Back to Journals » Drug Design, Development and Therapy » Volume 20
Neurohormonal-Immune Dysregulation in Rosacea: Emerging Perspectives from the Skin-Gut-Brain Axis
Authors Shi L ![]() , Li S, Yao X, Zhang Z, Dong Q
, Li S, Yao X, Zhang Z, Dong Q ![]() , Zhang H, Wang X, Bai J, Han H, Fu X, Zheng K, Liang L
, Zhang H, Wang X, Bai J, Han H, Fu X, Zheng K, Liang L
Received 12 March 2026
Accepted for publication 16 May 2026
Published 16 June 2026 Volume 2026:20 608151
DOI https://doi.org/10.2147/DDDT.S608151
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Anastasios Lymperopoulos
Lei Shi,1 Siying Li,1 Xiaodong Yao,1 Zijian Zhang,2 Qinyi Dong,2 Han Zhang,1 Xinman Wang,1 Jiahao Bai,1 Huiyan Han,1 Xiaoyi Fu,2 Kaili Zheng,1 Lili Liang1,2
1The Cosmetic and Plastic Surgery, Department of Shanxi Provincial People’ s Hospital, Shanxi Medical University, Taiyuan, 030012, People’s Republic of China; 2The Third Clinical College, Shanxi University of Chinese Medicine, Taiyuan, People’s Republic of China
Correspondence: Lili Liang, The Cosmetic and Plastic Surgery, Department of Shanxi Provincial People’ s Hospital, Shanxi Medical University, 29 Shuangta Temple St, Taiyuan, Shanxi, 030012, People’s Republic of China, Email [email protected]
Abstract: Rosacea is a chronic inflammatory skin disease with a global prevalence of approximately 5.1%. Existing evidence suggests that its pathogenesis may be associated with dysregulation of the neuro-hormone-immune network within the skin-gut-brain axis framework. This review summarizes the potential roles of stress hormones, sex hormones, and insulin-like growth factor-1 in the four major subtypes. In erythematotelangiectatic rosacea, glucocorticoid resistance within keratinocytes may induce CCL20-driven Th17 inflammation, while catecholamines released by sympathetic nerves are associated with neurovascular flushing. In papulopustular rosacea, androgen excess, relative estrogen deficiency, LL-37-mediated innate immune activation, and gut microbiota dysbiosis may collectively contribute to the formation of inflammatory skin lesions.In the phymatous type, insulin-like growth factor-1 and androgens may interact through the PI3K/Akt/mTOR and FoxO1 pathways, promoting sebaceous gland hyperplasia and fibrosis. Ocular rosacea is associated with gut-derived low-grade systemic inflammation and neurogenic inflammation. For treatment, β-receptor blockers such as carvedilol and selective serotonin reuptake inhibitors such as paroxetine can be used for erythematotelangiectatic rosacea; anti-androgen drugs like spironolactone and metformin may be explored for papulopustular rosacea; metformin for the phymatous type; and for ocular rosacea, topical corticosteroids can be used cautiously for a short term under ophthalmological supervision. Adjunctive interventions such as eradication of small intestinal bacterial overgrowth, a low glycemic index diet, and mindfulness-based stress reduction therapy also demonstrate potential.Taken together, existing evidence supports viewing rosacea as a systemic disease potentially mediated by the skin-gut-brain axis and characterized by dysregulation of the neuro-hormone-immune network. However, more high-quality randomized controlled trials and stratified studies guided by hormone-related biomarkers are currently needed to further validate its mechanisms and advance precision treatment.
Keywords: rosacea, neuro-hormone-immune network, skin-gut-brain axis, targeted therapy
Introduction
Rosacea
Rosacea is a common chronic inflammatory skin disease primarily affecting the central facial region, characterized by persistent erythema, paroxysmal flushing, capillary telangiectasia, inflammatory papules, and pustules. Some patients may develop complications such as ocular involvement or nasal soft tissue hyperplasia.1,2 The Global Burden of Disease Study indicates that the prevalence of rosacea is approximately 5.1%, with the highest incidence observed among adults aged 30 to 50 years, and the morbidity is significantly higher in females than in males.3,4 The disease not only causes local discomfort and cosmetic impairment but also substantially increases the risk of psychological comorbidities such as anxiety, depression, and social avoidance, thereby seriously affecting patients’ quality of life.5,6
The pathogenesis of rosacea involves complex interactions among multiple factors, including genetic susceptibility, neurovascular dysregulation, innate immune hyperactivation, skin barrier dysfunction, and aberrant colonization of follicular microorganisms.7 (Table 1) Abnormal activation of transient receptor potential (TRP) channels can induce the release of various neuropeptides, triggering vasodilation and neurogenic inflammation.8,9 Antimicrobial peptide LL-37 is overexpressed in skin lesions and amplifies the inflammatory cascade by activating immune cells.10,11 Following impaired skin barrier, external irritants and microorganisms can readily invade, further inducing local inflammation.12,13 Psychological stress is also the most common trigger of acute onset in clinical settings, capable of directly inducing facial flushing and burning sensation.14 Models based solely on local skin inflammation are insufficient to fully account for the clinical heterogeneity and complexity of rosacea.15 In recent years, the concept of the skin-gut-brain axis has been introduced into this field. This axis integrates gut microbiota, neuroimmune signaling, autonomic nerve function, and stress-related neuroendocrine regulation, describing an integrated system of bidirectional communication among the central nervous system, the gut, and the skin via neural, endocrine, and immune pathways.16,17 Emerging evidence suggests that rosacea may be a systemic disease actively regulated by the central nervous system, and that it can be interpreted within the framework of the skin-gut-brain axis.18 The strength of evidence supporting these mechanisms varies, with some derived from robust clinical observations and others primarily from in vitro or animal studies.
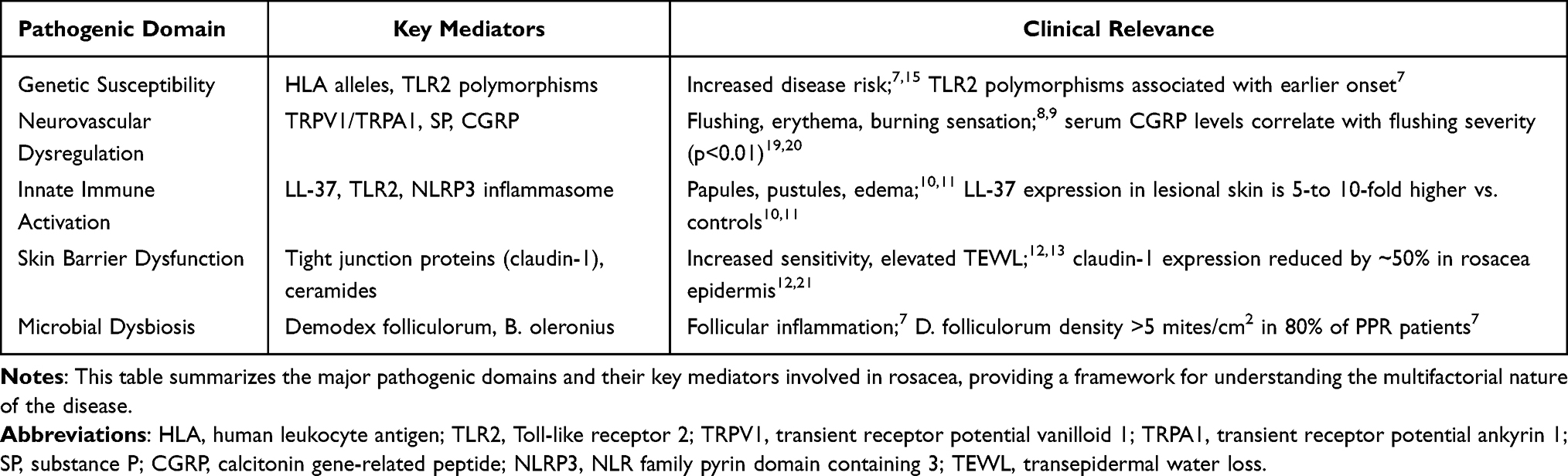 |
Table 1 Key Pathogenic Mechanisms in Rosacea |
Subtypes of Rosacea
According to the recommendations of the International Rosacea Expert Committee, the disease is classified into four subtypes based on characteristic clinical features: erythematotelangiectatic subtype (erythematotelangiectatic rosacea, ETR), papulopustular subtype (papulopustular rosacea, PPR), phymatous subtype (phymatous rosacea), and ocular subtype (ocular rosacea).1 Each subtype has relatively distinct pathophysiological mechanisms, although clinical overlap is common.
Erythematotelangiectatic Subtype (ETR)
ETR is characterized primarily by central facial persistent erythema and capillary telangiectasia, with neurovascular dysregulation as its core driving mechanism. Aberrant activation of TRP channels and the release of neuropeptides, such as substance P (SP) and calcitonin gene-related peptide (CGRP), represent key molecular events.8,9 In ETR skin lesions, glucocorticoid receptor (GR) resistance may be present, causing cortisol to shift from an anti-inflammatory signal to a pro-inflammatory signal: cortisol can induce keratinocytes to overexpress CCL20, which subsequently recruits Th17 cells, thereby forming a stress-inflammation positive feedback loop.21,22 Psychological stress further amplifies the aforementioned vascular and inflammatory responses by activating the central hypothalamic-pituitary-adrenal (HPA) axis and the sympathetic nervous system.23,24
Papulopustular Subtype (PPR)
PPR is characterized by the development of inflammatory papules and pustules superimposed on persistent erythema. Its pathological mechanisms involve innate immune dysregulation and sex hormone influences. Overexpression of antimicrobial peptide LL-37 is a prominent feature of PPR.10,11 Androgens stimulate sebaceous gland hyperfunction and upregulate pro-inflammatory cytokines, whereas physiological doses of estrogen may exert a protective effect by suppressing the TLR2/NF-κB pathway.25,26 Sex hormone imbalance can also alter intestinal flora composition and disrupt intestinal barrier integrity, leading to a state of systemic low-grade inflammation that further aggravates skin lesions27–29 (Figure 1).
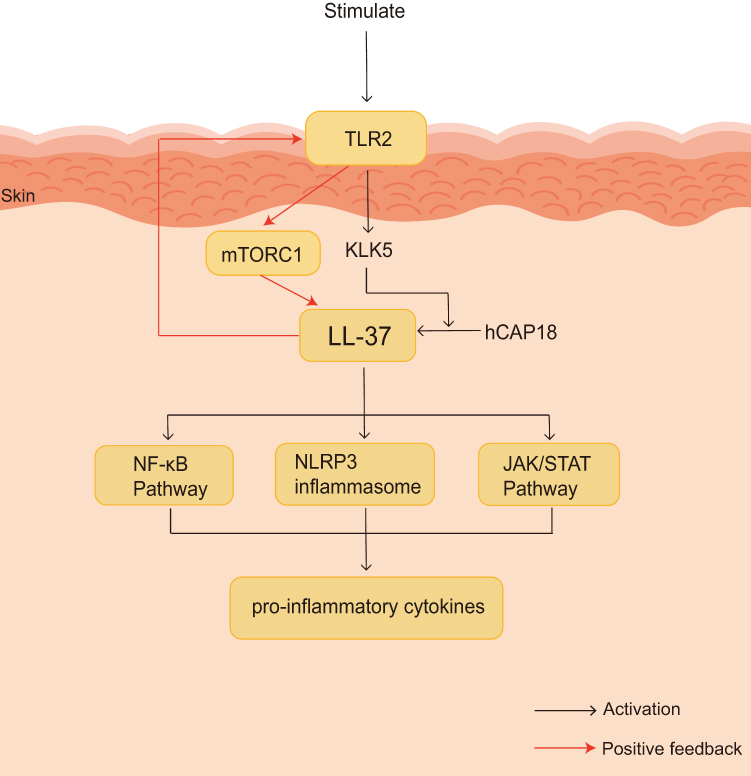 |
Figure 1 Positive feedback loop of innate immune activation in rosacea skin. Abbreviations: TLR2, Toll-like receptor 2; KLK5, kallikrein-related peptidase 5; hCAP18, human cationic antimicrobial protein 18; LL-37, cathelicidin-derived peptide; NF-κB, nuclear factor κB; NLRP3, NOD-like receptor thermal protein domain-associated protein 3; JAK/STAT, Janus kinase/signal transducer and activator of transcription; mTORC1, mammalian target of rapamycin complex 1. Notes: The figure illustrates how interconnected signaling pathways in keratinocytes drive skin inflammation. Activation of TLR2 and KLK5 promotes the processing of hCAP18 into the active antimicrobial peptide LL-37. LL-37 subsequently activates multiple downstream pathways, including NF-κB, the NLRP3 inflammasome, and JAK/STAT, leading to the production of pro-inflammatory cytokines. These cytokines further activate mTORC1, which in turn enhances LL-37 expression, thereby establishing an inflammation-amplifying loop (positive feedback). Ultimately, this cascade drives the development of the rosacea skin phenotype. |
Hypertrophic Subtype
The hypertrophic subtype is characterized by sebaceous gland hyperplasia and connective tissue hypertrophy, most commonly affecting the nose and manifesting as rhinophyma. Insulin-like growth factor-1 (IGF-1) promotes sebum production, keratinocyte proliferation, and fibrotic changes through activation of the PI3K/Akt/mTOR signaling pathway.30–32 Overactivation of the androgen receptor (AR) can further enhance tissue overgrowth via IGF-1-mediated inactivation of FoxO1.33 Chronic inflammation and aberrant mechanotransduction may synergistically drive the process of fibrosis.1
Ocular Subtype
The ocular subtype of rosacea primarily manifests as meibomian gland dysfunction, conjunctival inflammation, and keratitis. Dysregulation of the skin-gut axis frequently coexists with this subtype, and small intestinal bacterial overgrowth (SIBO) has been detected in a subset of affected patients.27,34 Neurogenic inflammation and tear film instability are important mechanisms underlying ocular surface injury.35 Systemic inflammation originating from the gut can directly affect ocular tissues through shared immune pathways.27,28
The subtype-specific mechanisms described above are not mutually exclusive, and overlapping features are commonly observed in clinical practice. Although previous studies have separately examined the roles of neurovascular regulation, hormonal imbalance, immune-mediated inflammation, and gut microbiota in rosacea, most reviews remain focused on single mechanisms or conventional treatments, lacking systematic integration of these factors within the skin-gut-brain axis framework. Hormones, as central messengers linking the brain, gut, and skin, have not been sufficiently integrated with respect to their differential regulatory roles across subtypes; likewise, subtype-specific treatment strategies grounded in the neuro-hormone-immune network lack systematic synthesis of clinical evidence. This review systematically integrates, within the skin-gut-brain axis framework, the regulatory roles of endogenous and exogenous hormones in the neuro-hormone-immune network of rosacea, proposes that rosacea may represent a systemic disease characterized by neuro-hormone-immune network dysregulation, and summarizes the existing clinical evidence for hormone-targeted therapy, neurovascular intervention, and gut microbiota modulation across the four clinical subtypes, with the aim of providing a theoretical reference for precise stratified treatment.
Search Strategy
This review strictly adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines to ensure rigor and transparency throughout the literature screening and analysis process. Relevant studies were retrieved from four major electronic databases, namely PubMed, Web of Science, Embase, and China National Knowledge Infrastructure (CNKI), with the search period spanning from each database’s inception to May 2026. To balance currency and academic traceability, the search focused primarily on innovative studies published within the past 15 years (2011–2026) while also incorporating early landmark foundational studies. Search terms combined Medical Subject Headings (MeSH) and free text terms, including: “rosacea,” “neurohormonal-immune network,” “skin-gut-brain axis,” “glucocorticoid,” “sex hormone,” “insulin-like growth factor-1,” “IGF-1,” “TRP channel,” “neurogenic inflammation,” “gut microbiota,” “central sensitization,” “targeted therapy,” “beta-blocker,” “SSRIs,” “spironolactone,” “metformin,” and “probiotic.”Search strategies were constructed based on the research topics using Boolean operators (AND, OR, NOT). The literature screening process followed the PRISMA 2020 flow diagram. First, duplicate records were removed using EndNote 2025 software based on matching criteria including title, author, journal, and publication year. Second, two independent researchers screened out and excluded irrelevant studies by reading titles and abstracts. Third, full-text assessment was conducted for potentially eligible studies. Finally, all discrepancies were resolved through discussion with a third independent researcher. Structured quality assessment was applied to all included studies to ensure that only studies of moderate-to-high quality were incorporated into the final synthesis.
Regulation by Endogenous Hormones
Stress Hormones
The skin possesses independent neuroendocrine function. The epidermis, dermis, and skin appendages harbor a complete steroid synthetic pathway capable of de novo synthesis of biologically active glucocorticoids from cholesterol via the key enzymes CYP11A1 and CYP11B1.36 This synthetic pathway is coupled to a local hypothalamic-pituitary-adrenal (HPA) axis homologous system, namely the corticotropin-releasing hormone (CRH)-pro-opiomelanocortin (POMC) axis. Endogenous glucocorticoids exert negative feedback regulation on this axis, thereby maintaining local cutaneous immune-inflammatory homeostasis.37 11β-hydroxysteroid dehydrogenase type 1 (11β-HSD1), which is highly expressed in skin cells, regulates the conversion of corticosterone to active cortisol and serves as the core molecular switch governing local hormone levels.38
Ultraviolet radiation (UV) exposure or physical and chemical stimulation can disrupt this local homeostasis. UV radiation activates the cutaneous HPA-like axis in a wavelength-dependent manner, inducing high CRH expression and promoting the cleavage of POMC into neuropeptides such as melanocyte-stimulating hormone (MSH) and pro-inflammatory factors.39 This stress response circuit simultaneously stimulates endogenous glucocorticoid synthesis and interferes with glucocorticoid negative feedback regulation, resulting in dysregulation of local hormone synthesis and metabolism.40
Psychological stress activates the central HPA axis, triggering the release of glucocorticoids and catecholamines.23,24 Whether functional glucocorticoid receptor (GR) resistance exists in rosacea skin lesions remains to be clarified. Chronic stress can downregulate GR expression and impair its nuclear translocation.22 In human keratinocytes, glucocorticoids promote CCL20 expression by directly binding to the CCL20 enhancer region via activated GR.21 CCL20 recruits Th17 cells to infiltrate lesional sites, a mechanism that may contribute to inflammatory amplification in rosacea.
Activation of the sympathetic nervous system during psychological stress leads to the release of catecholamines.23 Catecholamines bind to α- and β-adrenergic receptors on keratinocytes, vascular endothelial cells, and immune cells, thereby modulating cutaneous vasodilation, vascular permeability, and the production of inflammatory cytokines.24 In rosacea, sympathetic dominance and autonomic dysfunction contribute to facial flushing and persistent erythema.41,42 Clinical evidence that beta-blockers alleviate neurovascular symptoms suggests that catecholamines may be involved.43,44 Catecholamines may act synergistically with glucocorticoids. Glucocorticoids establish a pro-inflammatory environment through GR resistance and CCL20 induction, while catecholamines trigger acute vasomotor episodes. Within this integrated stress hormone network, glucocorticoids mediate chronic immune reprogramming whereas catecholamines drive acute vascular responses.
This mechanism provides a possible explanation for the dysregulation of the brain-skin axis: cortisol, which is released from the central nervous system via the HPA axis and should exert an anti-inflammatory effect, may be erroneously converted into a pro-inflammatory signal due to GR resistance.45
Stress hormones contribute to the pathogenesis of ETR primarily through neurovascular dysregulation. GR resistance may be present in ETR skin lesions, shifting cortisol from an anti-inflammatory to a pro-inflammatory signal and amplifying inflammation via the CCL20–Th17 axis.21 Catecholamines released through sympathetic nerve activation directly induce facial flushing and persistent erythema.41,42 In PPR, GR resistance-mediated Th17 immune responses are likewise implicated in the formation of papules and pustules.46,47 Direct evidence linking stress hormones to phymatous rosacea and ocular rosacea is limited, and their influence in these subtypes may be mediated indirectly through systemic inflammation.
Sex Hormones
Rosacea exhibits pronounced sexual dimorphism: prevalence is higher in females, whereas males are more prone to developing severe phymatous rosacea.These differences are closely related to the regulatory roles of sex hormones in the skin, immune system, and gut microbiota.
Estrogen exerts a protective role in rosacea by promoting keratinocyte proliferation, enhancing skin barrier repair, and upregulating ceramide synthesis.48 Estrogen modulates the sensitivity of TRPV1 and TRPA1 channels and nitric oxide production, thereby regulating neurovascular reactivity and attenuating flushing and erythema.49,50 Estrogen also downregulates TLR2 expression, suppresses the NF-κB signaling pathway, and reduces the production of pro-inflammatory cytokines.26
Androgen stimulates sebaceous gland hyperfunction and excessive sebum secretion, promoting follicular inflammation.51 By binding to androgen receptors (AR) in sebaceous gland cells, androgen activates downstream signaling pathways, thereby promoting sebaceous gland cell proliferation and lipid synthesis.5α-reductase converts testosterone into the more potent dihydrotestosterone (DHT).51 Androgens exert a negative regulatory effect on skin barrier integrity by suppressing the expression of lipid synthases.52
Sex hormones and gut microbiota. Sex hormones directly influence the composition of gut microbiota. Hyperandrogenemia reduces beneficial bacteria and impairs intestinal barrier function, leading to endotoxin translocation and systemic low-grade inflammation.27,28 These inflammatory signals reach the skin via the bloodstream, thereby exacerbating rosacea. Estrogen may counteract these effects by maintaining microbial diversity and intestinal barrier integrity, although clinical evidence remains limited.27 Gut microbiota can also modulate sex hormone metabolism: gut microorganisms express β-glucuronidase, which cleaves conjugated estrogens and androgens, thereby facilitating their reabsorption [27].Environmental endocrine disruptors such as bisphenol A can mimic endogenous hormones and aberrantly activate local cutaneous hormone signaling pathways.53,54
Sex hormone imbalance and subtype involvement. Androgens promote the formation of inflammatory papules and pustules in PPR.25,26 In phymatous rosacea, androgens act synergistically with IGF-1 to drive sebaceous gland hyperplasia and fibrosis.33 Estrogen exerts a protective effect, particularly in female patients with PPR.55 In ocular rosacea, a subset of patients exhibits relative hypoandrogenism.27 The direct association between ETR and sex hormones is relatively weak.
Pregnancy-related hormone fluctuations can significantly affect the clinical course of rosacea.56 A single-center retrospective survey of 39 patients found that approximately half of the women experienced symptom worsening during the gestational period, approximately one-third showed no appreciable change, and only approximately one-sixth demonstrated improvement.56 Pregnancy may also trigger fulminant rosacea, a rare condition. Bettolini et al compiled 27 pregnancy-related cases, of which 54% had onset during the first trimester, 58% had a prior history of acne or rosacea, and 45% were primiparous.57 Furthermore, a prospective cohort analysis based on the Nurses’ Health Study II indicated that nulliparous women face a higher risk of developing rosacea than parous women, and that both early and advanced age at first birth are associated with increased risk.55 A 2025 systematic review evaluating the effects of menopause and menopausal hormone therapy on common dermatoses found that rosacea generally showed an improving trend after menopause.However, postmenopausal hormone therapy was associated with an increased risk of rosacea. The review also explicitly noted that the available evidence remains limited and inconsistent,58 indicating that future prospective studies with larger sample sizes and standardized MHT formulations are needed to establish causality.A retrospective cohort study enrolling 210,274 women using intrauterine devices found a significant association between the use of a high-dose hormone intrauterine device containing 52 mg levonorgestrel and an increased risk of rosacea diagnosis, with a 47.2% increase in risk after 5 years of use.59
Insulin-Like Growth Factor-1
Insulin-like growth factor-1 (IGF-1) is a polypeptide hormone that possesses both metabolic regulation and inflammation regulation functions.30 By activating the downstream PI3K/Akt/mTOR signaling pathway,31 IGF-1 promotes the expression of inflammatory markers in sebaceous gland cells and stimulates sebum production,51 while also mediating keratinocyte proliferation and promoting the release of pro-inflammatory factors and angiogenic factors.32 IGF-1 enhances the sensitivity of skin nerve endings, upregulates the expression levels of transient receptor potential channels, and exacerbates neurovascular symptoms such as facial flushing and burning sensation in rosacea patients.30 High-sugar diet and excessive dairy intake can elevate serum IGF-1 levels.33 Metformin inhibits IGF-1-related signaling pathways in LL-37 induced mouse models60 and upregulates anti-angiogenic thrombospondin-1 via the NF-κB and Erk1/2/Erk5 pathways.61
IGF-1 is primarily involved in the hypertrophic subtype and PPR. In the hypertrophic subtype, IGF-1 promotes sebaceous gland hyperplasia, keratinocyte proliferation, and dermal fibrosis.31,32 In PPR, IGF-1 enhances sebaceous gland inflammatory marker expression51 and may exacerbate neurovascular symptoms by upregulating TRP channel sensitivity.30 In ETR, the effect of IGF-1 is primarily manifested as the worsening of flushing symptoms.30 There is no direct research evidence for the ocular subtype.
The Challenge of Exogenous Hormones
Topical Glucocorticoids
Glucocorticoids are widely used anti-inflammatory agents in clinical practice; however, prolonged topical or systemic use of glucocorticoids can paradoxically induce or exacerbate rosacea symptoms, a condition referred to as steroid-induced rosacea.62 The core mechanisms by which exogenous hormones trigger rosacea are closely associated with impaired skin barrier, local HPA axis inhibition, aggravated GR resistance, and abnormal activation of inflammatory pathways.62 A systematic review demonstrated that topical and systemic glucocorticoids are the most common causative agents in drug-induced rosacea, accounting for 89.2% of the 2,205 drug-induced rosacea cases included.63 A case-control study further confirmed that serum cortisol levels in patients with hormone-related rosacea were significantly lower than those in patients with non-hormone-related rosacea, suggesting that long-term topical glucocorticoid use can suppress local HPA axis activity.47
Other Exogenous Hormone Interventions
Beyond topical glucocorticoids, other exogenous steroid hormone preparations and hormone replacement therapy regimens can also significantly affect the clinical course of rosacea, with sex hormone-related preparations exerting the most prominent effects.64 In some female rosacea patients receiving oral contraceptives or estrogen replacement therapy, disease symptoms exhibit marked interindividual variability, manifesting as two distinct clinical outcomes: symptom remission or symptom exacerbation.65 This clinical phenomenon is closely associated with individualized factors such as baseline hormone levels, gut microbiota composition, and immune response sensitivity, which also provide a clinical basis for implementing hormone-targeted personalized intervention strategies in rosacea management.27 Environmental endocrine disruptors and exogenous growth factor preparations can mimic the biological actions of endogenous hormones, thereby aberrantly activating local cutaneous hormone signaling pathways and indirectly modulating the inflammatory process and disease severity of rosacea.53 This aberrant activation of hormone signaling pathways mediated by the aforementioned exogenous factors represents an important exogenous trigger for clinical disease fluctuation in rosacea.54
Integration of the Neuro-Hormonal-Immune Network
Central Nervous System
Within the framework of the skin-gut-brain axis, the central nervous system actively regulates the pathological processes of rosacea.18 (Figure 2) This regulation is achieved through three interrelated mechanisms: central sensitization, autonomic dysfunction, and stress-related neuroendocrine activation.66
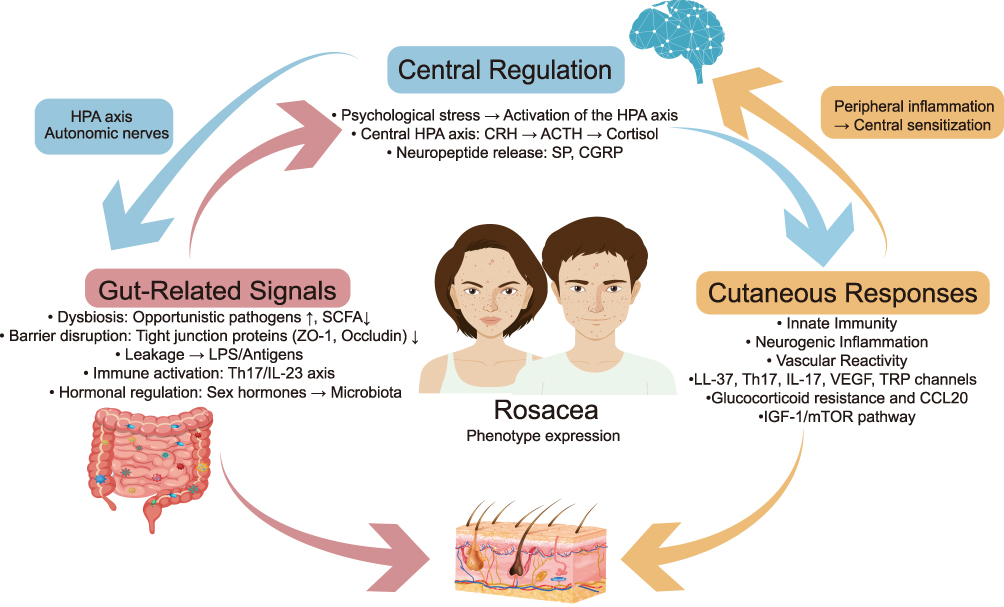 |
Figure 2 Schematic diagram of the neuro-hormone-immune integration mechanism in rosacea. Abbreviations: HPA, hypothalamic-pituitary-adrenal; CRH, corticotropin-releasing hormone; ACTH, adrenocorticotropic hormone; SP, substance P; CGRP, calcitonin gene-related peptide; SCFA, short-chain fatty acids; LPS, lipopolysaccharide; Th17, T helper 17 cell; IL-23, interleukin-23; LL-37, cathelicidin; TRP, transient receptor potential; VEGF, vascular endothelial growth factor; IGF-1, insulin-like growth factor-1; mTOR, mammalian target of rapamycin; CCL20, chemokine ligand 20. Notes: Central regulation(Blue) involves psychological stress activating the HPA axis and central sensitization accompanied by neuropeptide release. Gut-related signals(Red) include gut microbiota dysbiosis, barrier disruption leading to LPS/antigen leakage and Th17/IL-23 immune activation, and hormone regulation. Skin responses(Yellow) encompass innate immunity, neurogenic inflammation, vascular reactivity, and key molecular pathways, such as LL-37, Th17, IL-17, VEGF, TRP channel, glucocorticoid resistance accompanied by CCL20, and the IGF-1/mTOR pathway, ultimately leading to rosacea phenotype expression. Overall framework of the skin-gut-brain axis. This figure integrates central regulation, gut-related signals, and skin response, all of which collectively contribute to the expression of the rosacea phenotype. Arrow legend: Solid arrows (→) indicate positive regulation (promotion, activation, or increased expression). |
Central sensitization refers to the enhanced reactivity of central pain and sensory pathways resulting from repeated or sustained peripheral input.67 Altered brain activity has been observed in patients with rosacea, suggesting the potential involvement of central sensitization.68 Trigeminal afferent fibers converge with cervical afferent pathways at the cervicothoracic trigeminal nucleus, providing an anatomical basis for the central amplification of craniofacial sensory abnormalities.69 Autonomic nervous system dysfunction serves as a critical mediator of brain-skin interactions. Autonomic imbalance characterized by sympathetic predominance and attenuated parasympathetic regulation exacerbates vasodilation, increases facial skin blood flow, and promotes neurogenic inflammation.41,42 Patients with rosacea frequently present with psychiatric comorbidities such as anxiety and depression.70
Psychological stress triggers activation of the central HPA axis and the sympathetic branch of the autonomic nervous system, leading to the release of glucocorticoids and catecholamines. These hormones directly modulate skin immune cell activity, vascular tone, and barrier function.23,24 Stress-related neuroendocrine activation also exerts profound effects on gastrointestinal function, altering intestinal motility, increasing intestinal mucosal permeability, and reshaping intestinal flora composition.16,17 This, in turn, amplifies neurogenic inflammation and vascular reactivity in rosacea through shared autonomic and immune pathways.
Hormones and the Neuro-Immune-Barrier Network
Neurovascular dysfunction is a key pathological feature underlying facial flushing, persistent erythema, and burning sensation in rosacea.71 Sex hormones regulate the functional homeostasis of the skin neurovascular system through multidimensional mechanisms.72 Estrogen suppresses keratinocyte proliferation and reduces pro-inflammatory cytokine release via the GPER1-mediated non-classical pathway.73 The GPER1 signaling pathway also modulates calcium ion concentration and nitric oxide synthase activity in vascular endothelial cells.74 Plasma calcitonin gene-related peptide (CGRP) levels are elevated in patients with rosacea.19 Serum CGRP levels in patients with neurogenic rosacea are positively correlated with clinical severity, flushing severity, and treatment outcome.20 Activation of the TRPV1–NGF–TrkA pathway is associated with neurogenic inflammation in rosacea, and the expression of pathway-related markers is elevated in the presence of Demodex folliculorum.75 The stress-responsive neurovascular axis modulates skin immune accessibility.76
A close interaction exists between the hormone system and the skin innate immune system. The TLR2 pathway is a central component of innate immune activation in rosacea and is markedly overexpressed in keratinocytes from affected patients. Activation of TLR2 signaling promotes the assembly of the NLRP3 inflammasome, driving the release of potent pro-inflammatory factors such as IL-1β, thereby amplifying inflammation and contributing to the formation of facial papules, pustules, and vasodilation.77
Glucocorticoids exhibit paradoxical effects within the pathological microenvironment of rosacea.At physiological concentrations, cortisol binds to GR and exerts anti-inflammatory effects by suppressing the activity of pro-inflammatory transcription factors such as NF-κB. However, under conditions of sustained aberrant activation of the TLR2 pathway in rosacea skin lesions, glucocorticoids paradoxically induce high CCL20 expression in keratinocytes.21 CCL20 recruits Th17 cells and immature dendritic cells to the lesional site, driving Th17-mediated chronic inflammatory reactions.
The structural and functional integrity of the skin barrier depends on normal keratinocyte proliferation and differentiation, tight junction protein expression, and formation of the epidermal extracellular lipid layer.7 Estrogen selectively activates specific receptors in keratinocytes,78 thereby promoting keratinocyte proliferation and differentiation, upregulating the biosynthesis of key barrier lipids,79 and enhancing both the structural integrity of the skin barrier and its capacity for injury repair.80 This mechanism has not yet been directly demonstrated in rosacea.In contrast, androgens exert a negative regulatory effect on skin barrier formation and repair by suppressing the expression of epidermal lipid synthesis-related enzymes.25 Chronic psychological stress or prolonged use of topical glucocorticoids downregulates the expression of tight junction proteins, including claudin-1 and occludin, in keratinocytes.22 Aberrant expression of tight junction proteins leads to increased transepidermal water loss, thereby heightening epidermal susceptibility to environmental irritants and microbial invasion.12 This establishes a self-amplifying cycle of inflammation and barrier damage.Skin barrier disruption promotes local inflammation upon exposure to external stimuli and microbial invasion; pro-inflammatory cytokines further suppress the expression of barrier-related proteins, perpetuating the deterioration of skin barrier function.13 The hormone system plays a regulatory role in the composition and function of the skin and gut microbiota. (Figure 3)Androgen-driven sebaceous gland hyperfunction provides a nutritional source for Demodex folliculorum, potentially altering the skin surface microecological environment and promoting the colonization and proliferation of opportunistic pathogens.81 The immunosuppressive effect of glucocorticoids impairs the immune surveillance ability of the skin immune system against resident and opportunistic microorganisms, thereby increasing secondary infection risk.25 Sex hormone imbalance and alteration of intestinal flora structure exhibit a bidirectional interaction. Sex hormones directly influence the composition and metabolic function of the gut microbiota, while the gut microbiota in turn regulates the enterohepatic circulation and metabolic clearance of sex hormones.Modulating the gut microbiota through probiotics, prebiotics, or dietary interventions may indirectly ameliorate systemic and local inflammatory pathways associated with hormonal metabolism.82 Treatment strategies for neurogenic rosacea include interventions targeting neuroinflammatory pathways.83
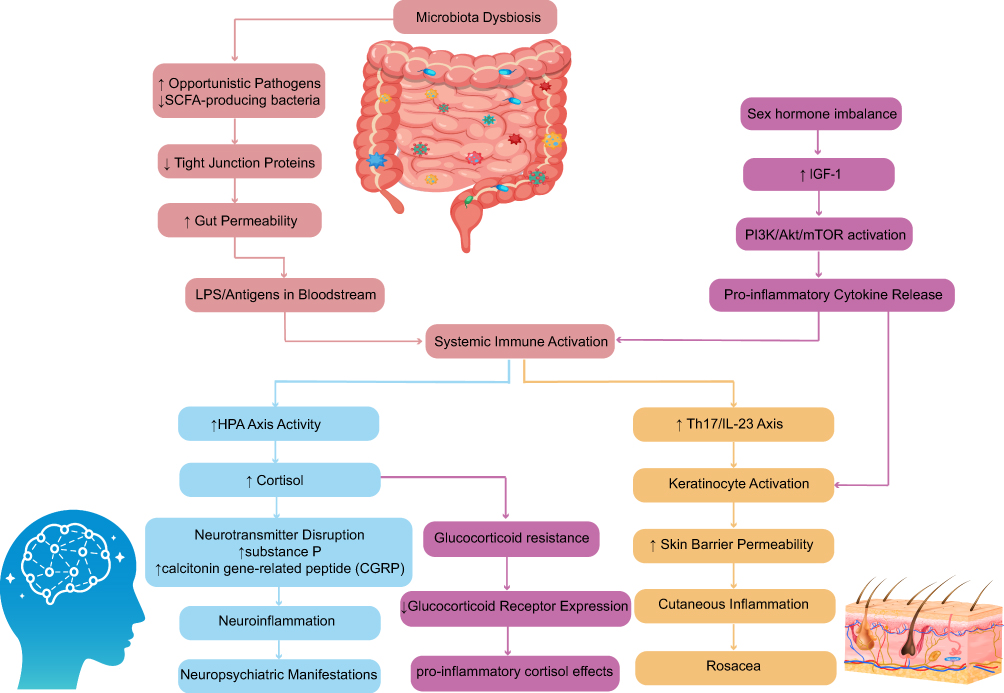 |
Figure 3 Schematic illustration of proposed neurohormone-immune network dysregulation in rosacea pathogenesis, centered on the skin-gut-brain axis. Abbreviations: SCFA, short-chain fatty acids; LPS, lipopolysaccharide; HPA, hypothalamic-pituitary-adrenal; IGF-1, insulin-like growth factor-1; PI3K, phosphatidylinositol 3-kinase; Akt, protein kinase B; mTOR, mammalian target of rapamycin; Th17, T helper 17 cell; IL-23, interleukin-23; CGRP, calcitonin gene-related peptide. Notes: The figure depicts a sequence of events initiated by gut microbiota dysbiosis. This dysbiosis leads to downregulation of tight junction protein, increased gut permeability, and bacterial product translocation into the bloodstream, thereby triggering systemic immune activation. Systemic inflammation stimulates the hypothalamic-pituitary-adrenal (HPA) axis, resulting in elevated cortisol levels. Cortisol-induced neurotransmitter dysregulation promotes neuroinflammation and contributes to neuropsychiatric manifestation. Concurrently, sex hormone imbalance and elevated Insulin-like growth factor-1 (IGF-1) activate the PI3K/Akt/mTOR pathway, driving pro-inflammatory cytokine release and expansion of the Th17/IL-23 axis.These events lead to keratinocyte activation, glucocorticoid resistance, and increased skin barrier permeability, ultimately resulting in skin inflammation and the clinical phenotype of rosacea. Arrows indicate multiple feedback loops; for example, neuroinflammation exacerbates gut microbiota dysbiosis. Color meanings: Blue: Central regulation. Red: Gut-related signals. Yellow: Skin responses. Purple: Hormones. Arrow legend: All solid arrows indicate positive regulation (promotion, activation, expression, or increased activity). Up/down arrows (↑/↓) indicate increases or decreases in the levels of specific microbial taxa or molecules. |
Various hormone systems interact through complex signal networks.8 IGF-1 activates the PI3K/Akt signaling pathway, leading to the phosphorylation and inactivation of FoxO1 and its retention in the cytoplasm. This process relieves FoxO1-mediated suppression of androgen receptor (AR) transcriptional activity, thereby enhancing AR signaling and the expression of its downstream target genes.33 Elevated serum IGF-1 levels induced by a high-sugar diet and excessive dairy intake amplify the pathological effects of androgens through the same molecular mechanism, closely linking metabolic disorders to the inflammatory process of rosacea. The four subtypes exhibit distinct integration patterns within the neuro-hormonal-immune network. ETR is centered on central sensitization, autonomic dysfunction, and the glucocorticoid paradox mediated by GR resistance. PPR is characterized by sex hormone imbalance, Th17-driven inflammation, and gut-skin axis interactions. The hypertrophic subtype is defined by IGF-1-androgen crosstalk-driven fibrosis. The ocular subtype is closely associated with gut-skin axis dysregulation and neurogenic inflammation.84
Treatment Strategies and Prospects Based on Regulatory Networks
Subtype-Specific Treatment Strategies
Treatment options for rosacea are highly subtype-dependent, as each subtype is driven by distinct pathophysiological mechanisms.1,7 The clinical evidence is summarized below by subtype.
Erythematotelangiectatic Subtype (ETR)
ETR is characterized by neurovascular hyperreactivity without significant androgen-driven pathology.8,9 Anti-androgen therapy is not applicable for ETR alone. In mixed rosacea where ETR coexists with PPR, the hormone-targeted therapy options described in Papulopustular Subtype (PPR) may be considered.25,26
Avoiding glucocorticoids is particularly important in ETR. Long-term use of topical glucocorticoids can induce steroid-induced rosacea, manifesting as flushing, capillary telangiectasia, and erythema.62 ETR patients should be advised to avoid using potent or moderate-potency topical glucocorticoids on the face.62
The targeting of the IGF-1 pathway by metformin has not been directly studied in ETR. IGF-1 can enhance the sensitivity of TRP channels and exacerbate flushing.30 The potential of metformin to reduce IGF-1 levels warrants investigation in ETR patients with flushing driven by metabolic factors.85
Papulopustular Subtype (PPR)
PPR involves Th1/Th17 inflammation, LL-37 dysregulation, and sex hormone influences.10,21,25 Spironolactone possesses anti-androgen activity.86 Its use in female PPR is primarily based on data from common acne studies.87 Preclinical studies have shown that spironolactone-loaded nanofibers reduce erythema scores in a croton oil-induced inflammation model.88 Spironolactone nanoformulations demonstrate topical treatment potential.89
Combined oral contraceptives containing antiandrogen progestogens can reduce ovarian androgen secretion, increase hepatic sex hormone-binding globulin synthesis, and lower circulating free androgen levels.90,91 Their efficacy in rosacea has not been validated by dedicated randomized controlled trials (RCTs).
Clascoterone 1% cream is a topical androgen receptor antagonist.92 Its efficacy in rosacea has not been directly studied.93 Studies specifically targeting PPR are warranted.
Metformin improves rosacea-like skin lesions in a rosacea mouse model induced by LL-37 and TNF-α.60 Multiple reviews have highlighted its potential therapeutic value.94 Until human clinical trial evidence is obtained, metformin cannot be recommended for routine treatment of rosacea.
Long-term use of topical glucocorticoids can lead to steroid-induced rosacea, with clinical manifestations resembling PPR.62 A detailed history of topical glucocorticoid use should be obtained from all patients with PPR, and gradual dose discontinuation under medical supervision should be implemented.62
Hypertrophic Subtype
Hypertrophic rosacea is characterized by fibrosis and sebaceous gland hyperplasia, accompanied by overactivation of the IGF-1 and androgen pathways.31,33
Metformin has shown promise in preclinical studies. An LL-37-induced rosacea mouse model demonstrated that metformin treatment reduced dermal fibrosis, inflammatory cell infiltration, and angiogenic markers.95 Human data are currently lacking. Metformin is not recommended for routine use in hypertrophic rosacea outside of clinical trials.61
Glucocorticoids are contraindicated in hypertrophic rosacea. Glucocorticoids cannot reduce pre-existing fibrotic tissue and may suppress local immunity.62
Ocular Subtype
Ocular rosacea involves meibomian gland dysfunction and ocular surface inflammation. Androgens play a regulatory role in meibomian gland function.96 A randomized controlled trial (RCT) demonstrated that eyelid application of 4.5% testosterone gel improved tear film stability in patients with moderate-to-severe dry eye.97 To date, no large-scale randomized controlled trial specifically designed for ocular rosacea has been conducted.98 Androgen replacement therapy is not recommended as a routine treatment.Metformin and other IGF-1 modulators have not been studied in ocular rosacea99 (Table 2).
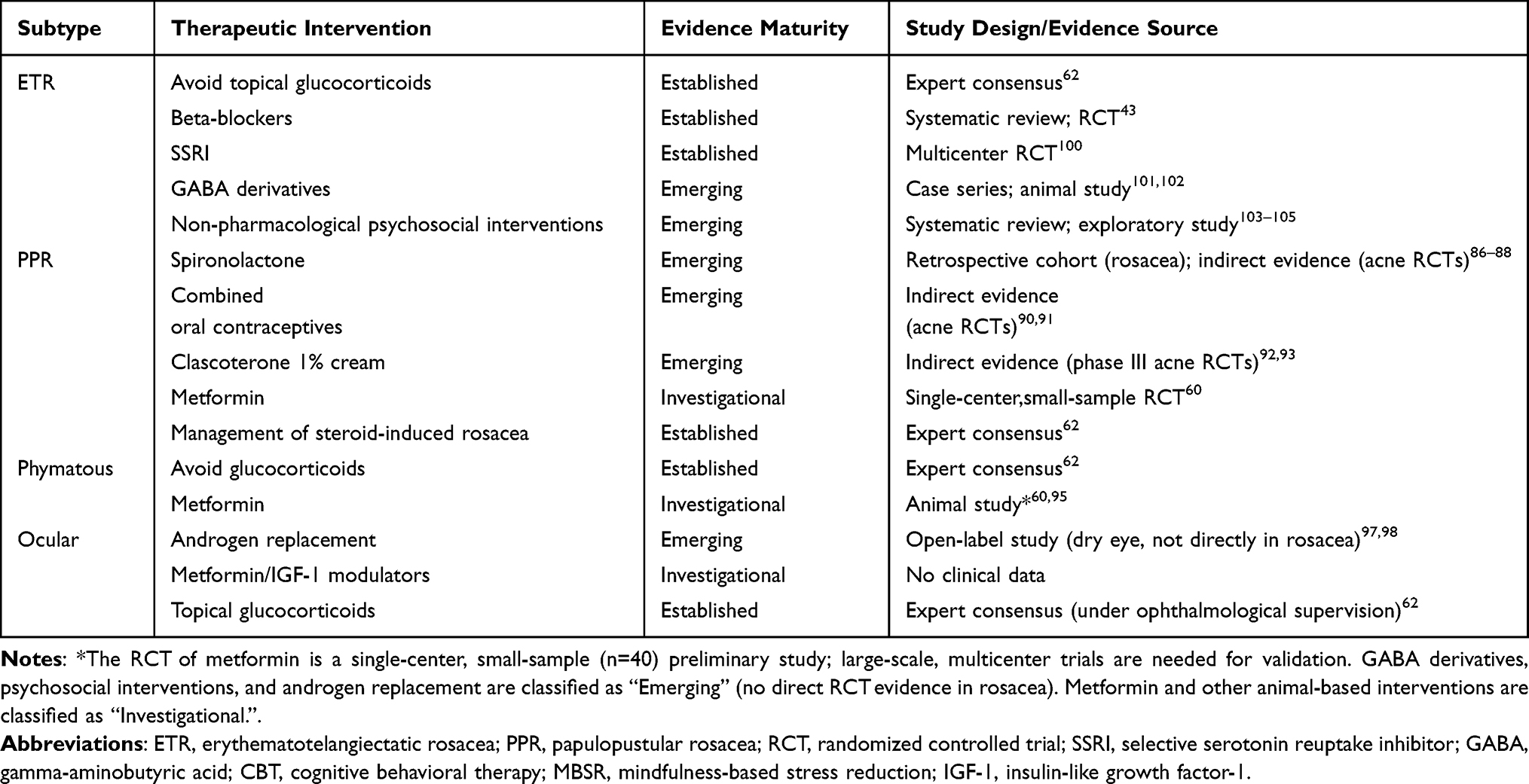 |
Table 2 Summary of Treatment Evidence for Rosacea by Subtype |
The use of glucocorticoids in ocular rosacea requires caution. Short-term, low-potency topical ophthalmic glucocorticoids may be used for severe acute exacerbations under the supervision of an ophthalmologist.35,62
Targeted Gut and Lifestyle Intervention
The prevalence of small intestinal bacterial overgrowth (SIBO) is elevated in patients with rosacea. Eradication of SIBO can improve facial skin lesion symptoms in affected patients.34 Probiotics, prebiotics, and dietary adjustment may be beneficial.27 High glycemic load and excessive dairy intake can increase serum IGF-1 levels.30,85 A low glycemic index diet with controlled dairy intake is recommended as an adjunctive measure.85 Avoiding known trigger factors such as sun exposure, high temperature, alcohol, spicy food, and emotional stress is a universally recommended measure.35 The use of sunscreen and mild skin care to maintain skin barrier integrity is essential.12,35
Neuropsychiatric and Neurovascular Intervention
Based on central sensitization and autonomic dysfunction, the central and autonomic nervous system play an important regulatory role in the pathogenesis of rosacea.70 Targeting the brain component of the skin-gut-brain axis, multiple interventions have demonstrated clinical efficacy.
Neurovascular Pharmacological Intervention
Beta-adrenergic blockers such as carvedilol and propranolol reduce facial flushing and persistent erythema.A systematic review including randomized controlled trials (RCTs) and open-label studies provided moderate-to-high-quality evidence for their efficacy in the erythematotelangiectatic subtype (ETR).43,44 In a randomized trial, carvedilol also improved anxiety and depression scores compared with topical brimonidine.43
Selective serotonin reuptake inhibitors (SSRIs) such as paroxetine exert dual effects on emotion and neurogenic inflammation.106 A multicenter RCT enrolling 97 patients with refractory erythema reported that paroxetine significantly improved clinical erythema assessments, flush success rates, and depression scores.100 The underlying mechanism may involve interactions between the serotonergic pathway and TRP channel activity and vascular tone.83 GABA derivatives inhibit the TRP channel pathway and reduce neuropeptide release. Clinical observations have demonstrated their efficacy in patients with ETR accompanied by severe burning sensation.101 A transcriptomics study confirmed that gabapentin suppresses neurogenic inflammation in rosacea via the NF-κB signaling pathway.102
Psychotherapy
Non-pharmacological psychotherapy approaches can serve as adjuncts to drug therapy. Cognitive behavioral therapy (CBT) is beneficial for patients with fear of blushing and social anxiety.103 An exploratory trial conducted in 14 patients with rosacea demonstrated that an 8-week mindfulness-based stress reduction (MBSR) program reduced blushing severity scores and improved depression, anxiety, and stigma scores.104 A systematic review concluded that CBT, mindfulness-based interventions, and habit reversal therapy are the most promising mind-body techniques in dermatology.105
Future Directions and Personalized Treatment
Personalized treatment requires comprehensive assessment of hormone status, particularly in female patients.58,59 Future large-scale randomized controlled trials should stratify patients by rosacea subtype and measure hormone-related biomarkers, including serum IGF-1, androgen/estrogen ratio, and fecal calprotectin.107 Biomarker-guided subtype classification will facilitate more precise selection of hormone-targeted or neuroimmunmodulatory therapies.108
Central sensitization is an emerging therapeutic target. Patients with refractory rosacea frequently exhibit neural hyperreactivity.Further exploration of central sensitization modulators, such as gabapentinoids and serotonin-norepinephrine reuptake inhibitors, holds promise for providing new strategies to break the vicious circle of neurogenic inflammation and flushing.69,77
High-quality clinical trials are urgently needed to validate the long-term efficacy and safety of hormone-targeted drugs specifically for rosacea. Currently, most evidence has been extrapolated from common acne or derived from preclinical studies.107 Establishing a clinical diagnosis and treatment pathway based on the skin-gut-brain axis represents a critical step toward precision medicine.18
Discussion
This study integrates the neuro-hormone-immune network within the skin-gut-brain axis framework to examine its role in the pathogenesis of rosacea. Stress hormones, sex hormones, and IGF-1 serve as messenger molecules linking the brain, gut, and skin, and their signaling pathways may collectively contribute to disease onset and the formation of clinical heterogeneity. This model suggests that the central nervous system may play an active regulatory role.18
Glucocorticoids induce CCL20 expression in keratinocytes.21 This mechanism provides a possible explanation for how psychological stress and ultraviolet irradiation trigger or exacerbate rosacea.6,45 Estrogen promotes barrier repair and downregulates innate immune responses.55 Androgens promote sebum secretion and enhance NLRP3 inflammasome activity.25,26 Hyperandrogenism disrupts gut microbiota structure and impairs the intestinal mucosal barrier,28 contributing to the maintenance of systemic low-grade inflammation and amplifying local skin injury,29 thereby forming a regulatory axis encompassing sex hormones, gut microbiota, intestinal barrier, and skin inflammation.27 IGF-1 participates in the regulation of sebum secretion, keratinocyte proliferation, and pro-inflammatory factor release via the PI3K/Akt/mTOR pathway,31,32 while also enhancing nerve ending sensitivity and influencing flushing symptoms.30 Based on evidence from acne research, IGF-1 may indirectly modulate androgen receptor signaling through the suppression of FoxO1.33 This mechanism remains to be confirmed in rosacea.Exogenous factors may disrupt hormone network homeostasis. Prolonged use of topical glucocorticoids contributes to the development of steroid-induced rosacea by impairing barrier function, suppressing local HPA axis-like activity, and exacerbating GR resistance.62 Sex hormone replacement therapy and environmental endocrine disruptors may influence disease course.53,64 The stratified combination therapy strategy offers a potential direction for rosacea treatment, shifting from local anti-inflammatory approaches toward systemic multi-target regulation.18 Hormone-targeted drugs exert therapeutic effects by modulating androgen signaling.92,109 Metformin exerts anti-inflammatory and anti-angiogenic effects by inhibiting the IGF-1-mediated metabolic-inflammatory cascade.61 Beta-blockers improve neurovascular-related symptoms by modulating autonomic nerve function.43,44 Personalized interventions targeting the three major axes of skin, gut, and central nervous system hold promise for improving therapeutic precision.110
Current research has certain limitations. Most key mechanisms are derived from in vitro or animal experiments95 and require further validation through in situ human studies. Clinical evidence for hormone-targeted drugs in the treatment of rosacea remains limited, with a lack of support from large-scale randomized controlled trials.107 Hormone detection methods have yet to be standardized, and the comparability of results needs improvement.4 The absence of specific biomarkers constrains the precision of disease assessment and prognostic evaluation.58 The association between thyroid hormone and other endocrine factors and rosacea remains unclear.7 Future research may conduct high-quality randomized controlled trials to evaluate the long-term efficacy and safety of hormone-targeted drugs,108 explore standardized biomarkers to achieve precision typing, investigate central sensitization mechanisms in greater depth,108 and establish clinical diagnosis and treatment pathways based on the skin-gut-brain axis.18
Conclusion
The integrative model of the neuro-hormone-immune network suggests that rosacea may be a systemic disease characterized by dysregulation of this network. Stress hormones, sex hormones, and IGF-1, as key messenger molecules, may be involved in central-peripheral signal transduction, sex-specific expression, and metabolic-inflammatory association, respectively.31 Glucocorticoids can induce CCL20 expression in keratinocytes.21 Gut-skin axis interaction associated with sex hormone imbalance27,28 and IGF-1-FoxO1-AR crosstalk31,33 may together constitute an important pathological basis for disease development.
Therapeutic strategies may shift from local anti-inflammatory approaches toward systemic multi-target regulation. Hormone-targeted drugs exert therapeutic effects by intervening in core signaling pathways.109 Beta-blockers improve neurovascular symptoms.43,44 Stratified management addressing skin inflammation, gut microbiota, and central hyperreactivity34,35 offers new directions for personalized treatment. Future research should conduct high-quality clinical research to evaluate the efficacy and safety of hormone-targeted drugs,107 explore hormone-related biomarkers to achieve precision typing,58 and further investigate central sensitization mechanisms and their therapeutic targets.108
Abbreviations
11β-HSD1, 11β-hydroxysteroid dehydrogenase type 1; Akt, protein kinase B; AR, androgen receptor; CBT, cognitive behavioral therapy; CCL20, C-C motif chemokine ligand 20; CGRP, calcitonin gene-related peptide; CNKI, China National Knowledge Infrastructure; CRH, corticotropin-releasing hormone; DHT, dihydrotestosterone; ETR, erythematotelangiectatic rosacea; FoxO1, forkhead box O1; GABA, gamma-aminobutyric acid; GPER1, G protein-coupled estrogen receptor 1; GR, glucocorticoid receptor; HPA, hypothalamic-pituitary-adrenal; IGF-1, insulin-like growth factor-1; IL-1β, interleukin-1 beta; MBSR, mindfulness-based stress reduction; MeSH, Medical Subject Headings; MSH, melanocyte-stimulating hormone; mTOR, mechanistic target of rapamycin; NF-κB, nuclear factor kappa-B; NGF, nerve growth factor; NLRP3, NOD-like receptor family pyrin domain containing 3; PI3K, phosphoinositide 3-kinase; POMC, pro-opiomelanocortin; PPR, papulopustular rosacea; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCT, randomized controlled trial; SIBO, small intestinal bacterial overgrowth; SP, substance P; SSRI, selective serotonin reuptake inhibitor; Th17, T helper 17; TLR2, Toll-like receptor 2; TRP, transient receptor potential; TrkA, tropomyosin receptor kinase A; UV, ultraviolet.
Data Sharing Statement
Not applicable, this manuscript does not report data generation or analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Supported by Fundamental Research Program Shanxi Province [grant numbers: 202303021211236].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fisher GW, Travers JB, Rohan CA. Rosacea pathogenesis and therapeutics: current treatments and a look at future targets. Front Med. 2023;10:1292722. doi:10.3389/fmed.2023.1292722
2. Hua NJ, Chen J, Geng RSQ, Sibbald RG, Sibbald C. Efficacy of treatments in reducing facial erythema in rosacea: a systematic review. J Cutan Med Surg. 2025;29(1):43–17. doi:10.1177/12034754241287546
3. Parisi R, Yiu ZZN. The worldwide epidemiology of rosacea. Br J Dermatol. 2018;179(2):239–240. doi:10.1111/bjd.16788
4. Gether L, Overgaard LK, Egeberg A, Thyssen JP. Incidence and prevalence of rosacea: a systematic review and meta-analysis. Br J Dermatol. 2018;179(2):282–289. doi:10.1111/bjd.16481
5. Sharifi S, Katamanin O, Jafferany M. Exploring the psychodermatologic burden and associated psychiatric manifestations in rosacea: a systemic review. Arch Dermatol Res. 2025;317(1):427. doi:10.1007/s00403-025-03982-w
6. Alzahrani NA, Almajed E, Alotaibi K, et al. Impact of rosacea on the quality of life: a population-based cross-sectional study in Saudi Arabia. Clin Cosmet Investig Dermatol. 2025;18:2079–2092. doi:10.2147/CCID.S543510
7. Geng RSQ, Bourkas AN, Mufti A, Sibbald RG. Rosacea: pathogenesis and therapeutic correlates. J Cutan Med Surg. 2024;28(2):178–189. doi:10.1177/12034754241229365
8. Tu KY, Jung CJ, Shih YH, Chang ALS. Therapeutic strategies focusing on immune dysregulation and neuroinflammation in rosacea. Front Immunol. 2024;15:1403798. doi:10.3389/fimmu.2024.1403798
9. Aedo G, Chahuán M, Gatica E, et al. Managing a burning face: clinical manifestations and therapeutic approaches for neurogenic rosacea. Int J Mol Sci. 2025;26(5):2366. doi:10.3390/ijms26052366
10. Long J, Deng Z, Chen M, Liu T. Impaired angiogenesis and Th1/Th17 polarization: a possible explanation for the decreased incidence of rosacea in the aged. Immun Inflamm Dis. 2024;12(12):e70108. doi:10.1002/iid3.70108
11. Ansari AW, Habib T, Ahmad F, et al. Cathelicidin LL-37-Induced transcriptome of human keratinocyte identifies chemokine CXCL10 link to T-Cell-Mediated rosacea pathogenesis through Jak1/STAT1 pathway. J Invest Dermatol. 2026;146(3):711–721.e6. doi:10.1016/j.jid.2025.08.003
12. Dajnoki Z, Kapitány A, Eyerich K, Eyerich S, Törőcsik D, Szegedi A. Topographical variations in the skin barrier and their role in disease pathogenesis. J Eur Acad Dermatol Venereol. 2025;39(7):1228–1238. doi:10.1111/jdv.20463
13. Chen LX, Hao PS. The role of skin barrier and immune abnormalities in the pathogenesis of Rosacea. Clin Exp Med. 2025;25(1):324. doi:10.1007/s10238-025-01859-w
14. Sun MD, Rieder EA. Psychosocial stress and mechanisms of skin health: a comprehensive update. J Drugs Dermatol. 2021;20(1):62–69. doi:10.36849/JDD.5608
15. Van Zuuren EJ, Arents BWM, Van der Linden MMD, Vermeulen S, Fedorowicz Z, Rosacea TJ. New concepts in classification and treatment. Am J Clin Dermatol. 2021;22(4):457–465. doi:10.1007/s40257-021-00595-7
16. Hawkins B, Montgomery M, Bokota G, Santoyo M, Giron E, Eltokhi A. Gut microbiota dysbiosis at the interface of neuropsychiatric disorders and their dermatological comorbidities. Gut Microbes. 2025;17(1):2574934. doi:10.1080/19490976.2025.2574934
17. Cryan JF, O’Riordan KJ, Cowan CSM, et al. The microbiota-gut-brain axis. Physiol Rev. 2019;99(4):1877–2013. doi:10.1152/physrev.00018.2018
18. Lazić Mosler E, Mužević M V, Karlović D, Tarle M, Raguž M. Revisiting rosacea through the skin-gut-brain axis: a neuroimmune perspective. Life. 2026;16(2):347. doi:10.3390/life16020347
19. Wienholtz NKF, Christensen CE, Ashina H, et al. Elevated plasma levels of calcitonin gene-related peptide in individuals with rosacea: a cross-sectional case-control study. J Eur Acad Dermatol Venereol. 2025;39(1):181–188. doi:10.1111/jdv.19954
20. Wu C, Zhang K, Guo Y, et al. Clinical characteristics and serum CGRP level differences between neurogenic rosacea and non-neurogenic rosacea. Int J Dermatol. 2025;64:42–51. doi:10.1111/ijd.70071
21. Wang L, Yang M, Wang X, et al. Glucocorticoids promote CCL20 expression in keratinocytes. Br J Dermatol. 2021;185(6):1200–1208. doi:10.1111/bjd.20594
22. Xu D, Wu Y. Ectoin attenuates cortisone-induced skin issues by suppression GR signaling and the UVB-induced overexpression of 11β-HSD1. J Cosmet Dermatol. 2024;23(12):4303–4314. doi:10.1111/jocd.16516
23. Zhang H, Wang M, Zhao X, Wang Y, Chen X, Su J. Role of stress in skin diseases: a neuroendocrine-immune interaction view. Brain Behav Immun. 2024;116:286–302. doi:10.1016/j.bbi.2023.12.005
24. Qing Y, Wu J, Xu B, et al. DNAJB2 attenuates rosacea skin inflammation and angiogenesis by inhibiting the endoplasmic reticulum stress-mediated TLR2/Myd88/NF-κB pathway. Inflammation. 2025;48(5):3472–3486. doi:10.1007/s10753-025-02278-5
25. Del Rosso JQ, Kircik L. The cutaneous effects of androgens and androgen-mediated sebum production and their pathophysiologic and therapeutic importance in acne vulgaris. J Dermatolog Treat. 2024;35(1):2298878. doi:10.1080/09546634.2023.2298878
26. Li Y, Deng N, Luo X, et al. Unveiling estrogen’s role: a comprehensive review of its impact on skin health and disease. Apoptosis. 2026;31(1):34. doi:10.1007/s10495-025-02244-4
27. Tang J, Chen P, Huang C, et al. 17β-Estradiol promotes LL37-induced rosacea-like skin inflammation via G protein-coupled estrogen receptor 30. J Dermatol Sci. 2025;119(3):101–111. doi:10.1016/j.jdermsci.2025.05.005
28. Çerman A A, Aktaş Karabay E, Kaya HE, et al. Evaluation of fecal calprotectin as a marker of gastrointestinal inflammation in rosacea: a case-control study. Dermatol Ther. 2021;34(3):e14946. doi:10.1111/dth.14946
29. Santos-Marcos JA, Mora-Ortiz M, Tena-Sempere M, Lopez-Miranda J, Camargo A. Interaction between gut microbiota and sex hormones and their relation to sexual dimorphism in metabolic diseases. Biol Sex Differ. 2023;14(1):4. doi:10.1186/s13293-023-00490-2
30. Andrusiewicz A, Khimuk S, Mijas D, Shmorhun B, Nowicka D. Molecular mechanisms in the etiopathology of rosacea-systematic review. Int J Mol Sci. 2025;26(23):11292. doi:10.3390/ijms262311292
31. Fan M, Lai Y, Fan X, et al. Potential role of insulin-like growth factor 1 and growth hormone in acneiform eruptions: evidence from a rat model of acromegaly. J Endocrinol Invest. 2026;49(1):55–68. doi:10.1007/s40618-025-02692-4
32. Chen B, Wu C, Liao Y, et al. Bioinformatic analysis and experimental validation implicate STAT2-mediated angiogenic responses in rosacea pathogenesis. Arch Dermatol Res. 2025;317(1):398. doi:10.1007/s00403-025-03915-7
33. Guertler A, Volsky A, Eijkenboom Q, Fiedler T, French LE, Reinholz M. Dietary patterns in acne and rosacea patients-a controlled study and comprehensive analysis. Nutrients. 2023;15(20):4405. doi:10.3390/nu15204405
34. Sánchez-Pellicer P, Eguren-Michelena C, García-Gavín J, et al. Rosacea, microbiome and probiotics: the gut-skin axis. Front Microbiol. 2024;14:1323644. doi:10.3389/fmicb.2023.1323644
35. Thiboutot D, Anderson R, Cook-Bolden F, et al. Standard management options for rosacea: the 2019 update by the National Rosacea Society Expert Committee. J Am Acad Dermatol. 2020;82(6):1501–1510. doi:10.1016/j.jaad.2020.01.077
36. Kong L, Liang X, Liu A, et al. Icariin inhibits inflammation via immunomodulation of the cutaneous hypothalamus-pituitary-adrenal axis in vitro. Clin Exp Dermatol. 2019;44(2):144–152. doi:10.1111/ced.13735
37. Saric-Bosanac S, Clark AK, Sivamani RK, Shi VY. The role of hypothalamus-pituitary-adrenal (HPA)-like axis in inflammatory pilosebaceous disorders. Dermatol Online J. 2020;26(2):
38. Kim BJ, Lee NR, Lee CH, et al. Increased expression of 11β-Hydroxysteroid dehydrogenase type 1 contributes to epidermal permeability barrier dysfunction in aged skin. Int J Mol Sci. 2021;22(11):5750. doi:10.3390/ijms22115750
39. Slominski RM, Chen JY, Raman C, Slominski AT. Photo-neuro-immuno-endocrinology: how the ultraviolet radiation regulates the body, brain, and immune system. Proc Natl Acad Sci U S A. 2024;121(14):e2308374121. doi:10.1073/pnas.2308374121
40. Li Q, Chan H. Vitamin D and skin disorders: bridging molecular insights to clinical innovations. Mol Med. 2025;31(1):259. doi:10.1186/s10020-025-01311-5
41. Li J, Wei J, Zhang M, et al. Transcutaneous auricular vagus nerve stimulation treatment for erythematotelangiectatic rosacea: a randomized clinical trial. JAMA Dermatol. 2025;161(12):1229–1237. doi:10.1001/jamadermatol.2025.3796
42. Han Y, Wang B, Gao H, et al. Vagus nerve and underlying impact on the gut microbiota-brain axis in behavior and neurodegenerative diseases. J Inflamm Res. 2022;15:6213–6230. doi:10.2147/JIR.S384949
43. Li J, Tang JY, Fu J, et al. Carvedilol ameliorates persistent erythema of erythematotelangiectatic rosacea by regulating the status of anxiety/depression. J Dermatol. 2022;49(11):1139–1147. doi:10.1111/1346-8138.16525
44. Alhazmi AM, Basendwh MA, Aman AA, Dajam M, Aljuhani TS. The role of systemic and topical beta-blockers in dermatology: a systematic review. Dermatol Ther. 2023;13(1):29–49. doi:10.1007/s13555-022-00848-1
45. Wei R, Wang X, Lei W, Yang J, Feng Y. Patients with rosacea exhibit lower minimal erythema doses to both UVA and UVB. Photodermatol Photoimmunol Photomed. 2025;41(3):e70019. doi:10.1111/phpp.70019
46. Mellett M, Danis J, Meier-Schiesser B. Editorial: impact of the innate and adaptive immune system in driving type 1 inflammatory skin disease. Front Immunol. 2025;16:1568773. doi:10.3389/fimmu.2025.1568773
47. Kim TM, Cho S. Clinical and laboratory differences between steroid-associated and non-steroid-associated rosacea: a retrospective study. Acta Derm Venereol. 2024;104:adv40045. doi:10.2340/actadv.v104.40045
48. Murakami K, Sawada A, Mori T, Sakuyama S, Tokudome Y. Effect of estrogen/progesterone ratio on the differentiation and the barrier function of epidermal keratinocyte and three-dimensional cultured human epidermis. Life Sci. 2022;293:120356. doi:10.1016/j.lfs.2022.120356
49. Xiao T, Sun M, Zhao C, Kang J. TRPV1: a promising therapeutic target for skin aging and inflammatory skin diseases. Front Pharmacol. 2023;14:1037925. doi:10.3389/fphar.2023.1037925
50. Rivera-Mancilla E, Al-Hassany L, Marynissen H, et al. Functional analysis of TRPA1, TRPM3, and TRPV1 channels in human dermal arteries and their role in vascular modulation. Pharmaceuticals. 2024;17(2):156. doi:10.3390/ph17020156
51. Li J, Mao B, Tang X, et al. Endocrine and metabolic drivers of sebum dysregulation: mechanisms and therapeutic strategies. Life Sci. 2025;383:124044. doi:10.1016/j.lfs.2025.124044
52. Yin X, Yan Y, Li J, et al. Nuclear receptors for epidermal lipid barrier: advances in mechanisms and applications. Exp Dermatol. 2024;33(6):e15107. doi:10.1111/exd.15107
53. Demircioglu D, Cinar N, Pektas SD, Edgunlu T, Unal M, Yazgan Aksoy D. Bisphenol-A and pentachlorophenol sodium levels in patients with rosacea. Cutan Ocul Toxicol. 2024;43(3):232–236. doi:10.1080/15569527.2024.2383242
54. Rao A, Douglas SC, Hall JM. Endocrine disrupting chemicals, hormone receptors, and acne vulgaris: a connecting hypothesis. Cells. 2021;10(6):1439. doi:10.3390/cells10061439
55. Wu WH, Geng H, Cho E, et al. Reproductive and hormonal factors and risk of incident rosacea among US White women. J Am Acad Dermatol. 2022;87(1):138–140. doi:10.1016/j.jaad.2021.06.865
56. Benedetti G, Shao C, Velasco R, et al. Rosacea changes during pregnancy: a single-center retrospective survey study. Int J Womens Dermatol. 2023;9(4):e113. doi:10.1097/JW9.0000000000000113
57. Bettolini L, Perantoni M, Mezzana S, et al. A case of rosacea fulminans during pregnancy. J Dtsch Dermatol Ges. 2023;21(11):1399–1403. doi:10.1111/ddg.15193
58. Roster K, Fleshner L, Karatas TB, et al. Menopause and common dermatoses: a systematic review. Am J Clin Dermatol. 2026;27(1):67–84. doi:10.1007/s40257-025-00994-0
59. Arza A, Stitzlein E, Gupta M, Ilyas EN. Incidence of rosacea associated with hormonal intrauterine devices: a comparative study with nonhormonal intrauterine devices. J Am Acad Dermatol. 2025;92(2):351–352. doi:10.1016/j.jaad.2024.10.029
60. Li Y, Yang L, Wang Y, et al. Exploring metformin as a candidate drug for rosacea through network pharmacology and experimental validation. Pharmacol Res. 2021;174:105971. doi:10.1016/j.phrs.2021.105971
61. Pantazopoulos D, Papachristou S, Gouveri E, Papi M, Papazoglou D, Papanas N. Metformin: old drug, new therapeutic potential in the skin? A brief narrative review. Adv Ther. 2025;42(8):3606–3620. doi:10.1007/s12325-025-03256-x
62. Burshtein J, Chovatiya R, Golant A, et al. Risks of topical corticosteroid therapy and role for advanced targeted topical treatments for inflammatory skin diseases: an expert consensus panel. Dermatol Online J. 2025;31(1):. doi:10.5070/D331164978
63. Rijal H, Geng R, Wilken B, Slomovic J, Sibbald C. Drug-Induced rosacea: a systematic review. J Cutan Med Surg. 2024;28(5):496–497. doi:10.1177/12034754241265719
64. Williams NM, Randolph M, Rajabi-Estarabadi A, Keri J, Tosti A. Hormonal contraceptives and dermatology. Am J Clin Dermatol. 2021;22(1):69–80. doi:10.1007/s40257-020-00557-5
65. Girnita A, Bjerring P, Llado Grove G, et al. INDIVIDUAL ARTICLE: a practical algorithm for the prevention and treatment of cutaneous side effects of hormonal cancer therapy. J Drugs Dermatol. 2025;24(5):49631s3–49631s10. doi:10.36849/JDD.49631
66. Petrut SM, Bragaru AM, Munteanu AE, Moldovan AD, Moldovan CA, Rusu E. Gut over mind: exploring the powerful gut-brain axis. Nutrients. 2025;17(5):842. doi:10.3390/nu17050842
67. Curatolo M. Central sensitization and pain: pathophysiologic and clinical insights. Curr Neuropharmacol. 2024;22(1):15–22. doi:10.2174/1570159X20666221012112725
68. Song D, Jiang P, Tang Y, et al. Exploring the neural basis of rosacea: altered brain activity and its links with social anxiety. Clin Exp Dermatol. 2025;50(10):2022–2029. doi:10.1093/ced/llaf291
69. Raguž M, Tarle M, Hat K, et al. Refractory neuropathic pain in the head and neck: neuroanatomical and clinical significance of the cervicotrigeminal complex. Life. 2025;15(9):1457. doi:10.3390/life15091457
70. Abdi P, Haq Z, Diaz MJ, Maibach HI. Psychiatric comorbidities associated with rosacea: a propensity score-matched case-control study in the All of Us database. Clin Exp Dermatol. 2024;49(4):400–403. doi:10.1093/ced/llad417
71. Chen C, Wang P, Zhang L, et al. Exploring the pathogenesis and mechanism-targeted treatments of rosacea: previous understanding and updates. Biomedicines. 2023;11(8):2153. doi:10.3390/biomedicines11082153
72. Slominski RM, Raman C, Jetten AM, Slominski AT. Neuro-immuno-endocrinology of the skin: how environment regulates body homeostasis. Nat Rev Endocrinol. 2025;21(8):495–509. doi:10.1038/s41574-025-01107-x
73. Pérez-Escudero N, Cabas I, Corbalán-Vélez R, et al. GPER1 reduces skin inflammation by inhibiting keratinocyte proliferation. Cell Death Discov. 2026;12(1):166. doi:10.1038/s41420-026-03059-1
74. Arterburn JB, Prossnitz ER. G protein-coupled estrogen receptor GPER: molecular pharmacology and therapeutic applications. Annu Rev Pharmacol Toxicol. 2023;63:295–320. doi:10.1146/annurev-pharmtox-031122-121944
75. Lee SG, Kim J, Lee YI, et al. Cutaneous neurogenic inflammation mediated by TRPV1-NGF-TRKA pathway activation in rosacea is exacerbated by the presence of Demodex mites. J Eur Acad Dermatol Venereol. 2023;37(12):2589–2600. doi:10.1111/jdv.19449
76. Yu Y, Su R, Wang W, et al. A stress-responsive neurovascular axis shapes skin immune accessibility. iScience. 2026;29(3):115122. doi:10.1016/j.isci.2026.115122
77. Yang F, Wang L, Song D, et al. Signaling pathways and targeted therapy for rosacea. Front Immunol. 2024;15:1367994. doi:10.3389/fimmu.2024.1367994
78. Xu N, Chen Y, Guo D, et al. Rhein promotes the proliferation of keratinocytes by targeting oestrogen receptors for skin ulcer treatment. BMC Complement Med Ther. 2022;22(1):209. doi:10.1186/s12906-022-03691-1
79. Kendall AC, Pilkington SM, Wray JR, et al. Menopause induces changes to the stratum corneum ceramide profile, which are prevented by hormone replacement therapy. Sci Rep. 2022;12(1):21715. doi:10.1038/s41598-022-26095-0
80. Zomer HD, Cooke PS. Targeting estrogen signaling and biosynthesis for aged skin repair. Front Physiol. 2023;14:1281071. doi:10.3389/fphys.2023.1281071
81. Liang L, Qi X, Jiang X, Chen T, Dong L. Lactobacillus plantarum MH-301 as an effective adjuvant to isotretinoin in the treatment of acne vulgaris: a randomized and open-label trail. Front Med. 2024;10:1340068. doi:10.3389/fmed.2023.1340068
82. Li X, Cheng W, Shang H, Wei H, Deng C. The interplay between androgen and gut microbiota: is there a microbiota-gut-testis axis. Reprod Sci. 2022;29(6):1674–1684. doi:10.1007/s43032-021-00624-0
83. Ivanic MG, Oulee A, Norden A, Javadi SS, Gold MH, Wu JJ. Treatment of neurogenic rosacea: a literature review. J Drugs Dermatol. 2023;22(6):566–575. doi:10.36849/JDD.7181
84. Grafanaki K, Bakoli Sgourou D, Maniatis A, Pasmatzi E. The exposomal imprint on rosacea: more than skin deep. J Eur Acad Dermatol Venereol. 2026;40(3):387–403. doi:10.1111/jdv.70112
85. Rahaman SMA, De D, Handa S, et al. Association of insulin-like growth factor (IGF)-1 gene polymorphisms with plasma levels of IGF-1 and acne severity. J Am Acad Dermatol. 2016;75(4):768–773. doi:10.1016/j.jaad.2016.05.019
86. Searle TN, Al-Niaimi F, Ali FR. Spironolactone in dermatology: uses in acne and beyond. Clin Exp Dermatol. 2020;45(8):986–993. doi:10.1111/ced.14340
87. Kow CS, Ramachandram DS, Hasan SS, Thiruchelvam K. Spironolactone for the treatment of moderate to severe acne in adult women: a systematic review and meta-analysis of randomised controlled trials. Australas J Dermatol. 2025;66(3):165–168. doi:10.1111/ajd.14428
88. Elhesaisy NA, Swidan SA, Tawfiq RA, El-Nabarawi MA, Teaima MH. Fabrication and characterization of anti-rosacea 3D nanofibrous customized sheet masks as a novel scaffold for repurposed use of spironolactone with pre-clinical studies. Int J Pharm. 2023;636:122816. doi:10.1016/j.ijpharm.2023.122816
89. Dereiah S, Ghori MU, Conway BR. A systematic review of spironolactone nano-formulations for topical treatment of skin hyperandrogenic disorders and chronic wounds. Pharmaceutics. 2024;17(1):27. doi:10.3390/pharmaceutics17010027
90. Tommasino N, Annunziata MC, Potestio L, Napolitano M. Efficacy and safety of hormonal therapies for acne: a narrative review. Clin Cosmet Investig Dermatol. 2025;18:3331–3337. doi:10.2147/CCID.S574341
91. Clayton RW, Langan EA, Ansell DM, et al. Neuroendocrinology and neurobiology of sebaceous glands. Biol Rev Camb Philos Soc. 2020;95(3):592–624. doi:10.1111/brv.12579
92. Choi U, Xiong G, Metko D, et al. Efficacy of oral isotretinoin monotherapy compared to combination isotretinoin and topical clascoterone for severe acne vulgaris: a multi-center retrospective study. J Dermatolog Treat. 2025;36(1):2525287. doi:10.1080/09546634.2025.2525287
93. Hebert A, Eichenfield L, Thiboutot D, et al. Efficacy and safety of 1% clascoterone cream in patients Aged > 12 years with acne vulgaris. J Drugs Dermatol. 2023;22(2):174–181. doi:10.36849/JDD.7000
94. Cho M, Woo YR, Cho SH, Lee JD, Kim HS. Metformin: a potential treatment for acne, hidradenitis suppurativa and rosacea. Acta Derm Venereol. 2023;103:adv18392. doi:10.2340/actadv.v103.18392
95. Yoon SH, Hwang I, Lee E, et al. Antimicrobial peptide LL-37 drives rosacea-like skin inflammation in an NLRP3-Dependent manner. J Invest Dermatol. 2021;141(12):2885–2894.e5. doi:10.1016/j.jid.2021.02.745
96. Wang LX, Deng YP. Androgen and meibomian gland dysfunction: from basic molecular biology to clinical applications. Int J Ophthalmol. 2021;14(6):915–922. doi:10.18240/ijo.2021.06.18
97. Jiang JR, Khankan R, Ridder WH, Nguyen AL, Paugh JR. A pilot randomized controlled trial of topical androgen treatment in dry eye. Ocul Surf. 2025;38:56–63. doi:10.1016/j.jtos.2025.06.002
98. Wang L, Deng Y. The applications of androgen in the treatment of dry eye disease: a systematic review of clinical studies. Endocr J. 2020;67(9):893–902. doi:10.1507/endocrj.EJ20-0178
99. Avraham S, Khaslavsky S, Kashetsky N, et al. Treatment of ocular rosacea: a systematic review. J Dtsch Dermatol Ges. 2024;22(2):167–174. doi:10.1111/ddg.15290
100. Wang B, Huang Y, Tang Y, et al. Paroxetine is an effective treatment for refractory erythema of rosacea: first results from a prospective randomized clinical trial of refractory erythema of rosacea. J Am Acad Dermatol. 2023;88(6):1300–1307. doi:10.1016/j.jaad.2023.01.044
101. Li D, Yang W, Chen N, Xu Y. Advances in gamma-aminobutyric acid derivatives for the treatment of rosacea. Clin Cosmet Investig Dermatol. 2025;18:2207–2214. doi:10.2147/CCID.S550614
102. Jiang Z, Ding T, Zhao Y, et al. Transcriptomic and metabolomic study of gabapentin in the treatment of neurogenic inflammation in rosacea. Commun Biol. 2026;9(1):430. doi:10.1038/s42003-026-09662-3
103. Mar K, Rivers JK. The mind-skin connection in patients with dermatologic diseases: a literature review. J Cutan Med Surg. 2023;27(6):628–640. doi:10.1177/12034754231204295
104. Song D, Jiang X. PS06 Mindfulness-based stress reduction reduces blushing and negative emotions in patients with rosacea: an exploratory study. Br J Dermatol. 2024;191(Suppl 1):i178. doi:10.1093/bjd/ljae090.377
105. Rafidi B, Kondapi K, Beestrum M, Basra S, Lio P. A systematic review of psychotherapeutic and psychosomatic techniques in the treatment of dermatological diseases. J Clin Dermatol. 2022;23(6):755–773. doi:10.1007/s40257-022-00714-y
106. Dionisie V, Filip GA, Manea MC, Manea M, Riga S. The anti-inflammatory role of SSRI and SNRI in the treatment of depression: a review of human and rodent research studies. Inflammopharmacology. 2021;29(1):75–90. doi:10.1007/s10787-020-00777-5
107. Li S, Lin J, Li J, Mo X, Ju Q. Therapeutic landscape of rosacea: from clinical trials to future directions. J Cosmet Dermatol. 2025;24(5):e70182. doi:10.1111/jocd.70182
108. Moran SK, Wong SC, Taylor SL, Feldman SR. Early investigational agents for the treatment of rosacea: drugs in phase I and II clinical development. Expert Opin Investig Drugs. 2025;34(1–2):27–36. doi:10.1080/13543784.2025.2463093
109. Smith CA, Gosnell E, Karatas TB, Deitelzweig C, Collins EMB, Yeung H. Hormonal therapies for acne: a comprehensive update for dermatologists. Dermatol Ther. 2025;15(1):45–59. doi:10.1007/s13555-024-01324-8
110. Chang HC, Huang YC, Lien YJ, Chang YS. Association of rosacea with depression and anxiety: a systematic review and meta-analysis. J Affect Disord. 2022;299:239–245. doi:10.1016/j.jad.2021.12.008
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.