Back to Journals » Eye and Brain » Volume 12
Neurofibromatosis Type 1: Ocular Electrophysiological and Perimetric Anomalies
Authors Nebbioso M ![]() , Moramarco A, Lambiase A
, Moramarco A, Lambiase A ![]() , Giustini S
, Giustini S ![]() , Marenco M
, Marenco M ![]() , Miraglia E, Fino P, Iacovino C, Alisi L
, Miraglia E, Fino P, Iacovino C, Alisi L ![]()
Received 24 March 2020
Accepted for publication 14 August 2020
Published 21 October 2020 Volume 2020:12 Pages 119—127
DOI https://doi.org/10.2147/EB.S255184
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Margaret Wong-Riley
Marcella Nebbioso,1,* Antonietta Moramarco,1,* Alessandro Lambiase,1 Sandra Giustini,2 Marco Marenco,1 Emanuele Miraglia,2 Pasquale Fino,2 Chiara Iacovino,2 Ludovico Alisi1
1Department of Sense Organs, Sapienza University of Rome, Rome, Italy; 2Department of Dermatology, Sapienza University of Rome, Rome, Italy
*These authors contributed equally to this work
Correspondence: Alessandro Lambiase
Department of Sense Organs, Sapienza University of Rome, Viale del Policlinico 155, Rome 00161, Italy
Tel +390649975357
Fax +390649975425
Email [email protected]
Introduction: Neurofibromatosis type 1 (NF1) is a multisystemic disease caused by the mutation of Nf1 gene located on chromosome 17q11.2. The mutation determines the loss of function of the protein neurofibromin with consequent uncontrolled cellular proliferation. Patients are characterized by a wide range of dermatological, neurological, and ophthalmological symptoms.
Purpose: The aim of the study was to evaluate, through pattern visual evoked potentials (p-VEPs) and frequency doubling technology (FDT) Matrix perimetry, the objective and psychophysical functionality of the optic pathways in a group of NF1 patient.
Methods: The study group consisted of 26 patients affected by NF1 and 17 healthy controls. Each patient underwent a complete ophthalmological examination, p-VEPs with the evaluation of amplitude and latency of the P100 wave, and FDT perimetry, with the evaluation of central sensitivity (CS), mean deviation (MD), pattern standard deviation (PSD) and glaucoma hemifield test (GHT).
Results: NF1 patients showed a statistically significant alteration in the transmission of visual impulse. P-VEPs results highlighted a reduced amplitude and an increased latency of the P100 wave, suggesting an involvement of the visual pathway. Visual field analysis showed a significant reduction in all the observed parameters as well (CS, MD, PSD, and GHT).
Conclusion: The present study showed, in NF1 patients, a qualitative and quantitative alteration in the conduction of stimuli through the visual pathways. The observed alterations are present, although, only at a subclinical level. None of the patients included in the study showed any manifest visual deficit nor had any concomitant pathology that might have affected the outcome of the study. In conclusion, electrophysiological exams and computer perimetry may take part, alongside a wider array of exams, in the differential diagnosis and later monitoring of NF1.
Keywords: electrophysiologic testing, frequency doubling technology Matrix perimetry, FDT, neurofibromatosis type 1, optic glioma, pattern visual evoked potentials
Introduction
Neurofibromatosis type 1 (NF1) also known as the von Recklinghausen disease is one of the most common hereditary diseases, with an estimated prevalence of 1/3000.1 The disease is characterized by a wide spectrum of ophthalmological manifestations. Specifically, Lisch’s nodules (iris hamartomas) are included as one of the main diagnostic criteria for NF1. Choroidal nodules, retinal vascular abnormalities,2–4 cutaneous café-au-lait spots, and neurofibromas are some of the other clinical features.5 NF1 patients, also show the development of optic nerve gliomas, breast cancer and leukemia6 as well as frequent cognitive deficits and behavioral abnormalities.7
From a genetic point of view, NF1 is determined by the inactivation of the tumor suppressor gene NF1 which encodes the protein neurofibromin. This mechanism is responsible for the activation of the RAS protein pattern that determines a significant increase in cellular growth and survival, leading to the development of neoplasm and other clinical features.8
In NF1 patients, alterations were observed in the diffusion tensor images (DTI) acquired with magnetic resonance, suggesting an involvement of the Nf1 gene in myelination processes.9,10 It has been hypothesized, that the loss of function of the Nf1 gene may determine the inhibition of myelin production by mature oligodendrocytes and a progressive decompaction of the myelin itself, particularly at the level of the optic nerve.11 These processes, through molecular mechanisms not yet fully known, could be the cause of some of the organic and cognitive alterations in NF1 patients.11 Numerous alterations have been reported in NF1 patients. Koini et al demonstrated that in the anterior thalamic radiations, microscopic white matter alterations may be responsible for the development of behavioral abnormalities.12 Common findings in NF1 are the unidentified bright objects (UBOs), probably determined by intramyelinic edema.13 Numerous works have highlighted the importance of UBOs in the development of cognitive and behavioral anomalies in NF1 patients. Nevertheless, to this day, no universal consensus has been reached on the role of UBOs.14 Visual pathways are not exempted from the generalized involvement of the central nervous system in NF1. Numerous studies report a consistent visuospatial impairment with a substantial impact on the quality of life.15 Violante et al demonstrated that NF1 patients are characterized by a deficient visual cortex activation. This functional MRI study demonstrated low-level visual processing deficits that do not tend to ameliorate with the age.16
The objective of our study was to examine the function of retrobulbar visual pathways in patients with NF1, comparing it with a group of healthy subjects. In detail, we aimed to evaluate the integrity of nerve stimulus transmission in NF1 patients without evident active neoplasms or any other manifest pathology at the level of the optical pathways. We, therefore, conducted two specific instrumental examinations on all subjects: pattern visual evoked potentials (p-VEPs) and frequency-doubling technology (FDT) campimetry.
Materials and Methods
In our observational study, 26 patients (52 eyes) with NF1 followed at the Sapienza University of Rome, and 17 healthy controls (34 eyes) were recruited between October 2017 and December 2018. The two groups were homogeneous for age, sex, and race.
Informed consent was obtained from all subjects. The study protocol was approved by the Ethics Committee of the University of Rome “Sapienza”. The research followed the tenets of the Declaration of Helsinki.
Patients were diagnosed with NF1 according to the 1988 National Institute of Health (NIH) clinical criteria.17
The exclusion criteria were:
- Best-corrected visual acuity (BCVA) measured by early treatment diabetic retinopathy study (ETDRS) charts at 4 meters in logarithm of the minimum angle of resolution (logMAR) less than 0.0 logMAR in each eye;
- Refractive defects greater than ±4 diopters (spherical equivalent);
- Presence of ophthalmic, systemic and neurological pathologies that could alter transmission or visual perception (eg glaucoma, cataract, uveitis, retinal dystrophy, optic nerve gliomas or other brain neoplasms);
- Poor collaboration, which prevented the correct execution of diagnostic tests.
All patients involved in the study underwent a dermatological examination, to identify cutaneous signs indicative of NF1, and a neurological examination with 1.5 Tesla magnetic resonance imaging (MRI) of the brain and spinal cord with contrast, to assess the integrity of the retrobulbar visual pathways and the absence of coexisting intracranial pathologies. MRI was performed with multiplanar sequences, T1, T2 weighted, FLAIR, DWI, and FSPGR post-contrast multiplanar imaging. Spine exam was performed directly after contrast with multiplanar sequences FS T1 and T2 weighted.
Patients underwent eye examination including measurement of BCVA, intraocular pressure, anterior segment biomicroscopy, and mydriatic indirect fundus biomicroscopy.
The study of bioelectric conduction of visual pathways was carried out following standard ISCEV parameters employing p-VEPs.18 The exam was performed using a reversal type pattern stimulus with a spatial frequency of 120’, 60ʹ, and 15ʹ (MONPAK3 METROVISION Pérenchies France). Each eye was examined separately with an active electrode placed on the scalp at 3.5 cm above the inion. The latency and amplitude values of the P100 wave, obtained for each spatial stimulation frequency in NF1 patients, were compared with the values obtained in the control group.
The study of the visual field was carried out by means of a computerized FDT perimeter (Welch Allyn, Skaneateles, NY, Zeiss Humphrey, San Leonardo, CA). The perimeter indices taken into consideration were: Central Sensitivity (CS), Mean Deviation (MD), Pattern Standard Deviation (PSD) and Glaucoma Hemifield Test (GHT). An average on both eyes has been calculated for every parameter. The overall assessment of the visual field was carried out taking into consideration the reliability and collaboration of the patient, excluding subjects who had poor reliability (more than 20% fixation losses, false negative or false positive responses).
To avoid the learning effect only the third exam was taken into consideration for the statistical analysis (Figure 1).
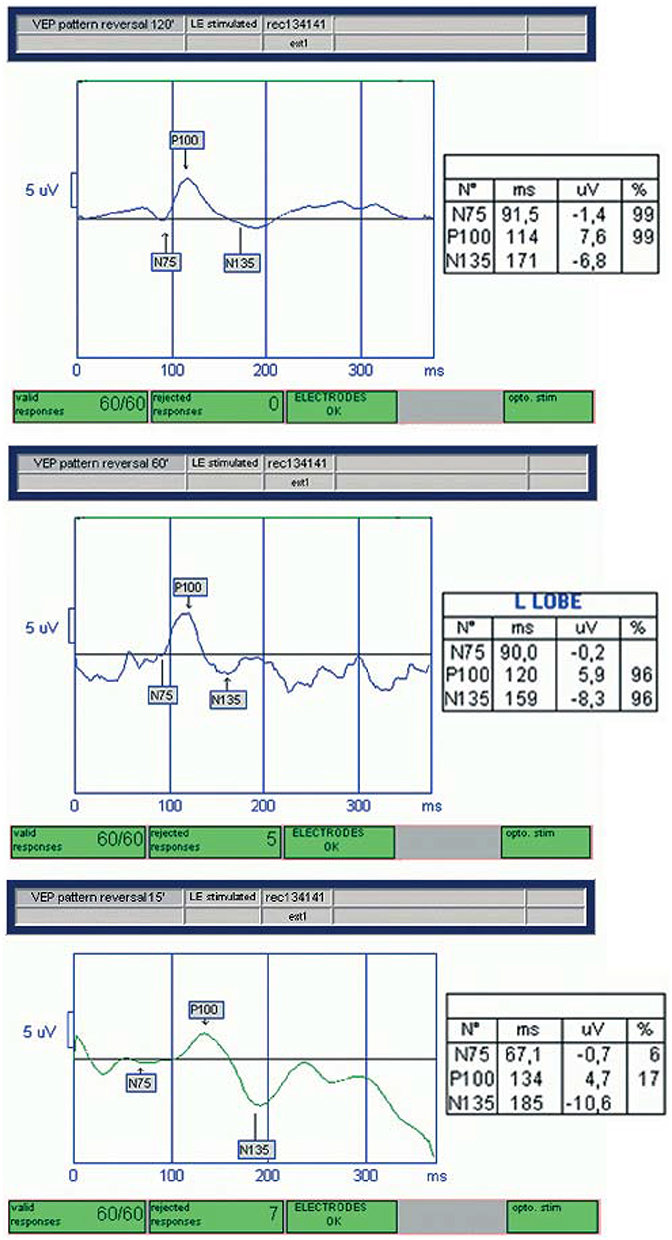 |
Figure 1 Neurofibromatosis type 1 (NF1) patient. Pattern visual evoked potentials (p-VEPs): Latency (increased) and amplitude (reduced) values of the P100 waves, obtained for each spatial stimulation frequency (120ʹ, 60ʹ, and 15ʹ). |
Each parameter obtained in patients with NF1 was compared with the results of the control group.
Statistical Analysis
Descriptive statistical analysis was performed considering all collected data. For each quantitative variable, mean, standard deviation, and median were calculated; for each categorical variable numerosity and percentage were calculated instead.
The chi-square test was used to evaluate the relationship between the two groups and the categorical variables.
Student’s T-test for independent data was used to compare the parameters between the two groups. Linear regression was applied to test the potential correlation between age and perimetric or electrophysiological findings. Student’s T-test was also applied to compare differences between males and females in the NF1 group.
A p-value <0.05 was considered statistically significant. All analyzes were performed with STATA 14.1.
Results
The study collected data from 43 recruited subjects; the sample of patients with NF1 was represented by 10 males and 16 females (n = 26) of average age 37 years (range 17 to 60 yo; sd ± 12.9); the healthy controls were represented by 5 males and 12 females (n = 17) of average age 41 years (range 14 to 72 yo; sd ± 18.1).
Table 1 shows the mean and median values for each spatial stimulation frequency (120ʹ, 60ʹ, and 15ʹ) of the amplitude and latency of the P100 wave and the results of the parametric (p) tests.
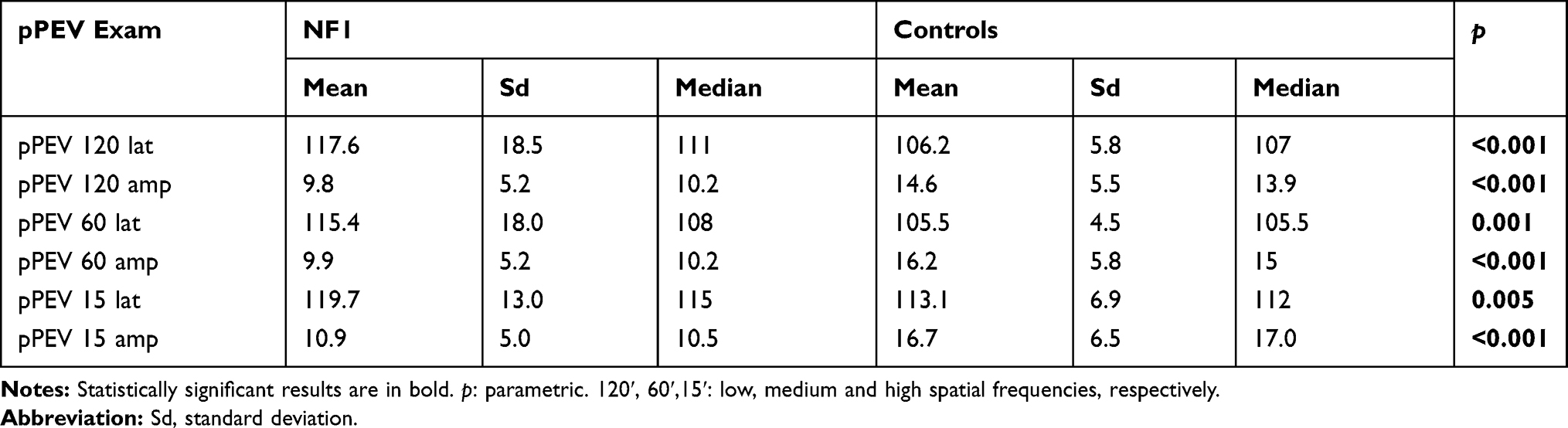 |
Table 1 Pattern Visual Evoked Potentials (pVEPs) Amplitude (Amp in Micronvolts = μV) and Latency (Lat in Milliseconds = ms) Results in Both Studied Groups, Neurofibromatosis Type 1 (NF1) Patients and Healthy Subjects |
The results obtained show a statistically significant reduction in the P1 wave amplitude in the 120ʹ, 60ʹ, and 15ʹ frequencies in NF1 patients, compared to controls.
Similarly, the latency of the P1 wave is increased in NF1 patients compared to the healthy group at the stimulation frequencies 120ʹ, 60ʹ, and 15ʹ (Table 1).
The data of computerized campimetry (GHT, CS, MD and PSD) were compared between the 2 groups and are illustrated in Table 2.
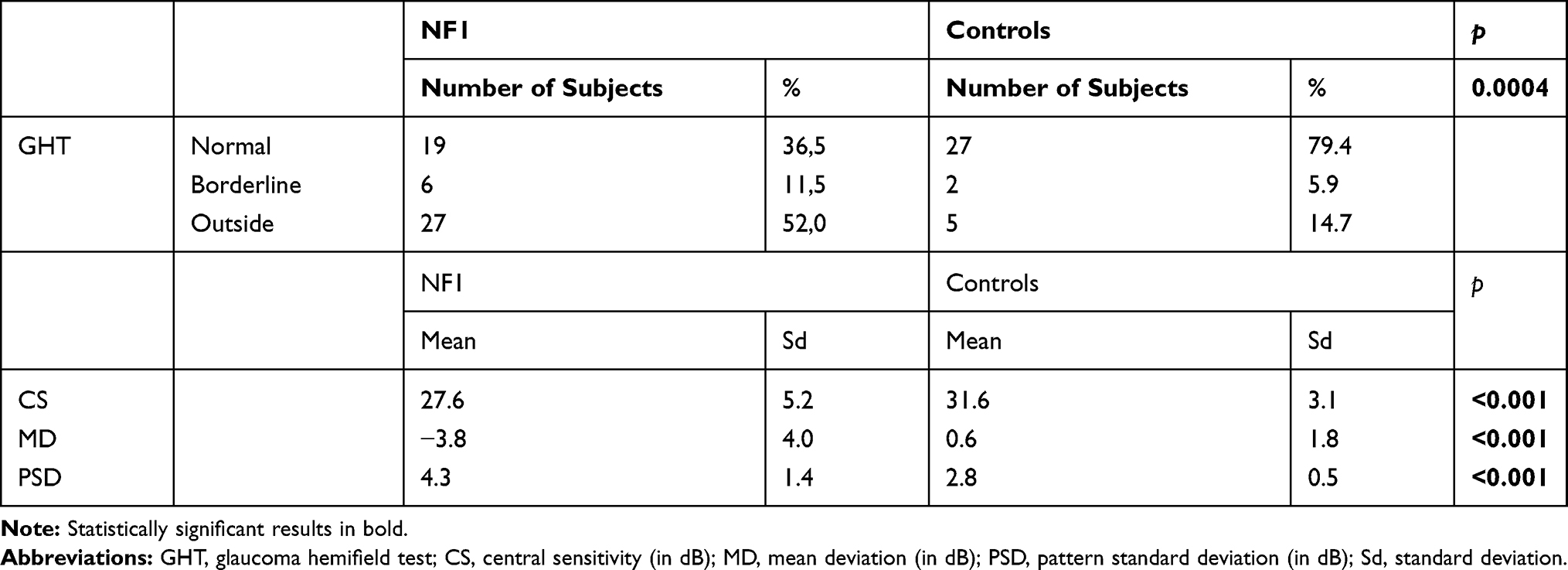 |
Table 2 Results of the Visual Field Carried Out by Means of a Computerized Frequency Doubling Technology (FDT) Matrix Perimetry in Both Studied Groups, Neurofibromatosis Type 1 (NF1) Patients and Healthy Controls |
The GHT was found within the limit in 79.4% of the cases in the healthy group, while in the NF1 group, the percentage was consistently lower: 36.5%.
Similar results were obtained for the remaining perimeter indices. CS, MD, and PSD were found to be considerably reduced in patients with NF1 (Table 2). T-test did not show any significant difference in p-VEPs results between males and females. Linear regression of p-VEPs with age in the NF1 group did not show any significant results. Complete radiologic, ophthalmologic, and dermatologic findings are displayed in additional material (see Supplementary Tables 1–3).
Discussion
The objective of our study was to examine the function of retrobulbar visual pathways in NF1 patients compared to a group of healthy subjects using two instrumental tests, the pattern VEPs and the perimetry with FDT Matrix. (Figures 1 and 2)
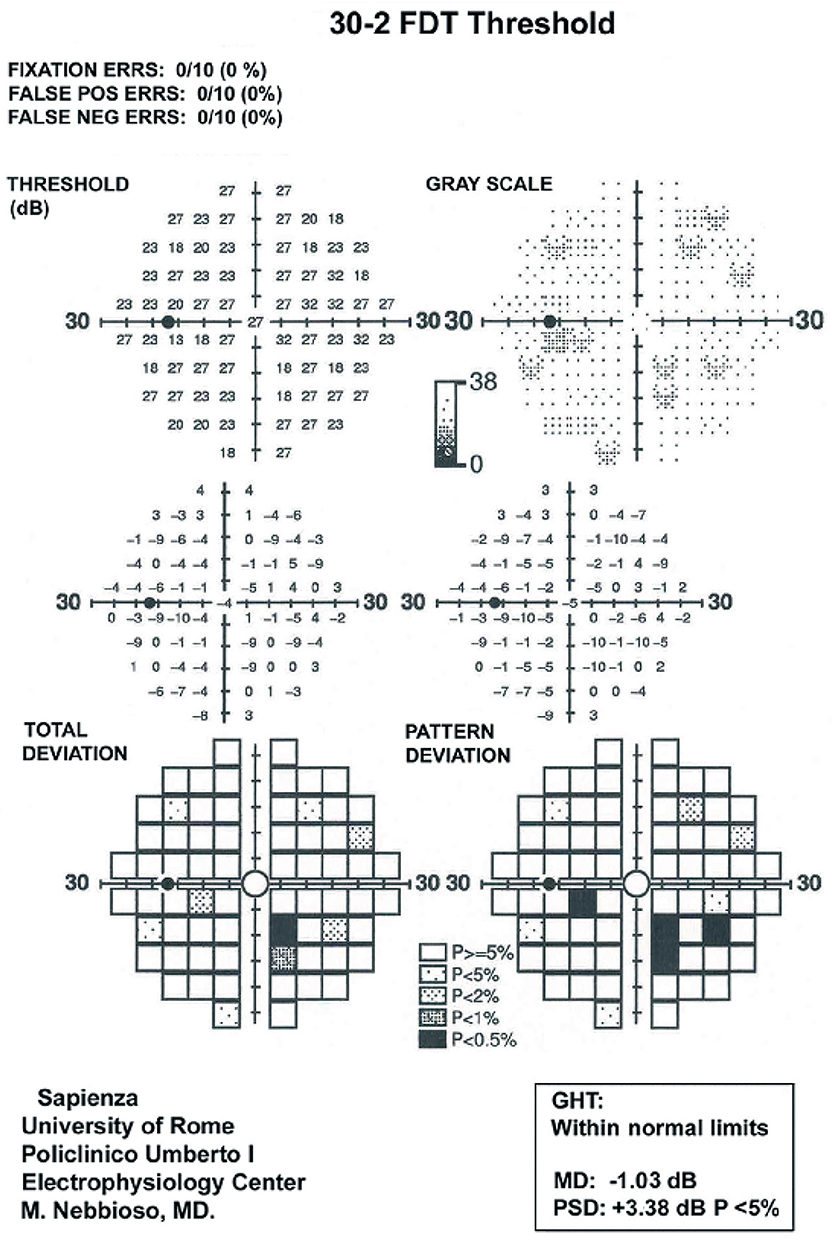 |
Figure 2 Altered perimetry, performed with frequency doubling technology (FDT) Matrix. |
The examination of p-VEPs showed, in the NF1 group, an increase in latency time and a simultaneous reduction in amplitude, both results were statistically significant (Table 2).
The presence of alterations in the studied electrophysiological parameters is indicative of a disorder of nerve conduction both qualitative, expressed by the increase in latency time, and quantitative expressed by the reduction in amplitude.19–21 In agreement with Rosenbaum et al, the delay of the transmission of the visual impulse could be explained by the demyelination of the nerve fibers constituting the optical pathways. Neurofibromin regulates the transduction of the intracellular signal that leads to the production of myelin in Schwann cells.22 In NF1 patients, the mutation of this gene may alter the molecular cascade, related to the Ras family proteins, responsible for the activation at a nuclear level of a pattern of genes stimulating the process of myelination.11,22,23
Through the p-VEPs, we analyzed the transmission of the visual impulse along the nerve fibers constituting the optical pathways up to the calcarine cortex. The peripheral and intermediate fibers were explored through the p-PEVs at 120ʹ and 60′ (low and medium spatial frequencies), which in the control group reported higher conduction velocity values than those reported for central fibers, examined with the p-VEPs 15ʹ (high spatial frequencies), results congruous with existing literature.24,25 In the NF1 group, the p-VEPs 120ʹ and 60ʹ showed a statistically significant increase in latency and a reduction in amplitude. These data may indicate the suffering of the outermost fibers of the visual pathways.
Although the results obtained for the p-VEPs 15ʹ showed significant differences between the NF1 and the control group in both amplitude and latency we do not consider these results suggestive of a potential alteration in nerve conduction. In fact, even though the observed differences between p-VEPs 15ʹ amplitude and latency between the 2 groups are statistically significant, the results still are comprised in the physiological spectrum. No consistent information can be deduced concerning the impairment of the nervous stimulus conduction in the central part of the nerve studied with the p-VEPs 15ʹ. In NF1 patients, therefore, the functionality of the papillo-macular bundle would seem more conserved than the outermost fibers of the optical pathways. A minor impairment of the central fibers could also explain the absence of alterations of visual perception, both subjective and objective. The subjects selected for our study had visual acuity greater than or equal to 0.00 logMAR and did not complain of alterations of the visual acuity.
The analysis of the visual field parameters found also significant differences between healthy controls and NF1 patients.
The NF1 group showed a statistically significant reduction of all perimetric indices, thus revealing an overall alteration of the visual field due to the presence of both generalized (MD) and localized (PSD) defects, also present in the comparison between the upper and lower hemi-camps (GHT). The CS threshold was also reduced in NF1 patients, although it appeared to be less involved than the previous perimetric indexes (Table 2). This result is in line with what has already been stated regarding the p-VEPs: the papillo-macular beam is less affected by the alterations and this causes the preservation of the CS rather than the peripheral one.
The alterations of the perimetric indexes described may, on the other hand, be traced back to the attention disorder often present in NF1 patients.26–28 In the evaluation of the results, individual variability must also be considered in tests such as computerized perimetry FDT, in which it is not possible to exclude the psychophysical component.
The already described cognitive deficits and behavioral abnormalities in NF1 subjects do not allow, however, to univocally explain the campimetric anomalies underlined in our patients, as they are supported, in our work, by the objective data of electrophysiological examinations.
In fact, we believe that p-VEPs guarantee a high degree of sensitivity and objectivity of the results especially if the patient is continuously checked by the examiner. Therefore, in our opinion, the observed alterations of p-VEPs are likely to be related to optic nerve conduction alterations rather than to the poor attention span of NF1 patients.29 Interestingly no significant correlation was found comparing perimetric or electrophysiological results by age (linear regression not significant) or gender group (T-test not significant). This result shows how the subclinical deficit in the transmission through the optic pathway may not be progressive. It may be an innate characteristic not conditioned by age or gender. To the best of our knowledge, we have found only one previously published article investigating the connections between NF-1 and p-VEPs, conducted by a team of neurologists led by Jabbari B. In 1985 they found an increase in the latency and a reduction in the amplitude of nerve impulses, suggesting p-VEPs as a valuable screening test in asymptomatic NF1 patients.30 The modern technology used for our tests allows us to acquire new information that confirms and expand the considerations that emerged in the work mentioned above.
Our study shows that, in subjects suffering from NF1, the conduction of visual stimuli along the retrobulbar optic pathways is significantly slower compared to the subjects of the control group. There is also a reduction in the amplitude of the electrical impulse, which indicates an objective worsening of the perceived image, although patients do not report alterations in visual acuity or in the subjective perception of the images. The electrophysiological examinations can, therefore, be considered, in the ophthalmologic field, a further useful tool for the study and monitoring of NF1 patients; adding to those already used in clinical practice such as the biomicroscopic examination of the anterior segment, the examination of the fundus oculi and OCT, which allow to identify some of the characteristic signs of the disease (Lisch nodules, microvascular anomalies and choroidal spots).31–34
In conclusion, neurofibromatosis is a complex and heterogeneous disease that requires an integrated multidisciplinary approach. To fully understand all the aspects of this complex pathology it is necessary to continue the studies, expanding the sample under examination and promoting an interdisciplinary work that involves the collaboration of different professional figures, among whom the ophthalmologist can play a key role.
Abbreviations
p-VEPs, pattern visual evoked potentials; FDT, frequency doubling technology; CS, central sensitivity; MD, mean deviation; PSD, pattern standard deviation; GHT, glaucoma hemifield test; NF1, Neurofibromatosis type 1.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Funding
No funding was received for this research.
Disclosure
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus, membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
References
1. Uusitalo E, Leppävirta J, Koffert A, et al. Incidence and mortality of neurofibromatosis: a total population study in Finland. J Invest Dermatol. 2015;135(3):904–906. doi:10.1038/jid.2014.465
2. Moramarco A, Miraglia E, Mallone F, et al. Retinal microvascular abnormalities in neurofibromatosis type 1. Br J Ophthalmol. 2019;103(11):1590–1594. doi:10.1136/bjophthalmol-2018-313002
3. Moramarco A, Lambiase A, Mallone F, Miraglia E, Giustini S. A characteristic type of retinal microvascular abnormalities in a patient with neurofibromatosis type 1. Clin Ter. 2019;170(1):e4–e9. doi:10.7417/CT.2019.2101
4. Kinori M, Hodgson N, Zeid JL. Ophthalmic manifestations in neurofibromatosis type 1. Surv Ophthalmol. 2018;63(4):518–533. doi:10.1016/j.survophthal.2017.10.007
5. Leppävirta J, Kallionpää RA, Uusitalo E, et al. Congenital anomalies in neurofibromatosis 1: a retrospective register-based total population study. Orphanet J Rare Dis. 2018;13(1):5. doi:10.1186/s13023-017-0756-4
6. Hirbe AC, Gutmann DH. Neurofibromatosis type 1: a multidisciplinary approach to care. Lancet Neurol. 2014;13(8):834–843. doi:10.1016/S1474-4422(14)70063-8
7. Gutmann DH, Ferner RE, Listernick RH, Korf BR, Wolters PL, Johnson KJ. Neurofibromatosis type 1. Nat Rev Dis Primers. 2017;3:17004. doi:10.1038/nrdp.2017.4
8. Basu TN, Gutmann DH, Fletcher JA, Glover TW, Collins FS, Downward J. Aberrant regulation of ras proteins in malignant tumour cells from type 1 neurofibromatosis patients. Nature. 1992;356(6371):713–715. doi:10.1038/356713a0
9. Karlsgodt KH, Rosser T, Lutkenhoff ES, Cannon TD, Silva A, Bearden CE. Alterations in white matter microstructure in neurofibromatosis-1. PLoS One. 2012;7(10):e47854. doi:10.1371/journal.pone.0047854
10. López-Juárez A, Titus HE, Silbak SH, et al. Oligodendrocyte Nf1 controls aberrant notch activation and regulates myelin structure and behavior. Cell Rep. 2017;19(3):545–557. doi:10.1016/j.celrep.2017.03.073
11. Mayes DA, Rizvi TA, Titus-Mitchell H, et al. Nf1 loss and Ras hyperactivation in oligodendrocytes induce NOS-driven defects in myelin and vasculature. Cell Rep. 2013;4(6):1197–1212. doi:10.1016/j.celrep.2013.08.011
12. Koini M, Rombouts SARB, Veer IM, et al. White matter microstructure of patients with neurofibromatosis type 1 and its relation to inhibitory control. Brain Imaging Behav. 2017;11(6):1731–1740. doi:10.1007/s11682-016-9641-3
13. DiPaolo DP, Zimmerman RA, Rorke LB, et al. Neurofibromatosis type 1: pathologic substrate of high-signal-intensity foci in the brain. Radiology. 1995;195(3):721–724. doi:10.1148/radiology.195.3.7754001
14. Baudou E, Nemmi F, Biotteau M, et al. Can the cognitive phenotype in neurofibromatosis type 1 (NF1) be explained by neuroimaging? A review. Front Neurol. 2020;10:1373. doi:10.3389/fneur.2019.01373
15. Bulgheroni S, Taddei M, Saletti V, et al. Visuoperceptual impairment in children with NF1: from early visual processing to procedural strategies. Behav Neurol. 2019;2019:7146168. doi:10.1155/2019/7146168
16. Violante IR, Ribeiro MJ, Cunha G, et al. Abnormal brain activation in neurofibromatosis type 1: a link between visual processing and the default mode network. PLoS One. 2012;7(6):e38785. doi:10.1371/journal.pone.0038785
17. Neurofibromatosis. Conference statement. National Institutes of Health Consensus Development Conference. Arch Neurol. 1988;45(5):575–578.
18. Odom JV, Bach M, Brigell M, et al. ISCEV standard for clinical visual evoked potentials: (2016 update). Doc Ophthalmol. 2016;133(1):1–9. doi:10.1007/s10633-016-9553-y
19. Fishman GA, Birch DG, Holder GE, Brigell MG. Electrophysiologic Testing in Disorders of the Retina, Optic Nerve, and Visual Pathway.
20. Hemptinne C, Liu-Shuang J, Yuksel D, et al. Rapid objective assessment of contrast sensitivity and visual acuity with sweep visual evoked potentials and an extended electrode array. Invest Ophthalmol Vis Sci. 2018;59(2):1144–1157. doi:10.1167/iovs.17-23248
21. Nebbioso M, Barbato A, Pescosolido N. Scotopic microperimetry in the early diagnosis of age-related macular degeneration: preliminary study. Biomed Res Int. 2014;2014:671529. doi:10.1155/2014/671529
22. Rosenbaum T, Kim HA, Boissy YL, Ling B, Ratner N. Neurofibromin, the neurofibromatosis type 1 Ras-GAP, is required for appropriate P0 expression and myelination. Ann N Y Acad Sci. 1999;883:203–214. doi:10.1111/j.1749-6632.1999.tb08583.x
23. Shin J, Padmanabhan A, de Groh ED, et al. Zebrafish neurofibromatosis type 1 genes have redundant functions in tumorigenesis and embryonic development. Dis Model Mech. 2012;5(6):881–894. doi:10.1242/dmm.009779
24. Nebbioso M, Gregorio FD, Prencipe L, Pecorella I. Psychophysical and electrophysiological testing in ocular hypertension. Optom Vis Sci. 2011;88(8):E928–E939. doi:10.1097/OPX.0b013e31821c6ca4
25. Nebbioso M, Steigerwalt RD, Pecori-Giraldi J, Vingolo EM. Multifocal and pattern-reversal visual evoked potentials vs. automated perimetry frequency-doubling technology matrix in optic neuritis. Indian J Ophthalmol. 2013;61(2):59–64. doi:10.4103/0301-4738.99638
26. Miguel CS, Chaim-Avancini TM, Silva MA, Louzã MR. Neurofibromatosis type 1 and attention deficit hyperactivity disorder: a case study and literature review. Neuropsychiatr Dis Treat. 2015;11:815–821. doi:10.2147/NDT.S75038
27. Torres Nupan MM, Velez Van Meerbeke A, López Cabra CA, Herrera Gomez PM. Cognitive and Behavioral Disorders in Children with Neurofibromatosis Type 1. Front Pediatr. 2017;5:227. doi:10.3389/fped.2017.00227
28. Lion-François L, Herbillon V, Peyric E, et al. Attention and Executive disorders in neurofibromatosis 1: comparison between NF1 with ADHD symptomatology (NF1 + ADHD) and ADHD Per Se. J Atten Disord. 2017:1087054717707579. doi:10.1177/1087054717707579.
29. Ribeiro MJ, d’Almeida OC, Ramos F, Saraiva J, Silva ED, Castelo-Branco M. Abnormal late visual responses and alpha oscillations in neurofibromatosis type 1: a link to visual and attention deficits. J Neurodev Disord. 2014;6(1):4. doi:10.1186/1866-1955-6-4
30. Jabbari B, Maitland CG, Morris LM, Morales J, Gunderson CH. The value of visual evoked potential as a screening test in neurofibromatosis. Arch Neurol. 1985;42(11):1072–1074. doi:10.1001/archneur.1985.04060100054022
31. Moramarco A, Giustini S, Nofroni I, et al. Near-infrared imaging: an in vivo, non-invasive diagnostic tool in neurofibromatosis type 1. Graefes Arch Clin Exp Ophthalmol. 2018;256(2):307–311. doi:10.1007/s00417-017-3870-z
32. Moramarco A, Giustini S, Miraglia E, Sacchetti M. SD-OCT in NIR modality to diagnose retinal microvascular abnormalities in neurofibromatosis type 1. Graefes Arch Clin Exp Ophthalmol. 2018;256(9):1789–1790. doi:10.1007/s00417-018-4028-3
33. Moramarco A, Sacchetti M, Franzone F, et al. Ocular surface involvement in patients with neurofibromatosis type 1 syndrome. Graefes Arch Clin Exp Ophthalmol. 2020;258(8):1757–1762. doi:10.1007/s00417-020-04717-5
34. Nebbioso M, Grenga R, Karavitis P. Early detection of macular changes with multifocal ERG in patients on antimalarial drug therapy. J Ocul Pharmacol Ther. 2009;25(3):249–258. doi:10.1089/jop.2008.0106
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.