Back to Journals » Drug Design, Development and Therapy » Volume 13
Nicorandil prior to primary percutaneous coronary intervention improves clinical outcomes in patients with acute myocardial infarction: a meta-analysis of randomized controlled trials
Authors Xu L, Wang L, Li K, Zhang Z, Sun H, Yang X
Received 25 November 2018
Accepted for publication 21 February 2019
Published 29 April 2019 Volume 2019:13 Pages 1389—1400
DOI https://doi.org/10.2147/DDDT.S195918
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qiongyu Guo
Li Xu, Lefeng Wang, Kuibao Li, Zhiyong Zhang, Hao Sun, Xinchun Yang
Heart Center and Beijing Key Laboratory of Hypertension, Beijing Chaoyang Hospital, Capital Medical University, Beijing 100020, People’s Republic of China
Background: Nicorandil prior to reperfusion by primary percutaneous coronary intervention (PCI) in patients with ST-segment elevated myocardial infarction (STEMI) has been suggested to be beneficial. However, results of previous randomized controlled trials (RCTs) were not consistent. We aimed to perform a meta-analysis to systematically evaluate the effect of periprocedural nicorandil in these patients.
Methods: Related studies were obtained by searching PubMed, Embase and Cochrane’s Library. Effects of perioperative nicorandil on the incidence of no-reflow phenomenon (NRP), corrected thrombolysis in myocardial infarction (TIMI) frame count (CTFC), wall motion score (WMS), left ventricular ejection fraction (LVEF), heart failure (HF) exacerbation of rehospitalization and incidence of major cardiovascular adverse events (MACE) were analyzed.
Results: Eighteen RCTs with 2,055 patients were included. Treatment of nicorandil prior to PCI significantly reduced the incidence of NRP (risk ratio [RR]: 0.47, P<0.001), and reduced CTFC (weighed mean difference [WMD]: −4.54, P<0.001) immediately after PCI. Moreover, although nicorandil did not significantly affect WMS (WMD: 0.04, P=0.91), treatment of nicorandil significantly increased LVEF in STEMI patients undergoing primary PCI (WMD: 1.89%, P<0.001). In addition, nicorandil significantly reduced the risk of HF exacerbation or rehospitalization (RR: 0.44, P=0.001) and the incidence of MACE (RR: 0.68, P<0.001). Further analyses showed that effects of nicorandil on LVEF, HF exacerbation and MACE were consistent within one month after PCI and during follow-up.
Conclusions: Periprocedural nicorandil improves coronary blood flow, cardiac systolic function and prognosis in STEMI patients receiving primary PCI.
Keywords: ST-segment elevated myocardial infarction, Nicorandil, primary percutaneous coronary intervention, no-reflow phenomenon, meta-analysis
A Letter to the Editor has been published for this article.
Introduction
Early myocardial reperfusion by primary percutaneous coronary intervention (PCI) has become an important treatment strategy for patients with ST-segment elevated myocardial infarction (STEMI), which is associated with reduced infarct size, preserved cardiac function and improved clinical outcomes in these patients.1,2 However, despite effective reperfusion by PCI, a considerable proportion of patients with STEMI still have impaired cardiac function and increased cardiovascular mortality.3,4 It has been demonstrated that coronary microvascular dysfunction and obstruction, which occur in almost half of STEMI patients after primary PCI, are important causes of subsequent deterioration of cardiac function and poor prognosis in these patients.5,6 Therefore, it is hypothesized that early application of agents that attenuate coronary microvascular dysfunction and obstruction may further improve the prognosis of patients with STEMI despite effective revascularization.7
Nicorandil, as a hybrid of an adenosine triphosphate (ATP)-sensitive opener of potassium channel and nitrates, has been demonstrated to improve coronary microvascular dysfunction and obstruction via its vasodilatory effect on small coronary arteries.8,9 Clinically, nicorandil is applied as a treatment of chronic stable angina in patients with effort-induced symptoms arising from epicardial coronary artery stenoses, coronary vasospasm and microvascular dysfunction.10 A few clinical trials have indicated that nicorandil is effective to reduce the frequency of angina episodes and improve exercise capacity in patients with stable angina.11 Moreover, nicorandil is well tolerated by most patients, with a satisfactory safety profile as evidenced by accumulating studies.12 Pharmacologically, despite its benefit on coronary microcirculation, nicorandil may also exert cardio-protective efficacies via anti-oxidation, anti-inflammation and mimicking of ischemic preconditioning.10,13 Therefore, it is hypothesized that administration of nicorandil prior to primary PCI in STEMI patients may also confer additional benefits in these patients via its improvement on microvascular dysfunction and obstruction. Indeed, two previous meta-analyses of randomized controlled trials (RCTs) have been published to evaluate the efficacy of perioperative nicorandil in STEMI patients undergoing PCI. One study published in 2013 including 14 RCTs indicated that perioperative administration of nicorandil improved coronary blood flow and preserved cardiac function in STEMI patients undergoing PCI.14 However, it failed to show a beneficial effect of nicorandil on clinical outcomes, which, from the authors’ perspective, is probably due to the limited sample sizes of the included RCTs.15–28 Another study published in 2016 including 13 RCTs showed that perioperative administration of nicorandil improved in-hospital outcomes in STEMI patients undergoing PCI without significant benefit on clinical outcomes from discharge to eight months during follow-up.29 However, this meta-analysis is with some flaws since four validated RCTs16,22,23,25 were missed, while a cardiac magnetic resonance imaging sub-study of an already included RCT was repeatedly included.30 Moreover, some relevant studies have been published since the last meta-analysis.31–33 Therefore, we aimed to perform an updated meta-analysis to evaluate effect of nicorandil prior to PCI on coronary blood flow, cardiac systolic function and clinical outcomes in STEMI patients.
Methods
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement34 and the Cochrane Handbook guidelines35 were followed during the design and performance of this systematic review and meta-analysis.
Literature searching
PubMed, Embase and the Cochrane Library (Cochrane Center Register of Controlled Trials) databases were systematically searched for relevant RCTs. The search strategy included a combination of the following terms: (1) Nicorandil OR “2-Nicotinamidoethyl Nitrate” OR “2 Nicotinamidoethyl Nitrate” OR “Nitrate, 2-Nicotinamidoethyl” OR “2-Nicotinamidethyl Nitrate” OR “2 Nicotinamidethyl Nitrate” OR “Nitrate, 2-Nicotinamidethyl” OR SG-75 OR “SG 75” OR “SG75” OR “KATP channel openers” OR “sigmart” OR “Ikorel”; (2) “myocardial infarction” OR “percutaneous coronary intervention” OR “PCI” and (3) “random” OR “randomize” OR “randomly” OR “randomization” OR “randomized” OR “randomised”. We applied the limitation of study type as studies in humans. Besides, the references of the original articles and reviews were also screened as a complementary process. The date of final database search was October 20, 2018.
Inclusion and exclusion criteria
The inclusion criteria for the potential studies were: (1) full-length articles published in English or Chinese in peer-reviewed journals; (2) designed as RCTs to evaluate the effect of perioperative administration of nicorandil in patients with STEMI undergoing primary PCI; (3) nicorandil was applied intravenously or intracoronarily prior to the reperfusion by PCI; (4) included a control group with placebo or no nicorandil treatment and (5) reported at least one of the following outcomes: no-reflow phenomenon (NRP) and corrected thrombolysis in myocardial infarction (TIMI) frame count (CTFC) after PCI, wall motion score (WMS), left ventricular ejection fraction (LVEF), risk of heart failure (HF) exacerbation of rehospitalization and incidence of major cardiovascular adverse events (MACE) during follow-up. Definition of NFP was consistent with the criteria used in the original studies, which referred to the appearance of TIMI 0–1 coronary flow in angiography after PCI despite adequate dilation of the target vessel and without angiographic mechanical obstruction.36 The MACEs were defined as composite outcomes of all-cause death, target vessel revascularization, recurrent angina or myocardial infarction, stroke and severe HF. Reviews, observational studies, crossover studies, studies with nicorandil used after perfusion and those with unavailable data were excluded.
Data extraction and quality assessment
Two independent authors performed the database search, data extraction and quality evaluation according to inclusion criteria. Discrepancies were resolved by consensus with a third author. Extracted data included study design, age and gender of the patients, proportions of patients with diabetes mellitus [DM], percentiles of those with left anterior descending artery occlusion, time from symptom onset to reperfusion, nicorandil administration routes and regimens. For quality evaluation of the included RCTs, the seven domains of the Cochrane Risk of Bias Tool was applied,35 which quantified the quality of the included RCTs with the following aspects: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessors, incomplete outcome data, selective outcome reporting and other potential threats to validity.
Statistical analysis
Continuous data were evaluated via weighted mean difference (WMD), whereas categorized data were analyzed using risk ratios (RR) with 95% confidence interval (CI). For the test of heterogeneity, the Cochrane’s Q test was used,35 which indicated a significant heterogeneity if P<0.10. I2 statistic, which reflected the percentage of total variation among studies that is caused by heterogeneity rather than chance,37 was also calculated. If a significant heterogeneity was detected, a random-effect model was applied to pool the results. Otherwise, a fixed-effect model was used. Further analyses were applied to evaluate whether the effects of nicorandil on LVEF, HF exacerbation and MACE were consistent in short term (within one month after PCI) or during follow-up. Potential publication bias was assessed with Egger’s regression asymmetry test,38 or visual inspection of the symmetry of the funnel plots. A P<0.05 indicated statistical significance. We used RevMan (Version 5.1; Cochrane, Oxford, UK) and Stata software (Version 12.0; Stata, College Station, TX) software for statistical analyses.
Results
Database searching
The flowchart of literature search is presented in Figure 1. A total of 488 RCTs were identified via initial database search, and 453 studies were excluded after reading titles and abstracts because of their irrelevance. Of the remaining 35 studies that underwent full-text review, 17 were further excluded with the reasons listed in Figure 1. Finally, 18 RCTs15–33,39 were included.
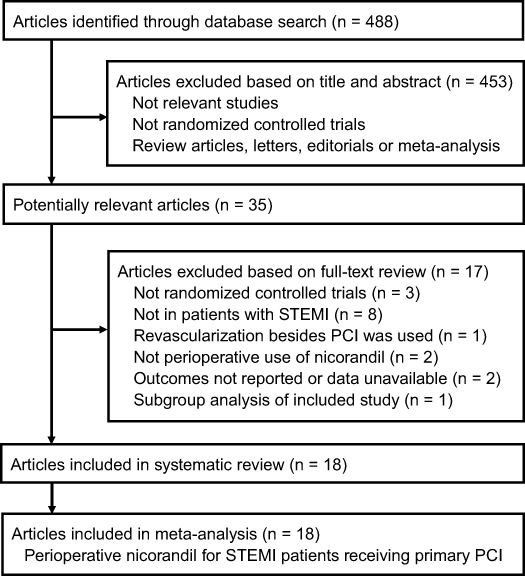 | Figure 1 Flowchart of literature search and study identification. Abbreviations: PCI, percutaneous coronary intervention; STEMI, ST-segment elevated myocardial infarction. |
Study characteristics
Overall, 18 RCTs with 2,055 patients were included in the meta-analysis. Since one study included two comparisons of different administration routes of nicorandil,24 and another study included two comparisons with and without subsequently oral administration of nicorandil,22 these comparisons were included separately and finally made 20 comparisons included. All of the RCTs were performed in Asia. The baseline characteristics of the patients are summarized in Table 1. Nicorandil was administered intravenously, intracoronarily or combined. In some studies, patients in the nicorandil group also received sequential oral administration of nicorandil.15,21–23
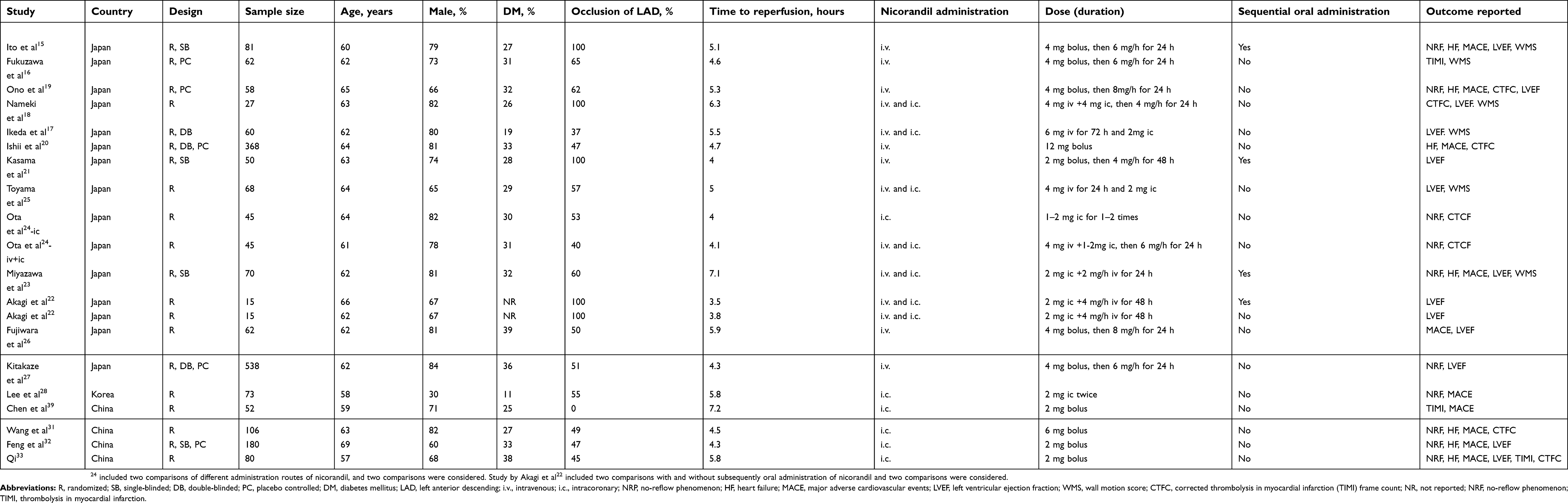 | Table 1 Characteristics of the included RCTs |
Quality evaluation
The details of quality evaluation in each domain of the Cochrane’s Risk of Bias Tool are listed in Table 2. Overall, the quality of the included RCTs was moderate. Three of them were double-blinded RCT,17,20,27 with the generation of random sequences reported in two studies27,31 and the strategies for allocation concealment reported in four19,20,24,27 studies.
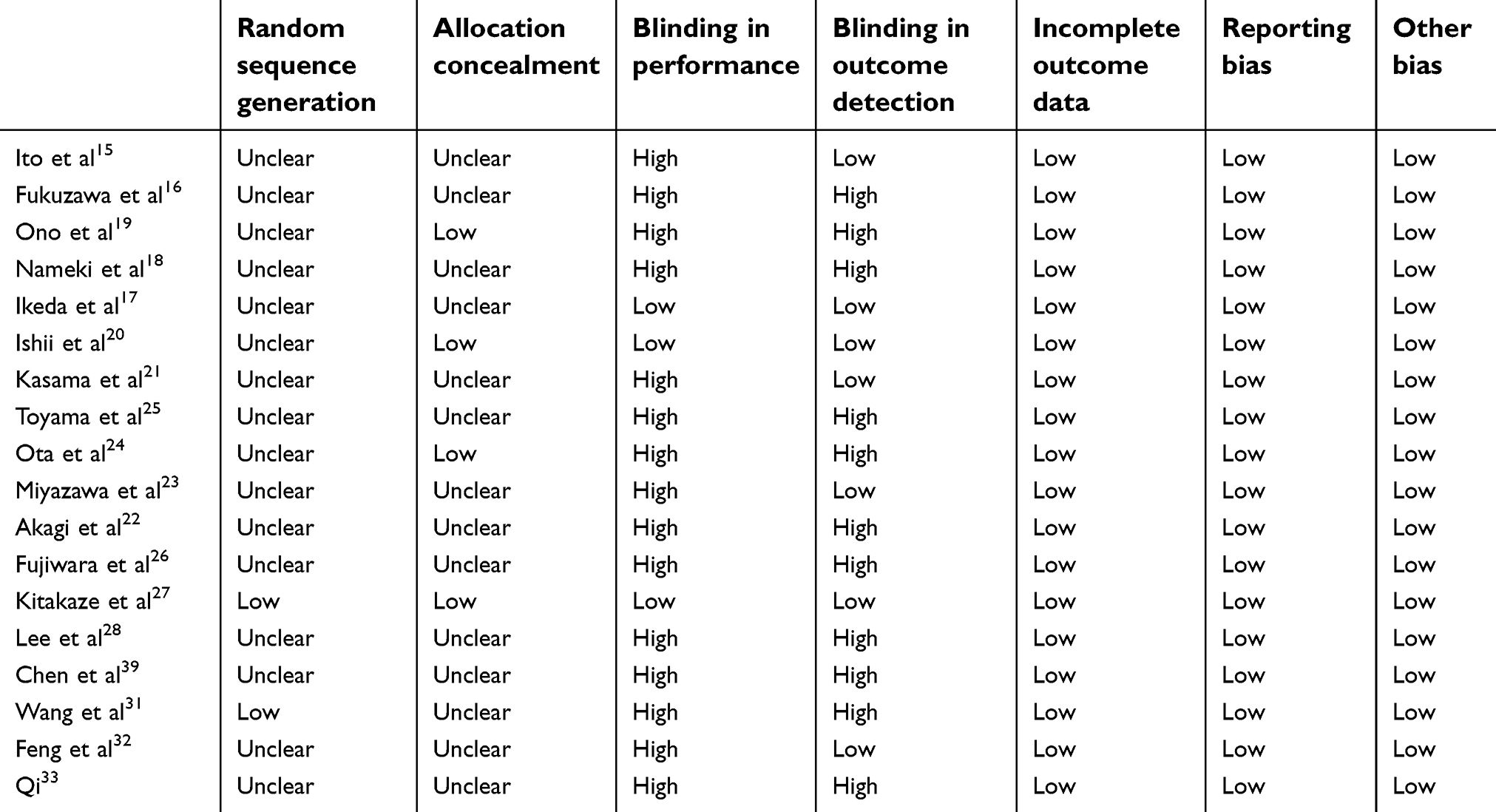 | Table 2 Quality evaluation by cochrane risk of bias tool |
Effects of perioperative nicorandil on coronary blood flow immediately after PCI
Ten comparisons with 1,273 STEMI patients evaluated the effect of nicorandil on the incidence of NRP after PCI. Results of meta-analysis with a fixed-effect model showed that nicorandil significantly reduced the incidence of NRP (RR: 0.47, 95% CI: 0.33~0.67, P<0.001; Figure 2A) with no significant heterogeneity (P for Cochrane’s Q test: 0.55, I2 = 0%). Moreover, meta-analysis of seven comparisons showed that nicorandil significantly reduced CTFC (WMD: −4.54, 95% CI: −6.91~ −2.17, P<0.001, I2 = 49%; Figure 2B). These results suggested that nicorandil significantly improved coronary blood flow in STEMI patients after primary PCI.
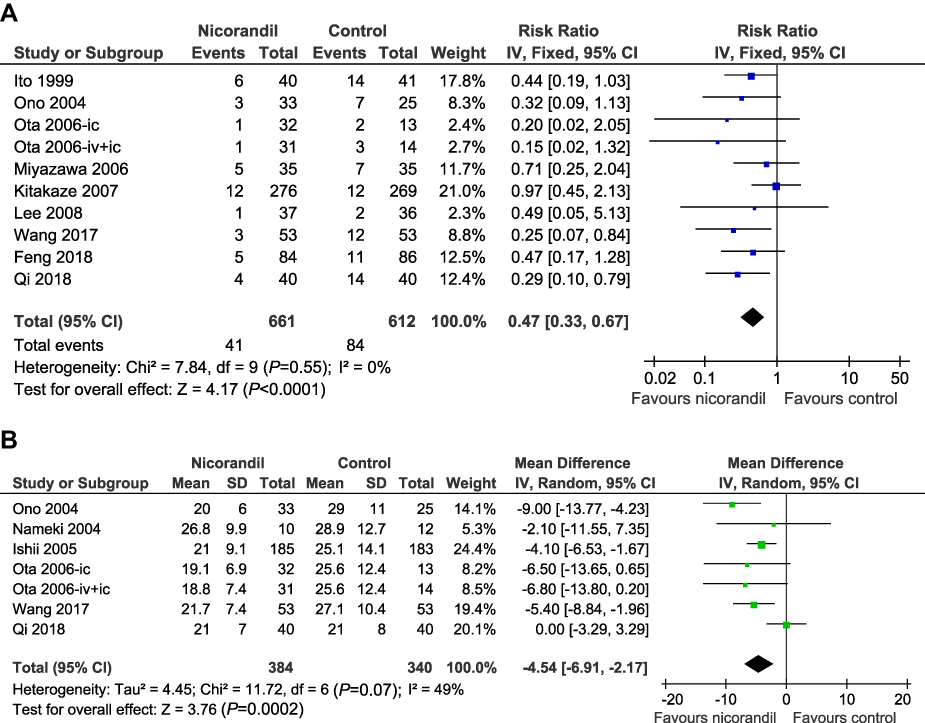 | Figure 2 Forest plots for the meta-analysis of the influences of nicorandil on coronary blood flow in STEMI patients undergoing primary PCI; (A) effects of nicorandil on the incidence of NRP; (B) effects of nicorandil on CTFC. Abbreviations: PCI, percutaneous coronary intervention; STEMI, ST-segment elevated myocardial infarction; NRP, no-reflow phenomenon; CTFC, corrected thrombolysis in myocardial infarction (TIMI) frame count. |
Effects of perioperative nicorandil on wall motion and cardiac systolic function
Meta-analysis with six comparisons did not show that nicorandil significantly improved WMS in STEMI patients after PCI (WMD: 0.04, 95% CI: −0.71~0.80, P=0.91; Figure 3A) with significant heterogeneity (I2 = 49%). However, nicorandil was associated with significantly increased LVEF in STEMI patients undergoing primary PCI (WMD: 1.89%, 95% CI: 1.08~2.71%, P<0.001, I2 = 29%; Figure 3B). Further analysis showed that nicorandil increased LVEF in STEMI patients within one month after PCI (WMD: 1.89%, P<0.001) and during subsequent follow-up (WMD: 1.90%, P=0.002). These results indicated that although effect seemed to be moderate, nicorandil significantly improved cardiac systolic function in STEMI patients after primary PCI.
 | Figure 3 Forest plots for the meta-analysis of the influences of nicorandil on wall motion and cardiac systolic function in STEMI patients undergoing primary PCI; (A) effects of nicorandil on WMS; (B) effects of nicorandil on LVEF.Abbreviations: PCI, percutaneous coronary intervention; STEMI, ST-segment elevated myocardial infarction; WMS, wall motion score; LVEF, left ventricular ejection fraction. |
Effects of perioperative nicorandil on HF exacerbation and MACE
Results of meta-analysis showed that nicorandil significantly reduced the risk of HF exacerbation or rehospitalization (RR: 0.44, 95% CI: 0.26~0.72, P=0.001; Figure 4A) and the incidence of MACE (RR: 0.68, 95% CI: 0.54~0.85, P<0.001; Figure 4B) without significant heterogeneities (I2 = 0% and 35%, respectively). Moreover, further analysis showed that the preventative efficacies of nicorandil on HF exacerbation and MACE in STEMI patients were consistent within one month after PCI and during subsequent follow-up. These results indicated that nicorandil significantly improved the prognosis in STEMI patients undergoing primary PCI.
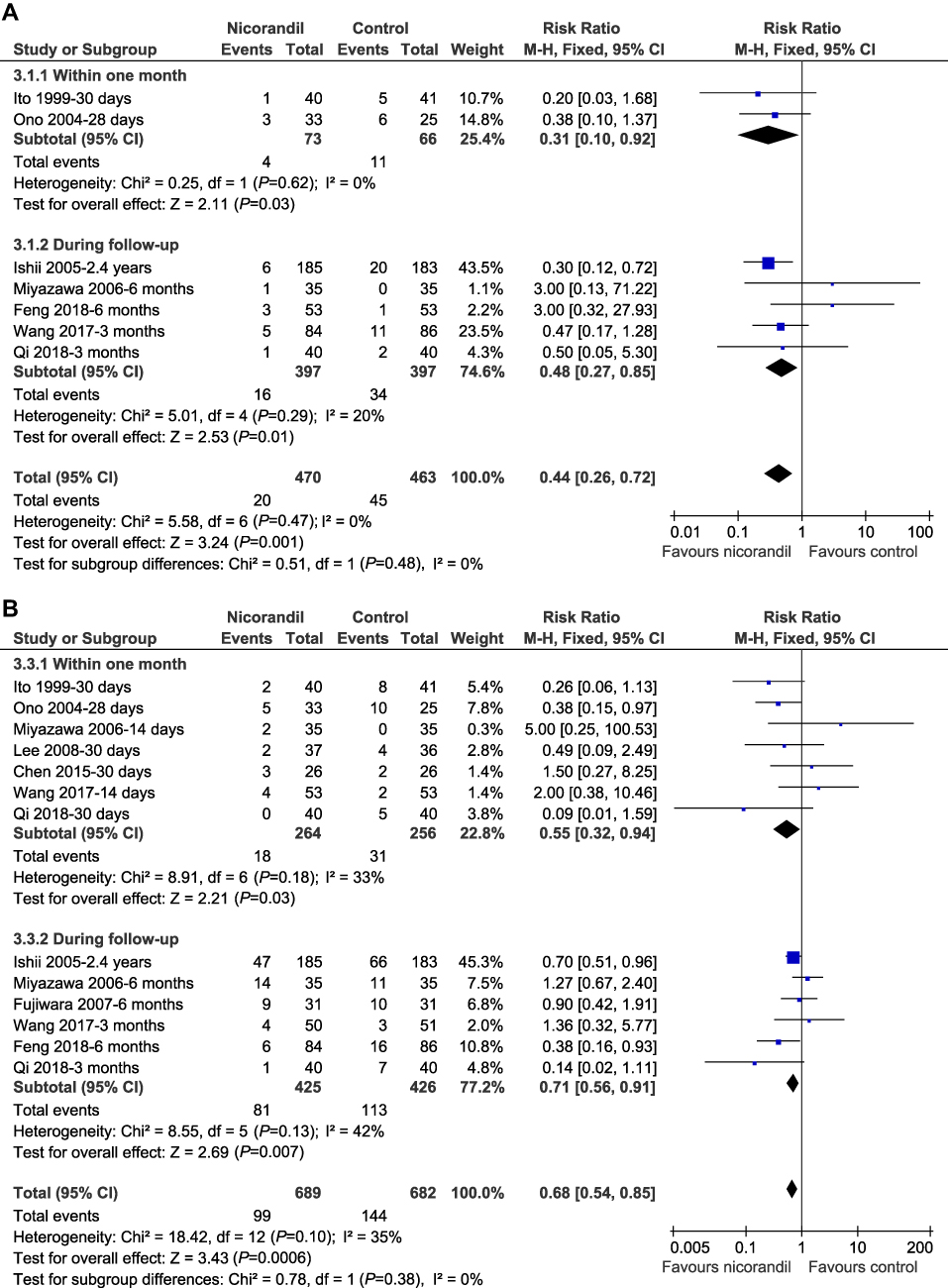 | Figure 4 Forest plots for the meta-analysis of the influences of nicorandil on clinical outcomes in STEMI patients undergoing primary PCI; (A) effects of nicorandil on the risk of HF exacerbation or rehospitalization; (B) effects of nicorandil on the incidence of MACE. Abbreviations: PCI, percutaneous coronary intervention; STEMI, ST-segment elevated myocardial infarction; MACE, major adverse cardiovascular events; HF, heart failure. |
Publication bias
The funnel plots for the meta-analyses of the effects of nicorandil on NRP, CTFC, WMS, LVEF, HF exacerbation and MACE were symmetry on visual inspection, and Egger’s regression tests also indicated no significant publication biases within the meta-analysis (data not shown).
Discussion
Results of the study showed that perioperative treatment with nicorandil is associated with a lower risk of NRP and reduced CTFC as compared with controls in STEMI patients receiving primary PCI, indicating that nicorandil significantly improved coronary blood flow in these patients. Moreover, nicorandil preserved cardiac systolic function in these patients, as evidenced by a moderate increase of LVEF in patients allocated to the nicorandil treatment as compared with control group. Importantly, nicorandil significantly reduced the risk of HF exacerbation or rehospitalization and the incidence of MACE in STEMI patients undergoing primary PCI in both short-term and long-term follow-up. Taken together, these results suggested that periprocedural nicorandil improves coronary blood flow, cardiac systolic function and clinical outcomes in STEMI patients receiving primary PCI.
Previous studies indicated that the potential cardioprotecive effect of nicorandil is multifactorial, of which, improvement of coronary microvascular dysfunction may be the most important underlying mechanisms. An early pharmacological study in dogs showed that the vessels <100 microns were more sensitive to nicorandil than other size vessels, and that ATP-sensitive potassium channels were responsible in mediating the nicorandil-induced dilation of vessels smaller than 100 microns.40 Subsequent study with Gadomer-enhanced magnetic resonance imaging as a tool for the quantification of small microvascular obstruction showed that intravenous nicorandil attenuated the formation of microvascular obstruction regions in rats that underwent coronary artery occlusion and reperfusion.41 Moreover, a recent clinical study showed that intracoronary nicorandil administration after primary PCI significantly decreased the index of microvascular resistance, resulting in improved coronary flow reserve derived from the transthoracic Doppler and ventricular function in patients with STEMI undergoing primary PCI.42 Besides its direct dilatory effect on microvessels, other mechanisms such as anti-oxidative stress and anti-inflammation have also been suggested to be involved in its benefits on coronary microcirculation.43 Our results expanded these findings by showing that periprocedural nicorandil improves coronary blood flow, cardiac systolic function and clinical outcomes in STEMI patients receiving primary PCI, which highlight the potential benefits of clinical administration of nicorandil prior to primary PCI in STEMI patients. Since the potential benefits of nicorandil on cardiac function and clinical outcomes have been confirmed in patients with stable CAD44 and HF,45 administration of nicorandil for patients with STEMI, stable CAD and HF should be recommended, which may be a reflection of the importance of coronary microcirculatory dysfunction in the pathogenesis and progression of the diseases.
Our study has limitations. Firstly, different routes and regimens were applied for nicorandil administration. Therefore, the optimal route, dose and duration of nicorandil administration prior to PCI in patients with STEMI should be investigated. Secondly, part of the patients for the 1-month and follow-observations were overlapped. Therefore, rather than a strict subgroup analysis, our study that compared the effect of nicorandil on related outcomes during short-term and long-term follow-up may introduce bias by including the data of overlapped patients. However, we believe it is more accurate to include as more datasets as possible in order to compare the effect of nicorandil on related outcomes during short-term and long-term follow-up. Thirdly, all RCTs included were performed in Asia. The potential efficacies of nicorandil in STEMI patients from other countries should be determined. Fourthly, influences of other study characteristics besides ethnicities, such as gender and comorbidities (hypertension or diabetes) on the effect of prior nicorandil in STEMI patients receiving primary PCI were unknown since the stratified results according to these characteristics were rarely reported in the included RCTs. Future studies are warranted. Fifthly, the qualities of the included studies were moderate. Our findings should better be confirmed in future RCTs with high quality. Finally, the comparative efficacy of nicorandil and other agents that may also improve coronary microvascular dysfunction and obstruction, such as verapamil and diltiazem46 adenosine, nicardipine, nicorandil and sodium nitroprusside,47 should also be determined in future studies.
To sum up, this meta-analysis showed that periprocedural nicorandil improves coronary blood flow, cardiac systolic function and prognosis in STEMI patients receiving primary PCI. Treatment with nicorandil prior to primary PCI should be recommended in STEMI patients.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ibanez B, James S, Agewall S, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119–177. doi:10.1093/eurheartj/ehx393
2. [Guideline on the diagnosis and therapy of ST-segment elevation myocardial infarction]. Zhonghua Xin Xue Guan Bing Za Zhi. 2015;43(5):380–393.
3. Shvartsur R, Shiyovich A, Gilutz H, Azab AN, Plakht Y. Short and long-term prognosis following acute myocardial infarction according to the country of origin. Soroka acute myocardial infarction II (SAMI II) project. Int J Cardiol. 2018;259:227–233. doi:10.1016/j.ijcard.2018.02.079
4. Li GX, Zhou B, Qi GX, et al. Current trends for ST-segment elevation myocardial infarction during the past 5 years in rural areas of China’s liaoning province: a multicenter study. Chin Med J (Engl). 2017;130(7):757–766. doi:10.4103/0366-6999.202742
5. Bulluck H, Foin N, Tan JW, Low AF, Sezer M, Hausenloy DJ. Invasive assessment of the coronary microcirculation in reperfused ST-segment-elevation myocardial infarction patients: where do we stand? Circ Cardiovasc Interv. 2017;10(3). doi:10.1161/CIRCINTERVENTIONS.116.004373
6. Niccoli G, Scalone G, Lerman A, Crea F. Coronary microvascular obstruction in acute myocardial infarction. Eur Heart J. 2016;37(13):1024–1033. doi:10.1093/eurheartj/ehv484
7. Taqueti VR, Di Carli MF. Coronary microvascular disease pathogenic mechanisms and therapeutic options: JACC state-of-the-art review. J Am Coll Cardiol. 2018;72(21):2625–2641. doi:10.1016/j.jacc.2018.09.042
8. Tarkin JM, Kaski JC. Vasodilator therapy: nitrates and nicorandil. Cardiovasc Drugs Ther. 2016;30(4):367–378. doi:10.1007/s10557-016-6668-z
9. Frampton J, Buckley MM, Nicorandil FA. A review of its pharmacology and therapeutic efficacy in angina pectoris. Drugs. 1992;44(4):625–655. doi:10.2165/00003495-199244040-00008
10. Tarkin JM, Kaski JC. Nicorandil and long-acting nitrates: vasodilator therapies for the management of chronic stable angina pectoris. Eur Cardiol. 2018;13(1):23–28. doi:10.15420/ecr.2018.9.2
11. Zhu H, Xu X, Fang X, Zheng J, Chen T, Huang J. Effects of mitochondrial ATP-sensitive potassium channel activation (nicorandil) in patients with angina pectoris undergoing elective percutaneous coronary interventions: a meta-analysis of randomized controlled trials. Medicine (Baltimore). 2019;98(3):e14165. doi:10.1097/MD.0000000000014165
12. Lee JM, Kato D, Oi M, et al. Safety and efficacy of intracoronary nicorandil as hyperaemic agent for invasive physiological assessment: a patient-level pooled analysis. EuroIntervention. 2016;12(2):e208–e215. doi:10.4244/EIJV12I2A34
13. Markham A, Plosker GL, Goa KL. Nicorandil. An updated review of its use in ischaemic heart disease with emphasis on its cardioprotective effects. Drugs. 2000;60(4):955–974. doi:10.2165/00003495-200060040-00007
14. Wu M, Huang Z, Xie H, Zhou Z. Nicorandil in patients with acute myocardial infarction undergoing primary percutaneous coronary intervention: a systematic review and meta-analysis. PLoS One. 2013;8(10):e78231. doi:10.1371/journal.pone.0078231
15. Ito H, Taniyama Y, Iwakura K, et al. Intravenous nicorandil can preserve microvascular integrity and myocardial viability in patients with reperfused anterior wall myocardial infarction. J Am Coll Cardiol. 1999;33(3):654–660.
16. Fukuzawa S, Ozawa S, Inagaki M, et al. Nicorandil affords cardioprotection in patients with acute myocardial infarction treated with primary percutaneous transluminal coronary angiosplasty: assessment with thallium-201/iodine-123 BMIPP dual SPECT. J Nucl Cardiol. 2000;7(5):447–453. doi:10.1067/mnc.2000.107273
17. Ikeda N, Yasu T, Kubo N, et al. Nicorandil versus isosorbide dinitrate as adjunctive treatment to direct balloon angioplasty in acute myocardial infarction. HeartHeart. 2004;90(2):181–185. doi:10.1136/hrt.2003.013789
18. Nameki M, Ishibashi I, Miyazaki Y, et al. Comparison between nicorandil and magnesium as an adjunct cardioprotective agent to percutaneous coronary intervention in acute anterior myocardial infarction. Circ J. 2004;68(3):192–197.
19. Ono H, Osanai T, Ishizaka H, et al. Nicorandil improves cardiac function and clinical outcome in patients with acute myocardial infarction undergoing primary percutaneous coronary intervention: role of inhibitory effect on reactive oxygen species formation. Am Heart J. 2004;148(4):1–7.
20. Ishii H, Ichimiya S, Kanashiro M, et al. Impact of a single intravenous administration of nicorandil before reperfusion in patients with ST-segment-elevation myocardial infarction. Circulation. 2005;112(9):1284–1288. doi:10.1161/CIRCULATIONAHA.104.530329
21. Kasama S, Toyama T, Kumakura H, et al. Effects of nicorandil on cardiac sympathetic nerve activity after reperfusion therapy in patients with first anterior acute myocardial infarction. Eur J Nucl Med Mol Imaging. 2005;32(3):322–328. doi:10.1007/s00259-004-1672-0
22. Akagi T, Sarazawa K, Inai Y, et al. Continuous administration of nicorandil decreases QT dispersion during the chronic phase of acute myocardial infarction. Int Heart J. 2006;47(3):351–361.
23. Miyazawa A, Ikari Y, Tanabe K, et al. Intracoronary nicorandil prior to reperfusion in acute myocardial infarction. EuroIntervention. 2006;2(2):211–217.
24. Ota S, Nishikawa H, Takeuchi M, et al. Impact of nicorandil to prevent reperfusion injury in patients with acute myocardial infarction – Sigmart Multicenter Angioplasty Revascularization Trial (SMART). Circ J. 2006;70(9):1099–1104.
25. Toyama T, Seki R, Hoshizaki H, et al. Nicorandil administration shows cardioprotective effects in patients with poor TIMI and collateral flow as well as good flow after AMI. Ann Nucl Med. 2006;20(4):277–285.
26. Fujiwara T, Matsunaga T, Kameda K, et al. Nicorandil suppresses the increases in plasma level of matrix metalloproteinase activity and attenuates left ventricular remodeling in patients with acute myocardial infarction. Heart Vessels. 2007;22(5):303–309. doi:10.1007/s00380-007-0975-z
27. Kitakaze M, Asakura M, Kim J, et al. Human atrial natriuretic peptide and nicorandil as adjuncts to reperfusion treatment for acute myocardial infarction (J-WIND): two randomised trials. Lancet. 2007;370(9597):1483–1493. doi:10.1016/S0140-6736(07)61634-1
28. Han CL, Sung GA, Choi JH, et al. Effect of intra-coronary nicorandil administration prior to reperfusion in acute ST segment elevation myocardial infarction. Circ J. 2008;72(9):1425–1429.
29. Goenka L, George M, Karthikeyan B. Does periprocedural nicorandil improve cardiovascular outcomes in acute myocardial infarction? Meta-analysis. J Evid Based Med Healthc. 2016;3(97):5348–5357. doi:10.18410/jebmh/2016/1112
30. Yamada K, Isobe S, Ishii H, et al. Impacts of nicorandil on infarct myocardium in comparison with nitrate: assessed by cardiac magnetic resonance imaging. Heart Vessels. 2016;31(9):1430–1437. doi:10.1007/s00380-015-0752-3
31. Wang ZQ, Chen MX, Liu DL, et al. [The effect on myocardial perfusion and clinical outcome of intracoronary nicorandil injection prior to percutaneous coronary intervention in ST-segment elevation myocardial infarction]. Zhonghua Xin Xue Guan Bing Za Zhi. 2017;45(1):26–33. doi:10.3760/cma.j.issn.0253-3758.2017.01.006
32. Feng C, Liu Y, Wang L, Niu D, Han B. Effects of early intracoronary administration of nicorandil during percutaneous coronary intervention in patients with acute myocardial infarction. Heart Lung Circul. 2018. doi:10.1016/j.hlc.2018.05.097
33. Qi QJTHTZ. Intracoronary nicorandil and the prevention of the no-reflow phenomenon during primary percutaneous coronary intervention in patients with acute ST-segment elevation myocardial infarction. Med Sci Monit. 2018;24:2767–2776. doi:10.12659/MSM.906815
34. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. doi:10.1136/bmj.b2651
35. Higgins J, Green S. Cochrane handbook for systematic reviews of interventions version 5.1.0. Cochrane Collab. 2011. Available from:
36. Galasso G, Schiekofer S, D’Anna C, et al. No-reflow phenomenon: pathophysiology, diagnosis, prevention, and treatment. A review of the current literature and future perspectives. Angiology. 2014;65(3):180–189. doi:10.1177/0003319712474336
37. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–1558. doi:10.1002/sim.1186
38. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634.
39. Chen C, Fu X, Li W, et al. Intracoronary administration of anisodamine and nicorandil in individuals undergoing primary percutaneous coronary intervention for acute inferior myocardial infarction: a randomized factorial trial. Exp Ther Med. 2015;10(3):1059–1065. doi:10.3892/etm.2015.2623
40. Akai K, Wang Y, Sato K, et al. Vasodilatory effect of nicorandil on coronary arterial microvessels: its dependency on vessel size and the involvement of the ATP-sensitive potassium channels. J Cardiovasc Pharmacol. 1995;26(4):541–547.
41. Krombach GA, Higgins CB, Chujo M, Saeed M. Gadomer-enhanced MR imaging in the detection of microvascular obstruction: alleviation with nicorandil therapy. Radiology. 2005;236(2):510–518. doi:10.1148/radiol.2362030847
42. Kostic J, Djordjevic-Dikic A, Dobric M, et al. The effects of nicorandil on microvascular function in patients with ST segment elevation myocardial infarction undergoing primary PCI. Cardiovasc Ultrasound. 2015;13:26. doi:10.1186/s12947-015-0020-9
43. Tritto I, Zuchi C, Vitale S, Ambrosio G. Therapy against reperfusion-induced microvascular injury. Curr Pharm Des. 2013;19(25):4586–4596.
44. Li Y, Liu H, Peng W, Song Z. Nicorandil improves clinical outcomes in patients with stable angina pectoris requiring PCI: a systematic review and meta-analysis of 14 randomized trials. Expert Rev Clin Pharmacol. 2018;11(9):855–865. doi:10.1080/17512433.2018.1508342
45. Zhao F, Chaugai S, Chen P, Wang Y, Wang DW. Effect of nicorandil in patients with heart failure: a systematic review and meta-analysis. Cardiovasc Ther. 2014;32(6):283–296. doi:10.1111/1755-5922.12097
46. Wang L, Cheng Z, Gu Y, Peng D. Short-term effects of verapamil and diltiazem in the treatment of no reflow phenomenon: a meta-analysis of randomized controlled trials. Biomed Res Int. 2015;2015:382086.
47. Salinas P, Jimenez-Valero S, Moreno R, et al. Update in pharmacological management of coronary no-reflow phenomenon. Cardiovasc Hematol Agents Med Chem. 2012;10(3):256–264.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.