Back to Journals » International Medical Case Reports Journal » Volume 18
Neurological Sequelae After Sacral Radiofrequency Ablation: A Case of Acute Cauda Equina Syndrome
Authors Elimam N ![]() , Elimam E
, Elimam E ![]() , Dovbonos T
, Dovbonos T
Received 26 August 2025
Accepted for publication 19 November 2025
Published 26 November 2025 Volume 2025:18 Pages 1489—1493
DOI https://doi.org/10.2147/IMCRJ.S541369
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tanvi Dhere
Noon Elimam,1 Eman Elimam,2 Tetiana Dovbonos1,3
1Department of Neurology, Bogomolets National Medical University, Kyiv, Ukraine; 2Department of Neurology, Tbilisi State Medical University, Tbilisi, Georgia; 3Department of Neurology, Kyiv City Hospital Number 4, Kyiv, Ukraine
Correspondence: Noon Elimam, Email [email protected]
Abstract: Radiofrequency ablation (RFA) is a minimally invasive technique that uses high-frequency electrical currents to generate heat, causing controlled destruction of targeted tissues through ionic agitation. RFA-associated neuropathy is a rare but recognized complication. We present a case of cauda equina syndrome and sensorimotor neuropathy following RFA of a sacral bone metastasis. Electromyography confirmed peripheral neuropathy, particularly affecting the peroneal nerve, and MRI revealed degenerative changes and a pelvic mass near the sacrum. The patient was treated with corticosteroids and neurotrophic supplementation and subsequently discharged for oncology follow-up. This case highlights the potential for RFA-induced neuropathy, emphasizing the need for careful procedural planning, post-treatment monitoring, and further research on the role of corticosteroids in mitigating neurological complications. This finding also raises questions about the role of corticosteroids in managing such complications, emphasizing the need for personalized care and further research to improve patient outcomes.
Plain Language Summary: Radiofrequency ablation (RFA) uses heat to destroy tumors and relieve pain and is generally safe, but it can rarely cause nerve damage. We report a 52-year-old woman with endometrial cancer metastasized to the sacrum who developed leg weakness, numbness, pain, and bladder and bowel difficulties after RFA. Tests confirmed peripheral nerve injury, mainly affecting the peroneal nerve.
She was treated with pain medications, nerve-supporting vitamins, and corticosteroids, with gradual improvement before returning to oncology follow-up. This case highlights that RFA, while effective for painful bone metastases, can cause severe nerve complications. The role of corticosteroids remains uncertain, emphasizing the need for careful planning, monitoring, and further research to guide individualized treatment.
Keywords: radiofrequency ablation, metastasis, neuropathy, cauda equina, corticosteroids
Key Clinical Message
Radiofrequency ablation (RFA) for sacral bone metastases can rarely cause severe peripheral nerve injury, including motor, sensory, and autonomic deficits. Early recognition is critical. Corticosteroids may provide symptomatic relief, but evidence is inconsistent. Careful procedural planning and post-procedure monitoring near major nerves are essential. Further studies are needed to define the role of steroids in RFA-related neuropathy.
Introduction
Radiofrequency ablation (RFA) is a minimally invasive technique that uses high-frequency electrical currents to generate heat, causing controlled destruction of targeted tissues through ionic agitation, this localized heating raises tissue temperature above 60°C, inducing coagulation necrosis by denaturing proteins and destroying tumor cells.1 RFA is increasingly accepted as a treatment for various solid tumors, including primary and metastatic liver cancer, renal cell carcinoma, lung cancer, and bone metastases.2,3In bone metastases, RFA provides effective pain palliation by destroying tumor cells and disrupting sensory nerve fibers in the periosteum and surrounding microenvironment that contribute to nociception. This often results in rapid and durable relief from metastatic bone pain, improving patient quality of life. Additionally, image-guided RFA enables precise targeting of lesions with minimal damage to surrounding healthy tissue, making it generally safe and well-tolerated.3,4,5
Despite these benefits, complications from RFA can occur. Among these, neuropathic pain or neuropathy, though rare, is clinically significant. Neurological injury may result from direct thermal damage to adjacent nerves or neural structures, mechanical trauma from needle placement, or secondary effects such as local edema or hematoma causing nerve compression. The risk of neurological sequelae is influenced by factors including lesion location, procedure duration, and proximity of critical nerves. Timely recognition and management are essential to prevent permanent deficits6. Cauda equina syndrome (CES) is a serious neurological condition caused by compression or injury of the sacral nerve roots. It is characterized by lower-limb weakness, sensory deficits in the saddle area, and autonomic dysfunction including bowel and bladder disturbances.7 CES can result from various etiologies, including traumatic injury, tumors, infection, or iatrogenic causes such as surgical procedures or radiofrequency ablation in anatomically sensitive regions. Recognition of CES is critical because delayed diagnosis or treatment may lead to irreversible neurological deficits.
This report describes a patient who developed CES and sensorimotor peripheral neuropathy following RFA for sacral bone metastasis secondary to endometrial cancer. This case illustrates the potential for serious neurological complications after RFA in anatomically sensitive areas and highlights the importance of careful procedural planning, monitoring, and consideration of adjunct therapies to mitigate nerve injury.
Case Presentation
A 52-year-old woman was admitted to the neurology department two months after undergoing radiofrequency ablation of a sacral bone metastasis with progressive lower-limb weakness, sensory disturbances, and bladder and bowel dysfunction. On examination, the patient reported numbness and pain over the lateral dorsal surface of the foot, reduced lower-limb reflexes, shooting pain radiating from the perineal region, and a sensation of tightness in the buttocks and lower legs, limiting mobility. These findings were consistent with lumbosacral involvement (L5–S2), suggestive of cauda equina syndrome secondary to neural injury following RFA. According to the American Spinal Injury Association (ASIA) Impairment Scale, the patient demonstrated partial motor preservation below the neurological level, with weakness in both lower limbs, diminished reflexes, and sensory loss in perineal and dorsal foot dermatomes. Bladder and bowel dysfunction indicated sacral segment involvement (S2–S5). Given these findings, the presentation was consistent with ASIA Grade C (motor incomplete), reflecting partial preservation of motor and sensory function below the level of injury, with more than half of the key muscles below that level exhibiting a muscle strength grade of less than 3/5.
Her medical and surgical history included uterine cancer (T2N0M1), which was diagnosed two years prior and managed with a radical hysterectomy. One year after surgery, the patient began experiencing pain in the sacral region, left lower limb, and right buttock, radiating to the external genitalia. Imaging revealed metastasis in the sacral bone (S1), and RFA was initiated three months later to manage the local lesion. Before undergoing RFA, the patient had no neurological symptoms; however, these symptoms developed acutely following the initiation of the procedure. They were initially mild but progressively worsened over the subsequent two months, leading to her admission.
A complete blood count, basic metabolic panel, renal and liver function tests, cerebrospinal fluid analysis, vitamin B6, vitamin B12, folic acid, thyroid and parathyroid hormone levels, and viral serologies (hepatitis B, hepatitis C, HIV) were all within normal limits. Spinal MRI and CT revealed degenerative changes and the formation of a mass in the pelvic region near the sacrum and in the thoracic spine, with some signs of lymph node involvement but without evidence of nerve root compression on imaging. Importantly, the patient did not exhibit any neurological symptoms prior to the RFA; her symptoms appeared acutely after the procedure. This temporal relationship strongly supports our conclusion that the RFA itself was the likely cause of the neurological deficits, rather than the pre-existing masses.
Serological evaluations for immunological markers of disease, including antinuclear antibodies (ANA), anti-double-stranded DNA (anti-dsDNA), anti-neutrophil cytoplasmic antibodies (anti-PR3 and anti-MPO), complement components C3 and C4, anti-Ro, anti-La, beta-2 glycoprotein, anti-thyroid peroxidase (anti-TPO), and antithyroglobulin antibodies, were all within normal limits. Antiganglioside antibodies (IgM and IgG), including GM1, GM2, GM3, GD1a, GD1b, GD2, GD3, GT1a, GT1b, and GQ1b, were negative. Additionally, the rheumatoid factor test was negative.
Electromyography (EMG) revealed evidence of peripheral neuropathy, affecting both motor and sensory components. The common peroneal nerve demonstrated the most significant reduction in conduction velocity at 30.8 m/s. Similarly, the tibialis anterior nerve showed a reduced conduction velocity of 33.6 m/s, further confirming notable dysfunction (Figure 1).
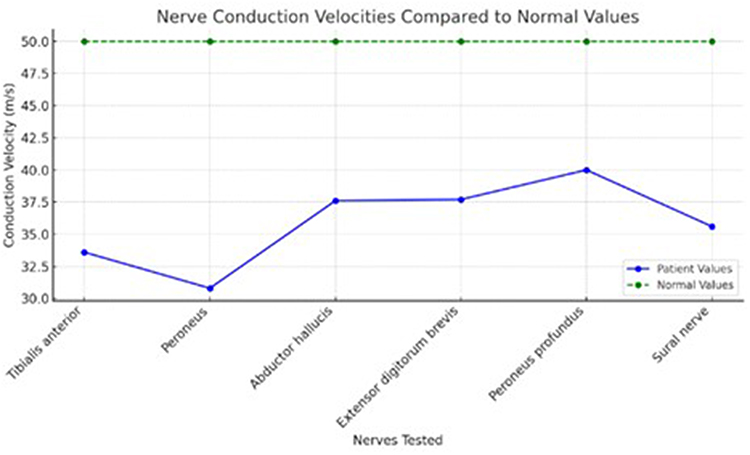 |
Figure 1 Comparison of patient’s nerve conduction velocities to normal values suggesting sensorimotor peripheral neuropathy. |
The treatment plan was initiated with dexamethasone (8 mg once daily for 10 days), after which the patient showed significant improvement in motor and sensory symptoms following the first dose. Subsequently, adjunct therapies were introduced, including alpha-lipoic acid (600 mg once daily for 1 month), Keltican (uridine monophosphate, vitamin B12, folic acid; 5 mg once daily for 1 month), meloxicam (15 mg in the morning for 10 days), dexketoprofen for severe pain management, Mediatron (20 mg twice daily for 20 days), pregabalin (150 mg twice daily), and escitalopram (10 mg in the morning for 6 months). The pain symptoms and motor function continued to improve progressively, and the patient was referred for oncology follow-up. At a 12-month follow-up, the patient demonstrated complete resolution of the neurological deficit with no residual motor or sensory impairment.
Discussion
Radiofrequency ablation (RFA) is a widely used therapeutic modality for managing various medical conditions, including both benign and malignant tumors, chronic venous insufficiency and chronic back and neck pain.3 The fundamental mechanism involves the use of radiofrequency energy to induce ionic agitation within tissues, leading to friction and localized heat generation. Once a critical temperature threshold is reached, the cellular water evaporates, and the heat denatures the cellular proteins, resulting in cell death and achieving the desired therapeutic effect.8
Despite its utility, complications occur in up to 17% of cases, with neurological injury being among the rarest but most disabling outcomes. The incidence and nature of complications depend on factors such as the type of tissue being ablated, the size of the lesion, the duration of the procedure, and the proximity of vital anatomical structures. Potential complications include bleeding, infection, and damage to nearby nerves, blood vessels, bile ducts, the diaphragm, or adjacent organs.9 Among these, neurological complications associated with RFA have rarely been reported in the literature, but when they occur, they can significantly impact patient outcomes.
In our patient, RFA for sacral metastasis resulted in cauda equina syndrome with mixed axonal–demyelinating neuropathy, most pronounced in the peroneal nerve. Although adverse events following RFA for skeletal metastases are relatively uncommon,4 this case highlights a significant neurological complication. Similar complications have been documented in various clinical settings. For example, phrenic nerve injury has been reported following RFA near the pulmonary vein orifice during atrial fibrillation treatment, trigeminal nerve injury has occurred after RFA for trigeminal neuralgia, and rare cases of peripheral nerve damage, including injuries to the common peroneal, sural, or saphenous nerves, have also been reported.10,11 These cases demonstrate the potential for RFA to cause unintentional damage to critical nearby nerves, resulting in severe functional impairments.
Although the mechanisms underlying RFA-associated neurological injury are not fully understood, animal studies suggest that there may be a correlation between the temperature used during RFA and the development of neuropathological damage.8 Higher temperatures during RFA can lead to thermal injury, which may cause inflammation, nerve damage, and subsequent neurological complications. Postprocedural nerve damage can also arise from local compression due to surrounding edema or hematomas, further exacerbating the risk of neurological injury.12 These findings highlight the importance of carefully selecting procedural parameters, such as temperature and duration, to minimize thermal and mechanical trauma to neural structures.
In addition to direct thermal injury and compression-related damage, other hypotheses have been proposed to explain the development of neuropathy following RFA.4 For example, in cases where RFA is used to treat skeletal lesions, the rapid resolution of pain may predispose patients to overuse syndromes. When muscles have become deconditioned due to prolonged disuse, a sudden increase in physical activity after pain relief can lead to the release of cytokines and reactive oxygen species into the surrounding tissues. This inflammatory response can result in local leukocytosis, contributing to nerve damage and amplifying nociceptive processes.13
This inflammatory response adds to the complexity of post-RFA neuropathy and highlights the challenges in managing it effectively. Since nerve damage can result from multiple factors, treatments need to target both inflammation and nerve repair. Corticosteroids, known for their anti-inflammatory and regenerative properties, may offer potential in managing these complications.14 However, their efficacy in treating post-RFA neuropathy remains an area of active investigation, with studies yielding mixed results.
A randomized controlled pilot study by Shustorovich et al demonstrated a statistically significant reduction in post-neurotomy pain when dexamethasone was administered post-procedurally, suggesting a potential benefit in pain management.15 However, other studies have indicated that adding steroids to post-procedural RFA did not consistently provide added benefits in reducing the incidence of post-neurotomy neuritis. Williams et al reported no significant difference in pain scores or neuritis rates when comparing cervical and lumbar RFA with or without steroid use, concluding that the anatomical location alone does not appear to modify the efficacy of corticosteroids,16 In line with this, Singh et al evaluated lumbar facet RFN and found that post-procedural steroid administration did not reduce the incidence of neuritis, reinforcing that procedural context, such as facet joint neurotomy versus RFA for sacral metastasis, may underlie outcome variability rather than anatomical site per se,17 these findings suggest that while steroids may mitigate inflammation in some RFA contexts, their effectiveness likely depends on factors beyond anatomy, such as underlying pathology, lesion characteristics, and procedural technique.
Consent
Written informed consent was obtained from the patient for the publication of case details and accompanying images. Institutional approval was not required for the publication of the case reports.
Acknowledgments
We would like to thank the patient and her family for their support of this work and acknowledge the contribution of consultant colleagues and other clinical specialists at our hospital, in the ongoing care of the patient described in this report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Goldberg SN, Gazelle GS, Halpern EF, et al. Radiofrequency tissue ablation: importance of local temperature along the electrode tip exposure in determining lesion shape and size. Acad Radiol. 1996;3(3):212–218. doi:10.1016/s1076-6332(96)80443-0
2. Meloni MF, Andreano A, Laeseke PF, et al. Breast cancer liver metastases: US-guided percutaneous radiofrequency ablation--intermediate and long-term survival rates. Radiology. 2009;253(3):861–869. doi:10.1148/radiol.2533081968
3. Friedman M, Mikityansky I, Kam A, et al. Radiofrequency ablation of cancer. Cardiovasc Intervent Radiol. 2004;27(5). doi:10.1007/s00270-004-0062-0
4. Glaiberman CB, Brown DB. Reversible neuropathy caused by overuse following radiofrequency ablation of metastatic pelvic lesions. J Vascular Intervent Radiol. 2004;15(11):1307–1310. doi:10.1097/01.RVI.0000136827.08722.C5
5. Kwon H-J, Kim PN, Byun JH, et al. Various complications of percutaneous radiofrequency ablation for hepatic tumors: radiologic findings and technical tips. Acta Radiol. 2014;55(9):1082–1092. doi:10.1177/0284185113513893
6. Racz GB, Ruiz Lopez R. Radiofrequency procedures. Pain Prac. 2006;6(1):46–50. doi:10.1111/j.1533-2500.2006.00058.x
7. Gitelman A, Hishmeh S, Morelli BN, et al. Cauda equina syndrome: a comprehensive review. Am J Orthop. 2008;37(11):556–562.
8. Dong Y, Chen Y, Yao B, et al. Neuropathologic damage induced by radiofrequency ablation at different temperatures. Clinics. 2022;77:100033. doi:10.1016/j.clinsp.2022.100033
9. Lahat E, Eshkenazy R, Zendel A, et al. Complications after percutaneous ablation of liver tumors: a systematic review. Hepatobiliary Surg Nutr. 2014;3.
10. Adragão PP, Cavaco DM, Santos KR, et al. Percutaneous ablation of atrial fibrillation: assessment of outcomes at 1-year follow-up. Rev Port Cardiol. 2003;22(11):1301–1308.
11. Ricci S. Ultrasound observation of the sciatic nerve and its branches at the popliteal fossa: always visible, never seen. Euro J Vascular Endovasc Surg. 2005;30(6):659–663. doi:10.1016/j.ejvs.2005.06.004
12. Ricci S, Georgiev M, Jawien A, et al. Sciatic nerve varices. Euro J Vascular Endovasc Surg. 2005;29(1):83–87. doi:10.1016/j.ejvs.2004.09.009
13. Kayashima S, Ohno H, Fujioka T, et al. Leucocytosis as a marker of organ damage induced by chronic strenuous physical exercise. Eur J Appl Physiol Occup Physiol. 1995;70(5):413–420. doi:10.1007/BF00618492
14. Wordliczek J, Szczepanik AM, Banach M, et al. The effect of pentoxifiline on post-injury hyperalgesia in rats and postoperative pain in patients. Life Sci. 2000;66(12):1155–1164. doi:10.1016/s0024-3205(00)00419-7
15. Shustorovich A, AlFarra T, Arel AT, et al. Dexamethasone effectively reduces the incidence of post-neurotomy neuropathic pain: a randomized controlled pilot study. Pain Physician. 2021;24(8):517–524.
16. Williams MR, Philip A, Sheen S, et al. Non-inferiority study assessing the utility of postcervical and lumbar radiofrequency ablation steroid use. Reg Anesth Pain Med. 2024; rapm–2024–105501. doi:10.1136/rapm-2024-105501
17. Singh JR, Miccio VF, Modi DJ, et al. The impact of local steroid administration on the incidence of neuritis following lumbar facet radiofrequency neurotomy. Pain Physician. 2019;22(1):69–74. doi:10.36076/ppj/2019.22.69
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.