Back to Journals » Clinical Interventions in Aging » Volume 21
Non-Contiguous OVCF Patients Had a Higher Risk of AVF After PVP Operation Related to Poor Bone Mineral Density Rather Than Aggravated Stress Concentration
Authors Tang X, Huang K, Jia L, Li H, Wang Y, Xie L, Li J ![]()
Received 26 February 2026
Accepted for publication 27 April 2026
Published 14 May 2026 Volume 2026:21 600293
DOI https://doi.org/10.2147/CIA.S600293
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Xuebin Tang,1,2,* Kai Huang,1,* Lijunpeng Jia,3 Hua Li,1 Yunqing Wang,1 Lin Xie,2 Jingchi Li3
1Department of Orthopedics, The Second Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, 221000, People’s Republic of China; 2Department of Orthopedics, Affiliated Hospital of Integrated Traditional Chinese and Western Medicine, Third Clinical Medical College, Nanjing University of Chinese Medicine, Nanjing, Jiangsu, 210028, People’s Republic of China; 3Department of Orthopedics, Luzhou Key Laboratory of Orthopedic Disorders, The Affiliated Traditional Chinese Medicine Hospital, Southwest Medical University, Luzhou, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lin Xie, Email [email protected] Jingchi Li, Email [email protected]
Background: Biomechanical deterioration and low bone mineral density (BMD) are two primary triggers for adjacent vertebral fracture (AVF) after percutaneous vertebroplasty (PVP) operation. Sandwich vertebral body (SVB) refers to a vertebral body situated between two osteoporotic vertebral compressive fractures (OVCF) segments. There exists a contradiction regarding whether the SVB are at a heightened risk of AVF, and the underlying mechanism has yet to be elucidated.
Methods: Clinical data of PVP treated OVCF patients were included in this study. Patients were divided into two groups: those with single-level OVCF and those with SVB resulting from non-contiguous two-level OVCF. Statistical comparisons and logistic regression analyses were performed to investigate whether patients with two-level non-contiguous OVCFs constitute a risk factor for AVF. Furthermore, PVP procedures involving single-level and non-contiguous two-level OVCFs were simulated in models with identical bony density. Biomechanical indicators associated with AVF were computed under physiological loading conditions.
Results: This study enrolled 173 patients with PVP-treated OVCF, including 134 with single-segment fractures and 39 with non-contiguous two-level fractures. Among these patients, the overall incidence of AVF was 22.39% (30/134) in the single-segment group and 38.46% (15/39) in the non-contiguous two-level group. The incidence of AVF was significantly higher in patients with non-contiguous two-level OVCF (P = 0.044). Correspondingly, HU values were significantly lower in those with two-level OVCF. However, only a lower HU value was judged to be an independent risk factor for AVF. Furthermore, the maximum difference between the two models with identical BMD was found to be less than 5%. The only exception observed was the cortical stress value in the L3 vertebral body under extension loading conditions. In this case, the stress value of the SVB increased by 10.41% compared to the control group (i.e. single-level OVCF at L2), and the difference in stress between groups was not influenced by the presence or absence of compressive load.
Conclusion: Patients with two-level non-contiguous OVCF experiences a higher incidence of AVF primarily due to poor BMD, rather than the exacerbation of stress concentration caused by two adjacent segmental cement augmentations.
Keywords: adjacent vertebral fracture, percutaneous vertebroplasty, sandwich vertebral, osteoporosis progression, biomechanical environment
Introduction
Osteoporosis is a prevalent metabolic disorder in elderly patients. Its main characteristic is a reduction in bone strength.1 Consequently, osteoporosis serves as the pathological basis for fragility fractures that occur under low-energy trauma.2 The osteoporotic vertebral compression fracture (OVCF) is a typical example of such low-energy fractures, and cement augmentation has proven to be an effective surgical technique in the treatment of OVCF.3 Percutaneous vertebroplasty (PVP) has been widely adopted in OVCF treatment, and there has been a stepwise increase in the incidence of postoperative complications.4 Among these, adjacent vertebral fractures (AVF) are frequently observed complications that lead to recurrence of clinical symptoms in patients.5 The sandwich vertebral body (SVB) is defined as a vertebral body that is adjacent to both cranial and caudal OVCF segments.6 There exists a contradiction in the literature regarding whether SVBs experience a higher incidence of AVF. Some studies have reported an increased incidence of AVF in SVB compared to normal adjacent vertebral bodies,6,7 while others have indicated comparable rates of AVF.8,9 Furthermore, studies that documented a higher incidence of AVF did not elucidate the underlying mechanisms contributing to this phenomenon.
The progression of osteoporosis and postoperative stress concentration on adjacent vertebral bodies are two primary factors contributing to an increased incidence of AVF.10,11 Specifically, the advancement of osteoporosis can further diminish patients’ bone strength,12 making them more susceptible to fractures.1 From a different perspective, the fundamental mechanism of fracture can be understood as the stress on bony structures exceeding their yield strength.10 Consequently, localized stress concentration on vertebral bodies adjacent to the PVP segment may also elevate the risk of AVF.13 Therefore, the potential mechanisms underlying any risk factors associated with AVF can be elucidated from these two perspectives. Theoretically, patients with multi-segmental OVCFs may exhibit more severe osteoporosis, which could explain the heightened risk associated with SVBs. Additionally, it has been observed that the stiffness of bone cement significantly exceeds that of osteoporotic cancellous bone. This increased stiffness in augmented vertebral bodies may result in stress concentration within adjacent segments. Augmentation on both cranial and caudal sides may exacerbate this tendency and induce greater stress concentration on the SVB. However, whether these two factors lead to a high incidence of AVF in SVB patients and which factor plays a dominant role have yet to be identified. A clinical evidence-based biomechanical study was conducted to address this issue, to enhance awareness of the mechanism of AVF in SVB patients.
Materials and Methods
Clinical Review
Patient Data Collection, Inclusion and Exclusion Criteria
Patient data collection was conducted with approval from the ethics committees of the Second Affliated Hospital of Xuzhou Medical University. In accordance with similar studies, informed consent was waived as patient data were retrospectively collected without any additional intervention. Patients who underwent bilateral transpedicular PVP operation for OVCF between April 2020 and December 2022 were included in this study, with an average clinical follow-up period of approximately two years. Demographic data, including age, sex, body mass index, and smoking history, were recorded based on medical records. According to the number of OVCF, patients were categorized into two groups: those with single-level OVCF and those with two-level non-contiguous OVCF.
Patient inclusion and exclusion criteria are outlined as follows, based on published studies and similar research: PVP-treated patients were required to have experienced severe back pain due to an acute OVCF (less than 2 weeks in duration). The diagnostic criteria for acute OVCF are as follows: patients experience severe pain in the thoracic or lumbar back after acute trauma (such as a fall), and MRI examination indicates high signal intensity on T2-weighted imaging of a specific vertebra along with morphological changes. Eligible participants must have undergone comprehensive imaging examinations at our hospital’s imaging department and completed clinical follow-up for approximately two years. Exclusion criteria included injuries to the middle column (such as burst fractures rather than compressive fractures); the need for nerve decompression due to bony compression; pathological vertebral fractures resulting from tumors or any type of infection (including tuberculosis or non-specific bacterial infections); loss of follow-up or death during the follow-up period; remote segmental fractures involving more than one SVBs (eg., patients with simultaneous L3 and T10 OVCFs); and two-level contiguous OVCF (Figure 1).
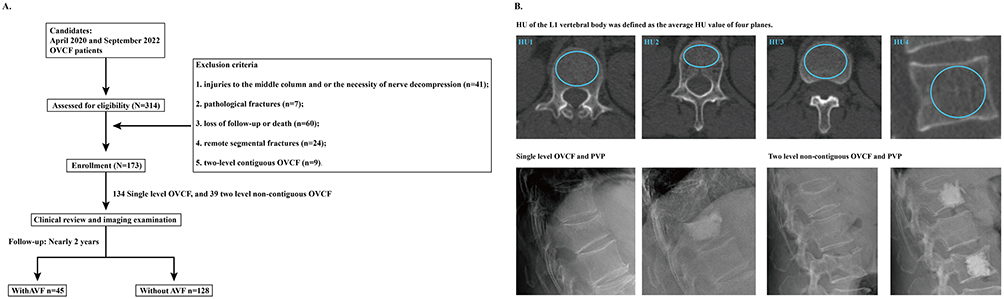 |
Figure 1 (A) Schematic for patients inclusion and exclusion criteria; (B) Schematic for the measurement of HU values and two different fracture types (i.e., single-level OVCF and two level non-contiguous OVCF). The blue circles in the figure denote the ROI for HU measurement. |
Radiographic Data Measurement
The measurement of imaging-based parameters was conducted by a senior spine surgeon on our research team. Patients were diagnosed with AVF and enrolled in this group if they presented with recurrent low back pain after a low-energy injury, accompanied by typical imaging findings (such as high intensity on T2-weighted MRI and vertebral collapse) in adjacent vertebral bodies. Since the overall incidence of AVF was being compared across fracture types, patients with AVF on either the cranial or caudal side were enrolled in a single AVF group. All other patients were assigned to the non-AVF control group. The Hounsfield unit (HU) value, rather than the T-score from DXA, was measured using thoracic CT scans to assess the BMD in the current patient series.14 The tube voltage was set at 120 kV during this process, consistent with published studies.15 When measuring HU values for patients, the region of interest (ROI) was expanded to encompass the largest area within the cancellous bone. Meanwhile, cortical bone, bony endplates (BEP), any type of osteophytes, and venous plexuses were excluded from the ROI.16 In accordance with similar studies, HU values were obtained from four different planes: including those adjacent to superior and inferior to BEPs, as well as central transverse and sagittal planes. The average HU value across these four planes was designated as representative for each patient.17 Furthermore, for patients presenting with L1 OVCF, the HU value of the T12 vertebral body was measured to represent their BMD accurately (Figure 1).11
Statistical Analyses
Statistical analyses were performed using IBM SPSS version 26.0 software. Continuous variables are presented as the mean ± standard deviation, while categorical variables are expressed as percentages. To evaluate interobserver and intraobserver repeatability in measuring HU values, a random selection of 20 patients was made.18 One week after the initial assessment of imaging data, both a spine surgeon and an experienced radiologist re-evaluated the imaging data for these selected patients. The (ICC) was calculated to assess the repeatability of HU values.19 To assess the rationality of the existing sample size, we conducted a comprehensive evaluation through effect size analysis, post hoc power analysis, and Bootstrap resampling analysis.20 Cohen’s h was used to evaluate the effect size of the inter-group differences in the 2×2 contingency table, and statistical power was calculated to determine the ability of the current sample size to detect the effect.21 Based on the binomial logistic regression model, 1000 and 5000 Bootstrap resampling procedures were performed.22
Significant differences were compared between patient series with and without AVF, and between those with different fracture types (ie., single-level and two-level non-contiguous fractures).23 Moreover, logistic regression analysis was employed to identify independent risk factors associated with AVF. Univariate analyses were performed for each demographic and imaging parameter, and only those with a significance level of p < 0.1 were included in subsequent multivariate analyses (a more liberal entry criterion is recommended in univariate regression analysis to avoid omitting potentially important predictors, and this threshold is widely adopted in similar studies).12,24 Variables yielding P < 0.05 in multivariate analysis were considered independent risk factors for AVF. Finally, receiver operating characteristic (ROC) curve analyses were executed to evaluate the predictive value of HU measured by different methods, with the area under the curve (AUC) computed as an indicator for assessing the predictive performance of parameters.25
Biomechanical Research
Construction of the Intact Model
We have constructed, calibrated, and validated a lumbar numerical model (encompassing the L1-L4 motion segments) to identify differences in the biomechanical environment between single-level and two-level non-contiguous OVCF treated with PVP operation.14 Although OVCF most frequently occur at the thoracolumbar junction, the scarcity of biomechanical experimental data for this specific region makes it difficult to properly calibrate and validate a computational model. In contrast, the lumbar spine benefits from more established experimental data and methodologies. This available data enables rigorous multi-directional model calibration and validation against multiple indicators, which is a critical prerequisite for ensuring the reliability of the computational results.26 In constructing the bony structures, cortical bone, cancellous bone, and BEPs for different segments were developed separately. The cortical thickness was established at 0.8 mm. BEP models with varying thicknesses, concave depths, and concave angles of segmental BEPs were created based on published anatomical and imaging studies.27 When constructing intervertebral disc (IVD) models, the annulus, nucleus, and cartilage endplates (CEPs) were each developed separately. Based on published studies, the average radius of the IVD was established at 95.5% of the vertebral body size, with a ratio of 1.62 between the anterior and posterior annulus dimensions set in the central sagittal plane to define the relative position of the nucleus.28,29 The outline of the nucleus was made identical to that of the annulus, and CEPs cover the nucleus and the inner half of annulus. Additionally, both sides’ articular processes maintained consistent outlines and facet orientations.30
Material Property Definition and Muti-Indicators Model Validation
In the characterization of material properties, bony structures were defined as having osteoporotic material properties,31 with cortical and cancellous bone classified as anisotropic materials, while other components were designated as isotropic materials.11 The annulus was modeled as a hypoelastic material, with stiffness parameters defined separately for various layers and regions.29 The nucleus was treated as a semi-fluid incompressible material.26 Ligaments and capsules were represented by cable elements that exhibited distinct load-deformation curves.32 To ensure computational credibility, the computed disc compression (DC), and range of motions (ROM) under different directional loading conditions with varying sizes of load and moment were analyzed.33 Given that the differences between computed values and average tested values were less than one standard deviation, the calibrated model effectively represents the local biomechanical environment and is suitable for surgical simulation across diverse operative scenarios (Figure 2).
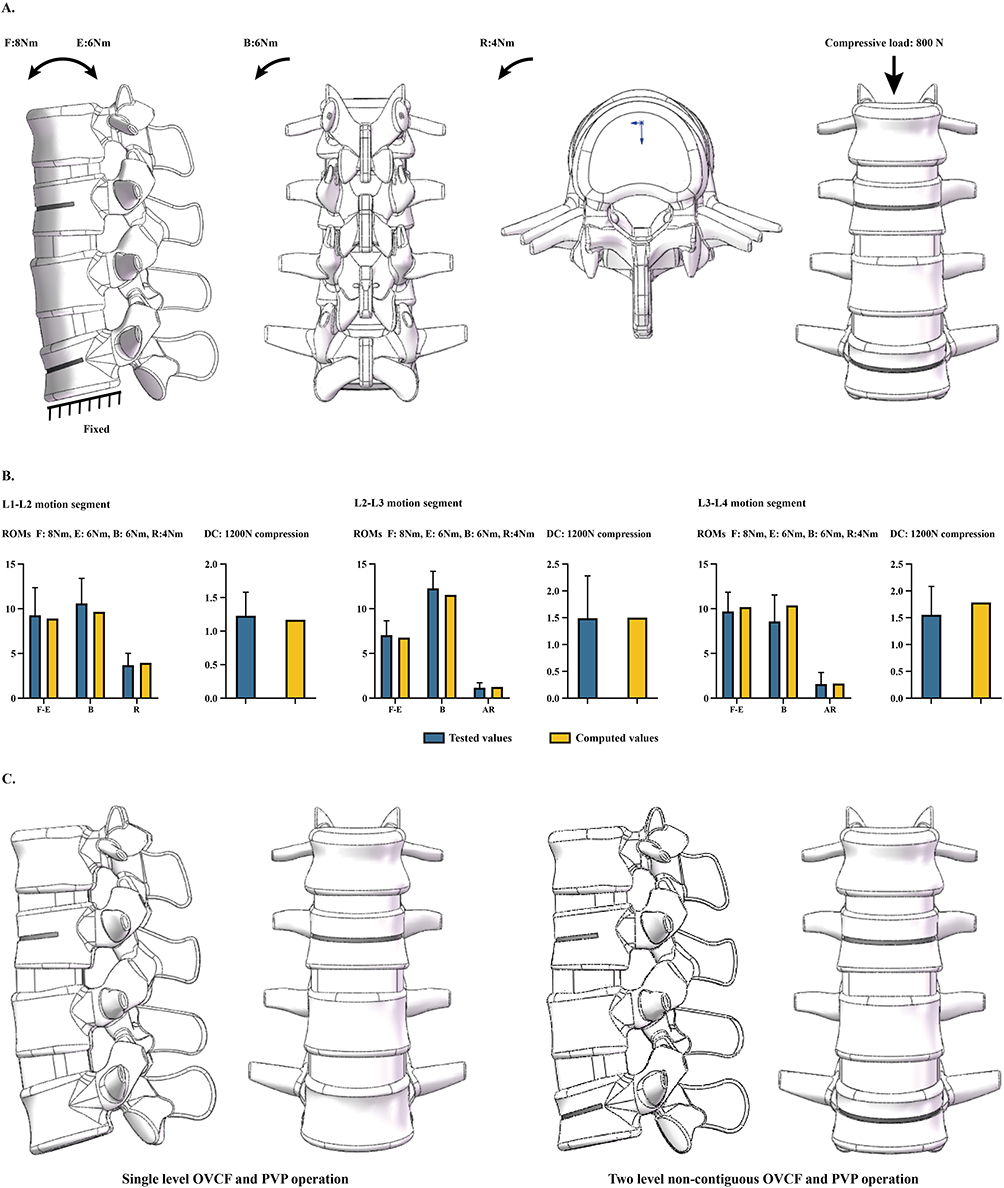 |
Figure 2 (A) Schematic for different directional moments and vertical compressive load during the stress value computational process; The black arrow indicates the loading direction. The blue asterisk (*) denotes the origin of the three-dimensional coordinate system. The blue arrow schematically depict the spatial orientation of the model. (B) Multi-indicators model validation of the calibrated intact model; (C) Schematic for single level and two level non-contiguous PVP operation simulations. |
PVP Simulation in Models with Single and and Two-Level Non-Contiguous OVCF
The simulation of OVCF was conducted on the L2 and L4 vertebral bodies. The surgical simulation methods employed were entirely consistent across these two segments. In the model representing a single-level OVCF, only the L2 OVCF and PVP operation were simulated. Additionally, models for PVP in both the L2 and L4 segments were constructed to simulate two non-contiguous levels of OVCF and corresponding PVP operations. To replicate the fracture and vertebral collapse associated with OVCF pathology, we reduced the anterior vertebral height by 10%. A cleft measuring 20 mm in depth and 2 mm in height was created within the vertebral body, oriented vertically relative to its axis.34 During the simulation of OVCF, PMMA bone cement was utilized to completely fill the anterior two-thirds of the PVP augmented vertebral body; concurrently, we replaced the material properties of cancellous bone in that region with PMMA. BMD remained identical across both postoperative models (Figure 2).35
Boundary and Loading Conditions
When it comes to mesh generation, different sizes of tetrahedral and hexahedral elements were selected for various components of the models. To eliminate the confounding effects caused by mesh size on computational results, the intact model underwent a mesh convergence test in published studies.36 During this process, intradiscal pressure (IDP) values with varying mesh sizes were recalculated through a stepwise reduction in mesh size until changes in computed IDP values were less than 3%. By employing this mesh generation strategy, the average mesh size was maintained at over 0.8, effectively ensuring the credibility of the computed values.37 Six freedom degrees were fixed under inferior surfaces of L4. Different directional moments and 800N vertical compressive load were applied on superior surfaces of L1.11 As above mentioned, bilateral facet orientation were keep identical. Correspondingly, current numerical models were symmetrical along the central sagittal plane.29 And only unilateral bending and rotation loading conditions were applied to optimize the computational efficiency (Figure 2).
Results
Clinical Review
Patient Data Collection and Imaging Measurement Repeatability
This study enrolled a total of 173 patients, comprising 139 females and 34 males, with a clinical follow-up period of approximately two years. The series included 134 patients with single-segment OVCF and 39 patients with non-contiguous two-level OVCF, resulting in a total of 212 fracture levels. Consistent with previous studies of a similar nature, the thoracolumbar junction was the most prevalent site for OVCFs. The inter- and intra-observer ICC values for measuring the HU values of the patients were found to be 0.897 and 0.901, respectively, indicating excellent repeatability based on these ICC values. Moreover, based on the effect size analysis and post hoc power analysis, the incidence rates of the two groups were 77.61% and 61.54%, respectively, with a corresponding effect size (Cohen’s h) of 0.3522, indicating a moderate difference between the groups. Two Bootstrap resampling analyses were conducted with 1000 and 5000 repeated samplings, respectively, yielding ORs of approximately 2.15 and 2.18, with the effect direction being largely consistent. These results suggest that under the current sample size conditions, the effect value has a certain magnitude and directional stability.
Significant Difference Computation and Independent Risk Factors Judgement
The overall incidence of AVF in the cohort was 26.01% (45/173). When analyzed by fracture type, the incidence was 22.39% (30/134) in patients with single-segment OVCF and 38.46% (15/39) in those with non-contiguous two-level OVCF, a difference that was statistically significant (P = 0.044) (Table 1). Of the patients with single-segment OVCF, AVF occurred in 21 cranial and 9 caudal vertebral bodies. Among patients with non-contiguous two-level OVCF, AVF involved the SVB in 8 patients and the cranial vertebral body in 6 patients, with only one patient exhibiting AVF in both locations concurrently. Furthermore, patients with non-contiguous two-level OVCF exhibited significantly lower HU values compared to those with single-level OVCF (Table 2). Furthermore, in the comparison between the two fracture types, patients with non-contiguous two-level fractures were significantly older and had lower HU values than those with single-level fractures (Table 3).
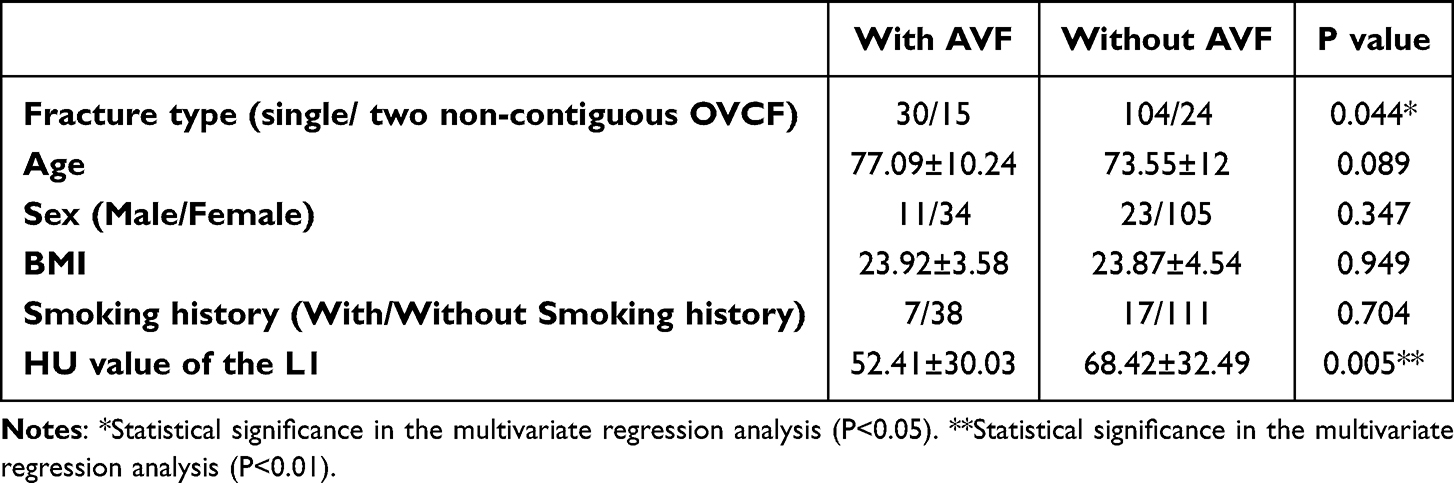 |
Table 1 Significant Differences for Covariates Between Patients with and without AVF |
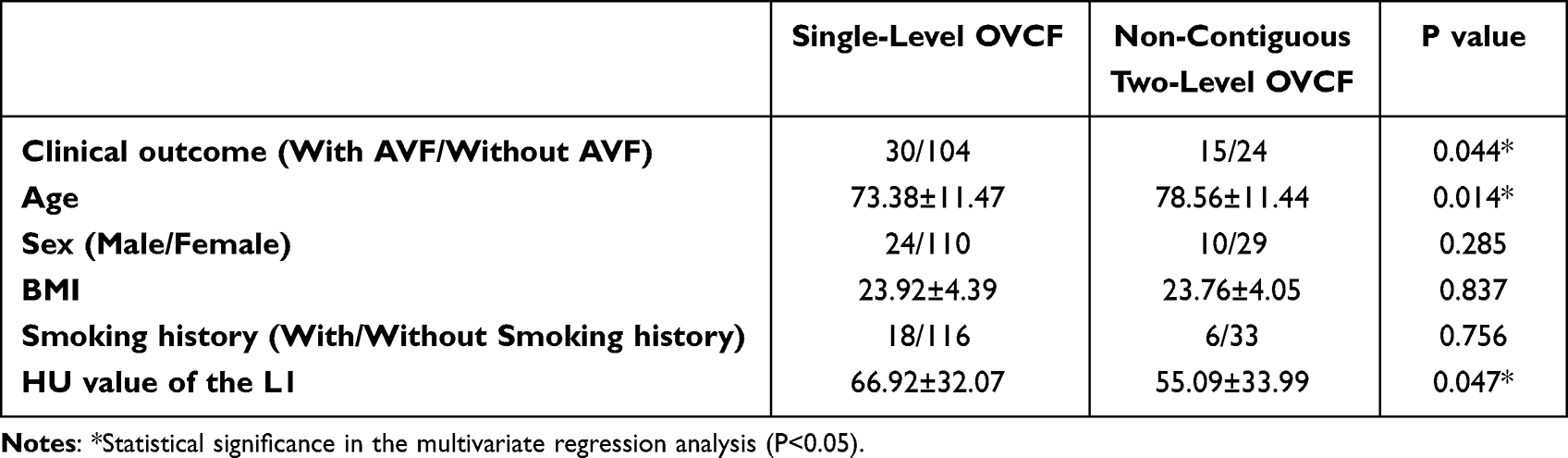 |
Table 2 Significant Differences for Covariates Between Patients with Two Different Fracture Types |
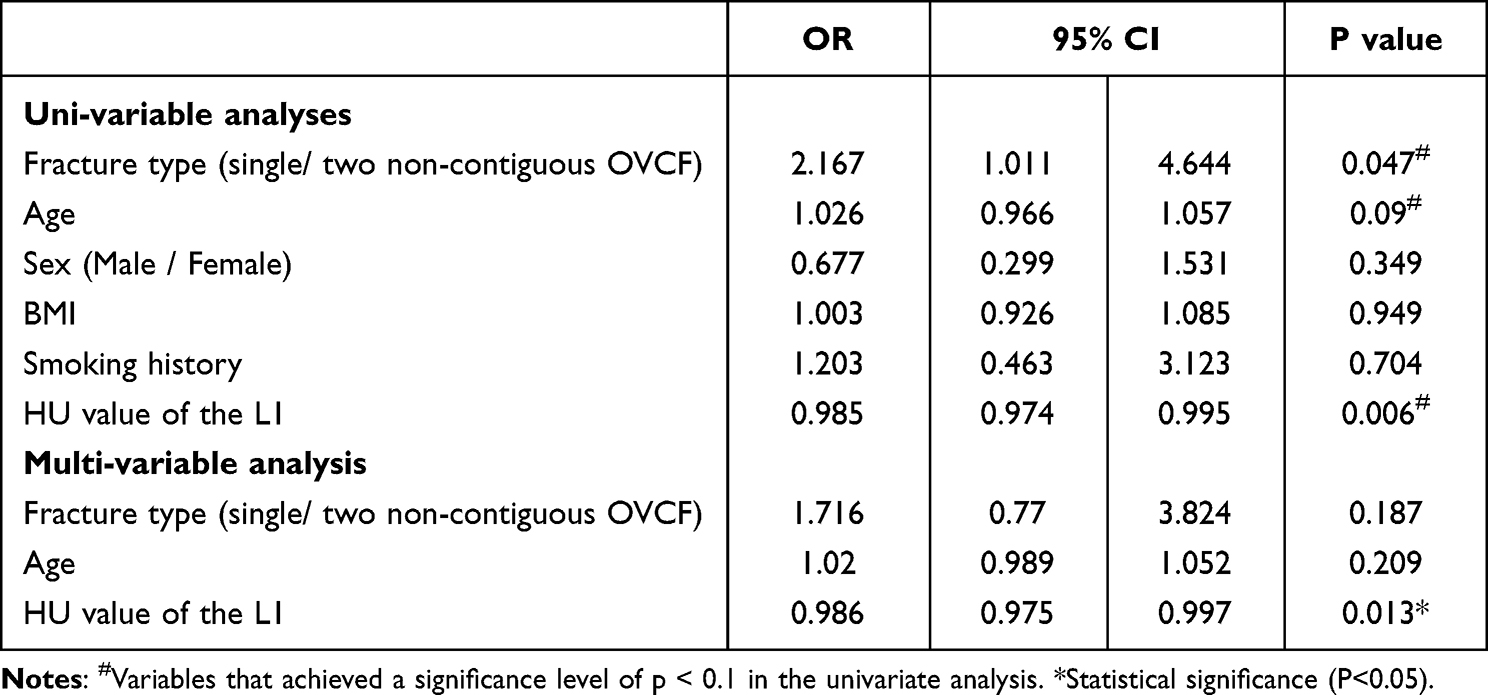 |
Table 3 Logistic Regression Analysis of AVF |
In identifying independent risk factors for AVF, univariate analyses revealed that the P-values for non-contiguous two-level fractures, older age, and reduced HU values were less than 0.1; however, only the P-value associated with lower HU values fell below 0.05 in multivariate analysis, and thus it can be judged as an independent risk factor for AVF (OR: 0.986; 95% CI: 0.975, 0.997). Consequently, non-contiguous two-level OVCF does not qualify as an independent risk factor for AVF (OR: 1.716; 95% CI: 0.77, 3.824) (Table 4). Finally, based on ROC curve analysis, AUC values for non-contiguous two-level OVCF were determined to be 0.573 and 0.652 respectively (Table 4 and Figure 3).
 |
Table 4 The AUC and Corresponding P value for AVF Prediction |
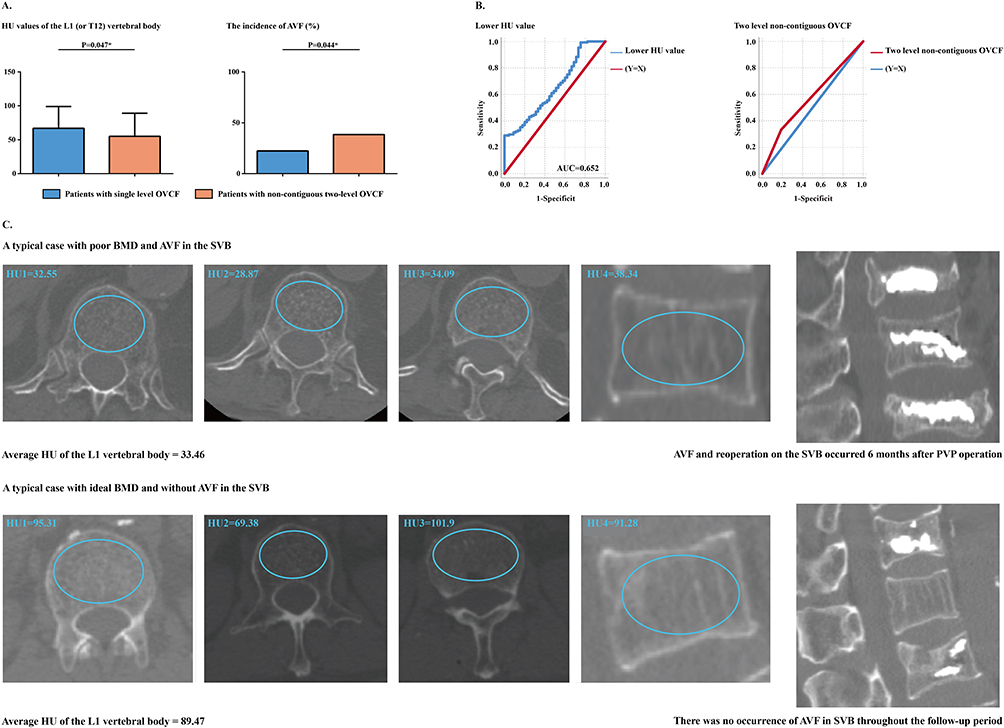 |
Figure 3 (A) Significant difference computation in patients with and without AVF; (B) ROC curves for AVF prediction of lower HU values and two level non-contiguous OVCF and PVP operation; (C) Typical cases for patients with AVF: Changes in BMD can affect the incidence of AVF of SVB. The blue circles in the figure denote the ROI for HU measurement. |
Numerical Mechanical Simulations
Multi-Indicators Validation
The computed ROM, and DC across different motion segments were analyzed under varying sizes and directional moments. The discrepancies between the computed values and the average tested values were found to be less than one standard deviation from the mechanical tests. Consequently, we assert that the currently selected intact model accurately represents the local biomechanical environment, encompassing local stress and motility characteristics. This model can effectively assess the biomechanical effects associated with two distinct fracture types: single-level OVCF and non-contiguous two-level OVCF, along with their corresponding PVP operations (Figure 2).
Biomechanical Differences in Models with Single and Non-Contiguous Two Level PVP Operation
Maximum stress values for both cortical (including BEPs) and cancellous bone were calculated separately in models subjected to flexion, extension, bending, and rotation loading conditions with and without an 800N vertical compressive load. No significant differences in stress values were observed between the two models across all loading conditions. The maximum difference between the two models was found to be less than 5% in these two models with identical bony density. The only exception observed was the cortical stress value in the L3 vertebral body under extension loading conditions. In this case, the stress value of the SVB increased by 10.41% compared to the control group (ie., single-level OVCF at L2). Moreover, bone structures exhibited higher stress under vertical compressive load conditions; however, the difference in stress between groups was not influenced by the presence or absence of compressive load (Figure 4).
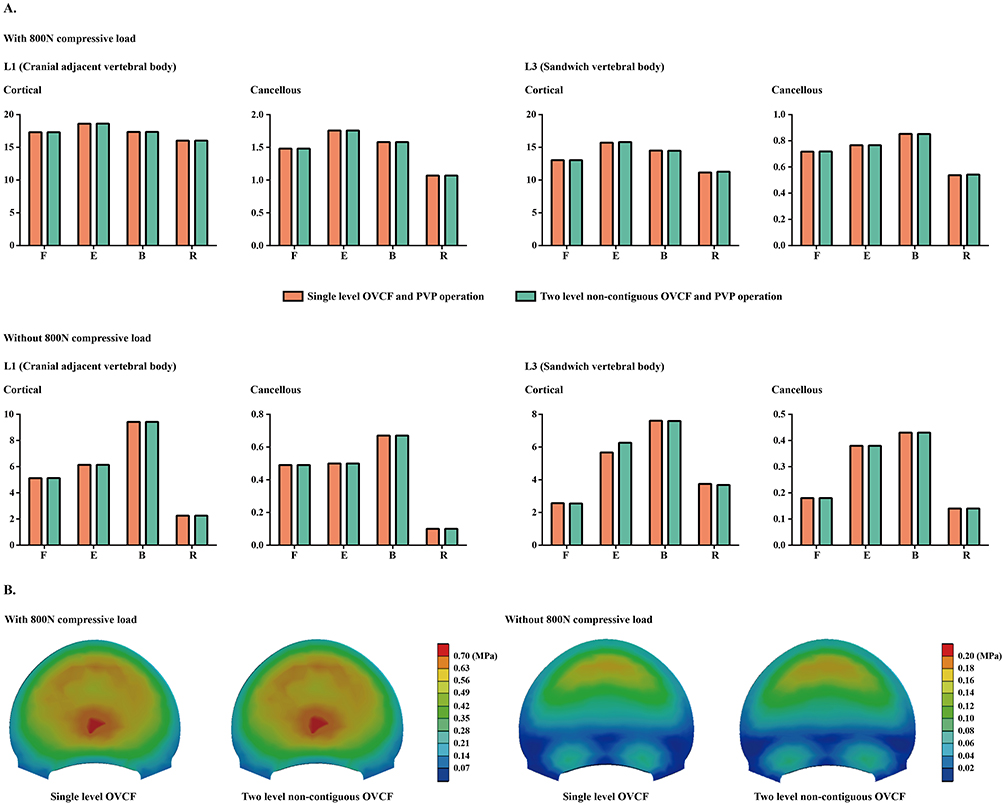 |
Figure 4 (A) Computational result on BEP and cancellous bone in models with single or two non-contiguous OVCF and PVP operations under different directional moments with and without 800N compressive load; (B) Nephograms for stress distribution on cancellous bone of SVB under the flexion loading condition with and without 800N compressive load. |
Discussion
As a distinct type of vertebral segment situated adjacent to both cranial and caudal PVP-augmented segments, there remains an ongoing debate regarding whether the incidence of AVF is elevated in SVB compared to normal adjacent vertebral bodies.9 Furthermore, the underlying mechanisms associated with this contradiction have yet to be elucidated. To address these topics, this study conducts a clinical evidence‑based biomechanical investigation. The mutual corroboration between clinical and biomechanical research can enhance the credibility of research conclusions, particularly when exploring mechanisms related to topics with contradictory conclusions in previously published literature.38 The clinical review indicates that although patients with two non‑contiguous vertebral fractures exhibit a significantly higher incidence of AVF, lower HU values, rather than the fracture type itself, emerge as an independent risk factor for AVF progression. The computational results could corroborate the clinically observed phenomenon: when comparing models with identical osteoporotic BMD, those featuring only L2 segmental cement augmentation exhibited stress values that were generally comparable to those in models incorporating both L2 and L4 segmental cement augmentations. Consequently, patients with two-level non‑contiguous OVCF experience a higher incidence of AVF primarily related to poor bone mineral density (BMD), rather than the exacerbation of stress concentration caused by two adjacent segmental cement augmentations.
The discrepancy between our expectations and the computed results warrants detailed discussion. Specifically, it is widely accepted that an increase in segmental stiffness resulting from various interventions (such as pedicle screw fixation, interbody fusion, or cement augmentation) within a specific motion segment can lead to compensatory stress concentration and increased range of motion in adjacent segments.39 These alterations may precipitate several biomechanical complications related to deterioration (for instance, adjacent segment disease (ASD) following lumbar interbody fusion with pedicle screw fixation).40 Consequently, strategies aimed at reducing the stiffness of the surgical segment, through methods such as selecting low‑stiffness internal fixation devices and using appropriate bone cements, have been demonstrated to effectively mitigate compensatory stress concentration in adjacent segments.41 Therefore, considering that the stiffness of PMMA cement significantly exceeds that of cancellous bone,42 we infer that additional segmental cement augmentation could elevate local stiffness levels and exacerbate compensatory stress concentration in adjacent segments.
However, contrary to our expectations, according to our computed mechanical results, comparable stress values were observed in the L2 vertebral body in models with single-level and non-contiguous two-level OVCF. Consequently, the compensatory stress concentration in the vertebral body adjacent to the PVP segments was minimal under most directional physiological loading conditions. We hypothesize that this compensatory stress concentration is effectively counteracted by the IVD’s ability to achieve uniform distribution of local load during load transmission. This perspective is supported by the fact that one of the most crucial biomechanical functions of the IVD is its ability to distribute stress uniformly;43 thus, the effectiveness of compensatory stress concentration resulting from additional segmental cement augmentation may be mitigated by the normal biomechanical function of the IVD. Another study supports this perspective, indicating that direct contact between leaked cement and adjacent vertebral bodies can lead to a higher incidence of AVF by compromising the local biomechanical environment.10
From the methodological perspective, following advantages and limitations should be clarified. Firstly, the incidence of single-segmental OVCF was significantly higher than that of non-contiguous OVCF.6 Consequently, in a retrospective study from a single center, the sample size of the single-segmental OVCF group was larger than that of the non-contiguous OVCF group. Thus, the sample size of the non-contiguous two-level group is relatively small, which may reduce the ability to detect weak effects, and the confidence interval of the regression analysis may be relatively wide. Further validation with an expanded sample size is needed in future studies.
Besides, computational mechanical analysis from numerical models with only one difference allows for the discretization of key biomechanical variables by adjusting entry parameters accordingly.44 This biomechanical change corroborates the findings from clinical observations. However, according to our computational results, when the difference in computed stress values of bony structures is within 5%, we usually consider this difference to be minor.45 Given that the stress difference in cortical bone between the two groups of models exceeded 10% under extension loading conditions, there might be a certain degree of cumulative damage risk under this condition, and this topic should still be validated in future fatigue mechanical testing with cyclic loading.46 Finally, the biomechanical effects of paraspinal muscles have not been considered in this study. Considering the definite clinical and biomechanical value of paraspinal muscles, the biomechanical interaction between fracture type changes and paraspinal muscle degeneration also needs to be further verified in subsequent work.
Conclusion
By conducting a clinical evidence based biomechanical research, this study presents that patients with two-level non‑contiguous OVCF (with SVB) experience a higher incidence of AVF primarily related to poor BMD, rather than the exacerbation of stress concentration caused by two adjacent segmental cement augmentations. Therefore, it is advisable to recommend regular anti‑osteoporosis treatment, particularly for patients with multiple OVCF, to mitigate the risk of AVF.
Data Sharing Statement
All the data of the manuscript are presented in the paper.
Ethics Approval and Consent to Participate
Approval for this study was obtained from the Ethics committee of The Second Affiliated Hospital of Xuzhou Medical University. Due to the nature of the study—retrospective analysis of anonymized patient data without any intervention or identifiable personal information—the committee did not issue a formal approval number, in accordance with its standard policy for such non-interventional studies. The study was conducted in accordance with institutional regulations and the Declaration of Helsinki, and the requirement for written informed consent was waived by the committee. Consent for publication is not applicable. This study does not include any individual patient data (e.g., images or identifiable clinical details) requiring consent for publication.
Funding
This study was supported by Sichuan Medical Association 2025 Orthopedics Special Project (2025SAT21); Southwest Medical University 2025 Integrated Traditional Chinese and Western Medicine Special Project (2025ZXYZX10), Luzhou Science and Technology Program (2024JYJ019), and Sichuan Natural Science Foundation youth project (25QNJJ2155).
Disclosure
Xuebin Tang and Kai Huang are co-first authors for this study. The authors have no conflicts of interest to disclose in relation to this article.
References
1. Johnell O, Kanis J. Epidemiology of osteoporotic fractures. Osteoporos Int. 2005;16(S02):S3–12. doi:10.1007/s00198-004-1702-6
2. Lane NE. Epidemiology, etiology, and diagnosis of osteoporosis. Am J Obstet Gynecol. 2006;194(2 Suppl):S3–11. doi:10.1016/j.ajog.2005.08.047
3. Liu Z, Zhang H, Ma X, Zhang W, Shi B. Comparison of the efficacy of unilateral versus bilateral pedicle approach vertebroplasty in the treatment of osteoporotic thoracic and lumbar vertebral compression fractures: a retrospective cohort study. Medicine. 2025;104(31):e43632. doi:10.1097/md.0000000000043632
4. Yang CC, Chien JT, Tsai TY, Yeh KT, Lee RP, Wu WT. Earlier vertebroplasty for osteoporotic thoracolumbar compression fracture may minimize the subsequent development of adjacent fractures: a retrospective study. Pain Physician. 2018;21(5):E483–e491.
5. Xi Z, Xie Y, Chen S, et al. The cranial vertebral body suffers a higher risk of adjacent vertebral fracture due to the poor biomechanical environment in patients with percutaneous vertebralplasty. Spine J. 2023. doi:10.1016/j.spinee.2023.08.003
6. Zhang Y, Sun Z, Yin P, Zhu S, Hai Y, Su Q. Do sandwich vertebral bodies increase the risk of post-augmentation fractures? A retrospective cohort study. Archives of Osteoporosis. 2021;16(1):180. doi:10.1007/s11657-021-00922-9
7. Han S, Jang IT. Analysis of adjacent fractures after two-level percutaneous vertebroplasty: is the intervening vertebral body prone to re-fracture? Asian Spine J. 2018;12(3):524–532. doi:10.4184/asj.2018.12.3.524
8. Jia P, Tang H, Chen H, et al. Prophylactic vertebroplasty procedure applied with a resorbable bone cement can decrease the fracture risk of sandwich vertebrae: long-term evaluation of clinical outcomes. Regen Biomater. 2017;4(1):47–53. doi:10.1093/rb/rbw037
9. An Y, Li L, Lin X, Zhang Z, Zheng Z, Wang C. Risk assessment for sandwich vertebral fractures in the treatment of osteoporosis vertebral compression fractures using two methods of bone cement reinforcement. J Orthopaedic Surg Res. 2023;18(1):524. doi:10.1186/s13018-023-04006-x
10. Wang YT, Wu XT, Chen H, Wang C, Mao ZB. Adjacent-level symptomatic fracture after percutaneous vertebral augmentation of osteoporotic vertebral compression fracture: a retrospective analysis. J Orthop Sci. 2014;19(6):868–876. doi:10.1007/s00776-014-0610-7
11. Xie S, Cui L, Wang C, et al. Contact between leaked cement and adjacent vertebral endplate induces a greater risk of adjacent vertebral fracture with vertebral bone cement augmentation biomechanically. Spine J. 2024. doi:10.1016/j.spinee.2024.09.021
12. Xi Z, Xie Y, Sun S, Liu M, Li J. The lowest HU value on transverse planes: a predictive factor for cranial adjacent vertebral fracture risk after percutaneous vertebroplasty. Quant Imaging Med Surg. 2025;15(2):1275–1286. doi:10.21037/qims-24-1559
13. Aquarius R, Homminga J, Verdonschot N, Tanck E. The fracture risk of adjacent vertebrae is increased by the changed loading direction after a wedge fracture. Spine. 2011;36(6):E408–12. doi:10.1097/BRS.0b013e3181f0f726
14. Li J, Xie Y, Sun S, et al. Regional differences in bone mineral density biomechanically induce a higher risk of adjacent vertebral fracture after percutaneous vertebroplasty: a case-comparative study. Int J Surg. 2023. doi:10.1097/js9.0000000000000273
15. Li J, Zhang Z, Xie T, Song Z, Song Y, Zeng J. The preoperative hounsfield unit value at the position of the future screw insertion is a better predictor of screw loosening than other methods. Eur Radiol. 2022. doi:10.1007/s00330-022-09157-9
16. Chen Z, Chen Y, Zhou J, He Y, Li J. The bony density of the pedicle plays a more significant role in the screw anchorage ability than other regions of the screw trajectory. Orthop Surg. 2024. doi:10.1111/os.14299
17. Gausden EB, Nwachukwu BU, Schreiber JJ, Lorich DG, Lane JM. Opportunistic use of CT imaging for osteoporosis screening and bone density assessment: a qualitative systematic review. J Bone Joint Surg Am Vol. 2017;99(18):1580–1590. doi:10.2106/jbjs.16.00749
18. Perazzo H, Fernandes FF, Soares JC, et al. Learning curve and intra/interobserver agreement of transient elastography in chronic hepatitis C patients with or without HIV co-infection. Clin Res Hepatol Gastroenterol. 2016;40(1):73–82. doi:10.1016/j.clinre.2015.04.004
19. Kelcey B, Shen Z, Spybrook J. Intraclass correlation coefficients for designing cluster-randomized trials in sub-saharan africa education. Eval Rev. 2016;40(6):500–525. doi:10.1177/0193841x16660246
20. Baniasadi M, Babaie GR, Zeraati H, Memari F. Application of bootstrap sample-resample method in logistic regression in analysis of breast cancer data. J School Public Health Institute Public Health Res. 2006;80(4):801–804.
21. Lakens DJCP. Sample size justification. Collabra. 2022;8(1).
22. Quach NE, Yang K, Chen R, et al. Post-hoc power analysis:a conceptually valid approach for power based on observed study data. General Psychiat. 2022;35(4):266–272.
23. Mishra P, Singh U, Pandey CM, Mishra P, Pandey G. Application of student’s t-test, analysis of variance, and covariance. Ann Cardiac Anaesthesia. 2019;22(4):407–411. doi:10.4103/aca.ACA_94_19
24. Hampton CB, Berliner ZP, Nguyen JT, et al. Aseptic loosening at the tibia in total knee arthroplasty: a function of cement mantle quality? J Arthroplasty. 2020;35(6s):S190–s196. doi:10.1016/j.arth.2020.02.028
25. Christensen DL, Nappo KE, Wolfe JA, et al. Ten-year fracture risk predicted by proximal femur Hounsfield units. Osteoporosis Int. 2020;31(11):2123–2130. doi:10.1007/s00198-020-05477-y
26. Schmidt H, Heuer F, Simon U, et al. Application of a new calibration method for a three-dimensional finite element model of a human lumbar annulus fibrosus. Clin Biomech. 2006;21(4):337–344. doi:10.1016/j.clinbiomech.2005.12.001
27. DeLucca JF, Cortes DH, Jacobs NT, Vresilovic EJ, Duncan RL, Elliott DM. Human cartilage endplate permeability varies with degeneration and intervertebral disc site. J Biomechanics. 2016;49(4):550–557. doi:10.1016/j.jbiomech.2016.01.007
28. Li J, Xu C, Zhang X, et al. Disc measurement and nucleus calibration in a smoothened lumbar model increases the accuracy and efficiency of in-silico study. J Orthop Surg Res. 2021;16(1):498. doi:10.1186/s13018-021-02655-4
29. Xu C, Xi Z, Fang Z, et al. Annulus calibration increases the computational accuracy of the lumbar finite element model. Global Spine J. 2022:21925682221081224. doi:10.1177/21925682221081224
30. Xi Z, Xie Y, Sun S, Hu F, Li J. Sagittal-oriented articular processes and intervertebral disc degeneration phenotypes can concurrently lead to an increased presence of annulus tears in the cranial adjacent motion segment: a clinical review and biomechanical simulation. Bone Joint Res. 2025;14(9):777–790. doi:10.1302/2046-3758.149.Bjr-2024-0461.R2
31. Tsouknidas A, Sarigiannidis SO, Anagnostidis K, Michailidis N, Ahuja S. Assessment of stress patterns on a spinal motion segment in healthy versus osteoporotic bony models with or without disc degeneration: a finite element analysis. Spine J. 2015;15(3 Suppl):S17–s22. doi:10.1016/j.spinee.2014.12.148
32. Heuer F, Schmidt H, Claes L, Wilke HJ. Stepwise reduction of functional spinal structures increase vertebral translation and intradiscal pressure. J Biomechanics. 2007;40(4):795–803. doi:10.1016/j.jbiomech.2006.03.016
33. Renner SM, Natarajan RN, Patwardhan AG, et al. Novel model to analyze the effect of a large compressive follower pre-load on range of motions in a lumbar spine. J Biomechanics. 2007;40(6):1326–1332. doi:10.1016/j.jbiomech.2006.05.019
34. Zhang L, Yang G, Wu L, Yu B. The biomechanical effects of osteoporosis vertebral augmentation with cancellous bone granules or bone cement on treated and adjacent non-treated vertebral bodies: a finite element evaluation. Clin Biomech. 2010;25(2):166–172. doi:10.1016/j.clinbiomech.2009.10.006
35. Liang D, Ye LQ, Jiang XB, et al. Biomechanical effects of cement distribution in the fractured area on osteoporotic vertebral compression fractures: a three-dimensional finite element analysis. J Surg Res. 2015;195(1):246–256. doi:10.1016/j.jss.2014.12.053
36. Ottardi C, Galbusera F, Luca A, et al. Finite element analysis of the lumbar destabilization following pedicle subtraction osteotomy. Med Engineer Phys. 2016;38(5):506–509. doi:10.1016/j.medengphy.2016.02.002
37. Ottardi C, La Barbera L, Pietrogrande L, Villa T. Vertebroplasty and kyphoplasty for the treatment of thoracic fractures in osteoporotic patients: a finite element comparative analysis. J Appl Biomaterial Funct Material. 2016;14(2):e197–204. doi:10.5301/jabfm.5000287
38. Xi Z, Xie Y, Sun S, et al. Stepwise reduction of bony density in patients induces a higher risk of annular tears by deteriorating the local biomechanical environment. Spine J. 2024. doi:10.1016/j.spinee.2023.12.007
39. Hashimoto K, Aizawa T, Kanno H, Itoi E. Adjacent segment degeneration after fusion spinal surgery-a systematic review. Int Orthop. 2019;43(4):987–993. doi:10.1007/s00264-018-4241-z
40. Park P, Garton HJ, Gala VC, Hoff JT, McGillicuddy JE. Adjacent segment disease after lumbar or lumbosacral fusion: review of the literature. Spine. 2004;29(17):1938–1944. doi:10.1097/01.brs.0000137069.88904.03
41. Gornet MF, Chan FW, Coleman JC, et al. Biomechanical assessment of a PEEK rod system for semi-rigid fixation of lumbar fusion constructs. J Biomech Eng. 2011;133(8):081009. doi:10.1115/1.4004862
42. Kim MJ, Park SY, Kang S, et al. Low modulus PMMA-based bone cement for the reduction of adjacent vertebral fractures after vertebroplasty. Acta Biomater. 2025;203:399–411. doi:10.1016/j.actbio.2025.07.053
43. Adams MA, Roughley PJ. What is intervertebral disc degeneration, and what causes it?). Spine. 2006;31(18):2151–2161. doi:10.1097/01.brs.0000231761.73859.2c
44. Li JC, Xie TH, Zhang Z, Song ZT, Song YM, Zeng JC. The mismatch between bony endplates and grafted bone increases screw loosening risk for OLIF patients with ALSR fixation biomechanically. Front Bioeng Biotechnol. 2022;10:862951. doi:10.3389/fbioe.2022.862951
45. Wu W, Wang H, Liu W, et al. Comparative analysis of internal fixation modalities for PER type IV ankle fractures: a finite element study. J Orthopaedic Surg Res. 2024;19(1).
46. Kang DG, Lehman RA, Bevevino AJ, et al. Pedicle screw “hubbing” in the immature thoracic spine: a biomechanical and micro-computed tomography evaluation. J Pediatr Orthop. 2014;34(7):703–709. doi:10.1097/bpo.0000000000000166
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.