Back to Journals » Clinical Ophthalmology » Volume 20
Non-Interventional Study to Evaluate the Effect of Non-Diffractive Extended Depth of Focus Intraocular Lens Centration and Tilt on Visual Performance
Authors Shetty R, Chokshi A, Paauw M, Francis J, Freidl K, Orey D, Egli A, Keeton H, Click K, Schaffner H, Wagner I ![]() , Hasan A, Gayasaddin O, Lott M, Goldfaden R
, Hasan A, Gayasaddin O, Lott M, Goldfaden R ![]()
Received 30 January 2026
Accepted for publication 30 May 2026
Published 9 June 2026 Volume 2026:20 600053
DOI https://doi.org/10.2147/OPTH.S600053
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Rajesh Shetty,1 Amit Chokshi,1 Mark Paauw,1 Joanne Francis,1 Kathryn Freidl,1 Dontia Orey,2 Anna Egli,1 Haleigh Keeton,2 Kaitlyn Click,2 Hannah Schaffner,2 Isabella Wagner,3 Akbar Hasan,1 Omar Gayasaddin,1 McGregor Lott,1 Rebecca Goldfaden2
1Florida Eye Specialists, Jacksonville, FL, USA; 2East Coast Institute for Research, Jacksonville, FL, USA; 3University of Florida, College of Medicine, Jacksonville, FL, USA
Correspondence: Rebecca Goldfaden, East Coast Institute for Research, 3550 University Blvd S #101, Jacksonville, FL, 32216, USA, Tel +1904-854-1354, Fax +1904-854-1355, Email [email protected]
Purpose: Evaluate whether visual acuity is influenced by intraocular lens (IOL) decentration or tilt with Clareon® Vivity® and Clareon® Vivity® Toric IOLs.
Methods: This was a non-interventional, retrospective, single-arm, observational study. Adults with Clareon® Vivity® or Vivity® Toric IOLs without significant posterior capsule opacification, significant history of ocular surgery, or major ocular pathologies were included. Postoperative assessments performed ≥ 1 month after surgery included monocular high-contrast corrected and uncorrected distance visual acuity (CDVA, UDVA, 4 m), distance-corrected and uncorrected intermediate visual acuity (DCIVA, UIVA, 66 cm), manifest refraction spherical equivalent (MRSE), low-contrast CDVA, IOL decentration and tilt, mesopic pupil size, and corneal higher-order aberrations. The primary outcome was the association between the CDVA and IOL decentration or tilt.
Results: A total of 202 eyes (n=101) were analyzed: 140 eyes (69%) received Clareon® Vivity® and 62 eyes (31%) received Vivity® Toric. The mean IOL decentration was 0.211 mm (SD 0.13) and the mean tilt was 5.6° (SD = 1.18). Mean CDVA was 0.056 logMAR, UCDVA was 0.155 logMAR, DCIVA was 0.018 logMAR, UCIVA was 0.019 logMAR, and MRSE was – 0.147 D. In unadjusted analyses, no significant correlations were found between CDVA and decentration (r = 0.12, p = 0.08) or tilt (r = 0.06, p = 0.43), nor between DCIVA and decentration (r = 0.07, p = 0.34) or tilt (r = – 0.13, p = 0.07). In adjusted multivariable regression analyses, IOL decentration was significantly associated with postoperative CDVA100 (β=0.618, p=0.023), whereas residual refractive cylinder and IOL tilt were not independently associated with postoperative visual outcomes.
Conclusion: Clareons’ Vivity® and Vivity® Toric IOLs demonstrated excellent distance and intermediate visual acuity. Visual outcomes remained generally favorable despite modest decentration or tilt, although adjusted analyses identified a modest association between decentration and postoperative CDVA100, supporting clinical reliability of this IOL design.
Keywords: cataracts, IOL implant, EDOF
Introduction
Cataracts are a leading cause of treatable blindness worldwide.1 However, cataract surgery is among the most common and successful procedures performed in the United States (US), with success rates exceeding 97%.2 Cataract surgery involves the removal of the natural opacified lens and replacement with an artificial intraocular lens (IOL) implant. The procedure involves removal of the opacified crystalline lens and implantation of an artificial IOL. While the original purpose of cataract surgery was to restore basic functional vision, advances in surgical techniques and IOL technology have shifted expectations toward achieving high-quality uncorrected vision across multiple distances (near, intermediate, and distance).
Since the first IOL implantation in 1949, significant innovations have been made in the IOL materials and designs. Numerous US Food and Drug Administration (FDA)- approved IOLs are now available, and advancements in their design and technology have improved over time.3 Among these, extended depth of focus (EDOF) lenses have gained attention for their ability to reduce dependence on corrective lenses post-surgery while minimizing visual disturbances commonly associated with diffractive multifocal IOLs. Non-diffractive EDOF designs extend the range of vision while reducing the risks of halos and glare.
Despite these advances, postoperative IOL tilt and decentration may still occur because of preoperative anatomy, intraoperative techniques, or postoperative changes.4 The literature suggests that a tilt greater than 3° or decentration exceeding 0.3 mm can degrade optical quality and negatively affect patient satisfaction.4 This has raised interest in developing IOLs that maintain visual performance even when minor misalignment occurs.
Several studies evaluating multifocal and EDOF IOLs have demonstrated that tilt and decentration may induce higher-order aberrations (HOAs), including coma, and may adversely affect visual performance, specifically in diffractive and negative spherical aberration-correcting designs.5,6 McCabe C et al demonstrated that decentration and tilt of aspheric IOLs may increase wavefront aberrations and reduce optical quality, particularly in lenses with negative spherical aberration correction.6 Similarly, IOL misalignment may contribute to dysphotopsia, coma, and reductions in visual quality.4 However, nondiffractive wavefront-shaping EDOF platforms such as Clareon Vivity® (Alcon Inc., Fort Worth, Texas, USA) may demonstrate greater tolerance to modest positional variability because they do not rely on diffractive step transitions for focal extension.7 In 2022, Alcon introduced Clareon® (Alcon Inc., Fort Worth, Texas, USA), a next-generation hydrophobic acrylic IOL material containing hydroxyethyl methacrylate (HEMA). Compared with the widely used AcrySof® (Alcon Inc., Fort Worth, Texas, USA) platform, Clareon® incorporates a higher and more evenly distributed water content (1.5% vs. 0.4%), which enhances optical clarity and renders the lens glistening-free.8 The Clareon Vivity® IOL applies this material advancement to a novel, nondiffractive EDOF design. Unlike traditional multifocal or diffractive EDOF lenses that split light into multiple foci (often producing negative visual side effects such as halos), Clareon® Vivity® employs proprietary X-WAVE™ wavefront-shaping technology to extend the range of vision while minimizing photic phenomena.7
Clareon® IOLs have demonstrated excellent mechanical stability in FDA registration studies.9 However, to date, no study has specifically assessed how decentration and tilt affect the visual performance of Clareon® Vivity® and Vivity®-toric lenses. The present study was designed to evaluate whether the unique non-diffractive design of these IOLs reduces sensitivity to misalignment, and to assess the impact of decentration and tilt on visual outcomes.
Methods
This was a retrospective, non-interventional, single-center, single-arm, multi-surgeon, observational study. The study population included patients who had previously been implanted with Clareon® Vivity® and Clareon® Vivity® Toric IOLs. After informed consent was obtained, preoperative and operative implantation data were collected retrospectively, and postoperative assessments were performed at least one month postoperatively. Examinations included measurements of manifest refraction spherical equivalent (MRSE) monocular uncorrected and corrected distances, and intermediate visual acuities. Decentration and tilt of the IOLs were measured using the CASIA2 anterior segment optical coherence tomography (AS-OCT) system (Tomey Corp., Nagoya, Japan) under standard dilated conditions. The CASIA2 utilizes swept-source OCT imaging to produce anterior segment images and automatically calculate IOL position relative to the vertex normal, which served as the reference axis in this study. The vertex normal is defined as a line perpendicular to the corneal surface at the corneal vertex that passes through the fixation point of the eye. IOL decentration was defined as the linear distance (mm) between the IOL optic center and the vertex normal. IOL tilt was defined as the angle (degrees) between the IOL optic axis and the vertex normal. IOL tilt and decentration measurements were obtained using the CASIA2’s automated software following image acquisition centered on the visual axis.
The coma (vertical and horizontal) and spherical higher-order aberrations (HOAs) of the cornea were measured using an iTrace wavefront aberrometer (Tracey Technol., Houston, Texas). This study was approved by the Advarra Institutional Review Board (IRB) (approval number: Pro00070379), conducted in accordance with the Health Insurance Portability and Accountability Act (HIPAA) regulations and participant consent, and adhered to the Tenets of the Declaration of Helsinki. The registration number of This study was registered on the National Institute of Health (NIH) website https://clinicaltrials.gov/ (NCT05827133).
The relationship between dilated IOL decentration and tilt to all visual acuity (VA) endpoints was analyzed by varying the measurements of monocular VA, including corrected distant VA (CDVA; 4m; logMAR), uncorrected distant VA (UCDVA; 4 m; logMAR), distance-corrected intermediate VA (DCIVA; 66 cm; logMAR), and uncorrected intermediate VA (UCIVA, 66 cm; logMAR), manifest refraction/MRSE, mesopic pupil size (mm), dilated IOL decentration (mm) and tilt (°), and dilated corneal coma and spherical HOA (µm). CDVA, UCDVA, DCIVA, and UCIVA were measured with 100% contrast under photopic conditions using the ETDRS Sloan chart with logMAR notation and ETDRS Format chart. In addition to 100% contrast, CDVA was measured at 25% contrast as an exploratory endpoint.
Adult patients eligible to participate in the study demonstrated a history of adult cataract and uneventful, refractive cataract surgery with Clareon® Vivity® and Vivity® Toric IOL with manifest refraction/manifest refraction spherical equivalent (MRSE) within ±1.00 D and a willingness to undergo an eye exam with pupil dilation. Patients excluded from the study had any of the following: moderate to severe posterior capsule opacification (2+ or more), yttrium aluminum garnet (YAG) laser capsulotomy within one month prior to enrollment, laser-assisted in situ keratomileusis (LASIK) or photorefractive keratectomy (PRK) within the one year prior to IOL implantation or any time after IOL implantation, any previous ocular surgery (excluding YAG, LASIK, PRK), clinically significant ocular pathology, severe diabetic retinopathy, age-related macular degeneration (AMD), glaucoma, severe dry eye, irregular astigmatism, zonular weakness, pseudoexfoliation, ocular trauma, any additional procedure(s) at the same time as the cataract surgery (including but not limited to microinvasive glaucoma surgery (MIGS)), women who were pregnant at the time of screening (based on self-reported history), medical or other problems which in the opinion of the investigator render study participation unsafe.
The exposures of interest were IOL decentration (mm) and tilt (°), and the primary endpoint was monocular CDVA (4 m) (logMAR). Secondary endpoints were monocular UCDVA (4 m) (logMAR), monocular DCIVA (66 cm) (logMAR), monocular UCIVA (66 cm) (logMAR), and MRSE (D). The exploratory endpoints were the mean photopic low-contrast (25%) monocular CDVA (4 m) (logMAR), mesopic pupil size (mm), and HOAs (coma and spherical) of the cornea (µm).
The sample size was based on the primary outcome of the CDVA. The primary modelling strategy was multiple linear regression, as described below. For the CDVA outcome, we modeled CDVA (treated as a continuous variable) as the dependent or outcome variable and tilt and decentration as the independent variables of interest. Sample size justification based on simulations indicated that with a two-sided α<0.05, 200 eyes would provide ≥87% power to detect a population effect size of 5 letters (0.1 in logMAR scale) per 1° change in tilt and 4 letters (0.08 in logMAR scale) per 0.1 mm variation in decentration.
Baseline summary measures (mean ± standard deviation (SD), median [range], and n [%]) were used to characterize the enrolled patient population, including measures of the primary exposures of interest (decentration and tilt) and outcomes (visual acuity measures (s)). The study explored unadjusted associations between exposures and outcomes of interest, followed by adjusted associations between exposures and outcomes of interest in each case following a similar approach. For example, for the primary outcome, we first correlated monocular CDVA and decentration, and separately correlated monocular CDVA and tilt. For adjusted analyses, we fitted a multiple linear regression model with CDVA as the outcome (dependent variable), decentration and tilt as the primary exposures (independent variables) of interest, and additional covariates (MRSE and mesopic pupil size). Each visual acuity outcome was modelled in a similar fashion, exchanging the dependent variable in the model and, if necessary, adjusting the covariates included in the model.
Additional sensitivity analyses were performed for the primary endpoint (CDVA100) and multivariable linear regression models were expanded to include postoperative residual refractive cylinder (manifest refractive cylinder [mRC]) as a covariate. Stratified analyses were also conducted based on residual refractive cylinder (≤0.50 D, >0.50 D, and ≤0.75 D) and IOL type (ie. toric versus non-toric). Interactions between decentration and mRC and between tilt and mRC were evaluated to assess whether residual refractive cylinder modified the relationship between IOL decentration or tilt and postoperative visual outcomes.
Lastly, since both eyes from subjects were included in the analysis, a sensitivity analyses using generalized estimating equations (GEE) with an exchangeable working correlation structure was also performed to account for within-subject inter-eye correlation.
Results
Table 1 outlines the baseline preoperative characteristics of the study population (202 eyes of 101 subjects). The mean age at surgery was 71 years (standard deviation [SD], 6 years), with a range from 54.9 to 88.7 years and a median of 70.75 years. The cohort comprised of 45 males (45%) and 56 females (55%). With respect to intraocular lens type, 140 eyes (69%) received a non-toric IOL, and 62 eyes (31%) received a toric IOL. The baseline CDVA at 4 m under high-contrast conditions (CDVA100) averaged 0.177 logMAR (SD, 0.166; range, 0–1.0), with a median of 0.10 logMAR. The mean MRSE was –0.031 D (SD 2.801), ranging from –15.62 D to +4.75 D, with a median of +0.685 D.
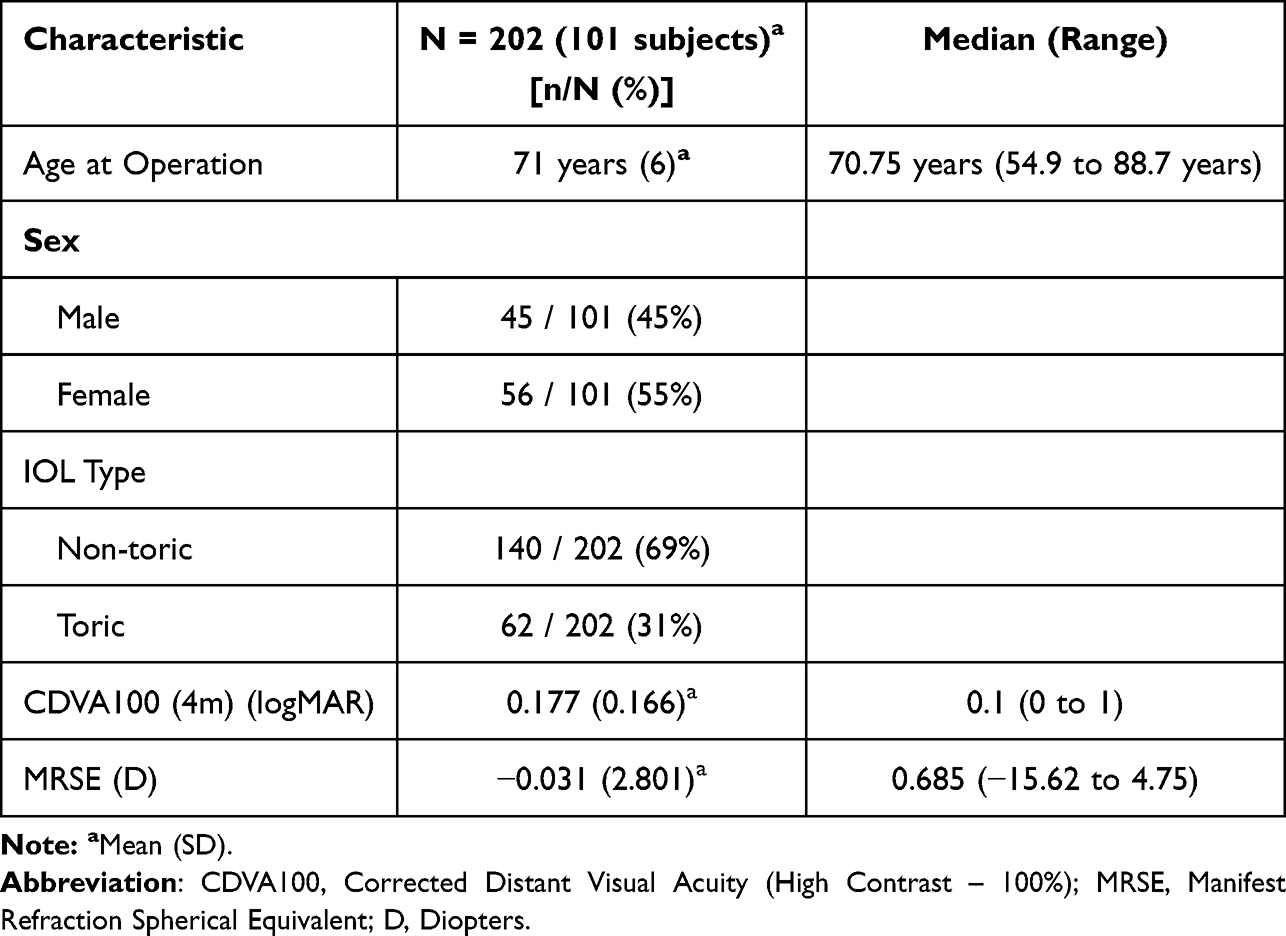 |
Table 1 Baseline Characteristics and Pre-Operational Biometric Data |
Table 2 and Figure 1 summarize the postoperative biometric measurements. The mean CDVA under high-contrast conditions (CDVA100, 4 m) was 0.056 logMAR (SD, 0.110), with values ranging from –0.10 to 1.00 and a median of 0.00. CDVA at low contrast (CDVA25) averaged 0.171 logMAR (SD 0.119; range 0.00 to 0.60; median 0.20). UCDVA under high-contrast conditions (UCDVA100) was 0.155 logMAR (SD 0.143), spanning –0.10 to 1.00 with a median of 0.10. At an intermediate distance (66 cm), the mean UCIVA under high-contrast conditions (UCIVA100) was 0.019 logMAR (SD 0.100; range –0.20 to 0.40; median, 0.00), whereas that under high-contrast conditions (DCIVA100) was 0.018 logMAR (SD 0.068; range –0.10 to 0.30; median 0.00).
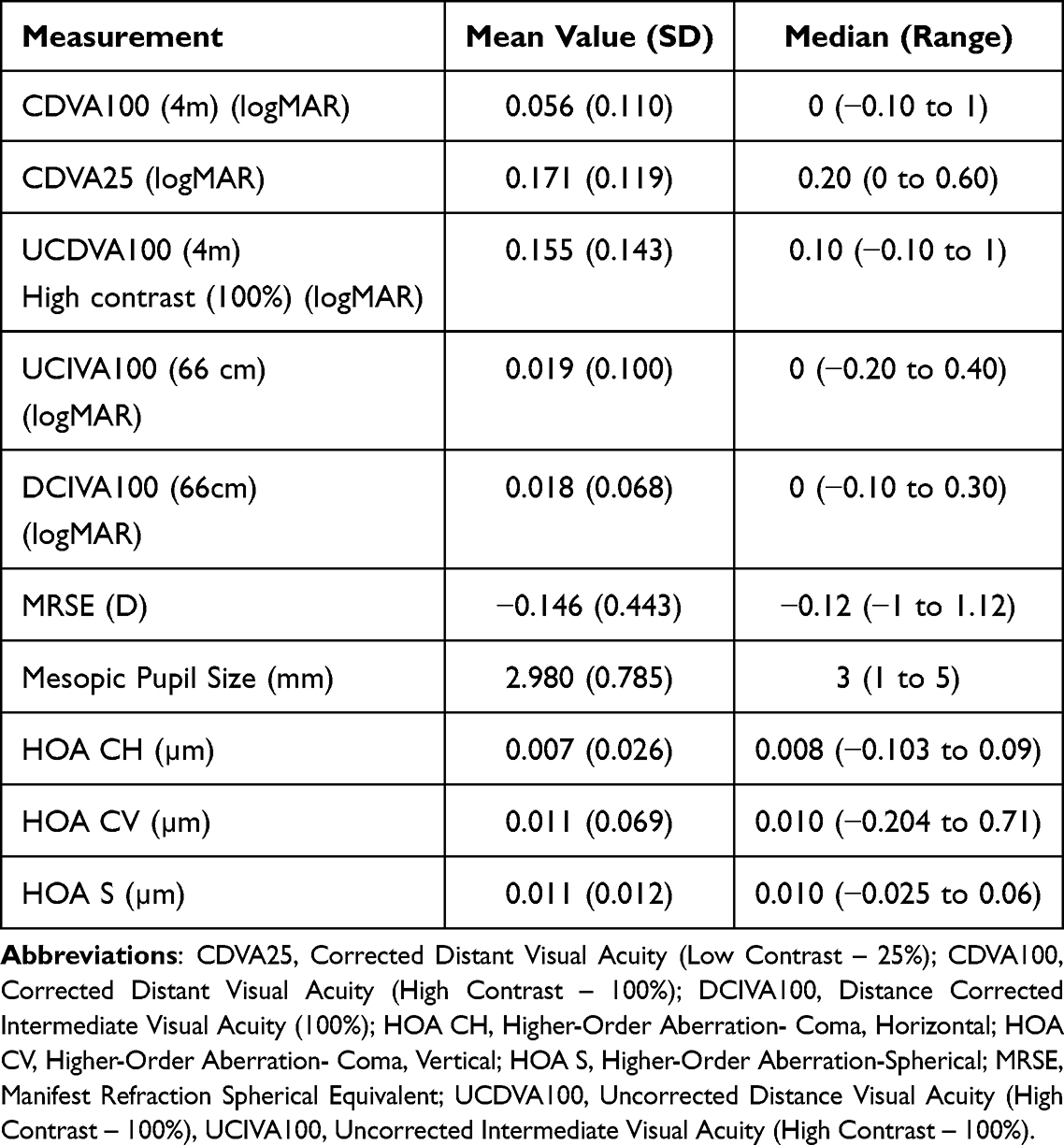 |
Table 2 Post-Operational Biometric Data |
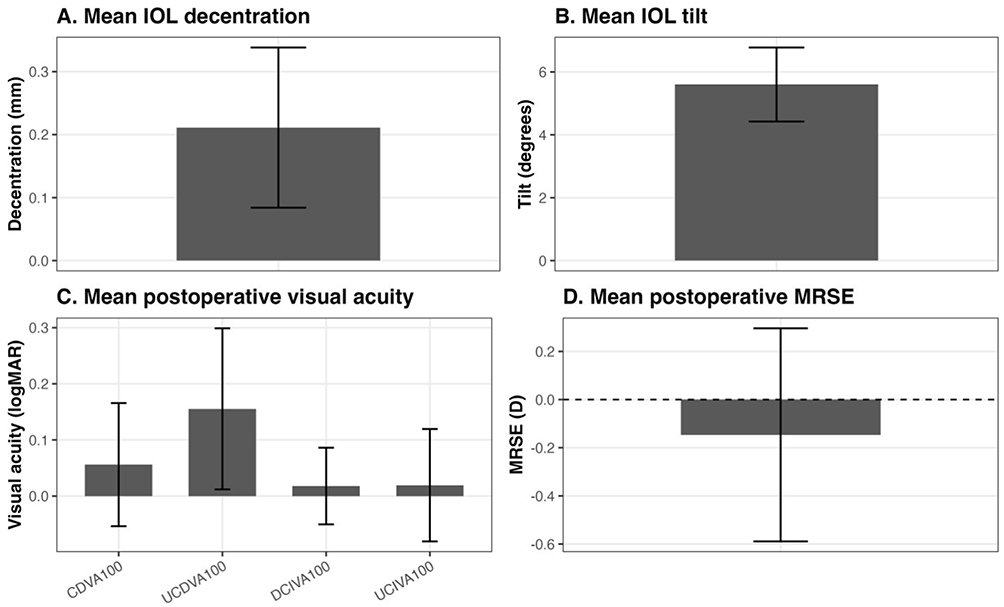 |
Figure 1 Post-Operational Biometric Data and Primary Exposures of Interest. (A) Mean IOL decentration. (B) Mean IOL tilt. (C) Mean postoperative visual acuity measures (CDVA100, UCDVA100, DCIVA100, and UCIVA100). (D) Mean postoperative manifest refraction spherical equivalent (MRSE). |
The mean MRSE was –0.146 D (SD 0.443; range –1.00 to +1.12 D; median –0.12 D). Mesopic pupil size averaged 2.98 mm (SD 0.785), ranging from 1.00 to 5.00 mm with a median of 3.00 mm. The HOA values were minimal for horizontal coma (0.007 µm, SD 0.026; range: −0.103 to 0.090), vertical coma (0.011 µm, SD 0.069; range –0.204 0.710), and spherical aberration (0.011 µm, SD = 0.012; range: 0.025 to 0.060).
Primary Exposures of Interest
Table 3 and Figure 1 summarize the primary exposures of interest, intraocular lens (IOL) decentration, and tilt. The mean IOL decentration was 0.211 mm (SD 0.127), with values ranging from 0 mm to 0.84 mm and a median of 0.19 mm. The mean IOL tilt was 5.6° (SD = 1.178), ranging from 2.6° to 8.6° with a median of 5.6°.
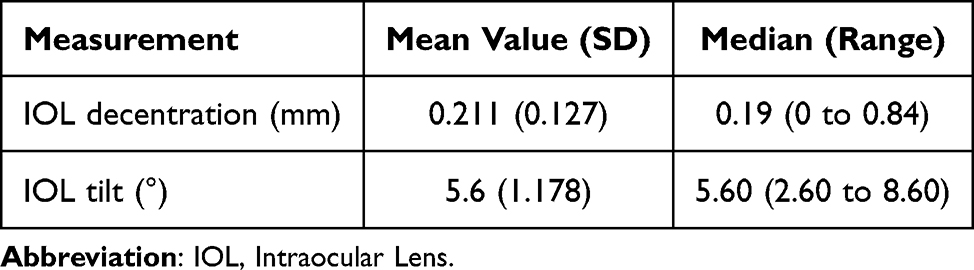 |
Table 3 Primary Exposures of Interest |
Primary Endpoint
Table 4 and Figure 2 present the relationship between corrected distance visual acuity (DVA under high-contrast conditions (100% at 4 m)) and the IOL positioning parameters. The CDVA showed only a weak, non-significant correlation with IOL decentration (r = 0.12, p = 0.08; 95% CI: –0.02 0.26) and tilt (r = 0.056, p = 0.43; 95% CI: –0.08, 0.19).
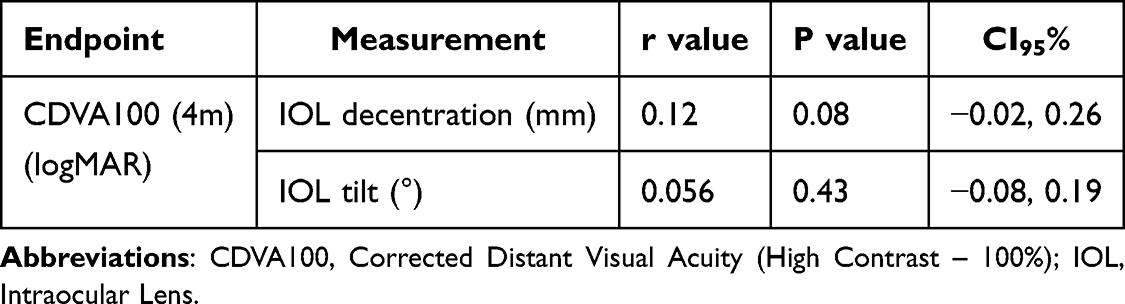 |
Table 4 Primary Endpoint- Relationship Between CDVA with IOL Decentration and IOL Tilt |
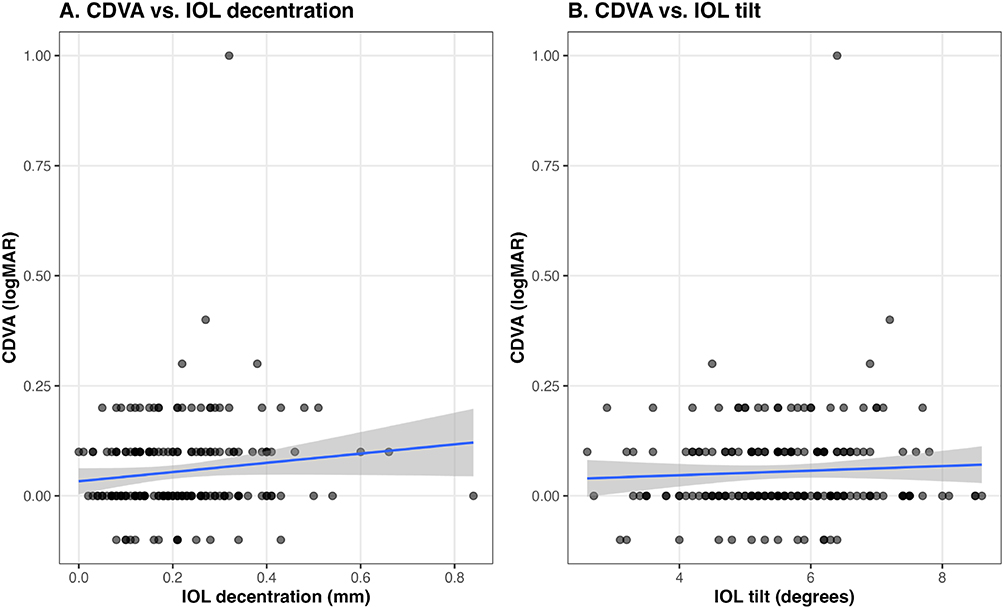 |
Figure 2 Primary Endpoint- Relationship between CDVA with IOL Decentration and IOL Tilt. (A) Relationship between CDVA100 and IOL decentration. (B) Relationship between CDVA100 and IOL tilt. |
In multivariable regression analyses (Table 5) adjusting for mesopic pupil size, IOL tilt, and postoperative residual refractive cylinder (mRC), IOL decentration remained significantly associated with postoperative CDVA100 (p=0.023), whereas mRC and IOL tilt were not independently associated with CDVA100. The interaction between decentration and mesopic pupil size demonstrated a borderline statistically significant association (p=0.057).
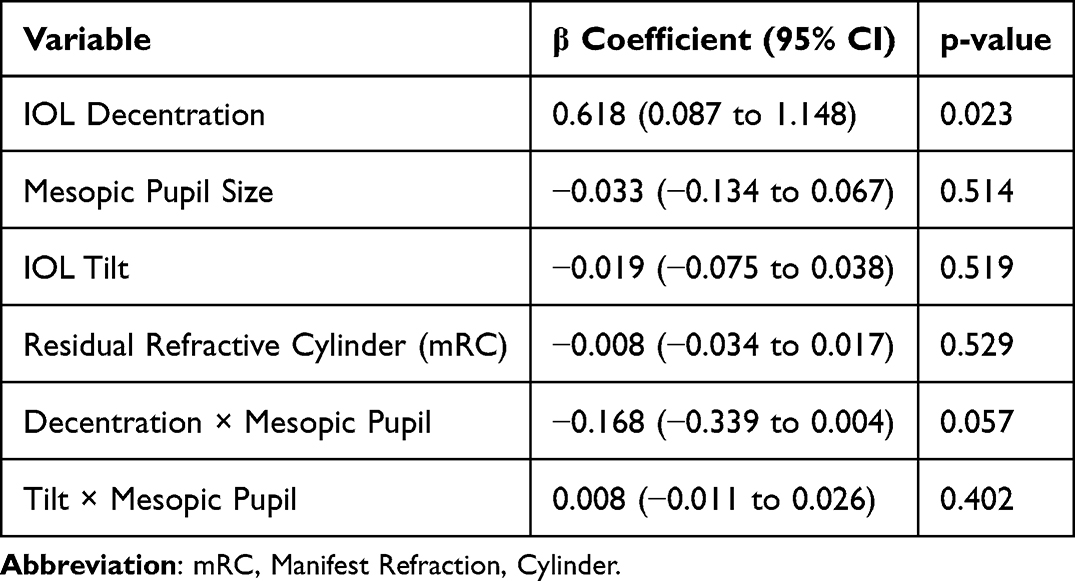 |
Table 5 Multivariable Regression Analysis for CDVA100 |
Multiple subgroup analyses were performed and Table 6 list the results of the associations between IOL decentration and postoperative CDVA100. Stratified analyses demonstrated that the association between decentration and CDVA100 remained significant in eyes with low residual refractive cylinder (mRC ≤0.50 D; p=0.027) and in eyes with mRC ≤0.75 D (p=0.028). No significant association was identified in eyes with mRC >0.50 D, although this subgroup was limited by small sample size.
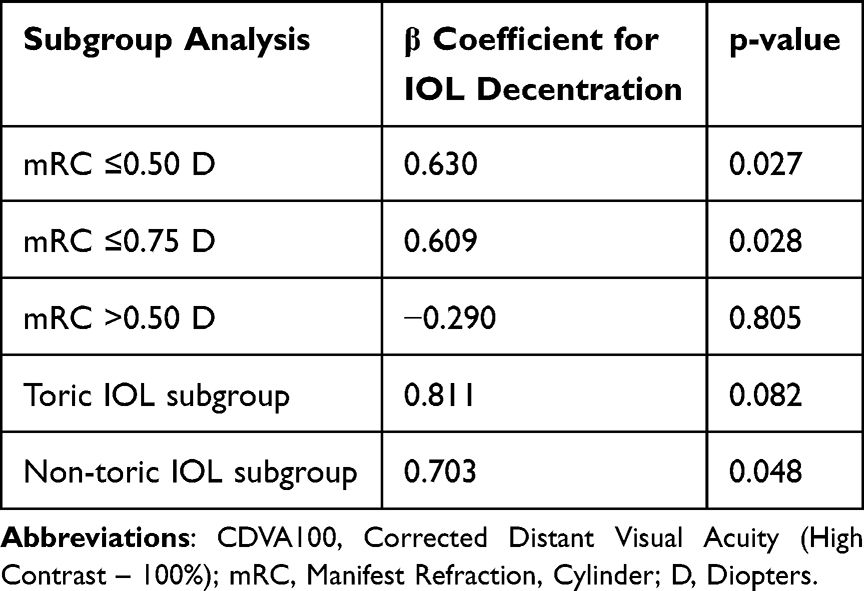 |
Table 6 Subgroup Analysis Evaluating the Association Between IOL Decentration and Postoperative CDVA100 |
When stratified by IOL type, the regression models demonstrated similar results between toric and non-toric subgroups. Decentration remained minimally significantly associated with CDVA100 in the non-toric subgroup (p=0.048), whereas the toric subgroup demonstrated a comparable association that did not reach statistical significance (p=0.082), potentially due to reduced sample size.
Interaction analyses evaluating decentration × mRC and tilt × mRC did not exhibit statistically significant interaction effects, suggesting that residual refractive cylinder did not significantly change the relationship between IOL decentration or tilt and postoperative visual acuity outcomes.
Sensitivity analyses using Generalized Estimating Equation (GEE) to account for inter-eye correlation produced similar findings (Table 7), with IOL decentration remaining significantly associated with postoperative CDVA100 (p=0.035), whereas IOL tilt and mRC were not significantly associated with postoperative visual outcomes.
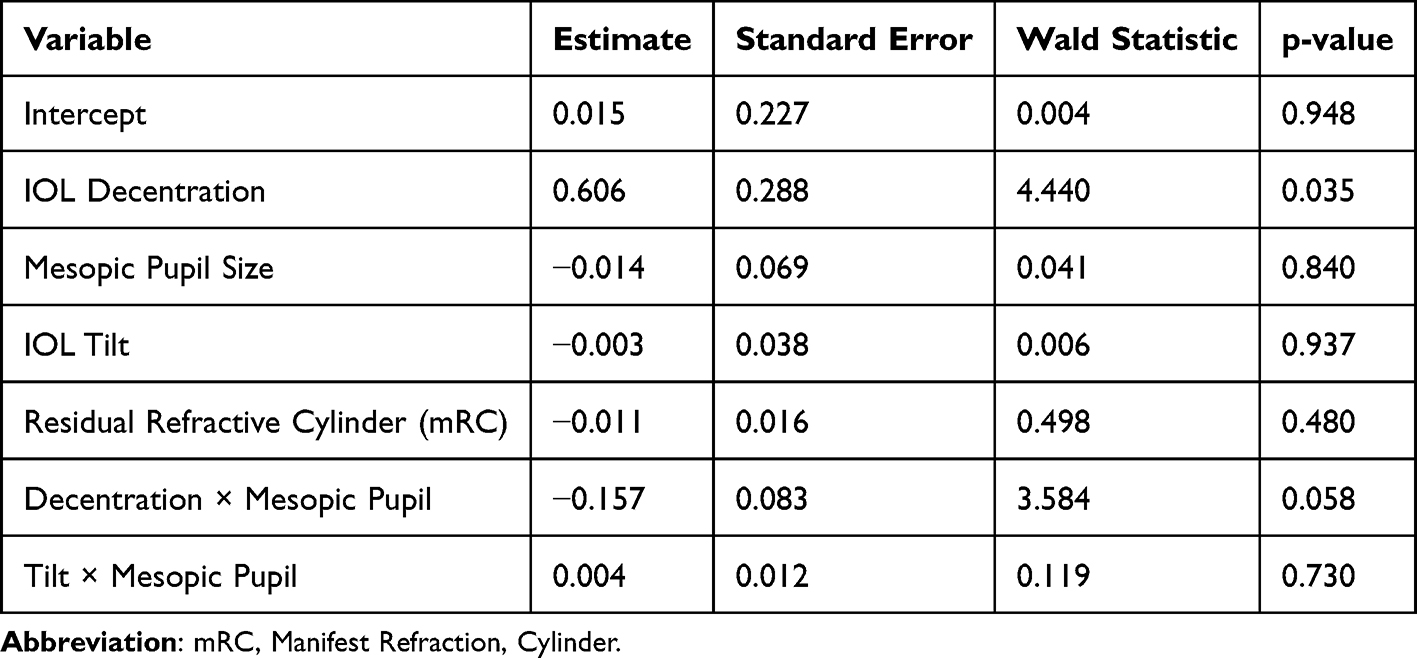 |
Table 7 Generalized Estimating Equation (GEE) Analysis for Postoperative CDVA100 |
Secondary Endpoints
Table 8 shows the correlations between IOL decentration and tilt, and secondary visual and refractive outcomes. For the DCIVA at 66 cm under high-contrast conditions, the correlations with both decentration (r = 0.07, p = 0.34; 95% CI: –0.07 0.20) and tilt (r = –0.13, p = 0.07; 95% CI: –0.26 0.0088) were weak and not statistically significant. Similarly, for UCIVA, no meaningful associations were observed with decentration (r = 0.002, p = 0.98) or tilt (r = –0.13, p = 0.06).
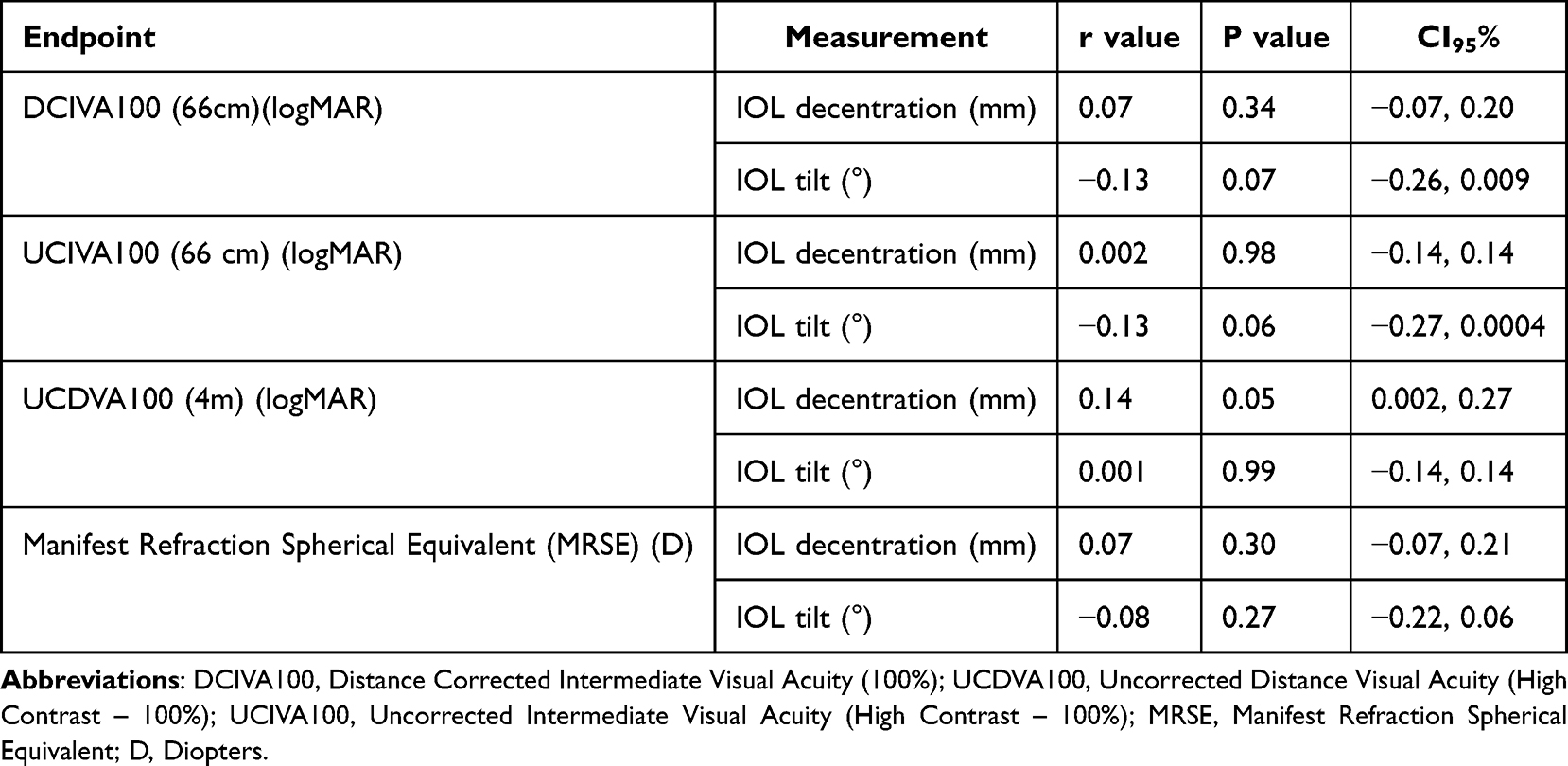 |
Table 8 Secondary Endpoint- Relationship with Secondary Measures with IOL Decentration and IOL Tilt |
For UCDVA, a borderline significant correlation was observed with IOL decentration (r = 0.14, p = 0.05; 95% CI: 0.002–0.27), whereas tilt was not associated (r = 0.0006, p = 0.99). Finally, MRSE showed no significant correlation with either decentration (r = 0.07, p = 0.30) or tilt (r = − 0.08, p = 0.27).
Exploratory Endpoints
Table 9 presents the exploratory analyses examining the relationship between IOL decentration and tilt with additional visual and biometric parameters. For low-contrast CDVA (CDVA25), neither IOL decentration (r = –0.004, p = 0.96; 95% CI –0.14 to 0.13) nor tilt (r = –0.04, p = 0.53; 95% CI –0.18 to 0.09) showed significant correlation. Mesopic pupil size demonstrated weak, non-significant associations with both decentration (r = 0.09, p = 0.23) and tilt (r = 0.04, p = 0.56). Similarly, spherical aberration (HOA-S) was not meaningfully related to decentration (r = –0.01, p = 0.87) or tilt (r = –0.03, p = 0.66). For horizontal coma (HOA-CH), correlations were weak for both decentration (r = –0.02, p = 0.75) and tilt (r = –0.06, p = 0.38). Vertical coma (HOA-CV) showed slightly stronger but still non-significant trends, with decentration (r = –0.09, p = 0.21; 95% CI –0.23 to 0.05) and tilt (r = –0.13, p = 0.07; 95% CI –0.26 to 0.01).
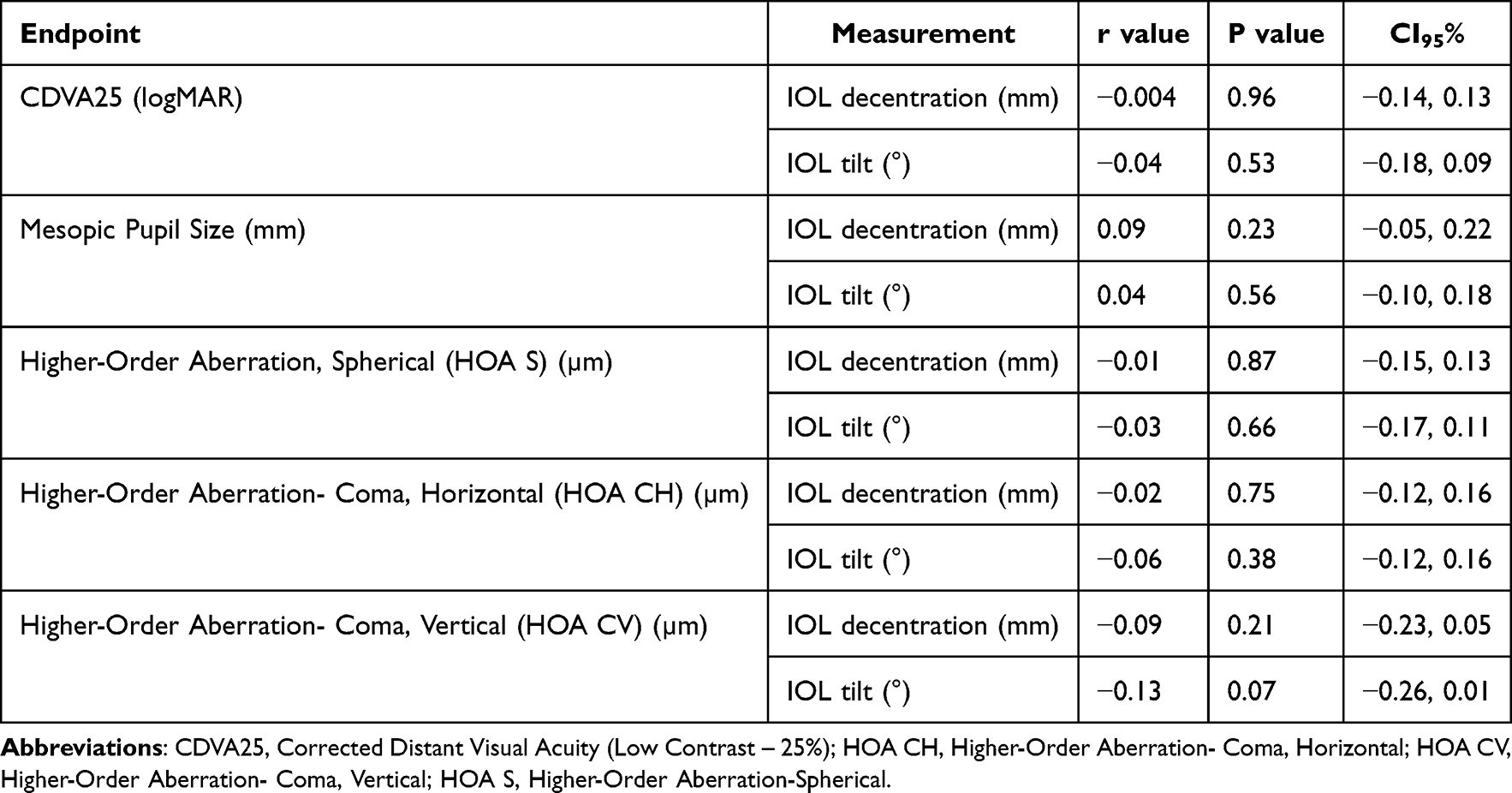 |
Table 9 Exploratory Endpoints- Relationship with Exploratory Measures with IOL Decentration and IOL Tilt |
Discussion
This non-interventional study evaluated the relationship between IOL positioning, specifically decentration and tilt, and a range of visual, refractive, and optical quality outcomes following the implantation of Clareon® Vivity® and Clareon® Vivity® Toric intraocular lenses. Across 202 eyes from 101 patients, IOL decentration (0.211 mm) and tilt (5.6°) were small and within the ranges commonly reported in prior IOL positioning studies. The primary unadjusted analyses demonstrated no statistically significant correlation between IOL decentration or tilt and postoperative visual acuity outcomes. However, in adjusted multivariable analyses, IOL decentration demonstrated a modest but statistically significant association with postoperative CDVA100, whereas IOL tilt and residual refractive cylinder (mRC) were not independently associated with visual outcomes.
These findings support that while the Clareon® Vivity® platform demonstrates optical resilience to modest IOL misalignment, slight effects of decentration on postoperative CDVA may be identified under adjusted modeling conditions.
For the primary endpoint, CDVA at 4 m under high contrast (CDVA100), neither decentration nor tilt correlated meaningfully with the visual outcomes. Although a weak correlation was observed between decentration and CDVA, it did not reach statistical significance and is unlikely to represent a clinically meaningful effect. Similar findings were observed for the secondary measures. Neither DCIVA nor UCIVA at 66 cm under high contrast (DCIVA100 and UCIVA100) correlated with IOL position. A borderline association was observed between UCDVA under high-contrast conditions (UCDVA100) and decentration; however, the magnitude of the observed relationship was small and of uncertain clinical significance. The MRSE remained stable and was not significantly associated with IOL alignment parameters, which is consistent with its excellent refractive predictability.
Exploratory analyses confirmed the lack of meaningful associations. Low-contrast CDVA (CDVA25), mesopic pupil size, and corneal HOA measures, including coma (horizontal and vertical) and spherical aberrations, showed no significant associations with IOL positioning. However, these HOA measurements represented corneal aberrations obtained from iTrace rather than total ocular aberrations directly induced by IOL positioning. Therefore, these exploratory analyses should be carefully interpreted since corneal HOAs may act as confounding factors influencing postoperative visual outcomes independently of IOL tilt or decentration. Furthermore, the lack of significant associations resulting from this study does not confirm that IOL decentration or tilt does not affect total ocular aberrations or visual outcomes.
Additional analyses demonstrated that the relationship between decentration and postoperative CDVA100 persisted even after controlling for residual refractive cylinder and accounting for inter-eye correlation. Furthermore, the lack of a statistically significant interaction between mRC and IOL decentration or tilt demonstrates that residual refractive cylinder did not confound or change these relationships.
The nondiffractive wavefront-shaping technology of the Clareon® Vivity® platform may provide greater tolerance to modest tilt and decentration compared with traditional diffractive multifocal or negative spherical aberration-correcting IOLs, which are known to be more sensitive to coma-related aberrations and visual outcomes from IOL misalignment. These results align with emerging evidence that nondiffractive EDOF designs, such as Clareon® Vivity®, are less sensitive to positional variability than traditional diffractive multifocal lenses, providing more stable postoperative vision across a range of distances. Walters (2022) and others have also reported excellent stability of the Clareon® material and design, likely contributing to these findings.10
Importantly, IOL tilt and decentration may partially reflect baseline capsular or crystalline lens anatomy rather than just the IOL decentration or tilt. However, preoperative crystalline lens orientation and angle kappa were not measured so this study cannot determine if, or how much, potential neural adaptation to baseline ocular alignment may have affected the findings.
Previous studies of both spherical and aspheric foldable IOLs have shown that typical decentration and tilt levels are generally insufficient to significantly reduce visual acuity.5 In addition, measurement variability may be proportionally greater at very small magnitudes of IOL decentration, which should be considered when interpreting subtle positional differences within the relatively narrow range of decentration observed in this study. Negative spherical aberration-correcting aspheric IOLs are known to be sensitive to positional misalignment because decentered light rays may induce additional astigmatism and higher-order aberrations, particularly coma. In contrast, the nondiffractive wavefront shaping design of Clareon® Vivity® may inherently reduce susceptibility to these issues, potentially contributing to the relative tolerance to modest positional variability observed in this study, and offering an additional margin of safety in routine clinical practice. However, data with aspheric IOLs possessing varying spherical aberration profiles demonstrated that tilt and decentration can influence visual outcomes, as IOL misalignment is correlated with increased wavefront aberrations such as RMS astigmatism and coma.6
The key strengths of this study include its relatively large sample size, use of objective imaging modalities (CASIA2 for decentration/tilt and iTrace for HOAs), and the comprehensive assessment of both visual acuity and optical quality endpoints. Limitations include the observational design, short follow-up period, and narrow focus on a single IOL type, which may limit the generalizability to other IOL types.
From a clinical perspective, these findings may be relevant in routine cataract surgery setting where small degrees of positional variability can occur despite careful preoperative planning and intraoperative alignment. The ability of the Clareon® Vivity® IOLs platform to maintain generally favorable visual outcomes despite modest positional variability may be particularly valuable in presbyopia-correcting and toric lens designs, in which alignment has historically been an important determinant of visual performance.
Conclusion
In this retrospective observational study, Clareon® Vivity® and Vivity® Toric IOLs demonstrated favorable postoperative distance and intermediate visual outcomes across the study population. Although adjusted analyses identified a modest association between IOL decentration and postoperative CDVA100, residual refractive cylinder and IOL tilt did not appear to explain or modify this relationship and visual outcomes. These results suggest that the nondiffractive wavefront-shaping design of the Clareon® Vivity® platform maintains generally favorable visual outcomes despite modest positional variability, which may contribute to improved patient satisfaction.
Abbreviations
IOL, Intraocular Lens, CDVA, Corrected Distance Visual Acuity, UCDVA, Uncorrected Distance Visual Acuity, DCIVA, Distance-Corrected Intermediate Visual Acuity, UIVA, Uncorrected Intermediate Visual Acuity, MRSE, Manifest Refraction Spherical Equivalent, US, United States, FDA, Food and Drug Administration, EDOF, Extended Depth of Focus, HEMA, Hydroxyethylmethacrylate, HOA, Higher-Order Aberration, HOA CV, HOA Coma Vertical, HOA S, HOA Spherical, IRB, Institutional Review Board, HIPAA, Health Insurance Portability and Accountability Act, NIH, National Institute of Health, VA, Visual Acuity, ETDRS, Early Treatment Diabetic Retinopathy Study, YAG, Yttrium Aluminum Garnet, LASIK, Laser-Assisted In Situ Keratomileusis, PRK, Photorefractive Keratectomy, AMD, Age-Related Macular Degeneration, MIGS, Microinvasive Glaucoma Surgery, SD, Standard Deviation.
Data Sharing Statement
All data are available upon reasonable request to the corresponding author.
Acknowledgment
Stephen Smith aided with developing the statistical analysis plan and conducting the data analysis.
Funding
This study was financially supported by Alcon.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nartey A. The pathophysiology of cataract and major interventions to retarding its progression. MedCraveOnline; 2017. Available from: https://medcraveonline.com/AOVS/the-pathophysiology-of-cataract-and-major-interventions-to-retarding-its-progression-a-mini-review.html.
2. Gurnani B, Kaur K. Phacoemulsification. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2026.
3. Apple D, Sims J. Harold Ridley and the invention of the intraocular lens. Surv Ophthalmol. 1996;40:279–11.
4. Ashena Z, Maqsood S, Ahmed SN, Nanavaty MA. Effect of intraocular lens tilt and decentration on visual acuity, dysphotopsia and wavefront aberrations. Vision. 2020;4(3):41. PMID: 32937750; PMCID: PMC7559075. doi:10.3390/vision4030041
5. Shamie N, Micheletti JM, Shafer B, Werner L. Clareon IOL: next Generation. Cataract & Refractive Surgery Today (CRST). n.d. Available from: https://crstoday.com/articles/clareon-iol-the-next-generation/clareon-iol-the-next-generation-3?
6. McCabe C, Berdahl J, Reiser H, et al. Clinical outcomes in a U.S. registration study of a new EDOF intraocular lens with a nondiffractive design. J Cataract Refract Surg. 2022;48(11):1297–1304. PMID: 35616507; PMCID: PMC9622364. doi:10.1097/j.jcrs.0000000000000978
7. Lehmann R, Maxwell A, Lubeck DM, Fong R, Walters TR, Fakadej A. Effectiveness and safety of the clareon monofocal intraocular lens: outcomes from a 12-month single-arm clinical study in a large sample. Clin Ophthalmol. 2021;Volume 15:1647–1657. doi:10.2147/OPTH.S295008
8. Baumeister M, Bühren J, Kohnen T. Tilt and decentration of spherical and aspheric intraocular lenses: effect on higher-order aberrations. J Cataract Refract Surg. 2009;35(6):1006–1012. PMID: 19465285. doi:10.1016/j.jcrs.2009.01.023
9. Pérez-Gracia J, Varea A, Ares J, Vallés JA, Remón L. Evaluation of the optical performance for aspheric intraocular lenses in relation with tilt and decenter errors. PLoS One. 2020;15(5):e0232546. doi:10.1371/journal.pone.0232546.
10. Walters TR, Lehmann R, Moyes A, French JW, Sreenivasan V, Modi SS. Rotational stability of the clareon monofocal aspheric hydrophobic acrylic intraocular lens 6 months after implantation. Clin Ophthalmol. 2022;16:401–409. doi:10.2147/OPTH.S348551
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.