Back to Journals » International Journal of Women's Health » Volume 17
Nomogram-Based Prediction of Live Birth in GnRH Antagonist Protocol Fresh IVF/ICSI Cycles
Authors Zhong Y, Kang Q, Pang X, Wang N
Received 24 March 2025
Accepted for publication 20 September 2025
Published 5 November 2025 Volume 2025:17 Pages 4143—4164
DOI https://doi.org/10.2147/IJWH.S525614
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Vinay Kumar
Yanyu Zhong,* Qian Kang,* Xin Pang,* Nan Wang
Department of Reproductive Medicine Center, The First Affiliated Hospital of Soochow University, Suzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Nan Wang, Department of Reproductive Medicine Center, The First Affiliated Hospital of Soochow University, No. 899, Pinghai Street, Gusu District, Suzhou, People’s Republic of China, Email [email protected]
Objective: This investigation sought to determine optimal prognostic indicators and develop an implementable predictive framework for estimating live birth probabilities in subfertile individuals receiving gonadotropin-releasing hormone antagonist-based ovarian stimulation during fresh embryo transfer cycles of assisted reproductive technology.
Methods: In this observational cohort analysis, we examined consecutive fresh in vitro fertilization/embryo transfer (IVF/ET) cycles utilizing GnRH antagonist protocols (training = 587, validation = 168 cycles; 2017– 2022). Live birth rate served as the principal outcome measure. Through multivariable regression modeling, we identified key predictive variables and constructed a visual prediction tool. Model robustness was assessed using ROC-AUC metrics and decision curve validation with 500 bootstrap iterations.
Results: The final predictive algorithm incorporated six clinical parameters: serum progesterone on post-ovulation day 9 (serum P (OPU+9) ≥ 51.4 ng/mL), transferred embryo count, progesterone–follicle ratio (PFR), triggering-day progesterone levels, progesterone-to-total follicle ratio, and creatinine concentrations. The training cohort demonstrated moderate discriminative capacity (ROC-AUC 0.72, 95% CI 0.68– 0.76), with enhanced performance in validation samples (AUC 0.81, 95% CI 0.73– 0.89). Decision curve evaluations confirmed the model’s clinical applicability.
Conclusion: Our prognostic scoring chart offers an accessible and practical clinical instrument for estimating reproductive success in GnRH antagonist-based IVF/ICSI cycles. This tool facilitates personalized treatment planning and therapeutic strategy optimization, potentially improving resource allocation in fertility care.
Keywords: reproductive outcomes prediction, IVF prognostic model, ovarian stimulation protocol, progesterone–follicular index, assisted reproduction technology
Introduction
According to the World Health Organization’s latest “Global Infertility Prevalence Estimates (1990–2021)” report, approximately 17.5% of adults worldwide—or one in six people—will experience infertility challenges during their lifetime.1 The evolution of assisted reproductive technologies (ART) has revolutionized treatment paradigms, enabling approximately 8 million ART-conceived births since 1978.2
Introduced in clinical practice since the 1990s, gonadotropin-releasing hormone (GnRH) antagonist protocols have transformed controlled ovarian stimulation through competitive inhibition of pituitary receptors. This mechanism achieves rapid, reversible suppression of gonadotropin release, effectively mitigating premature luteinizing hormone (LH) surges.3 Compared to traditional agonist protocols, antagonist regimens demonstrate clinical benefits including decreased gonadotropin consumption, abbreviated stimulation periods, and diminished ovarian hyperstimulation risks.4
Despite protocol optimizations, fresh cycle outcomes under antagonist regimens remain suboptimal relative to long agonist protocols, evidenced by reduced implantation and clinical pregnancy rates.4,5 Emerging evidence suggests these discrepancies stem primarily from endometrial receptivity alterations rather than embryological factors.6 While elective cryopreservation strategies mitigate some risks, deferred transfers introduce new challenges including escalated treatment costs, prolonged time-to-pregnancy, and elevated obstetrical risks such as placental adhesion disorders (OR 2.5) and hypertensive complications.7–9
This therapeutic dichotomy underscores the critical need for validated prognostic tools to optimize cycle selection.10–13 Current IVF prediction models lack integration of treatment-specific hormonal dynamics, particularly mid-luteal progesterone measurements in GnRH antagonist protocols. Our study addresses this gap by developing a multivariable predictive algorithm for live birth probability assessment in fresh antagonist cycles. Such stratification enables personalized clinical decision-making, potentially reducing unnecessary cryopreservation (current utilization >40% in some centers) while maintaining favorable neonatal outcomes. A nomogram translates regression output into an intuitive bedside point system, enabling cycle-specific counselling within 30 seconds.
Materials and Methods
Research Design & Population
This monocentric retrospective analysis was performed at a tertiary reproductive medicine center in Eastern China. The derivation cohort encompassed 587 initial ART cycles employing flexible antagonist-based ovarian stimulation protocols with fresh embryo transfers between July 2017 and October 2021. For temporal validation, an independent sample of 215 subsequent cycles (November 2021–December 2022) was analyzed. The training cohort consisted of 587 cycles, while the validation cohort included 168 cycles after applying exclusion criteria.
Sample Size Calculation
The sample size was calculated based on the Peduzzi rule, which stipulates a minimum of 10 events per predictor variable for logistic regression models. With six predictor variables progesterone on post-ovulation day 9 (serum P (OPU+9), number of embryos transferred, progesterone-to-follicle index (PFI), progesterone (P) at trigger, P/number of total follicles at trigger, and creatinine (Cr)), at least 60 live birth events were required. Given the live birth rate of 46.85% (275/587) in the training cohort, the total sample size of 587 significantly exceeded the minimum requirement (60/0.4685≈128). Additionally, the validation cohort included 168 patients, representing 22% of the total sample, which aligns with the recommended range (20–30%) to ensure external validity. Thus, the sample size was deemed adequate for model development and validation.
Data Collection
Clinical data acquisition involved retrospective mining of anonymized EMRs (electronic medical records) from our center’s reproductive treatment database, adhering to institutional ethics committee regulations for secondary data analysis (Protocol ID: RE-2023-076). Research procedures strictly maintained original treatment protocols without therapeutic modifications.
Participant Selection Criteria
Eligibility Requirements
- Primary assisted reproduction attempts with fresh transfers
- Implementation of flexible GnRH antagonist regimens
- Comprehensive cycle documentation (≥80% completeness)
Exclusionary Conditions
- Sperm donation cycles;
- Surgical sperm retrieval cycles;
- Chromosomal abnormalities in either partner;
- Incomplete medical records.
Study Flow & Outcomes
The analytical sample comprised 587 derivation cases and 168 temporal validation cases (Figure 1), representing consecutive treatment cycles meeting inclusion criteria. Clinical pregnancy confirmation occurred in 308 cases, translating to a per-transfer clinical pregnancy rate of 52.47%. Subsequent reproductive outcomes demonstrated 275 live birth events, corresponding to a 46.85% live birth rate per embryo transfer. Early pregnancy discontinuation was observed in 24 instances, representing a 4.01% preclinical loss rate. Notably, nine cycles (1.53%) were complicated by ectopic implantation.
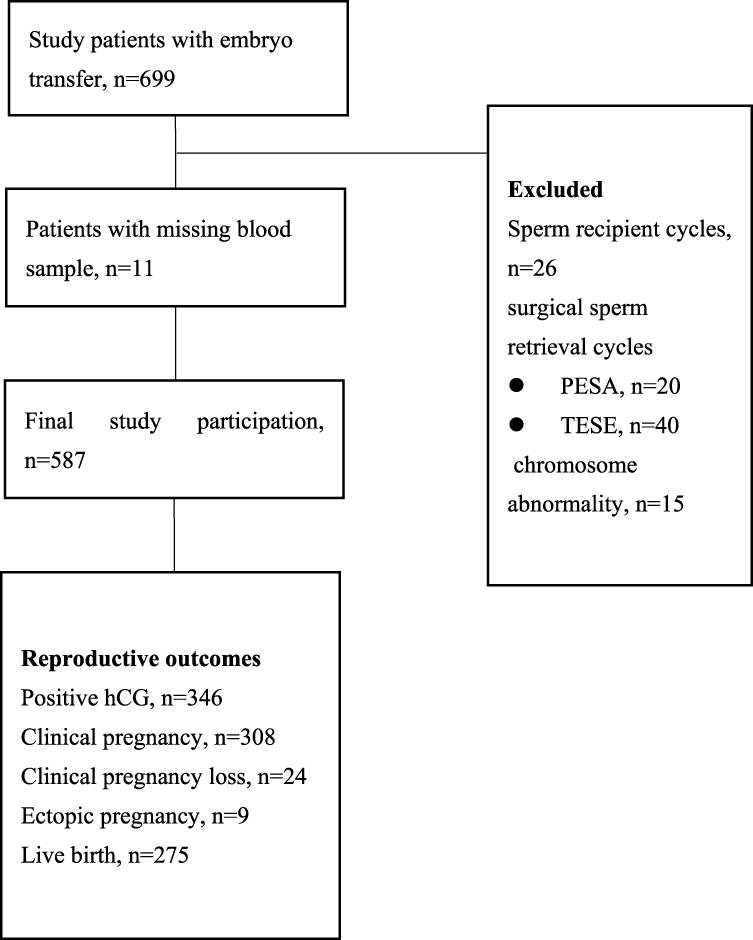 |
Figure 1 Flowchart of study participation. Abbreviations: PESA, Percutaneous Epididymal Sperm Aspiration; TESE, Testicular Sperm Extraction; HCG, human chorionic gonadotropin. |
Outcome metrics were calculated per initiated embryo transfer cycle in accordance with International Committee for Monitoring Assisted Reproductive Technologies reporting standards. Early pregnancy loss required both biochemical evidence (serum beta-human chorionic gonadotropin (β-hCG) decline >50% from peak) and ultrasonographic confirmation of non-viability prior to 12 weeks’ gestation.
Etiological stratification of infertility followed ASRM classification guidelines, encompassing seven distinct categories:
- Ovarian pathophysiology (diminished reserve/anovulation)
- Fallopian tube obstruction/hydrosalpinx
- Confirmed endometriosis (ASRM stage I–IV)
- Andrological abnormalities (oligo/astheno/teratozoospermia)
- Uterine anomalies (congenital/acquired)
- Idiopathic infertility (diagnosis of exclusion)
- Multifactorial etiologies
Patient Information and Data Collection
Demographic parameters encompassing chronological age and infertility duration were self-reported by participants. Clinical specialists systematically documented treatment-related metrics including endocrine profiles (follicle-stimulating hormone (FSH)/luteinizing hormone (LH)/estradiol (E2)), serological biomarkers (anti-Müllerian hormone (AMH)/thyroid-stimulating hormone (TSH)), controlled ovarian stimulation parameters, and quantitative reproductive outcomes (oocyte yield/viable embryo counts).
GnRH Antagonist Protocol
Controlled ovarian hyperstimulation was initiated on menstrual cycle day 2 using recombinant FSH (rFSH; Gonal-F®, Merck Serono) with dose individualization (75–300 IU/d) guided by anthropometric parameters (weight/BMI) and ovarian reserve markers (antral follicle count [AFC]/AMH). GnRH antagonist supplementation (Cetrotide® 0.125–0.25 mg/d) commenced upon dominant follicle maturation (≥14 mm mean diameter), with dosage titration contingent upon serial LH monitoring and follicular growth kinetics.
Dual trigger strategy implementation followed ASRM guidelines:
- Standard protocol: r-hCG 250 μg (Ovidrel®)
- High OHSS risk: GnRH agonist 0.2 mg (Daflin®) + hCG 2000 IU
- Severe OHSS risk (≥20 follicles ≥11 mm): Agonist-only trigger with cycle cancellation
Transvaginal oocyte retrieval (TVOR) was performed 36.5±0.5 hours post-trigger. Embryo transfer protocols adhered to ESHRE consensus standards:
- Cleavage-stage transfer (Day 3): ≤35 years with ≥1 grade A embryo
- Blastocyst transfer (Day 5): ≥35 years or suboptimal embryo quality
- Extended transfer (n=1): RIF cases with ≤2 fair-quality embryos
Protocol discontinuation thresholds included:
- Late follicular progesterone >2 ng/mL (≥P95 for cohort)
- Estradiol >5000 pg/mL with ≥25 follicles
- Emergent OHSS symptoms (abdominal ascites/hematocrit >45%)
Progesterone Administration
Pharmacological intervention began at oocyte retrieval, with standardized regimens continuing through gestational week 8–10, then followed by a stepwise withdrawal protocol. All participants received dual-phase endometrial support, including progesterone supplementation with Crinone® 8% gel (90 mg/d intravaginally) and oral dydrogesterone (40 mg/d; Duphaston®), as well as estradiol support with oral estradiol valerate (4 mg/d; Progynova®) starting on embryo transfer day. Serial serum analyses were performed at defined intervals for endocrine monitoring, including quantitative P/E2 assessment on post-ovulation day 9 and secondary hormonal profiling on post-ovulation day 17.
Hormone Assays
Phlebotomy procedures were standardized during morning hours (07:00–08:00) under ambient conditions. Automated chemiluminescent immunoassays (CLIA) were performed using a Beckman DXI800 platform within 120 minutes post-collection, adhering to CLSI EP17-A2 guidelines. Certified laboratory personnel conducted all analyses, with pre-analytical dilution protocols ensuring measurement accuracy for hyperconcentrated specimens through serial dilution with manufacturer-provided matrix solution.
Estradiol quantification demonstrated linearity across 15–5200 pg/mL (55.1–19,089 pmol/L) with intra/inter-assay precision <10% and <15%, respectively. Progesterone detection spanned 0.1–40 ng/mL (0.32–127.2 nmol/L) maintaining intra/inter-assay CVs below 7.25% and 6.59%. Method validation confirmed assay robustness through dilutional linearity testing (R²>0.98). Serum creatinine was quantified by an enzymatic colorimetric assay (Beckman AU5821, coefficient of variation < 3%).
Embryological Assessment Protocol
Embryo morphological evaluation followed international consensus criteria: for cleavage-stage, the Istanbul Consensus Criteria (ICC) were applied;14 for blastocyst-stage, the Gardner Grading System (GGS) was used. Top-tier embryos (Grades I–II) had ≤10% fragmentation and symmetrical blastomere configuration (Peter classification system).
Reproductive outcomes were defined as follows: biochemical pregnancy was serum β-hCG ≥25 IU/L (Architect i2000SR) at 14/12 days post-cleavage/blastocyst transfer; clinical pregnancy was an intrauterine gestational sac with embryonic cardiac activity (TVUS at 4–5 weeks) per ESHRE criteria;11 spontaneous pregnancy loss was development cessation prior to 28 gestational weeks (WHO ICD-11); and live birth was neonatal survival ≥28 weeks with an Apgar score ≥4 at 5 minutes.
Pregnancy surveillance involved standardized telemedicine follow-up (biweekly until 12 weeks, monthly thereafter) with electronic medical record verification for data capture.
Outcome Metrics Specification
Outcome metrics were specified using WHO-recommended ART parameters.10 Primary efficacy was assessed by live birth rate (LBR), calculated as live births per 100 completed embryo transfers (live birth (LB)/embryo transfer (ET)%). Early pregnancy loss was defined as biochemical/clinical pregnancy termination before 12 gestational weeks per 100 initiated cycles (early pregnancy loss (EPL)/ET%)
All outcome determinations followed ICMART 2023 definitions.12 Live birth confirmation needed neonatal vitality documentation at ≥28 weeks. Pregnancy loss stratification was based on FIGO timing criteria.13 The TRIPOD guidelines were followed for transparent reporting of the prediction model.15
Statistical Methodology
Statistical analyses were performed using an integrated computational framework combining SPSS 23.0 and R 4.2.1, following TRIPOD guidelines.7
For variable screening, parametric t-tests or Mann–Whitney U-tests were used for continuous variables, depending on distribution normality (Shapiro–Wilk p<0.05). Categorical variables were analyzed using χ²-tests with Yates’ correction or Fisher’s exact tests when expected cell counts were below 5.
Predictive modeling involved univariate logistic regression (p<0.10 entry criterion), followed by multivariable optimization through stepwise selection using the Akaike Information Criterion (ΔAIC >2). Internal validation was conducted via bootstrap resampling (500 iterations).
Model performance was assessed using ROC-AUC for discrimination, Brier score and calibration slope for calibration, and decision curve analysis (DCA) for clinical utility.
All analyses were implemented through EmpowerStats 3.0 with Monte Carlo simulations for sensitivity testing, maintaining statistical significance at α=0.05 (two-tailed).
Results
Demographic and Clinical Characteristics
The baseline demographic profile of the study cohort is comprehensively outlined in Table 1. Numeric parameters are reported as mean values with corresponding standard deviations, whereas categorical measures are quantitatively represented through frequency distribution analyses. This dual approach ensures appropriate characterization of both continuous and discrete variables in accordance with STROBE reporting guidelines for observational studies. The demographic and clinical characteristics showed no significant differences between training and validation cohorts, supporting the validity of temporal validation.
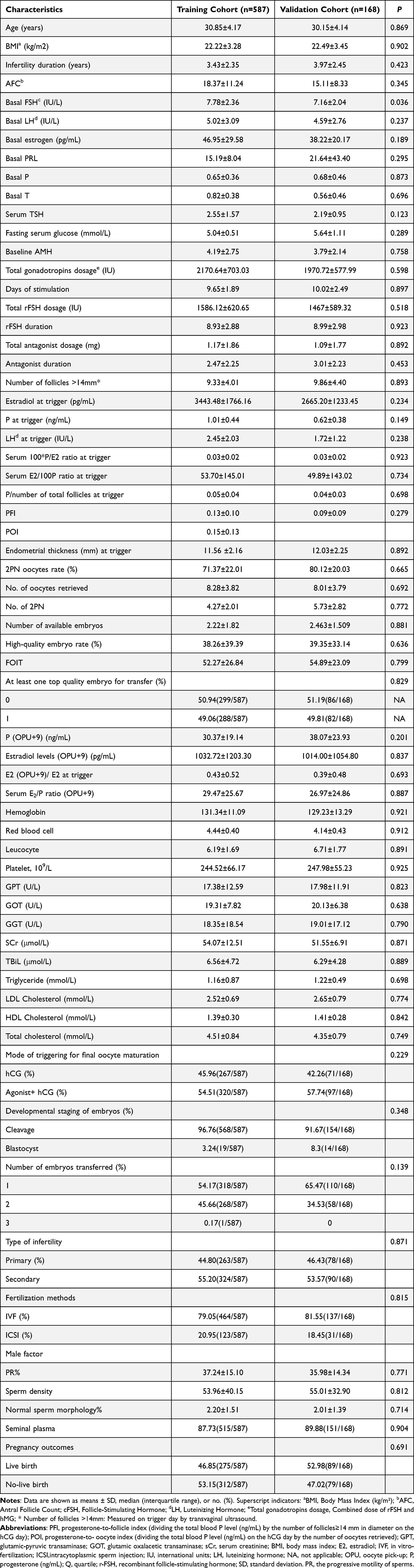 |
Table 1 Characteristics of the Training and Validation Cohorts |
Univariate Analysis of Factors Influencing Live Birth
Univariate analysis identified several factors associated with an increased likelihood of live birth. These included higher basal FSH levels, lower basal estradiol levels, lower progesterone levels at trigger, lower PFI and progesterone-to-oocyte index (POI) at trigger, higher numbers of 2PN oocytes and 2PN oocyte rates, a greater number of available embryos, higher high-quality embryo rates, elevated P and E2 levels 6 days after embryo transfer (ET), a higher ratio of E2 levels 6 days post-ET to E2 at trigger, increased low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C) levels, the transfer of top-quality embryos, and a higher number of embryos transferred (Table 2).
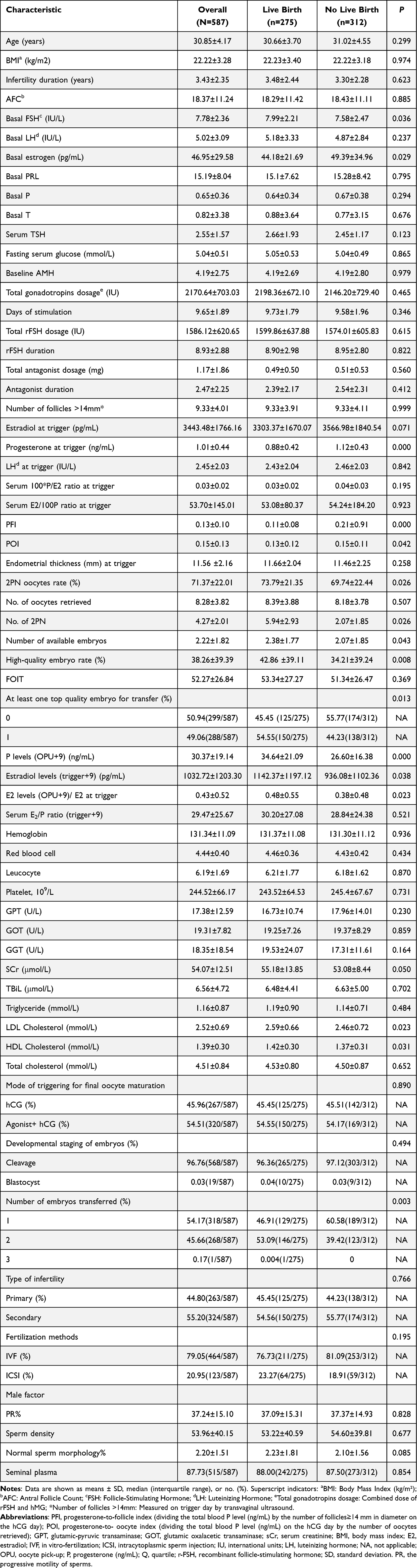 |
Table 2 The Baseline Characteristics and Ovarian Stimulation Data of Case (Women with Live Birth) and Control Groups in the Training Cohort (N = 587) |
Multivariable Regression Analysis
Multivariable unconditional logistic regression analysis was conducted with live birth as the dependent variable. The final model included the following predictors: P (OPU+9), number of embryos transferred, PFI, P at trigger, and serum creatinine (Cr) (Table 3).
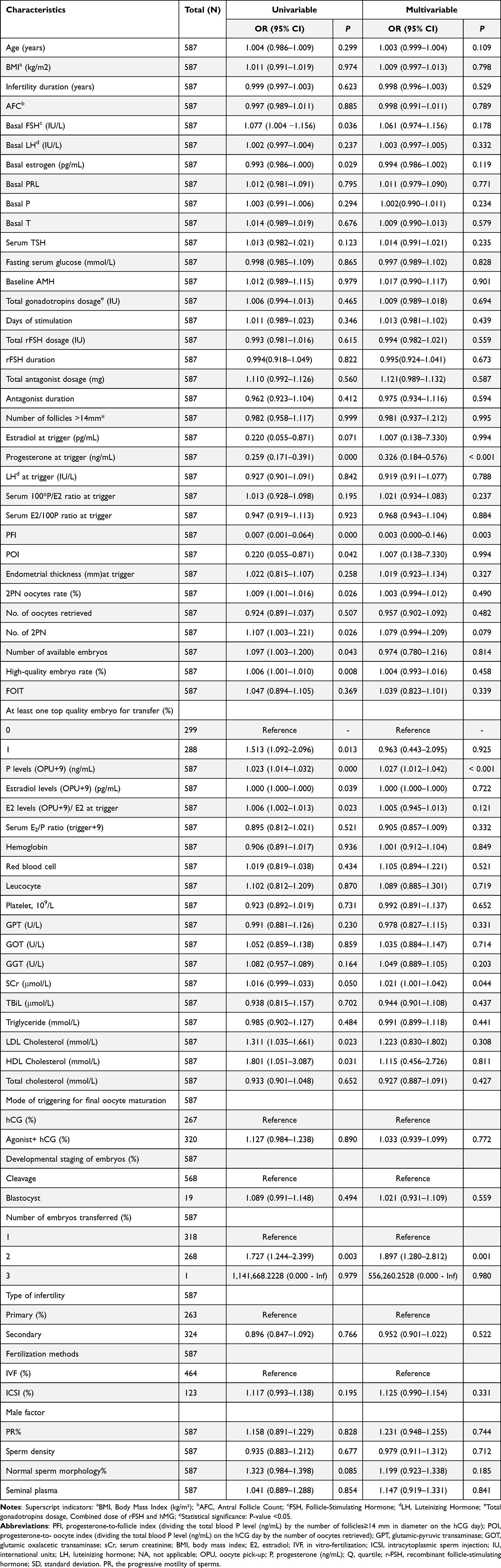 |
Table 3 The Univariate and Multivariable Logistic Regression Analysis for Factors Associated with Live Birth in the Training Cohort |
Development of a Nomogram for Predicting Clinical Outcomes
A multivariable prognostic algorithm was developed via stepwise regression to estimate reproductive success likelihood in fresh embryo transfer cycles. This visual prediction tool incorporated six key biomarkers: post-ovulatory progesterone levels (quantified on Day OPU+9), embryological transfer parameters (quantity), progesterone-to-follicle index (PFI), trigger-phase hormonal dynamics (absolute progesterone), follicular progesterone density (progesterone/total follicle ratio), and renal function marker (serum creatinine concentration).
The finalized model architecture, schematically presented in Figure 2, showed variable weighting through scaled point allocation. Internal validation using bootstrapping (500 iterations) confirmed the model’s stability across subsamples.
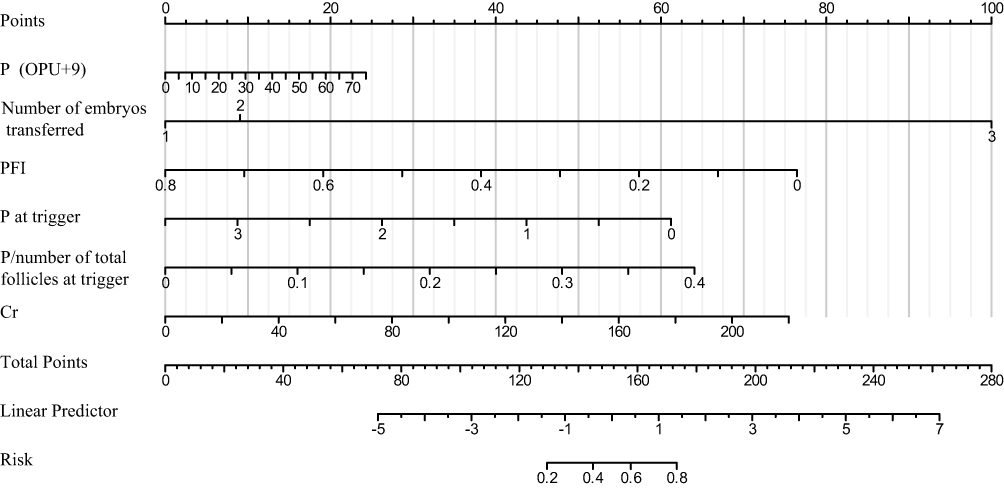 |
Figure 2 Nomogram to predict the probability of live birth for fresh IVF/ICSI patients. The nomogram incorporates six predictive variables identified through multivariable analysis: P (OPU+9), number of embryos transferred, PFI, P at trigger, P/number of total follicles at trigger, and Cr. To use the nomogram: (1) locate the patient’s value for each variable on its corresponding axis, (2) draw a vertical line up to the Points axis to determine the points for that variable, (3) sum all points from the six variables to obtain the Total Points, (4) draw a vertical line down from the Total Points to the Linear Predictor scale, and (5) from the Linear Predictor, determine the corresponding Risk (probability of live birth). Abbreviations: PFI, progesterone-to-follicle index; OPU, oocyte pick-up; P, progesterone (ng/mL); Cr, creatinine (μmol/L). |
Model Performance and Validation
The likelihood ratio test statistic for the model was 95.485, with a C-index of 0.72 (95% CI: 0.68–0.76; P < 0.001), indicating strong predictive accuracy. The goodness-of-fit test yielded a statistic of 10.118 (P = 0.257), suggesting no significant discrepancy between observed and predicted frequencies, thus confirming the model’s robustness.
The predictive accuracy of the nomogram was further validated using ROC curves (Figure 3) and a calibration curve (Figure 4), which demonstrated a strong correlation between predicted and observed outcomes, even at prediction probabilities below 20% (Table 4).
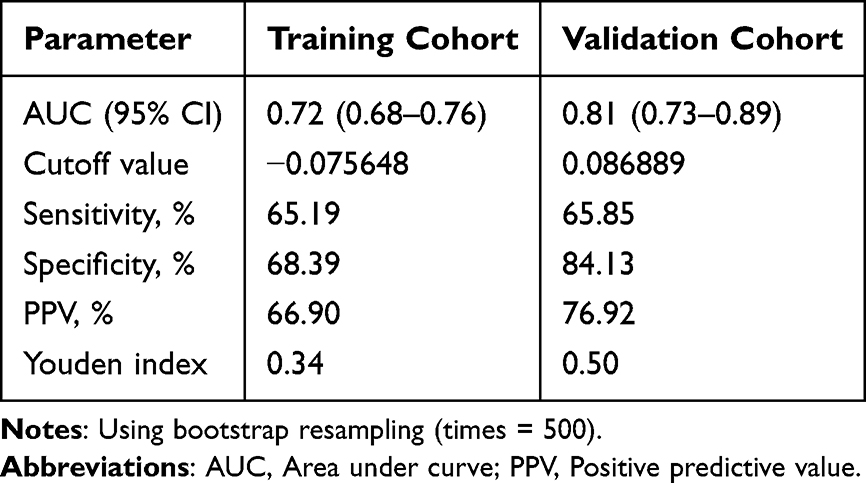 |
Table 4 Prediction Performance of the Nomogram for Estimating Live Birth |
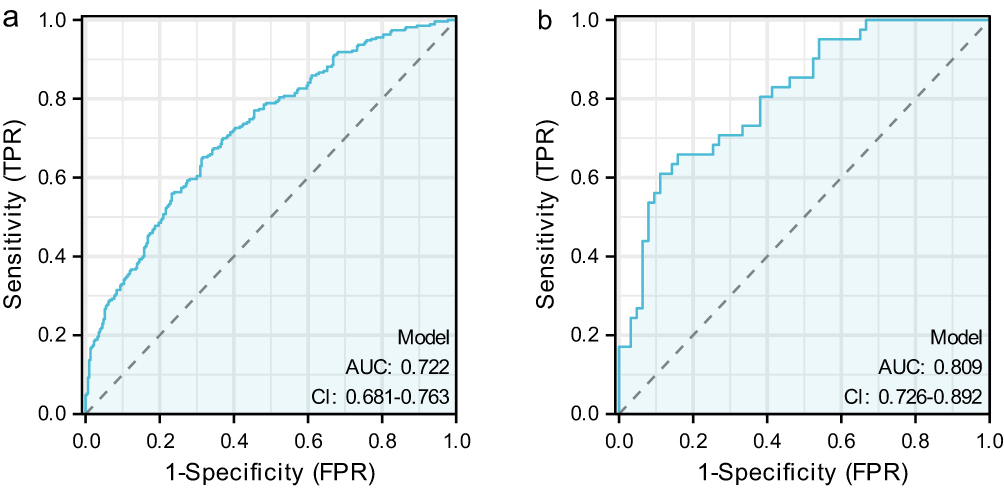 |
Figure 3 The ROC curves of the nomogram for probability of live birth for patients in the training cohort and validation cohort. a: In the training cohort, the AUC was 0.72 (0.68–0.76), b: In the validation cohort, the AUC was 0.81 (0.73–0.89). The curves demonstrate good discrimination ability with improved performance in the validation cohort. |
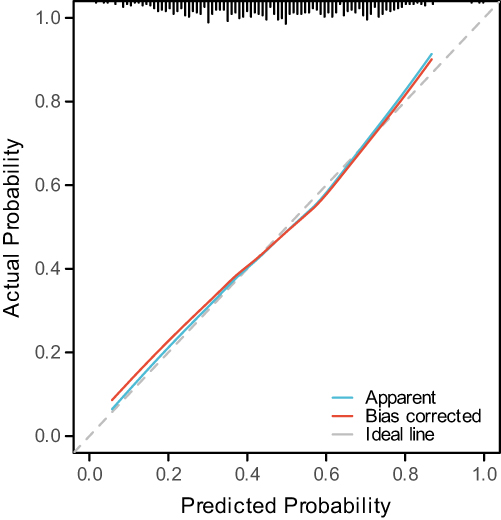 |
Figure 4 Calibration curve. The calibration plot shows good agreement between predicted probabilities (x-axis) and observed outcomes (y-axis). The diagonal line represents perfect calibration, and the proximity of the actual calibration curve to this line indicates excellent model calibration across the range of predicted probabilities. |
Internal Validation and Optimal Cutoff Values
The model underwent internal validation through 500 bootstrap resampling iterations. Within the training dataset, the nomogram demonstrated an optimal threshold of −0.075648, achieving a sensitivity of 65.19% and specificity of 68.39%. When applied to the validation dataset, these metrics improved to 65.85% and 84.13%, respectively. The ROC curve analysis revealed an AUC of 0.72 (95% confidence interval: 0.68–0.76) for the training set, while the validation set showed enhanced discrimination with an AUC of 0.81 (95% confidence interval: 0.73–0.89), demonstrating robust and stable predictive accuracy across both cohorts (Table 4). The validation set contained proportionally fewer borderline-probability cases, leading to a higher specificity at the same cutoff.
Optimal Cutoff Values for Predictive Factors
ROC analysis determined the optimal cutoff values for key predictors of live birth in fresh cycles (Figure 5). These included P (OPU+9) at 51.4 ng/mL, number of embryos transferred at 1.5, PFI at 0.073, P at trigger at 1.06 ng/mL, P/number of total follicles at trigger at 0.073, and serum creatinine (SCr) at 58.3 μmol/L (Table 5).
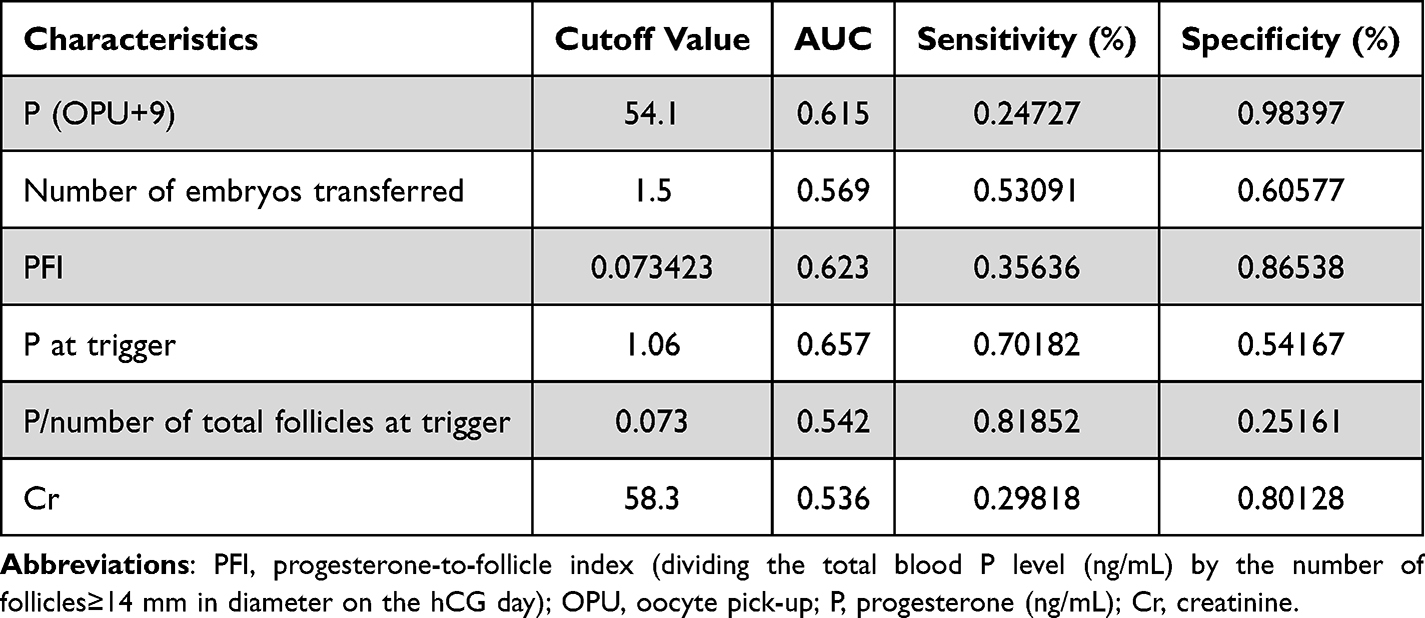 |
Table 5 Optimal Cutoff Values of Related Factors for Live Birth Prediction |
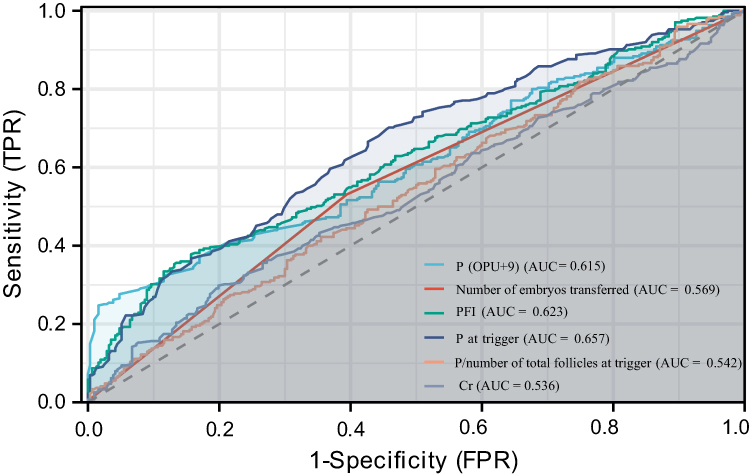 |
Figure 5 The ROC curves of each related factor. Individual ROC curves for each predictor variable demonstrate their independent discriminative abilities. P (OPU+9) shows the highest individual AUC among the continuous variables, supporting its importance in the multivariable model. |
Discussion
This investigation, designed as a retrospective analysis, sought to determine the key predictors affecting live birth outcomes in fresh IVF/ICSI cycles employing the GnRH antagonist protocol. By developing a predictive model, we sought to help clinicians identify patients who are most likely to benefit from fresh embryo transfer, thereby avoiding unnecessary freeze-all cycles and reducing economic and time burdens. Additionally, the model could guide clinicians in adjusting luteal phase support and other treatment strategies to optimize clinical outcomes. The baseline demographic profile of the study cohort demonstrates typical characteristics of subfertile populations undergoing ART. The mean age of 30.85±4.17 years reflects contemporary trends in delayed childbearing, while the infertility duration of 3.43±2.35 years indicates appropriate timing for ART intervention. The comparable characteristics between training and validation cohorts strengthen the external validity of our findings.
The study revealed that P (OPU+9) and the quantity of transferred embryos showed a positive association with live birth rates. Conversely, factors such as the progesterone-to-follicle index (PFI), progesterone levels at trigger, the ratio of progesterone to total follicles at trigger, and creatinine (Cr) levels demonstrated an inverse relationship with live birth outcomes. These findings imply that increased progesterone concentrations in the late follicular phase might impair endometrial receptivity, whereas sufficient progesterone during the luteal phase is essential for effective implantation and sustaining pregnancy.
Progesterone in the late follicular phase plays a critical role in advancing the endometrium from the proliferative to the secretory phase, thereby preparing it for embryo implantation. The impact of heightened progesterone levels on the day of hCG administration on live birth rates remains a contentious topic, with ongoing debates and no definitive agreement on its influence on clinical pregnancy and live birth outcomes.
Current literature demonstrates significant heterogeneity regarding the correlation between luteal progesterone levels and reproductive outcomes: while some studies confirm a negative association between elevated progesterone and pregnancy rates,9,16 others suggest a beneficial effect in specific populations, particularly hyper-responders.17 This discrepancy may stem from the variability in diagnostic thresholds, as no universal progesterone cutoff has been established.
Recent studies emphasize the critical role of ovarian response stratification in determining progesterone thresholds. Poor responders undergoing intensive stimulation protocols exhibit significantly inferior reproductive outcomes in fresh cycles compared to normal and high responders.18 Xu et al further proposed a dynamic threshold model: progesterone cutoffs on hCG day increased with ovarian response—1.5 ng/mL for poor responders, 1.75 ng/mL for intermediate responders, and 2.25 ng/mL for high responders. Exceeding these thresholds was associated with a 42–58% reduction in ongoing pregnancy rates.19
Our analytical outcomes demonstrate substantial concordance with existing evidence. Initial univariate assessment revealed a significant inverse correlation between progesterone elevation and reproductive success metrics. However, advanced multivariable modeling identified the trigger-day progesterone-to-follicle index (PFI) as a superior prognostic indicator for live birth outcomes in GnRH antagonist-based fresh IVF/ICSI cycles, surpassing the predictive utility of isolated progesterone measurements.
These findings align with existing evidence demonstrating that cycles maintaining progesterone-to-oocyte index (POI) <0.15 achieved significantly enhanced pregnancy rates (35.3% vs 18.8%, p=0.001) without compromising fertilization or cleavage parameters.20 Aflatoonian’s multicenter analysis of 378 cycles across diverse stimulation protocols further validated this association, reporting substantially improved implantation rates (28.5% vs 8.0%, p<0.0001) in cycles with POI <0.32.21 These consistent findings across different stimulation regimens suggest that progesterone-related indices may serve as universal predictors of reproductive success, independent of specific ovarian stimulation protocols.
Progesterone-to-follicle index (PFI) shows an inverse linear correlation with reproductive success. Contemporary evidence distinguishes etiological mechanisms: elevated late-phase progesterone exerts adverse clinical impact when driven by excessive per-follicular steroidogenesis (PFI ≥0.32), whereas equivalent progesterone levels from augmented follicular recruitment (≥20 mature follicles) have neutral prognostic implications.22
The negative prognostic value of hCG-day PFI in IVF outcomes is well documented, but the precise endocrine mechanisms remain unclear. Hypothesized pathways include dysregulation of endometrial steroidogenic enzymes, premature corpus luteum secretory patterns, and paracrine disruption of implantation window synchronization. This mechanistic ambiguity underscores the need for multi-omics investigations that integrate transcriptomic profiling of endometrial tissue with follicular fluid proteomic analyses.
Contemporary research consensus confirms that premature progesterone elevation during ovarian triggering predominantly impacts endometrial receptivity parameters rather than oocyte developmental competence.23 This pathophysiological mechanism is substantiated by transcriptomic analyses demonstrating significant alterations in endometrial receptivity biomarkers (HOXA10, integrin αvβ3) following premature progesterone surges (>1.5 ng/mL) during the follicular phase.24
The two-cell regulatory paradigm25 elucidates gonadotropin-mediated steroidogenesis: follicle-stimulating hormone (FSH) stimulates granulosa cell conversion of cholesterol to progesterone (P), while luteinizing hormone (LH) drives theca cell aromatization of P into androgens. Subsequent androgen transport to granulosa cells facilitates estradiol (E2) synthesis via cytochrome P450 aromatase activity (CYP19A1). Three main factors influence ovarian progesterone output during controlled ovarian hyperstimulation: follicular quantification, FSH stimulation intensity, and LH bioavailability. Follicular quantification is directly correlated with antral follicle count and total progesterone production. FSH stimulation intensity upregulates 3β-hydroxysteroid dehydrogenase activity in a dose-dependent manner. LH bioavailability modulates the efficiency of 17α-hydroxylase/C17-20 lyase conversion.26 This mechanistic framework predicts enhanced late-follicular P levels in high responders, evidenced by 62% higher P concentrations in patients with >15 oocytes retrieved compared to normal responders (p<0.01).27 Notably, high responders demonstrate compensatory mechanisms where superior embryo quality (blastocyst formation rate: 45.7% vs 32.1%) counterbalances P-mediated endometrial dyssynchrony, achieving comparable live birth rates (52.3% vs 48.9%, p=0.18).27
Post-ovulatory progesterone secretion is a crucial physiological regulator. It maintains myometrial quiescence by downregulating connexin-43, creating a stable uterine environment for pregnancy. Progesterone also boosts endometrial perfusion through VEGF-mediated angiogenesis, ensuring adequate nutrition for embryo implantation and development. Moreover, it induces maternal–fetal immunotolerance by modulating regulatory T-cells, preventing maternal immune rejection of the fetus and ensuring a smooth pregnancy. These functions highlight progesterone’s essential role in maintaining pregnancy.28,29 The GnRH agonist trigger protocol combined with follicular aspiration disrupts luteal steroidogenesis by removing granulosa-lutein cell mass, necessitating pharmacological progesterone supplementation. Quantitative analyses reveal mid-luteal progesterone thresholds for successful implantation in stimulated cycles (32.8 ± 4.1 ng/mL) significantly exceed natural cycle requirements (12.4 ± 2.7 ng/mL, p<0.001), reflecting iatrogenic luteal phase deficiency.30
While historical observations identified pathophysiological links between mid-luteal progesterone concentrations and conception success, with suboptimal progesterone levels (<10 ng/mL) potentially disrupting endometrial receptivity,31 the precise threshold for optimal reproductive outcomes in fresh embryo transfer cycles remains clinically undefined. This knowledge gap persists due to the absence of standardized luteal-phase monitoring protocols in routine assisted reproductive technology (ART) practice. Current ART protocols rarely incorporate systematic luteal-phase endocrine profiling, compounded by methodological inconsistencies in existing research—notably, temporal variability in serum sampling (48–120 hours post-transfer) and assay methodology discrepancies (chemiluminescence vs LC-MS/MS). Furthermore, the physiological complexity of iatrogenic luteal environments, characterized by supra-physiological steroid levels and disrupted corpus luteum function, challenges direct extrapolation of natural cycle progesterone thresholds to stimulated cycles. Emerging data suggest that individualized progesterone thresholds may vary by 30–45% depending on endometrial transcriptomic patterns and ovarian response profiles, necessitating advanced predictive modeling integrating hormonal kinetics with molecular biomarkers. Uniform mid-luteal sampling at 6–7 days post-ET remains difficult across centres; our web tool therefore allows the user to input the actual sampling time for dynamic calibration.
Existing studies are progressively uncovering the clinical threshold effects of luteal-phase progesterone levels in controlled ovarian stimulation. Yding Andersen’s team, through mechanistic research, has confirmed that to achieve optimal reproductive outcomes, mid-luteal progesterone levels during the stimulation cycle need to surpass a critical threshold of 80–100 nmol/L (23.4–29.2 ng/mL, conversion factor 0.292).32 This finding engages methodologically with conclusions from Thomsen et al’s large-scale prospective cohort study of 602 IVF cycles. Using multivariable regression analysis, Thomsen et al identified a serum progesterone window of 47–78 ng/mL (150–250 nmol/L) for optimal pregnancy rates, about 2.3 times higher than traditionally recognized, possibly reflecting endocrine features of modern high-responder populations.33 Notably, a third multicenter study, analyzing 1200 fresh embryo transfer cycles, proposed an optimal range of 41–60 ng/mL (140–205 nmol/L),34 showing significant consistency with this study’s empirical threshold of 51.4 ng/mL (176 nmol/L) (Bland-Altman limits of agreement ± 8.7 ng/mL). Differences may arise from patient population heterogeneity (eg, ovarian response and embryo quality) and standardization of testing time points (mid-luteal defined as 5–7 days post-embryo transfer), indicating the need for individualized luteal-phase progesterone monitoring.
There is ongoing academic debate regarding support treatment strategies for patients with mid-luteal progesterone deficiency. Aslih et al’s randomized controlled trial (n=320) showed that even with progesterone doses raised to 300 mg/day (double the routine dose), clinical pregnancy rates (38.2% vs 36.7%) and live-birth rates (29.1% vs 27.9%) did not improve statistically significantly (p>0.05).35 This challenges the effectiveness of the traditional empirical dose-escalation strategy, suggesting that simply upping the pharmacological dose may not reverse impaired endometrial receptivity. However, some studies advocate differentiated interventions. For patients with mid-luteal progesterone <10 ng/mL (31.4 nmol/L), combined use of exogenous progesterone (200 mg vaginal + 50 mg intramuscular) and low-dose hCG (1500 IU, q72h) can significantly boost luteal function indicators (progesterone level up by 82%, p<0.001) and improve ongoing pregnancy rates (41.3% vs 28.6%, OR 1.72).36 This conflicting evidence may stem from patient heterogeneity. High-responders, with fewer luteal cells due to excessive follicular fluid aspiration, may be more sensitive to hCG rescue therapy. In contrast, luteal defects in low-responders often come with endometrial gene expression abnormalities, requiring combined receptivity-modulation treatment. Current consensus suggests stratified management based on ovarian response type and dynamic progesterone monitoring to guide individualized dose adjustment.
This inconsistency may partly be explained by the fact that the window of implantation spans days 2–6 following OPU. It is possible that assessing P levels earlier in the implantation window (days 2–6) may be beneficial for adjustment of the optimal dosage. Inadequate P doses during that time and increasing P only at the mid-luteal point would be ineffective since the window would have already passed.37
Serum creatinine is a sensitive indicator of glomerular filtration function. Lower levels indicate good renal blood flow and metabolic status, which can reduce oxidative stress, improve uterine artery perfusion and luteal support, thereby increasing embryo implantation and live birth rates. Conversely, elevated creatinine suggests insufficient microcirculation perfusion and toxin retention, which weakens endocrine homeostasis and endometrial receptivity, hindering placental formation.38,39 Our multivariable model adjusted for key confounders including maternal age (OR 0.94, 95% CI 0.91–0.98) and BMI. However, the study population was predominantly Han Chinese from Eastern China, which may limit generalizability to other ethnic populations.
The live birth rates (LBRs) associated with double-embryo transfer (DET) are significantly higher than those of single-embryo transfer (SET) (54.28% versus 40.57%, p<0.05). However, the incidence of twin and multiple pregnancies also increases in DET cycles. Since 2015, our center has limited the number of embryos transferred to no more than two in an effort to reduce pregnancy complications related to multiple gestations, such as preeclampsia, preterm premature rupture of membranes, and cesarean delivery in mothers, as well as prematurity and low birth weight in infants. In our center, the multiple pregnancy rates for DET and SET cycles are 37.87% and 0.002%,40,41 respectively. Recent studies have identified independent predictors of dual embryo implantation in DET cycles through multivariable regression analysis: female age, endometrial thickness, number of high-quality embryos, and previous number of transfers.42 To optimize perinatal outcomes of assisted reproductive technology (ART), the American Society for Reproductive Medicine (ASRM) and the Society for Assisted Reproductive Technology (SART) have gradually established a system of guidelines for the number of embryo transfers since 2004,43 recommending elective single embryo transfer (eSET) for patients under 35 years old with a good prognosis. The indications include: (1) first IVF cycle or previous successful IVF pregnancy; (2) high-quality embryos as assessed by morphology; (3) availability of remaining high-quality embryos for cryopreservation.44 This shift in strategy reflects a paradigm shift in the field of ART from simply pursuing pregnancy rates to optimizing maternal and infant safety outcomes.
Before embryo transfer, clinicians should systematically evaluate and inform patients of the risk–benefit ratio of single embryo transfer (SET) and double embryo transfer (DET), with a focus on clarifying the probability of multiple pregnancies and their clinical impacts. By providing a detailed explanation of the dual risks of multiple pregnancies to both the mother (such as hypertensive disorders of pregnancy, postpartum hemorrhage, etc) and the fetus (such as preterm birth, low birth weight, etc), an evidence-based decision support system can be established. This patient-centered counseling model helps promote informed choice, enabling patients to autonomously decide on the transfer strategy based on individualized risk assessment results, thereby effectively reducing the rate of multiple pregnancies and related complications.
Conclusion
This study established and validated a prognostic algorithm for estimating live birth probability in GnRH antagonist-based fresh IVF/ICSI cycles. The model exhibited superior discriminative capacity (AUC 0.81, 95% CI 0.73–0.89), incorporating critical predictive variables including post-ovulatory progesterone levels (OPU+9), embryo transfer parameters, and progesterone-to-follicle ratio. This clinical decision-support tool enables individualized outcome prediction, facilitating optimized treatment strategy formulation while minimizing unnecessary medical interventions. This nomogram has been developed into a web-based calculator for convenient bedside application. Future studies will validate and refine the model through multicenter prospective cohorts.
The retrospective design imposed certain methodological constraints, notably the exclusion of cycles with late follicular progesterone exceeding 2 ng/mL. Additionally, the therapeutic implications of luteal phase support in patients with mid-luteal progesterone deficiency remain to be elucidated. These clinically relevant questions have been incorporated into our prospective research framework, with randomized controlled trials planned to address late follicular progesterone threshold optimization, luteal phase support protocol efficacy, and individualized progesterone supplementation strategies.
Ethics Approval and Consent to Participate
Since the study used de-identified data, the research was exempted by the ethics committee of The First Affiliated Hospital of Soochow University. Due to the anonymized patient’s information, informed consent is waived with the approval of the ethics committee of The First Affiliated Hospital of Soochow University. We confirm that the research was performed in accordance with the principles stated in the Declaration of Helsinki.
Funding
There is no funding to report.
Disclosure
Yanyu Zhong, Qian Kang and Xin Pang are co-first authors for this study. All of the authors had no any personal, financial, commercial, or academic conflicts of interest separately for this work.
References
1. World Health Organization. Infertility Prevalence Estimates, 1990-2021. Geneva: WHO; 2023.
2. Mohajer N, Culty M. IMPACT OF REAL-LIFE ENVIRONMENTAL EXPOSURES ON REPRODUCTION: impact of human-relevant doses of endocrine-disrupting chemical and drug mixtures on testis development and function. Reproduction. 2025;169(1):e240155. doi:10.1530/REP-24-0155
3. Jing M, Lin C, Zhu W, et al. Cost-effectiveness analysis of GnRH-agonist long-protocol and GnRH-antagonist protocol for in vitro fertilization. Sci Rep. 2020;10(1):8732. doi:10.1038/s41598-020-65558-0
4. Zhang LJ, Liu D, Xu LQ, et al. Impact of luteinizing hormone on IVF/ICSI assisted reproduction on the initiation day of gonadotropin-releasing hormone antagonist protocol. Endocr Metab Immune Disord Drug Targets. 2024. doi:10.2174/0118715303281640240722070348
5. Liu C, Tian T, Lou Y, et al. Live birth rate of gonadotropin-releasing hormone antagonist versus luteal phase gonadotropin-releasing hormone agonist protocol in IVF/ICSI: a systematic review and meta-analysis. Expert Rev Mol Med. 2023;26:e2. doi:10.1017/erm.2023.25
6. Hsu CC, Hsu I, Dorjee S, Chen YC, Chen TN, Chuang YL. Ovarian sensitivity index affects clinical pregnancy and live birth rates in gonadotropin-releasing hormone agonist and antagonist in vitro fertilization cycles. Front Endocrinol. 2024;15:1457435. doi:10.3389/fendo.2024.1457435
7. Hesters L, Sermondade N, Lambert C, et al. Child health following IVF Collaborative Group members of BLEFCO. Is large for gestational age in singletons born after frozen embryo transfer associated with freezing technique or endometrial preparation protocol? A longitudinal national French study. Hum Reprod. 2024;39(4):724–732. doi:10.1093/humrep/deae027
8. He T, Shi W, Xue X, Shi J. Impact of blastocyst biopsy for preimplantation genetic testing on maternal and neonatal outcomes following single frozen embryo transfer cycles. BMC Pregnancy Childbirth. 2025;25(1):74. doi:10.1186/s12884-024-07107-5
9. Shokeir T, Abdelshaheed M. Retraction notice to “Sonohysterography as a first-line evaluation for uterine abnormalities in women with recurrent failed in vitro fertilization-embryo transfer” [Fertil Steril 91 (2008) 1321-1322]. Fertil Steril. 2022;117(2):466. doi:10.1016/j.fertnstert.2021.12.008
10. Zegers-Hochschild F, Adamson GD, Dyer S, et al. The international glossary on infertility and fertility care, 2017. Fertil Steril. 2017;108(3):393–406. doi:10.1016/j.fertnstert.2017.06.005
11. ESHRE Guideline Group on the Number of Embryos to Transfer, Alteri A, Arroyo G, Baccino G, et al. ESHRE guideline: number of embryos to transfer during IVF/ICSI. Hum Reprod. 2024;39(4):647–657.
12. Kupka MS, Chambers GM, Dyer S, et al. ICMART world report: assisted reproductive technology, 2015 & 2016. Fertil Steril. 2024. doi:10.1016/j.fertnstert.2024.07.009
13. Henry L, Berek JS, Diaz I, et al. FIGO statement: fertility preservation. Int J Gynecol Obstet. 2023;163:790–794. doi:10.1002/ijgo.15187
14. Balaban B, Brison D, Calderon G, et al. Alpha scientists in reproductive medicine; ESHRE SIG embryology. The istanbul consensus workshop on embryo assessment: proceedings of an expert meeting. Hum Reprod. 2011;26(6):1270–1283. doi:10.1093/humrep/der037
15. Collins GS, Reitsma JB, Altman DG, Moons KGM. Transparent reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): the TRIPOD statement. BMC Med. 2015;13:1. doi:10.1186/s12916-014-0241-z
16. Pitner I, Mikuš M, Šprem Goldštajn M, et al. Effects of different progesterone levels on reproductive outcomes in assisted reproductive technologies: from molecular basis to treatment strategies. Gynecol Endocrinol. 2023;39(1):2190806. doi:10.1080/09513590.2023.2190806
17. Tokgoz VY, Ekici GC, Tekin AB. The efficiency of progesterone/estradiol and progesterone/follicle ratio without elevated trigger-day progesterone levels on the reproductive outcomes of GnRH antagonist IVF/ICSI cycles. Gynecol Endocrinol. 2021;37(10):885–890. doi:10.1080/09513590.2021.1878137
18. Friis Wang N, Skouby SO, Humaidan P, Andersen CY. Response to ovulation trigger is correlated to late follicular phase progesterone levels: a hypothesis explaining reduced reproductive outcomes caused by increased late follicular progesterone rise. Hum Reprod. 2019;34(5):942–948. doi:10.1093/humrep/dez023
19. Xu B, Li Z, Zhang H, et al. Serum progesterone level effects on the outcome of in vitro fertilization in patients with different ovarian response: an analysis of more than 10,000 cycles. Fertil Steril. 2012;97(6):
20. Lin H, Huang X, Zhao Y, et al. Low-dose human chorionic gonadotropin supplementation initiated at the onset of ovarian stimulation can improve oocyte quality without impairing endometrial receptivity: case series. Medicine. 2022;101(48):e32175. doi:10.1097/MD.0000000000032175
21. Aflatoonian A, Davar R, Hojjat F. Elevated serum progesterone/ MII oocyte ratio on the day of human chorionic gonadotropin administration can predict impaired endometrial receptivity. Iran J Reprod Med. 2014;12(6):427–434.
22. Shufaro Y, Sapir O, Oron G, et al. Progesterone-to-follicle index is better correlated with in vitro fertilization cycle outcome than blood progesterone level. Fertil Steril. 2015;103(3):669–74.e3. doi:10.1016/j.fertnstert.2014.11.026
23. Kofinas JD, Mehr H, Ganguly N, et al. Is it the egg or the endometrium? Elevated progesterone on day of trigger is not associated with embryo ploidy nor decreased success rates in subsequent embryo transfer cycles. J Assist Reprod Genet. 2016;33(9):1169–1174. doi:10.1007/s10815-016-0752-y
24. Van Vaerenbergh I, Fatemi HM, Blockeel C, et al. Progesterone rise on HCG day in GnRH antagonist/rFSH stimulated cycles affects endometrial gene expression. Reprod Biomed Online. 2011;22(3):263–271. doi:10.1016/j.rbmo.2010.11.002
25. Moon YS, Tsang BK, Simpson C, Armstrong DT. 17 beta-Estradiol biosynthesis in cultured granulosa and thecal cells of human ovarian follicles: stimulation by follicle-stimulating hormone. J Clin Endocrinol Metab. 1978;47(2):263–267. doi:10.1210/jcem-47-2-263
26. Younis JS. The role of progesterone/estradiol ratio in exploring the mechanism of late follicular progesterone elevation in low ovarian reserve women. Med Hypotheses. 2019;125:126–128. doi:10.1016/j.mehy.2019.02.047
27. Nagaraja N, Talwar P, Mukherjee B, Chakrabarty BK. Correlation between serum progesterone level on the day of ovulation trigger during in vitro fertilization and its effect on treatment outcome. J Hum Reprod Sci. 2019;12(2):136–140. doi:10.4103/jhrs.JHRS_115_18
28. Labarta E, Rodríguez C. Progesterone use in assisted reproductive technology. Best Pract Res Clin Obstet Gynaecol. 2020;69:74–84. doi:10.1016/j.bpobgyn.2020.05.005
29. Kim YJ, Shin JH, Hur JY, Kim H, Ku SY, Suh CS. Predictive value of serum progesterone level on β-hCG check day in women with previous repeated miscarriages after in vitro fertilization. PLoS One. 2017;12(7):e0181229. doi:10.1371/journal.pone.0181229
30. Dilday E, Gigg M, Hoyos L, Quinn M, Markovic D, Kroener L. Luteal phase support with progesterone does not improve pregnancy rates in patients undergoing ovarian stimulation with letrozole. Reprod Biomed Online. 2023;46(1):123–128. doi:10.1016/j.rbmo.2022.09.012
31. Suthaporn S, Jayaprakasan K, Thornton J, et al. Suboptimal mid-luteal progesterone concentrations are associated with aberrant endometrial gene expression, potentially resulting in implantation failure. Reprod Biomed Online. 2021;42(3):595–608. doi:10.1016/j.rbmo.2020.10.018
32. Xu Z, Lin Q, Liang Z, et al. Optimising luteinising hormone levels on trigger day for improved ovarian response and pregnancy outcomes in gonadotropin-releasing hormone antagonist protocols: a retrospective cohort study. BJOG. 2025. doi:10.1111/1471-0528.18064
33. Thomsen LH, Kesmodel US, Erb K, et al. The impact of luteal serum progesterone levels on live birth rates-a prospective study of 602 IVF/ICSI cycles. Hum Reprod. 2018;33(8):1506–1516. doi:10.1093/humrep/dey226
34. Benmachiche A, Benbouhedja S, Zoghmar A, Al Humaidan PSH. The impact of preovulatory versus midluteal serum progesterone level on live birth rates during fresh embryo transfer. PLoS One. 2021;16(2):e0246440. doi:10.1371/journal.pone.0246440
35. Aslih N, Ellenbogen A, Shavit T, Michaeli M, Yakobi D, Shalom-Paz E. Can we alter pregnancy outcome by adjusting progesterone treatment at mid-luteal phase: a randomized controlled trial. Gynecol Endocrinol. 2017;33(8):602–606. doi:10.1080/09513590.2017.1298742
36. Lawrenz B, Coughlan C, Fatemi HM. Individualized luteal phase support. Curr Opin Obstet Gynecol. 2019;31(3):177–182. doi:10.1097/GCO.0000000000000530
37. Zhao J, Hao J, Li Y. Individualized luteal phase support after fresh embryo transfer: unanswered questions, a review. Reprod Health. 2022;19(1):19. doi:10.1186/s12978-021-01320-7
38. Cheung KL, Lafayette RA. Renal physiology of pregnancy. Adv Chronic Kidney Dis. 2013;20(3):209–214. doi:10.1053/j.ackd.2013.01.012
39. Kang J, Hwang S, Lee TS, et al. Gestational age-specific serum creatinine can predict adverse pregnancy outcomes. Sci Rep. 2022;12:11224. doi:10.1038/s41598-022-15450-w
40. Sazonova A, Källen K, Thurin-Kjellberg A, Wennerholm UB, Bergh C. Neonatal and maternal outcomes comparing women undergoing two in vitro fertilization (IVF) singleton pregnancies and women undergoing one IVF twin pregnancy. Fertil Steril. 2013;99(3):731–737. doi:10.1016/j.fertnstert.2012.11.023
41. Banker M, Dyer S, Chambers GM, et al. International Committee for Monitoring Assisted Reproductive Technologies (ICMART): world report on assisted reproductive technologies, 2013. Fertil Steril. 2021;116(3):741–756. doi:10.1016/j.fertnstert.2021.03.039
42. Huang X, Liu R, Shen W, et al. An elective single cleavage embryo transfer strategy to minimize twin live birth rate based on a prediction model from double cleavage embryos transfer patients. J Matern Fetal Neonatal Med. 2022;35(9):1775–1782. doi:10.1080/14767058.2020.1770215
43. Practice Committee. Society for assisted reproductive technology and the American society for reproductive medicine. Guidelines on the number of embryos transferred. Fertil Steril. 2004;82(3):773–774. doi:10.1016/j.fertnstert.2004.06.031
44. Practice Committee of the American Society for Reproductive Medicine and the Practice Committee for the Society for Assisted Reproductive Technologies. Electronic address: [email protected]. Guidance on the limits to the number of embryos to transfer: a committee opinion. Fertil Steril. 2021;116(3):651–654. doi:10.1016/j.fertnstert.2021.06.050
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Estradiol Decline Before hCG Administration in COH Has a Negative Effect on IVF Outcomes in Patients Without OC Pretreatment
Zhu Y, Zheng Z, Fan B, Sun Y, Zhai J, Du Y
International Journal of Women's Health 2024, 16:411-419
Published Date: 6 March 2024
Assisted Reproductive Technology Outcomes in Women with Normal Ovarian Response Receiving Recombinant Luteinizing Hormone/Human Menopausal Gonadotropin: An Observational Study
Liang Y, Hou X, Chen H, Yang R, Wang R, Mao R, Zhao J, Chen H, Cheng J
International Journal of Women's Health 2024, 16:1103-1111
Published Date: 14 June 2024