Back to Journals » International Journal of Women's Health » Volume 18
Nomogram Predicting Intrapartum Cesarean Delivery in Singleton Pregnancies at Term: A Prospective Observational Study Utilizing an Ultrasound-Based System
Authors Wang Q, Wu H ![]() , Wang Y, Meng Y, Yang J, Shi J, Xu H, Weng-Y, Chai Y
, Wang Y, Meng Y, Yang J, Shi J, Xu H, Weng-Y, Chai Y
Received 3 November 2025
Accepted for publication 1 April 2026
Published 16 April 2026 Volume 2026:18 578740
DOI https://doi.org/10.2147/IJWH.S578740
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Qiumeng Wang,1,* Hanglin Wu,1,* Yun Wang,1 YaNi Meng,1 Jiali Yang,1 Juanjuan Shi,1 Hongmiao Xu,1 Yinan Weng,2 Yun Chai1
1Department of Obstetrics and Gynecology, Hangzhou Women’s Hospital, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Ultrasound, Hangzhou Women’s Hospital, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yun Chai, Department of Obstetrics and Gynecology, Hangzhou Women’s Hospital, No. 369 Kun Peng Road, Hangzhou, Zhejiang, People’s Republic of China, Email [email protected]
Purpose: The objective of this study was to develop and validate a nomogram designed to predict the likelihood of intrapartum cesarean delivery in singleton pregnancies at term, utilizing an ultrasound-based system.
Patients and Methods: This prospective study involved women who gave birth at Hangzhou Women’s Hospital from August 2022 to March 2024. The study recruited pregnant women who were in a cephalic position, had singleton pregnancies at term (37+0 to 41+6 weeks), and expressed a preference for vaginal delivery. The LaborPro system was employed to perform infrapubic ultrasound imaging and to assess fetal head positioning. A nomogram was generated through multivariate logistic regression analysis, incorporating various maternal, fetal, and pregnancy-related characteristics. The predictive accuracy and discriminative capacity of the nomogram underwent internal validation via 1000-bootstrap resampling. A decision curve analysis was performed to determine a net-benefit threshold for the predictive model.
Results: A total of 705 women were included, with an observed intrapartum cesarean delivery rate of 13.6%. The logistic regression analysis identified six significant predictors of intrapartum cesarean delivery: maternal height, parity, onset of labor, interspinous diameter, fetal position and estimated fetal weight. Following bootstrap resampling for internal validation, the nomogram demonstrated good calibration, achieving an area under the curve of 0.77 (95% confidence interval, 0.72– 0.82). In the induction of labor subgroup, the inclusion of the Bishop score significantly enhanced predictive performance, outperforming existing clinical models (P < 0.001). Decision curve analysis indicated a substantial net benefit across a wide threshold range (0.1– 0.7), supporting its utility in shared decision-making.
Conclusion: The LaborPro-based nomogram provides a validated, objective tool for individualized ICS risk stratification. The integration of internal pelvic dimensions with traditional cervical assessments offers superior predictive accuracy, particularly for women undergoing induction. Future multi-center studies are warranted to externally validate these findings across diverse populations.
Keywords: intrapartum cesarean delivery, LaborPro system, multivariate logistic regression, nomogram
Introduction
In clinical practice, intrapartum caesarean section (ICS) is frequently employed to address dystocia and to avert severe complications for both mothers and newborns. Currently, cesarean section rates are rising worldwide. In many regions, the rate of ICS for first-time mothers with full-term, singleton pregnancies remains high, often between 21% and 29.4%.1,2 However, ICS is associated with an elevated risk of maternal infections, postpartum hemorrhage, and increased likelihood of respiratory distress and neonatal asphyxia.3–5 Consequently, a primary concern for obstetricians and laboring women is the ability to accurately predict labor outcomes.
To address this challenge, various prediction models have been developed to assist obstetricians in identifying women who are at a higher risk for requiring ICS.6–12 These models consider a range of variables as potential risk factors, including maternal demographic information, antenatal history, and findings from cervical examinations. However, there is a clear gap in these models: they rarely include precise measurements of the internal pelvis. This is a problem because the fit between the fetal head and the maternal pelvis is a key factor in labor success. In the past, internal pelvic measurements were hard to get. External measurements are not accurate enough, and clinical exams of the pelvic interior are difficult to quantify.
The X-ray imaging system is utilized for the measurement of pelvic dimensions; however, its safety during pregnancy raises significant concerns. Some researchers have explored the use of magnetic resonance imaging (MRI) with three-dimensional reconstruction technology to analyze the female pelvis. Nonetheless, MRI is associated with several limitations, including extended imaging durations, high costs, and restricted accessibility.13–15 Conversely, the LaborPro system employs magnetic field spatial positioning and tracking techniques, which are controlled by computer software. This system generates a non-invasive, low-power magnetic field environment and enables the identification of marker points through a position sensor held by the examiner, allowing for automatic calculation of radial line lengths. This method is characterized by its convenience, cost-effectiveness, and absence of radiation, enabling it to be performed concurrently with a vaginal examination.
The present study was undertaken to develop a novel predictive model that incorporates pelvic measurements to assess the risk of ICS, with the objective of mitigating unnecessary ICS.
Materials and Methods
Study Population and Data Collection
This prospective cohort study was carried out from August 2022 to March 2024 at a tertiary specialty hospital and received approval from the medical ethics committee of Hangzhou Women’s Hospital (2022-A-5-10). This study was conducted in accordance with the Declaration of Helsinki, and the researchers are committed to safeguarding the personal privacy of participants and ensuring the security of their information. All participants provided written informed consent prior to enrollment. This study adheres to the TRIPOD (Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis) statement, while external validation was beyond the scope of this single-center study. Participants were recruited at admission using consecutive sampling based on the following inclusion criteria: (1) singleton term pregnancy (explicitly defined as 37+0 to 41+6 weeks of gestation confirmed by first-trimester ultrasound); (2) cephalic presentation; (3) prior to active labor (cervical dilation < 5 cm); (4) planned trial of labor.
Exclusion criteria were: (1) multiple gestation; (2) non-cephalic presentation; (3) known contraindications to vaginal delivery, including placenta previa, active genital herpes infection, prior classical cesarean section, and severe fetal anomalies; (4) major fetal congenital anomalies; (5) contraindications to LaborPro measurement (eg, implanted electronic devices); and (6) refusal to participate. To enhance the generalizability of our findings, the study also included women experiencing spontaneous labor as well as multiparous women. Spontaneous labor was defined as the presence of regular uterine contractions (at least 1 every 5 minutes) associated with cervical effacement and a cervical dilatation of 1 cm.
Following the enrollment process, data pertaining to maternal and neonatal characteristics were systematically gathered, which comprised: maternal age, height, weight at the time of delivery, parity, the onset of labor, and clinical estimated fetal weight. Variables were selected a priori based on their established clinical significance in previous literatures.6–12 For participants undergoing induction of labor, the cervical Bishop score was additionally assessed by clinical examination upon admission. Clinical fetal weight estimation is based on ultrasound estimations, which was conducted utilizing a sonographic model that incorporated measurements of the head, body, and femur.16 The mathematical representation of this model is as follows:
Log10 estimated fetal weight = 1.326–0.00326* abdominal circumference* femur length + 0.0107* head circumference + 0.0438* abdominal circumference + 0.158 femur length.
The LaborPro system (LaborPro®, Trig Medical Ltd., Haifa, Israel; model: LaborPro Prenatal; software version: 3.0.3.100) was utilized in conjunction with a vaginal examination for each participant at clinical admission. The accuracy and reliability of the LaborPro system for pelvic measurement have been previously validated in multiple studies, demonstrating high intra- and inter-operator reproducibility and strong correlation with conventional imaging modalities.17,18 All LaborPro measurements were performed at clinical admission with the participant in the dorsal lithotomy position, with the hips flexed and abducted. Measurements were obtained after bladder emptying to minimize potential interference with pelvic anatomy. All measurements were conducted by a designated sonographer who had completed a standardized training protocol (at least 50 supervised scans). To ensure objectivity, the operators performing the LaborPro scans were blinded to the participants’ clinical history and the subsequent delivery outcomes and were not involved in the management of labor. The implementation of the LaborPro system is delineated in the following steps:19
Step 1 involves the spatial localization of the pelvic inlet plane and the birth canal. This process entails the mapping of the maternal pelvis through the identification of specific anatomical points utilizing small positional sensors in conjunction with ultrasound technology. The L5 spinous process serves as a reference point, ensuring that measurements remain consistent and are not influenced by variations in the maternal position or movement.
Step 2 focuses on the determination of fetal station via infrapubic ultrasound imaging. In this phase, the superior and inferior boundaries of the symphysis pubis, along with the intersection point between the birth canal and the fetal skull, are marked either automatically or manually. The system then computes and displays the station of the fetal head in relation to the pelvic inlet plane and the birth canal, providing real-time data.
The evaluation of fetal head positioning by the system is conducted by assessing the spatial relationship of key head landmarks to the center of the birth canal. This is achieved by designating one of several ultrasound landmarks on the display, which may include the biparietal or occipitofrontal diameter, cervical vertebra, midline, or orbits. The results are graphically represented according to the measured degree of rotation.
Statistical Analysis
The primary outcome was ICS, defined as cesarean delivery performed after the initiation of a trial of labor. Predictors included maternal age, BMI, parity, gestational age, cervical dilation at admission, and pelvic inlet diameter measured by LaborPro. Women who did not achieve successful labor induction through various methods were included in the ICS group. Missing data were addressed using Multiple Imputation by Chained Equations (MICE) under the assumption that data were missing at random. Following data imputation, multicollinearity among the predictors was assessed using the Variance Inflation Factor (VIF). Any variable with a VIF exceeding 5 was further evaluated for potential removal or combination to ensure model stability. Continuous variables were expressed as means with standard deviations, whereas categorical variables were reported as frequencies and percentages. The comparison between the two groups, along with univariate analyses, was performed using appropriate statistical tests, including Student’s t-test, Mann–Whitney test, Chi-square test, or Fisher’s exact test. Variables that yielded a p-value of less than 0.1 in the univariate analysis were subsequently incorporated into a multivariate logistic regression model. Covariates were systematically removed in a stepwise manner until all remaining covariates in the final model had a p-value of less than 0.05.
A nomogram was developed utilizing coefficients derived from a logistic regression model implemented in R. The internal validation of the nomogram involved assessments of both discrimination and calibration. The model’s discriminative capability was evaluated using the area under the receiver operating characteristic (ROC) curve, which ranges from 0.5, indicating no discrimination, to 1, indicating perfect discrimination. The differences between AUCs were compared using the DeLong test.20 The optimal cutoff value for risk stratification was determined using Youden’s index based on the ROC curve. Model calibration was evaluated using both the Hosmer-Lemeshow test and a visual calibration plot. Furthermore, the nomogram underwent 1000 bootstrap resampling for internal validation to evaluate its predictive accuracy. A decision curve analysis was also conducted to identify a net-benefit threshold for prediction.21,22 An interactive, web-based dynamic nomogram application was created using Shinyapps.io (Published July 22, 2024).
To evaluate the incremental value of incorporating pelvic measurements, we compared the performance of our proposed model with a baseline model that included only conventional predictors (maternal demographic information and antenatal history). To evaluate our nomogram, we compared its performance with existing models designed for both nulliparous and multiparous women.7,23 Pre-specified subgroup analyses were conducted to evaluate the model’s performance across clinically relevant subgroups, including: (1) nulliparous vs multiparous women; (2) spontaneous vs induced labor. All analyses were performed in RStudio version 2023.09.1 Build 494 within the R environment version 4.3.3 (2024-02-29). Results with a p-value of less than 0.05 were deemed statistically significant and are reported as odds ratios (ORs) accompanied by 95% confidence intervals (CIs).
The minimum sample size was determined based on the criteria proposed by Riley et al for developing clinical multivariable prediction models.24 Assuming a c-statistic of 0.80 and an anticipated outcome prevalence of 20% for ICS according to a previous prospective study,25 a model with 15 predictor parameters requires a minimum of 666 participants. To account for a potential 5% rate of missing data or loss to follow-up, we planned to recruit a total of 700 participants, which would provide approximately 140 primary outcome events.
Results
Baseline Characteristics of the Study Population
A total of 705 women satisfied the inclusion criteria and were subsequently enrolled in the present study. Table 1 presents the baseline characteristics of the participants and the labor circumstances within the study cohort. The incidence of ICS was found to be 13.6%. It was observed that women who underwent ICS were older in comparison to those who delivered vaginally. Additionally, women who experienced induced labor exhibited a greater likelihood of resulting in ICS compared to their counterparts who had spontaneous labor. The fetal weight assessed clinically and the neonatal weight were observed to be comparable in both groups.
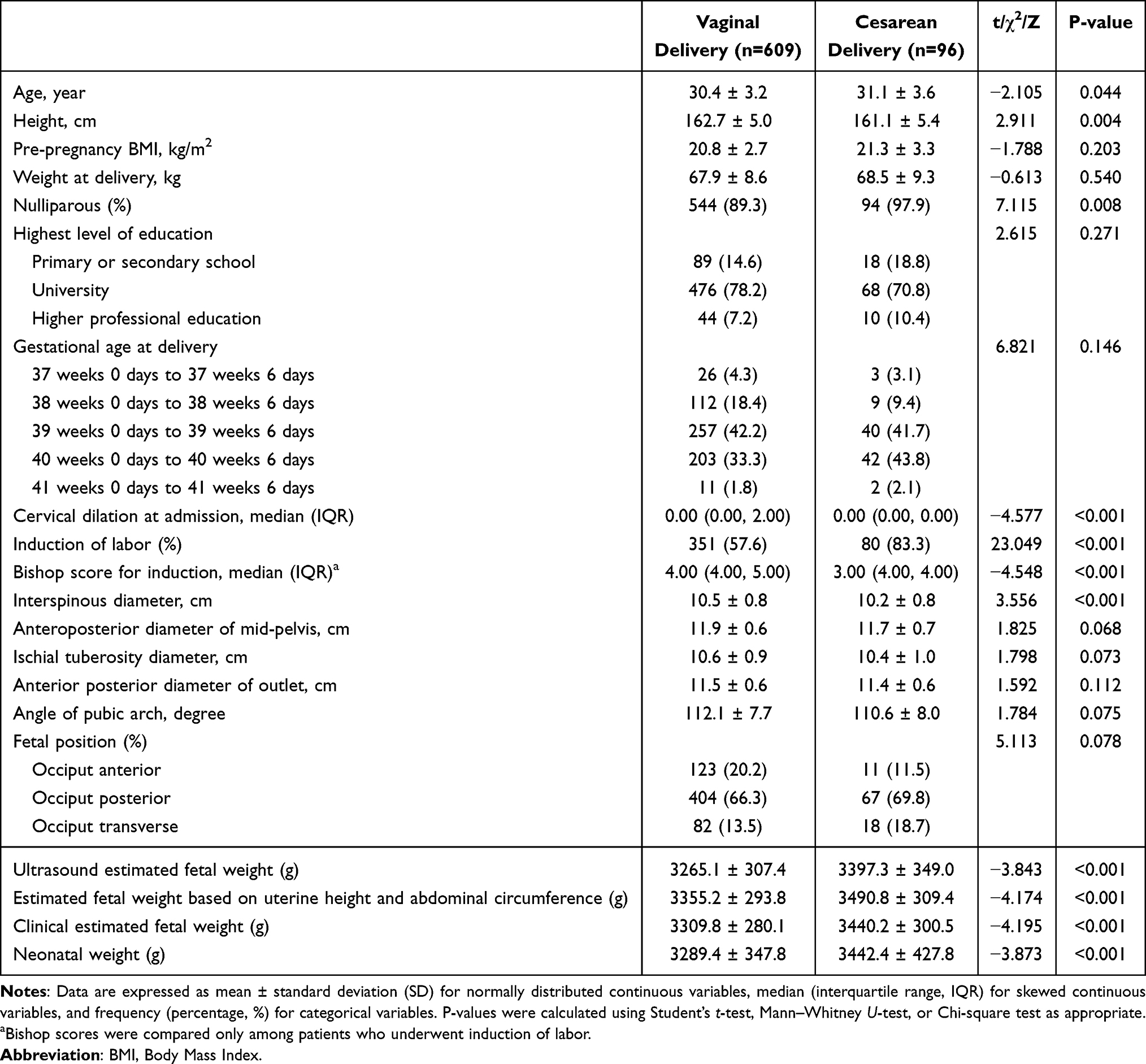 |
Table 1 Baseline Participant and Labor Characteristics |
Univariate and Multivariate Analysis of Risk Factors
To ensure the parsimony and stability of the final model, cervical dilation and weight were removed to minimize the impact of multicollinearity (Supplementary Figures 1 and 2). In the univariate analysis, several variables demonstrated a significance level of P<0.1 and were subsequently included in the multivariate logistic regression modeling. These variables comprised maternal age, height, pre-pregnancy BMI, parity, onset of labor, interspinous diameter, anteroposterior diameter of mid-pelvis, ischial tuberosity diameter, angle of pubic arch, fetal position and estimated fetal weight. Among these variables, height, parity, onset of labor, interspinous diameter, fetal position and estimated fetal weight retained its significance in the multivariate logistic regression analysis (Table 2). Each 1 cm increase in height was associated with a 7.1% reduction in the risk of ICS after adjusting for other clinical confounders (OR 0.92, 95% CI 0.88–0.97). Women who experienced induced labor exhibited more than a threefold increase in the risk of ICS compared to those who underwent spontaneous labor (OR 3.68, 95% CI 2.10–6.44). Additionally, a 1 cm increase in interspinous diameter was associated with a 46.6% reduction in the odds of ICS (OR 0.53, 95% CI 0.38–0.75), while an increase of 100 grams in estimated fetal weight corresponded to a 29.7% increase in the odds of ICS (OR 1.30, 95% CI 1.18–1.43). While estimated fetal weight and labor induction occupied the top two positions, interspinous diameter served as the foundational anatomical predictor, outperforming both maternal height and parity in its contribution to the model’s variance (Supplementary Figure 3).
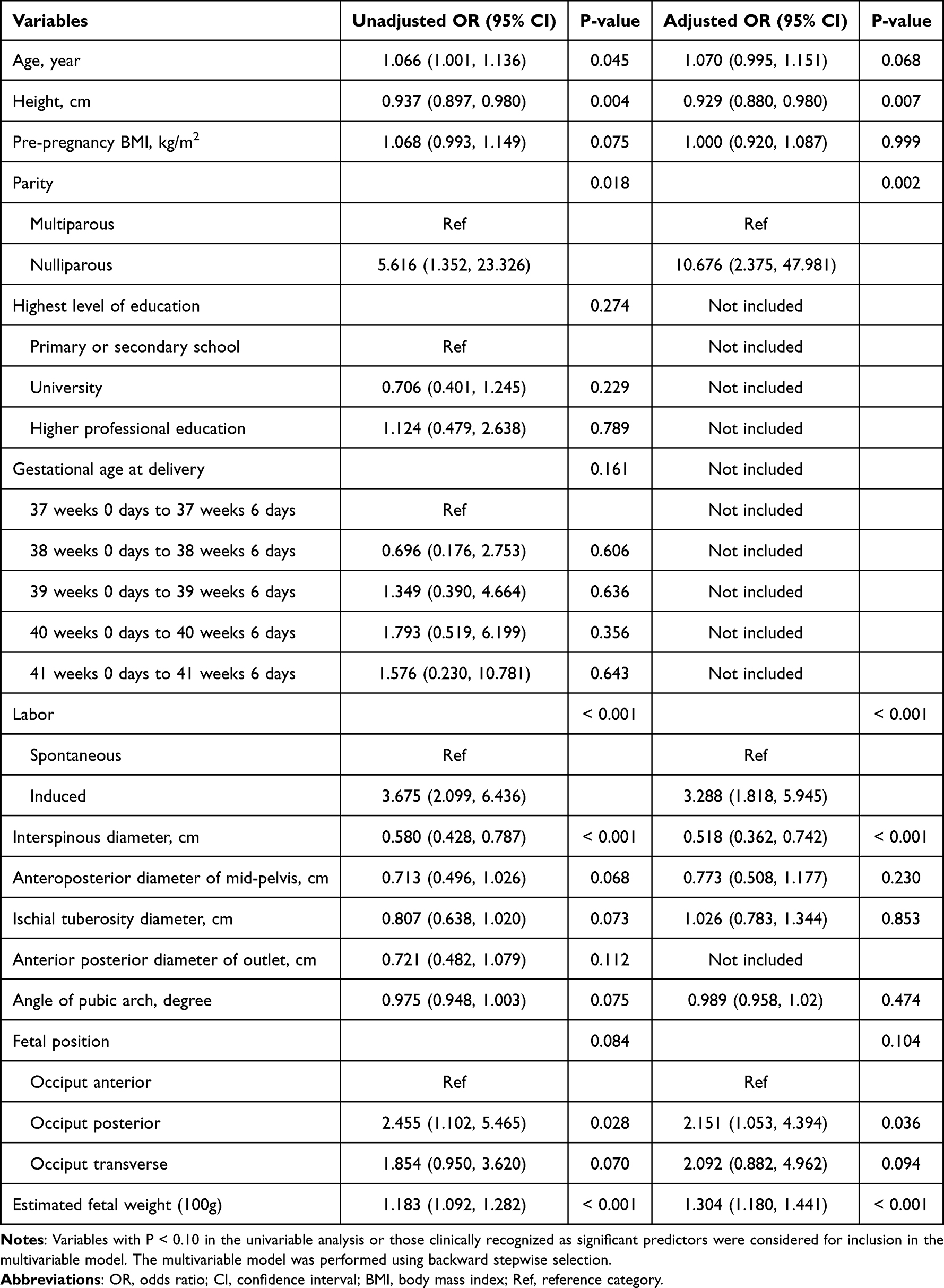 |
Table 2 Univariable and Multivariable Logistic Regression Analyses of Risk Factors for Intrapartum Cesarean Delivery |
Nomogram Development and Model Performance
The final logistic model was formulated as a user-friendly nomogram, as illustrated in Figure 1A, and is accessible online (https://wuhanglin.shinyapps.io/Cesarean-Calculator/), as depicted in Figure 1B. The calibration plot for the nomogram, presented in Figure 2, indicated a strong correlation between the observed and predicted risks of ICS, with a mean absolute error of 0.016. The Hosmer-Lemeshow test results (P = 0.697) confirm that the model is well-calibrated and reliable for clinical use. The full model achieved a marginally significant superior AUC of 0.771 (95% CI: 0.720–0.823, Figure 3), outperforming the clinical (AUC = 0.752) and basic (AUC = 0.751) models. At the optimal Youden index threshold, the full model demonstrated a marked improvement in specificity (73.07%) and accuracy (72.77%) compared to the basic model (62.73% and 64.26%, respectively, Supplementary Table 1).
 |
Figure 1 Established (A) and online dynamic (B) nomogram predicting risk of intrapartum cesarean delivery in singleton pregnancies at term. We considered a representative case of a nulliparous woman (163 cm in height) admitted for induction of labor. Her clinical parameters included a clinical estimated fetal weight of 3300g, an interspinous diameter of 10.0 cm, and a fetus in the occiput anterior position. According to the dynamic nomogram, the predicted probability of intrapartum cesarean delivery for this participant was approximately 12%. Abbreviations: OA, Occiput anterior; OP, Occiput posterior; OT, Occiput transverse. |
 |
Figure 2 Calibration curve of the nomogram for intrapartum cesarean delivery prediction. The x-axis represents the predicted probability calculated by the nomogram, and the y-axis represents the actual observed rate of cesarean delivery. The dashed line represents an ideal match between predictions and observations. The solid blue line indicates the performance of our model, with the shaded area representing the 95% confidence interval calculated via the Wilson score method. The model shows high predictive accuracy with a Mean Absolute Error of 0.016. |
 |
Figure 3 Comparison of ROC curves for the three predictive models. The ROC curves represent the discrimination performance of the full model (solid blue line), the clinical model (dashed Orange line, excluding interspinous diameter), and the basic model (dotted red line, further excluding fetal position). At the blue optimal cutoff point (Youden’s index), the full model achieved a sensitivity of 70.83% and a specificity of 73.07%. Pairwise comparisons of AUCs were performed using the DeLong test. Abbreviations: ROC, receiver operating characteristic; AUC, area under the curve. |
The decision curve analysis for the nomogram is illustrated in Figure 4. The threshold range (0.1–0.7) represents a spectrum of clinical scenarios: from conservative monitoring (low threshold) to strict surgical intervention (high threshold). The nomogram model (red line) consistently outperformed the “treat-all” strategy, which loses its clinical viability when the risk threshold exceeds 15%, and the “treat-none” strategy, which fails to capture any high-risk events. Specifically, within the most common clinical decision-making window (20–40% risk), our model provides a significant standardized net benefit, thereby optimizing the balance between avoiding unnecessary procedures and ensuring timely surgical intervention.
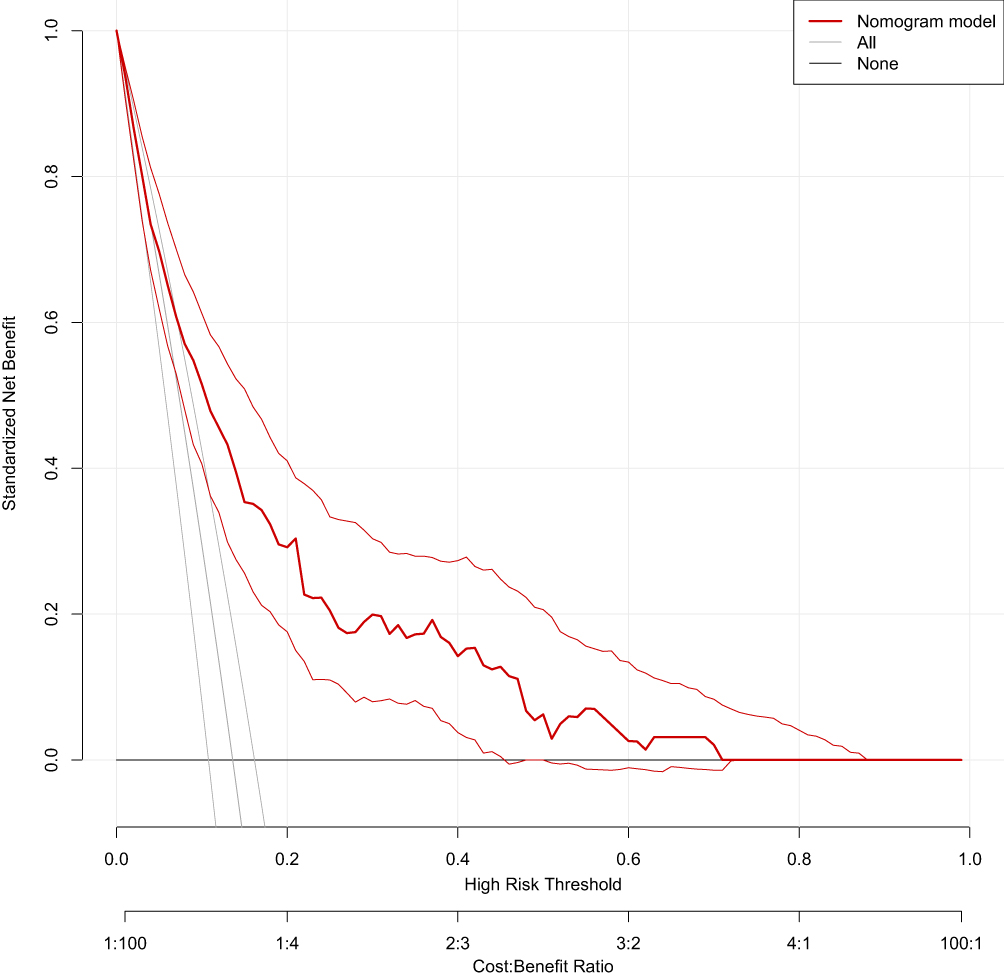 |
Figure 4 Decision curve analysis of the nomogram. The y-axis represents the standardized net benefit, and the x-axis represents the high-risk threshold probability. The red solid line indicates the net benefit of using the nomogram model. The grey line (All) represents the strategy of assuming all patients will require a cesarean delivery, and the horizontal black line (None) represents the strategy of assuming no patients will require a cesarean delivery. The nomogram model curve remains above both the “All” and “None” lines across most threshold probabilities, particularly in the 10–70% range, indicating its practical clinical utility in optimizing delivery mode management. |
Sensitivity Analysis and Subgroup Analysis
Given that nulliparous women constituted the vast majority of the study population (n = 638, 90.5%), a sensitivity analysis was performed exclusively within this subgroup to ensure the robustness of the predictive model. The multivariable logistic regression analysis within the nulliparous cohort yielded results highly consistent with the primary analysis (Supplementary Table 2 and Supplementary Figures 4, 5). The stratified subgroup analysis was performed based on the mode of labor onset. Though the adjusted OR (aOR) for interspinous diameter was nearly identical between the spontaneous (aOR = 0.51) and induced labor (aOR = 0.52) groups, and maternal height showed a consistent aOR of 0.93 in both cohorts, the spontaneous labor group exhibited notably wider 95% CI without statistical significance compared to the induced labor group (Supplementary Table 3). The lack of statistical significance in the spontaneous group is likely a reflection of diminished statistical power due to the smaller sample size and wider confidence intervals in this stratum.
Given the inherent uncertainties observed in the spontaneous labor cohort and the focus of existing literature on induced populations, an enhanced multivariable model was developed specifically for the induction of labor subgroup (n = 431). This model incorporated the cervical Bishop score alongside the previously predictors. Following multivariable adjustment, the Bishop score emerged as a significant independent predictor of delivery mode (Supplementary Table 4). The enhanced nomogram achieved a significantly higher AUC: 0.791 (95% CI: 0.736–0.846) compared to the Alavifard model (AUC: 0.631; 95% CI: 0.568–0.695) and the Rossi model (AUC: 0.665; 95% CI: 0.601–0.729). Pairwise comparisons using the DeLong test confirmed that the improvements in discrimination were highly statistically significant (P < 0.001, Supplementary Figure 6).
Discussion
In this prospective cohort study, we identified several independent risk factors for ICS, including maternal height, parity, onset of labor, interspinous diameter, fetal position and estimated fetal weight. The model demonstrated good discriminative ability with an AUC of 0.771 (95% CI: 0.720–0.823), indicating that it can correctly distinguish between women who will and will not require ICS in approximately 77% of cases. The superior performance of our model likely reflects the incremental value of objective pelvic measurements, which have been underutilized in previous models due to limitations in measurement techniques.7,23,26 From a clinical perspective, this level of discrimination suggests that the model could serve as a valuable adjunct to clinical judgment, helping to identify women at sufficiently low risk to safely continue labor, as well as those at sufficiently high risk to warrant heightened preparedness for cesarean delivery. The significant advancement in the enhanced nomogram underscores the necessity of integrating objective pelvic measurements with traditional cervical assessments (Bishop score) to optimize induction outcomes.
Key factors contributing to successful vaginal delivery include maternal pelvic size and shape, soft tissue thickness, the molding of the birth canal during labor, the coordination and intensity of the laboring force, as well as the size of the fetus, fetal head size, and its ability to undergo deformation.27 Current obstetric consensus widely acknowledges that the match between maternal pelvic size and fetal size is a critical determinant for successful vaginal delivery. Throughout pregnancy, fluctuating hormonal levels affect the laxity of pelvic joints and ligaments, while the descent of the fetal presenting part imposes pressure on the pelvis, resulting in dynamic changes in maternal pelvic dimensions at different stages of pregnancy, before, and during labor. Prior predictive models for vaginal delivery based solely on single imaging measurements such as ultrasound, CT, or MRI have consistently failed to encompass all these influential factors, resulting in unsatisfied predictive outcomes.13,14
Our research develops a predictive model integrating intrapelvic measurement using the LaborPro system to assess the risk of ICS. The LaborPro system measures pelvic dimensions directly via a vaginal probe, estimates fetal weight through ultrasound, and identifies the fetal head engagement and position, mitigating the impact of variables such as differences in soft tissue thickness and joint ligament laxity within the birth canal, fetal obesity, and the cranial suture overlapping ability of deformed fetal heads on model establishment. LaborPro system, since its invention and clinical application, has seen reports on its clinical applicability in determining fetal position during labor and vaginal measurements.18,28 Based on our limited literature review, there is currently no evidence regarding the use of the LaborPro system to develop a predictive model for pelvic-fetal compatibility in predicting vaginal delivery, making this study pioneering in this field.
In our study, maternal age showed a borderline significant association with intrapartum cesarean delivery (aOR = 1.070, P = 0.068), suggesting a potential trend consistent with several previous reports.1,8,23 Although it did not reach strict statistical significance in the multivariable model, the observed trend may still be linked to age-related physiological changes. This finding may be attributed to age-related physiological changes in myometrial function, including reduced uterine contractility and diminished responsiveness to oxytocin, as well as progressive stiffening of the pelvic connective tissue and decreased pelvic joint mobility, all of which may impair the efficiency of labor progression.29 In the literature by Li Jun et al, maternal BMI was utilized as an indicator, concluding that an elevated BMI is a detrimental factor for vaginal delivery13 Considering the individual variability in weight and body shape changes during pregnancy, similar BMI values may correspond to different body compositions and pelvic characteristics. To further elucidate the isolated effects of height and weight, we conducted separate analyses for each variable. The findings indicate that height serves as an independent influencing factor, corroborating the results of previous studies.30,31 Another explanation may be due to the dominant predictive power of internal anatomical metrics (interspinous diameter) which override indirect markers like BMI in determining cephalopelvic compatibility.
Our findings indicate that the transverse diameter of the mid-pelvic plane, specifically the interspinal distance, is the most significant indicator related to the occurrence of ICS. One research study posited that a minimum interspinal distance of 10 cm at the mid-pelvic plane is a critical criterion for the passage of a fetus weighing 3400 grams.32 Additionally, research conducted by Li Jun et al suggested that the interspinal distance at the mid-pelvic plane, along with the ischial tuberosity distance at the outlet plane, serves as predictive indicators for successful vaginal delivery13 The mid-pelvic plane represents the narrowest section of the pelvis; thus, any constriction at this level may hinder internal rotation, subsequently affecting the descent of the fetal head and leading to labor stagnation, with a higher incidence of ICS at such times.33 Notably, among Chinese women, characteristics such as a female pelvis and flat pelvis are predominant, with instances of outlet diameters being smaller than those at the mid-pelvic plane being relatively rare. Our research findings corroborate this observation. Some studies have utilized radiological measurements, such as fetal biparietal diameter and abdominal circumference, to indirectly reflect fetal weight.13,34 In contrast, this model employs the clinical estimated fetal weight as the predictive indicator. By integrating maternal abdominal height, fetal abdominal circumference, and multiple ultrasound measurements, the model comprehensively estimates fetal weight, thereby mitigating disturbances related to estimation accuracy, fetal adiposity, and fetal head molding capabilities. In our study, the average clinical estimated weight closely approximated the actual newborn weight, enhancing the robustness of our model and substantiating that fetal weight is a significant influencing factor for ICS.
Historically, the findings from numerous early observational studies contributed to a widespread belief among healthcare providers and patients that labor induction is linked to an increased likelihood of failed labor and cesarean delivery.35,36 This was attributed to the potential for exogenous oxytocin to induce contractions before cervical ripening is complete, leading to dysfunctional labor patterns, as well as the absence of physiological priming that occurs during spontaneous labor onset.37 Similar to our research, these conclusions were drawn from comparisons between women undergoing induction and those experiencing spontaneous labor, which is both an inadequate and unrealistic comparison. The ARRIVE trial provided evidence that elective induction at 39 weeks of gestation in low-risk nulliparous women is correlated with a lower rate of cesarean births, without a corresponding rise in adverse perinatal outcomes when compared to expectant management.38 Furthermore, a recent systematic review and meta-analysis indicated that labor induction does not elevate the risk of emergency cesarean section.39
We propose the following stepwise approach for clinical implementation of the nomogram: First, perform LaborPro pelvic measurement at admission to the delivery unit prior to active labor (cervical dilation < 5 cm). The measurement can be performed concurrently with the initial cervical examination, minimizing additional time and patient discomfort. Then input the following variables into the online dynamic nomogram: height, parity, onset of labor, interspinous diameter, fetal position and estimated fetal weight. The tool generates an individualized predicted risk of ICS. The clinical utility of the LaborPro model was further demonstrated through three representative cases across a risk spectrum from 4% to 83% (Supplementary Table 5). The proposed prediction model is designed to complement existing labor management protocols. Current guidelines emphasize the use of partograms, cervical dilation progression, and clinical judgment to monitor labor and identify dystocia.40,41
The economic implications of adopting LaborPro-based pelvic measurement warrant consideration. In the Chinese healthcare context, the per-procedure cost of LaborPro measurement is approximately ¥200, which is modest compared to the incremental cost of an unnecessary cesarean section. Notably, beyond direct cost savings, reducing unnecessary cesarean deliveries confers additional benefits, including lower risks of surgical complications, shorter postpartum recovery, and improved outcomes for subsequent pregnancies.
This study has several notable strengths. First, the prospective cohort design minimized recall bias and allowed for standardized data collection, ensuring consistency across participants. Second, the use of the LaborPro system provided objective, quantitative pelvic measurements with demonstrated reliability, overcoming the limitations of subjective clinical assessment. Third, our model incorporated a comprehensive set of predictors, including both traditional risk factors and novel pelvic dimensions, enabling a more holistic assessment of ICS risk. Fourth, we employed rigorous methodological approaches, including bootstrap internal validation to mitigate overfitting and decision curve analysis to evaluate clinical utility. Fifth, we have developed an online dynamic nomogram (available at https://wuhanglin.shinyapps.io/Cesarean-Calculator/) that facilitates easy implementation in clinical settings, allowing clinicians to obtain individualized risk estimates without requiring specialized software.
The main limitation of this study is the reliance on the interspinous diameter of the ischium, which necessitates an accurate method of internal pelvic measurement. In regions where such precise techniques are unavailable, traditional vaginal examination becomes the alternative measurement, potentially compromising the accuracy of the results. Although in our cohort, the clinical estimated fetal weight demonstrated a high correlation with birth weight, with a Mean Absolute Percentage Error of approximately 6.33%, a more standardized and quantifiable fetal weight estimation model is necessary to enhance the certainty of fetal weight estimation, thereby improving the predictive accuracy of this model. Secondly, due to the single-institute nature of our research, external validation of data from other institutions could not be conducted, thereby affecting the robustness of the proposed model. We have made the prediction program available online and will seek to engage additional centers for the purpose of further validating the model in future studies. Thirdly, the study focused solely on pregnant women of Chinese descent, which may restrict the applicability of the model to women of other ethnic backgrounds. Lastly, although the integration of cervical readiness and internal pelvic dimensions significantly improved risk stratification, the sample size for this specific subpopulation (n = 431) remains relatively modest.
To address the limitation, future research should focus on: (1) external validation in diverse populations to confirm generalizability; (2) a multi-center randomized controlled trial comparing nomogram-guided care versus standard care; (3) integration with electronic health records to enable automated real-time risk calculation; (4) a formal cost-effectiveness analysis incorporating the per-procedure cost of LaborPro; and (5) validation in women with prior cesarean undergoing trial of labor after cesarean (TOLAC).
Conclusion
The LaborPro system demonstrates high accuracy and reliability in measuring the pelvic diameter. Maternal height, parity, onset of labor, interspinous diameter, fetal position and estimated fetal weight are independent influencing factors for ICS. The ICS prediction model provides a validated tool for individualized risk stratification that can be integrated into routine obstetric practice at the time of admission, supporting shared decision-making between clinicians and patients. Future multicenter external validation in diverse populations is essential to confirm generalizability before widespread clinical adoption.
Acknowledgments
We extend our thanks to the clinical staffs at Hangzhou Women’s Hospital for their assistance in data collection, and the contributions of all participants in this study.
Funding
This study was supported by two research initiatives: the Hangzhou Specialised Scientific Programme for Supporting Biological Duty and Health Industry Development entitled “Study on the Value of Three-dimensional Intrapartum Navigation System in Prenatal Cephalopelvic Disproportion Assessment” (No. 2022WJC057), and the Hangzhou Medical and Health Research Project titled “Clinical Significance of Prenatal Cervical Elastography in Cervical Maturation Evaluation” (No. A20230784).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tolcher MC, Holbert MR, Weaver AL, et al. Predicting cesarean delivery after induction of labor among nulliparous women at term. Obstet Gynecol. 2015;126:1059–13. doi:10.1097/AOG.0000000000001083
2. Burke N, Burke G, Breathnach F, et al. Prediction of cesarean delivery in the term nulliparous woman: results from the prospective, multicenter Genesis study. Am J Obstet Gynecol. 2017;216:598.e1–598.e11. doi:10.1016/j.ajog.2017.02.017
3. Bodner K, Wierrani F, Grünberger W, et al. Influence of the mode of delivery on maternal and neonatal outcomes: a comparison between elective cesarean section and planned vaginal delivery in a low-risk obstetric population. Arch Gynecol Obstet. 2011;283:1193–1198. doi:10.1007/s00404-010-1525-y
4. Karlström A, Lindgren H, Hildingsson I. Maternal and infant outcome after caesarean section without recorded medical indication: findings from a Swedish case-control study. BJOG. 2013;120:479–486. doi:10.1111/1471-0528.12129
5. Werner EF, Han CS, Savitz DA, et al. Health outcomes for vaginal compared with cesarean delivery of appropriately grown preterm neonates. Obstet Gynecol. 2013;121:1195–1200. doi:10.1097/AOG.0b013e3182918a7e
6. Kamel RA, Negm SM, Youssef A, et al. Predicting cesarean delivery for failure to progress as an outcome of labor induction in term singleton pregnancy. Am J Obstet Gynecol. 2021;224:609.e1–609.e11. doi:10.1016/j.ajog.2020.12.1212
7. Alavifard S, Meier K, Shulman Y, et al. Derivation and validation of a model predicting the likelihood of vaginal birth following labour induction. BMC Pregnancy Childbirth. 2019;19:130. doi:10.1186/s12884-019-2232-8
8. Kawakita T, Reddy UM, Huang CC, et al. Predicting vaginal delivery in nulliparous women undergoing induction of labor at term. Am J Perinatol. 2018;35:660–668. doi:10.1055/s-0037-1608847
9. Janssen PA, Stienen JJ, Brant R, et al. A predictive model for cesarean among low-risk nulliparous women in spontaneous labor at hospital admission. Birth. 2017;44:21–28. doi:10.1111/birt.12257
10. Yang JM, Hyett JA, Mcgeechan K, et al. Is ultrasound measured fetal biometry predictive of intrapartum caesarean section for failure to progress? Aust N Z J Obstet Gynaecol. 2018;58:620–628. doi:10.1111/ajo.12776
11. Yang Y. An intrapartum calculator for predicting cesarean birth due to dystocia: preliminary findings from a single-center study in Korea. Birth. 2022;49:628–636. doi:10.1111/birt.12629
12. Mateus J, Stevens DR, Grantz KL, et al. Fetal and maternal factors predictive of primary cesarean delivery at term in a low-risk population: NICHD fetal growth studies-singletons. Am J Perinatol. 2025;42:256–267. doi:10.1055/s-0044-1788274
13. Li J, Lou Y, Chen C, et al. Predictive value of MRI pelvimetry in vaginal delivery and its practicability in prolonged labour-a prospective cohort study. J Clin Med. 2023;12:442. doi:10.3390/jcm12020442
14. Liao KD, Yu YH, Li YG, et al. Three-dimensional magnetic resonance pelvimetry: a new technique for evaluating the female pelvis in pregnancy. Eur J Radiol. 2018;102:208–212. doi:10.1016/j.ejrad.2018.03.024
15. Shimaoka R, Takahashi Y, Ono H, et al. Magnetic resonance imaging pelvimetric measurements as predictors for emergent cesarean delivery in obstructed labor. Eur J Obstet Gynecol Reprod Biol X. 2023;19:100216. doi:10.1016/j.eurox.2023.100216
16. Dlock FP, Harrist RB, Sharman RS, et al. Estimation of fetal weight with the use of head, body, and femur measurements--a prospective study. Am J Obstet Gynecol. 1985;151:333–337. doi:10.1016/0002-9378(85)90298-4
17. Nizard J, Haberman S, Paltieli Y, et al. How reliable is the determination of cervical dilation? Comparison of vaginal examination with spatial position-tracking ruler. Am J Obstet Gynecol. 2009;200:402.e1–4. doi:10.1016/j.ajog.2009.01.002
18. Haberman S, Paltieli Y, Gonen R, et al. Association between ultrasound-based assessment of fetal head station and clinically assessed cervical dilatation. Ultrasound Obstet Gynecol. 2011;37:709–711. doi:10.1002/uog.8875
19. Nizard J, Haberman S, Paltieli Y, et al. Determination of fetal head station and position during labor: a new technique that combines ultrasound and a position-tracking system. Am J Obstet Gynecol. 2009;200:404.e1–5. doi:10.1016/j.ajog.2008.10.051
20. Zhou ZR, Wang WW, Li Y, et al. In-depth mining of clinical data: the construction of clinical prediction model with R. Ann Transl Med. 2019;7:796. doi:10.21037/atm.2019.08.63
21. Zhang Z, Rousson V, Lee WC, et al. Decision curve analysis: a technical note. Ann Transl Med. 2018;6:308. doi:10.21037/atm.2018.07.02
22. Vickers AJ, van Calster B, Steyerberg EW. A simple, step-by-step guide to interpreting decision curve analysis. Diagn Progn Res. 2019;3:18. doi:10.1186/s41512-019-0064-7
23. Rossi RM, Requarth E, Warshak CR, et al. Risk calculator to predict cesarean delivery among women undergoing induction of labor. Obstet Gynecol. 2020;135:559–568. doi:10.1097/AOG.0000000000003696
24. Riley RD, Ensor J, Snell KIE, et al. Calculating the sample size required for developing a clinical prediction model. BMJ. 2020;368:m441. doi:10.1136/bmj.m441
25. Bahadori F, Ayatollahi H, Naghavi-Behzad M, et al. Predicting factors on cervical ripening and response to induction in women pregnant over 37 weeks. Med Ultrason. 2013;15:191–198. doi:10.11152/mu.2013.2066.153.fb1ha2
26. Zhao X, Yang L, Peng J, et al. A predicting model for intrapartum cesarean delivery at admission using a nomogram: a retrospective cohort study in China. BMC Pregnancy Childbirth. 2025;25:164. doi:10.1186/s12884-025-07280-1
27. Ami O, Maran JC, Gabor P, et al. Three-dimensional magnetic resonance imaging of fetal head molding and brain shape changes during the second stage of labor. PLoS One. 2019;14:e0215721. doi:10.1371/journal.pone.0215721
28. Vitner D, Paltieli Y, Haberman S, et al. Prospective multicenter study of ultrasound-based measurements of fetal head station and position throughout labor. Ultrasound Obstet Gynecol. 2015;46:611–615. doi:10.1002/uog.14821
29. Luca AM, Carvalho JCA, Ramachandran N, et al. The effect of morbid obesity or advanced maternal age on oxytocin-induced myometrial contractions: an in vitro study. Can J Anaesth. 2020;67:836–846. doi:10.1007/s12630-020-01615-6
30. Levine LD, Downes KL, Parry S, et al. A validated calculator to estimate risk of cesarean after an induction of labor with an unfavorable cervix. Am J Obstet Gynecol. 2018;218:254.e1–254.e7. doi:10.1016/j.ajog.2017.11.603
31. Zhou H, Gu N, Yang Y, et al. Nomogram predicting cesarean delivery undergoing induction of labor among high-risk nulliparous women at term: a retrospective study. BMC Pregnancy Childbirth. 2022;22:55. doi:10.1186/s12884-022-04386-8
32. Joyce DN, Giwa-Osagie F, Stevenson GW. Role of pelvimetry in active management of labour. Br Med J. 1975;4:505–507. doi:10.1136/bmj.4.5995.505
33. Gleason RL, Yigeremu M, Debebe T, et al. A safe, low-cost, easy-to-use 3D camera platform to assess risk of obstructed labor due to cephalopelvic disproportion. PLoS One. 2018;13:e0203865. doi:10.1371/journal.pone.0203865
34. Chen C, Yang M, Zheng W, et al. Magnetic resonance imaging-based nomogram to antenatal predict cesarean delivery for cephalopelvic disproportion in primiparous women. J Magn Reson Imaging. 2022;56:1145–1154. doi:10.1002/jmri.28164
35. Vardo JH, Thornburg LL, Glantz JC. Maternal and neonatal morbidity among nulliparous women undergoing elective induction of labor. J Reprod Med. 2011;56:25–30.
36. Dunne C, Da Silva O, Schmidt G, et al. Outcomes of elective labour induction and elective caesarean section in low-risk pregnancies between 37 and 41 weeks’ gestation. J Obstet Gynaecol Can. 2009;31:1124–1130. doi:10.1016/S1701-2163(16)34372-9
37. Uvnäs-Moberg K. The physiology and pharmacology of oxytocin in labor and in the peripartum period. Am J Obstet Gynecol. 2024;230:S740–S758. doi:10.1016/j.ajog.2023.04.011
38. Grobman WA, Rice MM, Reddy UM, et al. Labor induction versus expectant management in low-risk nulliparous women. N Engl J Med. 2018;379:513–523. doi:10.1056/NEJMoa1800566
39. Hong J, Atkinson J, Roddy Mitchell A, et al. Comparison of maternal labor-related complications and neonatal outcomes following elective induction of labor at 39 weeks of gestation vs expectant management: a systematic review and meta-analysis. JAMA Network Open. 2023;6:e2313162. doi:10.1001/jamanetworkopen.2023.13162
40. Wright A, Nassar AH, Visser G, et al. FIGO good clinical practice paper: management of the second stage of labor. Int J Gynaecol Obstet. 2021;152:172–181. doi:10.1002/ijgo.13552
41. American College of Obstetricians and Gynecologists. First and second stage labor management: ACOG Clinical Practice Guideline No. 8. Obstet Gynecol. 2024;143(1):144–162. doi:10.1097/AOG.0000000000005447
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.