Back to Journals » Medical Devices: Evidence and Research » Volume 18
New Bipolar Electrosurgical Vessel Sealing Device Provides Improved Performance and Procedural Efficiency
Authors Chambers R, Sarno D ![]() , Roweton S
, Roweton S
Received 12 October 2024
Accepted for publication 20 January 2025
Published 25 January 2025 Volume 2025:18 Pages 75—86
DOI https://doi.org/10.2147/MDER.S498873
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rheagan Chambers, Danielle Sarno, Susan Roweton
Surgical Research and Development, Surgical Operating Unit, Medtronic, Lafayette, CO, USA
Correspondence: Susan Roweton, Email [email protected]
Purpose: This study compared the performance of the new LigaSure™ XP Maryland Jaw Sealer/Divider (XP Maryland) to that of LigaSure Atlas™ (Atlas) and LigaSure™ Dolphin Tip (Dolphin Tip), two early LigaSure™ (LigaSure) devices characterized by consistent and reliable clinical performance.
Methods: Ex vivo bench testing on porcine renal arteries compared burst pressures, seal times, and rates of sticking, incomplete cuts, and charring between XP Maryland and Atlas and between XP Maryland and Dolphin Tip. In vivo acute testing on a porcine model compared thermal spread, seal times, and rates of hemostasis, sticking, and incomplete cuts between XP Maryland and the two early LigaSure devices.
Results: Ex vivo, XP Maryland showed a significantly faster mean seal time compared to Dolphin Tip (P < 0.0001) and Atlas (P < 0.0001). XP Maryland had fewer incomplete cuts than Dolphin Tip (P < 0.0001) and fewer sticking incidents than Atlas (P = 0.0019). Atlas had a statistically higher average burst pressure compared to XP Maryland (P < 0.0001). As with ex vivo results, XP Maryland had a significantly faster mean seal time in vivo compared to Dolphin Tip (P = 0.0168) and Atlas (P < 0.0001). Other in vivo results showed XP Maryland had fewer incomplete cuts compared to Dolphin Tip (P < 0.0001) and statistically less lateral thermal spread than Atlas (P = 0.0010). For all other ex vivo and in vivo performance characteristics, no statistically significant differences were found between XP Maryland and the other devices.
Conclusion: The study demonstrated the consistent and reliable performance of XP Maryland and the two early LigaSure devices. In addition, the studies showed XP Maryland has some improved performance characteristics when compared to Atlas and Dolphin Tip that may result in improved procedural efficiency and may reduce potential surgical risks.
Keywords: LigaSure, radiofrequency energy, electrosurgery
Introduction
LigaSure™ (LigaSure) instruments use radiofrequency (RF) energy and pressure to seal blood vessels and tissue bundles and to achieve hemostasis during tissue dissection. LigaSure technology was introduced in 1998 and has since been used in over 25 million surgical procedures.1 A variety of LigaSure instruments are available for both laparoscopic and open procedures to address unique challenges in a range of specialties including general, thoracic, gynecologic, bariatric, and colorectal surgery. In all applications, LigaSure instruments must demonstrate consistent and reliable clinical performance. This was true for early LigaSure instruments, and it continues to be essential as new LigaSure instruments with improved design and performance characteristics are developed.
The LigaSure Atlas™ Tissue Fusion Laparoscopic Instrument (Atlas) is an early LigaSure device approved by the FDA in 2001. It has been in continuous use since its introduction over 20 years ago and is sold in and outside of the United States. The Atlas LS1020 has a 20-cm shaft length and is indicated for use in open procedures. The Atlas LS1037 has a 37-cm shaft length and is designed to fit inside a 10-mm cannula for laparoscopic procedures. Atlas handsets seal vessels ≤ 7 mm and comprise blades for dividing either sealed or unsealed tissue.2 Review of literature from 2001 through 2024 reveals descriptions of the clinical use of Atlas in a range of surgeries. These include splenectomies,3–5 gastrectomy procedures,6–10 liver resections,11,12 bowel resections,13,14 a thyroidectomy,15 an adrenalectomy,16 and gynecologic surgery.17 The literature review found preclinical studies investigating Atlas’ key performance characteristics not easily measured clinically. Seal time, seal strength (burst pressure), and the amount of thermal tissue effect adjacent to the seal (thermal spread) have been investigated for Atlas.18–22 Studies involved comparison of Atlas to other commercially available vessel sealing devices. Two other preclinical studies focused on specific applications for Atlas. One porcine study assessed the use of Atlas for liver resection23 and another focused specifically on the ability of Atlas to seal vessel bundles.24
The LigaSure™ Dolphin Tip Laparoscopic Sealer/Divider (Dolphin Tip) is another early LigaSure device. It was approved in 2003 and is currently available outside of the United States. The Dolphin Tip LS1500 has a 37-cm shaft length and a 5-mm shaft diameter and is designed for use during laparoscopic procedures. Like Atlas, Dolphin Tip seals vessels ≤ 7 mm and has a deployable cutting blade. A literature review found publications concerning the clinical use of Dolphin Tip, the most recent publication being from 2022. Papers describe the use of Dolphin Tip for a gastrectomy,25 liver resections,26–28 and thyroidectomies.15,29 As with Atlas, literature also described preclinical studies evaluating performance characteristics of Dolphin Tip. In most cases, studies compared Dolphin Tip’s performance to that of other vessel sealing technologies. Seal time, seal burst pressure, and thermal spread were measured for Dolphin Tip.19,20,30–33 Two studies evaluated Dolphin Tip’s cutting performance32,33 and one of these studies also measured tissue sticking to the instrument jaws.33
The LigaSure™ XP Maryland Jaw Sealer/Divider (XP Maryland) is a new instrument. It is a Maryland-style LigaSure device with a 5-mm diameter shaft that is provided in shaft lengths for both open and laparoscopic procedures. It can be used on vessels ≤ 7 mm in diameter. Considerable design differences have been implemented in the XP Maryland, though, to differentiate it from LigaSure predecessors. The XP Maryland is the first LigaSure device with 360° continuous jaw rotation. It is offered with two handle options, a latching handle or a one-step sealing handle. The XP Maryland also has fine, relatively long jaws that allow sealing and cutting to the jaw tips for improved dissection precision (Figure 1).
 |
Figure 1 Seal and cut length information for LigaSure Atlas, Dolphin Tip, and XP Maryland. |
It is important to assess the performance of the new XP Maryland device to ensure it demonstrates the consistent and reliable performance associated with early, trusted LigaSure technology. The purpose of this study was to compare the XP Maryland to both the Atlas and Dolphin Tip, two early LigaSure devices.
Materials and Methods
Performance characteristics were evaluated in both ex vivo and in vivo testing and included the evaluation of burst pressure, seal time, thermal spread, and hemostasis for the XP Maryland, Dolphin Tip, and Atlas. The XP Maryland and the Atlas were used with the Valleylab™ FT10 Energy Platform (FT10) for both ex vivo and in vivo testing. The Dolphin Tip was used with the ForceTriad™ Energy Platform (ForceTriad) for all testing as it is not compatible with the FT10. All instruments were used on the default settings of their respective generators. Instruments were used per the manufacturer’s instructions for use (IFU).
Ex vivo Bench Testing
Burst pressure testing evaluated the strength of the seals created with the LigaSure devices. For burst pressure, a minimum sample size was determined using a statistical power analysis followed by an adjustment for the correlation in seal strength values between seal halves. The effective sample size equation shown below was used:34

where  =estimated intraclass correlation=0.60,
=estimated intraclass correlation=0.60,  =number of measurements per seal, and
=number of measurements per seal, and  =number of seals/clusters.
=number of seals/clusters.
The calculated minimum sample size was determined to be 40 seals (80 bursts) per device group to achieve 90% power. The actual minimum number of seals required per device group was then increased to 42 seals (84 bursts). This ensured an equal number of seals were made across each of the two devices tested within each group as well as across three vessel size categories. The vessel size categories ensured the full indicated vessel size range was tested and were defined as small (≤ 3 mm), medium (3.1–5.0 mm), and large (5.1–7.0 mm).
Ex vivo porcine renal arteries of outer diameter ≤ 7 mm were sealed. The ex vivo tissue was a by-product of the food production industry and was from a USDA-inspected abattoir. Porcine kidneys from domestic swine, approximately 6 months old, were obtained. The renal arteries were dissected from these kidneys and utilized for testing within 24–36 hours postmortem. Prior to each activation, the tester flattened the vessel to simulate dilation due to blood flow. Flattened vessel diameters were measured with digital calipers and then vessels were sealed and bisected at the site of the measurement. Each sealed and bisected vessel yielded two burst pressure values. Each sealed vessel half was infused with de-ionized water at 100 mL/h until leakage occurred. The maximum burst pressure achieved for each sealed half was included in the analysis performed using JMP® 16 Statistical Software. Seal time, or the total time in seconds from the activation start to end of seal audible tone, was recorded by the energy platforms. Additional attributes that contribute to overall device performance were evaluated. Incomplete cuts were defined as when the user fully deploys the knife blade, but the blade does not fully transect the seal zone. A sticking incident was defined as when the user must manually remove the sealed or desiccated tissue from the seal plate of the device. A charring incident was defined as when the user observed the seal zone was burned and/or visibly blackened.
A graphical analysis of the relationship between burst pressure and vessel diameter was made to assess the seal performance of the LigaSure devices across the entire indicated vessel size range. The effective use of a scatter plot combined with a quadratic regression model and associated 90% prediction limits enhanced seal performance visualization. A simulation was run against the regression model to objectively estimate the reliability of having a burst value exceeding 360 mmHg or three times the normal systolic blood pressure of a healthy human. First, a vessel diameter was simulated based on a uniform distribution of the burst pressures collected. This is conservative as large vessels are as likely to be selected as small or medium-sized vessels. Using the regression model and the simulated vessel diameter value, a burst pressure value was simulated. Experimental error was also simulated based on the residual error of the respective model and then added to the prediction. One million burst pressure values were simulated, and the conformance rate was determined by evaluating whether or not the simulated values met the 360 mmHg burst limit. The estimated conformance rate for a LigaSure device should be ≥ 95% for optimal burst pressure performance.
In vivo Acute Testing
An in vivo study was conducted at Inotiv (Ft. Collins, Colorado). The study design and animal usage were reviewed and approved by the Inotiv Institutional Animal Care and Use Committee (IACUC) for compliance with regulations prior to study start. Animal welfare for this study was compliant with the United States Department of Agriculture (USDA) Animal Welfare Act, National Research Council of the National Academies Guide for the Care and Use of Laboratory Animals (8th edition), National Institutes of Health Office of Laboratory Animal Welfare Public Health Service (PHS) Policy on Humane Care and Use of Laboratory Animals, and the American Veterinary Medical Association (AVMA) Guidelines for Euthanasia.
In vivo testing was conducted to evaluate performance characteristics including thermal spread and ability to achieve hemostasis. The sample size for both thermal spread and hemostasis evaluation were calculated using a method like that described previously for burst pressure. For thermal spread, the calculated minimum sample size was determined to be 18 measurements (minimum of five seals having four measurements each) per device group to achieve 90% power. The actual minimum number of seals made per device group was then increased to 64 measurements (16 seals) to account for correlation between seal halves and to obtain a number that divided evenly among the devices within a group. For hemostasis, a minimum sample size of 190 seals per device group was determined to detect a 10% difference in non-hemostatic seals on various tissue types.
Acute testing utilized three female pigs weighing 40–80 kg. A variety of vessels and tissue types were sealed including epigastric veins, small bowel mesentery, root of small bowel mesentery, broad ligament, omentum, gastrosplenic artery/vein bundles, gastroepiploic artery/vein bundles, splenic arteries, short gastric artery/vein bundles, saphenous artery/vein bundles, lumbar artery/vein bundles, femoral arteries, iliac arteries, renal arteries, and carotid arteries.
Each animal underwent standard surgical preparation and positioning for exploratory laparotomy. Each pig was pre-medicated, placed in a dorsal recumbent position, and maintained under anesthesia. Systolic blood pressures were monitored and maintained within a range of 80–120 mmHg throughout the procedure. The left and right epigastric veins were carefully skeletonized and sealed to evaluate both hemostasis and thermal spread. After activations were performed on the epigastric veins, a midline celiotomy was performed to expose the viscera. Dissection along with multiple surgical procedures including, but not limited to, bowel resection, splenectomy, gastrectomy, and nephrectomy were performed to locate and expose vasculature and tissue for evaluation of vessel sealing. Isolated vessels and artery/vein bundles were measured in situ with calipers. Isolated bundles were measured across the entire bundle and then measurements were made of the individual arteries within each bundle. All devices were used in each animal and the devices were evenly rotated throughout the procedure. Vessels were placed in the middle of the instrument jaws and sealed and transected according to the device’s IFU. Hemostasis, meaning no active blood flow (either pulsatile or oozing) from the vessel seal, was visually verified. Seal times were recorded by the energy platforms. Sticking incidents and incomplete cuts were assessed in the same manner described for ex vivo bench testing.
Histology samples were collected to evaluate the amount of lateral thermal spread. Each specimen of interest was preserved in 10% phosphate buffered formalin for a minimum of 24 hours prior to undergoing standard histological processing. Histological evaluation was conducted with the use of picrosirius red (PSR) staining. Thermal spread measurements were made by a blinded histologist. For each sealed vessel half, there were potentially two resulting measurements for thermal spread analysis as shown in Figure 2.
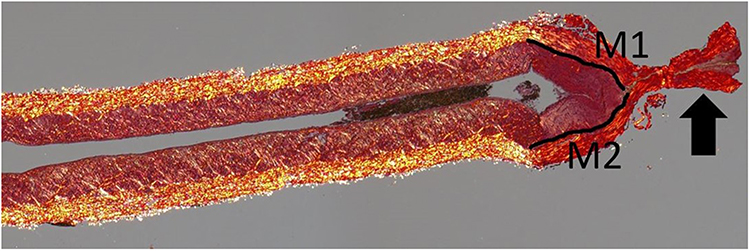 |
Figure 2 One-half of a sealed and divided blood vessel stained with picrosirius red (PSR). Thermal spread measurements M1 and M2 are shown as solid black lines along the vessel walls. The black arrow indicates the seal zone created by the LigaSure XP Maryland device. |
Results
Ex vivo Bench Testing
Mean burst pressure and standard deviation were calculated for each device group (Table 1). XP Maryland (1082 ± 347 mmHg) had a higher mean burst pressure and a lower standard deviation Dolphin Tip (1065 ± 413 mmHg) indicating less variation in burst pressure, fewer outliers, and more clustering of burst pressure data points near the mean (Figure 3). A multi-factor ANOVA method was used for analysis of continuous burst pressure and seal time data.34 No statistical difference was found between the XP Maryland and Dolphin Tip mean burst pressures (P = 0.9263). Ex vivo mean seal time on renal arteries for XP Maryland (1.94 ± 0.72s) was less than that of Dolphin Tip (3.23 ± 0.61s), and the difference was statistically significant (P < 0.0001). The mean seal time for the XP Maryland was 40% faster than the average seal time for the Dolphin Tip (Figure 4). The probability of achieving a burst pressure ≥ 360 mmHg for sealed renal arteries ≤ 7 mm was calculated to be 98.0% for XP Maryland and 95.8% for Dolphin Tip. The quadratic regression model (Figure 5) allows for visualization of any trends and the relationship between burst pressure and vessel diameter. It is useful for assessing the performance of the device across the vessel diameter range. Prediction bands shown in light gray are where a high percentage of burst pressure values are expected to fall based on the simulation.
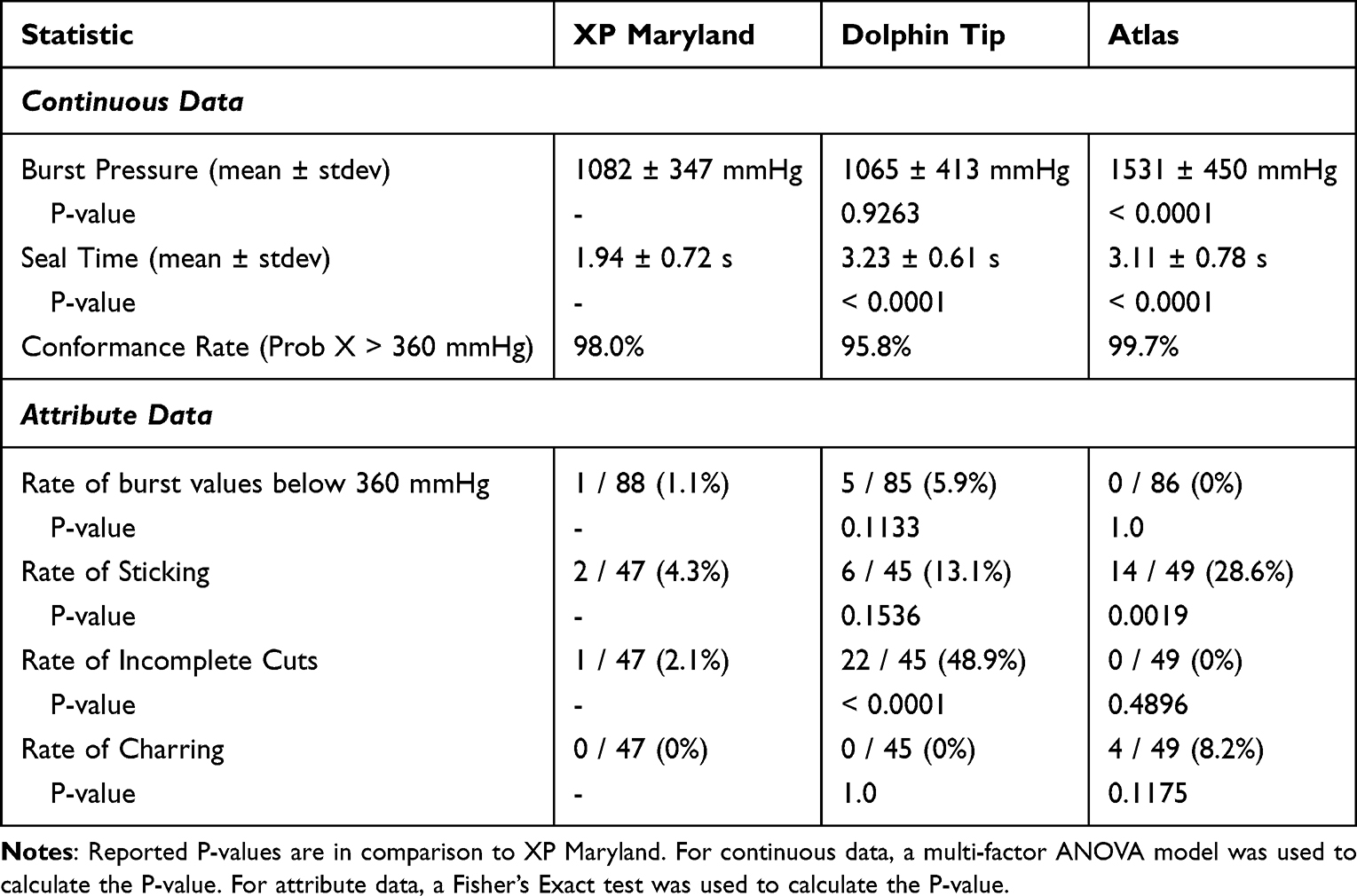 |
Table 1 Summary of XP Maryland Vs Dolphin Tip and XP Maryland Vs Atlas Ex Vivo Bench Results |
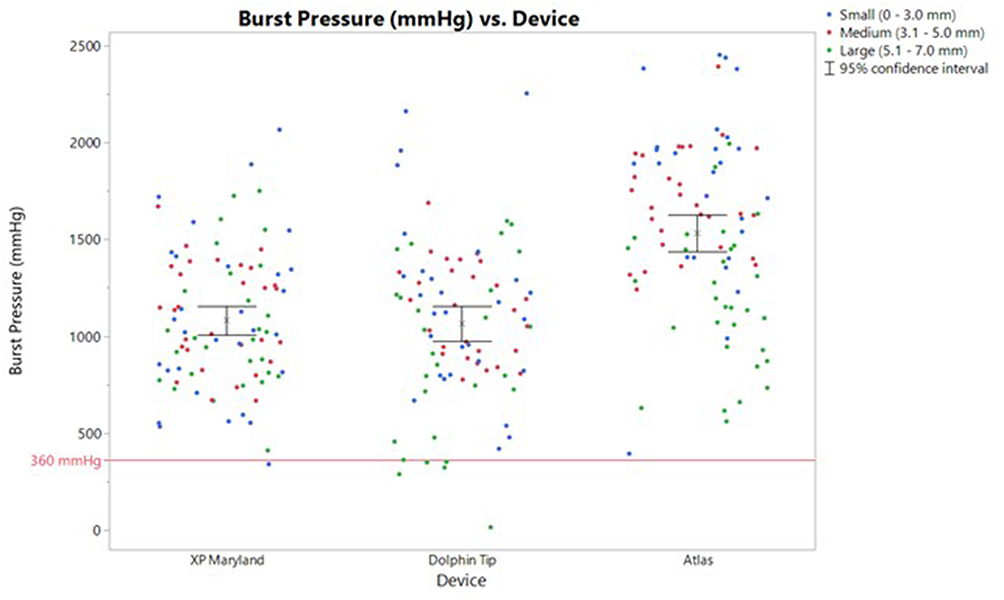 |
Figure 3 Burst pressures of renal artery seal half by device group. Data points are color coded by vessel size category. The mean “x” and 95% confidence interval of the mean (bars) are indicated for each group. The Lower Specification Limit (LSL) for LigaSure devices of 360 mmHg, or three times normal systolic blood pressure, is denoted by a red line. |
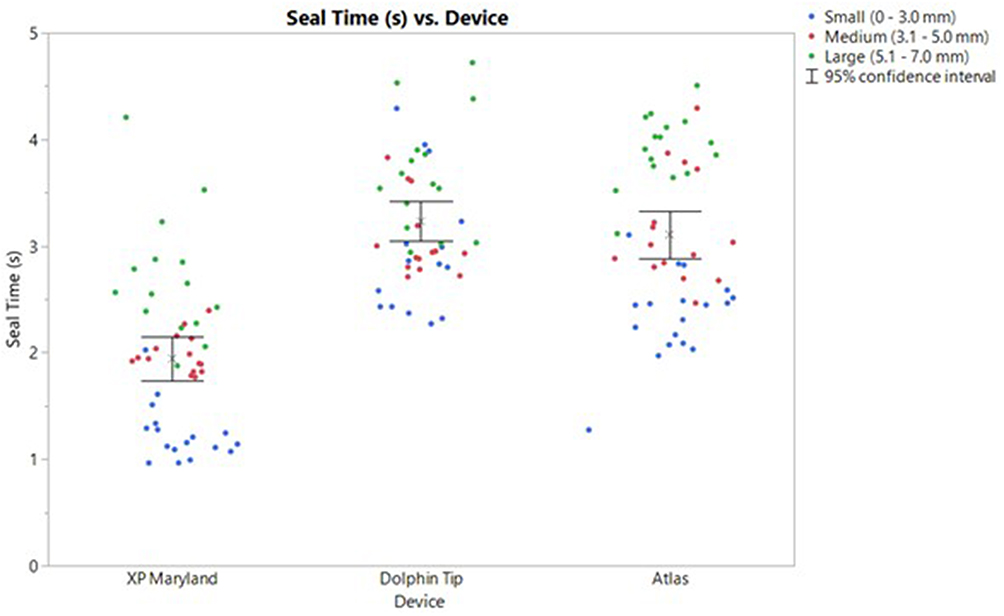 |
Figure 4 Seal time by device group is color coded by vessel size category. The mean “x” and 95% confidence interval of the mean (bars) are indicated for each group. |
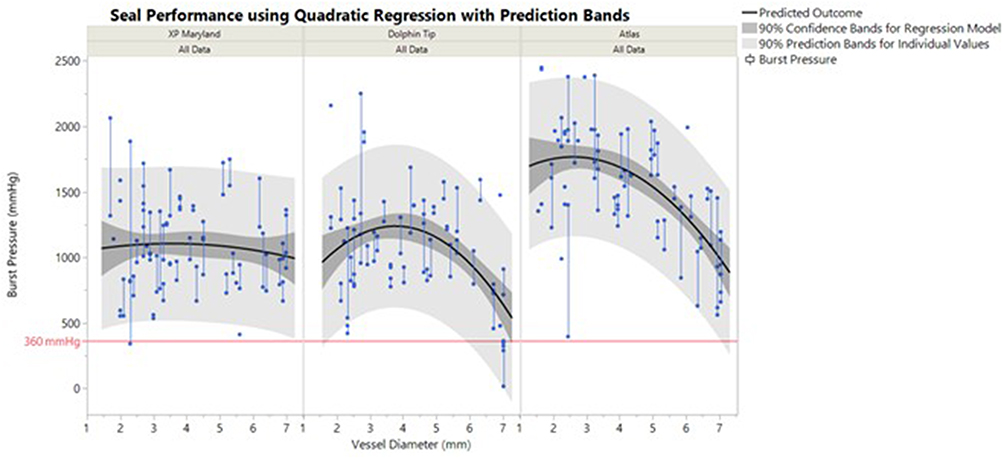 |
Figure 5 Burst pressure versus vessel diameter. Burst pressure renal artery seal half measurements are shown as solid blue circles, with both halves of one seal connected by vertical lines. The black line represents the quadratic regression model while the dark gray shade describes 90% confidence bands on the mean burst value. The light gray shaded area indicates the predicted range of simulated burst values via 90% prediction bands. |
All proportion-based statistics were compared by using Fisher’s exact test. The rate of burst values below the lower specification limit (LSL) of 360 mmHg for XP Maryland was one out of 88 total burst values while Dolphin Tip had five low burst values out of 85 total burst values. No statistical difference was found in the rate of low bursts between XP Maryland and Dolphin Tip (P = 0.1133). There were two sticking occurrences out of 47 seals for XP Maryland and six sticking occurrences out of 45 seals for Dolphin Tip. No statistical difference was identified for the rate of sticking between the two devices (P = 0.1536). There was one incomplete cut for XP Maryland out of 47 seal and cut cycles while Dolphin Tip had 22 incomplete cuts out of 45 seal and cut cycles. The XP Maryland had a significantly lower rate of incomplete cuts than Dolphin Tip (P < 0.0001). Dolphin Tip’s rate of incomplete cuts was 5.8 times more than that of the XP Maryland. There were no charring occurrences during bench testing for either XP Maryland or Dolphin Tip.
XP Maryland (1082 ± 347 mmHg) had a lower mean burst pressure and a lower standard deviation than Atlas (1531 ± 450 mmHg). A multi-factor ANOVA revealed Atlas had a statistically higher mean burst pressure than the XP Maryland (P < 0.0001). The mean burst pressure of Atlas was 1.4 times higher than that of the XP Maryland. Ex vivo mean seal time on renal arteries for XP Maryland (1.94 ± 0.72s) was less than that of Atlas (3.11 ± 0.78s), and the difference was statistically significant (P < 0.0001). The mean seal time for the XP Maryland was 38% faster than the mean seal time for the Atlas (Figure 4). The probability of achieving a burst pressure ≥ 360 mmHg for sealed renal arteries ≤ 7 mm was 98.0% for XP Maryland and 99.7% for Atlas.
Atlas had no burst values below 360 mmHg out of 86 total burst values, and there was no statistical difference in the rate of low bursts between XP Maryland and Atlas (P = 1.0). XP Maryland had statistically fewer sticking occurrences than Atlas that had 14 occurrences out of 49 seals (P = 0.0019). Atlas’ rate of sticking occurrences was 2.2 times more than that of the XP Maryland. Atlas had no incomplete cuts out of 49 seal and cut cycles, and no statistical difference was found in the rate of incomplete cuts between XP Maryland and Atlas (P = 0.4896). Atlas had four occurrences of charring out of 49 seals. There was no statistical difference in the rate of charring between XP Maryland and Atlas (P = 0.1175).
In vivo Acute Testing
Mean lateral thermal spread and standard deviation on isolated vasculature and artery/vein (A/V) bundles were measured for each device (Table 2). XP Maryland (1.29 ± 0.40 mm) had lower mean thermal spread than Dolphin Tip (1.54 ± 0.55 mm), but the difference was not statistically significant (P = 0.1186). A graph of all thermal spread measurements is included in Figure 6. Considering the arithmetic means for in vivo seal times, XP Maryland (2.71 ± 1.22s) had a higher mean seal time and a higher standard deviation than Dolphin Tip (2.64 ± 0.30s). However, XP Maryland was found to have a statistically smaller least squares mean seal time than Dolphin Tip (P = 0.0168) when considering the output from the multifactor ANOVA model analysis. The ANOVA considers the number of seals for each tissue type in addition to seal time values. XP Maryland sealed most tissue types more quickly than Dolphin tip, accounting for the observed difference in mean values. A graph of in vivo seal times by device is included in Figure 7.
 |
Table 2 Summary of XP Maryland Vs Dolphin Tip and XP Maryland Vs Atlas in Vivo Acute Results |
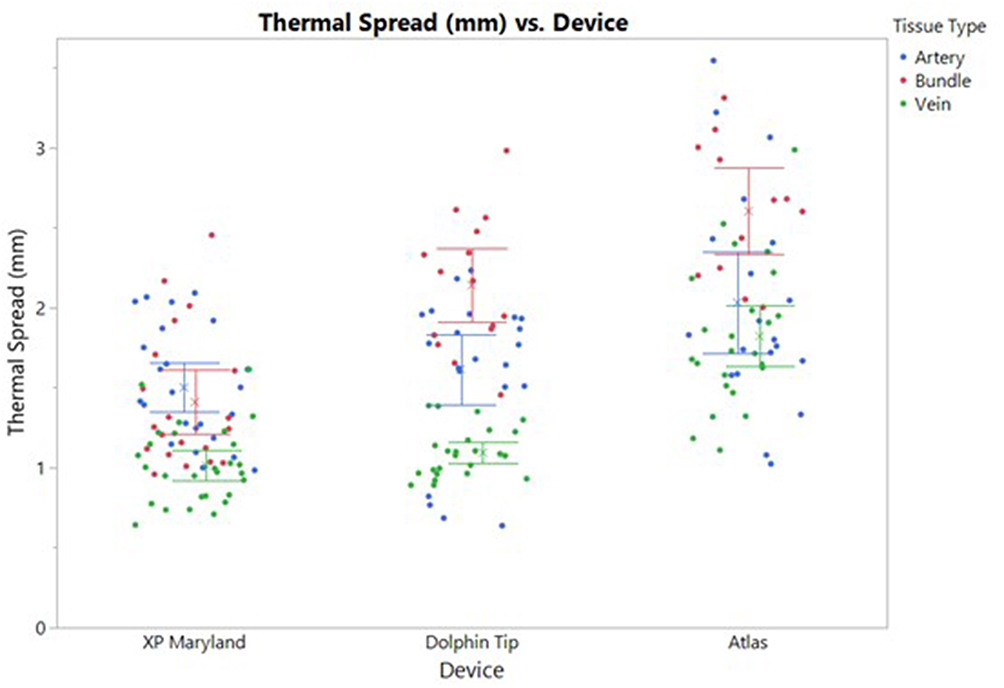 |
Figure 6 Thermal spread measurements by device with each data point color coded by general tissue type. The “x” represents the mean for each tissue type for each device, and the error bars indicate 95% confidence interval of the mean. |
 |
Figure 7 Seal times by device group with each data point color coded by tissue type. The “x” represents the mean seal times for each tissue type and the error bars indicate the 95% confidence interval around the mean. |
XP Maryland had 189 seals achieve hemostasis out of 196 total seals while Dolphin Tip had 193 seals out of 196 total seals achieve hemostasis. No statistical difference was found between the two devices (P = 0.3374). There was one sticking occurrence out of 196 seals for XP Maryland and five sticking occurrences out of 196 seals for Dolphin Tip, and this difference was not statistically significant (P = 0.2151). XP Maryland had statistically fewer incomplete cuts than Dolphin Tip (P<0.0001). It had one incomplete cut out of 196 seal and cut cycles while Dolphin Tip had 98 incomplete cuts out of 196 seal and cut cycles. Dolphin Tip’s rate of incomplete cuts in vivo was 26.7 times more than that of XP Maryland.
XP Maryland (1.29 ± 0.40 mm) had a significantly (P = 0.0010) lower mean thermal spread than Atlas (2.06 ± 0.61 mm). Atlas had 1.6 times more lateral thermal spread than XP Maryland. XP Maryland (2.71 ± 1.22s) had a shorter mean seal time but a higher standard deviation than Atlas (3.69 ± 0.84s). This difference in seal time was statistically significant (P < 0.0001), and the mean seal time of XP Maryland was 27% faster than Atlas.
Atlas had 185 seals out of 196 seals achieve hemostasis, and there was no statistical difference for hemostasis between Atlas and XP Maryland (P = 0.4702). Atlas had six sticking occurrences and five incomplete cuts out of 196 seals. No statistical difference was found between XP Maryland and Atlas for the rate of sticking (P = 0.1216) or the rate of incomplete cuts (P = 0.2151).
Discussion
Ex vivo bench and in vivo acute testing demonstrated the consistent and reliable performance of both early and recently released LigaSure instruments. Without compromising sealing performance, XP Maryland demonstrated improved performance characteristics compared to earlier devices. These included shorter seal times, reduced thermal spread, and fewer incomplete cuts and occurrences of sticking.
During ex vivo testing, all three LigaSure devices had mean burst pressures much higher than those seen in even the most severe clinical cases.35 Atlas had a statistically higher mean burst pressure than XP Maryland, but both values were above 1000 mmHg. Atlas’ higher mean value is attributed to the high burst pressure values seen on small vessels (0–3.0 mm) for Atlas (Figure 5). However, as vessel diameter increased, Atlas’ measured burst pressures decreased. This contributed to Atlas’ larger standard deviation when compared to XP Maryland. Dolphin Tip also exhibited a downward trend in burst pressure values as vessel diameter increased. XP Maryland had a more consistent burst pressure profile and uniform performance across the entire vessel size range than either Atlas or Dolphin Tip (Figure 5).
Both ex vivo and in vivo testing showed that XP Maryland had low rates of incomplete cuts and sticking, two performance characteristics that could potentially lead to reduced procedure times. The increased number of incomplete cuts observed with Dolphin Tip could lead to a need for the introduction of more instruments in the surgical field and an associated increase in procedure time. The reduced number of sticking occurrences exhibited by XP Maryland compared to Atlas may mean less tissue build-up on the device. This quality could decrease the number of times a device must be removed from the surgical field for cleaning and could reduce procedure time. Recent publications describe how shorter procedure times are associated with better postoperative outcomes. The longer the operation time, the higher the risk of surgical site infections due to longer exposure to microorganisms, reduced efficacy of perioperative antibiotics, and increased risk of breach of aseptic technique.36 The likelihood of surgical site infections has been observed to increase 5% for every 10 minutes in operation time, 13% for every 15 minutes, and 17% for every 30 minutes.37
XP Maryland had faster mean seal times ex vivo and in vivo compared to both Dolphin Tip and Atlas. Longer seal times associated with Dolphin Tip are related to performance improvements of the FT10 over its predecessor, the ForceTriad. When sealing with compatible LigaSure vessel sealers, the FT10 effectively manages energy delivery to tissue. The FT10 processes 434,000 data points per second, over 100 times more than the ForceTriad. The increased processing speed allows for increased monitoring of the electrical properties of tissue, and the vessel sealing algorithm applies the proportionate amount of energy based upon the composition and amount of tissue being sealed.38 These advantages facilitate reduced seal times.
XP Maryland had statistically less lateral thermal spread compared to Atlas (P = 0.0010) during in vivo testing. Minimizing the thermal spread to surrounding tissues without compromising seal integrity is essential for the safety and effectiveness of the device in both laparoscopic and open surgery. Excessive lateral thermal spread could lead to damage of surrounding structures.39 The reduction in lateral thermal spread for XP Maryland is associated with its much slimmer jaw profile. XP Maryland is unique in the LigaSure portfolio for its jaw design characterized by relatively long, narrow curved jaws. In addition to potentially facilitating a lower thermal spread profile, the Maryland style jaw design facilities visibility of the tip, better fine dissection, and enables skeletonization of vessels40,41 The curved jaw design follows the natural curvature of organs like the stomach and uterus, which make it useful in specialties like general, bariatric, and gynecologic surgery.6–10,17,25,42
Conclusion
The comparisons made in the ex vivo bench and in vivo acute testing showed that, as safe and effective performance continues to be the foundation of LigaSure technology, XP Maryland has some improved performance characteristics that may increase procedural efficiency and may minimize operative risks.
Funding
This work was funded by Medtronic.
Disclosure
All authors are employees of Medtronic. The authors report no other conflicts of interest in this work.
References
1. Medtronic. LigaSure 123. 2024. Available from: https://www.medtronic.com/covidien/en-gb/products/vessel-sealing/ligasure-123.html.
2. Mathomet O. LigaSure Atlas instrument. Minim Invasive Ther Allied Technol. 2002;11(5–6):237–242. doi:10.1080/13645706.2003.11873720
3. Yüney E, Höbek A, Keskin M, et al. Laparoscopic splenectomy and LigaSure. Surg Laparosc Endosc Percutan Tech. 2005;15(4):212–215. doi:10.1097/01.sle.0000174550.94671.30
4. Guaglio M, Romano F, Garancini M, et al. Is expertise in pediatric surgery necessary to perform laparoscopic splenectomy in children? An experience from a department of general surgery. Updates Surg. 2012;64(2):119–123. doi:10.1007/s13304-011-0130-3
5. Jankulovski N, Antović S, Petrusevska G, et al. Laparoscopic versus open splenectomy: a single center eleven-year experience. Acta Clin Croat. 2013;52(2):229–234.
6. Morales-Conde S, Dominguez G, Gomez JC, et al. Magnetic-assisted single-port sleeve gastrectomy. Surg Innov. 2011;20(4):NP9–NP11. doi:10.1177/1553350611427548
7. Kunisaki C, Makino H, Oshima T, et al. Application of the transorally inserted anvil (OrVil) after laparoscopy-assisted total gastrectomy. Surg Endosc. 2011;25(4):1300–1305. doi:10.1007/s00464-010-1367-5
8. Garneau PY, Abouzahr O, Garofalo F, et al. Decreasing complication rates for one-stage conversion band to laparoscopic sleeve gastrectomy: a retrospective cohort study. J Minim Access Surg. 2020;16(3):264–268.
9. Sermet M, Ozsoy MS. Effect of tranexamic acid on postoperative bleeding in sleeve gastrectomy: a randomized trial. Obes Surg. 2023;33(12):3962–3970. doi:10.1007/s11695-023-06902-x
10. Sermet M. Compression pre-stapler firing and post-ignition wait during sleeve gastrectomy: a prospective randomized trial. Sau Paulo Med J. 2023;142(3):e2023163. doi:10.1590/1516-3180.2023.0163.140823
11. Tepetes K, Zacharoulis D, Spyridakis M, Hatzitheofilou C. Liver resection using the Atlas vessel sealing system. Ann R Col Surg Eng. 2006;88(7):679–680. doi:10.1308/rcsann.2006.88.7.679
12. Tepetes K, Christodoulidis G, Spyridakis EM, Chatzitheofilou C. Tissue preserving hepatectomy by a vessel sealing device. J Surg Oncol. 2008;97(2):165–168. doi:10.1002/jso.20889
13. Panteleimonitis S, Ahmed J, Parker T, Qureshi T, Parvaiz A. Laparoscopic resection for primary and recurrent Crohn’s disease: a case series of over 100 consecutive cases. Int J Surg. 2017;47:69–76. doi:10.1016/j.ijsu.2017.09.055
14. Kössi J, Luostarinen M, Kontula I, Laato M. Laparoscopic sigmoid and rectal resection using an electrothermal bipolar vessel sealing device. J Laparoendosc Adv Surg Tech A. 2007;17(6):719–722. doi:10.1089/lap.2006.0238
15. Butskiy O, Wiseman SM. Electrothermal bipolar vessel sealing system (LigaSure) for hemostasis during thyroid surgery: a comprehensive review. Exper Rev Med Devices. 2013;10(3):389–410. doi:10.1586/erd.13.6
16. Sartori PV, Romano F, Uggeri F, et al. Energy-based hemostatic devices in laparoscopic adrenalectomy. Langenbecks Arch Surg. 2010;395(2):111–114. doi:10.1007/s00423-009-0563-z
17. Takeda A, Koike W. Clinical characteristics and laparoscopic surgical outcomes of ovarian dermoid cysts complicated by spontaneous rupture: nine cases and a literature review. J Int Med Res. 2023;51(5):1–13. doi:10.1177/03000605231171023
18. Campbell PA, Cresswell AB, Frank TG, Cuschieri A. Real-time thermography during energized vessel sealing and dissection. Surg Endosc. 2003;17(10):1640–1645. doi:10.1007/s00464-002-8781-2
19. Person B, Vivas DA, Ruiz D, Talcott M, Coad JE, Wexner SD. Comparison of four energy-based vascular sealing and cutting instruments: a porcine model. Surg Endosc. 2008;22(2):534–538. doi:10.1007/s00464-007-9619-8
20. Song C, Tang B, Campbell PA, Cuschieri A. Thermal spread and heat absorbance differences between open and laparoscopic surgeries during energized dissections by electrosurgical instruments. Surg Endosc. 2009;23(11):2480–2487. doi:10.1007/s00464-009-0421-7
21. Katsuno G, Nagakari K, Fukunaga M. Comparison of two different energy-based vascular sealing systems for the hemostasis of various types of arteries: a porcine model-evaluation of LigaSure forcetriad. J Laparoendosc Adv Surg Tech A. 2010;20(9):747–751. doi:10.1089/lap.2009.0438
22. Klar M, Haberstroh J, Timme S, et al. Comparison of a reusable with a disposable vessel-sealing device in a sheep model: efficacy and costs. Fertil Steril. 2011;95(2):795–798. doi:10.1016/j.fertnstert.2010.09.014
23. Gehrig T, Manzini G, Fonouni H, et al. Comparison of two different transection techniques in liver surgery-An experimental study in a porcine model. Langenbecks Arch Surg. 2013;398(6):909–915. doi:10.1007/s00423-013-1094-1
24. Nii A, Shimada M, Ikegami T, et al. Efficacy of vessel sealing system for major Glisson bundles and major bile ducts. J Hepatobiliary Pancreat Surg. 2008;15(5):522–527.
25. Smith JM, Elliott JA, Gillis AE, Ridgway PF. A rare case of perforated gastric duplication cyst associated with gastric diverticulum. BMJ Case Rep. 2021;14(3):e239971. doi:10.1136/bcr-2020-239971
26. Toyama Y, Yoshida S, Okui N, Kitamura H, Yanagisawa S, Yanaga K. Transumbilical single-incision laparoscopic hepatectomy using precoagulation and clipless technique in a patient with combined hepatocellular-cholangiocarcinoma: a case report. Surg Laparosc Endosc Percutan Tech. 2013;23(5):e194–e199. doi:10.1097/SLE.0b013e31828b8602
27. López-Ben S, Palacios O, Codina-Barreras A, et al. Pure laparoscopic liver resection reduces surgical site infections and hospital stay. Results of a case-matched control study in 50 patients. Langenbecks Arch Surg. 2014;399(3):307–314. doi:10.1007/s00423-014-1169-7
28. D’Hondt M, Pironet Z, Parmentier I, et al. One-stage laparoscopic parenchymal sparing liver resection for bilobar colorectal liver metastases: safety, recurrent patterns and oncologic outcomes. Surg Endosc. 2022;36(2):1018–1026. doi:10.1007/s00464-021-08366-5
29. Dionigi G, Boni L, Rovera F, Dionigi R. The use of electrothermal bipolar vessel sealing system in minimally Invasive video-assisted thyroidectomy (MIVAT). Surg Laparosc Endosc Percutan Tech. 2008;18(5):493–497.
30. Hruby GW, Marruffo FC, Durak E, et al. Evaluation of surgical energy devices for vessel sealing and peripheral energy spread in a porcine model. J Urol. 2007;178(6):2689–2693. doi:10.1016/j.juro.2007.07.121
31. Diamantis T, Gialikaris S, Kontos M, et al. Comparison of safety and efficacy of ultrasonic and bipolar thermal energy. Surg Laparosc Endosc Percutan Tech. 2008;18(4):384–390. doi:10.1097/SLE.0b013e31816f85c9
32. Mantke R, Halangk W, Habermann A, et al. Efficacy and safety of 5-mm-diameter bipolar and ultrasonic shears for cutting carotid arteries of the hybrid pig. Surg Endosc. 2011;25(2):577–585. doi:10.1007/s00464-010-1224-6
33. Milsom J, Trencheva K, Monette S, et al. Evaluation of the safety, efficacy, and versatility of a new surgical energy device (Thunderbeat) in comparison with Harmonic ACE, LigaSure V, and EnSeal devices in a porcine model. J Laparoendosc Adv Surg Tech A. 2012;22(4):378–386.
34. Pappas J, Roweton S, Kurtenbach J, Dunne JB. Comprehensive analysis of performance data for energized vessel sealing devices. J Test Eval. 2016;45(5):1553–1569. doi:10.1520/JTE20160216
35. American Heart Association. When to call 911 about high blood pressure. 2024. Available from: https://www.heart.org/en/health-topics/high-blood-pressure/understanding-blood-pressurereadings/hypertensive-crisis-when-you-should-call-911-for-high-blood-pressure.
36. Olasehinde O, Owojuyigbe A, Adeyemo A, et al. Use of energy device in general surgical operations: impact on peri-operative outcomes. BMC Surg. 2022;22(1):90. doi:10.1186/s12893-022-01540-z
37. Cheng H, Chen BP, Soleas IM, et al. Prolonged operative duration increases risk of surgical site infections: a systematic review. Surg Infect. 2017;18(6):722–735. doi:10.1089/sur.2017.089
38. Medtronic. Valleylab FT10 energy platform. 2024. Available from: https://www.medtronic.com/covidien/en-us/products/electrosurgical-hardware/valleylab-ft10-energy-platform.html.
39. Družijanić N, Pogorelić Z, Perko Z, Mrklić I, Tomić S. Comparison of lateral thermal damage of the human peritoneum using monopolar diathermy, Harmonic scalpel and LigaSure. Can J Surg. 2012;55(5):317–321.
40. Medtronic. LigaSure XP Maryland Jaw Sealer/Divider with nano-coating. 2024. Available from: https://www.medtronic.com/covidien/en-us/products/vessel-sealing/ligasure-xp-maryland-jaw-sealer-divider-nano-coating.html.
41. Park AE, Mastrangelo MJ, Gandsas A, Chu U, Quick NE. Laparoscopic dissecting instruments. Semin Laparosc Surg. 2001;8(1):42–52. doi:10.1053/slas.2001.23677
42. Medtronic. LigaSure maryland jaw open and laparoscopic sealer/divider with nanocoating. 2024. Available from: https://www.medtronic.com/covidien/en-us/products/vessel-sealing/ligasure-maryland-jaw-sealer-divider.html.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.