Back to Journals » Journal of Multidisciplinary Healthcare » Volume 12
Next of kin’s protracted challenges with access to relevant information and involvement opportunities
Received 14 August 2018
Accepted for publication 15 November 2018
Published 18 December 2018 Volume 2019:12 Pages 1—8
DOI https://doi.org/10.2147/JMDH.S183946
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Anita Strøm,1 Anne Dreyer2
1Faculty of Health, VID Specialized University, Oslo, Norway; 2Department of Health Sciences in Ålesund, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology, Ålesund, Norway
Background: Next of kin are considered a resource for both the patient and the health service. Need for information varies with severity and duration of health changes. A clear requirement is about what to expect upon homecoming, and what supportive services are available. The picture of relatives’ access to involvement and information is still somewhat unclear.
Objective: To investigate what information, knowledge, and involvement next of kin considered important for managing their caring role and collaboration with their close relatives who experienced events that led to chronic illness.
Design, setting, and methods: A qualitative exploratory design. Seventeen informants were recruited through various courses offered to relatives. Data were collected in 2017 from individual interviews, analyzed in an interpretative tradition, and involved qualitative content analysis.
Results: The results reflect a long intervening period in between the activating incident and a clarification of the situation. This period was characterized by unpreparedness for duration of anxiety and amount of energy involved in balancing the relationship. Further, the interviewees saw retrospectively that information about disease and treatment was available, but they had to find such resources themselves. Information about how to handle the situation was almost absent. Ultimately, they were disappointed over not being involved.
Conclusion: Previously provided prospective information about the embedded anxiety in the situation and consequences for relationships, involvement in patients’ services, and better communication about existing services seem to be significant. Health care professionals, especially in outpatient care, may improve their services by debating how they can implement family-oriented care in personalized treatment as usual. Focus on prospective information, early involvement, and relevant information about existing resources may empower relatives and relieve the experience of care burden.
Keywords: next of kin, chronic illness, information, involvement, care burden, informal care, relatives
Introduction
In the Norwegian health care service, where the focus in recent years has shifted from specialist to primary care, relatives are considered a resource. Home treatment and early discharge after acute exacerbation have become a trend.1 Next of kin’s support is part of the natural care that characterizes close relationships and family and is considered significant to the patient’s health.2 Despite carers’ support as part of the natural care provided in close relationships, the literature more often associates the role of caregivers with words such as “care burden”.3–8 Guidelines on relatives in the health and care services commits both hospitals and municipalities to allow relatives involvement and provide them with support.9 Despite this, relatives are, to some extent, seen by the health care service as an independent entity with their own needs.
The literature describes a variety of need for information, involvement, and support.10–15 Research also provides examples of effective services aimed at relatives.16–18 Next of kin’s experienced information needs and involvement opportunities considered important for managing their caring role and collaboration with their close relatives are discussed in this article.
Background
Studies of relatives’ need for information reveal a multifaceted competence requirement. It varies with the nature, severity, and duration of health changes, and with personal skills and preferences. However, something appears to be common. Namely, for the next of kin, there is a need to understand the patient’s condition, symptoms, and disease development.11,12,19 There is also a common need to understand the consequences these have on the relative–patient relationship in regard to practical, everyday life, and communication.12,19–21 Relatives require knowledge that prepares them for the demanding experiences that often follow, which include consequences for their own mental and physical health.20–22 It is claimed that relatives are rarely given relevant information and support related to their own health or to dealing with their role as relatives.23–25
The role of relatives is challenged in situations like discharge from hospital and not finding available services.10,26 The care burden increases when relatives lack social and professional support.27 Furthermore, it can be a challenge for relatives to provide continuous support and care in a landscape of poorly defined, shared responsibilities among relatives, patients, and health care professionals. Relatives need support from and cooperation with health care professionals throughout the course of illness and need information that is adapted to their needs and preferences.28–30
There are good examples of approaches directed at relatives. Group education courses for patients and relatives appear to meet the needs for relevant exchanges of knowledge and support. These courses provide opportunities to meet other relatives and share experiences, which in turn provide opportunities to find new strategies for coping with everyday life.31,32 Different forms of therapeutic conversations directed toward families also seem to have an impact. Benefits that have been reported include a more comprehensive understanding of the situation, a more manageable situation, strengthened family relationships, and feelings of support. Findings of these studies suggest that offers of support to relatives should be made early in the process.33,34 Services that do not require conversation and presence have also been researched.35 An intervention study found that the combination of electronic and face-to-face interventions is most effective as support for informal caregivers.36
A need for services relevant to relatives has been identified. In public documents, these services are described in general terms as support groups, educational programs for relatives, and similar services.2 The picture of what relatives really need to handle their caring role, however, is still somewhat unclear and unspecific.
Methods
Aim
The purpose of the current study was to explore what information, knowledge, and involvement next of kin considered important for managing their caring role and cooperation with their close relatives who experienced events that led to chronic illness.
Design
The study used a qualitative exploratory design.
Participants
Seventeen informants were recruited from different courses for relatives of patients with long-term health challenges. We chose to include relatives who attended first-time courses regardless of age, type of chronic illness, or duration of next of kinship. All relatives who participated in a course at a Norwegian hospital’s Learning and Coping Center (LCC) in the spring of 2017 were requested orally and in writing (via the course leader) to participate in individual interviews. Any statement of consent was sent directly to the researcher, so that those who recruited did not know who had agreed to participate. The sample size was considered sufficient to provide information power mainly due to the aim of the study and the quality of interview dialog, despite heterogeneity of the sample.37 Table 1 describes the sample.
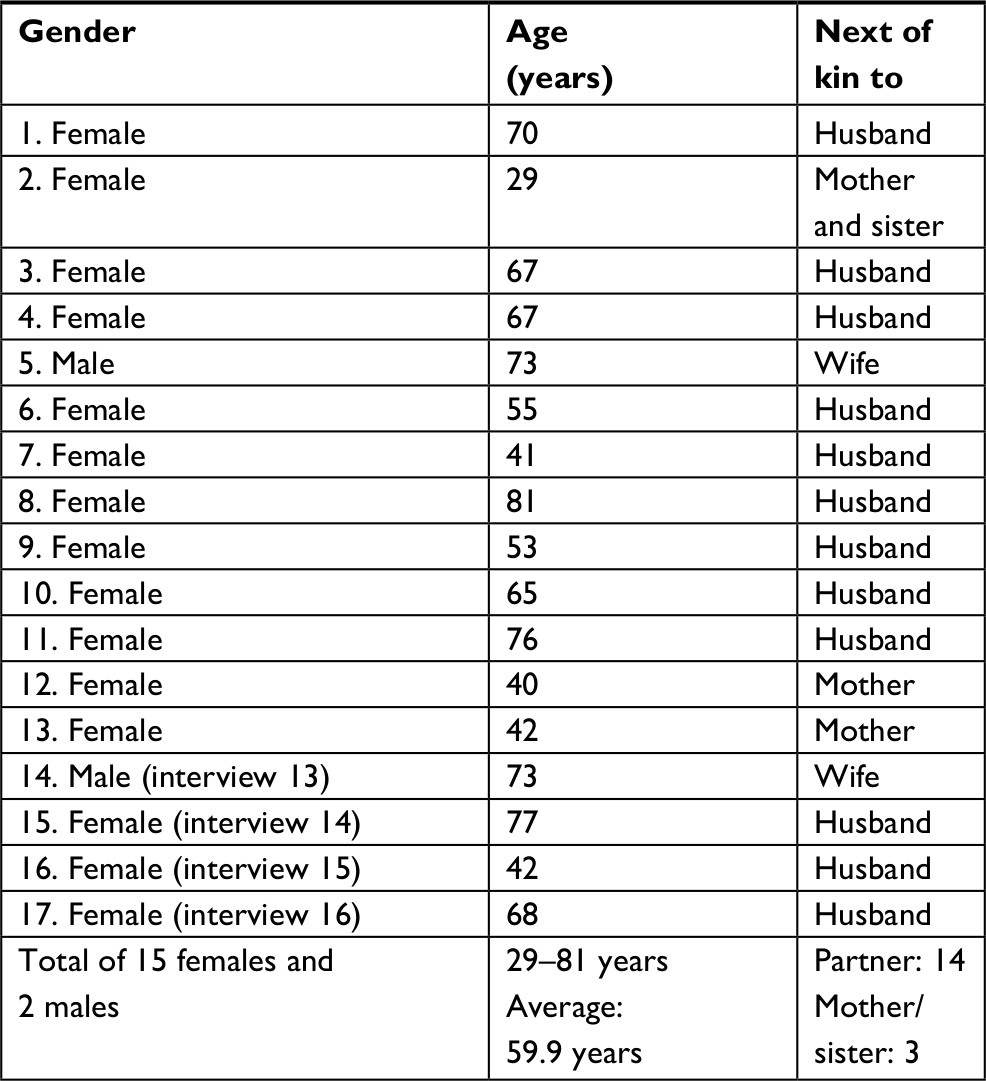 | Table 1 The sample described by gender, age, and relationship |
Data collection
Data were collected from individual interviews. The interviews were led by a thematic interview guide, with open questions to explore 1) how participants felt informed in the period as supportive relatives; 2) views on what knowledge and information they needed; 3) how they perceive themselves informed and involved; and 4) in what ways they would like access to information and relevant knowledge for their role. One of the researchers, with extensive experience of qualitative research interviews, conducted the interviews during spring of 2017. The qualitative interviews were conducted using the above theme, in an open dialog that took into account what the informants considered important.
Ethical considerations
The Data Protection Official for Research in Norway approved the study (Ref. no. 51380/12 01 2016). The investigation conforms to the principles outlined in the Declaration of Helsinki. Study participation was voluntary, all participants provided written informed consent, and all the patients agreed to their relatives’ participation.
Data analysis
The interviews were recorded and transcribed. The analyses were conducted in the interpretative tradition and involved qualitative content analysis, performed by both researchers.38 The text analysis of the transcribed interviews was conducted in different phases. First, each researcher did an open reading of all interviews and wrote a holistic essence of every interview. Thereafter, the researchers met together to conduct the first thematic analysis.39 Several preliminary themes were identified and named in the interviewees’ own words (eg, “worrying”, “uncertainty about limits”, “information jungle”, and “help yourself”). Then, from the main text, meaning units were extracted, condensed, and abstracted. Table 2 gives an illustration of one part of the analytical process, from transcription to main themes.
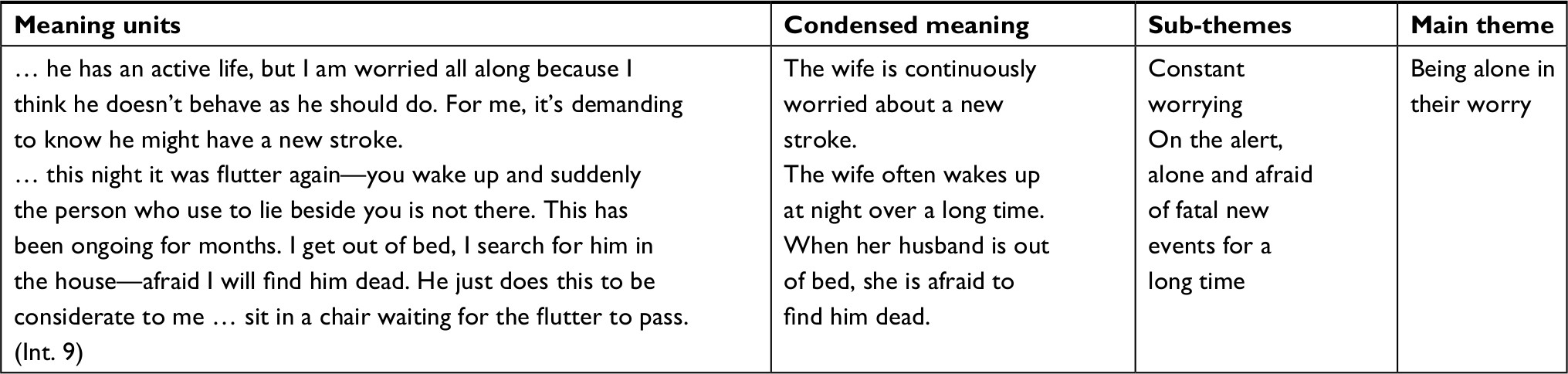 | Table 2 An illustration of a part of the analytic process – from data to main theme |
The final thematic analysis revealed three main themes related to “informational needs in limbo”: to be persistently anxious, to balance between encouragement and reassurance, and to find those persons and the services available.
Rigor
To achieve trustworthiness, the authors critically assessed and discussed all stages of the research bearing in mind the requirements for credibility, dependability, and transferability.40 Both authors read the transcripts independently, followed by discussions and co-analysis, to reach a mutual understanding of the findings, while being true to the meaning of the data.
Results
The results in this interview study reflect a long intervening period for the next of kin in between the triggering incident (eg, first suspicion of cognitive failure or chest pain) and a clarification of the patients’ situation. In retrospect, the next of kin expressed their unpreparedness for how long a period of time their anxiety lasted. The result was that their relationship to their respective patient became unstable. Further, they saw retrospectively that relevant information and courses were available, but they had to find such resources themselves.
Informational needs in limbo
Through the analysis of the interviews, a period of time emerges as a central feature of narratives. This period can be described as an interval – a limbo – the time between the acute scenario or the diagnostic point and a more settled situation via participating in courses or finding different services of a more permanent nature that is relevant to relatives too. This intervening period was described as lasting from a few months up to years. This period was characterized by almost absence of involvement of the next of kin, with some exceptions. A few of the relatives participated regularly in consultations in the outpatients’ department. If they were not directly invited, they were asked to be included.
Retrospectively, relatives were able to identify specific areas of everyday life where they could have needed professional help and support in that intervening period. Relational issue was one of them. The balance between being spot on or careless was mentioned. This was independent of type of chronic illness.
Those interviewed had few suggestions for new services. Their concern was that it was difficult to find existing resource persons and relevant services.
Being alone in their worry
Informants recognized it as normal to be frightened, shaken, and stirred when their next of kin became acute or progressively ill. The relatives were not prepared for the duration of this anxiety and worry. Moreover, it was demanding to discover that their own worry was out of step with their close ones:
I have been alert and very frightened – a longer period of time than I should have been. He was not much concerned about his own situation, and anxiety was transferred to me. Retrospectively, it is good to be aware that there are fewer risky things than I expected.
He wanted to travel, but I didn’t have any good feeling connected to that idea. It was too early. I felt responsible to react fast, and insecure of being far away from the city and the hospital.
Duration of the state of anxiety and the experience of being out of step with the patient led to a feeling of being alone in the situation. This loneliness was reinforced by silence in communication in relatives’ social networks:
Suddenly, I am regarded as the lonely, responsible carer for burdens and challenges. Friends have stopped asking, and neither can I give any answer to what will happen next or further deterioration.
Balancing between intervening and setting limits and letting the persons do what they want
The informants talked a lot about balancing between encouragement to activity and support for rest, between daring and taking into account, between being aware and understanding, and to normalize and overlook. This balancing act was regarded as both demanding and necessary. The informants were not prepared for the duration of this changed relational manner and mixed anticipation in their daily lives:
The stressed feeling of being educational is hard to bear. I want him to be as usual – funny, playful – but then I come to point a finger because I know – that’s a communicative balance – and this is a worry – more than I am aware of.
I am thinking much: What is he able to master, and what not? I have been continuously worried about his possible chest overstrain. Now I have learned he should be in normal activity and, ie, do the grass cutting. It’s really good to know; it makes me able to be more ignorant.
It is difficult to balance oneself in being supportive and demand her experience – not too much, not too little.
None of the informants was made aware of this imbalance between patient and relatives. Nobody had been informed by health personnel that this was something that could be expected and could last over time.
Finding those persons and the services available
The aim for the interviews was to explore what kind of information relatives needed and what kind of resources they wanted. In addition, constructive suggestions were sought for service improvement. Interviewees expressed their knowledge of available information, expertise, and technological resources but also expressed that it was difficult to find the relevant resources for their situations. These experiences revealed that they had to help themselves:
We have searched for much information by ourselves concerning medical treatment, consequences of disease, prospects, and information in general – because those needs have not been met. This is what we have been talking about: that is, there is a gap between the resources available and what is offered.
Obviously, a lot of information is available online. Several informants questioned the quality of this information that related to disease and treatment:
We make use of information online a lot, but you could become worse because there are uncritical people out there. I try searching for health educational sites. Such web forums might be counter-productive.
In addition, the informants were doubtful about the intentions and usefulness of the talks with the health care staff. Many of the relatives remarked the loss of a scheduled conversations or consultations. They questioned whether it was available or not and, in addition, how they could approach health personnel. There also seems to be a difference between relatives being invited to or actively taking initiative by themselves to approach health personnel when their partners met for consultations in the outpatients’ department:
When my husband eagerly wanted to return to his job, I wished somebody from the hospital said, “Come for a meeting.” I think we needed a name given to us, a person to be contacted.
I was never invited in together with my husband. If I had been there, I had got that information and could retrieve it and say, “Do you remember what they told you?
The informants referred to many situations where the coincidence caused them to receive information:
By a mere chance, I was present when the physiotherapist turned up. Then I learned much about what he can and cannot do.
While waiting for him, I saw a poster announcing a course for relatives twice a year. And, therefore, I was so surprised when I entered that course; we were eight participants, five spouses, and three grown up children. I supposed it was much more people present in such a great arrangement.
In addition, when discovering that there were relevant written information available, one of the informants in particular was frustrated because the health personnel did not use all of the relevant available written material:
While I am waiting, I look in the folders – look through. I am focused on the chronic aspects of it – and what kind of life it is possible to get in the future. What kind of obstacles and handicaps we will meet. I am careful not to mention it because I don’t paint it on the wall. There are a lot of leaflets available, but what is the use of them? Look through them and put them back. Somebody keeps them also. Actually, it should be more reasonable pushing people to bring these home, instead of leaving them there. It would be sensible to use those leaflets more actively.
The findings of the study deal with the duration of anxiety, the duration of imbalance in the relationship, and the long time it takes to find the right people and services that can provide information and support. Participants in the study do not request information on diagnosis or treatment. That information has both been received and found. They lack information that the professionals does not seem to have thought about and which includes longevity, changed relationships, and need for support.
Discussion
The results of the study are open for discussion of the consequences of insufficient information or involvement for the long interim period. It is natural, and known from the literature, that there must be a certain amount of time between initial events and a more clarified situation in terms of knowledge, understanding, and involvement. A current staged caregiver model has been developed by Aneshensel et al41 through research into dementia care. The model describes the development of caregiver career in three stages where the initial one is role acquisition and the next one is role enactment. This study’s participants found this first stage very long. No one had prepared them for it. One question to ask is what consequence such an indefinite period has on patients’ relatives.
The term “care burden” deals with perceived stresses for relatives and consequences for the next of kin’s own health in the broad sense. This burden can be linked to “care burden responsibilities”, which include support for activities of daily living, emotional support, symptom registration, and “role strains” that comprise relatives’ support for the patients. Next of kin must be both supportive and responsible and have to deal with their own reaction to changes in the relationship. Lack of social and professional support further increases the perception of care burden.27 Other studies focusing on the “care burden” suggest that time spent in the role and how long they have been relatives affect the degree of perceived care burden.3,42 Such longevity can be assumed a cost, also health-related, as relatives who experience greater care burden are more prone to more stress and their own illness.
One study found that relatives with a high level of “role strain” at the time of diagnosis also had the same high level after 1 year.43 This may imply a need for health care professionals to map the relatives’ initial experience of the situation. A randomized controlled trial found that the load and negative health effects did not significantly decrease after a follow-up program of relatives of patients with heart disease. Mapping relatives’ initial experiences may also provide a better customized follow-up program.44 This emphasizes the importance of both early and adapted support for relatives.34 One can assume that early information about anxiety, imbalance in relationship, and available services can reduce the impact of time on the perception of care burden. The mentioned caregiver model identify a need for early interventions in the first stage.41 Locating help for both patient and family is described as a core issue. There is still an open question about who is responsible for locating help when it comes to relatives, and where this will or may take place.
Participants in our study generally seemed satisfied with the information they received during the initial events. The information was aimed at the condition, symptoms, and disease development of the patient and was perceived as relevant. In the mid-term (limbo phase), relatives expressed that there were also other topics they were dealing with, such as their relationships with the ill and how to live together when their everyday lives changed. The relatives sought normality and a recovery of balance in their relationships. The long median period is characterized by emotional impact and concern, sometimes to a greater extent and longer duration for relatives than for the patients themselves. That these are common experiences and expressions of information and involvement needs are known from the research literature.10–15 The study’s informants wondered afterwards why the information they had received was so little provident. For example, they understood that one cannot be truly prepared for how troubled and worried one would become, but they still wanted to be informed that they would become troubled and worried. One of the issues seems to be that in the time around initial events and in meetings with the health service, prospective information has a low focus. For relatives to be able to prepare, acquire relevant knowledge, and gain control over the situation, the information provided must not only be oriented on the immediate situation but also forward-looking. More prospective information could be considered preventive health care.
Many relatives had to take initiative to become involved. When the health care staff did not involve them, for some, this increased the imbalances in their relationship with the patient. The results of a review on family-centered theory indicate that attitudes are a barrier to implementing family-oriented approaches.45 Taking a family perspective on long-term illness will have consequences for how health personnel should also relate to patients’ immediate relatives. Without the right opportunities, relatives may be excluded from a place they are entitled to in treatment and follow-up from the health service. Both professional and political guidance are far more apparent in the involvement of relatives of adult patients than a few years ago. This is, among other things, based on knowledge of the importance of care for the patient and his/her close ones as a unit in order to prevent unhealthiness.45 A public Norwegian guideline about next of kin in the health care service points out clearly the following:
Adult relatives with care tasks and/or loads should be offered individually adapted support and relief, training and guidance. This applies especially to relatives with demanding care tasks and loads.9
The findings in our study show that there is a large discrepancy between the relatives’ experiences and this guideline. There is a period after diagnosis, a limbo of considerable duration, where relatives do not receive proper care. Spouses of the serious chronically ill strive to create continuity in their lives.46,47 Here, organized support and relief services, training, guidance, and information should be central. It is part of what is encompassed in the concept of sound and caring health care in accordance with Norwegian legislation.48
Our study shows the informants’ descriptions of how they discovered through their own initiative (and almost randomly) different services and offers that they considered relevant. There seems to be a lack of structure in orientation about the opportunities to participate in courses and information meetings, along with the opportunities to participate in consultations and access low-threshold psychological help. This seems to represent a resource issue because existing services are not easily identifiable or available, but must be discovered through relatives’ own initiative. During the long to medium period in which we have turned on the spotlights, most of the relatives found, by themselves, a lot of what they were looking for. The authors’ interpretation of the findings is that relegation offers are fragmented and not very systematic.
Limitations
Next of kin were recruited from different courses at an LCC serving two hospitals. Their experiences with information access and how they were involved may be contextual. At the same time, the informants were relatives of patients with different long-term health changes and belonged to different departments, outpatient clinics, and general practitioners. All informants had, at the time of the interview, achieved more clarity regarding their roles and the need for competence.
Conclusion
Relatives wish to handle both the patients’ and their own situation. Previously provided prospective information about the embedded anxiety in the situation and consequences for relationships, involvement in patients’ services, and better communication about existing services seem to be significant. It appears that simple steps can be taken to satisfy relatives’ requests. It also appears that there is a lack of awareness about family-centered care, which is not necessarily easy to establish. Health care professionals, especially in outpatient care, can improve their services by debating how they can implement family-oriented care in personalized treatment as usual. Focus on prospective information, early involvement, and relevant information about existing resources may empower relatives and relieve the experience of care burden.
Acknowledgments
We thank Maxi Storm and Unni Martinsen, both leaders at the current LCC, for assistance with recruiting informants and for genuine interest in the project. The study is funded through our institutional affiliations.
Disclosure
The authors report no conflicts of interest in this work.
References
Ministry of the Health and Care Services. Report No. 47 to the Storting (2008–2009). The Coordination Reform — Proper Treatment – At the Right Place and Right Time. Oslo: Ministry of the Health and Care Services; 2009. | ||
Ministry of Health and Care Services. Morgendagens omsorg (Future Care). In. Meld. St. 29 (2012–2013). Oslo: Departementenes servicesenter; 2013:140 s. | ||
Luttik ML, Jaarsma T, Tijssen JG, van Veldhuisen DJ, Sanderman R. The objective burden in partners of heart failure patients; development and initial validation of the Dutch Objective Burden Inventory. Eur J Cardiovasc Nurs. 2008;7(1):3–9. | ||
Luttik ML, Jaarsma T, Veeger N, Tijssen J, Sanderman R, van Veldhuisen DJ. Caregiver burden in partners of Heart Failure patients; limited influence of disease severity. Eur J Heart Fail. 2007;9(6–7):695–701. | ||
Strömberg A, Luttik ML. Burden of caring: risks and consequences imposed on caregivers of those living and dying with advanced heart failure. Curr Opin Support Palliat Care. 2015;9(1):26–30. | ||
Olai L, Borgquist L, Svärdsudd K. Life situations and the care burden for stroke patients and their informal caregivers in a prospective cohort study. Ups J Med Sci. 2015;120(4):290–298. | ||
Grov EK, Fosså SD, Sørebø O, Dahl AA. Primary caregivers of cancer patients in the palliative phase: a path analysis of variables influencing their burden. Soc Sci Med. 2006;63(9):2429–2439. | ||
Gautun H, Werner A, Lurås H. Care challenges for informal caregivers of chronically ill lung patients: results from a questionnaire survey. Scand J Public Health. 2012;40(1):18–24. | ||
The Norwegian Directorate of Health. Veileder om pårørende i helse- og omsorgstjenesten (Guidelines for Relatives in the Health and Care Rervices). Oslo: The Norwegian Directorate of Health; 2017. | ||
White CL, Brady TL, Saucedo LL, Motz D, Sharp J, Birnbaum LA. Towards a better understanding of readmissions after stroke: partnering with stroke survivors and caregivers. J Clin Nurs. 2015;24(7–8):1091–1100. | ||
Hafsteinsdóttir TB, Vergunst M, Lindeman E, Schuurmans M. Educational needs of patients with a stroke and their caregivers: a systematic review of the literature. Patient Educ Couns. 2011;85(1):14–25. | ||
Ducharme F, Kergoat MJ, Coulombe R, Lévesque L, Antoine P, Pasquier F. Unmet support needs of early-onset dementia family caregivers: a mixed-design study. BMC Nurs. 2014;13(1):49. | ||
Solomi VL, Casiday RE. In sickness and in health: the strains and gains of caring for a chronically ill or disabled spouse. Chronic Illn. 2017;13(2):75–87. | ||
Näsström L, Luttik ML, Idvall E, Strömberg A. Exploring partners’ perspectives on participation in heart failure home care: a mixed-method design. J Adv Nurs. 2017;73(5):1208–1219. | ||
Happell B, Wilson K, Platania-Phung C, Stanton R. Filling the gaps and finding our way: family carers navigating the healthcare system to access physical health services for the people they care for. J Clin Nurs. 2017;26(13–14):1917–1926. | ||
Han A, Radel J. Spousal caregiver perspectives on a person-centered social program for partners with dementia. Am J Alzheimers Dis Other Demen. 2016;31(6):465–473. | ||
Parker C, Teel C, Leenerts MH, Macan A. A theory-based self-care talk intervention for family caregiver-nurse partnerships. J Gerontol Nurs. 2011;37(1):30–35. | ||
Regan TW, Lambert SD, Girgis A, Kelly B, Kayser K, Turner J. Do couple-based interventions make a difference for couples affected by cancer? A systematic review. BMC Cancer. 2012;12:279. | ||
Lu YF, Haase JE. Experience and perspectives of caregivers of spouse with mild cognitive impairment. Curr Alzheimer Res. 2009;6(4):384–391. | ||
Gullick J, Krivograd M, Taggart S, Brazete S, Panaretto L, Wu J. A phenomenological construct of caring among spouses following acute coronary syndrome. Med Health Care Philos. 2017;20(3):393–404. | ||
Agren S, Frisman GH, Berg S, Svedjeholm R, Strömberg A. Addressing spouses’ unique needs after cardiac surgery when recovery is complicated by heart failure. Heart Lung. 2009;38(4):284–291. | ||
Li QP, Mak YW, Loke AY. Spouses’ experience of caregiving for cancer patients: a literature review. Int Nurs Rev. 2013;60(2):178–187. | ||
Caress AL, Luker KA, Chalmers KI, Salmon MP. A review of the information and support needs of family carers of patients with chronic obstructive pulmonary disease. J Clin Nurs. 2009;18(4):479–491. | ||
Stenberg U, Cvancarova M, Ekstedt M, Olsson M, Ruland C. Family caregivers of cancer patients: perceived burden and symptoms during the early phases of cancer treatment. Soc Work Health Care. 2014;53(3):289–309. | ||
Stenberg U, Ekstedt M, Olsson M, Ruland CM. Living close to a person with cancer: a review of the international literature and implications for social work practice. J Gerontol Soc Work. 2014;57(6–7):531–555. | ||
Ivarsson B, Larsson S, Lührs C, Sjöberg T. Serious complications in connection with cardiac surgery – next of kin’s views on information and support. Intensive Crit Care Nurs. 2011;27(6):331–337. | ||
Strömberg A. The situation of caregivers in heart failure and their role in improving patient outcomes. Curr Heart Fail Rep. 2013;10(3):270–275. | ||
Liljeroos M, Agren S, Jaarsma T, Strömberg A. Perceived caring needs in patient-partner dyads affected by heart failure: a qualitative study. J Clin Nurs. 2014;23(19–20):2928–2938. | ||
Doherty LC, Fitzsimons D, McIlfatrick SJ. Carers’ needs in advanced heart failure: a systematic narrative review. Eur J Cardiovasc Nurs. 2016;15(4):203–212. | ||
Wallengren C, Segesten K, Friberg F. Relatives’ information needs and the characteristics of their search for information – in the words of relatives of stroke survivors. J Clin Nurs. 2010;19(19–20):2888–2896. | ||
Ivarsson B, Klefsgård R, Nilsson GC. Experiences of group education – a qualitative study from the viewpoint of patients and peers, next of kin and healthcare professionals. Nord J Nurs Res. 2011;31(2):35–39. | ||
Stenberg U, Haaland-Øverby M, Fredriksen K, Westermann KF, Kvisvik T. A scoping review of the literature on benefits and challenges of participating in patient education programs aimed at promoting self-management for people living with chronic illness. Patient Educ Couns. 2016;99(11):1759–1771. | ||
Halldórsdóttir BS, Svavarsdóttir EK. Purposeful therapeutic conversations: are they effective for families of individuals with COPD: a quasi-experimental study. Nord J Nurs Res. 2012;32(1):48–51. | ||
Benzein E, Olin C, Persson C. ‘You put it all together’ – families’ evaluation of participating in family health conversations. Scand J Caring Sci. 2015;29(1):136–144. | ||
Torp S, Hanson E, Hauge S, Ulstein I, Magnusson L. A pilot study of how information and communication technology may contribute to health promotion among elderly spousal carers in Norway. Health Soc Care Community. 2008;16(1):75–85. | ||
Torp S, Bing-Jonsson PC, Hanson E. Experiences with using information and communication technology to build a multi-municipal support network for informal carers. Inform Health Soc Care. 2013;38(3):265–279. | ||
Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. 2015;26(13):1753–1760. | ||
Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. | ||
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. | ||
Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. | ||
Aneshensel CS. Profiles in Caregiving: The Unexpected Career. San Diego: Academic Press; 1995. | ||
Saunders MM. Factors associated with caregiver burden in heart failure family caregivers. West J Nurs Res. 2008;30(8):943–959. | ||
Wagner CD, Tanmoy Das L, Bigatti SM, Storniolo AM. Characterizing burden, caregiving benefits, and psychological distress of husbands of breast cancer patients during treatment and beyond. Cancer Nurs. 2011;34(4):E21–E30. | ||
Liljeroos M, Ågren S, Jaarsma T, Årestedt K, Strömberg A. Long-term effects of a dyadic psycho-educational intervention on caregiver burden and morbidity in partners of patients with heart failure: a randomized controlled trial. Qual Life Res. 2017;26(2):367–379. | ||
Bamm EL, Rosenbaum P. Family-centered theory: origins, development, barriers, and supports to implementation in rehabilitation medicine. Arch Phys Med Rehabil. 2008;89(8):1618–1624. | ||
Aasbø G, Solbraekke KN, Kristvik E, Werner A. Between disruption and continuity: challenges in maintaining the ‘biographical we’ when caring for a partner with a severe, chronic illness. Sociol Health Illn. 2016;38(5):782–796. | ||
Bove DG, Zakrisson AB, Midtgaard J, Lomborg K, Overgaard D. Undefined and unpredictable responsibility: a focus group study of the experiences of informal caregiver spouses of patients with severe COPD. J Clin Nurs. 2016;25(3–4):483–493. | ||
The Health Personell Act. Lov om helsepersonell m.v. LOV-1999-07-02-64. 1999. Available from: https://lovdata.no/dokument/NL/lov/1999-07-02-64#KAPITTEL_3. Accessed December 7, 2018. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.