehret DEY, Okolo A, et al. Limited resources restrict the provision of adequate neonatal respiratory care in the countries of Africa. Acta Paediatr. 2021;111(2):275–283. doi:10.1111/apa.16050
30. Gerdes JS, Sivieri EM, Abbasi S. Factors influencing delivered mean airway pressure during nasal CPAP with the RAM cannula. Pediatr Pulmonol. 2016;51(1):60–69. doi:10.1002/ppul.23197
31. World Health Organization (WHO). Training for Health Care Providers: Children and Noise. Geneva: WHO; 2014. Available from https://www.who.int/ceh/capacity/noise.pdf.
32. Audu L, Otuneye A, Mukhtar M, Mairami A, Mshelia L, Garu M. Customized bubble continuous positive airway pressure (BCPAP) device at the National Hospital Abuja for the treatment of respiratory distress syndrome (RDS). Niger J Paediatr. 2013;40(3):275–277.
33. Amadi HO, Okonkwo IR, Abioye IO, et al. A new low-cost commercial bubble CPAP (bCPAP) machine compared with a traditional bCPAP device in Nigeria. Paediatr Int Child Health. 2019;39(3):184–192. doi:10.1080/20469047.2019.1598125
34. Ezenwa B, Akintan P, Fajolu I, Ladele J, Ezeaka C. Bubble CPAP in the management of respiratory distress syndrome in resource constrained settings: the LUTH experience. Pediatric Oncall. 2016;13(1):9–12. doi:10.7199/ped.oncall.2016.11
35. Baldursdottir S, Falk M, Donaldsson S, Jonsson B, Drevhammar T. Basic principles of neonatal bubble CPAP: effects on CPAP delivery and imposed work of breathing when altering the original design. Arch Dis Child Fetal Neonatal Ed. 2020;105:550–554. doi:10.1136/archdischild-2019-318073
36. Daga S, Mhatre S, Borhade A, Khan D. Home-made continuous positive airways pressure device may reduce mortality in neonates with respiratory distress in low-resource setting. J Trop Pediatr. 2014;60(5):343–347. doi:10.1093/tropej/fmu023
37. Myhre J, Immaculate M, Okeyo B, et al. Effect of treatment of premature infants with respiratory distress using low-cost bubble CPAP in a rural African hospital. J Trop Pediatr. 2016;62(5):385–389. doi:10.1093/tropej/fmw023
38. Van Den Heuvel M, Blencowe H, Mittermayer K, et al. Introduction of bubble CPAP in a teaching hospital in Malawi. Ann Trop Paediatr. 2011;31(1):59–65. doi:10.1179/1465328110Y.0000000001
39. McAdams RM, Hedstrom AB, DiBlasi RM, et al. Implementation of bubble CPAP in a rural Ugandan neonatal ICU. Respir Care. 2015;60(3):437–445. doi:10.4187/respcare.03438
40. Ettinger NA, Serazin N, Nguyen R, Werdenberg J, Huibers M, Torrey S. Testing positive pressure delivered from commercial and WHO-style pediatric bubble CPAP devices. BMC Pediatr. 2021;21(1):524. doi:10.1186/s12887-021-03006-2
41. Baldursdottir S, Falk M, Donaldsson S, Jonsson B, Drevhammar T. Basic principles of neonatal bubble CPAP: effects on CPAP delivery and imposed work of breathing when altering the original design. Arch Dis Child Fetal Neonatal Ed. 2020;105:F550–F554. doi:10.1136/archdischild-2019-318073
42. World Health Organization (WHO), UNICEF. Ending Preventable Deaths and Stillbirths by 2030: Moving Faster Towards High-Quality Universal Health Coverage in 2020–2025. Geneva: WHO; 2020. Available from: https://www.unicef.org/reports/ending-preventable-newborn-deaths-stillbirths-quality-health-coverage-2020-2025.
43. World Health Organization (WHO). Standards for Improving Quality of Care for Small and Sick Newborns in Health Facilities. Geneva: WHO; 2020. Available from: https://www.who.int/publications/i/item/9789240010765.
44. Won A, Suarez-Rebling D, Baker AL, Burke TF, Nelson BD. Bubble CPAP devices for infants and children in resource-limited settings: review of the literature. Paediatr Int Child Health. 2019;39(3):168–176. doi:10.1080/20469047.2018.1534389
45. Kasali BA, Gururaj A, Batra M. Newborn care technology investments for LMIC settings: a CPAP approach. BMJ Innovations. 2021;7:519–522. doi:10.1136/bmjinnov-2020-000598
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.