Back to Journals » International Journal of Women's Health » Volume 18
Non-Pharmacological Interventions for Symptom Cluster Management in Women with Cancer: A Scoping Review of Multicomponent and Mechanism-Based Approaches
Authors Irmala N ![]() , Solehati T
, Solehati T ![]() , Sukmawati S
, Sukmawati S ![]()
Received 30 March 2026
Accepted for publication 26 May 2026
Published 3 June 2026 Volume 2026:18 612228
DOI https://doi.org/10.2147/IJWH.S612228
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Novi Irmala,1 Tetti Solehati,2 Sukmawati Sukmawati2
1Master of Nursing Program, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Department of Maternity Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia
Correspondence: Tetti Solehati, Department of Maternity Nursing, Faculty of Nursing, Universitas Padjadjaran, Jl. Raya Bandung-Sumedang KM 21, Hegarmanah, Jatinangor, Sumedang, West Java, 45363, Indonesia, Tel +62 81224836837, Fax +6222-7795596, Email [email protected]
Background: Women with cancer frequently experience co-occurring symptoms, including cancer-related fatigue, sleep disturbance, and psychological distress, which negatively impact quality of life. Despite the increasing use of non-pharmacological interventions, current approaches remain largely fragmented and predominantly target individual symptoms rather than symptom clusters, highlighting the urgent need for integrated, cluster-based intervention models in women’s cancer care.
Purpose: This scoping review aimed to map recent non-pharmacological interventions for symptom management in women with cancer and to examine the extent to which these interventions address co-occurring symptom clusters.
Methods: A scoping review was conducted following Arksey and O’Malley’s framework and the Joanna Briggs Institute (JBI) guidance, and reported in accordance with PRISMA-ScR. A systematic search of PubMed, CINAHL, and Scopus identified studies published between January 2021 and December 2025. Eligible studies included experimental and quasi-experimental designs evaluating non-pharmacological interventions targeting fatigue, sleep disturbance, psychological distress, or related outcomes in women with cancer. Data were charted and synthesized descriptively.
Results: A total of 29 studies were included, predominantly randomized controlled trials. Interventions were categorized into five categories: exercise-based programs, mind–body and relaxation therapies, complementary therapies, psychosocial and behavioral interventions, and technology-based or nurse-led care models. Exercise-based interventions consistently reduced fatigue, likely through improvements in physical capacity. Mind–body approaches improved psychological distress and sleep quality by modulating stress responses. Psychosocial interventions enhanced coping and emotional regulation, while complementary therapies provided short-term relief of subjective symptoms, although with greater variability. Technology-based and nurse-led interventions improved accessibility, adherence, and self-management. While many interventions were associated with improvements in individual symptoms, multicomponent approaches demonstrated broader and more sustained benefits across fatigue, sleep, and psychological outcomes. However, only a limited number of studies explicitly incorporated a symptom-cluster framework.
Conclusion: Non-pharmacological interventions are associated with meaningful improvements in symptom burden among women with cancer. However, a critical gap persists between the multidimensional nature of symptom experience and the predominantly single-modality design of interventions. Future research should prioritize the development of integrated, multicomponent strategies explicitly targeting symptom clusters to enhance clinical effectiveness and patient-centered care.
Keywords: women with cancer, cancer-related fatigue, symptom cluster, non-pharmacological intervention, sleep disturbance
Introduction
Women with cancer experience a substantial and persistent symptom burden that extends beyond active treatment and significantly affects daily functioning and quality of life. This burden reflects not only the effects of disease and treatment, but also gender-specific influences, including hormonal changes, reproductive concerns, and psychosocial roles. Symptoms such as cancer-related fatigue, sleep disturbance, and psychological distress are recognized to co-occur and interact, forming clinically relevant symptom clusters that are associated with poorer outcomes and higher care needs.1–4
Globally, the cancer burden continues to rise, with an estimated 19.3 million new cases and approximately 10 million deaths recorded in 2020.5,6 Female breast cancer has now surpassed lung cancer as the most frequently diagnosed malignancy worldwide, accounting for 11.7% of all total cancer cases and 24.5% of all new cancer cases in women.5 Geographically, the distribution of these cases is disproportionate; Asia accounts for nearly half of global incidence (48.6%) and over half of all cancer deaths (55.5%) among women.5,6 Projections for the future are even more staggering, with the global cancer burden expected to reach 28.4 million cases by 2040, a 47% increase from 2020 levels.5 Current data indicates that one in four women diagnosed with cancer is affected by breast cancer, which remains the leading cause of cancer-related mortality among the female population.7,8 Furthermore, gynecological malignancies including cervical, ovarian, and endometrial cancers account for approximately 18% of all tumors in women globally.5,9
While therapeutic advancements have extended survival, they frequently trigger a cascade of debilitating side effects. Cancer-related fatigue (CRF) is the most pervasive symptom, with evidence showing that up to 99% of women undergoing chemotherapy experience it.10 The prevalence of CRF can range from 25% to 99% depending on the treatment approach.11 Alongside fatigue, sleep disturbances are highly prevalent, affecting more than 60% of patients.12 These symptoms rarely occur in isolation and often manifest as a symptom cluster, most notably the triad of fatigue, sleep disturbance, and depression (FSDSC).13 These clusters exert a synergistic negative impact on functional status and health-related quality of life (QoL), often proving more distressing than individual symptoms.12,13
Non-pharmacological interventions, including exercise, mind–body therapies, cognitive-behavioral approaches, and complementary modalities are widely used to support symptom management due to their safety and feasibility in clinical settings.1 These interventions have been shown to improve in level of fatigue, sleep, and psychological outcomes. However, most are designed to target individual symptoms, despite evidence that these symptoms frequently occur together and may share underlying mechanisms. As a result, current approaches may not fully address the complexity of symptom burden experienced by women with cancer.
Moreover, existing reviews tend to focus on specific intervention types or single outcomes, limiting their relevance for informing integrated, patient-centered care. There remains a lack of synthesis that evaluates how non-pharmacological interventions align with the clinical reality of co-occurring symptoms. Therefore, this scoping review aims to map recent non-pharmacological interventions in women with cancer and examine whether they address individual symptoms or co-occurring symptom clusters. By focusing on the fatigue–sleep disturbance–psychological distress cluster, this review seeks to provide clinically relevant insights to inform the development of more integrated and effective supportive care strategies in women’s oncology.
Methods
Study Design and Reporting
This study employed a scoping review methodology to systematically map and synthesize recent evidence on non-pharmacological interventions targeting symptom clusters among women with cancer. A scoping review design was selected to comprehensively examine the breadth, characteristics, and conceptual patterns of available literature, particularly in an emerging and methodologically heterogeneous field.14,15 This approach is particularly suitable for identifying intervention categories, clarify key concepts, and detect research gaps rather than to generate pooled effect estimates.
The review was conducted in accordance with the methodological framework proposed by Arksey & O’Malley and aligned with the Joanna Briggs Institute (JBI) guidance for scoping reviews.14,15 Reporting followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) guidelines to ensure transparency and reproducibility.15
The review process comprised five stages: (1) identifying the research question, (2) identifying relevant studies, (3) study selection based on predefined inclusion and exclusion criteria, (4) data charting and extraction, and (5) collating, summarizing, and reporting the results. Given the rapid evolution of integrative oncology interventions, the search was restricted to studies published between January 2021 and December 2025 to capture contemporary developments in symptom cluster management among women with cancer.
Outcomes
The primary objective of this scoping review was to map the types, characteristics, and targeted outcomes of non-pharmacological interventions implemented in women with cancer, with particular attention to whether these interventions addressed single symptoms or co-occurring symptom clusters such as fatigue, sleep disturbance, and psychological distress.
Search Strategy and Eligibility Criteria
A comprehensive literature search was conducted across three electronic databases: PubMed/MEDLINE, CINAHL, and Scopus. These databases were selected to ensure coverage of biomedical, nursing, psychological, and interdisciplinary oncology research.
The search strategy combined controlled vocabulary (MeSH terms where applicable) and free-text keywords related to: (neoplasm*OR cancer OR tumor*OR tumour*OR carcinoma*OR malignan*OR oncolog*) AND (non-pharmacological intervention) AND (fatigue OR “cancer-related fatigue”OR sleep OR insomnia OR “sleep disturbance*” OR “sleep quality”)
The search was limited to articles published between January 2021 and December 2025 and to studies published in English. Reference lists of included studies were manually screened to identify additional relevant publications. The research question used is: What types of non-pharmacological interventions have been implemented in women with cancer within the past five years to address symptom burden, and do these interventions target single symptoms or co-occurring symptom clusters such as fatigue, sleep disturbance, and psychological distress?
Inclusion and Exclusion Criteria
Eligibility criteria were defined a priori to ensure alignment with the research question and scope of this review. Studies were included if they involved adult women diagnosed with any type of cancer, predominantly breast cancer, who were undergoing active treatment such as chemotherapy or radiotherapy, or were in the survivorship phase. The review focused on studies evaluating at least one non-pharmacological intervention. To ensure relevance to symptom management, eligible studies were required to report outcomes related to symptom burden, particularly cancer-related fatigue, sleep disturbance, anxiety, depression, psychological distress, or quality of life. Randomized controlled trials, quasi-experimental studies, and controlled intervention trials were included. Only articles published within the past five years and written in English were considered in order to synthesize contemporary evidence.
Studies were excluded if they involved mixed-gender cancer populations without separate analysis for women, focused exclusively on pharmacological treatments, or employed observational, qualitative-only, cross-sectional, review, or case report designs. Conference abstracts without full intervention data were also excluded. Additionally, studies were excluded if they did not report symptom-related outcomes relevant to fatigue, sleep disturbance, or psychological distress, or if they were published outside the defined five-year timeframe. This review was not prospectively registered. However, the methodology was developed a priori and conducted in accordance with established scoping review frameworks, including the JBI guidance and PRISMA-ScR reporting standards.
Quality Appraisal
The results of the appraisal were used to inform interpretation of findings rather than to determine study inclusion. The methodological quality of included studies was evaluated using the Joanna Briggs Institute (JBI) Critical Appraisal Tools appropriate to each study design. Randomized controlled trials were assessed using the JBI checklist for randomized controlled trials, while quasi-experimental studies were evaluated using the JBI checklist for quasi-experimental designs. These tools assess domains such as randomization procedures, allocation concealment, baseline group similarity, blinding, completeness of follow-up, reliability of outcome measurement, and appropriateness of statistical analysis.
Each criterion was rated as “Yes,” “No,” “Unclear,” or “Not Applicable.” A score of one point was assigned for each “Yes” response, and total scores were converted into percentages based on applicable criteria. Although scoping reviews do not typically exclude studies based on methodological quality, a critical appraisal was conducted to provide contextual insight into the robustness of the included evidence. The Joanna Briggs Institute (JBI) Critical Appraisal Tools were applied according to study design. All 29 included studies met this threshold, indicating overall moderate to high methodological quality across the evidence base.
Data Extraction and Analysis
Conducting quality appraisal within this scoping review strengthens the credibility of the synthesis by demonstrating that the mapped interventions are supported by methodologically sound research. While the review does not exclude studies based on minor methodological limitations, reporting quality scores provides readers and reviewers with critical insight into the strength of the underlying evidence and supports the interpretation of identified research gaps. Data extraction was performed using a structured data-charting table that included the following variables: author and year of publication, country, study objective, population characteristics or sample size, study design, type of intervention, and key findings (Figure 1). This structured approach facilitated systematic organization and comparative analysis of the screened articles.
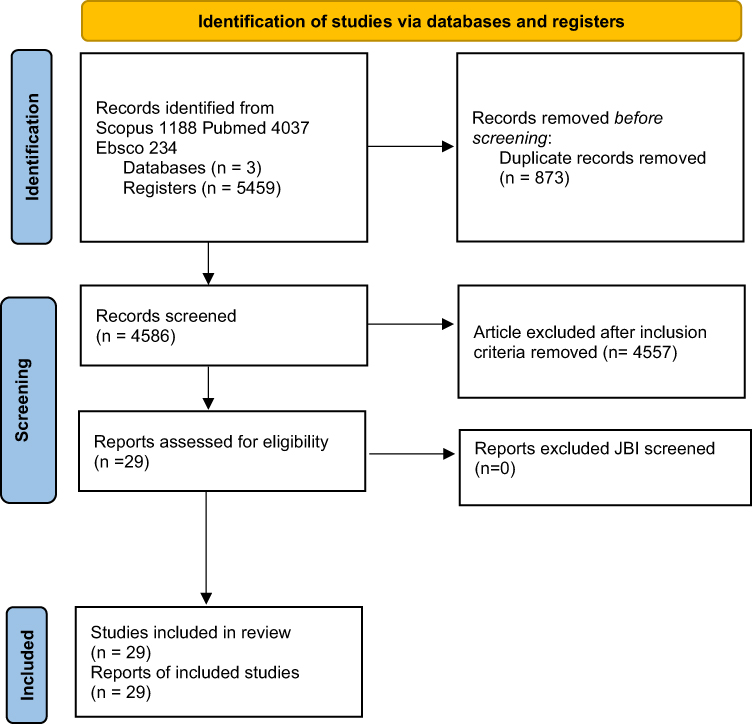 |
Figure 1 PRISMA Flow Diagram for the literature review on the Non-Pharmacological Interventions for Symptom Cluster Management in Women with Cancer. |
The extracted data were analyzed descriptively in accordance with the predefined table categories. Information from each study was entered into the corresponding columns to ensure consistency and transparency in reporting. In addition to the primary extraction table, a supplementary table was developed to detail specific intervention components and procedural steps. Due to the extensive variability and complexity of intervention protocols, this supplementary table was maintained separately to allow clearer identification of intervention structures. The findings of the included studies were synthesized narratively and interpreted in relation to previous research. Identified interventions were subsequently categorized into conceptually similar groups to support thematic classification and structured reporting.
Results
A total of 29 studies met the inclusion criteria and were included in this scoping review. The body of evidence demonstrates a clear dominance of experimental designs, with randomized controlled trials (RCTs) accounting for the majority (n=21), followed by quasi-experimental studies (n=6) and pilot or retrospective studies (n=2). This distribution indicates a moderate-to-high level of methodological rigor, although heterogeneity in intervention design and outcome measurement remains evident. Geographically, the evidence is heavily concentrated in Asia, particularly in China, Iran, and Turkey, with fewer studies conducted in Western settings. This uneven distribution suggests potential contextual and cultural influences on intervention design, delivery, and patient response, which may limit direct generalizability across settings. Sample sizes ranged from 16 to 176 participants, with most studies involving women undergoing active treatment (especially chemotherapy) or in the post-treatment survivorship phase. Notably, few studies explicitly stratified participants by cancer stage or treatment trajectory, indicating a gap in tailored intervention approaches. A detailed summary of study characteristics and intervention categorization is presented in Table 1. The methodological quality appraisal results are summarized in Table 2.
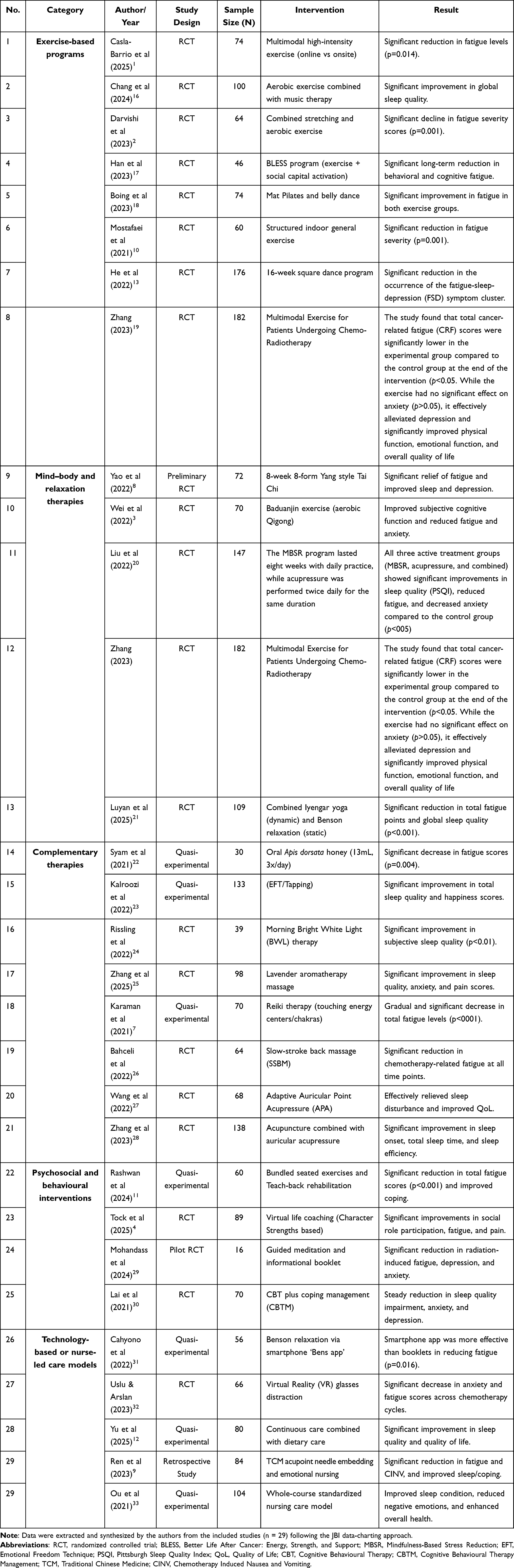 |
Table 1 Summary of Data Extraction and Intervention Categorization (n=29) |
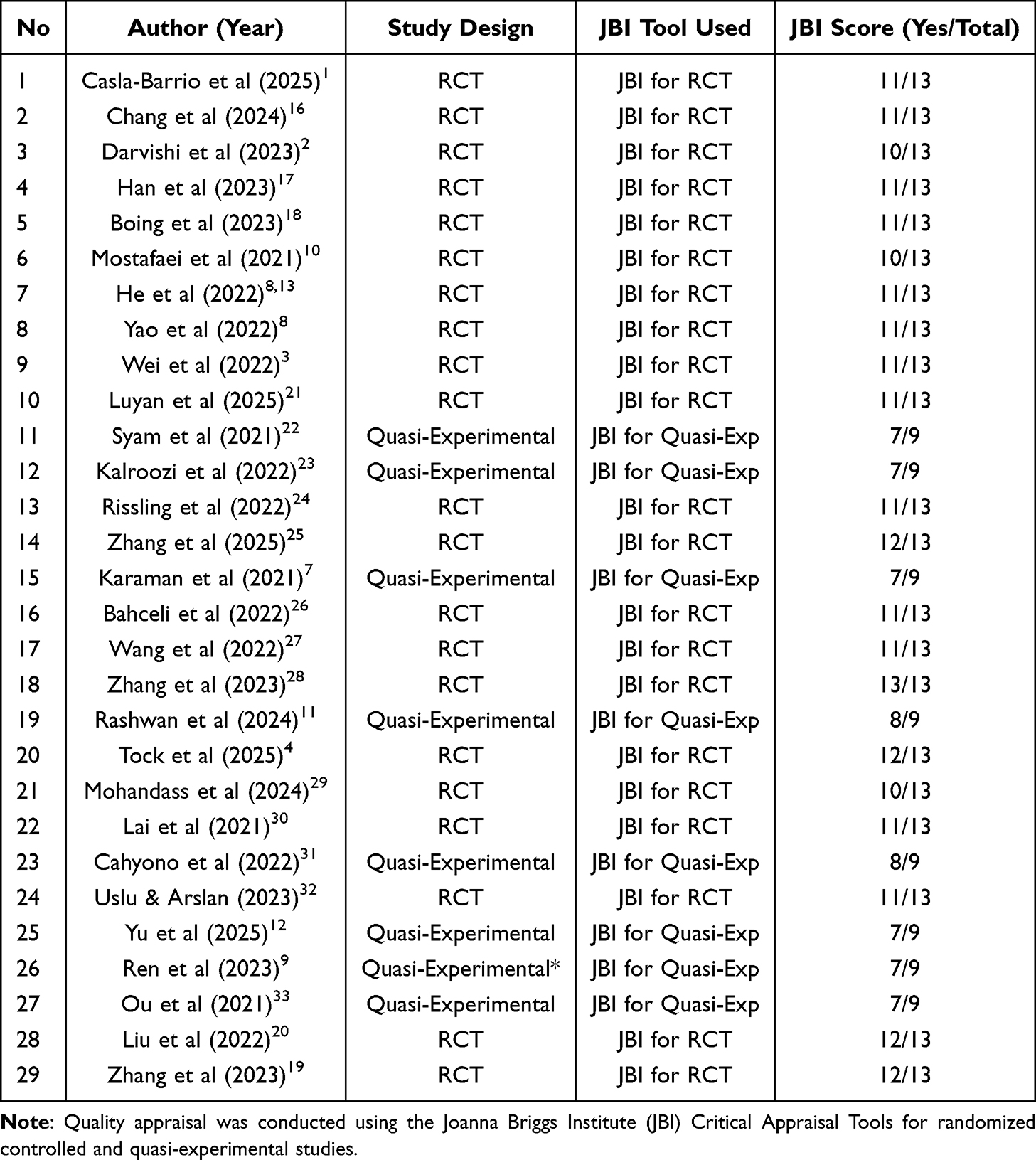 |
Table 2 JBI Critical Appraisal Scores of Included Studies (n=29) |
Across the included studies, interventions were categorized into five major domains: exercise-based interventions, mind–body and relaxation approaches, complementary and alternative therapies, psychosocial and behavioral interventions, and technology-based or nurse-led care models. Although these categories differ in their theoretical foundations and delivery methods, a consistent pattern emerged in which interventions targeting multiple mechanisms produced more comprehensive and clinically meaningful outcomes.
Exercise-Based Programs
Exercise-based interventions focused on structured physical activity to mitigate cancer-related fatigue (CRF) and enhance functional status. Multimodal high-intensity training, including endurance and resistance exercises, proved effective in significantly reducing fatigue levels (p=0.014) and increasing lean mass by 5.24%.1 A five-week multimodal exercise program was found to significantly reduce cancer-related fatigue, alleviate depressive symptoms, and improve both sleep quality and overall quality of life among breast cancer patients undergoing simultaneous radiotherapy and chemotherapy.19 The BLESS program, which integrates physical exercise with social capital activation, demonstrated significant long-term reductions in behavioral and cognitive fatigue.17 Culturally adapted and rhythmic activities, such as Square Dance, were particularly effective in addressing symptom clusters, showing a significant reduction in the occurrence of the FSD triad (p=0.003).13 Furthermore, combining aerobic exercise with music therapy significantly improved global sleep quality scores compared to routine care.16 Standardized indoor exercises also resulted in substantial declines in fatigue severity, with scores dropping from 8.17 to 5.56 in treated groups.2,10,18
Mind–Body and Relaxation Therapies
These therapies targeted the psychological and physiological underpinnings of the symptom burden. Traditional Chinese Exercises (TCEs), such as Tai Chi and Baduanjin, showed large effect sizes in relieving the FSD symptom cluster and improving subjective cognitive function.3,8 A pivotal finding in this category was the efficacy of multicomponent relaxation; the integration of dynamic Iyengar yoga postures with static Benson relaxation resulted in significantly greater reductions in total fatigue points and global sleep quality scores (p<0.001) compared to static relaxation alone.34 Additionally, Mindfulness-Based Stress Reduction (MBSR) proved superior in improving actigraphy-assessed sleep efficiency and total sleep time compared to routine care.34 The Benson relaxation technique and the combined dynamic-static relaxation therapy have been shown to effectively reduce fatigue and improve sleep quality in patients undergoing chemotherapy for breast cancer, with the combined dynamic-static relaxation therapy providing greater benefits.21
Complementary Therapies
Complementary strategies provided targeted relief for sensory and physiological distress. Acupuncture and acupressure interventions, including Adaptive Auricular Point Acupressure (APA), significantly improved objective sleep parameters, with sleep efficiency reaching 85.39% and a 56.5% cessation rate of sleep medications.20,27,28 Sensory-based interventions, such as lavender aromatherapy massage and morning bright white light (BWL) therapy, resulted in significantly improved subjective sleep quality and reduced anxiety levels.24,25 Energy-based and touch therapies, including Reiki and slow-stroke back massage (SSBM), were also validated; SSBM significantly lowered fatigue scores across multiple chemotherapy cycles (p<0.001).7,26 Biological interventions, such as the oral administration of Apis dorsata honey, were found to increase IL-37 levels and reduce fatigue.22 Finally, the Emotional Freedom Technique (EFT) significantly enhanced both sleep quality and happiness scores in post-surgical patients.23
Psychosocial and Behavioral Interventions
This domain utilized cognitive restructuring and psychoeducation to improve coping mechanisms. Cognitive Behavioral Therapy plus coping management (CBTM) showed a steady reduction in sleep quality impairment and a significant increase in mental quality of life.30 Teach-back psychoeducational rehabilitation bundled with seated exercises successfully reduced total fatigue scores and shifted patient coping styles toward “fighting spirit”.11 Furthermore, guided imagery and meditation during radiotherapy significantly reduced radiation-induced fatigue, depression, and anxiety.29 Conversely, while virtual life coaching provided short-term gains in social participation, these effects were not sustained at a 3-month follow-up, indicating the need for ongoing support.4
Technology-Based or Nurse-Led Care Models
Innovative delivery models enhanced patient adherence and clinical outcomes. The use of Virtual Reality (VR) glasses for nature-based distraction during chemotherapy significantly decreased post-test anxiety and fatigue across all cycles.32 Digital health innovations, like the “Bens app” for smartphone-guided relaxation, were found to be more effective than traditional booklets in reducing fatigue (p=0.016)31 Comprehensive nurse-led models—such as continuous nursing combined with dietary care or acupoint needle embedding with emotional nursing—resulted in high patient satisfaction (95.0% to 98.1%) and significant improvements in quality of life and chemotherapy-induced nausea and vomiting (CINV).9,12,33
A critical finding across the included studies is the consistent superiority of multicomponent interventions over single-modality approaches. Interventions that combined physical, psychological, and behavioral elements were more effective in producing broad and sustained improvements across multiple outcome domains. As a result, multicomponent interventions were particularly effective in addressing symptom clusters, such as the co-occurrence of fatigue, sleep disturbance, and psychological distress, which are common in women with cancer.
Overall, the evidence demonstrates that while individual non-pharmacological interventions yield meaningful benefits within specific domains, integrated approaches that address multiple mechanisms concurrently provide more comprehensive and clinically relevant outcomes. This pattern underscores the importance of moving beyond isolated intervention strategies toward more holistic and mechanism-informed models of care in cancer symptom management. The findings indicate lack of integration, where most strategies target isolated symptoms despite the multidimensional nature of symptom clusters. Notably, although multiple symptoms were measured concurrently across studies, few interventions were explicitly designed to target symptom clusters as interconnected phenomena. Most included studies focused on women with breast cancer, although several studies included other cancer types.
Discussion
This review mapped recent non-pharmacological interventions for symptom management in women with cancer and examined their alignment with a symptom-cluster perspective. Overall, the evidence base is expanding, with a growing number of well-designed studies, with a predominance of randomized controlled trials and increasing diversity of intervention approaches. Across studies, non-pharmacological interventions were consistently linked to improvements in fatigue, sleep disturbance, and psychological distress. However, a key finding of this review is that most interventions remain designed to target individual symptoms, despite the frequent co-occurrence of these outcomes.
A recurring pattern identified in this review is the clustering of cancer-related fatigue, sleep disturbance, and psychological distress. This triad was repeatedly assessed within the same studies, suggesting that these symptoms are not independent but rather interrelated and potentially mutually reinforcing. Clinically, this has important clinical implications, as patients rarely present with a single isolated symptom. Instead, unmanaged fatigue may exacerbate sleep disruption, which in turn may worsen emotional distress, creating a self-perpetuating cycle that negatively affects recovery, treatment adherence, and quality of life. Despite this, most interventions evaluated in the included studies did not explicitly adopt a symptom-cluster framework in their design or implementation. Although the findings are broadly applicable to women with cancer, the predominance of breast cancer studies in the existing literature highlights a potential limitation in generalizability across other cancer populations.
The conceptual model presented in Figure 2 provides a theoretical explanation for these findings, illustrating how integrated approaches provide more comprehensive outcomes target physiological, psychological, and behavioral pathways underlying symptom clusters. As illustrated in Figure 2, multicomponent interventions operate through integrated physiological, psychological, and behavioral mechanisms. The convergence of these pathways underscores the importance of addressing shared mechanisms rather than treating symptoms in isolation. Taken together, these findings suggest that future intervention development should move toward theoretically grounded, multicomponent designs that reflect the multidimensional nature of symptom experiences.
 |
Figure 2 Theoretical explanation for these findings, illustrating how integrated approaches provide more comprehensive outcomes target physiological, psychological, and behavioral pathways underlying symptom clusters. |
This discussion synthesizes the findings from 29 primary studies, mapping the current landscape of non-pharmacological interventions for managing symptom clusters, specifically the fatigue-sleep disturbance-depression (FSD) triad—in women with cancer. The evidence underscores a critical shift toward multicomponent and mechanism-based approaches, moving beyond traditional single-symptom management to address the synergistic nature of cancer-related distress.
The Role of Exercise and Cultural Adaptation in Functional Recovery
A core finding of this review is the robust efficacy of exercise-based programs, which range from multimodal high-intensity training to culturally adapted activities like Square Dance and Belly Dance.1,13,18 A unique contribution to the literature is the BLESS program, which emphasizes “social capital” as a driver for long-term adherence.17 The findings underscore that integrated non-pharmacological interventions, ranging from multimodal exercise programs to bundled psychoeducational rehabilitation using the teach-back method, provide feasible and cost-effective frameworks that significantly alleviate cancer-related fatigue while enhancing psychological resilience and quality of life for women with breast cancer.11,19 Furthermore, our findings on the importance of social support for adherence are reinforced by Pinto et al35 who argued that social environments are critical mediators for physical activity maintenance in breast cancer survivors. By integrating cultural and social components, these interventions move beyond purely physiological benefits to enhance psychosocial resilience.
Mind–Body Therapies and the “Common Mechanism” Theory
The efficacy of mind–body therapies, specifically Traditional Chinese Exercises (TCEs) like Tai Chi and Baduanjin, in alleviating the FSD symptom cluster suggests that these modalities target shared biological pathways.3,8 This review found that combining dynamic and static relaxation (Yoga and Benson relaxation) yielded superior outcomes in reducing total fatigue compared to routine care.34 This findings synergistic improvement supports the “common mechanism” theory proposed by Bower et al, which suggests that symptoms such as fatigue, depression, and sleep disturbance are driven by systemic inflammation and pro-inflammatory cytokine dysregulation (eg., IL-6 and TNF-alpha).36 By addressing these shared pathways rather than treating symptoms in isolation, mind–body interventions provide a more efficient and holistic therapeutic impact compared to pharmacological agents that are often limited to single-symptom relief.8
Complementary Therapies and Clinical Guideline Integration
Complementary strategies, including Adaptive Auricular Point Acupressure (APA) and Acupuncture, showed significant superiority in improving objective sleep parameters and reducing dependency on sedative-hypnotic medications.27,28 These results provide a robust argument for the clinical integration of non-invasive techniques. These findings are consistent with the Society for Integrative Oncology (SIO) and ASCO clinical practice guidelines, which recommend acupuncture and massage for managing treatment-related symptoms in breast cancer patients.37 Additionally, the validation of sensory-based therapies like lavender aromatherapy massage and slow-stroke back massage reinforces the role of non-pharmacological interventions in autonomic nervous system regulation during high-stress treatment phases.25,26
Psychosocial Interventions and the Digital Frontier
The review highlights a transition toward technology-based and nurse-led care models, such as the use of Virtual Reality (VR) for nature-based distraction32 and the “Bens app” for guided relaxation.31 These digital tools effectively bypass geographical barriers and enhance patient self-efficacy. However, the diminishing effects observed in virtual life coaching at 3-month follow-ups highlight a “washout effect” common in digital health4 This mirrors a broader trend noted by Kwekkeboom et al where sustained behavioral change in cancer survivors often requires ongoing support or “booster” sessions to maintain the benefits of cognitive-behavioral strategies38 Future technology-based models should prioritize longitudinal engagement strategies to ensure that clinical gains are preserved post-intervention. Nurse-led integrative models—combining continuous care with dietary interventions or emotional nursing with TCM needle embedding demonstrated high patient satisfaction and clinical efficacy.9,12 These models illustrate that oncology nurses are uniquely positioned to deliver multicomponent care within the social-medical model, addressing the physical, nutritional, and emotional needs of women with cancer.
Limitation
This review has several limitations. First, the heterogeneity of intervention types and outcome measures limits comparability across studies. Second, most studies were conducted in high-income countries, which may affect generalizability. Third, the limited use of explicit symptom-cluster frameworks in primary studies constrained deeper synthesis. The predominance of breast cancer populations in the included studies may limit the generalizability of findings to women with other cancer types.
Conclusion
Non-pharmacological interventions play a critical role in reducing symptom burden among women with cancer. However, the continued reliance on single-symptom approaches highlights a misalignment with the multidimensional nature of symptom experiences. Moving toward multicomponent, mechanism-informed interventions that explicitly target symptom clusters represents a promising direction for improving patient-centered outcomes and optimizing supportive care in women’s oncology.
Implications for Practice and Research
The findings have important implications for clinical practice and future research. In practice, they highlight the need to integrate exercise, mind–body, and psychosocial strategies within nurse-led care models, rather than implementing interventions in isolation. The growing evidence supporting technology-assisted delivery further underscores the feasibility of scaling such interventions in real-world settings. Nursing interventions should move beyond symptom-specific management toward integrated, patient-centered strategies that reflect the clustered and gender-sensitive nature of symptom experiences.
Future research should prioritize mediation analysis to further clarify the physiological mechanisms behind these interventions. For instance, the role of IL-37 in reducing fatigue, as explored by Syam et al,22 warrants further investigation to refine biological targets for non-pharmacological care There is a clear need to develop and test standardized integrated approaches guided by symptom-cluster frameworks, as well as to evaluate their long-term effectiveness and implementation across diverse populations and care settings. Advancing this line of inquiry will be essential to translate existing evidence into sustainable, patient-centered cancer care.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The author gratefully acknowledges Universitas Padjadjaran for providing access to research databases and financial support for this study.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Casla-Barrio S, Castellanos-Montealegre M, Pareja-Galeano H. The impact of multimodal high intensity exercise program comparing online and onsite interventions in breast cancer survivors: a randomized controlled trial. Clin Transl Oncol. 2025;28(1):184–14. doi:10.1007/s12094-025-03979-x
2. Darvishi E, Musarezaie A, Bahrami M, Karimian J. The effect of a combined exercise program on the fatigue severity of patients with breast cancer undergoing chemotherapy: a randomized clinical trial study. Iran J Nurs Midwifery Res. 2023;28(4):398–404. doi:10.4103/ijnmr.ijnmr_399_22
3. Wei X, Yuan R, Yang J, et al. Effects of Baduanjin exercise on cognitive function and cancer-related symptoms in women with breast cancer receiving chemotherapy: a randomized controlled trial. Support Care Cancer. 2022;30(7):6079–6091. doi:10.1007/s00520-022-07015-4
4. Tock WL, Maheu C, Blondin S, Lee V, Neuman S, Meterissian S. The effect of life coaching on post-traumatic growth and well-being in breast cancer survivors: a randomized controlled trial. Psychooncology. 2025;34(10). doi:10.1002/pon.70295
5. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
6. GLOBOCAN. Global Cancer Observatory: Cancer Today. 2022. Available from: https://gco.iarc.who.int/today.
7. Karaman S, Tan M. Effect of reiki therapy on quality of life and fatigue levels of breast cancer patients receiving chemotherapy. Cancer Nurs. 2021;44(6):E652–E658. doi:10.1097/NCC.0000000000000970
8. Yao LQ, Kwok SWH, Tan JY, et al. The effect of an evidence-based Tai chi intervention on the fatigue-sleep disturbance-depression symptom cluster in breast cancer patients: a preliminary randomised controlled trial. Eur J Oncol Nurs. 2022:61. doi:10.1016/j.ejon.2022.102202.
9. Ren Z, Cui W, Li YP. Application of traditional Chinese medicine acupoint needle embedding combined with emotional nursing in patients with gynecological malignant tumors. World J Psychiatry. 2023;13(9):645–653. doi:10.5498/wjp.v13.i9.645
10. Mostafaei F, Azizi M, Jalali A, Salari N, Abbasi P. Effect of exercise on depression and fatigue in breast cancer women undergoing chemotherapy: a randomized controlled trial. Heliyon. 2021;7(7):e07657. doi:10.1016/j.heliyon.2021.e07657
11. Rashwan ZI, Shaheen SR, El RASAEFA, Kamel NMF, Darweesh HAM. Empowering mind-body wellness: effect of bundling seated exercises and psychoeducational rehabilitation using the teach-back approach on fatigue and coping of women postmastectomy. BMC Womens Health. 2024;24(1). doi:10.1186/s12905-024-03242-5
12. Yu Z, Song L, Wei X, Wang L, Cui L. Effects of continuous care combined with dietary care on sleep quality and quality of life in patients with breast cancer fatigue. Breast Care. 1–8. doi:10.1159/000548024
13. He X, MSN N, Choi KC, WKW S. Effects of a 16-week dance intervention on the symptom cluster of fatigue-sleep disturbance-depression and quality of life among patients with breast cancer undergoing adjuvant chemotherapy: a randomized controlled trial. Int J Nurs Stud. 2022;133:104317. doi:10.1016/j.ijnurstu.2022.104317
14. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int. J. Soc. Res. Methodo. 2005;8(1):19–32. doi:10.1080/1364557032000119616
15. Peters MDJ, Marnie C, Tricco AC, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. 2020;18(10):2119–2126. doi:10.11124/JBIES-20-00167
16. Chang L, Wang Y, Zhang J, Zhao W, Li X, Yang L. Effect of music therapy combined with aerobic exercise on sleep quality among breast cancer patients undergoing chemotherapy after a radical mastectomy: a randomized controlled trial. BMC Womens Health. 2024;24(1). doi:10.1186/s12905-024-03241-6
17. Han J, Jang MK, Lee H, et al. Long term effects of a social capital-based exercise adherence intervention for breast cancer survivors with moderate fatigue: a randomized controlled trial. Integr Cancer Ther. 2023:22. doi:10.1177/15347354231209440.
18. Boing L, de B FT, Lynch BM, et al. Mat Pilates and belly dance: effects on patient-reported outcomes among breast cancer survivors receiving hormone therapy and adherence to exercise. Complement Ther Clin Pract. 2023:50. doi:10.1016/j.ctcp.2022.101683.
19. Zhang H, Meng Y, Jiang R, Ge S, Song M. Effect of multimodal exercise on cancer-related fatigue in patients undergoing simultaneous radiotherapy and chemotherapy: a randomized trial in patients with breast cancer. Altern Ther Health Med. 2023;29;(5):233–7
20. Liu Q, Wang C, Wang Y, et al. Mindfulness-based stress reduction with acupressure for sleep quality in breast cancer patients with insomnia undergoing chemotherapy: a randomized controlled trial. Eur J Oncol Nurs. 2022:61. doi:10.1016/j.ejon.2022.102219.
21. Luyan G, Lizhi Z, Shufang Z, et al. Effects of dynamic and static relaxation therapy on cancer-induced fatigue and sleep disorders in patients with breast cancer undergoing chemotherapy: a randomized control trial. Support Care Cancer. 2025;33(1). doi:10.1007/s00520-024-09123-9
22. Syam Y, Prihantono P, Sjattar EL, Puspitha A, Majid S. The effect of Apis dorsata honey as complementary therapy on IL-37 levels and fatigue in breast cancer patients undergoing chemotherapy. Breast Dis. 2021;40(S1):S129–S133. doi:10.3233/BD-219020
23. Kalroozi F, Moradi M, Ghaedi-Heidari F, Marzban A, Raeisi-Ardali SR. Comparing the effect of emotional freedom technique on sleep quality and happiness of women undergoing breast cancer surgery in military and nonmilitary families: a quasi-experimental multicenter study. Perspect Psychiatr Care. 2022;58(4):2986–2997. doi:10.1111/ppc.13150
24. Rissling M, Liu L, Youngstedt SD, et al. Preventing sleep disruption with bright light therapy during chemotherapy for breast cancer: a phase ii randomized controlled trial. Front Neurosci. 2022;16. doi:10.3389/fnins.2022.815872
25. Zhang F, Cheng L, Qin S, et al. Effect of aromatherapy massage with lavender essential oil on sleep quality, pain, and mental and psychiatric disorders among breast cancer patients undergoing chemotherapy: a randomized controlled trial. Support Care Cancer. 2025;33(8). doi:10.1007/s00520-025-09741-x
26. Bahceli PZ, Arslan S, Ilik Y. The effect of slow-stroke back massage on chemotherapy-related fatigue in women with breast cancer: an assessor blinded, parallel group, randomized control trial: effect of slow stroke back massage on CRF. Complement Ther Clin Pract. 2022;46:101518. doi:10.1016/j.ctcp.2021.101518
27. Wang Y, Li X, Ji X, et al. Adaptive auricular point acupressure for sleep disturbance in women with breast cancer: a randomized controlled trial. Evid Based Complement Alternat Med. 2022;2022:1–11. doi:10.1155/2022/8637386
28. Zhang J, Qin Z, So TH, et al. Acupuncture for chemotherapy-associated insomnia in breast cancer patients: an assessor-participant blinded, randomized, sham-controlled trial. Breast Cancer Res. 2023;25(1). doi:10.1186/s13058-023-01645-0
29. Mohandass B, Singh S, Kumar Bhalla N. Oncology and Radiotherapy © Effectiveness of Multicomponent Intervention on Radiotherapy Induced Fatigue and Its Corelates among Breast Cancer Patients. 2024.
30. Lai HL, Chen CI, Lu CY, Huang CY. Cognitive behavioral therapy plus coping management for depression and anxiety on improving sleep quality and health for patients with breast cancer. Brain Sci. 2021;11(12):1614. doi:10.3390/brainsci11121614
31. Cahyono HD, Irawaty D, Adam M. The effect of Benson relaxation application (‘Bens app’) on reducing fatigue in patients with breast cancer undergoing chemotherapy: a quasi-experimental study. Belitung Nurs J. 2022;8(4):304–310. doi:10.33546/bnj.1843
32. Uslu A, Arslan S. The effect of using virtual reality glasses on anxiety and fatigue in women with breast cancer receiving adjuvant chemotherapy: a pretest-posttest randomized controlled study. Semin Oncol Nurs. 2023;39(5):151503. doi:10.1016/j.soncn.2023.151503
33. Ou YY, Liu S, Zhang JL, Yuan HZ, Zheng YH. Effects of whole-course standardized nursing and humanistic care on the sleep condition and quality of life of elderly patients undergoing hysterectomy for cervical cancer. Eur J Gynaecol Oncol. 2021;42(1):154–160. doi:10.31083/j.ejgo.2021.01.2137
34. Yan Z, Xiao LD, Guo X, Hu Y, Wang N, Wang Y. The impact of social support and social constraints on sleep disturbances in patients with lung cancer undergoing chemotherapy: serial mediators of sleep cognition and anxiety-depression. Asia Pac J Oncol Nurs. 2025;12. doi:10.1016/j.apjon.2025.100740
35. Pinto BM, Dunsiger S, Waldemore M. Physical activity and psychosocial benefits among breast cancer patients. Psychooncology. 2013;22(10):2193–2199. doi:10.1002/pon.3272
36. Bower JE, Ganz PA, Irwin MR, Kwan L, Breen EC, Cole SW. Inflammation and behavioral symptoms after breast cancer treatment: do fatigue, depression, and sleep disturbance share a common underlying mechanism? J Clin Oncol. 2011;29(26):3517–3522. doi:10.1200/JCO.2011.36.1154
37. Greenlee H, DuPont-Reyes MJ, Balneaves LG, et al. Clinical practice guidelines on the evidence-based use of integrative therapies during and after breast cancer treatment. CA Cancer J Clin. 2017;67(3):194–232. doi:10.3322/caac.21397
38. Kwekkeboom K, Zhang Y, Campbell T, et al. Randomized controlled trial of a brief cognitive-behavioral strategies intervention for the pain, fatigue, and sleep disturbance symptom cluster in advanced cancer. Psychooncology. 2018;27(12):2761–2769. doi:10.1002/pon.4883
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.