Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
NLR and PLR as Adjunctive Markers of MRI-Derived Vertebral Bone Quality in a Preoperative Lumbar Cohort
Authors Ma L, Liu Y, Qin Y, Liu Y, Yu H, Ma Z, Nan C
Received 10 July 2025
Accepted for publication 2 December 2025
Published 10 December 2025 Volume 2025:21 Pages 1679—1687
DOI https://doi.org/10.2147/TCRM.S552982
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Liang Ma,1 Yuxiu Liu,2 Yazhuo Qin,1 Yong Liu,1 Hetong Yu,1 Zhanbei Ma,1 Chong Nan1
1Department of Orthopedic, Baoding No. 1 Central Hospital, Baoding, Hebei, People’s Republic of China; 2Department of Western Pharmacy, Baoding No. 1 Central Hospital, Baoding, Hebei, People’s Republic of China
Correspondence: Chong Nan, Department of Orthopedic, Baoding No. 1 Central Hospital, Baoding, Hebei, People’s Republic of China, Email [email protected]
Background: MRI-derived vertebral bone quality (VBQ) rises with marrow fat and denotes poorer bone integrity. We examined whether simple inflammatory ratios—neutrophil-to-lymphocyte (NLR) and platelet-to-lymphocyte (PLR)—relate to VBQ in degenerative lumbar disease.
Methods: We retrospectively studied 200 patients aged ≥ 50 years who underwent surgery between January 2022 and January 2024. VBQ was calculated on mid-sagittal T1-weighted MRI using vertebral and cerebrospinal-fluid regions of interest. Associations were tested with Spearman correlations and multivariable linear regression adjusting for age, sex, smoking, diabetes, and body mass index (BMI).
Results: Among 200 patients (mean age = 64.8 ± 8.7 years), those with higher VBQ values (indicating poorer bone quality) were older and had higher NLR and PLR (all p< 0.001). VBQ showed significant positive correlations with age (ρ = 0.650), NLR (ρ = 0.534), and PLR (ρ = 0.452) (all p< 0.001). In multivariable regression, age, NLR, and PLR remained independently associated with higher VBQ, whereas BMI, sex, smoking, and diabetes were not significant (adjusted R2=0.520; all VIF≤ 2.26). Standardized effect sizes indicated moderate independent contributions (β_std = 0.151 for NLR; β_std = 0.303 for PLR), corresponding to roughly 0.020-unit and 0.075-unit increases in VBQ per 1-unit NLR and 50-unit PLR increments, respectively.
Conclusion: Preoperative NLR and PLR were independently associated with higher MRI-derived VBQ and may aid imaging-based risk stratification; prospective validation with calibrated thresholds is needed.
Keywords: vertebral bone quality, neutrophil-to-lymphocyte, platelet-to-lymphocyte, osteoporosis
Introduction
Vertebral bone quality (VBQ) is a quantitative parameter derived from magnetic resonance imaging (MRI), primarily used to assess bone health and screen for osteoporosis or low bone mineral density (BMD). The concept relies on the observation that increased marrow fat content, as visualized on T1-weighted images, correlates with reduced trabecular bone strength.1 Compared to dual-energy X-ray absorptiometry (DXA), VBQ offers a radiation-free alternative that can be extracted from routine preoperative MRI scans without the need for specialized imaging protocols. In patients undergoing lumbar spine surgery, VBQ has been utilized as an opportunistic marker for predicting postoperative complications such as vertebral compression fractures, cage subsidence, adjacent segment degeneration, and pedicle screw loosening.2–4 Prior studies have shown that VBQ is influenced by multiple variables, including bone density, age, sex, MRI acquisition settings, and paraspinal muscle condition.5,6 However, the association between systemic inflammatory response and VBQ score has rarely been investigated.
Emerging evidence suggests a complex interplay between systemic inflammatory responses and osteoporosis pathogenesis, with underlying mechanisms encompassing immune cell activation, sustained release of pro-inflammatory cytokines, and subsequent disruption of bone metabolism homeostasis.7–9 Inflammatory biomarkers have shown promise in identifying individuals at risk of bone loss, reflecting the biological interactions between chronic inflammation and bone metabolism. Among these markers, the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) have been widely investigated as accessible indicators of inflammatory burden. A recent meta-analysis confirmed that individuals with osteoporosis tend to exhibit significantly elevated levels of NLR and PLR compared to those with normal BMD.10
Although dual-energy X-ray absorptiometry (DXA) and CT-derived Hounsfield units (HU) are widely used to assess bone status, they primarily reflect (areal) mineral density, whereas MRI-derived vertebral bone quality (VBQ) captures marrow-fat–sensitive signal that may more directly reflect trabecular integrity. Despite growing interest in VBQ, evidence in degenerative lumbar disease—particularly in preoperative cohorts where time, access, and radiation considerations often limit DXA/CT—is limited. Moreover, most inflammation studies have focused on BMD or HU; to our knowledge, it remains unclear whether simple inflammatory ratios—neutrophil-to-lymphocyte (NLR) and platelet-to-lymphocyte (PLR)—relate to MRI-derived VBQ in this setting.
Therefore, we aimed to test whether higher preoperative NLR and PLR are associated with higher VBQ (poorer bone quality) in patients with degenerative lumbar disease, and to assess the independence of these associations after adjustment for clinical covariates. We hypothesized that both ratios would show positive, independent associations with VBQ and could serve as adjunctive markers when DXA is unavailable.
Materials and Methods
Patient Samples
We retrospectively reviewed patients who underwent lumbar spine surgery at Baoding No.1 Central Hospital between January 2022 and January 2024. This retrospective study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Baoding No.1 Central Hospital. All participants provided informed consent prior to inclusion in the study. Clinical trial registration number: not applicable.
Inclusion criteria were: (1) age ≥ 50 years; (2) diagnosis of degenerative lumbar disease (lumbar spinal stenosis, lumbar disc herniation, or spondylolisthesis); (3) elective lumbar spinal surgery (decompression or fusion) performed during the study period; (4) availability of preoperative lumbar MRI within 3 months suitable for VBQ scoring; (5) complete blood count obtained within 30 days before surgery; and (6) complete clinical, laboratory, and imaging data.
Exclusion criteria included: (1) prior lumbar surgery, spinal trauma, tumors, or infections; (2) acute infection, autoimmune disease, chronic inflammatory conditions, or hematological disorders; (3) malignancy history or ongoing cancer treatment; (4) recent use of corticosteroids and immunosuppressants within 6 months; (5) poor-quality MRI images precluding VBQ measurement; and (6) missing essential clinical or laboratory data.
This was a retrospective, consecutive cohort; no a priori sample-size calculation was performed. The cohort size reflects case availability within the study period and is adequate for the planned multivariable modeling (EPV >10–15), with stable estimates and consistent sensitivity-analysis results.
Data Collection
Demographic and clinical characteristics, including age, sex, body mass index (BMI), smoking status, hypertension, and diabetes mellitus, were extracted from electronic medical records. Preoperative laboratory parameters were obtained from blood tests performed within 30 days before surgery.
Vertebral Bone Quality (VBQ) Scoring
Lumbar MRI was performed on a GE Signa HDxt, 1.5-T system. The mid-sagittal T1-weighted fast spin-echo (FSE) sequence was used with the following parameters: repetition time (TR) 350 ms; echo time (TE) 13.6 ms (minimum full); echo train length 3; refocusing flip angle 160°; slice thickness 4.0 mm; interslice gap 1.0 mm; field of view (FOV) 280×280 mm2; acquisition matrix 288 × 192; in-plane resolution approximately 1.0×1.5 mm; receiver bandwidth 31.25 kHz (≈ 217 Hz/pixel); NEX 1.0; echo spacing 9.0 ms; total slices 11; phase FOV 1.00; fat saturation none. Images were exported in DICOM format for analysis.
VBQ was calculated on the mid-sagittal slice as the ratio of mean vertebral marrow signal to cerebrospinal fluid (CSF) signal. Circular regions of interest (ROIs) were placed within the anterior two-thirds of L1–L4 vertebral bodies, avoiding cortical endplates, focal venous channels, Schmorl nodes, Modic changes, or artifacts. Vertebral ROIs had an area of 264 mm2 (≈18.3 mm diameter), and two ROIs per vertebra were averaged to obtain the vertebral signal. A CSF ROI of 13 mm2 (≈4.1 mm diameter) was placed at the L3 level within the thecal sac, avoiding flow voids and partial-volume effects. VBQ was computed as (mean vertebral signal)/(CSF signal), with higher values indicating poorer bone quality (Figure 1).
 |
Figure 1 Workflow and ROI placement for VBQ assessment on mid-sagittal T1-weighted lumbar MRI. Yellow circles indicate vertebral ROIs positioned within the anterior two-thirds of L1–L4, with a reference ROI placed in the CSF at L3. VBQ was calculated as the mean vertebral signal intensity divided by the CSF signal, where higher values indicate poorer bone quality. Abbreviations: VBQ, vertebral bone quality; CSF, cerebrospinal fluid; ROI, region of interest. |
To ensure measurement reliability, two independent observers, both experienced radiologists blinded to clinical information, performed VBQ scoring. Interobserver reliability was evaluated by calculating the intraclass correlation coefficient (ICC) based on a random sample of 30 MRI scans. An ICC value greater than 0.80 was considered indicative of excellent agreement.
Statistical Analysis
Continuous variables were tested for normality using the Shapiro–Wilk test and are presented as mean ± standard deviation or median (interquartile range), as appropriate. Categorical variables are expressed as counts and percentages. Between-group comparisons were performed using the independent-samples t test or Mann–Whitney U-test for continuous variables and the χ2-test for categorical variables.
Associations between vertebral bone quality (VBQ) and clinical parameters were evaluated using Spearman correlation analysis, as several variables (eg, NLR, PLR, and age) showed non-normal distributions. A multivariable linear regression model was then constructed with VBQ as the dependent variable and age, sex, smoking, diabetes, body mass index (BMI), NLR, and PLR as independent predictors. Multicollinearity was assessed by calculating the variance inflation factor (VIF) for each predictor, and all VIF values were below 2.5, indicating acceptable collinearity.
To improve interpretability, both unstandardized and standardized coefficients (βstd) were reported, along with 95% confidence intervals (CIs) and partial R2 values to quantify the unique contribution of each variable. In addition, results were expressed on clinically meaningful scales—for example, the change in VBQ per 1-unit increase in NLR and per 50-unit increase in PLR. The overall model performance was summarized using the adjusted R2 statistic. A two-tailed p < 0.05 was considered statistically significant. All analyses were performed using SPSS (version 26.0; IBM Corp., Armonk, NY, USA).
Results
The interobserver reliability for VBQ measurements was excellent, with an ICC of 0.864 (95% CI, 0.789–0.918; p < 0.001). Baseline demographic and clinical characteristics stratified by VBQ scores are summarized in Table 1.
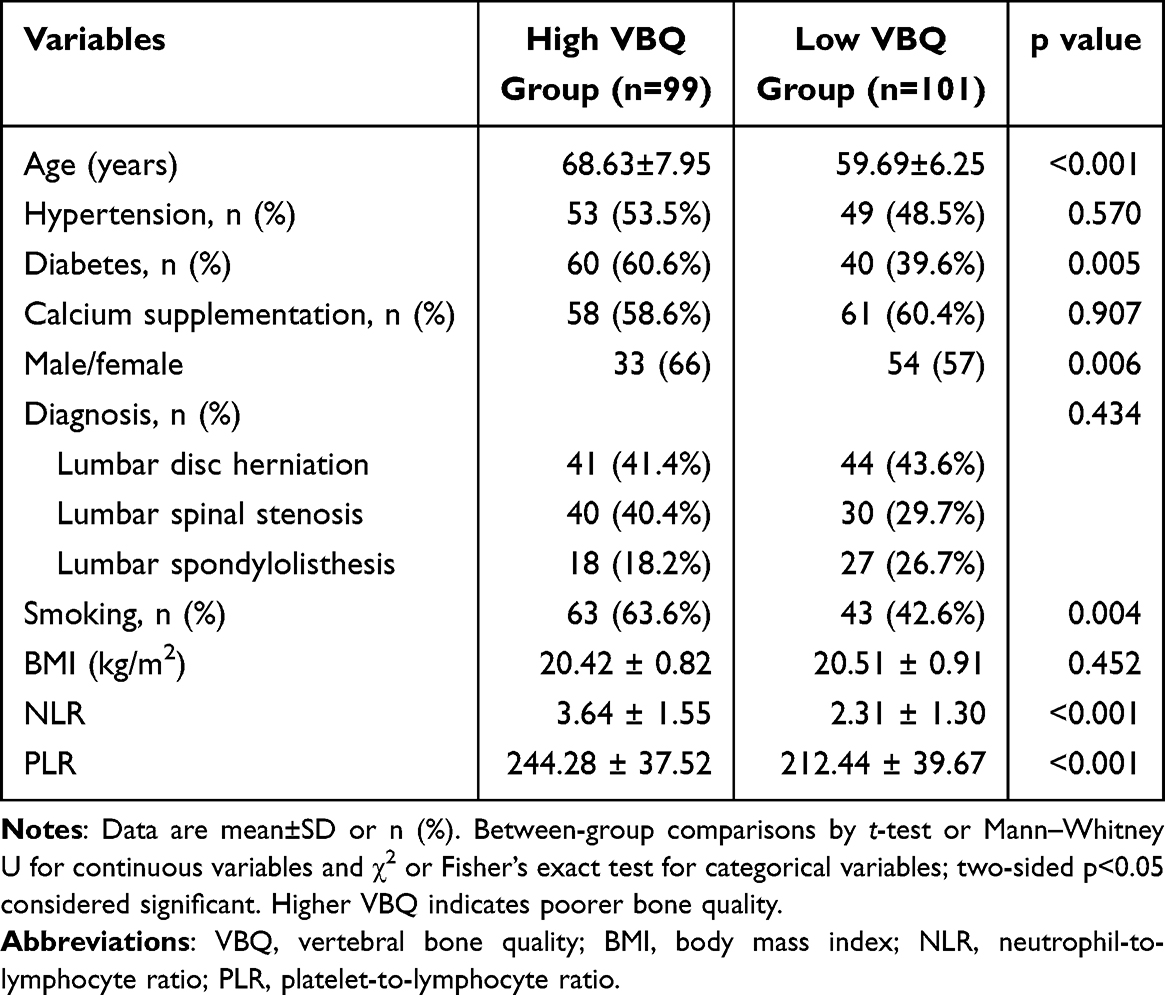 |
Table 1 Baseline Characteristics of the High and Low VBQ Groups |
We analyzed 200 patients and split the cohort at the median VBQ of 2.90, where a higher VBQ reflects poorer bone quality. Relative to the low-VBQ group, the high-VBQ group was older (mean difference 8.94 years, 95% CI 6.96–10.92) and showed higher inflammatory ratios (NLR +1.33, 95% CI 0.93–1.73; PLR +31.84, 95% CI 21.14–42.54). Diabetes and current smoking were more frequent (diabetes OR 2.35, 95% CI 1.33–4.14; smoking OR 2.36, 95% CI 1.34–4.17), whereas BMI was similar (mean difference −0.09 kg/m2, 95% CI −0.33 to 0.15). Rates of hypertension, calcium supplementation, and diagnostic subtypes were comparable between groups. These differences are consistent with a higher systemic inflammatory/metabolic load in patients with higher VBQ and set the context for the multivariable analyses. Accordingly, subsequent models adjusted for age, sex, BMI, smoking, and diabetes to mitigate confounding.
Correlation Analysis
Spearman correlation showed positive monotonic associations between VBQ and age (ρ = 0.650, p < 0.001; Figure 2), NLR (ρ = 0.534, p < 0.001; Figure 3), and PLR (ρ = 0.452, p < 0.001; Figure 4). BMI showed no meaningful monotonic correlation with VBQ (ρ = 0.093, p = 0.191). These patterns indicate that older age and higher inflammatory ratios are linked with poorer vertebral bone quality (higher VBQ).
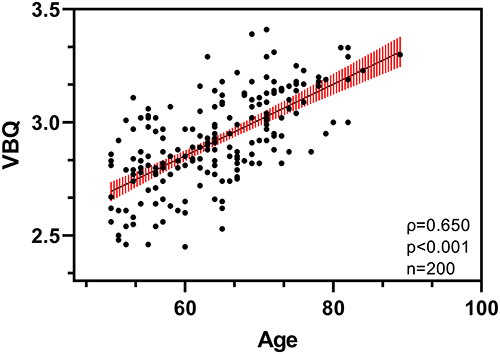 |
Figure 2 Scatter plot of VBQ versus age. Each point represents one patient. The solid line shows an ordinary least-squares trend with a 95% confidence band for visualization only; correlation inference is based on Spearman’s ρ (annotated on the panel). VBQ denotes the MRI-derived vertebral bone quality index; higher values indicate poorer bone quality. Observed values show a positive monotonic association between older age and higher VBQ, consistent with reduced vertebral integrity in older patients. |
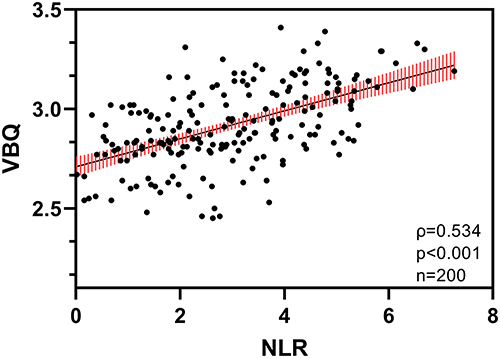 |
Figure 3 Scatter plot of VBQ versus NLR (neutrophil-to-lymphocyte ratio). Points represent individual patients. A trend line with a 95% confidence band is provided for visualization only; Spearman’s ρ, p, and n are annotated on the panel and used for inference. Higher VBQ reflects poorer bone quality; the positive monotonic pattern suggests greater systemic inflammatory burden (higher NLR) is associated with inferior vertebral marrow quality. |
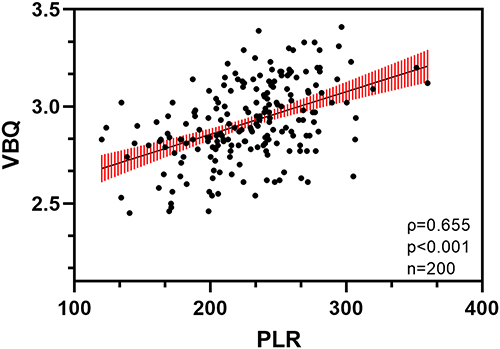 |
Figure 4 Scatter plot of VBQ versus PLR (platelet-to-lymphocyte ratio). Points represent individual patients. The solid line indicates a least-squares trend with 95% confidence band for visualization only; Spearman correlation (ρ) provides the statistical inference (ρ, p, n annotated). VBQ increases with poorer bone quality; the positive relationship with PLR supports the role of inflammatory tone as an adjunctive signal for skeletal risk stratification. |
Multifactor Linear Regression Analysis
In the multivariable linear model adjusting for age, sex, smoking, diabetes, and body mass index (BMI) (n=200), both inflammatory ratios remained independently associated with higher VBQ (poorer bone quality). PLR: β = 0.0015 (95% CI 0.0010–0.0020), p < 0.001; NLR: β = 0.0196 (95% CI 0.0021–0.0372), p = 0.028; Age: β = 0.0110 (95% CI 0.0074–0.0145), p < 0.001. BMI was not significant (β = 0.0072, 95% CI −0.0160–0.0304, p = 0.54), nor were sex, smoking, or diabetes (all p > 0.40). Model fit was adjusted R2 = 0.520, and multicollinearity was low (all VIF ≤ 2.26) (Table 2).
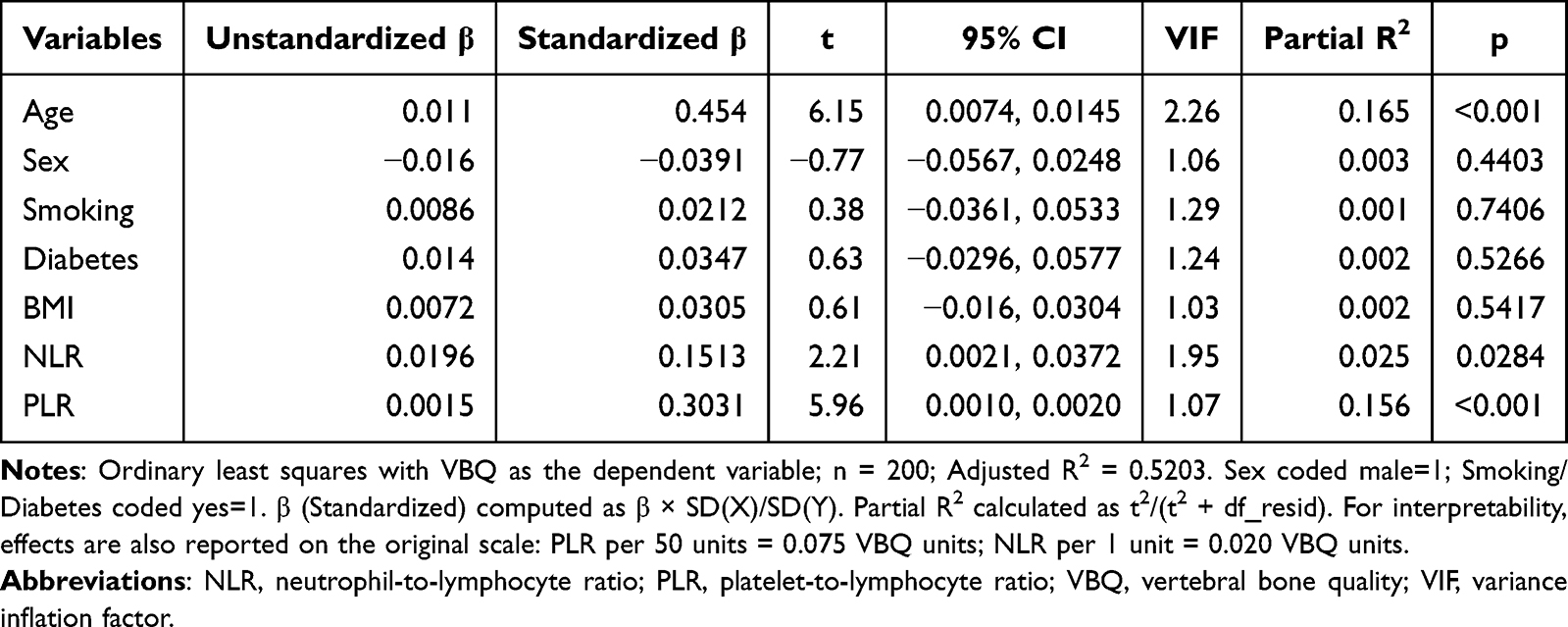 |
Table 2 Multifactor Linear Regression Analysis of VBQ |
To aid interpretation, we report standardized effects and unique contributions. PLR showed a standardized β (βstd) = 0.303 with partial R2 ≈ 0.156; NLR had βstd = 0.151 with partial R2 ≈ 0.025; age had βstd = 0.454 with partial R2 ≈ 0.165. On the original scale, each 50-unit increase in PLR corresponds to a 0.075-unit increase in VBQ, and each 1-unit increase in NLR corresponds to a 0.020-unit increase in VBQ.
Sensitivity analyses yielded consistent findings: with log-transformed ratios, PLR remained significant (β=0.3235, p<0.001) while lnNLR was positive but not significant (β=0.0270, p=0.098); after winsorization with HC3 robust SEs, both PLR (β=0.0015, p<0.001) and NLR (β=0.0198, p=0.023) remained significant; in a logistic specification (VBQ≥2.90), the OR per SD for lnNLR was 1.20 (95% CI 0.74–1.95), consistent with reduced power after dichotomization. Overall fit was unchanged (adjusted R2≈0.52). Across sensitivity analyses, effect directions were consistent and the overall inference was unchanged.
Discussion
In this study, we explored the associations between the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and vertebral bone quality (VBQ) in patients with degenerative lumbar disease. Analysis of 200 patients demonstrated significant positive correlations between both NLR and PLR and VBQ scores, suggesting that systemic inflammation may contribute to the deterioration of vertebral bone quality in this population.
Baseline comparisons showed that the high-VBQ group differed meaningfully from the low-VBQ group, highlighting factors linked to poorer vertebral quality. Female sex and current smoking were associated with higher VBQ, consistent with established risks for bone impairment; postmenopausal women are vulnerable due to estrogen deficiency, which accelerates resorption and alters marrow composition.6
Diabetes was more prevalent in the high-VBQ group, supporting a link between diabetes and impaired vertebral quality—potentially via altered calcium handling, reduced osteoblast activity, and AGE-mediated matrix damage.11 Calcium supplementation did not differ between groups (p = 0.907), which may reflect suboptimal adherence/exposure or the limited effect of calcium alone on established deterioration.12 Smoking was markedly more frequent with higher VBQ, aligning with evidence that oxidative stress and chronic inflammation suppress osteoblast function and calcium absorption.13 Hypertension and BMI showed no significant between-group differences; the BMI–bone relation is likely context-dependent and shaped by lipid, inflammatory, and hormonal pathways rather than a simple linear effect.14,15
The high VBQ group was significantly older than the low VBQ group (mean difference ≈ 9 years, p < 0.001), reinforcing age as a key determinant of vertebral bone quality. Aging is closely linked to progressive bone loss, reduced osteoblastic activity, and increased marrow adiposity, all of which contribute to impaired bone microarchitecture. These findings are consistent with prior studies showing that VBQ scores tend to rise with advancing age,16 reflecting deterioration in vertebral bone integrity. Given that age-related changes in bone metabolism are vary across different life stages,17 future studies should consider modeling age as a quadratic term or applying spline regression techniques to better characterize its effect. Additionally, potential interaction effects between age and systemic inflammation markers should be explored, particularly regarding their differential impact on vertebral bone quality across various age strata. These findings reinforce the multifactorial nature of vertebral bone loss and underscore the importance of addressing systemic risk factors in clinical assessment.
The lack of significant differences in VBQ scores across various diagnostic subtypes suggests that vertebral bone quality may not be substantially influenced by specific disease classifications within this cohort. Several factors could explain this observation. First, variability within each diagnostic group may obscure potential differences between subtypes. Second, other factors such as age, BMI, and bone density may have a greater impact on VBQ than diagnostic category alone. Additionally, the limited sample size and absence of refined diagnostic stratification may have reduced the ability to detect subtle variations. Future studies with larger cohorts and more detailed diagnostic subgrouping are needed to further clarify the relationship between diagnosis and VBQ.
Our data showed significant positive correlations between VBQ and NLR/PLR, in line with reports linking inflammatory tone to deterioration of bone quality, particularly in osteoporosis/osteopenia.18 Mechanistically, systemic inflammatory activation—with immune-cell–derived pro-inflammatory cytokines—can promote resorption and suppress formation, thereby degrading trabecular integrity and marrow quality.19 In multivariable linear regression, age, NLR, and PLR remained independently associated with higher VBQ; the full model explained ~52% of variance (adjusted R2 = 0.520), and standardized effects indicated that PLR (β_std ≈ 0.30) and NLR (β_std ≈ 0.15) provide complementary, non-redundant information. These findings support NLR/PLR as adjunctive markers rather than stand-alone predictors in preoperative skeletal risk appraisal.
Both diabetes and smoking are chronic conditions associated with sustained low-grade inflammation, which is a known contributor to bone loss. NLR and PLR, as composite indicators of systemic inflammation, may capture the cumulative inflammatory burden resulting from these conditions. Therefore, while diabetes and smoking history may not directly correlate with bone quality in the adjusted model, their pro-inflammatory effects are likely mediated through the elevation of NLR and PLR, supporting the role of these markers as more integrative predictors of bone deterioration.
Although dual-energy X-ray absorptiometry (DXA) and CT-derived Hounsfield units (HU) remain reference tools for assessing bone mineral density, their use can be constrained in routine perioperative workflows by availability, cost, and logistics. By contrast, inflammatory ratios such as the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) are inexpensive, universally obtained from preoperative blood tests, and require no additional imaging. Nevertheless, these indices are non-specific surrogates of systemic inflammation and can be influenced by factors not captured in our dataset (eg, subclinical infection, medication exposure, renal/hepatic dysfunction, and nutrition), so residual confounding cannot be excluded. In our cohort, the associations with MRI-derived VBQ persisted after adjustment but were modest to moderate on the standardized scale (β_std ≈ 0.15 for NLR; ≈ 0.30 for PLR), and the model’s explanatory power was moderate (adjusted R2 ≈ 0.52). From a pragmatic standpoint, NLR/PLR can be used as adjuncts to MRI-based VBQ in a tiered scheme: patients with higher VBQ (eg, upper cohort quantiles) and ratios above locally calibrated reference limits (institutional upper reference, cohort upper quartile, or a site-specific ROC/Youden cut-point) may be flagged for perioperative bone-health optimization (vitamin D/calcium review, management of correctable metabolic factors, smoking cessation, fall-risk precautions); discordant profiles (high VBQ with normal ratios, or vice versa) can be considered intermediate risk; and both low VBQ and low ratios indicate lower risk. Because absolute cut-offs for NLR/PLR vary by laboratory and population, we do not prescribe universal thresholds and recommend local calibration with reported operating characteristics. Accordingly, NLR and PLR should complement rather than replace imaging, and prospective, head-to-head studies against DXA/HU with standardized MRI protocols are needed to define actionable thresholds and clarify comparative performance.
Despite the strengths of a well-characterized surgical cohort and standardized VBQ assessment, several limitations merit consideration. First, the retrospective, cross-sectional design precludes causal inference. Second, inflammatory indices were limited to composite ratios; specific mediators (eg, interleukin-6, tumor necrosis factor-α) were not measured, and unmeasured confounding—including subclinical infections, medication exposure (eg, steroids or anti-osteoporotic agents), and nutritional factors such as calcium/vitamin D supplementation—may persist despite multivariable adjustment. Third, analyses were conducted within a single center using a uniform acquisition protocol, which may constrain generalizability. Finally, although interobserver agreement for VBQ was good, ROI-based measurements remain susceptible to residual measurement variability.
Conclusion
Preoperative inflammatory ratios—particularly NLR and PLR—showed positive, independent associations with MRI-derived VBQ after adjustment, linking routine laboratory signals to a quantitative MRI surrogate of vertebral integrity. These readily available markers are adjuncts, not substitutes, and may help prioritize skeletal risk assessment where DXA is not available. Given the retrospective, single-center design and absence of head-to-head comparisons with DXA/HU, prospective multicenter studies with standardized MRI and site-specific threshold calibration are needed to establish actionable cut-points and confirm clinical utility.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
This retrospective study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Baoding No.1 Central Hospital (Approval No. [2024]105). All participants provided informed consent prior to inclusion in the study. Clinical trial registration number: not applicable.
Funding
This study was supported by the S&T Program of Baoding (2441ZF051).
Disclosure
The authors declare no competing interests.
References
1. Ehresman J, Pennington Z, Schilling A, et al. Novel MRI-based score for assessment of bone density in operative spine patients. Spine J. 2020;20(4):556–562. doi:10.1016/j.spinee.2019.10.018
2. Kuo CC, Soliman M, Baig RA, et al. Vertebral bone quality score as a predictor of adjacent segment disease after lumbar interbody fusion. Neurosurgery. 2024;95:284–296. doi:10.1227/neu.0000000000002864
3. Hu YH, Chou JH, Yeh YC, et al. The MRI-based vertebral bone quality score is a predictor of pedicle screw loosening following instrumented posterior lumbar fusion. Sci Rep. 2025;15(1):1696. doi:10.1038/s41598-025-85625-8
4. Xue Y, Shi K, Dai W, Ma C, Li J. Prediction of subsequent vertebral fracture after percutaneous vertebral augmentation using MRI-based vertebral bone quality and CT-based Hounsfield units: a retrospective cross-sectional study. Sci Rep. 2025;15(1):3524. doi:10.1038/s41598-025-86721-5
5. Wang L, Deng Q, Wang B, et al. Comparison of the predictive values of MRI-based vertebral bone quality scores for the determination of osteoporosis in different diseases. Eur Spine J. 2024;33(4):1504–1510. doi:10.1007/s00586-024-08151-7
6. Zhao X, Wang Q, Wang P, Kong C, Lu S. Exploring the impact of body mass index on the accuracy of vertebral bone quality in determining bone mineral density in patients undergoing lumbar fusion surgery. J Orthop Surg Res. 2024;19(1):763. doi:10.1186/s13018-024-05195-9
7. Bousch JF, Beyersdorf C, Schultz K, Windolf J, Suschek CV, Maus U. Proinflammatory cytokines enhance the mineralization, proliferation, and metabolic activity of primary human osteoblast-like cells. Int J Mol Sci. 2024;25(22):12358. doi:10.3390/ijms252212358
8. Lisco G, Triggiani D, Giagulli VA, et al. Endocrine, metabolic, and immune pathogenesis of postmenopausal osteoporosis. Is there a therapeutic role in natural products. Endocr Metab Immune Disord Drug Targets. 2023;23(10):1278–1290. doi:10.2174/1871530323666230330121301
9. Wu Y, Yang Y, Wang L, et al. Effect of Bifidobacterium on osteoclasts: TNF-α/NF-κB inflammatory signal pathway-mediated mechanism. Front Endocrinol. 2023;14:1109296. doi:10.3389/fendo.2023.1109296
10. Liu YC, Yang TI, Huang SW, Kuo YJ, Chen YP. Associations of the neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio with osteoporosis: a meta-analysis. Diagnostics. 2022;12(12):2968. doi:10.3390/diagnostics12122968
11. Liu J, Ran C, Liu X, Guo W. Bibliometric analysis and visualisation of association studies between diabetes and osteoporosis. Asian J Surg. 2024;2024:
12. Subarajan P, Arceo-Mendoza RM, Camacho PM. Postmenopausal osteoporosis: a review of latest guidelines. Endocrinol Metab Clin North Am. 2024;53(4):497–512. doi:10.1016/j.ecl.2024.08.008
13. Suh YJ, McDonald MN, Washko GR, et al. Lung, fat and bone: increased adiponectin associates with the combination of smoking-related lung disease and osteoporosis. Chronic Obstr Pulm Dis. 2018;5(2):134–143. doi:10.15326/jcopdf.5.2.2016.0174
14. Asomaning K, Bertone-Johnson ER, Nasca PC, Hooven F, Pekow PS. The association between body mass index and osteoporosis in patients referred for a bone mineral density examination. J Womens Health. 2006;15(9):1028–1034. doi:10.1089/jwh.2006.15.1028
15. Fassio A, Idolazzi L, Rossini M, et al. The obesity paradox and osteoporosis. Eat Weight Disord. 2018;23(3):293–302. doi:10.1007/s40519-018-0505-2
16. Mosekilde L. Age-related changes in bone mass, structure, and strength—effects of loading. Z Rheumatol. 2000;59(Suppl 1):1–9. doi:10.1007/s003930070031
17. Manolagas SC. The quest for osteoporosis mechanisms and rational therapies: how far we’ve come, how much further we need to go. J Bone Miner Res. 2018;33(3):371–385. doi:10.1002/jbmr.3400
18. Chen S, Sun X, Jin J, Zhou G, Li Z. Association between inflammatory markers and bone mineral density: a cross-sectional study from NHANES 2007–2010. J Orthop Surg Res. 2023;18(1):305. doi:10.1186/s13018-023-03795-5
19. Lee SH, Ryu SY, Park J, Shin MH, Han MA, Choi SW. The relationship of neutrophil-lymphocyte ratio and platelet-lymphocyte ratio with bone mineral density in Korean postmenopausal women. Chonnam Med J. 2019;55(3):150–155. doi:10.4068/cmj.2019.55.3.150
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.