Back to Journals » International Medical Case Reports Journal » Volume 18
Neuromyelitis Optica-Associated Acute Intermediate Uveitis
Authors Balakrishnan P ![]() , Luckett JP, Vaphiades M
, Luckett JP, Vaphiades M
Received 27 July 2025
Accepted for publication 14 November 2025
Published 26 November 2025 Volume 2025:18 Pages 1501—1505
DOI https://doi.org/10.2147/IMCRJ.S555009
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Giuseppe Giannaccare
Poojitha Balakrishnan,1 John Paul Luckett,1,2 Michael Vaphiades1
1Department of Ophthalmology and Visual Sciences, University of Alabama at Birmingham, Birmingham, AL, USA; 2Alabama Ophthalmology Associates, Birmingham, AL, USA
Correspondence: Poojitha Balakrishnan, Department of Ophthalmology and Visual Sciences, University of Alabama at Birmingham, 1720 University Boulevard Suite 302, Birmingham, AL, 35233, USA, Email [email protected]
Abstract: Optic neuritis is one of the diagnostic criteria for Neuromyelitis Optica Spectrum Disorder (NMOSD). However, the presentation of other ophthalmic manifestations in a patient with NMOSD is less common. A case of intermediate uveitis in a patient with anti-aquaporin-4 antibody (AQP4) positivity is detailed in this report. We present here a case of a 17-year-old Southeast Asian woman who presented with segmental fullness of the optic disc margin, small hypopigmented lesion along inferior temporal arcade, trace vitreous cells and inferior snowballs consistent with unilateral intermediate uveitis. The patient subsequently presented with an episode of optic neuritis of the same eye, resulting in diagnostic workup conforming NMOSD including neuroimaging and AQP4 antibody. Our case report highlights that NMOSD should be considered in the differential for intermediate uveitis. Furthermore, the sequence of both intermediate uveitis and optic neuritis in our patient demonstrates the importance of continued ophthalmic exams in patients with NMOSD.
Keywords: neuromyelitis optica spectrum disorder, intermediate uveitis, optic neuritis, aquaporin-4 antibody
Introduction
Neuromyelitis Optica Spectrum Disorder (NMOSD) is a rare demyelinating disease of the central nervous system that has a classic ophthalmic association with bilateral optic neuritis.1,2 The diagnostic criteria for NMOSD differ based on the presence of anti–aquaporin-4 antibody (AQP4). In the presence of AQP4, NMOSD can be diagnosed with one of the following: optic neuritis, longitudinally extensive transverse myelitis, area postrema syndrome, and acute brainstem syndrome. While optic neuritis is a component of the NMOSD diagnostic criteria, other ophthalmic manifestations can include oscillopsia, nystagmus, oculomotor nerve palsy, optic perineuritis, posterior scleritis/uveitis, and retinal vasculitis.3–6
Intermediate uveitis has a well-established association with multiple sclerosis (MS) with prevalence estimates of approximately 1%.7,8 Recent literature has highlighted uveitic manifestations preceding the more classic presentation of demyelinating optic neuritis in other demyelinating conditions such as myelin oligodendrocyte glycoprotein associated disease (MOGAD) and acute disseminated encephalomyelitis (ADEM).3,5,9–11 However, the association between intermediate uveitis and NMO is rarely noted.3,12 We report a case of acute unilateral intermediate uveitis preceding NMOSD optic neuritis in the same eye.
Case Presentation
A 17-year-old Southeast Asian woman presented to eye emergency department with a one-month history of superior scotoma and floaters of the right eye (OD). There was no past ocular or medical history and no family history. Visual acuity, color vision using Ishihara color plates, confrontational visual fields, pupillary reaction, extraocular muscle movements, intraocular pressure and anterior segment examinations were normal in both eyes (OU). Fundoscopic exam was remarkable for superonasal fullness of the optic disc margin, small hypopigmented lesion along inferior temporal arcade, trace vitreous cells and inferior snowballs OD (Figure 1). The left fundus appeared normal. Fundus autofluorescence showed a focal white area, consistent with edema or a resolving cotton-wool spot OD (Figure 2). Humphrey visual field, fluorescein angiography, indocyanine green angiography, and optical coherence tomography of the macula were normal OU. Initial workup including comprehensive metabolic panel, complete blood count, infectious serology (HIV, Rocky Mountain Spotted Fever, Treponema, Bartonella, West Nile, Toxoplasma, QuantiFERON-TB), and chest x-ray were negative.
 |
Figure 1 Fundus imaging of right eye. Fundus photos of right eye with hypopigmented lesion along inferior temporal arcade (A) and inferior snowballs (black arrows) (B). |
 |
Figure 2 Fundus autofluorescence imaging of right eye. Fundus autofluorescence of right eye re-demonstrating the hypopigmented lesion (white arrow) with hypo-autofluorescence. |
The patient returned 6 weeks later with worsening vision OD (20/30) and pain with extraocular movements. The exam was otherwise unchanged. The patient was prescribed topical prednisolone OD for intermediate uveitis OD. The patient returned 3 days later with count finger visual acuity OD, a right relative afferent pupillary defect and circumferential blurred disc margins OD consistent with an optic neuropathy OD. The remainder of cranial nerve and peripheral neurological exam was within normal limits. Fat suppressed contrast-enhanced T1 weighted magnetic resonance imaging (MRI) of brain and orbits demonstrated right optic nerve enhancement (Figure 3) and white matter lesions in the right pericallosal region, left posterior frontal lobe and juxtacortical region on FLAIR sequences (Figure 3). The patient met the diagnostic criteria for NMOSD with optic neuritis, positive AQP4 and negative workup for alternative diagnoses. The patient was prescribed intravenous methylprednisolone with an oral prednisone taper. Patient was then transitioned to azathioprine. At the follow-up examination after 3 months, patient had resolution of the optic neuritis and vitreous cell/snowballs without change in acuity (Figure 4).
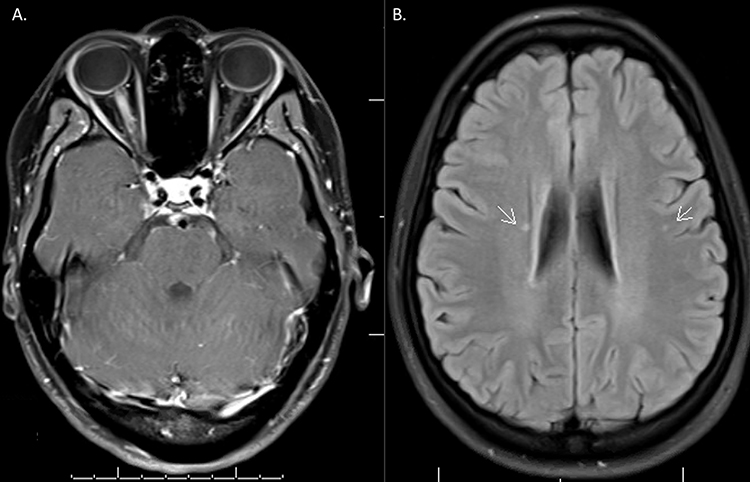 |
Figure 3 Neuroimaging with evidence of NMOSD. Fat suppressed contrast-enhanced T1 weighted magnetic resonance imaging (MRI) of brain and orbits demonstrated right optic nerve enhancement (A) and white matter lesions (white arrows) in the right pericallosal region, left posterior frontal lobe and juxtacortical region on FLAIR sequences (B). |
 |
Figure 4 Fundus imaging of right eye. Fundus photos of right eye with resolving hypopigmented lesion along inferior temporal arcade without macular or optic nerve edema. |
Written informed consent including publication of case details and images was obtained from the patient and from the legal medical decision maker (parent). The publication was exempt from institutional review.
Discussion
NMOSD is rare with a prevalence of approximately 0.4–4.0 per 100,000 and disproportionately affects younger White females with concomitant autoimmune conditions.1,6,13 Optic neuritis is a common presenting symptom in patients with NMOSD, estimated to be as high as half of patients and commonly bilateral.1,14,15 While the acute management includes high dose of systemic corticosteroids and/or plasmapheresis, long-term treatment incorporates immunomodulatory therapy such as azathioprine or more targeted therapies such as eculizumab.1,14–16
The discovery of AQP4 has highlighted the possible underlying pathophysiology of not only optic neuritis but also other rare ocular manifestations noted in patients with NMOSD.6,13,17 AQP4 is an integral cell membrane protein, which regulates water homeostasis, is found on astrocytes and expressed within optic nerves, brainstem, and spinal cord. It is also found in the iris and pars plicata epithelial cells and may have a role in aqueous humor production.1,9,17 Moreover, experimental rat models using intraperitoneal injection of aquaporin-specific T-cells with NMO-IgG demonstrated a temporal association with T-cell infiltrates in the retina and ciliary body.17
Intermediate uveitis is defined as intraocular inflammation primarily of the vitreous and peripheral retina, including pars planitis and posterior cyclitis.18,19 MS is strongly associated with intermediate uveitis. Both MS and uveitis have a genetic association with HLA-DRB1 and IL-2RA suggesting a common underlying mechanism.7,8 In addition to vitreous inflammation, MS has also been noted to be associated with retinal vasculitis.20,21 There have also been case reports of anterior/intermediate uveitis in patients with MOGAD9,10 and ADEM.11
Our case is novel in that it illustrates that intermediate uveitis is a rare presenting symptom in NMOSD. Uveitis preceded the presentation of NMOSD by approximately 2 years.3 The most prevalent subtype of uveitis is bilateral anterior uveitis, although posterior uveitis/retinal vasculitis have also been reported.6,11 While the current literature is not definitive on the association between uveitis and NMO, the high relative risk noted is highly suggestive.3 In our patient, intermediate uveitis preceded optic neuritis by only 6 weeks. There were no atypical neurological signs noted at presentation or on follow-up examinations. In addition, both intermediate uveitis and optic neuritis was unilateral highlighting the low threshold to consider NMOSD as a differential diagnosis in patients with intermediate uveitis. Unlike anterior uveitis, there is a high proportion of patients with systemic conditions, such as Behcet’s, sarcoidosis and MS.8,19 Our case emphasizes that NMOSD should also be in the differential for patients presenting with intermediate uveitis, especially in the setting of no known systemic conditions.
It remains possible that the preceding episode of intermediate uveitis in our patient was idiopathic and not related to NMOSD and later development of AQP4-positive optic neuritis in the same eye. Yet, the uveal expression of AQP4 channels highlights a possible underlying mechanism of intermediate uveitis in NMOSD. More research can help elucidate the association of intermediate uveitis in patients with NMOSD.
Conclusion
This case highlights that intermediate uveitis may be the initial presentation in patients with NMOSD. While rare, the uveitic presentations may in fact precede the more prevalent ophthalmic manifestation of optic neuritis. There is a strong systemic association previously noted in patients with intermediate uveitis. Therefore, there should be a high index of suspicion to include NMOSD in the differential in patients presenting with intermediate uveitis without known predisposing conditions. The prevalence of NMOSD-associated morbidity calls to attention the need for prompt diagnosis and treatment.
Abbreviations
ADEM, acute disseminated encephalomyelitis; AQP4, aquaporin-4; HIV, human immunodeficiency virus; MRI, magnetic resonance imaging; MOGAD, myelin oligodendrocyte glycoprotein associated disease; MS, multiple sclerosis; NMOSD, neuromyelitis optica spectrum disorder; OD, right eye; OU both eyes.
Acknowledgement
This manuscript was supported by Vision Science Research Center core grant P30 EY003039.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wingerchuk DM, Lennon VA, Lucchinetti CF, et al. The spectrum of neuromyelitis optica. Lancet Neurol. 2007;6(9):805–815. doi:10.1016/S1474-4422(07)70216-8
2. Wingerchuk DM, Banwell B, Bennett JL, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology. 2015;85(2):177–189. doi:10.1212/WNL.0000000000001729
3. Carey AR, Arevalo JF. Neuromyelitis optica spectrum disorder and uveitis. Ocul Immunol Inflamm. 2022;30(7–8):1747–1750. doi:10.1080/09273948.2021.1942499
4. Green AJ, Cree BA. Distinctive retinal nerve fibre layer and vascular changes in neuromyelitis optica following optic neuritis. J Neurol Neurosurg Psychiatry. 2009;80(9):1002–1005. doi:10.1136/jnnp.2008.166207
5. Ramanathan S, Fraser C, Curnow SR, et al. Uveitis and optic perineuritis in the context of myelin oligodendrocyte glycoprotein antibody seropositivity. Eur J Neurol. 2019;26(8):1137–e75. doi:10.1111/ene.13932
6. Jarius S, Kleiter I, Ruprecht K, et al. MOG-IgG in NMO and related disorders: a multicenter study of 50 patients. Part 3: brainstem involvement-frequency, presentation and outcome. J Neuroinflamm. 2016;13(1):281. doi:10.1186/s12974-016-0719-z
7. Casselman P, Cassiman C, Casteels I, et al. Insights into multiple sclerosis‐associated uveitis: a scoping review. Acta ophthalmologica. 2021;99(6):592–603. doi:10.1111/aos.14697
8. Ness T, Boehringer D, Heinzelmann S. Intermediate uveitis: pattern of etiology, complications, treatment and outcome in a tertiary academic center. Orphanet J Rare Dis. 2017;12(1):81. doi:10.1186/s13023-017-0638-9
9. Vosoughi AR, Ling J, Tam KT, et al. Ophthalmic manifestations of myelin oligodendrocyte glycoprotein-IgG-associated disorder other than optic neuritis: a systematic review. Br J Ophthalmol. 2021;105(11):1591–1598. doi:10.1136/bjophthalmol-2020-317267
10. Jeyakumar N, Waller S, Mahant N, et al. A case of CSF anti-MOG antibody-positive papillitis with intermediate uveitis in the setting of acute neurosyphilis. Neuroimmunol Rep. 2021;1:100033. doi:10.1016/j.nerep.2021.100033
11. Tan PY, Furness J, Sohal AS, et al. A case of intermediate uveitis as a precursor to acute disseminated encephalomyelitis (ADEM) in a teenager. Eye. 2014;28(5):625–627. doi:10.1038/eye.2014.30
12. Braithwaite T, Subramanian A, Petzold A, et al. Trends in optic neuritis incidence and prevalence in the UK and association with systemic and neurologic disease. JAMA Neurol. 2020;77(12):1514–1523. doi:10.1001/jamaneurol.2020.3502
13. Jarius S, Paul F, Franciotta D, et al. Mechanisms of disease: aquaporin-4 antibodies in neuromyelitis optica. Nat Clin Pract Neurol. 2008;4(4):202–214. doi:10.1038/ncpneuro0764
14. Papais-Alvarenga RM, Carellos SC, Alvarenga MP, Holander C, Bichara RP, Thuler LC. Clinical course of optic neuritis in patients with relapsing neuromyelitis optica. Arch Ophthalmol. 2008;126(1):12–16. doi:10.1001/archophthalmol.2007.26
15. Wingerchuk DM, Hogancamp WF, O’Brien PC, et al. The clinical course of neuromyelitis optica (Devic’s syndrome). Neurology. 1999;53(5):1107. doi:10.1212/WNL.53.5.1107
16. Papadopoulos MC, Bennett JL, Verkman AS. Treatment of neuromyelitis optica: state-of-the-art and emerging therapies. Nat Rev Neurol. 2014;10(9):493–506. doi:10.1038/nrneurol.2014.141
17. Zeka B, Hastermann M, Kaufmann N, et al. Aquaporin 4-specific T cells and NMO-IgG cause primary retinal damage in experimental NMO/SD. Acta Neuropathol Commun. 2016;4(1):82. doi:10.1186/s40478-016-0355-y
18. Jabs D, Nussenblatt R; Rosenbaum JTStandardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data: results of the First International Workshop. Am J Ophthalmol. 2005;140(3):509–516.
19. Teo AYT, Betzler BK, Hua KLQ, et al. Intermediate uveitis: a review. Ocul Immunol Inflamm. 2023;31(5):1041–1060. doi:10.1080/09273948.2022.2070503
20. Nawar A. Retinal-vasoproliferative tumor on top of intermediate uveitis as a sole ocular manifestation of multiple sclerosis. Ophthalmol Case Rep. 2020;4(1):20–22.
21. Paović J, Paović P, Vukosavljević M. Clinical and immunological features of retinal vasculitis in systemic diseases. Vojnosanitetski pregled. 2009;66(12):961–965. doi:10.2298/VSP0912961P
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.