Back to Journals » Drug Design, Development and Therapy » Volume 20
Next-Generation Pharmacotherapy for Depressive Disorders: From Novel Compounds to Optimized Use of Available Drugs
Authors Bu F ![]() , Qin L, Lou Z, Xie Y, Zhang S, Xiong L
, Qin L, Lou Z, Xie Y, Zhang S, Xiong L ![]() , Wen Y
, Wen Y ![]()
Received 24 March 2026
Accepted for publication 19 May 2026
Published 27 May 2026 Volume 2026:20 609327
DOI https://doi.org/10.2147/DDDT.S609327
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Anastasios Lymperopoulos
Fan Bu,1 Lan Qin,2,* Zhengchi Lou,3,* Yanfang Xie,4 Shaojian Zhang,4 Lile Xiong,4 Yi Wen4
1Department of Neurology, Dongzhimen Hospital Affiliated to Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 2Department of Neonatology, Shenzhen People’s Hospital, Shenzhen, Guangdong, People’s Republic of China; 3Department of Traditional Chinese Medicine, The Third Affiliated Hospital of Henan Medical University, Xinxiang, Henan, People’s Republic of China; 4Department of Thoracic Surgery, Shenzhen People’s Hospital, Shenzhen, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lile Xiong, Email [email protected] Yi Wen, Email [email protected]
Abstract: Depressive disorders remain a major source of disability worldwide, and many patients do not achieve sustained remission despite the availability of multiple antidepressant options. Unmet needs are particularly evident in treatment-resistant depression (TRD) and bipolar depression, where delayed onset of action, incomplete response, relapse, residual functional impairment, and tolerability limitations reduce the practical value of conventional monoaminergic strategies. This clinically oriented narrative review examines next-generation pharmacotherapy for depressive disorders from a drug-centered and mechanism-informed perspective. A targeted literature search was conducted across major biomedical and psychological databases and was supplemented by regulatory documents, prescribing information, pharmacogenomic recommendations, and selected real-world evidence. Representative next-generation approaches include N-methyl-D-aspartate (NMDA) receptor modulators and other rapid-acting agents, dextromethorphan–bupropion, multimodal antidepressants, neuroactive steroid-related therapies such as brexanolone and zuranolone, psychedelic-assisted pharmacotherapy, kappa-opioid receptor antagonists, and bipolar-relevant mood-stabilizing pharmacotherapies. The review also discusses mechanism-informed optimization of available drugs, including repurposing, augmentation, rational combination pharmacotherapy, dose and sequencing strategies, maintenance-oriented prescribing, and measurement-based care. Pharmacogenomics, pharmacokinetic/pharmacodynamic variability, and clinical stratification are considered as practical components of precision pharmacotherapy. Current evidence suggests that progress in depression pharmacotherapy depends not only on developing new compounds, but also on improving treatment selection, sequencing, monitoring, tolerability management, and sustained use in heterogeneous clinical populations. A next-generation framework should therefore integrate novel drug classes with improved use of established agents, while remaining sensitive to differences among unipolar depression, bipolar depression, and TRD.
Keywords: depressive disorders, treatment-resistant depression, bipolar depression, rapid-acting antidepressants, neuroactive steroids, psychedelic-assisted therapy
Introduction
Depressive disorders remain among the most consequential conditions in global mental health because they combine high prevalence with recurrent suffering, functional loss, and considerable long-term burden for patients, families, and health systems.1 Although the pharmacological armamentarium for depression has expanded substantially over the past several decades, routine clinical care still falls short of what many patients need. Some individuals do not respond meaningfully to treatment. Others improve only partially but continue to live with anergia, insomnia, anxious distress, cognitive inefficiency, emotional blunting, or occupational and social impairment. Still others initially respond and then relapse, or discontinue treatment because the burden of adverse effects outweighs the perceived benefit.2 In real-world practice, these limitations may be as clinically important as statistical separation from placebo under tightly controlled trial conditions.
The limitations of standard treatment become especially visible in treatment-resistant depression and bipolar depression. TRD exposes the weaknesses of a purely serial strategy in which one antidepressant is followed by another broadly similar one after an adequate but unsuccessful trial. Once several monoaminergic approaches have failed, additional substitutions within the same general pharmacological logic may offer diminishing informational value.3 Bipolar depression reveals a different problem. In bipolar illness, symptomatic improvement cannot be evaluated independently of switching risk, activation, mixed features, and the longer-term requirement for polarity stability.4 A treatment may appear useful if judged only by short-term symptom scores while still being unsatisfactory if it destabilizes the broader course of illness.
For these reasons, contemporary discussion of depression pharmacotherapy increasingly turns to the idea of “next-generation” treatment. Yet the term is often used too loosely, as if any recently marketed product necessarily represented meaningful therapeutic progress. A more clinically useful view is that next-generation pharmacotherapy refers to treatments that alter the therapeutic equation in ways that matter to patients and clinicians. This may involve mechanistic novelty, faster symptom relief, usefulness in difficult-to-treat populations, improved tolerability or sustainability, or better matching between patient profile and drug selection.5 Under that definition, genuinely novel compounds and better use of established drugs belong in the same conceptual field.
This broader view is important because depressive disorders are pharmacologically heterogeneous even when diagnostically grouped together. Patients with psychomotor slowing, anxious distress, insomnia, or bipolar-spectrum instability may all meet criteria for depression while requiring different treatment logic. Conventional monoaminergic models remain clinically relevant, but they have not resolved incomplete remission, relapse, functional impairment, or poor tolerability. The field increasingly needs drug strategies that do more than reproduce the same mechanism with minor variations.6
This narrative review therefore adopts a pharmacotherapy-centered but clinically integrative perspective. Its aim is not to provide an exhaustive systematic synthesis of every emerging treatment, but to examine representative drug classes and pharmacological strategies that illustrate how depression treatment is evolving. The emphasis is on mechanism of action, clinical positioning, safety and tolerability, and the practical issue of how treatments can be used in unipolar depression, bipolar depression, and TRD. Non-pharmacological interventions such as psychotherapy, neuromodulation, and electroconvulsive therapy are beyond the scope of the present review. Within this framework, progress in depression pharmacotherapy arises from two converging routes: the development of new compounds and the mechanism-informed optimization of available drugs. In this review, the term depressive disorders is used primarily to refer to major depressive disorder, treatment-resistant depression, postpartum depression where relevant to neuroactive steroid therapies, and bipolar depression as a polarity-sensitive depressive condition.
Review Scope and Literature Search Strategy
This article is a clinically oriented narrative review rather than a systematic review or meta-analysis. A targeted literature search was conducted across PubMed/MEDLINE, Embase, Web of Science, Scopus, the Cochrane Library, and PsycINFO, supplemented by Google Scholar searches and reference-list screening from database inception to March 1, 2026. Search terms included combinations of “major depressive disorder”, “depressive disorders”, “treatment-resistant depression”, “bipolar depression,” “rapid-acting antidepressants,” “NMDA receptor modulators,” “ketamine,” “esketamine,” “dextromethorphan-bupropion,” “multimodal antidepressants,” “neuroactive steroids,” “zuranolone,” “brexanolone,” “psilocybin,” “psychedelic-assisted therapy,” “kappa-opioid receptor antagonists,” “aticaprant,” “navacaprant,” “augmentation,” “combination pharmacotherapy,” “measurement-based care,” “pharmacogenomics,” “pharmacokinetics,” “pharmacodynamics,” and “precision pharmacotherapy.”
Eligible sources included randomized controlled trials, pivotal clinical trials, meta-analyses, systematic reviews, narrative reviews, treatment guidelines, regulatory documents, prescribing information, pharmacogenomic recommendations, translational studies, and selected real-world evidence reports. Priority was given to studies and documents with direct relevance to pharmacological mechanisms, clinical efficacy, safety and tolerability, regulatory status, treatment positioning, and real-world implementation. Because this was a narrative review, literature selection was purposive rather than exhaustive, and priority was given to clinically relevant, regulatory, guideline-based, and mechanistically informative sources. Formal PRISMA-based screening, quantitative synthesis, and risk-of-bias assessment were not performed.
Defining Next-Generation Pharmacotherapy in Depressive Disorders
The term “next-generation” is most useful when defined by clinical and pharmacological value rather than by recency alone. In depressive disorders, a treatment should be considered next-generation when it improves one or more domains in a clinically meaningful way: target engagement beyond conventional monoaminergic mechanisms, speed of symptom reduction, utility in difficult-to-treat populations such as TRD or bipolar depression, tolerability and sustainability of use, or greater precision in treatment selection. Under this framework, next-generation pharmacotherapy includes both novel compounds and the optimized, mechanism-informed use of established drugs when these approaches offer clinically meaningful advantages in speed, mechanistic diversity, tolerability, precision, durability, or real-world usability.7
This broader definition matters because therapeutic progress in depression does not emerge from a single pathway. One route is molecular and mechanistic novelty, as illustrated by rapid-acting glutamatergic strategies, neuroactive steroid-related approaches, and pharmacotherapies designed with greater relevance to bipolar depression. Another route is better use of what is already available. In routine practice, major advances often arise not because an entirely new drug appears, but because clinicians use existing drugs more intelligently through augmentation, rational combination treatment, dose optimization, improved sequencing, and maintenance planning.8 The next generation of treatment may therefore emerge as much from better pharmacological reasoning as from newer molecules.
The need for a broader definition also reflects the heterogeneity of depressive illness. Conventional antidepressant prescribing often begins from a relatively undifferentiated first-line model and becomes more individualized only after repeated failure. Next-generation pharmacotherapy, by contrast, starts from the assumption that better fit between drug mechanism and clinical context is itself a form of therapeutic innovation.
A functional definition also helps avoid two opposite mistakes: assuming that every new treatment is inherently superior, and assuming that older drugs are pharmacologically exhausted. In reality, a newly introduced agent may occupy only a narrow niche, whereas an established drug may gain new value through better augmentation, sequencing, or maintenance use. A next-generation framework is therefore best understood as a model of therapeutic fit, asking whether a drug or strategy meaningfully improves speed, mechanistic diversity, tolerability, stability, or long-term usability.
For that reason, this review treats next-generation pharmacotherapy as a drug-centered but clinically integrated field. Novel compounds are important because they broaden the mechanistic landscape beyond conventional serotonergic and noradrenergic antidepressants. At the same time, optimized use of available drugs remains equally important because the practical reality of depression care is determined not only by which drugs exist, but by how thoughtfully they are selected, combined, monitored, and continued over time. The central question is not which treatment is newest, but which treatment most meaningfully improves efficacy, safety, tolerability, implementation feasibility, and sustained clinical value.9
Novel Compounds and Emerging Drug Classes in Depressive Disorders
Novel compounds and emerging drug classes are expanding the pharmacological landscape of depressive disorders beyond traditional monoaminergic antidepressants.10 From a drug-development perspective, the most relevant advances include NMDA-related agents with rapid antidepressant effects, oral compounds with mixed or broadened mechanisms, neuroactive steroid-related approaches, psychedelic-assisted pharmacotherapy, kappa-opioid receptor antagonists, and mood-stabilizing pharmacotherapies with particular relevance to bipolar depression.11 What makes these agents important is not simply that they are newer. It is that they address problems that conventional antidepressant treatment has not solved adequately: delayed onset, mechanistic redundancy in resistant illness, incomplete symptom-domain coverage, and the need for polarity-sensitive treatment in bipolar depression.
To visualize the transition from traditional monoaminergic models to these diversified pathways, Figure 1 illustrates the primary neurobiological targets and downstream mechanisms of the representative next-generation compounds discussed in this section.
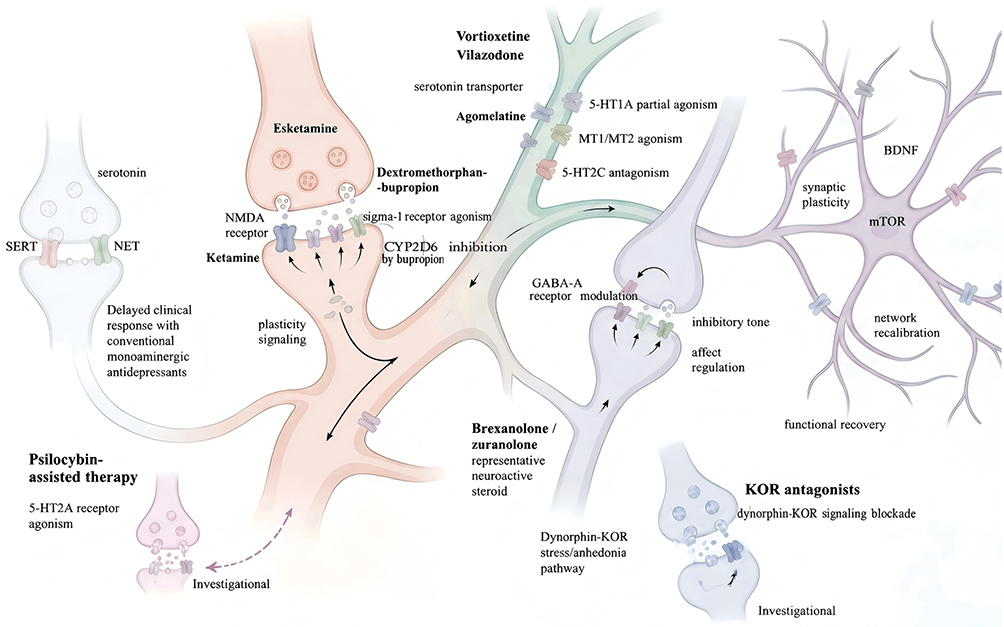 |
Figure 1 Mechanistic landscape of representative next-generation pharmacotherapies for depressive disorders. The figure summarizes major pharmacological pathways and representative therapeutic classes discussed in this review, including NMDA receptor modulation, multimodal serotonergic mechanisms, neuroactive steroid-related approaches, psychedelic-assisted therapy, kappa-opioid receptor antagonism, and bipolar-relevant mood-stabilizing strategies. Figure 1 was created by the authors and was not generated using BioRender or other third-party illustration software. |
NMDA Receptor Modulators and Rapid-Acting Antidepressants
Among emerging pharmacotherapies, NMDA receptor modulators have had the strongest impact on the conceptual development of next-generation antidepressant treatment. Esketamine nasal spray is approved in the United States for adults with treatment-resistant depression, administered either as monotherapy or in conjunction with an oral antidepressant, and for depressive symptoms in adults with major depressive disorder with acute suicidal ideation or behavior when used in conjunction with an oral antidepressant. However, its labeling should be interpreted carefully: the indication for MDD with acute suicidal ideation or behavior concerns depressive symptoms, and esketamine should not be presented as a treatment proven to prevent suicide or replace hospitalization when clinically indicated. Current prescribing information emphasizes risks of sedation, dissociation, respiratory depression, abuse and misuse, and the need for post-administration observation under a REMS program.12,13 Its significance lies not only in its regulatory status, but in what it has changed conceptually. Esketamine supports a model of antidepressant action in which glutamatergic modulation, synaptic plasticity, and circuit-level recalibration can be directly relevant to clinical benefit, especially in patients for whom waiting several weeks for conventional antidepressant response is itself a major limitation.
The practical importance of esketamine is greatest in clinically urgent or difficult-to-treat settings. In such contexts, speed is not a convenience but a therapeutic variable. Earlier symptom reduction may alter short-term risk, reduce hopelessness associated with repeated treatment failure, and improve engagement with care. From a drug-profile perspective, its clinical positioning is strongest where conventional oral antidepressant sequencing has already proved inadequate or too slow.14,15 These features do not negate its value, but they do mean that its place in care is selective rather than universal. Evidence is strongest in selected urgent or treatment-resistant settings rather than across all depressive populations.
Ketamine, although pharmacologically and operationally distinct from intranasal esketamine, remains central to the same broader therapeutic shift.16 Clinically, recent syntheses continue to support rapid antidepressant effects in treatment-resistant depression and reinforce the view that modulation of glutamatergic signaling and neuroplasticity may have direct therapeutic relevance in severe depressive states.17,18 Yet rapid benefit does not automatically translate into durable remission. The harder problem is how to stabilize benefit after early response and how to balance acute efficacy against long-term monitoring burden, accessibility, and uncertainty about continuation pathways.19
Rapid-acting treatments may also improve engagement by restoring therapeutic credibility after repeated failure. However, speed should not be confused with completeness, and these interventions are best viewed as components of staged care rather than self-sufficient solutions.
Dextromethorphan-bupropion further broadens the rapid-acting and glutamatergic conversation. In the United States, this oral combination is approved for major depressive disorder in adults; dextromethorphan contributes uncompetitive NMDA receptor antagonism and sigma-1 receptor agonism, while bupropion provides antidepressant activity and inhibits CYP2D6, thereby increasing dextromethorphan exposure.20 The practical significance of this combination lies in format as well as mechanism. Unlike esketamine, it is an oral therapy and therefore suggests that NMDA-related or neuroplasticity-linked antidepressant effects may be pursued through more scalable routine-care strategies in selected settings.21 In a pivotal Phase 3 trial, symptom improvement emerged early, but important questions remain regarding long-term comparative effectiveness, ideal sequencing after first-line failure, and which patients are most likely to benefit from this mixed pharmacological profile.22,23
Multimodal and Mechanistically Broadened Antidepressants
A second important group within next-generation pharmacotherapy consists of multimodal or mechanistically broadened antidepressants. These drugs do not fully depart from monoaminergic biology, but they attempt to move beyond simple transporter inhibition through differentiated receptor-level actions and broader symptom-domain coverage. Vortioxetine is approved in the United States for major depressive disorder in adults, combines serotonin transporter inhibition with multiple serotonin receptor actions, and is often discussed in relation to cognitive symptoms and functional recovery.24 Vilazodone is likewise approved for adult major depressive disorder and combines serotonin reuptake inhibition with 5-HT1A partial agonism, but its hypothesized clinical advantages over standard SSRIs have not been consistently demonstrated in comparative evidence.25 These agents illustrate a more incremental model of innovation: not radical rupture, but pharmacological refinement.
This refinement is clinically relevant because many patients show partial rather than absent responses to antidepressants; that is, they improve, but inadequately. Mood may lift slightly, while anxiety, sleep disruption, cognitive inefficiency, emotional blunting, or functional impairment remain substantial. In such situations, simple dose escalation or repeated substitution within a narrow class may yield only limited gains. Mechanistically broadened antidepressants are attractive because they aim to influence multiple clinically relevant symptom and functional domains, such as mood, anxiety, sleep, cognition, tolerability, and daily functioning without immediately requiring complex polypharmacy.
Neither drug resolves the core problems of severe TRD or bipolar-spectrum complexity, but both illustrate how pharmacological refinement within the monoaminergic space can remain clinically useful. Claims of superiority, however, should be restrained. Broader receptor pharmacology does not automatically translate into broader clinical benefit. These agents do not eliminate the core problems of depressive heterogeneity, relapse, or resistant illness. Their role is best understood as intermediate: they may be particularly useful for patients who are not well served by repeated standard SSRI or SNRI substitution, but they are unlikely to resolve the deeper problems represented by severe TRD or pronounced bipolar-spectrum complexity.
Agomelatine belongs to a somewhat different but related category. Authorized in Europe for major depression, it combines melatonergic agonism with 5-HT2C antagonism, represents a circadian-oriented pharmacological idea, and requires liver monitoring in routine use because of clinically relevant hepatic risk considerations.26 At the same time, agomelatine illustrates an important cautionary principle. Mechanistic distinctiveness does not exempt a drug from ordinary clinical scrutiny. Its overall benefit must still be weighed against comparative efficacy, tolerability, and implementation burden.
Neuroactive Steroid-Related Approaches
Neuroactive steroid-related approaches are relevant to next-generation pharmacotherapy because they expand antidepressant development beyond both conventional monoaminergic and explicitly glutamatergic models.27 Their importance is not limited to a single approved product. Rather, they reinforce the broader idea that depressive symptoms may, in at least some patient groups, be more directly linked to stress-system dysregulation, inhibitory tone, arousal control, and affective instability than can be addressed by conventional antidepressant designs.
Brexanolone, an intravenous formulation of allopregnanolone approved for postpartum depression, provided an earlier regulatory example of neuroactive steroid-based antidepressant treatment, although its intensive administration requirements and monitoring burden limit routine scalability.28
At present, zuranolone is approved in the United States for postpartum depression in adults, but not for the broader treatment of major depressive disorder.29 Current labeling underscores central nervous system depressant effects, psychomotor impairment risk, and CYP3A4-related interaction considerations.30 This means that the class currently occupies a narrower clinical niche than standard antidepressants or ketamine-based strategies.
Nevertheless, the field-wide importance of neuroactive steroid-related treatment extends beyond postpartum depression. It demonstrates that antidepressant development can move meaningfully toward pathways linked to stress regulation and GABAergic modulation, thereby broadening the neurobiological imagination of what an antidepressant can be.31 Their future significance for broader depressive populations will depend on whether the underlying mechanisms can be translated into scalable, tolerable, and sufficiently durable interventions beyond narrowly defined indications. Even with currently narrow indications, this class broadens the range of pharmacological hypotheses considered clinically credible in depression treatment.
Psychedelic-Assisted Pharmacotherapy
Psychedelic-assisted treatment, particularly psilocybin-assisted therapy, has generated increasing interest as a mechanistically distinct and highly supervised approach to depressive disorders. Its relevance lies not only in serotonergic 5-HT2A receptor agonism, but also in the treatment model through which pharmacological effects are combined with structured psychological support. Early and mid-stage clinical studies suggest potentially rapid and sustained antidepressant effects in selected populations with major depressive disorder or treatment-resistant depression, but the evidence base remains limited by sample size, trial heterogeneity, expectancy effects, intensive implementation requirements, and unresolved questions about long-term safety, durability, and scalability.32 For these reasons, psychedelic-assisted therapy is best considered an emerging and highly supervised treatment model rather than a routine pharmacological option.33
Kappa-Opioid Receptor Antagonists and Stress-Related Mechanisms
Kappa-opioid receptor antagonists represent another emerging direction in antidepressant drug development. Because dynorphin-kappa-opioid signaling has been implicated in stress responsivity, dysphoria, and anhedonia-related processes, agents such as aticaprant and navacaprant are being investigated as potential mechanism-based treatments for depressive symptoms, particularly when anhedonia or stress-related affective dysfunction is prominent.34 However, this field remains developmental, and current clinical positioning should be cautious. These compounds illustrate how next-generation pharmacotherapy may increasingly target symptom-relevant neurobiological systems beyond conventional monoaminergic pathways, while still requiring stronger evidence for efficacy, durability, safety, and patient selection.35
Bipolar-Relevant Pharmacotherapies and Mood-Stabilizing Approaches
Any discussion of emerging pharmacotherapy for depressive disorders is incomplete unless bipolar depression is treated as a distinct pharmacological problem rather than as a minor variant of unipolar depression. Bipolar depression imposes a more demanding definition of success. Treatment must reduce depressive symptoms without destabilizing polarity, increasing activation, or worsening mixed features, and current guideline summaries accordingly emphasize quetiapine, lurasidone, cariprazine, and olanzapine-fluoxetine as major drug-based options, with lithium and lamotrigine remaining important within broader mood-stabilizing strategies.36,37
These drug profiles are clinically important because they embody a treatment logic different from simple antidepressant intensification. Their value lies not only in reducing depressive symptoms, but also in supporting mood stabilization and long-term illness-course management. A drug may be “antidepressant” in a narrow sense and still be a poor fit for bipolar illness if it worsens activation or switching liability. Conversely, a treatment may deserve special value precisely because it reduces depressive burden without sacrificing illness stability.
Quetiapine and lurasidone are especially representative because they show that depressive symptom relief in bipolar disorder often depends on agents whose clinical value lies not in conventional antidepressant intensification, but in polarity-sensitive efficacy combined with tolerability management.36 Cariprazine is particularly relevant because it bridges two important domains of next-generation depression pharmacotherapy: bipolar depression and adjunctive treatment of major depressive disorder. Its U.S. labeling includes treatment of depressive episodes associated with bipolar I disorder in adults and adjunctive therapy to antidepressants for major depressive disorder in adults.38 This dual positioning makes cariprazine a useful example of how dopamine-serotonin partial agonist pharmacology may contribute both to polarity-sensitive treatment and to augmentation strategies after inadequate antidepressant response.
Lamotrigine occupies a somewhat different but highly relevant position. Its strength lies less in rapid acute relief than in longer-horizon management of depressive burden and recurrence vulnerability. This illustrates an important principle: next-generation value need not always mean faster or more dramatic symptom change. In some settings, the clinically meaningful advance lies in better alignment with the temporal structure of the illness. For bipolar depression, that often means maintenance relevance, polarity sensitivity, and tolerability over time.39 Even so, the evidence base in bipolar depression remains narrower and more polarity-sensitive than that in unipolar depression, and extrapolation from unipolar antidepressant data should remain limited. To synthesize the principal mechanistic and clinical distinctions among representative next-generation pharmacotherapies in depressive disorders, Table 1 summarizes representative agents by primary target, relevant clinical context, key efficacy signal, major safety concern, and practical clinical positioning.
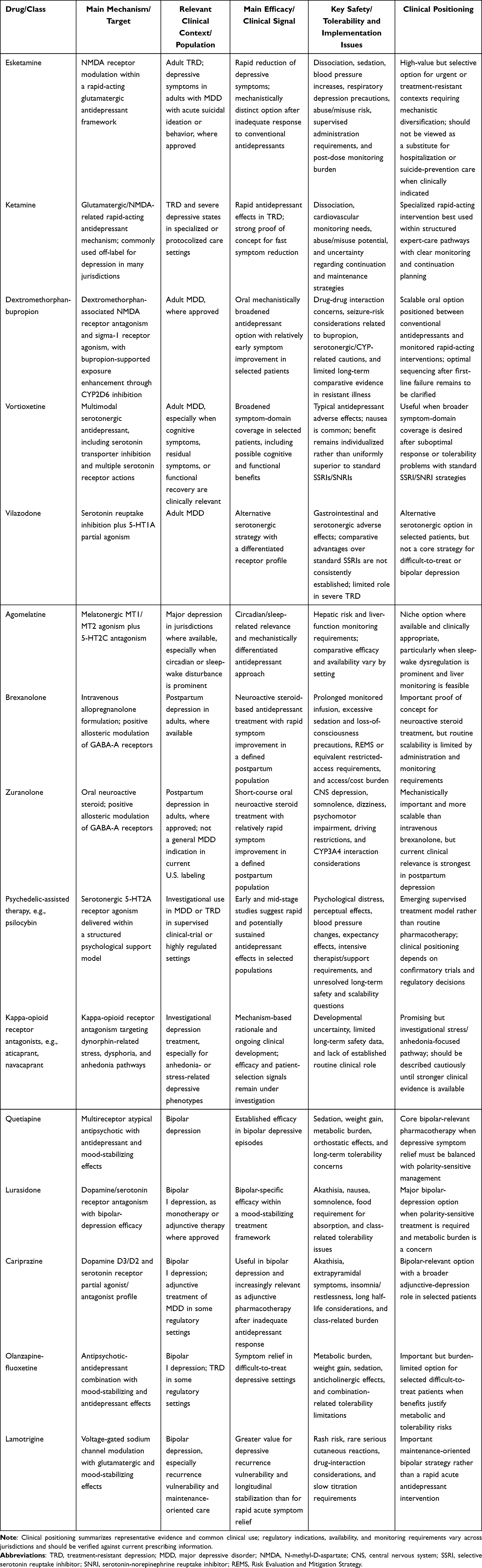 |
Table 1 Representative Next-Generation Pharmacotherapies in Depressive Disorders: Mechanisms, Clinical Signals, Safety Issues, and Clinical Positioning |
Optimizing the Use of Available Drugs
If novel compounds represent one frontier of next-generation pharmacotherapy, optimized use of available drugs represents another that is equally important. In depressive disorders, meaningful gains often arise not only from replacing older treatments, but also from using them with greater pharmacological precision, better timing, and clearer attention to long-term sustainability, especially in patients with partial response, relapse, treatment resistance, or clinical complexity that is poorly served by sequential monotherapy alone.40
This point is easy to overlook because innovation is often associated with the arrival of new drugs, whereas optimization may appear less dramatic. Yet from the standpoint of routine care, optimization is often where a large proportion of clinically meaningful progress occurs. Repurposing, augmentation, rational combination treatment, dose adjustment, sequencing, transition planning, and maintenance-oriented prescribing all represent ways in which the therapeutic value of available drugs can be extended. These strategies matter because depressive disorders are not only mechanistically heterogeneous; they are also longitudinally heterogeneous. Some patients require rapid reduction of acute burden, others broader symptom coverage, and others long-term simplification and relapse prevention.
Drug Repurposing
Drug repurposing is most useful when it is mechanism-informed rather than opportunistic.41 In depressive disorders, repurposing becomes meaningful when the pharmacology of an established agent maps onto a clinically recognizable unmet need that conventional antidepressants do not adequately address, such as severe insomnia, circadian disruption, residual anxiety, fatigue, or incomplete symptom-domain coverage.42 The appeal of repurposing is practical as well as conceptual. Established drugs often have known pharmacokinetics, safety profiles, and interaction patterns, which may shorten the translational path from pharmacological idea to clinical testing.
Repurposing should not be confused with unstructured improvisation. For it to represent meaningful progress, mechanism must map onto a defined clinical problem, the intended use must address a genuine gap left by standard treatment, and the expected benefit must justify the monitoring burden. Otherwise, repurposing risks becoming poorly bounded off-label accumulation rather than treatment innovation.43
This issue is especially important in difficult-to-treat populations, where desperation can expand the range of weakly justified off-label interventions. A next-generation framework does not reject repurposing. Rather, it insists that repurposing be pharmacologically coherent, clinically targeted, and transparent about evidentiary limits. When used in that way, repurposing can become a legitimate form of treatment innovation rather than an empirical afterthought.
Augmentation Strategies
Augmentation represents one of the clearest examples of mechanism-informed optimization, particularly when monotherapy leaves clinically relevant residual burden after an otherwise adequate trial.44,45 It becomes clinically important when monotherapy yields incomplete improvement and the unresolved burden is not simply insufficient drug exposure, but incomplete coverage of symptom dimensions such as anxiety, insomnia, psychomotor slowing, residual cognitive burden, or relapse vulnerability. Among augmentation strategies, lithium retains special importance because it adds mechanistic diversity beyond standard antidepressant escalation and remains especially relevant in difficult-to-treat depression and in patients for whom mood stabilization is part of the broader therapeutic goal.46 Second-generation antipsychotic augmentation, especially with aripiprazole, brexpiprazole, or cariprazine, represents another established route to pharmacological diversification in patients with inadequate antidepressant response.47,48 Thyroid hormone augmentation demonstrates that endocrine modulation may help selected patients when conventional antidepressant response has plateaued.49
Augmentation also has important implications for how clinicians interpret partial response. Partial response should not be treated as a meaningless state between success and failure.50 In many cases, it contains valuable pharmacological information. If mood symptoms improve but severe insomnia persists, if energy improves while anxiety remains disabling, or if core affective symptoms respond while cognition and function recover poorly, those patterns may indicate that the original treatment is doing something useful but incomplete. Under such conditions, a carefully chosen add-on strategy may be more rational than abandoning the original drug altogether, particularly in some treatment-resistant settings.51
At the same time, augmentation should remain disciplined, reversible, and reviewable. Every additional agent increases interpretive complexity and cumulative burden. Over time, the core discipline of augmentation is not only knowing when to add, but also knowing when to reassess whether the added drug still justifies its presence. For augmentation to qualify as genuinely next-generation, it should be guided by the dominant residual burden, expected benefit, interaction profile, and likely feasibility of sustained use.
Rational Combination Pharmacotherapy
Combination pharmacotherapy is frequently approached with justified caution because it can easily become associated with overmedication, interaction burden, and reduced clarity about which component is producing benefit or harm. Yet strict commitment to serial monotherapy may also be inefficient in clinically complex depression. Rational combination treatment becomes defensible when the components have nonredundant pharmacological roles, target distinct clinically relevant dimensions of illness, and do not impose an excessive cumulative burden.52
A useful way to distinguish rational combination treatment from indiscriminate polypharmacy is to ask whether each component would still be defensible if discussed independently. If the justification for one drug rests only on vague hope that “more treatment” may help, the combination is unlikely to be pharmacologically robust. By contrast, when one treatment addresses persistent insomnia, another unresolved affective burden, and another relapse liability or polarity instability, the regimen may remain coherent even if complex. The central requirement is that complexity be purposeful rather than accidental.
Combination therapy is therefore easy to either overpraise or overcriticize. The more balanced position is that it can be clinically valuable, but only when its nonredundancy, safety, and expected benefit are sufficiently clear. In that sense, rational combination treatment can be one of the most practical expressions of next-generation care, provided that complexity remains interpretable and proportionate.
Dose, Sequencing, and Transition Strategies
Pharmacological innovation in depression does not occur only at the level of new molecules; it also occurs through better use of time. Dose, titration speed, sequencing of mechanisms, and transition planning often determine whether a treatment can realize its theoretical value. In treatment-resistant illness, repeated switching among broadly similar antidepressants may consume months while adding little mechanistic diversity.53 Earlier augmentation, earlier use of a mechanistically distinct strategy, or earlier identification of pseudo-resistance due to poor exposure or intolerance may be more informative than another conventional substitution.54
Sequencing also influences how patients understand and engage with treatment. Repeated medication changes without a clear rationale can communicate therapeutic uncertainty and deepen patient frustration. By contrast, a sequence explicitly explained in pharmacological terms may improve understanding and adherence even when treatment remains difficult. In this sense, sequencing is not merely a technical issue; it is part of how treatment becomes interpretable and sustainable over time. This is especially relevant in TRD, where the cumulative experience of prior failure often influences response to the next intervention as much as the molecule itself.
Transition planning is equally important after rapid-acting interventions. Acute improvement can create the impression that the therapeutic problem has been solved, when in practice the harder question is how to preserve and extend benefit. Sequencing is therefore a core part of next-generation pharmacotherapy because it determines how mechanistic diversity, speed, and long-term management are connected rather than treated as separate concerns.
Maintenance Treatment and Sustained-Use Considerations
Depression pharmacotherapy is too often judged through the lens of acute response alone. For many patients, however, the decisive issue is whether benefit can be maintained without unacceptable cumulative burden.55 Maintenance-oriented prescribing requires active decisions about which components of an acute regimen remain necessary, which can be simplified, and how relapse prevention should be balanced over time as treatment goals change.56 Relapse prevention must also be balanced against metabolic effects, sexual dysfunction, emotional blunting, sedation, or discontinuation difficulty.57,58
Maintenance treatment should therefore be viewed as a phase of active therapeutic design rather than passive continuation. Once acute symptom pressure has been reduced, clinicians must reconsider the pharmacological architecture of the regimen. Which elements are still essential? Which were introduced for crisis containment and may no longer be needed? Which components impose the greatest long-term burden? These questions are central to next-generation care because a regimen that cannot be maintained, simplified, or eventually tapered in a tolerable way is less useful than one that offers somewhat smaller acute gains but better long-term viability.
This sustained-use perspective is especially important after aggressive augmentation, complex combinations, or rapid-acting interventions introduced during severe episodes. In real-world care, maintenance is often where the true success or failure of a pharmacological strategy becomes most visible. It is also where patient-centered treatment reasoning becomes most important. A regimen that works on paper but is difficult to live with is unlikely to retain long-term value. Because therapeutic progress in depressive disorders depends not only on novel compounds but also on more rational use of available agents, Table 2 outlines mechanism-informed optimization strategies that may improve treatment fit, tolerability, and long-term clinical utility.
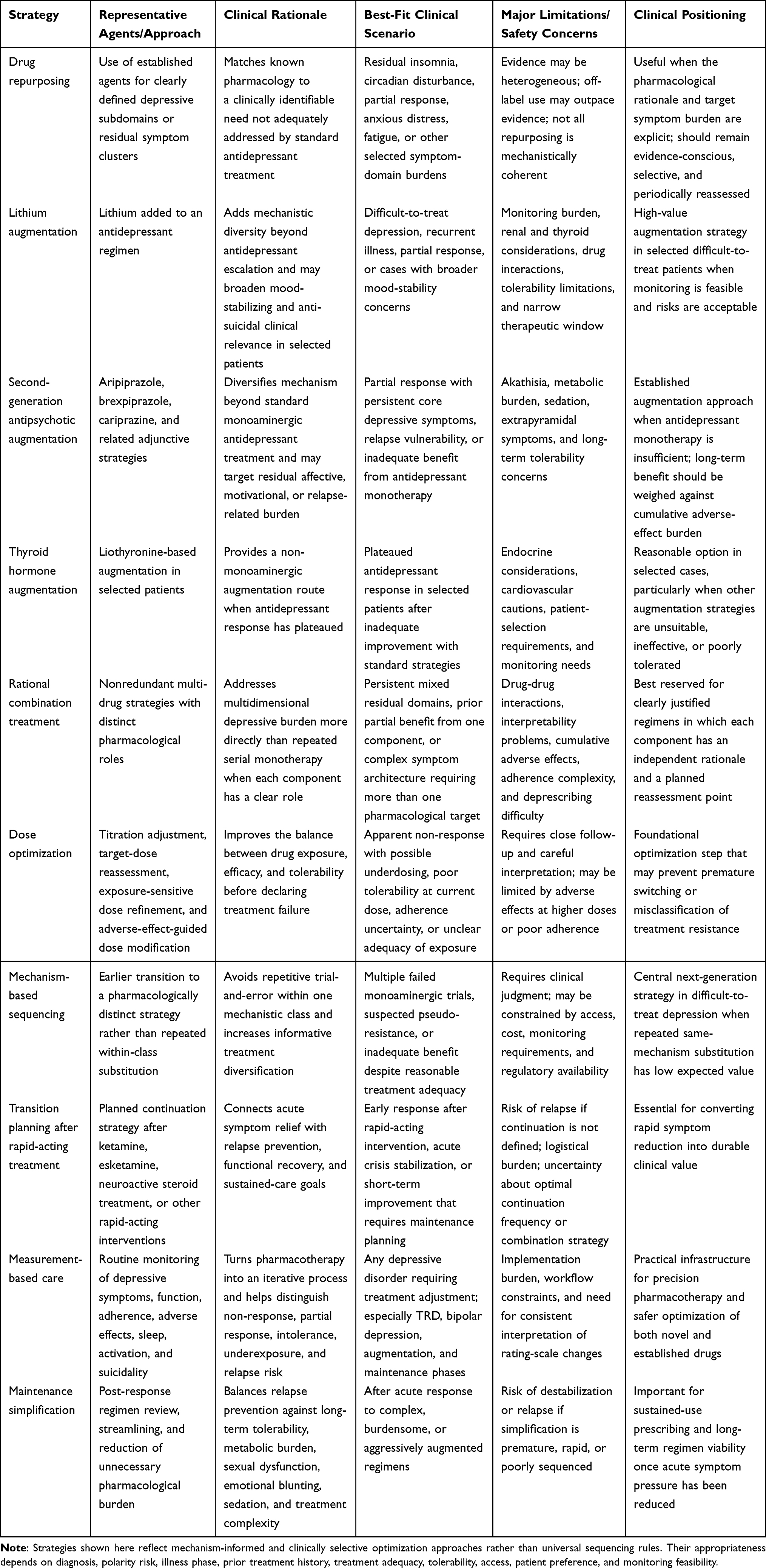 |
Table 2 Mechanism-Informed Optimization Strategies Using Available Drugs in Depressive Disorders |
Precision Pharmacotherapy: Pharmacogenomics, PK/PD Variability, and Clinical Stratification
Precision pharmacotherapy in depressive disorders aims to improve treatment selection and dosing by reducing avoidable mismatch between patient variability and drug exposure, tolerability, or mechanism of action. In current practice, its most actionable components include pharmacogenomics relevant to antidepressant metabolism, PK/PD-informed interpretation of apparent non-response or intolerance, and structured clinical stratification based on treatment history, polarity risk, symptom profile, and longitudinal course. Although current tools do not reliably identify the single best antidepressant for an individual patient, they can improve prescribing by helping clinicians identify patients who may require dose adjustment, closer monitoring, earlier augmentation, or movement to a mechanistically distinct therapy.59,60
The need for precision arises because depressive disorders are pharmacologically heterogeneous even when they appear diagnostically similar. Two patients may meet criteria for a depressive episode while differing substantially in polarity sensitivity, residual symptom domains, illness trajectory, and adverse-effect vulnerability. Yet routine treatment often begins from the assumption that the same first-line logic applies to both. As a result, what is labeled “non-response” may actually reflect inadequate exposure, intolerable adverse effects, bipolar-spectrum activation, poor adherence, premature discontinuation, or an initial mismatch between drug profile and dominant symptom burden. Precision pharmacotherapy helps separate these possibilities rather than collapsing them into a single category of failure.
Pharmacogenomics is one of the clearest examples of clinically usable precision, but it should be positioned realistically. Current CPIC guidance supports clinically relevant use of CYP2D6 and CYP2C19 genotype information for several serotonin reuptake inhibitor antidepressants and includes recommendations relevant to vortioxetine- and sertraline-related metabolism.61 In practice, such information may help explain why one patient develops adverse effects at standard doses while another appears to have unexpectedly weak exposure or poor tolerability.62 This is particularly useful after repeated treatment failures in which the usual interpretation of pure pharmacodynamic inefficacy appears incomplete.
Even so, pharmacogenomic testing is better viewed as a refinement tool than as a stand-alone treatment-selection algorithm. It does not yet offer a simple or consistently reliable map from genotype to antidepressant success. Its best use is therefore practical and bounded: helping clinicians avoid avoidable dose-related errors, interpret difficult treatment histories more intelligently, and tailor monitoring and sequencing decisions more carefully.
PK/PD variability broadens this perspective beyond genotype. Patients differ in absorption, distribution, metabolism, elimination, receptor sensitivity, interaction burden, and cumulative pharmacological load. These differences can substantially affect both benefit and harm. A patient may appear treatment resistant when the actual problem is poor exposure, food-related absorption variability, inhibition of a relevant metabolic pathway, or inability to tolerate the dose required for efficacy.63 In polypharmacy, the practical meaning of a regimen may change because of additive sedation, serotonergic burden, QT-related concerns, or metabolic competition among multiple agents.64
Clinical stratification remains equally important because some of the most useful predictors are still clinical rather than molecular. A patient with recurrent partial response and rapid relapse is not the same as a patient with repeated early activation, mixed symptoms, or likely bipolar-spectrum instability.65 A patient who repeatedly stops medication because of side effects presents a different pharmacological problem from one who tolerates multiple trials but derives little benefit from any of them. A next-generation framework treats these histories as patterns that guide earlier augmentation, closer monitoring, bipolar screening, maintenance planning, or transition to more mechanistically distinct interventions.
Precision pharmacotherapy should therefore be understood not as a distant or separate domain, but as a modifier of everyday prescribing decisions.66 Its practical value lies in making treatment less repetitive, less avoidably empirical, and more responsive to the differences that shape antidepressant response in real patients. Precision pharmacotherapy in depressive disorders extends beyond pharmacogenomic testing alone. As summarized in Table 3, individualized prescribing may also be informed by pharmacokinetic and pharmacodynamic variability, polarity-sensitive treatment selection, prior treatment history, tolerability vulnerability, and maintenance-related risk stratification.
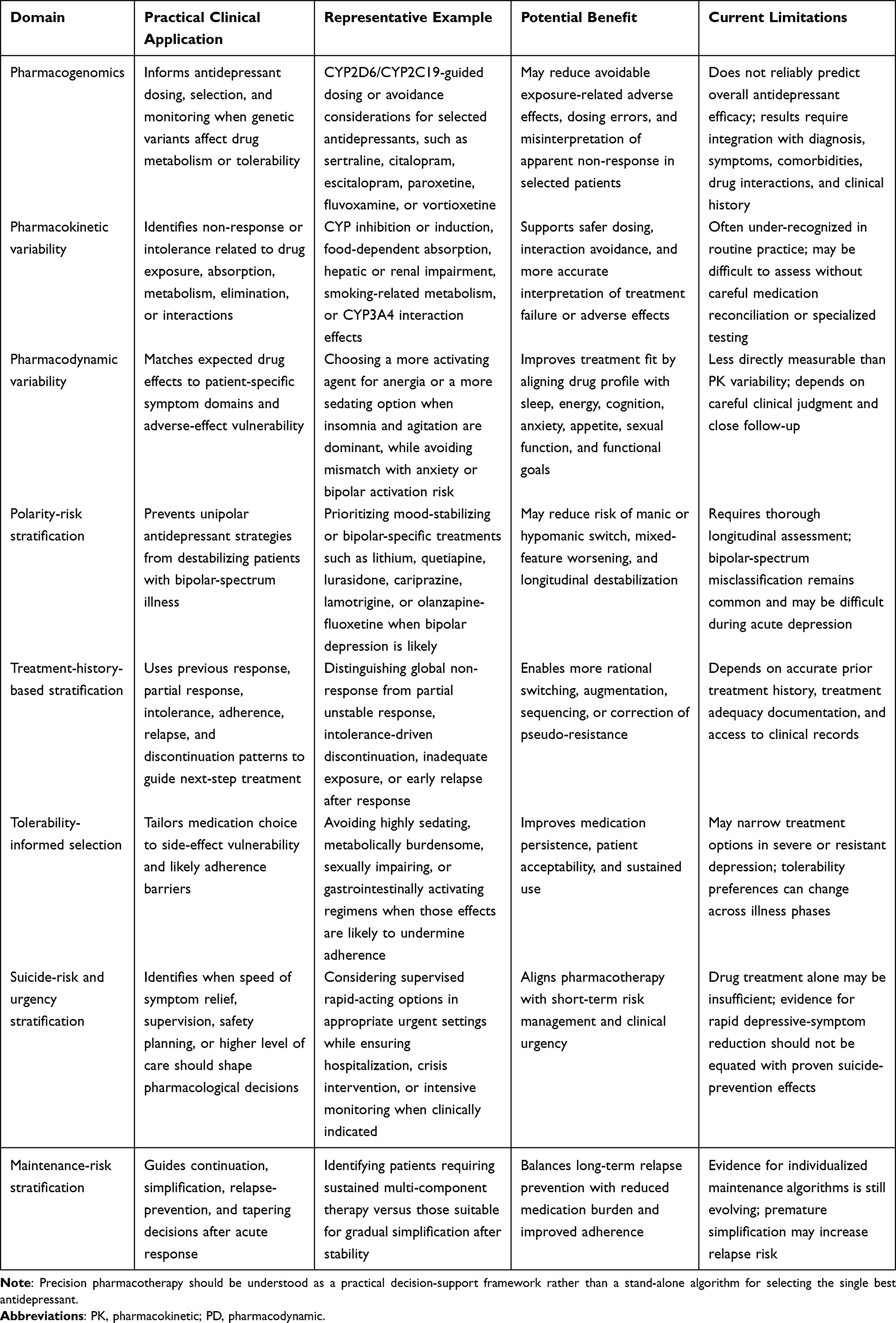 |
Table 3 Domains of Precision Pharmacotherapy in Depressive Disorders |
Measurement-based care provides a practical structure for implementing precision pharmacotherapy.67 Repeated assessment of symptom severity, functional recovery, adverse effects, adherence, sleep, activation, and suicidality can help distinguish non-response from partial response, intolerance, underexposure, or emerging bipolar-spectrum instability.68 In this sense, measurement-based care is not separate from pharmacotherapy; it is a clinical method for determining whether a drug strategy remains appropriate, requires optimization, or should be changed.
Treatment-Resistant Depression and Bipolar Depression as Key Clinical Contexts
Figure 2 depicts the conceptual integration of novel agents and optimization strategies within the specific clinical contexts of TRD and bipolar depression, highlighting a multidimensional approach to treatment selection and sequencing.
The value of next-generation pharmacotherapy becomes most visible not in straightforward cases, but in settings where conventional treatment logic fails most clearly. TRD and bipolar depression are therefore not merely subgroups of interest. They are high-value clinical contexts in which the strengths, limits, and trade-offs of contemporary pharmacological innovation are exposed most sharply.18 They show whether new drugs and optimized strategies genuinely improve care under pressure rather than only in relatively uncomplicated first-line treatment scenarios. These two settings are especially important because they are where both novel compounds and optimized use of available drugs are most severely tested.
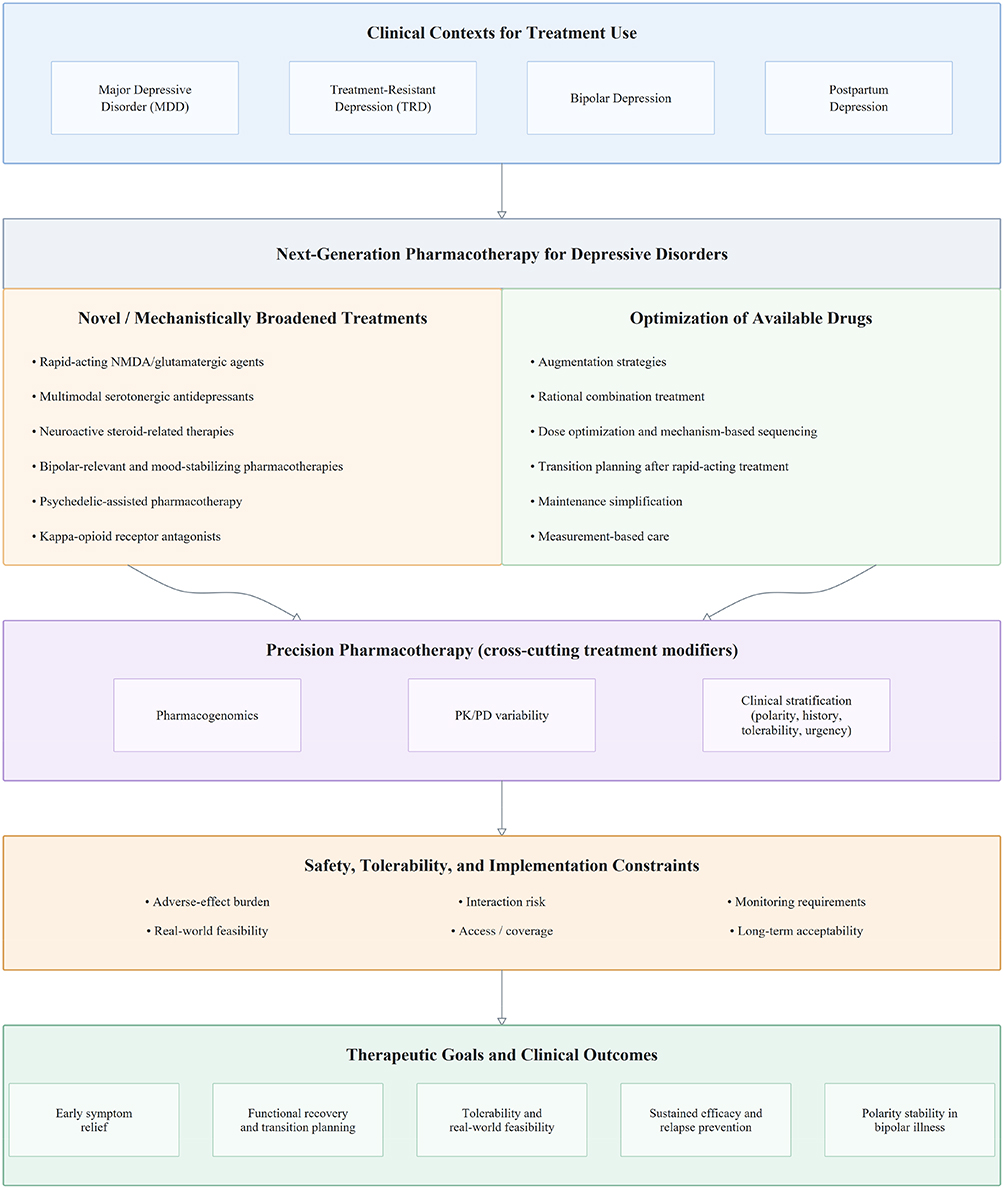 |
Figure 2 A clinically integrated framework for next-generation pharmacotherapy in depressive disorders. This framework illustrates how novel, rapid-acting, and mechanistically broadened treatments may be integrated with optimized use of available drugs across major depressive disorder, treatment-resistant depression, and bipolar depression. The model incorporates augmentation, rational combination treatment, sequencing and transition strategies, pharmacogenomic- and PK/PD-informed prescribing, and maintenance planning. Particular emphasis is placed on balancing early symptom relief, long-term tolerability, real-world feasibility, and polarity stability in bipolar illness. |
Treatment-Resistant Depression
Operational definitions of TRD vary substantially across trials and care settings, which limits direct comparison of pharmacological strategies.69,70 TRD is often defined numerically by the number of unsuccessful treatment trials, but its broader significance is more instructive. Repeated failure of monoaminergic strategies raises a mechanistic question rather than a purely numerical one: is the patient still waiting for the “right” antidepressant within the same general framework, or has the treatment model itself become too narrow for the biology and symptom architecture of the illness? This is why TRD occupies such a central place in discussions of next-generation treatment. It is the setting in which mechanistic diversification becomes not merely interesting but often necessary.
The current regulatory landscape reflects this point. Esketamine has a formal U.S. indication for adult treatment-resistant depression, and the olanzapine-fluoxetine combination is approved for the acute treatment of treatment-resistant depression in adults within its labeled definition.71 Their importance extends beyond the particular products themselves. They demonstrate that drug development is being translated most directly in the patient populations where conventional treatment has been least satisfactory. The practical challenge, however, is that TRD is not a monolithic category. Some patients are globally nonresponsive. Others show partial but unstable improvement. Others appear resistant because adverse effects prevented adequate trials, exposure was inadequate, bipolarity was underrecognized, or the drug addressed only part of the actual syndrome.72
TRD therefore teaches an interpretive lesson as much as a therapeutic one. Not all failure means the same thing, and a next-generation framework improves care not only by offering more options, but by interpreting failed options more intelligently. The goal is not simply to introduce more intensive or novel interventions, but to determine what kind of failure has occurred and what form of diversification is actually justified. In some patients, rapid-acting or mechanistically distinct interventions may be appropriate relatively early. In others, the more important advance may lie in correcting pseudo-resistance, clarifying bipolarity, or reorganizing an overly accumulated regimen.
TRD also illustrates why innovation must be accompanied by restraint.73 The more difficult the population, the easier it is to overread limited improvement, extrapolate from heterogeneous evidence, or ignore the possibility that prior care varied in adequacy. For this reason, next-generation treatment in TRD should not be equated with indiscriminate treatment intensification. Its aim is not “more treatment at any cost”, but better-targeted treatment based on what previous failure actually means.
Bipolar Depression
The evidence base for bipolar depression is narrower and more heterogeneous than that for unipolar major depression, and pharmacological transfer from unipolar depression is often clinically unsafe.74 Treatments that appear reasonable in unipolar depression may be much less acceptable in bipolar depression if they increase switching, activation, or mixed symptoms. This is why bipolar-specific pharmacotherapies deserve separate emphasis. Regulatory indications and guideline hierarchies consistently highlight quetiapine, lurasidone, cariprazine, and olanzapine-fluoxetine as major drug-based options for bipolar depression, while lithium and lamotrigine remain important for broader mood-stabilizing and maintenance strategies.75
The common feature of these treatments is not simply antidepressant efficacy, but efficacy within a polarity-sensitive framework. Bipolar depression therefore serves as an especially important stress test for the idea of next-generation care. It reminds us that pharmacological success cannot be defined solely by short-term symptom change. A treatment can be antidepressant in a narrow sense while still being clinically inadequate if it destabilizes the broader course of illness. Conversely, a drug may deserve special value precisely because it reduces depressive burden without worsening longitudinal instability.
This makes bipolar depression a setting for mechanism-informed caution. Pharmacological strategies effective in unipolar depression cannot be transferred to bipolar depression without considering switching liability, mixed features, and longitudinal instability.76,77 In unipolar depression, pharmacological progress is often discussed mainly in terms of response magnitude or speed. In bipolar depression, the framework must be wider. A treatment has to be assessed not only for whether it reduces depressive symptoms, but for how it influences switching risk, mixed phenomenology, overall instability, and long-term acceptability. From a drug development and therapy perspective, this is highly relevant because it shows that progress in depressive disorders cannot be judged only by whether a treatment is antidepressant in a narrow sense; it must also be judged by whether it is illness-appropriate over time.
Safety, Tolerability, Implementation Burden, and Real-World Use
The value of next-generation pharmacotherapy cannot be determined by efficacy alone. A treatment may appear highly innovative because it acts rapidly, engages a novel pathway, or expands options in difficult-to-treat populations, yet still occupy only a limited place in care if its tolerability profile, monitoring demands, cost, or implementation burden constrain routine use. Safety is therefore not a secondary filter applied after efficacy has been demonstrated. It is part of what determines whether a pharmacological strategy is genuinely useful. This is particularly relevant to drug development and therapy because innovation that cannot be feasibly deployed may have limited therapeutic impact despite mechanistic promise.
Early tolerability remains one of the most underestimated determinants of outcome.78,79 In depressive disorders, medication is often initiated during periods of hopelessness, cognitive slowing, heightened somatic sensitivity, or profound ambivalence about treatment. Under such conditions, even moderate early adverse effects may have disproportionate consequences for adherence. Nausea, akathisia, sedation, insomnia, activation, dizziness, dissociation, or subjective unfamiliarity may lead patients to abandon a potentially useful treatment before meaningful benefit can emerge. This is especially relevant for mechanistically distinct or rapid-acting interventions, in which novelty may coexist with unfamiliar subjective effects or more complex administration procedures.80
Long-term safety extends beyond persistent side effects alone. Sustained pharmacotherapy may affect metabolic health, sexual functioning, emotional range, sleep quality, cognition, and overall quality of life. A regimen that performs well acutely may lose much of its value if it becomes difficult to maintain without cumulative burden.81 This is particularly relevant in bipolar-relevant treatment and in augmentation-based regimens, where metabolic effects, akathisia, sedation, endocrine issues, or treatment complexity may progressively erode acceptability over time. A clinically useful strategy must therefore be evaluated not only by whether it works, but also by whether it remains acceptable and sustainable for patients over time.
Real-world implementation introduces additional barriers. Some next-generation treatments require structured supervision, post-dose observation, special clinical settings, or more frequent visits than standard antidepressants. Others are easier to prescribe but more difficult to sustain because of interaction issues, insurance coverage limitations, or poor patient tolerance. These barriers are not peripheral to treatment evaluation. They influence who can actually receive a drug, under what conditions, and for how long. For a journal focused on drug development and therapy, implementation burden is part of the therapeutic profile of a treatment, not an external inconvenience.
In bipolar populations, safety must be evaluated through an even broader lens. Relevant harms include not only conventional adverse effects, but also mood destabilization, switching, mixed-state worsening, and long-term disruption of illness course.82 This reinforces a broader principle: safety is not a fixed property of a molecule alone, but a context-dependent property of the drug-patient-illness interaction. Next-generation treatment becomes meaningful only when efficacy, tolerability, safety, and feasibility remain aligned strongly enough to support real clinical use.
Translational Challenges and Future Directions
Despite major progress in depression pharmacotherapy, the gap between mechanistic promise and routine clinical usefulness remains substantial.83 One reason is that depressive disorders are still often treated within diagnostic categories that are broader than the biological and longitudinal realities they are intended to capture. Patients classified under the same depressive label may differ significantly in symptom architecture, polarity risk, treatment sensitivity, relapse pattern, and adverse-effect vulnerability, yet clinical trials and treatment algorithms often remain more homogeneous than the populations to which they are applied. This mismatch limits both innovation and implementation.
The problem is especially visible in treatment-resistant depression. Definitions remain inconsistent across studies and clinical settings, making it difficult to compare interventions or determine whether apparent advances reflect true therapeutic improvement or simply differences in who was studied. Future progress in TRD will depend less on counting failed trials and more on characterizing the type of resistance involved: mechanistic non-response, partial unstable response, intolerance-driven discontinuation, underexposure, pseudo-resistance, bipolar-spectrum misclassification, or some combination of these factors. Better phenotyping is likely to be as important as the development of additional compounds.84
A parallel challenge exists in bipolar depression, where the evidence base remains narrower and more contested than in unipolar depression. Greater bipolar-specific drug development and more polarity-sensitive trial design are still needed.85 Without this, pharmacological knowledge in bipolar depression will remain too dependent on extrapolation from unipolar studies, which is conceptually weak and clinically risky.
Another major challenge is treatment selection. Pharmacogenomics, PK/PD-informed prescribing, and clinical stratification all offer value, but they do not yet provide highly reliable algorithmic guidance. Their future usefulness will depend on whether they can be integrated into practical models that improve early treatment fit rather than simply add complexity. For readers focused on drug development and therapy, the central translational challenge is no longer novelty alone, but how to connect mechanism, safety, feasibility, and illness-specific deployment.
The evidence base also remains limited in ways that directly affect translation. Head-to-head comparative studies remain relatively scarce, follow-up periods are often too short to determine whether acute response leads to sustained recovery, and real-world effectiveness data are not always well integrated with mechanistic or regulatory evidence.86 Some next-generation approaches also require specialized monitoring, intensive visits, or structured continuation pathways that many health systems are not yet equipped to provide. Conversely, some lower-technology forms of optimization, such as better sequencing or more disciplined augmentation, may offer substantial gains yet remain underemphasized because they lack the visibility of molecular innovation.
Future progress in depression pharmacotherapy is therefore likely to depend on integration rather than novelty alone: integration of drug mechanism, patient variability, illness course, safety, and real-world feasibility. Under this view, the future of next-generation pharmacotherapy lies not simply in discovering more treatments, but in building better frameworks for using treatments. Novel compounds, optimized use of available drugs, precision-informed prescribing, and illness-specific therapeutic models should be seen as interdependent rather than competing directions. In depressive disorders, real progress will come when these elements are connected more effectively in everyday clinical decision-making.
Limitations
Several limitations should be considered when interpreting this review. First, it is a clinically oriented narrative review rather than a systematic review or meta-analysis; therefore, formal PRISMA-based screening, quantitative synthesis, and risk-of-bias assessment were not performed. Second, the included evidence varies substantially across treatment classes. Some interventions, such as esketamine, dextromethorphan–bupropion, brexanolone, zuranolone, and selected bipolar-relevant pharmacotherapies, are supported by regulatory documents and clinical trial evidence, whereas others, including psychedelic-assisted pharmacotherapy and kappa-opioid receptor antagonists, remain investigational or dependent on further confirmatory studies. Third, regulatory status, availability, monitoring requirements, and implementation feasibility differ across jurisdictions and clinical settings. Finally, because depressive disorders are clinically heterogeneous, the treatment framework discussed here should be interpreted as a decision-support perspective rather than a universal prescribing algorithm.
Conclusion
The framework discussed in this review is not intended to replace disorder-specific treatment guidelines, but to clarify how novel and established pharmacotherapies can be interpreted within a mechanism-informed and clinically practical model.
Next-generation pharmacotherapy for depressive disorders should be understood as a mechanism-informed framework that integrates novel compounds with better use of available medications. Current progress is being shaped by rapid-acting and NMDA-related agents, multimodal antidepressants, neuroactive steroid-related approaches, psychedelic-assisted therapy, kappa-opioid receptor antagonists, bipolar-relevant pharmacotherapies, and more deliberate use of augmentation, combination treatment, sequencing, and maintenance planning. At the same time, pharmacogenomics, PK/PD variability, and clinically informed stratification may improve treatment selection and reduce avoidable mismatch in heterogeneous patient populations.
Future advances will depend not only on developing new drugs, but also on improving how treatments are selected, sequenced, combined, monitored, and sustained across unipolar depression, bipolar depression, and TRD. Under this broader view, innovation is defined less by recency alone than by whether a treatment improves pharmacological fit, real-world usability, and long-term clinical value.
Data Sharing Statement
Data sharing is not applicable to this article, as no new datasets were generated or analyzed during the current review.
Ethical Approval and Consent to Participate
This article is a narrative review and does not involve human participants, human data, human tissue, or animal experiments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Lan Qin and Zhengchi Lou contributed equally to this work and share co-first authorship.
Funding
This work was supported by the Shenzhen Science and Technology Program (JCYJ20240813104110014; JCYJ20250604142253071).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rong J, Wang X, Cheng P, Li D, Zhao D. Global, regional and national burden of depressive disorders and attributable risk factors, from 1990 to 2021: results from the 2021 Global Burden of Disease study. Br J Psychiatry. 2025;227(4):688–24. doi:10.1192/bjp.2024.266
2. Pigott HE, Kim T, Xu C, Kirsch I, Amsterdam J. What are the treatment remission, response and extent of improvement rates after up to four trials of antidepressant therapies in real-world depressed patients? A reanalysis of the STAR*D study’s patient-level data with fidelity to the original research protocol. BMJ Open. 2023;13(7). doi:10.1136/bmjopen-2022-063095
3. Jha MK, Mathew SJ. Pharmacotherapies for treatment-resistant depression: how antipsychotics fit in the rapidly evolving therapeutic landscape. Am J Psychiatry. 2023;180:3. doi:10.1176/appi.ajp.20230025
4. Keramatian K. The CANMAT and ISBD guidelines for the treatment of bipolar disorder: summary and a 2023 update of evidence. Focus. 2024;21(4). doi:10.1176/appi.focus.20230009
5. Marwaha S, Palmer E, Suppes T, Cons E, Young AH, Upthegrove R. Novel and emerging treatments for major depression. Lancet. 2022;401(10371):141–153. doi:10.1016/s0140-6736(22)02080-3
6. Njenga C, Ramanuj PP, de Magalhães FJ, Pincus HA. New and emerging treatments for major depressive disorder. BMJ. 2024;386. doi:10.1136/bmj-2022-073823
7. Zelek-Molik A, Litwa E. Trends in research on novel antidepressant treatments. Front Pharmacol. 2025;16:1544795. doi:10.3389/fphar.2025.1544795
8. Kupfer DJ, Duncko R, Giri Shankar V. Pharmacological management of depressive disorders. Medicine. 2024;52(9):583–588. doi:10.1016/j.mpmed.2024.06.015
9. Singh MK, Thase ME. Current progress in targeted pharmacotherapy to treat symptoms of major depressive disorder: moving from broad-spectrum treatments to precision psychiatry. CNS Spectrums. 2025;30(1):e16. doi:10.1017/S1092852925000094
10. IsHak WW, Hirsch D, Renteria S. Depressive disorders: systematic review of approved psychiatric medications (2009-April 2025) and pipeline phase 3 medications. BMC Psychiatry. 2025;25(1):939. doi:10.1186/s12888-025-07141-3
11. Uyar A, Gonul AS. New and emerging pharmacologic treatments for MDD. Front Psychiatry. 2025;16. doi:10.3389/fpsyt.2025.1621887
12. Zhdanava M, Teeple A, Pilon D, Shah A, Caron-Lapointe G, Joshi K. Esketamine nasal spray for major depressive disorder with acute suicidal ideation or behavior: description of treatment access, utilization, and claims-based outcomes in the United States. J Med Econo. 2023;26(1):691–700. doi:10.1080/13696998.2023.2208993
13. Lie PE, Lie TY, Nguyen M, Lie DYC. Ketamine as a bridge therapy: reducing acute suicidality in hospital settings. Healthcare. 2026;14(5):634. doi:10.3390/healthcare14050634
14. Reif A, Bitter I, Buyze J, et al. Esketamine nasal spray versus quetiapine for treatment-resistant depression. N Engl J Med. 2023;389(14):1298–1309. doi:10.1056/NEJMoa2304145
15. Janik A, Qiu X, Lane R, et al. Esketamine monotherapy in adults with treatment-resistant depression: a randomized clinical trial. JAMA psychiatry. 2025;82(9):877. doi:10.1001/jamapsychiatry.2025.1317
16. Repple J, Bayas M, Möser C, Kobayashi NF, Reif A. Current evidence for the role of rapid-acting antidepressants in bipolar depression: a perspective and plan for action. Biol Psychiatry. 2025;98(4):333–342. doi:10.1016/j.biopsych.2025.02.903
17. Rodolico A, Cutrufelli P, Di Francesco A, et al. Efficacy and safety of ketamine and esketamine for unipolar and bipolar depression: an overview of systematic reviews with meta-analysis. Front Psychiatry. 2024;15:1325399. doi:10.3389/fpsyt.2024.1325399
18. Havlik JL, Wahid S, Teopiz KM, McIntyre RS, Krystal JH, Rhee TG. Recent advances in the treatment of treatment-resistant depression: a narrative review of literature published from 2018 to 2023. Curr Psychiatry Rep. 2024;26(4):176–213. doi:10.1007/s11920-024-01494-4
19. Smith-Apeldoorn SY, Veraart JK, Spijker J, Kamphuis J, Schoevers RA. Maintenance ketamine treatment for depression: a systematic review of efficacy, safety, and tolerability. Lancet Psychiatry. 2022;9(11):907–921. doi:10.1016/S2215-0366(22)00317-0
20. Blanco J, Quimbaya P, Mena M, Dodd S, Bustos R-H. Profiling the combination of bupropion and dextromethorphan as a treatment option for major depressive disorder. Expert Rev Neurotherapeu. 2024;24(9):837–848. doi:10.1080/14737175.2024.2374024
21. Blair HA. Dextromethorphan/bupropion in major depressive disorder: a profile of its use. Drugs Therapy Perspect. 2023;39(8):270–278. doi:10.1007/s40267-023-01009-w
22. Iosifescu DV, Jones A, O’Gorman C, et al. Efficacy and safety of AXS-05 (dextromethorphan-bupropion) in patients with major depressive disorder. J Clin Psychiatry. 2022;83(4):21m14345. doi:10.4088/JCP.21m14345
23. Tabuteau H, Jones A, Anderson A, Jacobson M, Iosifescu DV. Effect of AXS-05 (dextromethorphan-bupropion) in major depressive disorder: a randomized double-blind controlled trial. Am J Psychiatry. 2022;179(7):490–499. doi:10.1176/appi.ajp.21080800
24. Wang P, Wang -W-W, Liu Y-Q, et al. The dose-response relationship of vortioxetine on major depressive disorder: an umbrella review. Psychiatry Res. 2024;340:116118. doi:10.1016/j.psychres.2024.116118
25. Chauhan M, Parry R, Bobo WV. Vilazodone for major depression in adults: pharmacological profile and an updated review for clinical practice. Neuropsychia Dis Treatment. 2022;18:1175. doi:10.2147/NDT.S279342
26. Perlemuter G, Cacoub P, Valla D, et al. Characterisation of agomelatine-induced increase in liver enzymes: frequency and risk factors determined from a pooled analysis of 7605 treated patients. CNS Drugs. 2016;30(9):877–888. doi:10.1007/s40263-016-0351-6
27. Raja A, Ahmed S, Basit Ali Siddiqui M, et al. Evaluating the safety and efficacy of zuranolone in the management of major depressive disorder and postpartum depression, with or without concurrent insomnia: a rigorous systematic review and meta-analysis. Front Psychiatry. 2024;15:1425295. doi:10.3389/fpsyt.2024.1425295
28. Garafola S, Shiferaw E, Dev V. Safety of brexanolone in adults with postpartum depression: postmarketing surveillance data. Drugs Real World Outcomes. 2023;10(3):351–356. doi:10.1007/s40801-023-00372-4
29. St. Onge E, Patel P, Whitner C. Zuranolone for the treatment of postpartum depression. J Pharmacy Technol. 2025;41(1):32–37. doi:10.1177/87551225241287383
30. Heo Y-A. Zuranolone: first approval: Y.-A. Heo. Drugs. 2023;83(16):1559–1567. doi:10.1007/s40265-023-01953-x
31. Hitt EM. Zuranolone: a narrative review of a new oral treatment for postpartum depression. Clin Ther. 2024;46(5):433–438. doi:10.1016/j.clinthera.2024.04.001
32. Goodwin GM, Aaronson ST, Alvarez O, et al. Single-dose psilocybin for a treatment-resistant episode of major depression. N Engl J Med. 2022;387(18):1637–1648. doi:10.1056/NEJMoa2206443
33. Raison CL, Sanacora G, Woolley J, et al. Single-dose psilocybin treatment for major depressive disorder: a randomized clinical trial. JAMA. 2023;330(9):843–853. doi:10.1001/jama.2023.14530
34. Wong S, Le GH, Vasudeva S, et al. Preclinical and clinical efficacy of kappa opioid receptor antagonists for depression: a systematic review. J Affective Disord. 2024;362:816–827. doi:10.1016/j.jad.2024.07.030
35. Juraev A, Shodiyeva E. Emerging pharmacological treatments for major depressive disorder: a narrative review of clinical trials from 2023 to 2025. J Clin Biomed Re. 2026;2(1):190–199.
36. Yildiz A, Siafis S, Mavridis D, Vieta E, Leucht S. Comparative efficacy and tolerability of pharmacological interventions for acute bipolar depression in adults: a systematic review and network meta-analysis. Lancet Psychiatry. 2023;10(9):693–705. doi:10.1016/S2215-0366(23)00199-2
37. Bahji A, Ermacora D, Stephenson C, Hawken ER, Vazquez G. Comparative efficacy and tolerability of adjunctive pharmacotherapies for acute bipolar depression: a systematic review and network meta-analysis. Can J Psychiatry. 2021;66(3):274–288. doi:10.1177/0706743720970857
38. Nabulsi N. Effects of adjunctive cariprazine formulary restrictions in major depressive disorder. Am J Manag Care. 2025;1(7).
39. Arnone D, Östlundh L, Mosa M, et al. Efficacy of lamotrigine in the treatment of unipolar and bipolar depression: meta-analysis of acute and maintenance randomised controlled trials. Pharmaceuticals. 2025;18(10):1590. doi:10.3390/ph18101590
40. Simon GE, Moise N, Mohr DC. Management of depression in adults: a review. JAMA. 2024;332(2):141–152. doi:10.1001/jama.2024.5756
41. Verma C, Jain K, Saini A, Mani I, Singh V. Exploring the potential of drug repurposing for treating depression. Progress Molecular Biol Transl Sci. 2024;207:79–105.
42. Kwaśny A, Włodarczyk A, Dywel A, Szarmach J, Strandberg O, Cubała WJ. Residual insomnia in major depressive disorder: a systematic review. Front Psychiatry. 2023;14:1190415. doi:10.3389/fpsyt.2023.1190415
43. Nagele P, Conway CR, Zorumski CF. Purposeful drug repurposing. JAMA psychiatry. 2025;82(7):638–639. doi:10.1001/jamapsychiatry.2025.0900
44. Scott F, Hampsey E, Gnanapragasam S, et al. Systematic review and meta-analysis of augmentation and combination treatments for early-stage treatment-resistant depression. J Psychopharmacol. 2023;37(3):268–278. doi:10.1177/02698811221104058
45. El Hussein MT, Bal R. Pharmacotherapy: major depressive disorder and difficult-to-treat depression: review for nurse practitioners. J Nurse Practit. 2025;21(8):105458. doi:10.1016/j.nurpra.2025.105458
46. Ercis M, Ozerdem A, Singh B. When and how to use lithium augmentation for treating major depressive disorder. J Clini Psych. 2023;84(2):23ac14813–14823ac14813. doi:10.4088/JCP.23ac14813
47. Furukawa Y, Hamza T, Cipriani A, Furukawa TA, Salanti G, Ostinelli EG. Optimal dose of aripiprazole for augmentation therapy of antidepressant-refractory depression: preliminary findings based on a systematic review and dose–effect meta-analysis. Br J Psychiatry. 2022;221(2):440–447. doi:10.1192/bjp.2021.165
48. Xie M, Qiu Y, Wang M, et al. Adjunctive cariprazine as a novel effective strategy for treating major depressive disorder: a systematic review and meta-analysis. J Psychiatr Res. 2024;172:71–80. doi:10.1016/j.jpsychires.2024.02.018
49. Singh B, Sundaresh V. Thyroid hormone use in mood disorders: revisiting the evidence. J Clini Psych. 2022;83(5):22ac14590. doi:10.4088/JCP.22ac14590
50. Gaddey HL, Mason B, Naik A. Depression: managing resistance and partial response to treatment. Am Family Phys. 2024;109(5):410–416.
51. Lenze EJ, Mulsant BH, Roose SP, et al. Antidepressant augmentation versus switch in treatment-resistant geriatric depression. N Engl J Med. 2023;388(12):1067–1079. doi:10.1056/NEJMoa2204462
52. Henssler J, Alexander D, Schwarzer G, Bschor T, Baethge C. Combining antidepressants vs antidepressant monotherapy for treatment of patients with acute depression: a systematic review and meta-analysis. JAMA Psychiatry. 2022;79(4):300–312. doi:10.1001/jamapsychiatry.2021.4313
53. Saelens J, Gramser A, Watzal V, Zarate CA, Lanzenberger R, Kraus C. Relative effectiveness of antidepressant treatments in treatment-resistant depression: a systematic review and network meta-analysis of randomized controlled trials. Neuropsychopharmacology. 2025;50(6):913–919. doi:10.1038/s41386-024-02044-5
54. Sackeim HA, Aaronson ST, Bunker MT, et al. Update on the assessment of resistance to antidepressant treatment: rationale for the antidepressant treatment history form: short form-2 (ATHF-SF2). J Psychiatr Res. 2024;176:325–337. doi:10.1016/j.jpsychires.2024.05.046
55. Kishi T, Ikuta T, Sakuma K, et al. Antidepressants for the treatment of adults with major depressive disorder in the maintenance phase: a systematic review and network meta-analysis. Mol Psychiatry. 2023;28(1):402–409. doi:10.1038/s41380-022-01824-z
56. Pan Z, Zhang H, Li B, et al. Strategies for antidepressant medications in the maintenance phase: a systematic review and network Meta-analysis. J Affective Disord. 2025;387:119460. doi:10.1016/j.jad.2025.119460
57. Stephenson JJ, Touya M, Chrones L, Pandya SA, Teng -C-C, Clayton AH. Antidepressant use and treatment-emergent sexual dysfunction among patients with major depressive disorder: results from an internet-based survey study. J Affect Disord Rep. 2024;16:100750. doi:10.1016/j.jadr.2024.100750
58. Zhang -M-M, Tan X, Zheng Y-B, et al. Incidence and risk factors of antidepressant withdrawal symptoms: a meta-analysis and systematic review. Mol Psychiatry. 2025;30(5):1758–1769. doi:10.1038/s41380-024-02782-4
59. Frye MA, Nemeroff CB. Pharmacogenomic testing for antidepressant treatment selection: lessons learned and roadmap forward. Neuropsychopharmacology. 2024;49(1):282–284. doi:10.1038/s41386-023-01667-4
60. Khorassani F, Jermain M, Cadiz C. Pharmacogenomic testing to guide treatment of major depressive disorder: a systematic review. Curr Treat Options Psychiatry. 2024;11(2):123–140. doi:10.1007/s40501-024-00316-x
61. Bousman CA, Stevenson JM, Ramsey LB, et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline for CYP2D6, CYP2C19, CYP2B6, SLC6A4, and HTR2A genotypes and serotonin reuptake inhibitor antidepressants. Clin Pharmacol Ther. 2023;114(1):51–68. doi:10.1002/cpt.2903
62. Xu L, Li L, Wang Q, Pan B, Zheng L, Lin Z. Effect of pharmacogenomic testing on the clinical treatment of patients with depressive disorder: a randomized clinical trial. J Affective Disorders. 2024;359:117–124. doi:10.1016/j.jad.2024.05.063
63. Funk CSM, Hart XM, Gründer G, et al. Is therapeutic drug monitoring relevant for antidepressant drug therapy? Implications from a systematic review and meta-analysis with focus on moderating factors. Frontiers in Psychiatry. 2022;13:826138. doi:10.3389/fpsyt.2022.826138
64. Dołoto A, Bąk E, Batóg G, Piątkowska-Chmiel I, Herbet M. Interactions of antidepressants with concomitant medications—safety of complex therapies in multimorbidities. Pharmacol Rep. 2024;76(4):714–739. doi:10.1007/s43440-024-00611-7
65. Oliva V, Fico G, De Prisco M, Gonda X, Rosa AR, Vieta E. Bipolar disorders: an update on critical aspects. Lancet Regional Health Euro. 2025;48:101135. doi:10.1016/j.lanepe.2024.101135
66. Laifenfeld D, Albeldas C, Solal TC, McIntyre RS, Stahl S. Toward precision psychiatry: innovations and prospects in treating depression. Primary Care companion CNS Disord. 2025;27(5):25nr03970. doi:10.4088/PCC.25nr03970
67. Husain MI, Nigah Z, Ansari SUH, et al. Measurement-based care to enhance antidepressant treatment outcomes in major depressive disorder: a randomized clinical trial. JAMA Network Open. 2025;8(9):e2529427. doi:10.1001/jamanetworkopen.2025.29427
68. Machleid F, Michnevich T, Huang L, et al. Remote measurement-based care interventions for mental health: systematic review and meta-analysis. JMIR Mental Health. 2026;13:e63088. doi:10.2196/63088
69. Paganin W. Treatment-resistant depression: time to rethink current definitions and clinical practice. Front Psychiatry. 2026;16:1733678. doi:10.3389/fpsyt.2025.1733678
70. Lundberg J, Cars T, Lööv S-Å, et al. Association of treatment-resistant depression with patient outcomes and health care resource utilization in a population-wide study. JAMA Psychiatry. 2023;80(2):167–175. doi:10.1001/jamapsychiatry.2022.3860
71. Lucido MJ, Dunlop BW. Emerging medications for treatment-resistant depression: a review with perspective on mechanisms and challenges. Brain Sci. 2025;15(2):161. doi:10.3390/brainsci15020161
72. Chopra A, Luccarelli J, Cohen JN, Mischoulon D, Stern TA. Evaluation, treatment, and referral of treatment-resistant depression in primary care. Primary Care companion CNS Disord. 2023;25(4):22f03438. doi:10.4088/PCC.22f03438
73. Thase ME. Recent developments pertaining to treatment-resistant depression: a 40-year perspective. World Psychiatry. 2023;22(3):413. doi:10.1002/wps.21134
74. Keramatian K, Chakrabarty T, DuBow A, Saraf G, Yatham LN. New pharmacologic approaches to the treatment of bipolar depression: K. Keramatian et al. Drugs. 2023;83(10):843–863. doi:10.1007/s40265-023-01872-x
75. Li S, Xu C, Hu S, Lai J. Efficacy and tolerability of FDA-approved atypical antipsychotics for the treatment of bipolar depression: a systematic review and network meta-analysis. Eur Psychiatry. 2024;67(1):e29. doi:10.1192/j.eurpsy.2024.25
76. Fung S. Treat bipolar depression with atypical antipsychotics and mood stabilisers; new therapies require further study. Drugs Therapy Perspect. 2024;40(3):109–114. doi:10.1007/s40267-024-01054-z
77. Oliva V, De Prisco M, La Spina E, et al. Switch to mania after acute antidepressant treatment for bipolar depression: a systematic review and network meta-analysis of randomised controlled trials. EClinicalMedicine. 2025;87.
78. Niarchou E, Roberts L, Naughton BD. What is the impact of antidepressant side effects on medication adherence among adult patients diagnosed with depressive disorder: a systematic review. J Psychopharmacol. 2024;38(2):127–136. doi:10.1177/02698811231224171
79. Del Pino-Sedeño T, Infante-Ventura D, Hernández-González D, et al. Sociodemographic and clinical predictors of adherence to antidepressants in depressive disorders: a systematic review with a meta-analysis. Front Pharmacol. 2024;15:1327155. doi:10.3389/fphar.2024.1327155
80. McIntyre RS, Bitter I, Buyze J, et al. Safety and tolerability of esketamine nasal spray versus quetiapine extended release in patients with treatment resistant depression. Eur Neuropsychopharmacol. 2024;85:58–65. doi:10.1016/j.euroneuro.2024.05.009
81. Zaki N, Chen L, Lane R, et al. Safety and efficacy with esketamine in treatment-resistant depression: long-term extension study. Int J Neuropsychopharmacol. 2025;28(6):yaf027. doi:10.1093/ijnp/pyaf027
82. Ramadan S, Tay L, Kaur H, et al. Bipolar disorder: systematic review of approved psychiatric medications (2008–2024) and pipeline Phase-3 medications. J Affect Disord. 2025;390:119778. doi:10.1016/j.jad.2025.119778
83. Kajumba MM, Kakooza-Mwesige A, Nakasujja N, Koltai D, Canli T. Treatment-resistant depression: molecular mechanisms and management. Mol Biomed. 2024;5(1):43. doi:10.1186/s43556-024-00205-y
84. Rost F, Booker T, Gonsard A, et al. The complexity of treatment-resistant depression: a data-driven approach. J Affective Disord. 2024;358:292–301. doi:10.1016/j.jad.2024.04.093
85. Nishida K, Osaka H, Kanazawa T. Development progress of drugs for bipolar disorder: 75 Years after lithium proved effective. J Psychiatr Res. 2024;180:177–182. doi:10.1016/j.jpsychires.2024.10.011
86. De Crescenzo F, De Giorgi R, Garriga C, et al. Real-world effects of antidepressants for depressive disorder in primary care: population-based cohort study. Br J Psychiatry. 2025;226(5):278–287. doi:10.1192/bjp.2024.194
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.